Embed Size (px)
Citation preview
Gastroenterologia Japonica Vol. 26, Suppl. 3 Copyright �9 1991 by The Japanese Society of Gastroenterology Printed in Japan
Diagnostic approaches and treatment of peptic ulcer at Chulalongkorn University Hospital, Bangkok
S. W I L A I R A T A N A , S. I S R A S E N A , and N. K L A D C H A R E O N Division of Gastroenterology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thialand
Introduction Treatment
Discrepancies in the diagnostic work-up and treatment of peptic ulcer are encountered in dif- ferent parts of the world. In Thailand, where gas- tric and duodenal ulcers are common, manage- ment policy must be based on our experiences in therapeutic trials and adjusted in accordance with the patient's economic station.
Diagnosis
Clinical symptoms are for the most part unreli- able. The pattern of pain is often atypical and unrelated to meals, while the first presentation is frequently one of complication.
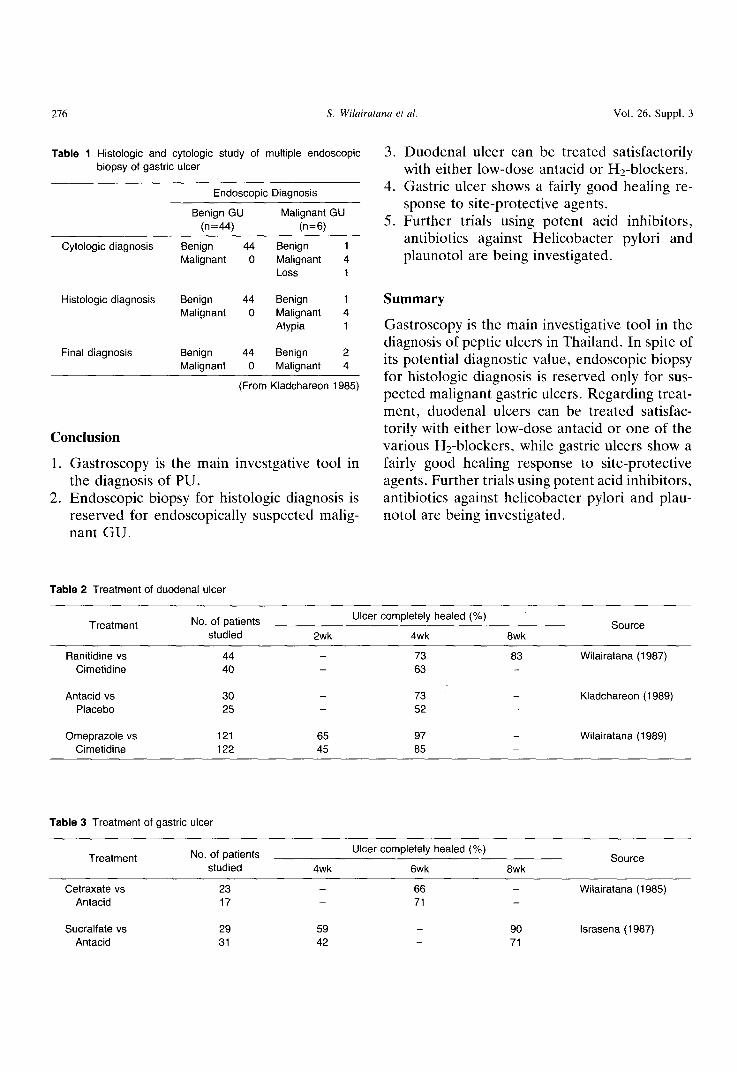
Endoscopy has increasingly become the princi- pal diagnostic method, UGI X-ray being chosen only when an endoscopy resource is unavailable. Endoscopy features even more prominently in relation to GU. In Thailand, endoscopic biopsy of Gu is not always routinely done. However, if malignancy is suspected, multiple biopsy is man- datory. Although histologic together with cyto- logic examination is recommended in such cir- cumstances, cytology dose not appear to offer any extra benefits over that of the histologic exami- nation along (Table 1). In most centers, cytologic study is, therefore, reserved only for the most problematic cases.
Duodenal ulcer A placebo response of nearly 50% was ob-
served in an clinical trial of DU treatment. The response to low-dose antacid liquid has been shown to be over 70% (Table 2). Treatment with Hz-blockers, of course, is associated with better response rates than with other agents. No signifi- cant difference in healing efficacy has been noted between cimetidine and ranitidine. Omeprazole, on the other hand, leads to a more rapid DU healing after 2 weeks of treatment compared to cimetidine. Bismuth and prostaglandins are not popular, mainly due to their high cost and signifi- cant side effects. Maintenance therapy is infre- quent, owing to expense and predictably poor patient compliance.
Gastric ulcer Clinical trials on GU are limited to treatment
with antacids and site-protective agents which have been found to exhibit good healing rates (70-90%) after rather prolonged duration of treatment of 5 to 8 weeks (Table 3). Trials using strong acid inhibitors such as omeprazole and famotidine are ongoing at our institution.
Plaunotol, an extract from a local plant of the Prachuabkirikhan province of Thailand that has been developed and put to use by a Japanese pharmaceutical company, is also being inves- tigated.
Gastroenterol Jpn 1991:26(Suppl 3)275-277 Address for correspondence: Prof. Sommai Wilairatana, M.D., Division of Gastroenterology, Department of Medicine, Chulalongkorn University Hospital, Bangkok 10330, Thailand.
276 S. Wilairatana et al. Vol. 26, Suppl. 3
Table 1 Histologic and cytologic study of multiple endoscopic biopsy of gastric ulcer
Endoscopic Diagnosis
Benign GU Malignant GU (n=44) (n=6)
Cytologic diagnosis
Histologic diagnosis
Benign 44 Benign 1 Malignant 0 Malignant 4
Loss 1
Benign 44 Benign 1 Malignant 0 Malignant 4
Atypia 1
Final diagnosis Benign 44 Benign 2 Malignant 0 Malignant 4
(From Kladchareon 1985)
Conclusion
1. Gastroscopy is the main investgative tool in the diagnosis of PU.
2. Endoscopic biopsy for histologic diagnosis is reserved for endoscopically suspected malig- nant GU.
3. Duodenal ulcer can be treated satisfactorily with either low-dose antacid or Hz-blockers.
4. Gastric ulcer shows a fairly good healing re- sponse to site-protective agents.
5. Further trials using potent acid inhibitors, antibiotics against Helicobacter pylori and plaunotol are being investigated.
Summary
Gastroscopy is the main investigative tool in the diagnosis of peptic ulcers in Thailand. In spite of its potential diagnostic value, endoscopic biopsy for histologic diagnosis is reserved only for sus- pected malignant gastric ulcers. Regarding treat- ment, duodenal ulcers can be treated satisfac- torily with either low-dose antacid or one of the various H2-blockers, while gastric ulcers show a fairly good healing response to site-protective agents. Further trials using potent acid inhibitors, antibiotics against helicobacter pylori and plau- notol are being investigated.
Table 2 Treatment of duodenal ulcer
Treatment No. of patients studied
Ulcer completely healed (%)
2wk 4wk 8wk Source
Ranitidine vs 44 - Cimetidine 40 -
Antacid vs 30 - Placebo 25 -
Omeprazole vs 121 65 Cimetidine 122 45
73 83 Wilairatana (1987) 63
73 - Kladchareon (1989) 52
97 - Wilairatana (1989) 85
Table 3 Treatment of gastric ulcer
Treatment No. of patients studied
Ulcer completely healed (%)
4wk 6wk 8wk Source
Cetraxate vs 23 - 66 - Wilairatana (1985) Antacid 17 - 71 -
Sucralfate vs 29 59 - 90 Israsena (1987) Antacid 31 42 - 71

July 1991 Diagnosis and treatment of peptic ulcer in Bangkok 277
References
1. Kladchareon N, Israsens S, Wilairatana S, et al: Hostologic and cytologic study of multiple endoscopic biopsy of gastric ulcer. Siriraj Hosp GAS 1985;37:1-9
2. Wilairatana S, Israsena S, Sriratanaban A; Comparison of raniti- dine and cimetidinc treatment in patients with active duodenal ulcer. In: New trends in peptic ulcer and chronic hepatitis. Part 1, Peptic Ulcer. Excerpta Medica, Tokyo. 1987;125-128
3. Kladchareon N, Anantapanpong S, Isrdsena S, et al: A study on
the effectiveness of low-dose liquid antacid in the treatment of duodenal ulcer Siriraj Hosp GAS 1989;41:474-480
4. Wilairatana S, Kurathong S, Atthapaisal C, et al: Omeprazole or cimetidine once daily for treatmetn of duodenal ulcers. Journal of Gastroenterology and Hepatology 1989;Supplement 2:45-47
5. Israsena S, Kladchreon N, Kullcavanijays P, et al: Sucralfate and antacid in the short-term treatment of gastric ulcer. Intern Med 1987;3:151-155
6. Wilairatana S, Kladcharcon N, Israsena D, et al: Cetraxate and antacid in the treatment of gastric ulcer. A controlled clinical trails. J Med Assoc Tahiland 1985;581:333-341