Embed Size (px)
Citation preview

AJR:193, September 2009 709
cular imaging in most European countries, and is well tolerated by patients [21–25]. In combination with nonlinear and nondestruc-tive sonographic techniques, such as pulse inversion operating at low acoustic power, sulfur hexafluoride allows real-time imaging of contrast enhancement in both lesions and splenic parenchyma throughout the vascular circulation [21, 25]. Sulfur hexafluoride has additionally shown a spleen-specific uptake after blood pool clearance, and the degree of the late phase uptake by a lesion may reflect its similarity to normal splenic tissue [26].
Early experience suggests promise for the use of contrast-enhanced sonography in the diagnosis of focal splenic lesions [27–37]. However, the diagnostic benefit of sul-fur hexafluoride-enhanced sonography has not yet been investigated in a larger series
Differentiation of Benign From Malignant Focal Splenic Lesions Using Sulfur Hexafluoride–Filled Microbubble Contrast-Enhanced Pulse-Inversion Sonography
Axel Stang1
Handan Keles1
Suna Hentschke1
Cay Uwe von Seydewitz1
Joachim Dahlke2
Ernst Malzfeldt2
Dietrich Braumann1
Stang A, Keles H, Hentschke S, et al.
1Department of Hematology and Oncology, Asklepios Klinik Altona, Paul-Ehrlich-Straße 1, D-22763 Hamburg, Germany. Address correspondence to A. Stang ([email protected]).
2Department of Radiology, Asklepios Klinik Altona, Hamburg, Germany.
Gastrointest ina l Imaging • Or ig ina l Research
AJR 2009; 193:709–721
0361–803X/09/1933–709
© American Roentgen Ray Society
Sonography is usually the first im-aging technique used to evaluate the spleen. However, convention-al gray-scale and color Doppler
sonography have limited diagnostic accura-cy (30–75%) in characterizing depicted focal splenic lesions [1–5], making the more fre-quently accurate contrast-enhanced CT [6–14] or MRI [15–20] mandatory for lesion di-agnosis. The introduction of sonographic microbubble contrast agents offers an option to improve the ability of sonography in char-acterizing splenic lesions, which would be a benefit for both patients and investigators.
The second-generation sonographic con-trast agent sulfur hexafluoride has a strong nonlinear response from microbubble oscil-lations when it is insonated with low acous-tic power, is licensed for abdominal and vas-
Keywords: contrast agents, diagnosis, focal lesions, sonography, spleen
DOI:10.2214/AJR.07.3988
Received March 14, 2008; accepted after revision January 1, 2009.
OBJECTIVE. The purpose of our study was to evaluate whether sonographic character-ization of focal splenic lesions could be improved by using low mechanical index pulse-inver-sion sonography after sulfur hexafluoride-filled microbubble injection.
MATERIALS AND METHODS. One hundred forty-seven splenic lesions (68 benign, 79 malignant) in 147 patients (81 men, 66 women; mean age, 51 years) underwent baseline gray-scale sonography and sulfur hexafluoride–enhanced low-acoustic-power pulse-inver-sion sonography (mechanical index < 0.1). Two site investigators assessed in consensus le-sion and splenic enhancement during arterial and parenchymal phases. Four readers (read-ers 1 and 2, blinded; and readers 3 and 4, unblinded to clinical data) independently reviewed baseline and contrast-enhanced sonograms and provided confidence rating for diagnosis of malignancy or benignancy. Accuracy, sensitivity, specificity, positive and negative predictive values, and areas under the receiver operating characteristic curves (Az) were calculated by considering biopsy results or splenectomy (51 patients) or CT or MR images followed by se-rial sonography 6–12 months apart (96 patients) as reference standards.
RESULTS. Benign lesions appeared predominately non- or isoenhancing relative to splen-ic parenchyma, whereas malignant lesions appeared predominately progressively hypoenhanc-ing. For correct diagnosis of benignancy or malignancy, review of contrast-enhanced sonogra-phy after baseline sonography yielded significantly improved diagnostic performance (overall accuracy, 51%, 43%, 70%, and 74% before vs 83%, 81%, 92%, and 91% after contrast-en-hanced sonography for readers 1, 2, 3, and 4; p < 0.05; respectively) and significantly improved diagnostic confidence (Az, 0.770, 0.678, 0.900, and 0.917 before vs 0.935, 0.917, 0.984, and 0.959 after contrast-enhanced sonography for readers 1, 2, 3, and 4; p < 0.05; respectively).
CONCLUSION. Sulfur hexafluoride–filled microbubble-enhanced sonography improves characterization of focal splenic lesions with and without the availability of clinical data.
Stang et al.Sonography of Focal Splenic Lesions
Gastrointestinal ImagingOriginal Research

710 AJR:193, September 2009
Stang et al.
with different clinical conditions. Because the clinical context in which splenic lesions occur is usually known at sonographic ex-amination and is helpful for differential di-agnosis [1, 2], it would be reasonable to addi-tionally evaluate the influence of knowledge of the patients’ presentation.
The aim of this study was to evalu-ate whether the characterization of splen-ic lesions could be improved by using low-acoustic-power pulse-inversion sonography after sulfur hexafluoride–filled microbubble injection, as compared with the lesion char-acterization achieved with nonenhanced baseline sonography, in readings performed both blinded and unblinded to patient clini-cal data.
Materials and MethodsPatients
This retrospective study was approved by the institutional ethics committee. All patients gave informed consent. Patients referred to our institu-tion for abdominal sonography with at least one splenic lesion larger than 1 cm identified on un-enhanced baseline sonography were recruited for the contrast sonography study at the time of the sonography examination. Exclusion criteria were critical illness, hypersensitivity to drugs, obvious simple anechoic cysts at baseline sonography, or contraindications to the licensed use of the con-trast agent SonoVue (Bracco) within the terms of the applicable country product license (i.e., preg-nancy, childhood, severe cardiac failure).
Between January 2002 and December 2005, 147 patients (85 men, 62 women; mean age, 51 years; range, 14–87 years) with 147 focal splen-ic lesions (size range, 1.0–9.7 cm; mean, 3.3 cm) were included in the contrast sonography study. Of the 151 initially recruited patients, four were ex-cluded because of instable coronary heart disease (n = 1), obvious cysts (n = 2), or technical limita-tions to adequate scanning of a splenic lesion near the diaphragm (n = 1). In 80 patients with multi-ple lesions, the largest was selected for evaluation. In 31 patients, the splenic lesion was an incidental finding. Characteristics of patients and lesions are summarized in Table 1.
Sonography ProceduresAll sonographic examinations were performed
by two investigators of the same institution who had more than 15 and 5 years, respectively, of sonography and contrast-enhanced sonography experience. The sonographic examinations were performed before the reference standard exami-nations using the same sonography equipment (EUB 8500 and convex-array 1–5-MHz transduc-
er EUP 314, Hitachi). Initially, baseline sonogra-phy was performed in the dynamic harmonic im-aging mode (transmit. 1–5 MHz; receive, 2–10 MHz; 25–30 frames per second; dynamic range, 70–75 dB; gain, 15–20 dB). Color or power Dop-pler evaluation was not included in the baseline sonographic study. Each patient underwent a com-plete evaluation of the abdomen. Thereafter, the splenic target lesion was scanned.
After baseline sonography, a pulse-inversion mode with low acoustic output (mechanical index < 0.1) was begun. The overall gain and the superfi-cial portion of the time–gain compensation curve were set to low. The focal zone was placed man-ually below the investigated lesion. After the IV bolus injection of 4.8 mL of sulfur hexafluoride (SonoVue, Bracco) via a 20-gauge cannula fol-lowed by a 10-mL normal saline flush, the lesion of interest was scanned continuously for 5 min-utes (typically 10–15 frames per second, dynamic range 60–65 dB). The transducer was kept in a fixed position. Contrast-enhanced scans were ob-tained during quiet respiration.
Digital cine clips of the splenic lesions were registered during baseline sonography (length of clips, 5–10 seconds) and during the early arte-rial (i.e., 10–30 seconds after injection) and late parenchymal (150–300 seconds after injection) phases. The early arterial and late parenchymal phase scans were chosen to show the maximum differences for changes in time between the en-hancement of the lesion and the enhancement of the adjacent splenic tissue. Cine clips were stored on a PACS (Raid 5, Dell) that was connected to the sonography system via a local area network link (DICOM 3.0 standard).
On-Site AnalysisExtent of lesion enhancement during the arte-
rial and parenchymal phases was subjectively as-sessed in consensus by the two site investigators as nonenhancing (no enhancement after contrast agent injection), isoenhancing (similar echoge-nicity relative to the spleen), or hypoenhancing (lower echogenicity than the spleen). For chang-es with time, the following parameters were con-sidered: progressively hypoenhancing (increas-ing lesion-to-parenchyma contrast while moving to the parenchymal phase), and no residual en-hancement 300 seconds after contrast agent injec-tion. Enhancement patterns related to the arterial and to the parenchymal phase were classified as rimlike (a continuous ring of peripheral enhance-ment), centripetal (peripheral filling with cen-tripetal progression), centrifugal (a central ves-sel branching from the center to the periphery followed by homogeneous enhancement), diffuse (homogeneous or heterogeneous enhancement of
the entire lesion), or dotted (tiny spots of enhance-ment distributed throughout the lesion). Contrast-enhanced sonograms were additionally evaluated for the presence or absence of intralesional vessels or focal intralesional perfusion defects.
Consensus assessment of lesion enhancement was performed before reference standard exam-inations. The specific features of enhancement were then analyzed in conjunction with the refer-ence standard diagnosis of each lesion to establish criteria for differential diagnosis of splenic lesions with contrast-enhanced sonography.
Off-Site AnalysisFour readers with 13 and 6, 10 and 6, 8 and 2,
15 and 8 years, respectively, of sonography and contrast-enhanced sonography experience, who were not involved in the sonographic examina-tions and who were blinded to the identification, biopsy results, and other imaging findings of the patients, independently reviewed stored digital cine loops on the screen of a PACS workstation. Readers 1 and 2 were blinded to any clinical in-formation. Readers 3 and 4 were aware of wheth-er the individual patient had a history of cancer; immunodeficiency conditions; a particular clini-cal condition (such as sepsis, endocarditis, drug abuse, pancreatic disease, or a hematologic disor-der); symptoms (such as fever, acute abdominal pain, abdominal discomfort, or weight loss); or a history of acute or past trauma. Readers 3 and 4 were also aware of the spleen size, focal pattern (size and number of splenic lesions), and con-current extrasplenic abdominal findings (number and sizes of solid liver lesions or enlarged lymph nodes, including maximum size).
Cine clips were randomly presented and dis-played in the following sequence: first, base-line sonography and next, contrast-enhanced sonography (first arterial and then parenchy-mal phase). For each lesion, readers were asked to give a diagnosis of benign or malignant after reviewing the baseline sonograms and then after reviewing the contrast-enhanced sonograms, ac-cording to the sonographic criteria listed in Ta-ble 2. The criteria were developed on the basis of our on-site analysis (see below) and imaging and enhancement pattern previously described at con-ventional sonography [1–5], contrast-enhanced sonography [27–37], CT [6–14], and MRI [15–20]. Readers 3 and 4 could additionally use clini-cal criteria (Table 2), which describe the typical context in which the respective benign or malig-nant lesions occur [1–3, 7–12, 14, 17, 28, 29]. All readers used a 5-point scale to grade diagnostic confidence: grade 1, definitively benign; 2, prob-ably benign; 3, indeterminate; 4, probably malig-nant; and 5, definitively malignant.

AJR:193, September 2009 711
Sonography of Focal Splenic LesionsT
AB
LE
1:
Gen
eral
Fea
ture
s an
d M
eth
od
s U
sed
to
Co
nfi
rm t
he
Dia
gno
sis
of
147
Fo
cal S
ple
nic
Les
ion
s
Diag
nosi
s
Patie
nts
Sple
nic
Lesi
ons
Abd
omin
al F
indi
ngsa
Clin
ical
His
tory
Clin
ical
Man
ifest
atio
neM
etho
d of
Con
firm
atio
neM
/Fa
Age
(y)b
Size
(mm
)cSi
ngle
/M
ultip
led
Sple
nom
egal
ydLi
ver
Lesi
onsd
Lym
ph
Nod
esd
Canc
er
Know
ndIm
mun
olog
ic
Defe
ctd
Infe
ctio
us
Bact
eria
l abs
cess
6/1
67 (3
8–79
)46
(32–
58)
7/0
30
01
3Fe
ver a
nd e
ndoc
ardi
tis (2
), dr
ugs
(2),
panc
reat
itis
(2),
or
seps
is (1
)
Sple
en b
iops
y (4
), sp
lene
ctom
y (2
), or
ba
cter
iolo
gy fr
om b
lood
cul
ture
with
CT
and
son
ogra
phic
follo
w-u
p (1
)
Fung
al a
bsce
ss1/
133
(27–
40)
17 (1
3–19
)0/
2 2
20
22
Feve
r and
agg
ress
ive
chem
othe
rapy
of l
euke
mia
(2
)
Bact
erio
logy
from
asp
iratio
n of
live
r le
sion
s w
ith C
T an
d so
nogr
aphi
c fo
llow
-up
(2)
Tube
rcul
osis
3/1
36 (3
1–47
)15
(12–
18)
0/4
43
40
4Fe
ver a
nd A
IDS
(3) o
r med
ical
im
mun
osup
pres
sion
(1)
Aut
opsy
(2) o
r ext
rasp
leni
c bi
opsy
with
CT
and
son
ogra
phic
follo
w-u
p (2
)
Cyst
ic
Post
trau
mat
ic2/
341
(14–
58)
51 (3
1–74
)5/
00
00
10
Inci
dent
al fi
ndin
g (4
) or
stag
ing
(1) w
ith h
isto
ry o
f re
mot
e tr
aum
a
Sple
nect
omy
(1) o
r his
tory
of t
raum
a w
ith C
T an
d so
nogr
aphi
c fo
llow
-up
(4)
Echi
noco
ccus
1/2
59 (5
8–67
)75
(52–
96)
0/3
31
00
0In
cide
ntal
(2) o
r pal
pabl
e (1
) m
ass
in a
pat
ient
from
en
dem
ic a
rea
Sple
nect
omy
(2) o
r pos
itive
ser
olog
y w
ith C
T an
d so
nogr
aphi
c fo
llow
-up
(1)
Beni
gn v
ascu
lar
Hem
angi
oma/
ham
arto
ma
type
15/1
148
(20–
72)
23 (1
1–50
)20
/63
32
80
Inci
dent
al fi
ndin
g (1
9) o
r tu
mor
sta
ging
(7)
Sple
nect
omy
(2),
auto
psy
(2),
or C
T (5
), M
RI (1
7), a
nd s
onog
raph
ic fo
llow
-up
(22)
Lym
phan
giom
a0/
151
300/
10
00
10
Inci
dent
al fi
ndin
g (1
)Sp
lene
ctom
y (1
)
Infa
rctio
n6/
561
(28–
78)
46 (2
7–75
)9/
27
03
71
Abd
omin
al p
ain
and
hem
atol
ogic
dis
orde
r (9)
or
panc
reat
ic c
ance
r (2)
Sple
nect
omy
(1),
auto
psy
(1),
or C
T an
d so
nogr
aphi
c fo
llow
-up
(9)
Hem
atom
a3/
138
(33–
48)
26 (1
5–34
)4/
00
00
00
Acut
e bl
unt a
bdom
inal
tr
aum
a (4
)CT
and
son
ogra
phic
follo
w-u
p (4
)
Mis
cella
neou
s
Sarc
oido
sis
2/2
51 (3
2–68
)19
(16–
28)
0/4
20
21
0In
cide
ntal
find
ing
(3) o
r tum
or
stag
ing
(1)
Sple
en b
iops
y (1
) or e
xtra
sple
nic
hist
olog
y w
ith C
T an
d so
nogr
aphi
c fo
llow
-up
(3)
Foca
l spl
eniti
s1/
056
170/
10
00
10
Tum
or s
tagi
ng (1
)Sp
lene
ctom
y (1
)
Mal
igna
nt
Lym
phom
a36
/31
51 (1
8–89
)33
(12–
95)
16/5
156
1040
474
Inci
dent
al (2
), st
agin
g (4
5), o
r pa
lpab
le m
ass
(12)
, or f
ever
w
ith a
bdom
inal
dis
com
fort
(8
)
Sple
en b
iops
y (1
8), s
plen
ecto
my
(3),
auto
psy
(3),
or e
xtra
sple
nic
hist
olog
y w
ith C
T an
d CT
or s
onog
raph
ic fo
llow
-up
(43)
Met
asta
sis
9/3
58 (3
6–74
)38
(19–
57)
3/9
69
210
0In
cide
ntal
(1),
stag
ing
(6),
or
wei
ght l
oss
with
abd
omin
al
disc
omfo
rt (5
)
Sple
en b
iops
y (2
), au
tops
y (5
), or
bio
psy
from
prim
ary
tum
ors
with
CT
and
sono
grap
hic
follo
w-u
p (5
)a A
ll da
ta a
re n
umbe
rs o
f pat
ient
s.b A
ll da
ta, e
xcep
t the
one
pat
ient
with
lym
phan
giom
a an
d on
e pa
tient
with
foca
l spl
eniti
s ar
e m
ean
(rang
e).
c All
data
, exc
ept t
he o
ne p
atie
nt w
ith ly
mph
angi
oma
and
one
patie
nt w
ith fo
cal s
plen
itis
are
mea
n (ra
nge)
of i
nves
tigat
ed le
sion
s.d De
tect
ed o
n ab
dom
inal
B-m
ode
base
line
exam
inat
ion.
e All
data
in p
aren
thes
es a
re n
umbe
rs o
f pat
ient
s.

712 AJR:193, September 2009
Stang et al.
TABLE 2: Diagnostic Criteria Used for Differentiation of Focal Splenic Lesions at Retrospective Off-Site Analysis
Lesion
Sonographic Criteria
Clinical CriteriaBaseline Contrast-Enhanced
Infectious
Bacterial abscess Variable echogenicity, irregular wall, size > 3 cm, sometimes containing septa or gas
Constantly nonenhancing, sharp delineation, sometimes enhancing septa or rim
Solitary lesion, fever or pain, often risk factors such as sepsis, endocarditis, drug abuse, immunodeficiency
Fungal abscess Hypoechoic, small (< 2 cm), sometimes centrally increased or decreased echogenicity
Progressively less-enhancing, lesion-to-parenchyma contrast increases in parenchymal phase
Multiple small (< 2 cm) concurrent splenic and hepatic lesions, no lymphadenopathy, immunodefi-ciency
Tuberculosis Homogeneously hypoechoic, small (< 2 cm)
Progressively less-enhancing, lesion-to-parenchyma contrast increases in parenchymal phase
Multiple small (< 2 cm) splenic lesions, concurrent lymphadenopathy (< 3 cm), immunodeficiency
Cystic
Posttraumatic Usually anechoic, reflective content can result from hemorrhage, wall calcifica-tions
Constantly nonenhancing, avascular round configuration, sharp delineation
Incidental finding, solitary lesion, history of temporally remote trauma (> 6 mo)
Echinococcus Well-defined (multi-)cystic mass, sometimes mixed reflectivity and solid-cystic appearance
Constantly nonenhancing lesion Incidental finding or palpable mass in patients from endemic areas
Benign vascular
Hemangioma/hamartoma type Usually hyperechoic, well-marginated, sometimes iso- to hypoechoic and with cystic changes or calcifications (> 3 cm)
Constantly homogeneously isoenhancing, rarely centripetal filling or spoke-wheel enhancement or less uptake in parenchymal phase
Incidental finding, often solitary lesion
Lymphangioma “Honeycomb” of multiple small cysts (containing lymphlike fluid), reflective septa, and wall
Constantly nonenhancing lesion, no enhancing of septa and rim
Rare incidental finding, multiple solid-cystic subcapsular lesions
Infarction Variable echogenicity, wedge-shaped, round or oval, irregular delineation
Constantly nonenhancing, wedge-shaped defect, sometimes with partially residual perfusion
Acute abdominal pain, underlying conditions such as hematologic disorder, pancreatic disease, endocarditis
Hematoma Initially hyperechoic, poorly marginated, irregular areas that become hypoechoic within hours or days
Constantly nonenhancing, irregular configured areas
Acute abdominal trauma, variable degrees of splenic injury (laceration, fracture, hematomas, rupture)
Miscellaneous
Sarcoidosis Homogeneously hypoechoic, < 3 cm Progressively less-enhancing, lesion-to-parenchyma contrast increases in parenchymal phase
Multiple splenic lesions (< 3 cm), ± lymphadenopathy (< 2 cm), immunocompetent individuals
Focal splenitis Homogeneously hypoechoic, < 2 cm Progressively less enhancing or nonenhancing
Multiple small (< 2 cm) peripheral splenic lesions
Malignant
Lymphoma Hypoechoic, well-marginated, rarely iso- or hyperechoic or inhomogeneous echogenicity
Progressively less-enhancing vessels during arterial phase, lesion-to-parenchyma contrast increases with dotted aspect at late phase (residual microcirculation without tumor enhancement)
Known lymphoma, found at staging procedure, single (3–10 cm) or multiple small (< 3 cm) lesions, concurrent abdominal lymphade-nopathy (> 3 cm) or splenomegaly
Metastasis Variable echogenicity, mainly hypoechoic solid or cystic-solid mass, sometimes a halo rim
Progressively less-enhancing vessels during arterial phase, lesion-to-parenchyma contrast increases with minimal enhancement at late phase, sometimes nonperfused necrotic areas or rim enhancement
Known cancer, abdominal discomfort, weight loss, concurrent solid hepatic lesions of varying size

AJR:193, September 2009 713
Sonography of Focal Splenic Lesions
Reference StandardsTable 1 provides information about the meth-
ods of confirmation. Pathologic, microbiologic, radiologic, and clinical reports, including notes on treatment and findings on follow-up imaging, were reviewed by two of the authors. CT and MR imag-es were interpreted by senior radiologists who had 10–25 years of experience in abdominal CT and MRI. Technical settings were used according to the experience and practice of the readers. Estab-lished CT [6–14] and MRI criteria [15–20] were used to characterize the lesions. For 51 (24 lym-phomas, seven metastases, six bacterial abscess-es, two tuberculoses, one posttraumatic cyst, two parasitic cysts, four benign vascular tumors, one lymphangioma, two infarctions, one sarcoidosis, one focal splenitis) of 147 lesions, the reference standard diagnosis was obtained at histologic or bacteriologic analysis of a needle biopsy (n = 25) or splenectomy (n = 14), obtained 1–22 days af-ter the sonography examination, or at autopsy (n = 12), obtained between 2 and 14 months after sonography examination. For 96 (43 lymphomas, five metastases, one bacterial abscess, two fungal abscesses, two tuberculoses, four posttraumatic cysts, 22 benign vascular tumors, nine infarctions, four hematomas, three sarcoidoses, one parasitic cyst) of 147 lesions, the reference standard diagno-sis was made using contrast-enhanced CT (n = 94) or contrast-enhanced MRI (n = 17), which depict-ed the typical reported imaging features of the re-spective specific lesion diagnoses at the time of di-agnosis, followed by serial sonography performed 6–12 months apart with no or adequate changes in lesion diameter either spontaneously or after spe-cific therapy considered to be confirmatory crite-ria for specific lesion diagnosis. The detailed cri-teria are listed in Appendix 1.
Statistical AnalysisThe relationship between contrast-enhance-
ment features determined at on-site analysis and lesion benignancy or malignancy determined at reference standard examination was assessed us-ing Fisher’s exact test. The value of the enhance-ment feature for the assessment of benignancy or malignancy was calculated in terms of accuracy, sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV).
The off-site retrospectively determined be-nign or malignant lesion diagnoses were judged as true-positive (malignant lesion correctly diag-nosed, confidence grade of 4 or 5); true-negative (benign lesion correctly diagnosed, confidence grade 1 or 2); false-negative (malignant lesion incorrectly assessed as benign, confidence grade 1 or 2; or judged to be indeterminate, confidence grade 3); or false-positive (benign lesion incor-
rectly assessed as malignant, confidence grade 4 or 5; or judged to be indeterminate, confidence grade 3).
Differences in diagnostic performance before and after contrast-enhanced sonography for the cor-rect diagnosis of each lesion as benign or malignant were assessed using the McNemar test to compare accuracy, sensitivity, and specificity, and Fisher’s ex-act test to compare positive and negative predictive values. Differences in diagnostic confidence were assessed at receiver operating characteristic (ROC) curve analysis using the response from the 5-point grade scale and by plotting the sensitivity (i.e., true-positive fraction against 1 – specificity (i.e., false-positive fraction). The areas under ROC curves (Az) were calculated using the trapezoidal rule; areas were compared with the SAS “ROC” macro based on the method of DeLong et al. [38] and Hanley and McNeil [39] for analyzing paired data.
Weighted kappa statistics were calculated to assess interreader agreement in diagnostic con-fidence at both review of the baseline sonograms and review of the contrast-enhanced sonograms. Agreement was graded as poor (κ < 0.20), moder-ate (κ, 0.20 to < 0.40), fair (κ, 0.40 to < 0.60), good (κ, 0.60 to < 0.80), or very good (κ, 0.80–1.00).
All statistical analyses were performed using the computer software package SAS (version 9.1, SAS Institute). For all tests, two-tailed p values of less than 0.05 were considered to indicate statisti-cal significance.
ResultsOn-Site Analysis
Table 3 summarizes the consensus classifi-cation of the arterial and parenchymal en-hancement features related to the reference standard diagnoses of the 147 splenic lesions. There were three major features that described the dynamic lesion enhancement relative to the spleen: constantly nonenhancing (Fig. 1), constantly isoenhancing (Figs. 2 and 3), and progressively hypoenhancing while moving to the parenchymal phase (Figs. 4–6). All 31 constantly nonenhancing lesions were benign (11 infarctions, seven bacterial abscesses, five posttraumatic cysts, three parasitic cysts, four hematomas, one lymphangioma). All 26 con-stantly isoenhancing lesions were benign vascu-lar lesions, either hemangioma or hamartoma. Of 90 progressively hypoenhancing lesions, 11 (12%) were benign (four sarcoidosis, four tuberculosis, two fungal abscesses, one focal splenitis) and 79 (88%) were malignant (67 lymphoma, 12 metastases). Significant differ-ences (p < 0.0001) were seen in the PPV pre-dicting malignancy or a benign cause when considering enhancement pattern as constantly
non or isoenhancing (PPV, 100% for benig-nancy) or progressively hypoenhancing (PPV, 87.8% for malignancy) (Table 4).
Of 26 isoenhancing lesions, 17 (65%) showed a diffuse homogeneous and nine (35%) a diffuse heterogeneous enhancement during the arterial phase. Centripetal filling was not observed. Two of 26 (8%) lesions judged to be isoenhancing showed a short pe-riod of slight hyperenhancement during the arterial phase, and eight of these 26 (31%) lesions developed a slightly lower intense en-hancement relative to the spleen at the end of the parenchymal phase (Fig. 4C). None of these lesions showed intralesion vessels.
Among the 90 progressively hypoenhanc-ing lesions, most were malignant (79 of 90); only a minority were benign (11 of 90). Giv-en a progressively hypoenhancing lesion, the following enhancement patterns appear to be indicative of malignancy: diffuse hetero-geneous enhancement in the arterial phase (59% [47/79] of malignant vs 36% [4/11] of benign lesions), a dotted aspect devel-oping during the parenchymal phase (87% [69/79] of malignant vs 27% [3/11] of be-nign lesions), irregular intralesional vessels (59% [47/79] of malignant vs 9% [1/11] of benign lesions), and probably the demarca-tion of nonperfused intralesional necrotic ar-eas (16% [13/79] of malignant vs 9% [1/11] of benign lesions) (Table 3).
With knowledge of the reference standard diagnoses, analysis of the enhancement fea-tures was applied empirically to develop the diagnostic criteria shown in Table 2.
Off-Site Retrospective AnalysisTable 5 summarizes the individual confi-
dence ratings of the four off-site readers for the 68 benign and 79 malignant splenic le-sions after review of baseline B-mode and contrast-enhanced sonograms. Review of contrast-enhanced sonograms significantly reduced the rate of indeterminate diagnoses for the blinded readers 1 and 2 (from 38% and 36% to 11% and 9%; p < 0.05; respec-tively) as well as the unblinded readers 3 and 4 (from 19% and 15% to 4.8% and 4.8%; p < 0.05; respectively). Interreader agreement improved after review of contrast-enhanced sonograms between the blinded readers 1 and 2 (from weighted κ = 0.63–0.79) and be-tween the unblinded readers 3 and 4 (from weighted κ = 0.72–0.86).
Table 6 presents the diagnostic performanc-es of all four off-site readers for differentiat-ing benign and malignant lesions at baseline

714 AJR:193, September 2009
Stang et al.T
AB
LE
3:
Co
ntr
ast
En
han
cem
ent
Du
rin
g L
ow
-Mec
han
ical
-In
dex
Pu
lse
-In
vers
ion
So
no
grap
hy
Aft
er S
ulf
ur–
Hex
aflu
ori
de
Ad
min
istr
atio
n in
147
Fo
cal
Sp
len
ic L
esio
ns
at O
n-S
ite
An
alys
is
Sple
nic
Lesi
ons
Exte
nt o
f Enh
ance
men
tPa
ttern
of E
nhan
cem
enta
Art
eria
l Pha
sePa
renc
hym
al P
hase
Art
eria
l Pha
seb
Pare
nchy
mal
Pha
seSp
ecia
l Fea
ture
s
Diag
nosi
sN
o. o
f Le
sion
sN
on-
enha
ncin
gIs
o-en
hanc
ing
Hyp
o-en
hanc
ing
Non
-en
hanc
ing
Iso-
enha
ncin
gH
ypo-
enha
ncin
g
Diffu
se
Hom
o-ge
neou
s
Diffu
se
Hete
ro-
gene
ous
Rim
like
Diffu
se
Hom
o-ge
neou
s
Diffu
se
Hete
ro-
gene
ous
Rim
like
Dotte
dIrr
egul
ar
Vess
els
Nec
rotic
A
reas
Infe
ctio
us
Bact
eria
l ab
sces
s7
70
07
00
00
0c0
00
00
0
Fung
al a
bsce
ss2
00
20
02c
20
02
00
00
0
Tube
rcul
osis
40
04
00
4c2
20
12
01
01
Cyst
ic
Post
trau
mat
ic5
50
05
00
00
00
00
00
0
Echi
noco
ccus
33
00
30
00
00
00
00
00
Beni
gn v
ascu
lar
Hem
angi
oma/
ham
arto
ma
type
260
26d
00
26e
017
90
179
00
00
Lym
phan
giom
a1
10
01
00
00
00
00
00
0
Infa
rctio
n11
11c
00
110
00
00
00
00
00
Hem
atom
a4
40
04
00
00
00
00
00
0
Mis
cella
neou
s
Sarc
oido
sis
40
04
00
4c2
20
20
02
10
Foca
l spl
eniti
s1
00
10
01c
10
01
00
00
0
Mal
igna
nt
Lym
phom
a67
08
590
067
c27
400
06
061
406
Met
asta
sis
120
012
00
12c
37
20
42
67
7
Tota
l ben
ign
lesi
ons
6831
f26
d11
3126
e11
c24
130g
2311
03
11
Tota
l mal
igna
nt
lesi
ons
790
871
00
79c
3047
20
102
6747
13
Not
e—A
rter
ial p
hase
: 10–
30 s
econ
ds a
fter
con
tras
t age
nt in
ject
ion;
par
ench
ymal
pha
se: 1
50–3
00 s
econ
ds a
fter
con
tras
t age
nt in
ject
ion
a No
lesi
on s
how
ed c
entr
ifuga
l or c
entr
ipet
al p
atte
rn o
f enh
ance
men
t.b N
o le
sion
sho
wed
dot
ted
patt
ern
of e
nhan
cem
ent d
urin
g ar
teria
l pha
se.
c All
lesi
ons
wer
e pr
ogre
ssiv
ely
hypo
enha
ncin
g w
ith in
crea
sing
lesi
on-t
o-pa
renc
hym
a co
ntra
st w
hile
mov
ing
to p
aren
chym
al p
hase
.d Tw
o le
sion
s ju
dged
isoe
nhan
cing
sho
wed
sho
rt p
erio
d (<
10
seco
nds)
of h
yper
enha
ncem
ent d
urin
g ar
teria
l pha
se.
e Eigh
t les
ions
judg
ed is
oenh
anci
ng d
evel
oped
dis
cret
e lo
wer
inte
nse
enha
ncem
ent r
elat
ive
to s
plee
n at
end
of p
aren
chym
al p
hase
.f Tw
o le
sion
s ju
dged
non
enha
ncin
g sh
owed
foca
lly m
inim
al re
perf
usio
n (<
5%
of e
ntire
lesi
on) d
urin
g ar
teria
l pha
se.
g One
lesi
on ju
dged
non
enha
ncin
g sh
owed
sm
all h
yper
enha
ncin
g rim
dur
ing
arte
rial p
hase
loca
ted
outs
ide
lesi
on b
ut in
spl
enic
tiss
ue.

AJR:193, September 2009 715
Sonography of Focal Splenic Lesions
B-mode and contrast-enhanced sonography. For correct diagnosis of benignancy or malig-nancy, contrast-enhanced sonography yielded a significantly improved diagnostic perfor-
mance (overall accuracy, 51%, 43%, 70%, and 74% before vs 83%, 81%, 92%, and 91% after contrast-enhanced sonography for read-ers 1, 2, 3, and 4; p < 0.05; respectively) and
significantly improved diagnostic confidence (Az values 0.770, 0.678, 0.900, and 0.917 be-fore vs 0.935, 0.917, 0.984, and 0.959 after contrast-enhanced sonography for readers 1,
A B
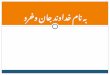
Fig. 1—35-year-old man with septic splenic infarction (Staphylococcus aureus) resulting from endocarditis.A, Baseline sonogram shows slightly enlarged spleen with wedge-shaped splenic defect (calipers) and pleural effusion.B, Contrast-enhanced sonogram shows clearly demarcated constantly nonenhancing area (calipers) (4 minutes after contrast injection).
A B
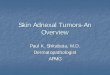
Fig. 2—61-year-old man with hepatitis and incidental detection of benign vascular splenic tumor of type hemangioma/hamartoma.A, Baseline sonogram shows slightly enlarged spleen with 4-cm slightly hyperechoic lesion (calipers).B, Contrast-enhanced sonogram shows similar enhancement of lesion and splenic tissue in parenchymal phase (calipers) (5 minutes after contrast injection).
A
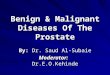
Fig. 3—58-year-old woman with incidentally detected benign vascular splenic tumor of type hemangioma/hamartoma.A, Baseline sonogram shows normal-sized spleen with 5-cm hypoechoic lesion (calipers).B, Contrast-enhanced sonogram shows isoenhancement compared with surrounding splenic tissue (calipers) in arterial phase (23 seconds after contrast injection).C, Contrast-enhanced sonogram shows discrete less contrast enhancement (calipers) compared with surrounding splenic tissue in parenchymal phase (4 minutes after contrast injection).
CB

716 AJR:193, September 2009
Stang et al.
A
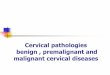
Fig. 4—52-year-old man with macronodular splenic sarcoidosis and mild splenomegaly.A, Baseline sonogram shows slightly enlarged spleen with 1.5-cm anechoic lesion resembling cyst (calipers) and smaller adjacent lesion (calipers).B, Contrast-enhanced sonogram shows vessels and slightly less enhancement (calipers) compared with adjacent splenic tissue in arterial phase (25 seconds after contrast injection).C, Contrast-enhanced sonogram shows two progressively less-enhancing lesions (calipers) in parenchymal phase (5 minutes after contrast injection).
CB
A
Fig. 5—57-year-old man with splenic non-Hodgkin’s lymphoma.A, Baseline sonogram shows enlarged spleen with 5-cm inhomogeneous hyperechoic lesion (calipers).B, Contrast-enhanced sonogram shows vessels and inhomogeneously less enhancement (calipers) compared with surrounding splenic tissue in arterial phase (30 seconds after contrast injection).C, Contrast-enhanced sonogram shows progressively less-enhancing lesion (calipers) in parenchymal phase with dotted aspect (5 minutes after contrast injection).
CB
A
Fig. 6—66-year-old man with spleen metastasis originating from melanoma.A, Baseline sonogram shows normal-sized spleen with 5-cm inhomogeneous hypoechoic lesion (calipers).B, Contrast-enhanced sonogram shows irregular vessels and small nonperfused necrotic area in less-enhancing lesion (calipers) in arterial phase (19 seconds after contrast injection).C, Contrast-enhanced sonogram shows progressively hypoenhancing lesion (calipers) in parenchymal phase (3 minutes after contrast injection).
CB

AJR:193, September 2009 717
Sonography of Focal Splenic Lesions
ed statistically the additional value of con-trast-enhanced sonography. This study pres-ents an on-site and off-site analysis of 147 focal splenic lesions identified in 147 pa-tients who underwent B-mode baseline and sulfur hexafluoride–enhanced low-mechan-ical-index pulse-inversion sonography. At on-site analysis, two site investigators were asked to assess the enhancement features of the lesions. With knowledge of the reference standard diagnosis, criteria for the differen-tial diagnosis of focal splenic lesions based on enhancement patterns were then pro-posed. At off-site analysis, four readers pro-vided confidence rating for either a benign or a malignant cause of these lesions on the basis of the diagnostic criteria. Two readers were blinded to patient history, whereas the two others were aware of patient data.
At on-site analysis, three major features were significantly correlated with benignan-cy or malignancy of the lesions: a constantly nonenhancing or constantly isoenhancing le-sion was 100% positively predictive for be-nignancy, whereas a progressively hypoen-hancing lesion was 87% positively predictive for malignancy. These results are in accor-dance with those of previous reports, which described the absence of microbubble up-take improving the identification of splenic infarcts [27–29, 31–34, 36] and lacerations [28, 29, 35] as well as the differentiation of
TABLE 4: Diagnostic Value of Contrast-Enhanced Sonography for Differentiation of Benign and Malignant Splenic Lesions Based on Three Major Contrast Enhancement Featuresa,b at On-Site Analysis
Parameter Values
Accuracy (%) 92.5 (87–96) [136/147]
Sensitivity (%) 100 (95–100) [79/79]
Specificity (%) 83.8 (73–92) [57/68]
Positive predictive value (%) 87.8 (79–94) [79/90]
Negative predictive value (%) 100 (94–100) [57/57]
Note—Data are percentages (95% CIs) [raw data].aProgressively hypoenhancing lesions: 79 malignant (true-positive), 11 benign (false-positive). Constantly non- or isoenhancing lesions: 57 benign (true-negative), 0 malignant (false-negative).
bSignificant difference between progressively hypoenhancing and constantly non- or isoenhancing lesion groups related to malignancy or benignancy of lesions (p < 0.0001, Fisher’s exact test).
TABLE 5: Confidence Rating of 147 Focal Splenic Lesions at Retrospective Off-Site Analysis
Rating Grade
Reader 1 Reader 2 Reader 3 Reader 4
Benign Lesions (n = 68)
Malignant Lesions (n = 79)
Benign Lesions (n = 68)
Malignant Lesions (n = 79)
Benign Lesions (n = 68)
Malignant Lesions (n = 79)
Benign Lesions (n = 68)
Malignant Lesions (n = 79)
Baseline B-mode sonography
1 6 7 24 28
2 22 17 5 16 17
3 24 32 19 34 13 15 10 12
4 9 22 19 14 12 16 9 15
5 7 25 6 26 3 48 4 52
Contrast-enhanced sonography
1 46 47 51 51
2 7 5 2 10 9
3 7 9 4 9 3 4 2 5
4 3 18 7 16 3 14 2 12
5 5 52 5 50 1 61 4 62
Note—Readers 1 and 2 were blinded to clinical data; readers 3 and 4 were unblinded to clinical data. Five-point grading system: 1, definitively benign; 2, probably benign; 3, indeterminate; 4, probably malignant; 5, definitively malignant.
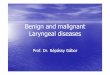
2, 3, and 4; p < 0.05; respectively) for all read-ers. Figure 7 illustrates the individual im-provements in diagnostic confidence using ROC analysis.
DiscussionIn the current clinical algorithm, patients
in whom a definite diagnosis of focal splenic lesions cannot be reached with conventional sonography alone are referred for contrast-enhanced CT or MRI. The most reliable di-agnostic criteria for noninvasive differentia-tion between benign and malignant splenic lesions are based on enhancement pattern seen after contrast agent injection on CT
[6–14] and MRI [15–20]. Contrast agents for sonography show the lesional and paren-chymal enhancement analogous to that seen on CT and MR images. A unique compo-nent of contrast-enhanced sonography is the real-time evaluation of lesional enhancement relative to the spleen during the arterial and parenchymal phases when performed with a low-mechanical-index, nonlinear sono-graphic technique combined with a second-generation agent such as sulfur hexafluoride [21, 25, 26]. Several studies have recently de-scribed contrast-enhanced sonography find-ings in various benign and malignant splenic lesions. However, no study has yet investigat-

718 AJR:193, September 2009
Stang et al.
avascular cystic processes or abscesses from solid splenic tumors [28, 33, 34], and which indicated low microbubble uptake in malig-nant lesions and similar uptake in heman-giomas compared with the splenic parenchy-ma [27–34, 37]. Our study underscores that real-time evaluation of the contrast dynam-ics of a lesion relative to the spleen is key for improving lesional characterization.
Sulfur hexafluoride has shown a late spleen- specific uptake that is probably related to mi-crobubbles pooling in splenic sinusoids [26]. Splenic hemangiomas arise from the sinusoi-
dal epithelium and contain capillary or cavern-ous vascular channels, whereas the rare ham-artomas are composed of a mixture of normal splenic components [12]. Without histolog-ic type, both could be summarized as benign vascular splenic tumors of the type heman-gioma/hamartoma [28]. As shown in this and previous studies [27–30, 34], this tumor type typically becomes isoenhancing and even un-detectable after sulfur hexafluoride injection. This effect could result from prolonged intra-tumoral blood pool phase or from accumula-tion in the sinusoidal components. Thirty-one
percent of lesions (8/26) classified as heman-gioma/hamartoma showed a minimal wash-out in the parenchymal phase. In such cases, the absence of major intralesional vessels was important for differentiation from lymphoma-tous lesions and metastases.
Unlike other studies using contrast-en-hanced sonography [27–29, 31, 33, 34, 37], we never observed a clearly hyperenhancing lesion or any centripetal filling. Although most splenic hemangiomas may appear con-stantly isoechoic [27–29, 34], some authors reported high-flow hemangiomas appearing hyperenhancing during the arterial phase [31, 33] and low-flow hemangiomas appear-ing progressively hyperenhancing on de-layed parenchymal phase scans [27, 29, 34, 37]. There are also reports describing cen-tripetal filling [28, 29, 31, 33, 34].
The described features are rare and are usually absent in small splenic hemangiomas [27–29, 34]. The lack of these features in our series might in part be explained by the small mean size (23 mm) of lesions classified as hemangioma/hamartoma. Another possi-ble explanation is that we administered the entire sulfur hexafluoride dose (4.8 mL). We wanted to ensure a high sensitivity for de-tecting the sonographic contrast agent in the initial phase of our experience and to identi-fy conditions in which a reduced dose would suffice. Bolus dynamics of the entire sulfur hexafluoride dose might have obscured the described features in our series. Further-more, we and other groups [28, 29] experi-enced that the enhancement after injection of 4.8 mL of sulfur hexafluoride can be so in-tense as to impair the examination of deeper parts of the spleen because of self-shadow-ing. As a consequence, we now recommend that not more than 2.4 mL sulfur hexafluo-ride be administered for contrast-enhanced sonography of splenic lesions.
A progressively hypoenhancing lesion type was 100% sensitive but not specific (83%) for malignancy. In general, this feature may in-dicate a perfused solid splenic lesion of tis-sue devoid of sinusoids. Given a progressively hypoenhancing lesion, the following pattern was typically associated with malignancy: heterogeneous enhancement with feeding pe-ripheral and irregular intralesional vessels in the arterial phase and a dotted aspect in the parenchymal phase representing residual microbubble microcirculation without tumor enhancement. This dynamic pattern also has been observed by other groups and may be indicative of a malignant lesion [27–30].
TABLE 6: Diagnostic Performance of Baseline and Contrast-Enhanced Sonography at Retrospective Off-Site Analysis
Performance Parameter Baseline SonographyContrast-Enhanced
Sonography p
Accuracya
Reader 1 51 (43–59) [75/147] 83 (76–89) [123/147] < 0.0001
Reader 2 43 (35–52) [64/147] 81 (74–87) [120/147] < 0.0001
Reader 3 70 (63–78) [104/147] 92 (87–96) [136/147] < 0.0001
Reader 4 74 (67–81) [110/147] 91 (85–95) [134/147] < 0.0001
Sensitivitya
Reader 1 59 (47–70) [47/79] 88 (79–94) [70/79] < 0.0001
Reader 2 50 (39–62) [40/79] 86 (76–92) [68/79] < 0.0001
Reader 3 81 (70–88) [64/79] 94 (87–98) [75/79] 0.0009
Reader 4 83 (73–90) [66/79] 93 (85–97) [74/79] 0.0047
Specificitya
Reader 1 41 (29–53) [28/68] 77 (66–87) [53/68] < 0.0001
Reader 2 35 (24–47) [24/68] 76 (64–85) [52/68] < 0.0001
Reader 3 58 (46–70) [40/68] 89 (79–95) [61/68] < 0.0001
Reader 4 64 (52–75) [44/68] 88 (78–94) [60/68] 0.0002
Positive predictive valuea
Reader 1 54 (42–64) [47/87] 82 (72–89) [70/85] < 0.0001
Reader 2 47 (36–58) [40/84] 80 (70–88) [68/84] < 0.0001
Reader 3 69 (58–78) [64/92] 91 (83–96) [75/82] 0.0003
Reader 4 73 (62–82) [66/90] 90 (81–95) [74/82] 0.0056
Negative predictive valuea
Reader 1 46 (33–60) [28/60] 85 (74–93) [53/62] < 0.0001
Reader 2 38 (26–51) [24/63] 82 (70–90) [52/63] < 0.0001
Reader 3 72 (59–83) [40/55] 93 (84–98) [61/65] 0.0022
Reader 4 77 (64–87) [44/57] 92 (82–97) [60/65] 0.0225
Azb
Reader 1 0.770 (0.700–0.844) 0.935 (0.891–0.978) < 0.0001
Reader 2 0.678 (0.595–0.761) 0.917 (0.870–0.964) < 0.0001
Reader 3 0.900 (0.853–0.947) 0.984 (0.965–1.003) 0.0001
Reader 4 0.917 (0.872–0.961) 0.959 (0.925–0.994) 0.0006aData are percentages (95% CIs) [raw data].bArea under the receiver operating characteristic curve. Data are actual values (95% CIs).

AJR:193, September 2009 719
Sonography of Focal Splenic Lesions
No clear features distinguished between metastasis and lymphomatous lesions, de-spite the fact that rapid washout and demar-cation of nonenhancing intratumoral necrot-ic areas were more frequent with metastases. In the case of successful chemotherapy, Catalano et al. [27–29] described that lym-phomatous lesions become anechoic on con-trast-enhanced sonograms with the absence of intralesional vessels and microcirculation [27–29]. The most apparent overlap between benign and malignant lesions was seen with lymphoma and nodular sarcoidosis, which each can appear with multiple progressively hypoenhancing lesions up to 3 cm in diam-eter. However, a progressively hypoenhanc-ing lesion at contrast-enhanced sonography is virtually diagnostic for splenic involve-ment in patients with an established diagno-sis of lymphoma.
For all off-site readers, the addition of con-trast-enhanced sonography significantly im-proved the diagnostic performance for correct diagnosis of benign and malignant splen-ic lesions. The degree of accuracy improve-ment from unenhanced sonography ranged from 17% to 38%. This correlates with data from a series of 46 focal splenic lesions re-ported by Görg et al. [31], who rated the di-agnostic value of using sulfur hexafluoride–enhanced low-acoustic-power pulse-inversion sonography as highly necessary for the sono-graphic diagnosis of lesions in 28% of cases.
Interreader agreement increased after re-view of contrast-enhanced sonograms between the two blinded (from κ = 0.63–0.79) and un-blinded (from κ = 0.72–0.86) readers, and the number of indeterminate lesions decreased for both blinded (from 36–38% to 9–11%) and unblinded (from 15–19% to < 5%) read-
ings. These results were based on our analysis of contrast enhancement patterns. The use of our proposed diagnostic criteria for interpre-tation of contrast-enhanced sonograms (Table 2) leads to an increased reliability and repro-ducibility in the differentiation of benign from malignant splenic lesions.
The readers with access to clinical infor-mation were more correct than the blinded readers in predicting the correct diagnosis at both baseline B-mode (70–74% vs 43–51% for blinded readers) and contrast-enhanced (91–92% vs 81–83% for blinded readers) sonography, indicating that interpretation without clinical information is more diffi-cult. Our results attest that, in a clinical set-ting, the addition of contrast material to a sonographic examination performed for the characterization of a focal splenic lesion pro-vides diagnostic accuracy that is similar to
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00.0 0.1 0.2 0.3 0.4 0.5
1 − Specificity
Sen
siti
vity
0.6 0.7 0.8 0.9 1.0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00.0 0.1 0.2 0.3 0.4 0.5
1 − Specificity
Sen
siti
vity
0.6 0.7 0.8 0.9 1.0
A
Fig. 7—Receiver operating characteristic curves are plotted to discriminate between benign and malignant focal splenic lesions after review of baseline (continuous line) and contrast-enhanced (dotted line) sonograms.A–D, Graphs illustrate increase in diagnostic confidence after review of contrast-enhanced sonograms for reader 1 (A), reader 2 (B), reader 3 (C), and reader 4 (D).
B
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00.0 0.1 0.2 0.3 0.4 0.5
1 − Specificity
Sen
siti
vity
0.6 0.7 0.8 0.9 1.0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00.0 0.1 0.2 0.3 0.4 0.5
1 − Specificity
Sen
siti
vity
0.6 0.7 0.8 0.9 1.0
C D

720 AJR:193, September 2009
Stang et al.
those that obtained using contrast-enhanced CT [6–14] or MRI [15–20].
In the clinical algorithm, contrast-en-hanced sonography can be readily imple-mented after the detection of an unclear splenic lesion on conventional sonography. The substantial reduction in the number of indeterminate diagnoses after contrast-en-hanced sonography would provide a reduc-tion in referrals for CT and MRI, with ben-efits in terms of a shorter time to diagnosis, earlier initiation of treatment, reduction of radiation risks, and reduction in costs.
Our study has limitations. First, approxi-mately two thirds of lesions were not verified by biopsy; however, the diagnoses were deter-mined using multitechnique imaging and long-term follow-up in combination with clinical information. For reasons of ethics, we decided not to perform biopsies in patients with lesions that were considered benign with available imaging data, or in whom the biopsy could be obtained with lower risk from extrasplenic sites, or in whom the biopsy result would not change the treatment or clinical outcome.
Second, our inclusion criteria specified an identified lesion visible on conventional sonography of larger than 1 cm. This criteri-on may have introduced some selection bias in favor of more easily visualized and char-acterized lesions. However, this limitation includes those of all sonography studies be-cause not all patients and lesions are suitable for sonographic examination.
Third, baseline sonograms were displayed first and contrast-enhanced sonograms there-after, which could have introduced bias be-cause more views of each lesion were seen as the reading progressed. However, this mim-ics the order in clinical use of microbubble-enhanced sonography.
Fourth, we always used the full sulfur hexafluoride dose (4.8 mL); a lower dose of ≤ 2.4 mL provides a better exploration of de-tails in the lesional enhancement and would additionally avoid self-shadowing, especially for spleens of normal size [28, 29].
Fifth, we did not analyze the additional val-ue of contrast agent injection on lesion detec-tion. Additional splenic lesions detected on contrast-enhanced sonography that were invis-ible on baseline sonography may be indicative of malignancy. This aspect can improve the di-agnostic value of contrast-enhanced sonogra-phy and should be investigated in future trials.
Sixth, despite the fact that patients were en-rolled prospectively, the diagnostic criteria of this study were applied retrospectively. A pro-
spective study is needed confirm the accuracy for the differential diagnosis of splenic lesions.
In conclusion, we show in a large series that the additional use of sulfur hexafluo-ride–enhanced low-acoustic-power pulse-inversion sonography significantly improved the diagnostic performance in the sono-graphic characterization of focal splenic le-sions as benign or malignant. If the contrast-enhanced sonographic diagnostic criteria are definitely categorized, this technique will be able to replace CT or MRI in several clinical scenarios, such as the incidental splenic le-sion at conventional sonography.
References 1. Kamaya A, Weinstein S, Desser TS. Multiple le-
sions of the spleen: differential diagnosis of cystic
and solid lesions. Semin Ultrasound CT MR 2006;
27:389–403
2. Wan YL, Cheung YC, Lui KW, Tseng JH, Lee
TY. Ultrasonographic finding and differentiation
of benign and malignant focal splenic lesions.
Postgrad Med J 2000; 76:488–493
3. Fried AM. Spleen and retroperitoneum: the essen-
tials. Ultrasound Q 2005; 21:275–286
4. Bachmann C, Görg C. The value of B-mode and
colour Doppler sonography in the diagnosis of fo-
cal splenic lesions [in German]. Ultraschall Med
2004; 25:444–447
5. Malik A, Saxena NC. Ultrasound in abdominal
tuberculosis. Abdom Imaging 2003; 28:574–579
6. Robertson F, Leander P, Ekberg O. Radiology of
the spleen. Eur Radiol 2001; 11:80–95
7. Paterson A, Frush DP, Donnelly LF, Foss JN,
O’Hara SM, Bisset GS. A pattern-oriented ap-
proach to splenic imaging in infants and children.
RadioGraphics 1999; 19:1465–1485
8. Bean MJ, Horton KM, Fishman EK. Concurrent
focal hepatic and splenic lesions: a pictorial guide
to differential diagnosis. J Comput Assist Tomogr
2004; 28:605–612
9. Carucci LR, Halvorsen RA. Abdominal and pel-
vic CT in the HIV-positive population. Abdom
Imaging 2004; 29:631–642
10. Schinina V, Rizzi EB, Mazuoli G, David V, Bib-
bolino C. US and CT findings in focal splenic le-
sions in AIDS. Acta Radiol 2000; 41:616–620
11. Urrutia M, Mego PJ, Ro LH, Torres GM, Ros PR.
Cystic masses of the spleen: radiologic–patholog-
ic correlation. RadioGraphics 1996; 16:107–129
12. Abbott RM, Levy AD, Aguliera NS, Gorope L,
Thompson WM. From the archives of the AFIP.
Primary vascular neoplasms of the spleen: radio-
logic–pathologic correlation. RadioGraphics
2004; 24:1137–1163
13. Ferrozzi F, Bova D, Draghi F, Garlaschi G. CT
findings in primary vascular tumors of the spleen.
AJR 1996; 166:1097–1101
14. Komatsuda T, Ishida H, Konno K, et al. Splenic
lymphangioma: US and CT diagnosis and clinical
manifestations. Abdom Imaging 1999; 24:414–417
15. Rabushka LS, Kawashima A, Fishman EK. Imag-
ing of the spleen: CT with supplemental MR ex-
amination. RadioGraphics 1994; 14:307–332
16. Luna A, Ribes R, Caro P, Luna L, Aumente E,
Ros PR. MRI of focal splenic lesions without and
with dynamic gadolinium enhancement. AJR
2006; 186:1533–1547
17. Elsayes KM, Narra VR, Mukundan G, Lewis JS,
Menia CO, Heiken JP. MR imaging of the spleen:
spectrum of abnormalities. RadioGraphics 2005;
25:967–982
18. Ito K, Mitchell DG, Honjo K, et al. MR imaging
of acquired abnormalities of the spleen. AJR 1997;
168:697–702
19. Ramani M, Reinhold C, Semelka RC, et al. Splen-
ic hemangiomas and hamartomas: MR imaging
characteristics of 28 lesions. Radiology 1997;
202:166–172
20. Ito K, Murata T, Nakanishi T. Cystic lymphangio-
ma of the spleen: MR findings with pathologic
correlation. Abdom Imaging 1995; 20:82–84
21. Claudon M, Cosgrove D, Albrecht T, et al. Guide-
lines and good clinical practice recommendations for
contrast-enhanced ultrasound (CEUS): update 2008
[in German]. Ultraschall Med 2008; 29:28–44
22. Cosgrove DO, Blomley MJ, Eckersley RJ, Harvey
C. Innovative contrast specific imaging with ul-
trasound. Electromedica 2002; 70:147–149
23. Burns PN, Wilson SR, Hope Simpson D. Pulse
inversion imaging of liver blood flow: improved
method for characterizing focal masses with mi-
crobubble contrast. Invest Radiol 2000; 35:58–71
24. Piscaglia F, Bolondi L. The safety of Sonovue in
abdominal applications: retrospective analysis of
23188 investigations. Ultrasound Med Biol 2006;
32:1369–1375
25. Stang A, Keles H, Seydewitz C, Hentschke S,
Braumann D. Contrast agents in transabdominal
ultrasonography: state of the art and perspectives
[in German]. Dtsch Med Wochenschr 2006; 131:
1813–1818
26. Lim AK, Patel N, Eckersley RJ. Evidence for
spleen-specific uptake of a microbubble contrast
agent: a quantitative study in healthy volunteers.
Radiology 2004; 231:785–788
27. Catalano O, Lobianco R, Sandomenico F, D’Elia
G, Siani A. Real-time contrast-enhanced ultra-
sound of the spleen: examination technique and
preliminary clinical experience. Radiol Med
2003; 106:338–356
28. Catalano O, Sandomenico F, Matarazzo I, Siani
A. Contrast-enhanced sonography of the spleen.
AJR 2005; 184:1150–1156
29. Catalano O, Sandomenico F, Vallone P, Gallipoli

AJR:193, September 2009 721
Sonography of Focal Splenic Lesions
D’Errico A, Siani A. Contrast-enhanced sonogra-
phy of the spleen. Semin Ultrasound CT MR
2006; 27:426–433
30. Tafuto S, Catalano O, Barba G, et al. Real-time
contrast-enhanced specific ultrasound in staging
and follow-up of splenic lymphomas. Front Biosci
2006; 11:2224–2226
31. Görg C, Bert T. Contrast-enhanced sonography of
focal splenic lesions with a second-generation con-
trast agent [in German]. Ultraschall Med 2005;
26:470–477
32. Görg C, Graef C, Bert T. Contrast-enhanced
sonography for differential diagnosis of an inho-
mogeneous spleen of unknown cause in patients
with pain in the left upper quadrant. J Ultrasound
Med 2006; 25:729–734
33. Görg C. The forgotten organ: contrast-enhanced
sonography of the spleen. Eur J Radiol 2007; 64:
189–201
34. Peddu P, Shah M, Sidhu PS. Splenic abnormali-
ties: a comparative review of ultrasound, mi-
crobubble-enhanced ultrasound and computed
tomography. Clin Radiol 2004; 59:777–792
35. McGahan JP, Horton S, Gercovich EO, et al. Ap-
pearance of solid organ injury with contrast-en-
hanced sonography in blunt abdominal trauma:
preliminary experience. AJR 2006; 187:658–666
36. Seeger M, Fölsch UR. Diagnosis of acute splenic
infarction by echo-enhanced ultrasound [in Ger-
man]. Dtsch Med Wochenschr 2004; 129:876–879
37. Chou YH, Chiou HJ, Tiu CM, Chiou SY, Hsia CY,
Tsay SH. Splenic hamartoma: presentation on
contrast-enhanced sonography. J Clin Ultrasound
2004; 32:425–428
38. DeLong ER, DeLong DM, Clarke-Pearson DL.
Comparing the areas under two or more correlated
receiver operating characteristics curves: a nonpara-
metric approach. Biometrics 1988; 44:837–845
39. Hanley JA, McNeil BJ. A method of comparing
the areas under receiver operating characteristic
curves derived from the same cases. Radiology
1983; 148:839–843
APPENDIX 1: Criteria for Lesion Diagnosis
The following criteria were used to establish reference standard lesion diagnoses:
Lymphoma or metastasis: Spleen biopsy showing lymphoma or metastasis or a biopsy-proven malignancy at another, extrasplenic site, with characteristic nodular spleen involvement at CT or MRI that had been shown to be progressively enlarging or reducing in size with chemotherapy at sonographic or CT follow-up.
Bacterial abscess: Bacteriologic proof obtained by spleen biopsy or from blood culture combined with typical features of a pyogenic abscess at contrast-enhanced CT (i.e., hypoattenuating lesion with ring enhancement) and regression or disappearance after antibiotic therapy at sonographic follow-up.
Fungal abscess: Liver biopsy showing candidiasis under immunosuppression, combined with typical features of hepatolienal candidi-asis at CT (i.e., multiple small, low-attenuation concurrent hepatic and splenic lesions) and regression or disappearance after antimycotic therapy at sonographic follow-up.
Nodular tuberculosis: Splenic or extrasplenic biopsy showing caseating epithelioid granulomas with presence of acid-fast bacilli and proof of Mycobacterium tuberculosis, combined with typical features of macronodular tuberculous splenic involvement at CT and re-gression after tuberculostatic therapy at sonographic follow-up.
Posttraumatic cyst: History of remote trauma combined with typical features at CT (i.e., a rounded, well-demarcated nonenhancing lesion with near-water attenuation and possible wall calcification) and no change on sonographic follow-up images obtained after more than 1 year.
Parasitic cyst: Splenectomy showing Echinococcus granularis or in a patient from an endemic area with positive serology for echi-nococcal disease combined with typical features at CT (i.e., a well-defined, nonenhancing, near-water attenuation multicystic mass) and regression or change in imaging appearance (i.e., solid cystic lesion with calcifications) after antiparasitic treatment at sonographic and CT follow-up.
Benign vascular splenic lesion of the hemangioma/hamartoma type: Spleen biopsy showing hemangioma or hamartoma or typi-cal features of hemangioma or hamartoma on dynamic contrast-enhanced CT or MRI, including hyperintensity on T2-weighted and ho-mogeneous or heterogeneous enhancement on delayed MR images, and no change on sonographic or CT follow-up images obtained af-ter more than 1 year.
Lymphangioma: Splenectomy, the only criterion.
Infarction: Splenectomy showing infarction or typically clinical conditions combined with characteristic features of infarction on contrast-enhanced CT and spontaneous regression or disappearance at sonographic or CT follow-up.
Hematoma and laceration: Acute blunt abdominal trauma combined with typical features of splenic injury on contrast-enhanced CT and spontaneous regression or disappearance at sonographic or CT follow-up.
Nodular sarcoidosis: Splenic or extrasplenic histologic proof of noncaseating epithelioid granulomas combined with features at contrast-enhanced CT or MRI compatible with a macronodular splenic sarcoidosis and regression or disappearance at sonographic follow-up, either spontaneously or after prednisolone.
Focal (nodular) splenitis: Splenectomy.