Embed Size (px)
Citation preview
548 Copyright © SLACK Incorporated
FEATURE
Diagnostic Approach to Limp in Children Ami P. Shah, MD, MPH; Sean Indra, MD; Nirupama Kannikeshwaran, MD; Earl Hartwig, MD; and Deepak Kamat, MD, PhD
Abstract“Limp” is a common complaint of chil-
dren presenting to the emergency de-
partment or physician’s office. For most
patients presenting with limp, the diagno-
sis and management can be completed
in the physician’s office or emergency de-
partment by gathering a detailed history,
performing a careful physical examination,
and requesting a few laboratory and imag-
ing studies. This article reviews common
causes of atraumatic limp in children and
discusses the evaluation and manage-
ment of these conditions. [Pediatr Ann.
2015;44(12):548-550, 552-554, 556.]
Limp is a common presentation in children. There are many causes for limp in children, so
it is important to identify the benign causes of limp by taking a good his-tory and performing a detailed physi-cal examination so that unnecessary laboratory and imaging studies are not performed. In this article, we discuss the common causes and management of atraumatic limp in children.
ILLUSTRATIVE CASES Case 1
A 3-year-old boy presented to the emergency department (ED) with complaint of a limp for the past 10 days noted by the parents. His fam-
ily denied any trauma, fever, or recent upper respiratory infection symptoms. The child had normal vital signs and physical examination. Would you re-assure parents that there is probably nothing wrong or would you run a few tests?
Case 2An 11-month-old healthy boy pre-
sented to the ED with refusal to stand or crawl. His parents noted a low-grade fever and a rash. On examination, the child was afebrile and had an ery-thematous rash that was target-shaped over the anterior chest and extremities. Both knees were mildly swollen; how-ever, the joints were nonerythematous,
Ami P. Shah, MD, MPH, is an Attending Physi-
cian, Pediatric Emergency Services, Children’s
Hospital of Nevada. Sean Indra, MD, is a Fellow,
Pediatric Emergency Medicine, Children’s Hospi-
tal of Michigan. Nirupama Kannikeshwaran, MD,
is an Associate Professor of Pediatrics and Emer-
gency Medicine, Children’s Hospital of Michigan.
Earl Hartwig, MD, is a Clinical Associate Professor
of Pediatrics and Emergency Medicine, Children’s
Hospital of Michigan. Deepak Kamat, MD, PhD,
is a Professor of Pediatrics, and the Vice Chair
of Education, Department of Pediatrics, Wayne
State University; and a Designated Institutional
Official, Children’s Hospital of Michigan. Address correspondence to Deepak Kamat,
MD, PhD, Children’s Hospital of Michigan, 3901 Beaubien Boulevard, Detroit, MI 48201; email: [email protected].
Disclosure: The authors have no relevant fi-nancial relationships to disclose.
doi: 10.3928/00904481-20151112-01
© S
hutte
rsto
ck
PEDIATRIC ANNALS • Vol. 44, No. 12, 2015 549
FEATURE
not warm, and had full range of mo-tion without any discomfort. What will your approach be for this patient?
Case 3A 2-year-old healthy girl presented
to the ED with refusal to walk since the morning. She had a runny nose and cough for a few day prior. She had a normal physical examination but re-fused to bear weight on her right side. There was no joint erythema, swell-ing, tenderness, or signs of trauma in the lower extremity. What tests will aid in the diagnosis?
EPIDEMIOLOGY“Limp” represents a common com-
plaint in children presenting to the ED. Although the majority of limping is related to trauma, atraumatic limp is reported in 1.8 per 1,000 children younger than age 14 years.1,2 The av-erage age of presentation is 4 years, and it typically affects boys more commonly than girls. Most children present with a unilateral limp that is painful. Slightly less than half of these patients have a preceding illness. The differential diagnosis for limp is ex-pansive and it is important to discern the benign from life-threatening con-ditions that cause an atraumatic limp in children (Table 1). Ultimately, for most patients presenting with limp, the diagnosis and management can be completed in the physicians’ office or ED.
ANATOMY OF GAITTo understand what causes a child
to limp, it is necessary to understand the anatomy of a normal gait. A child develops a mature gait pattern at age 3 years and it consists of a stance phase and swing phase.3 Disordered gait can be classified as antalgic and nonantal-gic. An antalgic gait results from pain in the affected extremity, resulting in a shortening of the stance phase and an
increase of the swing phase. This type of gait results typically from trauma or an infection.4 Types of nonantalgic gait include a Trendelenburg gait, in which the pelvis exhibits a downward tilt toward the unaffected side during the swing phase because of weakness in the contralateral gluteus medius muscle. This type of gait is usually seen in disorders of the hip such as developmental dysplasia of the hip (DDH), Legg-Calvé-Perthes (LCP) disease, or slipped capital femoral epiphysis (SCFE). A steppage gait
results from excessive flexion of the hip and knee joints during the swing phase due to an inability to dorsiflex the foot. A steppage gait is seen in patients with cerebral palsy and other neurologic disorders. Lastly, a vault-ing or circumduction gait occurs due to hyperextension and locking of the knees at the end of the stance phase and the child must vault over the af-fected extremity. This gait is usually associated with a limb-length discrep-ancy or a mechanical disorder leading to abnormal knee mobility.
TABLE 1.
Differential Diagnosis of Atraumatic Limp
Infectious Septic arthritis
Osteomyelitis
Discitis
Lyme disease
Psoas abscess
Gonococcal arthritis
Inflammatory Transient synovitis
Serum sickness
Henoch-Schonlein purpura
Rheumatic fever
Ankylosing spondylitis
Systemic lupus erythematous
Vascular Legg-Calve-Perthes disease
Osteonecrosis
Sickle cell disease
Neoplastic Leukemia
Tumors such as osteoblastoma or osteosarcoma
Congenital Developmental dysplasia of the hip
Other Intraabdominal
Inguinal hernia
Appendicitis
Pyelonephritis
Pelvic inflammatory disease
Intracranial pathology
Intracranial space occupying lesion (eg, tumor or abscess)

550 Copyright © SLACK Incorporated
FEATURE
HISTORY, PHYSICAL EXAMINATION, AND INVESTIGATIONS TO BE CONSIDERED IN A PATIENT WITH NEW-ONSET LIMP History
Evaluation of a limping child should begin with a thorough history elicited from both the child as well as the caregiver. The age of the child at onset of the limp helps to narrow the differential diagnoses. DDH is com-monly seen up to age 3 years whereas LCP disease, juvenile idiopathic ar-thritis (JIA), and leukemia should be considered among children ages 4 to 10 years. Joint sprains, overuse syn-dromes, SCFE, and tumors should be considered in the adolescent age group.4
Fever is an important historic fac-tor, as it may suggest an infectious (eg, osteomyelitis, septic arthritis or Lyme arthritis) or an inflammatory (eg, transient synovitis, discitis) cause for limping. Rheumatologic and onco-logic processes, such as JIA and leu-kemia, are less commonly associated with fever but should be considered in the differential diagnosis in the pres-ence of systemic symptoms such as weight loss, night sweats, loss of ap-petite, bone pain, or fatigue.5 In the setting of a recent febrile viral illness or streptococcal infection, postin-fectious causes of limping are more likely and include transient synovitis, myositis, or serum sickness.
Pain associated with limp may pro-vide clues as to the cause of the limp. Pain that is constant, localizing, and reproducible usually represents a frac-ture, osteomyelitis, or septic arthritis.6 Children may also have referred pain to the knee from disorders of the hip such as LCP disease or SCFE. Dif-ferentiating true pain from weakness is important, as weakness may be a clinical manifestation of a central or peripheral nervous system disorder.
Back pain or lateral thigh pain may indicate lumbar spinal disorders such as discitis, herniated disc, or vertebral fracture. Additionally, symptoms such as incontinence or leg weakness also suggest spinal cord lesions or pelvic mass.
The duration of the limp can help to differentiate between acute versus chronic etiologies. Typically, acute- onset limp presents in the setting of trauma or an infectious cause, such as a septic arthritis or osteomyelitis. A longer duration or insidious onset of symptoms may be more indicative of LCP disease, SCFE, or a rheumato-logic etiology.
Physical ExaminationA thorough physical examination
with the child completely undressed should be performed on all children presenting with a limp. The height and weight of the child should be noted and, if possible, compared to that from prior visits, as poor growth may be an indicator of an underlying chronic dis-ease. A complete neurologic examina-tion assessing for tone (hypotonia or spasticity), hypo- or hyperreflexia, presence of clonus, or loss of sensa-tion should be performed to rule out central or peripheral nervous system pathologies. Examination of the back/spine for curvature and point tender-ness is also an important aspect of the physical examination.
The gait of the patient should be as-sessed while they are wearing a short gown and walking in bare feet. Each leg should be assessed individually through the swing and stance phase.
Look for erythema, swelling, or signs of trauma such as abrasions, lacerations, or puncture wounds. The feet, legs, hips, and back should be palpated in small segments at a time to elicit tenderness or note any “step offs” or masses. Passive and active range of motion of joints should be as-
sessed and compared to the opposite side.
Specific clinical tests may have to be performed to confirm or rule out specific cause for a limp. For the Tren-delenburg test, the child stands on the affected leg and the observer looks for the drop of the pelvis toward the un-affected side. A positive test indicates disorders of the hip such as DDH, LCP disease, or SCFE. In the Galeazzi sign test, the child lies in the supine posi-tion with both hips and knees flexed. The practitioner observes heights of the knees and if one side is lower than the other, the test is positive, reveal-ing a limb-length discrepancy with the lower side shorter than the other. The Flexion, Abduction and External Ro-tation test is performed by having the child lay supine while the examiner flexes, abducts, and externally rotates the hip joint. If this results in hip pain or limitation of flexion, it implies a disorder of the sacroiliac joint.
One should also examine the in-guinal region to rule out hernias and scrotal/testicular lesions.
Laboratory Evaluation The differential diagnosis consid-
ered in a patient dictates the laboratory evaluation to be performed. When an infectious or inflammatory cause for the limp is suspected on clinical eval-uation, laboratory tests to be consid-ered include a complete blood count (CBC), blood culture, and acute phase reactants such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). A clinical guideline devel-oped by Kocher et al.7,8 proposed that a history of fever, nonweight-bearing on the affected side, ESR >40 mm/h, and serum white blood cell count of >12,000 cells/mm3 is indicative of septic arthritis as opposed to transient synovitis. They found that if only 1 of the 4 was present, the predicted prob-ability for septic arthritis was about
continued on page 552

552 Copyright © SLACK Incorporated
FEATURE
3%, but it increased to 99% when all four criteria were present. If the pa-tient lives in an area where Lyme dis-ease is endemic, it may be pertinent to obtain a two-step serologic test includ-ing an enzyme-linked immunosorbent assay followed by a confirmatory Western blot for Lyme disease. The synovial fluid can be tested for Lyme polymerase chain reaction as well. If there is a high suspicion for a septic joint, synovial fluid (obtained at bed-side or in the operating room) needs to be sent for Gram stain, cultures, white blood cell count, glucose, and protein analysis. If there is clinical suspicion for rheumatologic diseases, antinucle-ar antibody titers and rheumatoid fac-tor may need to be checked.
Imaging StudiesRadiography and ultrasonogram
(US) of the hip are the commonly used imaging modalities to evaluate a child with a limp. X-ray of the hip is particularly useful in the diagnosis of LCP disease and SCFE, whereas US of the hip is useful when DDH or sep-tic arthritis are suspected. Plain radio-graphs are not particularly sensitive in diagnosing acute osteomyelitis, so in those cases nuclear medicine scans can be used; however, they have low specificity in diagnosing acute os-teomyelitis. Recently, magnetic reso-nance imaging (MRI) has been used with high frequency to evaluate chil-dren with suspected acute or chronic osteomyelitis. MRI is also very use-ful in diagnosing discitis. A computed tomography (CT) scan is helpful in diagnosing chronic osteomyelitis as it clearly delineates cortical destruction as compared with MRI.9
COMMON CAUSES OF LIMP Inflammatory Conditions
The most common cause of non-traumatic limp in children age 10 years or younger is transient synovi-
tis.10 The exact etiology of this is un-clear, although the most commonly accepted explanation is an inflamma-tory reaction following a viral illness. Typical presentation is a limp that is noted in a child after a viral upper respiratory infection. On clinical ex-
amination, the child is well appearing, has full range of motion of the joints, and is usually able to bear weight after taking nonsteroidal anti-inflammatory drugs (NSAIDs). Laboratory evalu-ation, including CBC and serum in-flammatory markers such as CRP and ESR, are usually within normal limits. Symptoms usually resolve in 1 to 2 weeks. Rest and NSAIDs are the treat-ment of choice.
Other inflammatory causes of a nontraumatic limp in children include serum sickness, Henoch-Schonlein purpura (HSP), and rheumatologic disorders. Serum sickness is a type III hypersensitivity reaction to recent ill-ness or medication. Most commonly involved medications include the pen-icillins, cephalosporins, and NSAIDs. The child typically presents with fe-ver, rash, and joint pain or swelling. Rash typically resembles a target le-sion. Symptoms are noted 7 to 21 days after antigen exposure. Treatment is largely supportive care. If the child is taking antibiotics and if the medi-cation is suspected to be the cause of serum sickness, then it should be dis-continued immediately.
HSP is a vasculitis that affects young children. Purpuric rash is noted in the dependent areas after a viral ill-ness or vaccination. Clinical presen-tation includes low-grade fever, rash, and arthritis that usually involves the lower extremity joints. Joint involve-ment is inflammatory in origin, is nonerosive, and does not lead to per-manent damage. Symptoms respond well to NSAIDs. Gastrointestinal manifestations include nausea, vom-iting, and abdominal pain. Children with HSP are at higher risk for intus-susception and nephritis. Laboratory evaluation may show elevated serum inflammatory markers. Treatment is largely supportive. All symptoms re-solve in most patients within 4 weeks.
Acute rheumatic fever (ARF) is an inflammatory disorder with multior-gan involvement and is caused by an immune response to group A strepto-coccal infection. The Jones criteria are used for the diagnosis of rheumatic fe-ver. Major criteria include carditis, ar-thritis, chorea, erythema marginatum, and subcutaneous nodules. Minor criteria include fever, arthralgia, pro-longed PR interval, and elevated acute phase reactants. The presence of two major criteria, or one major and two minor criteria, along with laboratory evidence of a preceding streptococcal infection indicates a high likelihood of ARF.11
Rheumatologic disorders such as JIA present with erythematous swol-len joints with pain that typically im-proves with activity. This diagnosis should be considered in a child young-er than age 16 years who complains of early morning joint pain. It can affect single or multiple joints. Eye involve-ment in the form of uveitis is also commonly noted.3,5,10
Infectious ConditionsOsteomyelitis and septic arthritis
of the hip can present as limp, and
Radiography and ultrasonogram of the hip are the commonly used imaging modalities to
evaluate a child with a limp.
continued from page 550
PEDIATRIC ANNALS • Vol. 44, No. 12, 2015 553
FEATURE
their clinical presentation may mimic that of a transient synovitis. Early diag-nosis and timely treatment are required to prevent serious consequences such as joint damage and related complica-tions. Infection may reach the area via blood stream, direct contamination, or from infection of nearby skin (such as cellulitis). The most common causative organism in children is Staphylococcus aureus. Other organisms that can cause septic arthritis include Escherichia coli, group B streptococci in neonates, and Neisseria gonorrhoeae in a sexu-ally active teenager.
Septic arthritis is more common in children in the age group of 2 to 3 years. Fever may be more profound and the child may appear sicker compared to those with transient synovitis. Cry-ing when the child is picked up or with every diaper change should be a clue to consider septic arthritis, as should if the child refuses to move and bear weight on the affected extremity. Poor feeding and irritability may be seen in younger children and infants.3,9,10
Evaluation for these patients in-cludes CBC, blood culture, ESR, and CRP. An elevated CBC and inflamma-tory markers are noted in patients with osteomyelitis and septic arthritis. A clinician can use the Kocher criteria,7,8 which combine clinical and laboratory criteria, to consider septic arthritis.
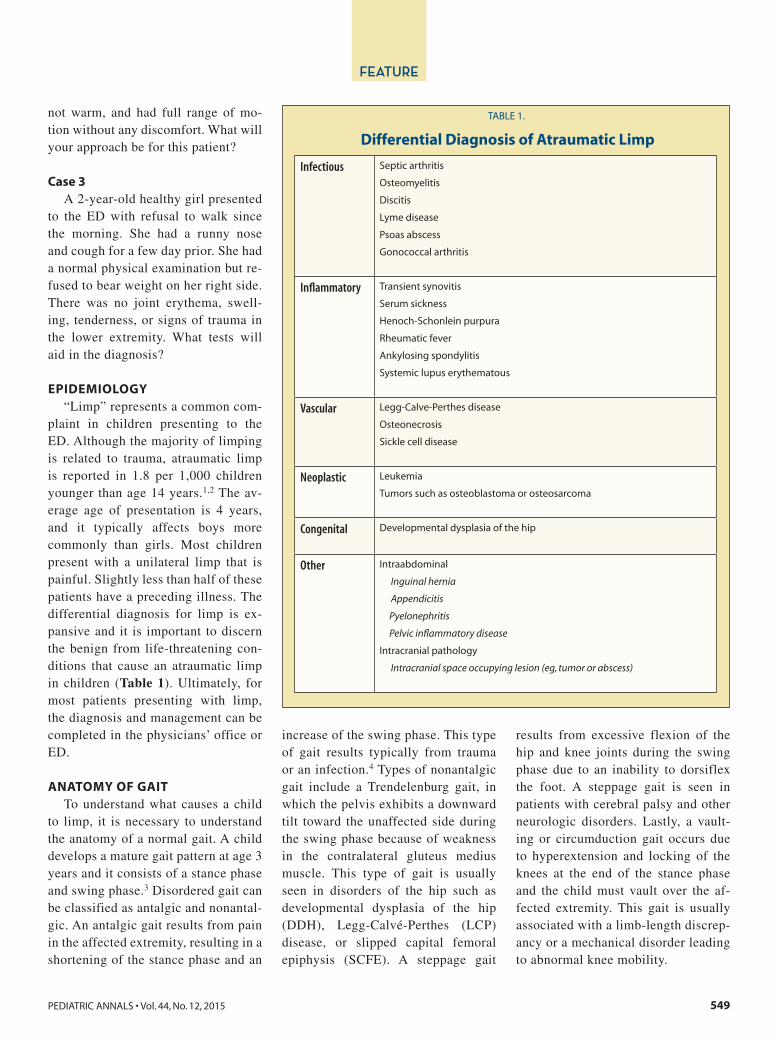
US of the affected joint should be obtained. US is a useful test to iden-tify effusion, although it cannot dis-tinguish between clear and purulent fluid.12,13 If the index of suspicion for septic arthritis is high, joint aspiration should be performed and the synovial fluid should be obtained for evalua-tion. Plain radiography has limited utility in children younger than age 9 years presenting with nontraumatic limp.14,15 Plain radiography findings in osteomyelitis include periosteal bone thickening, lytic lesions, and new bone apposition (Figure 1). These findings may not be apparent until 10 to 14 days of illness.16 The sensitivity of US for diagnosis of osteomyelitis ranges from 32% to 72% based on the stage of the
illness. The sensitivity can be further improved with use of high-resolution and power Doppler sonography.16,17 Deep soft tissue swelling, subperiso-teal abscess, fluid adjacent to the bone, cortical erosion, and increased flow within periosteum are some of the find-ings noted on US that are suggestive of osteomyelitis. Findings can be detect-ed by US much earlier than by plain radiography. CT scan is the preferred test for diagnosis of cortical destruc-tion in chronic osteomyelitis. Other-wise, MRI is the diagnostic study of choice in children with suspected acute or chronic osteomyelitis9 (Figure 2). Nuclear medicine scans are not used as often because of their low specificity in diagnosing osteomyelitis.
Early antibiotic therapy and ortho-pedic consultation are required for the management of these patients. Par-enteral clindamycin or vancomycin is the drug of choice in communities where methicillin-resistant S. aureus (MRSA) is prevalent. If the commu-nity prevalence of MRSA is <10%,
Figure 2. A magnetic resonance image showing osteomyelitis of the proximal tibia.
Figure 1. An X-ray of a foot showing osteomyelitis of the proximal end of the proximal phalanx of the 4th toe.
554 Copyright © SLACK Incorporated
FEATURE
intravenous nafcilin or oxacillin or a first-generation cephalosporin can be started as empiric therapy. Kingella kin-gii is a gram-negative coccobacillus and has been a common cause of osteoartic-ular infections in children younger than age 3 years. In this age group, empiric coverage with cefazolin or ceftriaxone is recommended in addition to the cov-erage for MRSA. Duration of therapy ranges from 4 to 6 weeks.18 Salmonella osteomyelitis should be a consideration in children with sickle cell disease.19
Discitis is an inflammation of the disc space and adjacent vertebral end plates that typically affects the lumbar spine. Neonates and young children are more susceptible to discitis because of char-acteristic anatomy of blood vessels in this age group: the small blood vessels terminate adjacent to the intervertebral disc, which renders the disc space more susceptible to infection. Also, children have a large network of interosseous col-lateral arteries as compared with adults.9 The possible role of infection in discitis is somewhat controversial, but the most commonly considered organisms are coagulase negative staphylococci and S. aureus. Presentation of discitis can be very nonspecific, and a high index of suspicion is required for diagnosis. Clin-ical presentation ranges from refusal
to walk or bear weight, and irritability on spine immobility.20 Point tenderness over the spine can aid in the diagnosis. Inflammatory markers may or may not be elevated early in the course of the ill-ness. Plain radiographs show narrowing of the disc space and end plate irregular-ities. These findings are noted only after 2 to 4 weeks of illness. MRI is the most sensitive and specific test for diagno-sis.20 Treatment includes consideration of parenteral antibiotics and immobili-zation of the spine. Operative treatment is rarely necessary.
Although rare, intracranial abscess should be considered in a patient with fever and limp. It is more prevalent in patients with congenital heart disease. It results from extension of local infection or due to septic emboli. The most com-mon organisms cultured are from the Streptococcus milleri group. CT scan of the head with contrast is the diagnostic test of choice. Therapy includes abscess drainage and intravenous antibiotics. Initial therapy should be with vancomy-cin and ceftriaxone. Subsequent therapy is tailored according to the culture re-sults.5
Vascular ConditionsLCP disease and sickle cell disease
are the common vascular causes of limp
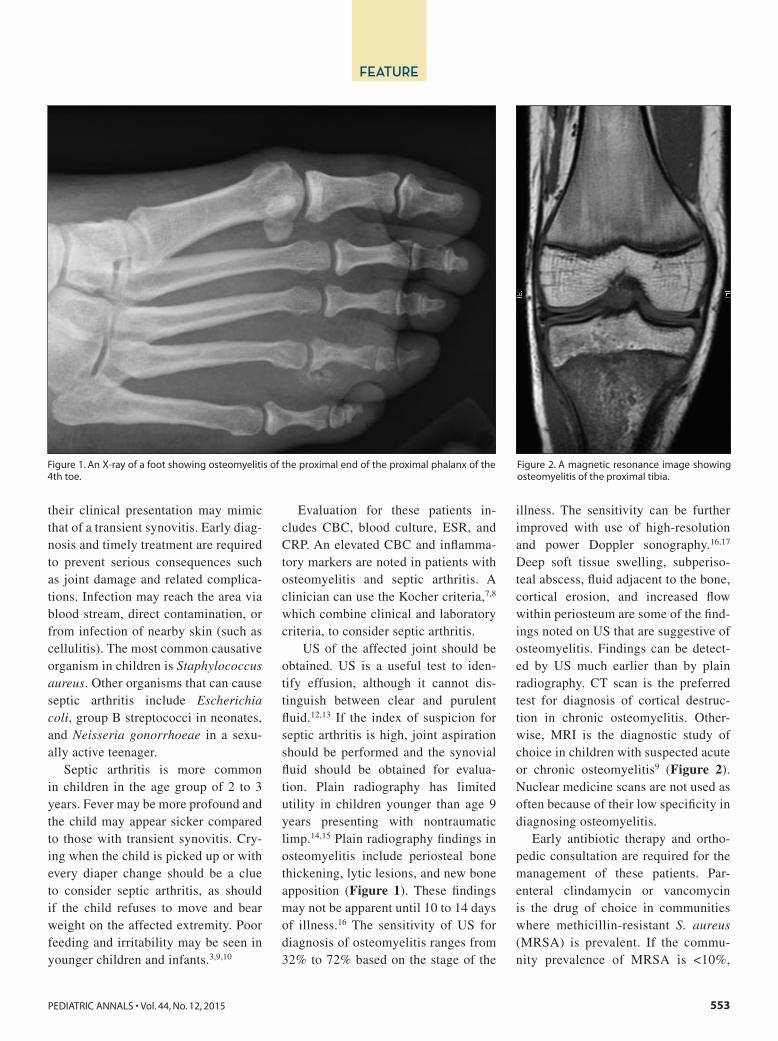
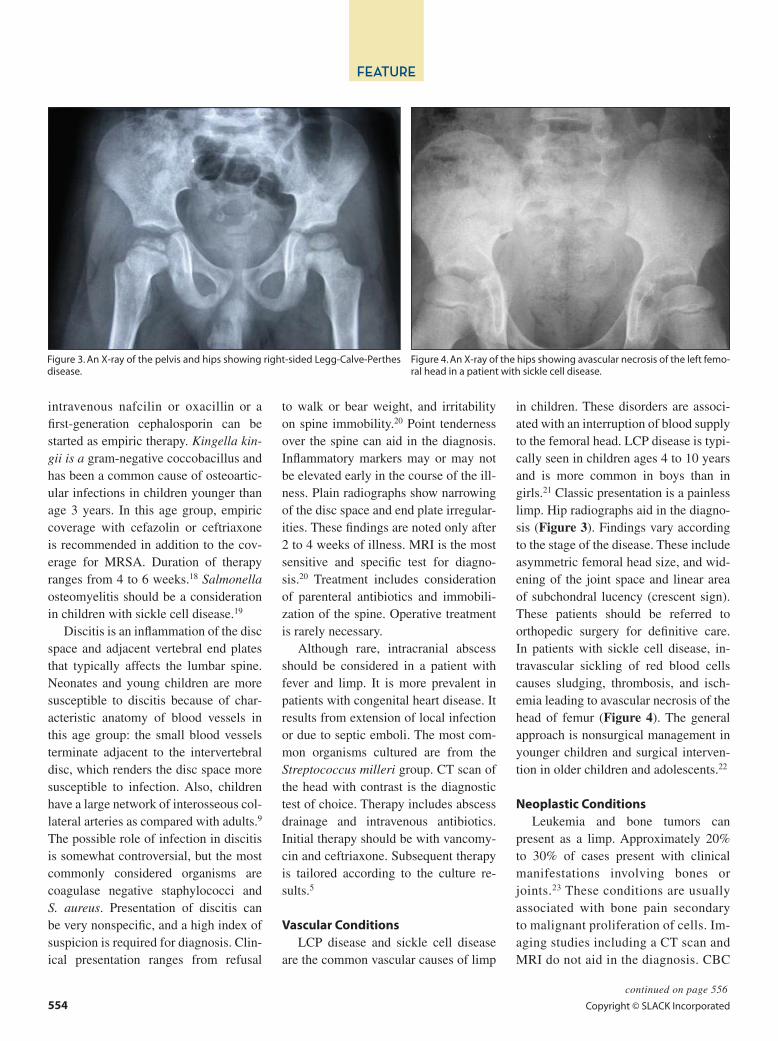
in children. These disorders are associ-ated with an interruption of blood supply to the femoral head. LCP disease is typi-cally seen in children ages 4 to 10 years and is more common in boys than in girls.21 Classic presentation is a painless limp. Hip radiographs aid in the diagno-sis (Figure 3). Findings vary according to the stage of the disease. These include asymmetric femoral head size, and wid-ening of the joint space and linear area of subchondral lucency (crescent sign). These patients should be referred to orthopedic surgery for definitive care. In patients with sickle cell disease, in-travascular sickling of red blood cells causes sludging, thrombosis, and isch-emia leading to avascular necrosis of the head of femur (Figure 4). The general approach is nonsurgical management in younger children and surgical interven-tion in older children and adolescents.22
Neoplastic ConditionsLeukemia and bone tumors can
present as a limp. Approximately 20% to 30% of cases present with clinical manifestations involving bones or joints.23 These conditions are usually associated with bone pain secondary to malignant proliferation of cells. Im-aging studies including a CT scan and MRI do not aid in the diagnosis. CBC
Figure 3. An X-ray of the pelvis and hips showing right-sided Legg-Calve-Perthes disease.
Figure 4. An X-ray of the hips showing avascular necrosis of the left femo-ral head in a patient with sickle cell disease.
continued on page 556
556 Copyright © SLACK Incorporated
FEATURE
may help establish the diagnosis, but a single negative result does not rule out leukemia. If limp persists, one should consider repeating the blood work and also consider bone marrow studies.
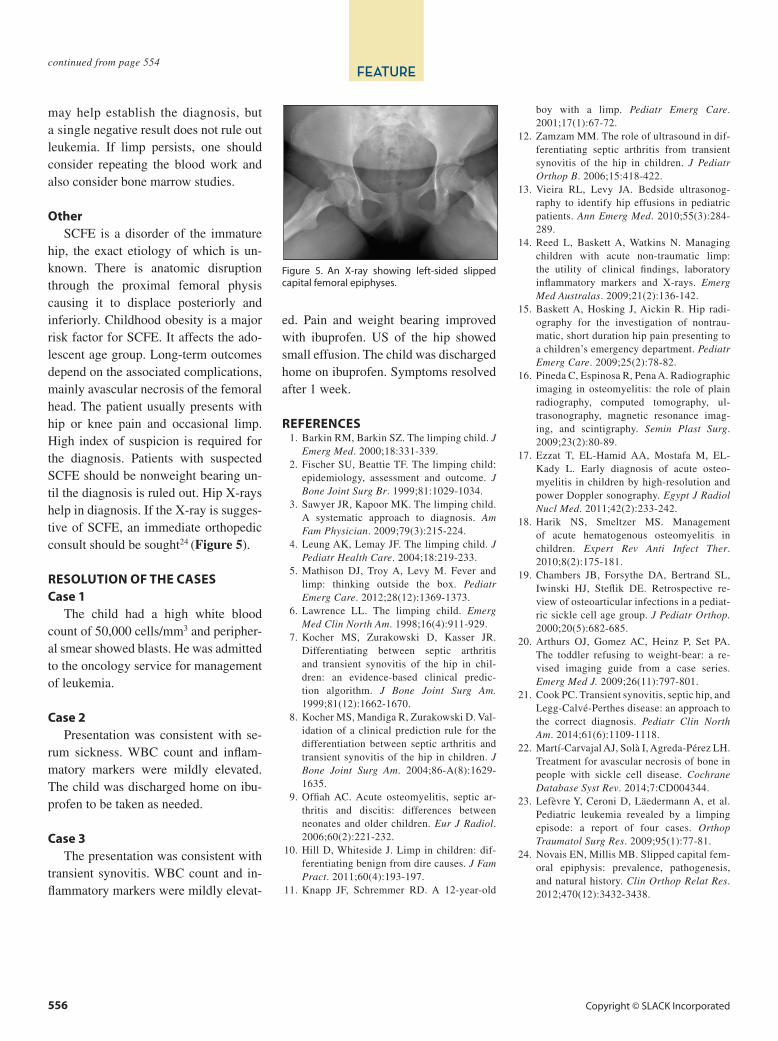
OtherSCFE is a disorder of the immature
hip, the exact etiology of which is un-known. There is anatomic disruption through the proximal femoral physis causing it to displace posteriorly and inferiorly. Childhood obesity is a major risk factor for SCFE. It affects the ado-lescent age group. Long-term outcomes depend on the associated complications, mainly avascular necrosis of the femoral head. The patient usually presents with hip or knee pain and occasional limp. High index of suspicion is required for the diagnosis. Patients with suspected SCFE should be nonweight bearing un-til the diagnosis is ruled out. Hip X-rays help in diagnosis. If the X-ray is sugges-tive of SCFE, an immediate orthopedic consult should be sought24 (Figure 5).
RESOLUTION OF THE CASES Case 1
The child had a high white blood count of 50,000 cells/mm3 and peripher-al smear showed blasts. He was admitted to the oncology service for management of leukemia.
Case 2 Presentation was consistent with se-
rum sickness. WBC count and inflam-matory markers were mildly elevated. The child was discharged home on ibu-profen to be taken as needed.
Case 3 The presentation was consistent with
transient synovitis. WBC count and in-flammatory markers were mildly elevat-
ed. Pain and weight bearing improved with ibuprofen. US of the hip showed small effusion. The child was discharged home on ibuprofen. Symptoms resolved after 1 week.
REFERENCES 1. Barkin RM, Barkin SZ. The limping child. J
Emerg Med. 2000;18:331-339. 2. Fischer SU, Beattie TF. The limping child:
epidemiology, assessment and outcome. J Bone Joint Surg Br. 1999;81:1029-1034.
3. Sawyer JR, Kapoor MK. The limping child. A systematic approach to diagnosis. Am Fam Physician. 2009;79(3):215-224.
4. Leung AK, Lemay JF. The limping child. J Pediatr Health Care. 2004;18:219-233.
5. Mathison DJ, Troy A, Levy M. Fever and limp: thinking outside the box. Pediatr Emerg Care. 2012;28(12):1369-1373.
6. Lawrence LL. The limping child. Emerg Med Clin North Am. 1998;16(4):911-929.
7. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in chil-dren: an evidence-based clinical predic-tion algorithm. J Bone Joint Surg Am. 1999;81(12):1662-1670.
8. Kocher MS, Mandiga R, Zurakowski D. Val-idation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am. 2004;86-A(8):1629-1635.
9. Offiah AC. Acute osteomyelitis, septic ar-thritis and discitis: differences between neonates and older children. Eur J Radiol. 2006;60(2):221-232.
10. Hill D, Whiteside J. Limp in children: dif-ferentiating benign from dire causes. J Fam Pract. 2011;60(4):193-197.
11. Knapp JF, Schremmer RD. A 12-year-old
boy with a limp. Pediatr Emerg Care. 2001;17(1):67-72.
12. Zamzam MM. The role of ultrasound in dif-ferentiating septic arthritis from transient synovitis of the hip in children. J Pediatr Orthop B. 2006;15:418-422.
13. Vieira RL, Levy JA. Bedside ultrasonog-raphy to identify hip effusions in pediatric patients. Ann Emerg Med. 2010;55(3):284-289.
14. Reed L, Baskett A, Watkins N. Managing children with acute non-traumatic limp: the utility of clinical findings, laboratory inflammatory markers and X-rays. Emerg Med Australas. 2009;21(2):136-142.
15. Baskett A, Hosking J, Aickin R. Hip radi-ography for the investigation of nontrau-matic, short duration hip pain presenting to a children’s emergency department. Pediatr Emerg Care. 2009;25(2):78-82.
16. Pineda C, Espinosa R, Pena A. Radiographic imaging in osteomyelitis: the role of plain radiography, computed tomography, ul-trasonography, magnetic resonance imag-ing, and scintigraphy. Semin Plast Surg. 2009;23(2):80-89.
17. Ezzat T, EL-Hamid AA, Mostafa M, EL-Kady L. Early diagnosis of acute osteo-myelitis in children by high-resolution and power Doppler sonography. Egypt J Radiol Nucl Med. 2011;42(2):233-242.
18. Harik NS, Smeltzer MS. Management of acute hematogenous osteomyelitis in children. Expert Rev Anti Infect Ther. 2010;8(2):175-181.
19. Chambers JB, Forsythe DA, Bertrand SL, Iwinski HJ, Steflik DE. Retrospective re-view of osteoarticular infections in a pediat-ric sickle cell age group. J Pediatr Orthop. 2000;20(5):682-685.
20. Arthurs OJ, Gomez AC, Heinz P, Set PA. The toddler refusing to weight-bear: a re-vised imaging guide from a case series. Emerg Med J. 2009;26(11):797-801.
21. Cook PC. Transient synovitis, septic hip, and Legg-Calvé-Perthes disease: an approach to the correct diagnosis. Pediatr Clin North Am. 2014;61(6):1109-1118.
22. Martí-Carvajal AJ, Solà I, Agreda-Pérez LH. Treatment for avascular necrosis of bone in people with sickle cell disease. Cochrane Database Syst Rev. 2014;7:CD004344.
23. Lefèvre Y, Ceroni D, Läedermann A, et al. Pediatric leukemia revealed by a limping episode: a report of four cases. Orthop Traumatol Surg Res. 2009;95(1):77-81.
24. Novais EN, Millis MB. Slipped capital fem-oral epiphysis: prevalence, pathogenesis, and natural history. Clin Orthop Relat Res. 2012;470(12):3432-3438.
Figure 5. An X-ray showing left-sided slipped capital femoral epiphyses.
continued from page 554





























