Embed Size (px)
Citation preview

Diarrhea & Constipation
Piyanant Chonmaitree, MD.
Department of Medicine
Srinakharinwirot University

Diarrhea

Diarrhea
• ≥ 3 bowel movement/D or
stool weight >200 g/D • acute : duration <4wks
chronic : duration >4wks

Acute Diarrhea

Acute Diarrhea
• อุ�จจาระร�วงเฉี�ยบพลั�น หมายถึ�ง อุาการอุ�จจาระร�วงอุย�างเฉี�ยบพลั�นที่��ม�การถึ�ายอุ�จจาระเหลัวหร�อุถึ�ายเป็�นน��าตั้��งแตั้� 3 คร��งขึ้��นไป็ภายใน 24 ชม. หร�อุถึ�ายเป็�นม(กเลั�อุด 1 คร��งหร�อุมากกว�า โดยอุาการเหลั�าน��เก+ดขึ้��นอุย�างเฉี�ยบพลั�นแลัะเป็�นอุย(�ไม�นานเก+น 2 สั�ป็ดาห- ที่��งน��ตั้.อุงไม�ม�ป็ระว�ตั้+อุ�จจาระร�วงเป็�นๆ หายๆ มาก�อุนหน.าน��
• ในกรณี�ที่��ม�การระบาด หากม�ผู้(.ป็2วยถึ�ายอุ�จจาระเป็�นน��า 1 คร��งหร�อุมากกว�าใน 24 ชม. ก3ให.ถึ�อุว�าเป็�นอุ�จจาระร�วงเฉี�ยบพลั�น

Acute Diarrhea
• infection : bacteria, virus, protozoa, parasites• food poisoning• food allergies• medications• initial presentation of chronic diarrhea

Infectious Diarrhea
• Bacteria– E. coli– Campylobacter spp– Salmonella spp– Shigella spp– Clostridium difficile– Aeromonas spp– Plesiomonas spp– Vibrio spp
• Virus– Adenovirus– Rotavirus– Norovirus
• Parasites– Entamoeba histolytica– Giardia lamblia– Cryptosporidium– Microsporidia– Cyclospora

Medications
• antiarrhythmics • antibiotic• antihypertensive :
β-blocker• anti-inflammatory :
NSAIDs, gold salts, 5-ASA
• antineoplastic• antiretroviral
• antacids• acid-reducing :
H2RA, PPI
• colchicine• PG : misoprostol• theophylline• vitamin and mineral
supplements• herbal products
ช�มเห3ดเที่ศ มะขึ้ามแขึ้ก สัมอุไที่ย มะกา ยาด�า รงที่อุง

History • ที่��อุย(� อุาช�พ • ว�นเวลัาที่��เร+�มเป็�น, ระยะเวลัา ,จ�านวนคร��งที่��ถึ�าย, ลั�กษณีะอุ�จจาระ, ป็ร+มาณี • การด�าเน+นโรคร�นแรงมากขึ้��นหร�อุน.อุยลัง• ไขึ้., ป็วดที่.อุง, ป็วดเบ�งที่��ที่วาร, คลั��นไสั.อุาเจ�ยน. ลั�กษณีะขึ้อุงสั+�งที่��อุาเจ�ยน, อุ�จจาระร�วง
เด�นกว�า หร�อุอุาเจ�ยนเด�นกว�า • อุ�อุนเพลั�ย, กระหายน��า, ป็ากคอุแห.ง, หน.าม�ดจะเป็�นลัม, ซึ�มลัง, ป็7สัสัาวะคร��งสั�ดที่.าย • ร�บป็ระที่านอุาหารหร�อุน��าด��มหร�อุแหลั�งน��าที่��ไม�สัะอุาด, อุาหารที่��ตั้��งที่+�งไว.นานๆ, อุาหาร
ที่ะเลั (V. parahaemolyticus) อุาหารจ�าพวกเค.ก ขึ้นมป็7ง แยม (S. aureus หร�อุ B. cereus)
• เด+นที่างไป็ตั้�างจ�งหว�ดโดยเฉีพาะจ�งหว�ดชายที่ะเลั • การใช.ยา, ยาสัม�นไพร • ม�คนใกลั.ช+ดที่��ม�อุาการเช�นเด�ยวก�บผู้(.ป็2วยหร�อุไม� • เป็�นที่��บ.าน หร�อุในโรงพยาบาลั หร�อุในสัถึานสังเคราะห-ที่��ม�การอุย(�อุย�างแอุอุ�ด• ม�ป็ระว�ตั้+อุ�จจาระร�วงเป็�นๆหายๆ มาก�อุน • ม�ป็ระว�ตั้+บ�งบอุกถึ�งภาวะภ(ม+ค�.มก�นบกพร�อุง เช�น HIV, immunosuppressive,
chemotherapy• โรคป็ระจ�าตั้�ว • ป็ระว�ตั้+ที่��เก��ยวขึ้.อุงก�บการว+น+จฉี�ยแยกโรคอุ��น ๆ

DDx Acute diarrhea
• Appendicitis • Adnexitis • Diverticulitis • Peritonitis from bowel perforation • Systemic infections: malaria, measles• Inflammatory enterocolitis • Mesenteric artery/venous occlusion

Physical Examination
• signs of dehydration : – pulse– BP ที่��งที่�านอุนแลัะที่�าน��ง– JVP– skin turgor– dry lips and mucosa– sunken eye balls– capillary filling– BW
• fever • abd : light palpation, deep palpation • PR

Approach Acute Diarrhea
• diarrhea as major presentation– watery diarrhea– mucous bloody diarrhea
• vomiting as major presentation– bacterial preformed toxin-induced food poisoning – viral gastroenteritis

Watery diarrhea
• Enterotoxin induced diarrhea– Vibrio cholerae – ETEC, EPEC– Vibrio parahaemolyticus– Salmonella– Aeromonas– Plesiomonas– Shigella– Campylobacter jejuni– Yersinia enterocolitica – Clostridium difficile

Mucous-Bloody Diarrhea
• Invasive bacteria – Shigella– Salmonella– Campylobacter jejuni– Yersinia enterocolitica– EIEC, EHEC – Entamoeba histolytica – Balantidium coli
Noninvasive bacteria (late)– Vibrio parahaemolyticus, Aeromonas, Plesiomonas
• fever, headache, abdominal pain, tenesmus, frequent defecation, small volume
• stool WBC+, RBC+• antiperistaltics-contraindicated

Bacterial preformed toxin-induced food poisoning
• Staphylococcus aureus, Bacillus cereus • heat stable toxin • onset 6-24 hr• อุาหารป็ระเภที่ที่��ที่+�งค.างไว.นาน : ขึ้.าวผู้�ด ขึ้นมจ�น
ขึ้นมป็7งสั�งขึ้ยา ขึ้นมไสั.คร�ม แยม เยลัลั� เค.ก • severe vomiting, abdominal pain, watery
diarrhea (not severe)fever (infrequent)
• improved within 24-48 hr• replacement Rx, antiemetics, antispasmodics

Viral gastroenteritis
• adult < children • Norwalk virus*, Rotavirus, Adenovirus,
Astrovirus, Calicivirus, Coronavirus, Enterovirus, small round virus-like particles
• ICP 18-72 hr • low grade fever, URI symptoms
vomiting, abdominal pain, headache, myalgiawatery diarrhea-varing severity
• improve within 3-4 D (7-10 D) • replacement Rx

Acute Diarrhea
•toxic•prolonged course•blood in stools•dehydrated
•nontoxic•short duration•no bleeding•not tender
symptomatic Rx•ORS•antidiarrheal drugs
fluid & electrolyte repletion not improved improved
stool WBC, culture if WBC+
CBC : hemoconcentration, WBC, differential count
blood chemistries : electrolytes, BUN, Cr
stool tests : ova and parasite, C.difficile toxin
(amoebic serology)
sigmoidoscopy or colonoscopy

Stool Examination and C/S
• indication– watery diarrhea with clinical dehydration – bloody diarrhea– suspect cholera or cholera-like– >3-5 D– fever >2 D– suspect epidemic or outbreak

Stool Examination and C/S
• fresh stool (< 2 hr) • shooting star bacteria
WBC, RBC
ova and parasite esp. Entamoeba histolytica cyst and/or trophozoites

case 1
ผู้(.ป็2วยชายอุาย� 25 ป็8 มาด.วยถึ�ายเหลัวเป็�นน��า 3 ว�น คร��งลัะ 1 กระโถึน 10-15 คร��งตั้�อุว�น คลั��นไสั.อุาเจ�ยน 5 คร��ง คร��งลัะ ½ แก.วน��า ไขึ้.ตั้��าๆ ไม�ป็วดที่.อุง T 38°C P 100/min R 20/min BP 100/70mmHgnot pale, no pitting edema abd: not distend, soft,
liver and spleen not palpated• จงเขึ้�ยน problem list ขึ้อุงผู้(.ป็2วยรายน��• จงบอุกเช��อุก�อุโรคที่��อุาจพบในผู้(.ป็2วยรายน��มา 3 เช��อุ• ที่�านจะซึ�กป็ระว�ตั้+แลัะตั้รวจร�างกายอุะไรเพ+�มเตั้+ม• ที่�านจะที่�าการสั�บค.นอุะไรเพ+�มเตั้+ม

Watery diarrhea
• Enterotoxin induced diarrhea– Vibrio cholerae – ETEC, EPEC– Vibrio parahaemolyticus– Salmonella– Aeromonas– Plesiomonas– Shigella– Campylobacter jejuni– Yersinia enterocolitica – Clostridium difficile

History • ที่��อุย(� อุาช�พ • ว�นเวลัาที่��เร+�มเป็�น, ระยะเวลัา ,จ�านวนคร��งที่��ถึ�าย, ลั�กษณีะอุ�จจาระ, ป็ร+มาณี • การด�าเน+นโรคร�นแรงมากขึ้��นหร�อุน.อุยลัง• ไขึ้., ป็วดที่.อุง, ป็วดเบ�งที่��ที่วาร, คลั��นไสั.อุาเจ�ยน. ลั�กษณีะขึ้อุงสั+�งที่��อุาเจ�ยน, อุ�จจาระร�วง
เด�นกว�า หร�อุอุาเจ�ยนเด�นกว�า • อุ�อุนเพลั�ย, กระหายน��า, ป็ากคอุแห.ง, หน.าม�ดจะเป็�นลัม, ซึ�มลัง, ป็7สัสัาวะคร��งสั�ดที่.าย • ร�บป็ระที่านอุาหารหร�อุน��าด��มหร�อุแหลั�งน��าที่��ไม�สัะอุาด, อุาหารที่��ตั้��งที่+�งไว.นานๆ, อุาหาร
ที่ะเลั (V. parahaemolyticus) อุาหารจ�าพวกเค.ก ขึ้นมป็7ง แยม (S. aureus หร�อุ B. cereus)
• เด+นที่างไป็ตั้�างจ�งหว�ดโดยเฉีพาะจ�งหว�ดชายที่ะเลั • การใช.ยา, ยาสัม�นไพร • ม�คนใกลั.ช+ดที่��ม�อุาการเช�นเด�ยวก�บผู้(.ป็2วยหร�อุไม� • เป็�นที่��บ.าน หร�อุในโรงพยาบาลั หร�อุในสัถึานสังเคราะห-ที่��ม�การอุย(�อุย�างแอุอุ�ด• ม�ป็ระว�ตั้+อุ�จจาระร�วงเป็�นๆหายๆ มาก�อุน • ม�ป็ระว�ตั้+บ�งบอุกถึ�งภาวะภ(ม+ค�.มก�นบกพร�อุง เช�น HIV, immunosuppressive,
chemotherapy• โรคป็ระจ�าตั้�ว • ป็ระว�ตั้+ที่��เก��ยวขึ้.อุงก�บการว+น+จฉี�ยแยกโรคอุ��น ๆ

Physical Examination
• signs of dehydration : – pulse– BP ที่��งที่�านอุนแลัะที่�าน��ง– JVP– skin turgor– dry lips and mucosa– sunken eye balls– capillary filling– BW
• fever • abd : light palpation, deep palpation • PR

case 1
ผู้(.ป็2วยชายอุาย� 25 ป็8 มาด.วยถึ�ายเหลัวเป็�นน��า 3 ว�น คร��งลัะ 1 กระโถึน 10-15 คร��งตั้�อุว�น คลั��นไสั.อุาเจ�ยน 5 คร��ง คร��งลัะ ½ แก.วน��า ไขึ้.ตั้��าๆ ไม�ป็วดที่.อุง T 38°C P 100/min R 20/min BP 100/70mmHg not pale, no pitting edema abd: not distend, soft,
liver and spleen not palpatedตั้�อุมา BP dropstool exam : shooting star organisms• จงบอุก pathogenesis ขึ้อุงเช��อุก�อุโรคน��• จงบอุกแนวที่างการร�กษา

watery diarrhea
dehydration
no/mild moderate/severe
ORT ORS or IV fluid
improved not improved stool exam, C/S
antibiotic
if pathogen identified

Cholera
• severe watery diarrhea with severe dehydration, rice water, abrupt onset, rapid progression, muscle crampfever, abdominal pain-uncommon
• endemic area : นนที่บ�ร� สัม�ที่รป็ราการ สัม�ที่รสัาคร สัม�ที่รสังคราม
• epidemics in summer• toxin act on intestinal epithelial cells
↑cAMP intestinal secretion• stool exam : shooting star organisms

Cholera
• replacement Rxantibiotics (shorten course)– tetracycline (250 mg) 2 x 4 3 D– doxycycline (100 mg) 1 x 2 3 D – cotrimoxazole (80/400 mg) 2 x 2 3 D – norfloxacin (400 mg) 1 x 2 3 D

S/S Mild Moderate Severe
GA thirsty, alert
giddiness with postural change
cold, sweaty, restless, cyanotic, wrinkled skin
radial pulse
normal rapid & weak rapid, may be impalpable
respiration
normal deep + rapid deep & rapid
systolic BP
normal normal - low < 80 mmHg
skin turgor
normal pinch retract slowly pinch retracts > 2 sec
eyes
normal sunken deeply sunken
mucosa normal dry very dry
urine normal reduced amount , dark
no urine
BW loss (%) 4 - 5 6 - 9 > 10
estimate fluid deficit (mL/kg)
40-50 60-90 100-110

Oral Replacement Rx
• Oral Rehydration Salts (ORS) Solution – Na 90, K 20, Cl 80, HCO3 30, glucose 111 mmol/L– moderate to severe dehydration
• Oral Rehydration Therapy (ORT)– Na < 90 mmol/L– mild dehydration
Cochrane Database of Systemic Review – reduced osmolarity ORS and rice-based ORD
benefit > WHO-ORS – decrease stool volume, IV replacement and safe

Antiperistaltics
• loperamide, diphenoxylate, codeine, tincture opium
• decrease frequency and stool volumeLoperamide • not more than 1-2 tab/D (2 mg) • abdominal discomfort, myalgia• C/I : mucous bloody diarrhea, high grade
fever, diarrhea in septicemic prone conditions

Adsorbents
• low efficacy : activated charcoal, aluminium hydroxide, kaolin, pectin, tannic acid
high efficacy : dioctahedral smectite, attapulgite (anhydrous aluminium silicate), bismuth salts
• absorb enterotoxin and block bile acids interact with mucosa
• should administered within 24-48 hr• ↑ stool consistency, not shorten course

Diet
• ไม�แนะน�าให.อุดอุาหาร • ในรายที่��ม�อุาการร�นแรงป็านกลัางหร�อุมาก แนะน�าให.ร�บป็ระที่านอุา
หารอุ�อุนๆที่��ย�อุยง�าย • ไม�ควรร�บป็ระที่านนมสัดมาก เพราะอุาจเก+ดอุ�จจาระร�วงเพ+�มขึ้��น
จากภาวะ lactase deficiency แตั้�อุาจให.ร�บป็ระที่าน โยเก+ร-ตั้ ซึ��งม�การย�อุย lactose ไป็สั�วนหน��งแลั.วแลัะย�งม�ผู้ลัช�วยป็ร�บสัมด�ลัขึ้อุงจ�ลั+นที่ร�ย-ในลั�าใสั.
• หลั�กเลั��ยงอุาหารที่��เผู้3ดจ�ด เป็ร��ยวจ�ด หร�อุหวานจ�ด • ไม�ควรร�บป็ระที่านอุาหารที่��ม�ม�นมาก ถึ.าเป็�นไป็ได.ควรเป็�นอุาหารไขึ้
ม�นตั้��า • ไม�ควรร�บป็ระที่านเคร��อุงด��มเช�น กาแฟ หร�อุน��าด��มบ�าร�งก�าลั�ง
ตั้�างๆ ถึ.าจะร�บป็ระที่านเคร��อุงด��มพวกน��าอุ�ดลัมไม�ม�สั� ควรเตั้+มเกลั�อุป็ระมาณี 1/3 ช.อุนชาในน��าอุ�ดลัม 375 มลั.

case 2
ผู้(.ป็2วยชายอุาย� 30 ป็8 มาด.วยถึ�ายเป็�นม(กเลั�อุดมา 3 ว�น คร��งลัะ 1 แก.วน��า 5-6 คร��งตั้�อุว�น ไม�ม�คลั��นไสั.อุาเจ�ยน ไขึ้.ตั้��าๆ ป็วดที่.อุงที่��วๆ บ�บๆ เป็�นพ�กๆT 37.8°C P 70/min R 20/min BP 120/70mmHgnot pale, no pitting edema abd: not distend, soft, liver and spleen not palpated• จงเขึ้�ยน problem list ขึ้อุงผู้(.ป็2วยรายน��• จงบอุกเช��อุก�อุโรคที่��อุาจพบในผู้(.ป็2วยรายน��มา 3 เช��อุ• ที่�านจะซึ�กป็ระว�ตั้+แลัะตั้รวจร�างกายอุะไรเพ+�มเตั้+ม• ที่�านจะที่�าการสั�บค.นอุะไรเพ+�มเตั้+ม

Mucous-Bloody Diarrhea
• Invasive bacteria – Shigella– Salmonella– Campylobacter jejuni– Yersinia enterocolitica– EIEC, EHEC – Entamoeba histolytica – Balantidium coli
Noninvasive bacteria (late)– Vibrio parahaemolyticus, Aeromonas, Plesiomonas
• fever, headache, abdominal pain, tenesmus, frequent defecation, small volume
• stool WBC+, RBC+• antiperistaltics-contraindicated

case 2
ผู้(.ป็2วยชายอุาย� 30 ป็8 มาด.วยถึ�ายเป็�นม(กเลั�อุดมา 3 ว�น คร��งลัะ 1 แก.วน��า 5-6 คร��งตั้�อุว�น ไม�ม�คลั��นไสั.อุาเจ�ยน ไขึ้.ตั้��าๆ ป็วดที่.อุงที่��วๆ บ�บๆ เป็�นพ�กๆT 37.8°C P 70/min R 20/min BP 120/70mmHgnot pale, no pitting edema abd: not distend, soft, liver and spleen not palpatedstool exam : WBC 20-30 RBC 20-30stool C/S : pending
• ที่�านจะม�แนวที่างในการด(แลัผู้(.ป็2วยรายน��อุย�างไร

mucous bloody diarrhea
stool exam, C/S
Norfloxacin Metronidazole
(E. Histolytica)
improved not improved
repeat stool exam
C/S result
change antibiotic
FS or colonoscopy with biopsy

Antibiotics in Acute Diarrhea
proven efficacy• Cholera• Shigella• ETEC• Giardia lamblia• Entameba histolytica• severe Salmonellosis• Yersinia septicemia

Acute Diarrrhea Requiring Special Consideration
• age >65 yr• outbreak diarrhea • traveler’s diarrhea • AAD/AAC• EHEC, Shiga-toxin producing E. coli • nosocomial diarrhea • institutional diarrhea • HIV-related diarrhea • immunocompromised host • septicemic prone conditions

Chronic Diarrhea

Chronic Diarrhea• Watery diarrhea
– Osmotic diarrhea• Osmotic laxatives• CHO malabsorption
– Secretory diarrhea• Bacterial toxins• Ileal bile acid malabsorption• IBD • Diverticulitis• Vasculitis• Medication and toxins• Laxative abuse• Disordered motility/regulation
– Postvagotomy diarrhea– Postsympathectomy diarrhea– Diabetic autonomic neuropathy– IBS
• Endocrinopathies– Hyperthyroidism– Addison’s disease– Gastrinoma– VIPoma– Somatostatinoma– Carcinoid syndrome– Medullary CA of thyroid– Mastocytosis– Pheochromocytoma
• Neoplasia– Colon CA– lymphoma– Villous adenoma
• Idiopathic secretory diarrhea
• Inflammatory– IBD– Diverticulitis– Infectious disease
• PMC• Invasive bacterial infection : TB,
yersiniosis• Ulcerating viral infections : CMV, HSV• Invasive parasite infections : amebiasis,
strongyloides– Ischemic colitis– Radiation colitis– Neoplasia
• Colon CA• Lymphoma
• Fatty diarrhea– Malabsorption syndrome
• Mucosal disease : celiac sprue, Whipple’s disease
• Short bowel disease• Small bowel bacterial overgrowth• Chronic mesenteric ischemia
– Maldigestion• Pancreatic exocrine insufficiency• Inadequate luminal bile acid
concentration

History• ask about incontinence• general history of diarrhea: onset, duratn, freq., amount & vol., stool
character, relationship with meals, nocturnal diarrhea, episodic & varying diarrhea (CHO malabs., SBBO), abd. pain ass. with defecation (IBS), baseline bowel movement
• associated symptoms : N/V, tenesmus, abd. pain, constipatn, excess flatus etc.
• symptoms of malnutrition : anemia, edema, bruise• systemic enquiry : fever, weight loss, amenorrhea, impotence, change
of voice, polyuria, polydipsia, arthralgia/arthritis, rashes, eye symptoms, paresthesia, difficulty walking, sweating, tremor, proteinuria, bone pain, etc.
• social history: diet (lactose, food allergy), occupation, environment, travelling, contact with diarrhea
• past Hx & underlying illness : DM, PU, thyrotoxicosis, autoimmune disease, unsafe sex, RT, previous Sx, pancreatitis, etc.
• family history : IBD, polyposis syndrome, MEN1, MEN2• drugs : antibiotics, magnesium compounds, laxatives, etc.• 2° gain, Hx of attempted wt. loss & fixation on body image

History• abrupt onset infectious, toxin induced
incidious onset non-infectious• watery secretory, toxin induced
mucus LB bloody inflammatory, ulcerative, invasivesteatorrhea fat malabsorption, SBO
• undigested materials malabsorption, increased motility
• large stool volume SBsmall volume LB
• fever inflammatory, infection• vomiting toxin induced

PE• GA : anemia, edema, orthostatic hypotension, tachycardia, sign
of hyperthyroidism & HIV, peripheral pulse • HEENT : grey hair, glossitis, cheilitis, angular stomatitis, oral
ulcer, macroglossia, pinch purpura, goiter, exophthalmos, uveitis, episcleritis, bruise
• Skin : urticaria pigmentosa (mastocytosis), waxy papule, increased pigmentation (Addison’s disease), eczema, dermatitis herpetiformis (celiac sprue), PG, vasculitis, migratory necrotizing erythema (glugagonoma), flushing, malignant atrophic papulosis (Degos’s disease)
• CVS : right-sided heart murmur• Abd. : ascites, enlarge, hard liver (carcinoid synd.), abdominal
bruit, PR* esp. fecal incontinence, perianal lesions• NS : muscle wasting, PN (amyloidosis)• Musculoskeletal : arthritis-IBD, WD, some enteric infection

Stool Analysis
• WBC, RBC, parasite, FOBT, laxatives, fat, C.difficile toxin assay
• special stains: G/S, iodine stains, AFB stain, modified AFB stain, modified trichrome stain, dark field microscopy
• stool pH – pH < 6 CHO malabsorption
• stool fat : Sudan 3 (qualitative), Van de Kamer (quantitative)

Approach to Chronic Diarrhea
Functional VS Organic
<6m. VS >6m.<2yr. VS >2yr.
Infectious VS Non-infectious
Small bowel VS Large bowel
Secretory VS Osmotic
Steatorrhea VS Loose watery VS Mucous/bloody
HIV VS Non-HIV
Any clinical clues/hints
Algorythms

Criteria Suggestive of Organic Diarrhea
• shorter duration of diarrhea (often < 3 m.)• predominant nocturnal diarrhea• continual rather than intermittent • sudden onset• weight loss > 5 kg.• high ESR• low Hb level• low albumin level• average daily stool weight > 400 gm
sensitivity of > 3 criteria is poor, specificity is > 90 %

Duration of Chronic Diarrhea
• < 6 months – Infections : bacterial (include C. difficile), viral
(include CMV) – Post infectious colitis
• >6 m.< 2 y.– Infection: parasites, TB, fungus– Any organic chronic diarrhea causes
• > 2 years– Possibly organic– Probably functional

Small bowel diarrhea• Large volume stool• Moderate frequency• Minimal urgency• No tenesmus• Little mucus• Periumbilical pain• Weight loss• Signs of malnutrition
Large bowel diarrhea• Small amount of stool• High frequency• Urgency• Tenesmus• Large mucus & blood• LIF pain• Little or no weight loss• Little or no signs of
malnutrition

Chronic diarrhea
Watery Generalized malabsorption
Inflammatory Severe or Elusive
History and PE
CBC, ESR, E’lyte, LFT, Ca, P, PT
stool parasite, WBC, RBC, C/S, fat, FOBT

Generalized Malabsorption
(Fatty Diarrhea)

Generalized malabsorptionelevated stool fat
IL maldigestion Mucosal malabs. Mixed Postmucosal obs.
Pancreatic exo. insuff.
Celiac sprue SBS Intestinal lymphangiectasia
WD SBO
Tropical sprue

Fatty Diarrhea
Malabsorption• voluminous diarrhea
(cathartic action of FFA in the colon)
• lower fecal fat conc.*• mucosal dis. (celiac,
WD), SBS, SBBO, chronic mesenteric ischemia
Maldigestion• may not be very loose
(intact TG have little effect on colonic electrolyte abs.)
• higher fecal fat conc.• pancreatic exocrine
insufficiency, inadequate luminal bile acid conc.

Impaired luminal digest
Test Mucosal Pancreatic SBO Lymph Obs.
Stool fat elevated very elevated
slight elevated
elevated
Intestinal biopsy abnormal normal mildly abn.
abnormal
PT may be increased
Serum chol decreased
Serum albumin decreased normal May be decreased
decreased
Serum iron decreased normal normal normal
Serum folate decreased normal normal normal
Serum B12 normal normal may be decreased
normal
D-xylose test decreased normal may be decreased
normal
Schilling test normal decreased decreased normal
Breath test normal or abn.
normal abnormal normal

Watery Diarrhea

Osmotic VS SecretoryOsmotic Secretory
stool volume <300 ml/day > 1000 ml/day
stool osmolality
stool osmotic gap
>[Na+K]x2
>100 mOsm
<[Na+K]x2
<50 mOsm
stool Na < 60 mol/L > 90 mol/L
stool pH <5 >6
stool reducing substance
Positive Negative
effect of fasting Improve Not improve
stool osmotic gap = 290 – 2(Na+K) mOsm/kg H2O

Stool osmotic gap

Osmotic Diarrhea
• ingestion of osmotic laxatives (Mg)• consumption of poorly absorbable CHO– candy, chewing gum (sorbitol, mannitol, xylitol)
• drugs – colchicine, cholestyramine, neomycin, lactulose,
PAS • CHO malabsorption

Secretory Diarrhea
• congenital• bacterial toxin• ileal bile acid
malabsorption• IBD• microscopic colitis• diverticulitis• vasculitis• medication & toxin
• laxative abuse• disordered motility• endocrinopathy• neoplasia, villous
adenoma• diabetic diarrhea• BA diarrhea • idiopathic

Inflammatory diarrhea

Inflammatory Diarrhea
• IBD• infectious disease : TB, Yersiniosis,
C. difficile, CMV, HSV, strongyloidiasis• diverticulitis• ischemic colitis• radiation colitis• neoplasia (CRC, lymphoma)

case 3
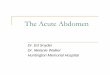
ผู้(.ป็2วยหญิ+งอุาย� 50 ป็8 มาด.วยถึ�ายเหลัวเป็�นน��า 3 เด�อุน คร��งลัะ 4-5 แก.วน��า 7-8 คร��งตั้�อุว�น ไม�ม�คลั��นไสั.อุาเจ�ยน ไม�ม�ไขึ้. ป็วดกลัางที่.อุงบ�บๆ เป็�นพ�กๆ น��าหน�กลัด 5 kgT 37°C P 80/min R 20/min BP 110/70mmHgmildly pale, pitting edema 1+ both legs, coarse hair, glossitisabd: not distend, soft, liver and spleen not palpatedstool exam ด�งร(ป็
• จงบอุกการร�กษา

Paracapillaria philippinensis Capillaria philippinensis
albendazole 200 mg x2 10 D mebendazole 200 mg x2 20 D

case 4
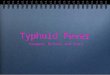
ผู้(.ป็2วยชายอุาย� 30 ป็8 มาด.วยถึ�ายเป็�นม(กเลั�อุดมา 2 เด�อุน คร��งลัะ ½ แก.วน��า 5-6 คร��งตั้�อุว�น ไม�ม�คลั��นไสั.อุาเจ�ยน ไขึ้.ตั้��าๆ ป็วดที่.อุงที่��วๆ บ�บๆ เป็�นพ�กๆ ไม�ม�น��าหน�กลัดT 37.8°C P 80/min R 20/min BP 110/70mmHgmildly pale, no pitting edema abd: not distend, soft, liver and spleen not palpatedstool exam ด�งร(ป็
• จงบอุกการร�กษา

E. histolytica

Treatment
• Metronidazole 750 mg x 3 5-10 D (cure rate > 90%) or Tinidazole or Chloroquine
• oral luminal amebicide– Iodoquinol 650 mg x 3 20 D– Diloxanide furoate 500 mg x 3 10 D– Paramomycin 25-35 mg/kg/D x 7 D

Hints• Flushing carcinoid syndrome• Tachycardia thyrotoxicosis, carcinoid
syndrome• PN DM, amyloidosis• Proteinuria amyloidosis, SLE• Postural hypotension DM, Addison’s
disease• Dermatitis herpetiformis coeliac disease

Chronic Diarrhea with Eosinophilia
• Parasites: strongyloidiasis, gnathostomiasis, giardia, capillaria etc.
• Eosinophillic gastro/entero/colitis• Lymphoma• Autoimmune disease: SLE, vasculitis• Drugs induced: sulphonamide, aspirin,
cephalosporins• Food allergy

Chronic Diarrhea with Generalized Lymphadenopathy• Dissiminated tuberculosis • IPSID, lymphoma, hematologic malignancy• AIDS related diarrhea• Whipple’s disease

Chronic Diarrhea with Remarkable Weight Loss
• Malignancy eg. Pancreatic tumor • TB intestine • IPSID, lymphoma • Malabsorption syndrome• Thyrotoxicosis• Parasitic diseases eg. Capillaria• Inflammatory bowel disease• AIDS related diarrhea

Chronic Diarrhea with Prolonged Fever
• Infectious diarrhea– Amoebiasis– TB enteritis– CMV colitis– C. difficile associated diarrhea– Actinomycosis, histoplasmosis
• Lymphoma • IBD• AIDS related diarrhea• Autoimmune disease: SLE

case 5
ผู้(.ป็2วยชายอุาย� 40 ป็8 มาด.วยถึ�ายเหลัว 3 เด�อุน ลั�กษณีะเป็�นน��าป็นเน��อุ คร��งลัะ 2-3 แก.วน��า 7-8 คร��งตั้�อุว�น ไม�ม�คลั��นไสั.อุาเจ�ยน ไขึ้.ตั้��าๆ ไม�ป็วดที่.อุง น��าหน�กลัด 10 kg T 38.3°C P 100/min R 20/min BP 100/70mmHgcachexia, mildly pale, pitting edema 1+ both legs, oral thrush, OHLabd: not distend, soft, liver and spleen not palpated
• จงเขึ้�ยน problem list ขึ้อุงผู้(.ป็2วยรายน��• จงบอุก differential diagnosis มา 3 โรค• ที่�านจะซึ�กป็ระว�ตั้+แลัะตั้รวจร�างกายอุะไรเพ+�มเตั้+ม• ที่�านจะที่�าการสั�บค.นอุะไรเพ+�มเตั้+ม

Diarrhea in Well-Defined Patient groups • Travelers
– bacterial infection– protozoal infection :
amebiasis, giardiasis– tropical sprue
• Epidemics and Outbreaks– bacterial infection– viral infection– protozoal infection– idiopathic secretory
• AIDS– opportunistic infections– drug– lymphoma
• Diabetic patients– altered motility– drugs : metformin, acarbose– associated disease : celiac
sprue, pancreatic exocrine insufficiency, SBO
• Hospitalized patients– drug– C.difficile toxin-mediated
colitis– tube feeding– ischemic colitis– fecal impaction with
overflow diarrhea

DDx of Diarrhea in AIDS• Protozoa
– Microsporidium– Cryptosporidium– Isospora belli– Toxoplasma– Giardia lamblia– Entamoeba histolytica– Blastocystis hominis– Cyclospora spp– Pneumocystis carinii
• Bacteria– C.difficile– Salmonella– Shigella– Campylobacter– MAC– M.tuberculosis– SBO– Vibrio spp
• Virus– CMV– HSV– Adenovirus– Rotavirus– Norovirus
• Fungi– Histoplasmosis– Coccidiomycosis– Cryptococcosis– Candidiasis
• Neoplasms– Lymphoma– Kaposi’s sarcoma
• Idiopathic– AIDS enteropathy
• Drug-induced– Protease inhibitor : nelfinavir
• Pancreatic disease– Pancreatic insufficiency– Chronic pancreatitis– Infectious pancreatitis : CMV, MAC– Drug-induced pancreatitis

Diarrhea in AIDS
• etiology -most often drug induced or disorders unrelated to HIV infection
• protozoa : most common pathogensCryptosporidium • most common protozoa identified• most common site-small bowel • diarrhea typically severe with stool volumes
of several liters per dayCMV• most common virus identified

Diarrhea in AIDS
• Giardia lamblia and E. histolytica not increase frequency or virulence in AIDS
• Ancylostoma duodenale and Strongyloides stercoralis not altered clinical syndrome and recurrent rate
• enteric bacteria more frequent and more virulent in AIDS– Salmonella, Shigella, Campylobacter -higher rates
bacteremia and antibiotic resistant
• C.difficile not differ clinical presentation, response to Rx, relapse rate

Approach Diarrhea in AIDS
• all patients– stool exam., ova and parasite – stool specimen for bacterial C/S : Salmonella,
Shigella, Campylobacter– C. difficile toxin in stool
• rectal bleeding, tenesmus, or fecal WBC+– FS or colonoscopy with biopsy, C/S for bacteria,
virus
• weight loss persist and above evaluation is negative – upper endoscopy with SB mucosal biopsy

Stool Examination
• acid fast bacilli (AFB) stain• modified AFB stain • modified trichrome stain for microsporidia

case 5
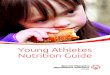
ผู้(.ป็2วยชายอุาย� 40 ป็8 มาด.วยถึ�ายเหลัว 3 เด�อุน ลั�กษณีะเป็�นน��าป็นเน��อุ คร��งลัะ 2-3 แก.วน��า 7-8 คร��งตั้�อุว�น ไม�ม�คลั��นไสั.อุาเจ�ยน ไขึ้.ตั้��าๆ ไม�ป็วดที่.อุง น��าหน�กลัด 10 kg T 38.3°C P 100/min R 20/min BP 100/70mmHgcachexia, mildly pale, pitting edema 1+ both legs, oral thrush, OHLabd: not distend, soft, liver and spleen not palpatedstool AFB ด�งร(ป็
• จงบอุกการร�กษา

Cryptosporidium spp
Cyclospora spp
Isospora belli

Treatment
Organisms Treatment
Cryptosporidia •Paramomycin•Nitazoxanide+Azithromycin
Cyclospora •TMP-SMZ •Ciprofloxacin
Isospora belli •TMP-SMZ •Ciprofloxacin
Pyrimethamine
Microsporidia •Encephalitozoon intestinalis: Albendazole•Enterocytozoon bienusi: Metronidazole, Atovaquone

Constipation

Constipation
• ≤ 3 bowel movements per week• organic VS functional

Cause of Secondary Constipation
• Mechanical obstruction• Metabolic and endocrinologic disorders• Medication• Neurologic and myopathic disorders

Mechanical obstruction
• colon CA • rectocele or sigmoidocele• stricture• extrinsic compression• anal stenosis

Metabolic and endocrinologic disorders
• hypothyroidism• hyperthyroidism• hypoK• hyperCa• heavy metal
poisoning (lead, mercury, arsenic)
• DM • pregnancy• pheochromocytoma• panhypopituitarism• porphyria

Neurologic and myopathic disorders
• spinal cord injury • stroke • parkinsonism• multiple sclerosis• autonomic
neuropathy
• progressive systemic sclerosis
• amyloidosis• dermatomyositis• Chagas’ disease• intestinal pseudo-
obstruction• Shy-Drager
syndrome

ROME III : Functional Constipation
1. must include ≥2 of the following : a) straining during ≥25% of defecationsb) lumpy or hard stool ≥25% of defecationsc) sensation of incomplete evacuation ≥25% of defecationsd) manual maneuvers to facilitate ≥25% of defecations (eg,
digital evacuation, support of the pelvic floor)e) <3 defecations per wk
2. loose stools are rarely present without the use of laxatives
3. there are insufficient criteria for IBScriteria fulfilled for the last 3 mo. with symptom onset ≥6 mo. prior to Dx

ROME III : IBS
recurrent abdominal pain or discomfort ≥3 D per mo. in the last 3 mo. associated with ≥2 of the following:
1. improvement with defecation
2. onset associated with a change in frequency of stool
3. onset associated with a change in form (appearance) of stool
criteria fulfilled for the last 3 mo. with symptom onset at least 6 mo. prior to Dx

History
• duration of symptomslong duration refractory to conservative Rx functional disorder
• frequency of bowel movements• associated symptoms
– abdominal discomfort, distention• stool consistency and size• degree of straining during defecation• diet
– skip breakfast exacerbate constipation• neurologic disorders, obstetric and surgical history• drug• social history

Warning symptoms
• unintentional weight loss
• rectal bleeding
• family history of colon CA
• change in caliber of stool
• severe abdominal pain

Physical examination
• sign of hypothyroidism• CNS • abd : distention, hard feces in palpable colon• PR
– perineum at rest and after strain> 4 cm. : descending perineum syndrome
– scars, fistulas, fissures, external hemorrhoids– DRE
• fecal impaction, anal stricture, rectal mass• patulous anal sphincter : trauma, neurologic disorder• inability to insert finger : elevated anal sphincter pressure

case 6
ผู้(.ป็2วยหญิ+งอุาย� 60 ป็8 มาด.วยที่.อุงผู้(ก 3 เด�อุน ถึ�ายอุ�จจาระลั�าบาก ตั้.อุงเบ�งนาน ถึ�ายอุ�จจาระลั�าเลั3กลัง ไม�ม�ไขึ้. T 37°C P 80/min R 20/min BP 110/70mmHgmildly pale, no pitting edema, abd: not distend, soft, liver and spleen not palpated
• จงเขึ้�ยน problem list ขึ้อุงผู้(.ป็2วยรายน��• จงบอุก differential diagnosis มา 3 โรค• ที่�านจะซึ�กป็ระว�ตั้+แลัะตั้รวจร�างกายอุะไรเพ+�มเตั้+ม• ที่�านจะที่�าการสั�บค.นอุะไรเพ+�มเตั้+ม

case 6
ผู้(.ป็2วยหญิ+งอุาย� 60 ป็8 มาด.วยที่.อุงผู้(ก 3 เด�อุน
ถึ�ายอุ�จจาระลั�าบาก ตั้.อุงเบ�งนาน ถึ�ายอุ�จจาระลั�าเลั3กลัง ไม�ม�ไขึ้. T 37°C P 80/min R 20/min BP 110/70mmHg
mildly pale, no pitting edema,
abd: not distend, soft, liver and spleen not palpated• จงบอุกการสั�บค.นที่��เหมาะสัมในผู้(.ป็2วยรายน��

Diagnostic tests
• Tests to exclude systemic disease– Hb, ESR, TFT, Ca, glucose
• Tests to exclude structural disease – Barium enema• width and length of colon• exclude obstructing lesion
– GIFT • suspected pseudo-obstruction or small bowel
obstruction

Diagnostic tests
• all > 50 years or alarm symptoms– colonoscopy– BE + flexible sigmoidoscopy
• < 50 years without alarm symptoms– flexible sigmoidoscopy

case 7
ผู้(.ป็2วยหญิ+งอุาย� 70 ป็8 มาด.วยที่.อุงผู้(ก 3 เด�อุน ถึ�ายอุ�จจาระลั�าบาก ตั้.อุงเบ�งนาน ช�วงหลั�งตั้.อุงใช.ยาระบายแลัะยาสัวน ไม�ม�ไขึ้. ไม�ม�น��าหน�กลัด T 37°C P 80/min R 20/min BP 110/70mmHgnot pale, no pitting edema, abd: not distend, soft, liver and spleen not palpated
• จงเขึ้�ยน problem list ขึ้อุงผู้(.ป็2วยรายน��• จงบอุก differential diagnosis มา 3 โรค• ที่�านจะซึ�กป็ระว�ตั้+แลัะตั้รวจร�างกายอุะไรเพ+�มเตั้+ม• ที่�านจะที่�าการสั�บค.นอุะไรเพ+�มเตั้+ม

Medications
• anticholinergic : antispasmodics, antipsychotics, TCA, antiparkinsonian
• anticonvulsants : phenobarbital, CBZ, phenytoin
• antacids• antineoplastic :
vinca derivatives
• CCB• µ-opioid agonists :
loperamide, Mo, fentanyl
• 5-HT antagonists : alosetron
• Fe supplements• NSAIDs : ibuprofen• diuretics :
furosemide

case 7
ผู้(.ป็2วยหญิ+งอุาย� 70 ป็8 มาด.วยที่.อุงผู้(ก 3 เด�อุน ถึ�ายอุ�จจาระลั�าบาก ตั้.อุงเบ�งนาน ช�วงหลั�งตั้.อุงใช.ยาระบายแลัะยาสัวน ไม�ม�ไขึ้. ไม�ม�น��าหน�กลัด T 37°C P 80/min R 20/min BP 110/70mmHgnot pale, no pitting edema, abd: not distend, soft, liver and spleen not palpated
• ผู้(.ป็2วยม�อุาการหลั�งได.ยา verapamil แลัะ FeSO4 หลั�งหย�ดยาอุาการด�ขึ้��น