If you can't read please download the document
Upload
muftihat-israr
View
104
Download
4
Tags:
Embed Size (px)
Citation preview
DIFFUSE TOXIC GOITER BackgroundThis condition was first described by the English physician Caleb H. Parry (1755-1822). The disorder is known as Graves disease (after Robert J. Graves) in the English-speaking world and as Basedow disease (after Karl A. von Basedow) in the rest of Europe. In diffuse toxic goiter, the thyroid gland is diffusely hyperplastic and excessively overproduces thyroid hormone. This results in accelerated metabolism in most body organs. The clinical response and its manifestations are variable in intensity, distribution, and are modified by age, gender, and associated premorbid medical problems. When the diffuse toxic goiter is associated with clinical evidence of oculopathy, or rarely with dermopathy/acropachy, the term Graves disease is often applied. Awareness is needed regarding the atypical clinical presentations.
PathophysiologyThe thyroid gland is usually enlarged to a variable degree and is vascular and diffusely affected. This results in a smooth, rubbery-firm consistency, and often a bruit is heard on auscultation. Microscopically, the thyroid follicular cells are hypertrophic and hyperplastic, and they contain little colloid (stored hormone) and show evidence of hypersecretion. Lymphocytes and plasma cells infiltrate into the thyroid gland and may aggregate into lymphoid follicles. This condition is an autoimmune disorder whereby the thyroid gland is overstimulated by antibodies directed to the thyroid-stimulating hormone (TSH) receptor on the thyroid follicular cells. This antibody stimulates iodine uptake, thyroid hormonogenesis and release, and thyroid gland growth. Although mainly produced within the thyroid gland, these antibodies reach the circulation and can be measured by various assays in most, but not all, cases. The association with another autoimmune thyroid disease, Hashimoto thyroiditis, and to a lesser degree, with other autoimmune diseases in other endocrine glands and other systems in the same person is high. A strong familial association exists with the same diffuse toxic goiter or the associated disorders, especially Hashimoto thyroiditis. The presence of Hashimoto thyroiditis, which has more of a destructive effect on the thyroid gland, or the presence of another antibody, TSH-receptor blocking antibody, results in a variable natural history of the course of diffuse toxic goiter.
EpidemiologyFrequencyUnited States Diffuse toxic goiter is the most common cause of spontaneous hyperthyroidism. A Minnesota study found 0.3 new cases per 1000 per year. In late childhood, the incidence rate is 3 per 100,000 in girls and 0.5 per 100,000 in boys. Prevalence studies show a rate of 2.7% in women and 0.23% in men. A marked increase in familial incidence is noted. International Prewar Copenhagen found 0.2 new cases per 1000 per year. British studies found 0.08-0.2 new cases per 1000 per year.
Mortality/MorbidityThe natural history is usually of a benign course, which may vary in intensity of the symptoms and even spontaneously remit. The intensity of the symptoms and effect on quality of life are variable from person to person and are affected by age and gender. Mortality is rare but is due to cardiovascular problems such as heart failure, arrhythmias, or myocardial infarction. Debility and infection may occur. Thyroid storm is rare but may be fatal from dehydration, hyperthermia, and organ failure.
Morbidity may result from increased bone turnover and osteoporosis, especially in postmenopausal women, or from atrial fibrillation and its sequelae, such as thromboembolism, especially in older men. Personality changes and psychopathology, muscular weakness, and systemic symptoms all lead to quality of life changes. Associated oculopathy may be symptomatic, especially with double vision. Rarely it may progress to affect the integrity of the cornea and may even endanger vision. Associated dermopathy is uncommon and is usually minimally symptomatic, but it may be symptomatic to become debilitating. Associated hypokalemic periodic paralysis, most commonly seen in Asian males, may be sudden, dramatic, and concerning but usually runs a benign course of recovery after a few hours of skeletal muscle paralysis. A higher risk of associated immunologic diseases, such as adrenal insufficiency, each has their own associated morbidity and mortality, especially if undiagnosed.
RaceNo racial predilection exists.
SexDiffuse toxic goiter is 7-10 times more common in women than in men. It is often associated with or following a pregnancy.
AgeDiffuse toxic goiter can occur in all ages, but it is rare in children younger than 10 years and unusual in elderly persons. The peak incidence is in third and fourth decades. Incidence is increased in postpartum women, often the first presentation of disease.
PRESENTATION HistorySymptoms of the hyperthyroidism, the goiter itself, and of comorbid conditions are present. The symptoms may be present for weeks, months, or even years before diagnosis. The hyperthyroid symptoms may be multisystemic or predominate in a single organ system and mask the correct diagnosis in this manner. Many symptoms are adrenergic in origin and may be misdiagnosed as an anxiety disorder. Elderly patients may have no adrenergic symptoms and present as weight loss (malignancy), atrial fibrillation (cardiac), or apathy (depression), and this presentation is referred to as apathetic thyrotoxicosis. The presenting symptoms may be modified by preexisting medical or psychiatric disorders, which may be modified or worsened. Symptoms are described below. ; ; ; ; ; Hypermetabolism with heat generation and protein catabolism - Weight loss with good appetite, heat intolerance, sweating, muscle weakness (proximal more than distal), osteoporosis Adrenergic - Palpitations, tremor, emotional lability, insomnia, restlessness, hyperdefecation Other - Gynecomastia, lighter menses, insomnia, decreased concentration, fatigue, shortness of breath on exertion, and decreased exercise tolerance Goiter - May be mildly tender, may have difficulty swallowing if large Associated oculopathy (clinically present in about 25% of cases) - Tearing, pain, puffiness, grittiness, double vision, prominent appearance, rarely visual loss
PhysicalGeneral physical examination findings may include restless appearance, evidence of weight loss, pruritus, palmar erythema, and onycholysis of the finger nails. ; Hypermetabolism with protein catabolism - Warm hands, often with heat radiation, velvety skin, proximal muscle weakness in the arms and legs compared with distal muscle strength
;
Hyperadrenergic - Bounding and fast pulse, wide pulse pressure with higher systolic and lower diastolic blood pressure, active precordium and abdominal aorta to palpation; lid retraction (upper eyelid more than halfway from pupil to top of iris) and lid lag or globe lag, tremor of fingers, brisk reflexes Organ decompensation - Atrial fibrillation, congestive heart failure, jaundice Oculopathy - Periorbital puffiness, chemosis, conjunctival redness, proptosis (sclera visible below iris), double vision with eye movements, loss of color vision (rare), or papilledema (rare) Thyroid gland - Mildly enlarged (but may be normal in size, many times normal in size, or difficult to palpate); smooth, rubbery firm in texture; nontender or mildly tender; systolic bruit on auscultation Miscellaneous - Pretibial myxedema (uncommon), rare may be finger clubbing, diffuse lymphadenopathy, and splenomegaly
; ; ; ;
CausesDiffuse toxic goiter and its hyperthyroidism are caused by TSH-receptor stimulating antibodies. Although the exact cause is not understood, it has been suggested that there is a genetic lack of suppressor T cells that results in the unregulated production of the antibody, resulting in the autoimmune disease. The antibody may pass the placenta and result in fetal and neonatal hyperthyroidism. As with most such disorders, usually a combination of genetic and environmental factors is present. The familial association indicates a strong genetic factor. Predisposing factors include genetic susceptibility (including HLA factors); female gender; mental stress; viral infection; surgery; postpartum state; iodine administration; drugs such as lithium and iodine-containing agents, such as amiodarone, interferons and interleukins, and antiretroviral agents. Associated ophthalmopathy is not well understood, but it is a related but separate autoimmune disorder directed toward the extraocular muscles. It may run a course similar to or different from the hyperthyroidism. Smoking is an environmental aggravating factor. The presence and degree of clinical ophthalmopathy does correlate with the degree of elevation of the anti-TSH receptor antibodies. Dermopathy (pretibial myxedema) may be brought on or aggravated by local trauma.
Laboratory Studies; If hyperthyroidism due to diffuse toxic goiter is suspected after history and physical examination, the following should be performed: o o Serum TSH (sensitive or third-generation assay): Levels suppressed below normal indicate the need for more tests. Normal serum TSH level rules out this diagnosis. Serum free thyroxin (T4), or equivalent test, that compensates for any changes in thyroidbinding globulin. If levels are elevated, then hyperthyroidism is diagnosed. Levels will be in the normal range in about 5% of cases. If free thyroxin is normal, then obtain total or free serum triiodothyronine (T3) level. If levels are elevated, then hyperthyroidism is diagnosed. If levels are normal, then subclinical hyperthyroidism is present. The presence of ophthalmopathy indicates the diagnosis, and no more diagnostic testing is needed regarding the cause of the hyperthyroidism. Serum anti-TSH receptor antibodies measurements can be obtained. These antibodies are present in more than 90% of cases of diffuse toxic goiter, depending on the assay. An alternative test is radioiodine uptake. It will separate diffuse toxic goiter (elevated or normal uptake) from the hyperthyroid phase of thyroiditis (suppressed uptake). If the hyperthyroid symptoms have been present for more than 4 months, then thyroiditis is not the cause. This test is contraindicated in women who are pregnant or breastfeeding. An elevated or normal uptake may be found with a single nodular goiter and a multinodular goiter. These may be separated from diffuse toxic goiter by the absence of anti-TSH receptor antibodies, clinical examination, or thyroid scan (technetium-99m or I-123) or ultrasonography. Concomitant presence of Hashimoto thyroiditis may be detected by serum antithyroid antibodies (anti-TPO or thyroperoxidase).
o
o o o
o
o
o ;
If confirmation of oculopathy is needed, then orbital CT or MRI may be performed.
Diffuse toxic goiter would have a suppressed serum TSH level, elevated serum free thyroxin level (or T3 if needed), elevated titer of anti-TSH receptor antibodies, or elevated radioiodine uptake. No further testing is needed. Consideration of complications: ECG should be performed if arrhythmia is suspected; liver function tests may be indicated. Consideration of associated disorders: If clinical suspicion, screen for adrenal insufficiency, type 1 diabetes, gonadal failure, other autoimmune disease (eg, pernicious anemia, rheumatoid arthritis, immune thrombocytopenic purpura). Concomitant Hashimoto thyroiditis may have an effect on spontaneous resolution or progression to a hypothyroid state. Drugs that may alter T4 laboratory results include anabolic steroids, androgens, estrogens, heparin, iodine, phenytoin, rifampin, salicylates, and thyroxine/triiodothyronine.
; ;
;
Medical CareEven though the natural history of diffuse toxic goiter is to possibly spontaneously remit (and perhaps later relapse), or even progress into hypothyroidism, observation without intervention, even in minimally symptomatic people, is not recommended. The risk of bone loss and atrial fibrillation occur, especially in older women and men, even in subclinical cases. The goals of therapy are to resolve hyperthyroid symptoms and to restore the euthyroid state. Each therapeutic choice has advantages and disadvantages, so treatment should be individualized. Patient input into the treatment choice is important and must be discussed and considered. The American Thyroid Association and American Association of Clinical Endocrinologists have released guidelines for the management of hyperthyroid and other causes of thyrotoxicosis, including the use of radioactive iodine or surgery to treat toxic multinodular goiter. Therapy may be by subtotal thyroidectomy, administration of radioiodine, antithyroid drugs, or a combination of these. In North America, radioiodine is the most common treatment and is available for all ages. Adjunctive symptomatic therapy, such as beta-blockers, may help adrenergic symptoms. Nonsurgical therapy occurs in the outpatient setting. Surgical therapy requires first normalization of the hyperthyroid state by medication. Cardiac decompensation or arrhythmias may require hospitalization. Thyroid storm is a rare emergency requiring intensive care support and therapy.
Surgical CareSubtotal thyroidectomy may be considered if it is the choice of the patient, second trimester of pregnancy, failure (resistance or intolerance) of drug therapy, or poor compliance to drug therapy. Risks are low with experienced surgeons but include anesthetic risks, hemorrhage, hypoparathyroidism, and vocal cord paralysis. Patients should be made euthyroid prior to surgery to minimize anesthetic risks, cardiovascular/hemodynamic complications, and risk of thyroid storm. If normalizing with antithyroid drugs is not possible, then betablockers and potassium iodide 4 drops/day for 10 days will decrease vascularity of the thyroid gland.
ConsultationsOculopathy usually requires ophthalmologic consultation, and dermopathy may require dermatologic consultation.
DietDiet must include caloric intake to meet the energy expenditure of the hypermetabolism. High iodinecontaining substances, such as kelp, should be avoided.
ActivityPhysical activity is limited by the presence of symptoms, until recovery occurs. Usually, shortness of breath on exertion, fatigue, and palpitations are the limiting symptoms.
Medication Summary
No standard treatment protocols exist; individualization of treatment based on clinical experience is protocol. Patient preference after informed consent affects all therapeutic decisions.
Beta-blockersBeta-blockers are used if symptomatic tremor or palpitations require their use. They may be used even as investigation is ongoing because they have no effect on thyroid gland function, but they block the betaadrenergic peripheral manifestations of the hyperthyroid state. Propranolol has an effect in decreasing the peripheral conversion of T4 to T3, but this is of unknown clinical significance with the usual doses. The dose may be decreased and then stopped when the euthyroid state occurs. They should not be used in the presence of bronchospasm, even the beta1-selective agents. Calcium channel blockers may be substituted.
ThionamidesThionamide drugs, propylthiouracil (PTU) and methimazole (MTZ), inhibit hormonogenesis within the thyroid gland. PTU has an effect in decreasing the peripheral conversion of T4 to T3, but this is of unknown added clinical significance. Other than in pregnancy and breastfeeding, MTZ has advantages over PTU by a longer half-life with once-a-day dosing, and possibly more rapid return to the euthyroid state. Although rare, agranulocytosis, lupuslike vasculitis, and hepatitis are more commonly associated with PTU than with MTZ. Agranulocytosis occurs in less that 0.1% of cases but is unpredictable; it may occur at any time. Routine monitoring of WBC count is not useful. Should any infection occur, such as a sore throat, the WBC count should then be measured. Discontinuation of the drug results in a rise of WBC within a few days. Granulocyte colony-stimulating factor may need to be administered. Skin rash may perhaps be more common with MTZ; incidence is about 3%, and it usually occurs within the first few weeks of therapy. Methimazole is the drug of choice. The US Food and Drug Administration (FDA) added a boxed warning, the strongest warning issued by the FDA, to the prescribing information for PTU. The boxed warning emphasizes the risk for severe liver injury and acute liver failure, some of which have been fatal. The boxed warning also states that PTU should be reserved for use in patients who cannot tolerate other treatments, such as methimazole, radioactive iodine, or surgery. The decision to include a boxed warning was based on the FDA's review of postmarketing safety reports and on meetings held with the American Thyroid Association, the National Institute of Child Health and Human Development, and the pediatric endocrine clinical community. The FDA has identified 32 cases (22 adult and 10 pediatric) of serious liver injury associated with PTU. Of the adults, 12 deaths and 5 liver transplants occurred, and among the pediatric patients, 1 death and 6 liver transplants occurred. PTU is indicated for hyperthyroidism due to Graves disease. These reports suggest an increased risk for liver toxicity with PTU compared with methimazole. Serious liver injury has been identified with methimazole in 5 cases (3 resulting in death). PTU is considered to be a second-line drug therapy, except in patients who are allergic to or intolerant of methimazole, or in women who are in the first trimester of pregnancy. Rare cases of embryopathy, including aplasia cutis, have been reported with methimazole during pregnancy. The FDA recommends the following criteria be considered for prescribing PTU Reserve PTU use during first trimester of pregnancy, or in patients who are allergic to or intolerant of methimazole. ; ; ; ; Closely monitor PTU therapy for signs and symptoms of liver injury, especially during the first 6 months after initiation of therapy. For suspected liver injury, promptly discontinue PTU therapy, evaluate the patient for evidence of liver injury, and provide supportive care. PTU should not be used in pediatric patients unless the patient is allergic to or intolerant of methimazole and no other treatment options are available. Counsel patients to promptly contact their health care provider for the following signs or symptoms: fatigue, weakness, vague abdominal pain, loss of appetite, itching, easy bruising, or yellowing of the eyes or skin.
Monitor the serum thyroid indices monthly until euthyroid, and then the dose of the drug may be decreased for maintenance. The lowest dose needed to maintain the euthyroid state is then used for long-term therapy.
Normalization of thyroid function with these drugs must occur for some time, at least 6 months and perhaps for 1-2 years, to maximize the remission rate after drug discontinuation. Despite this, the relapse rate is 50-70%, usually within the first few weeks or months, but occasionally after a few years. Remission is weakly predicted by a short duration of symptoms, age younger than 40 years, minimal enlargement of the thyroid gland, and concomitant presence of Hashimoto thyroiditis. Relapse after discontinuation of the drug requires a decision regarding radioiodine therapy or surgery for more definitive therapy, or return to the antithyroid drug. Although general practice is not to use these drugs longterm, there is no reason why this cannot occur, if that is what the patient chooses.
IodineIn severe cases, such as thyroid storm, iodine in the form of potassium iodide (SSKI) 10 drops twice a day or iopanoic acid 1-3 g/d may be given. They inhibit the release of thyroxin from the gland and inhibit peripheral conversion of T4 to T3. They help render a euthyroid state more rapidly in response to antithyroid drugs, or prepare for surgery, but will eliminate the use of radioiodine for many months due to expansion of the iodine pool and thus decrease the delivery of radioiodine to the thyroid gland.
RadioiodineOral administration of I 131 is incorporated into the thyroid follicular cells, and the beta emission results in cell destruction and glandular fibrosis. The effect is seen in 1 and a half to 4 months. Off medications, the thyroid hormone levels become normal (requiring continued monitoring), fall below normal (requiring thyroid hormone replacement therapy, likely for life), or remain elevated (requiring another administration of radioiodine). In those becoming euthyroid, the chance every year of becoming hypothyroid due to ongoing disease in the gland is 5%; occasionally, hyperthyroidism may reoccur. The usual dose is 6-8 mCi. The dose is adjusted based on size of the thyroid gland, age of the patient, and severity of the clinical picture. Resistance is increased by age older than 40 years, large goiters, prior therapy with PTU, and nodularity (not seen with diffuse toxic goiter). Recent reviews confirm the safety of the use of radioiodine. Radioiodine therapy is not used in clinically severe hyperthyroidism or thyroid storm until the hyperthyroid state is medically controlled. Because of transplacental transfer and lactation transfer, it is contraindicated in women who are pregnant or breastfeeding. For the theoretical ovarian exposure, conception in treated women is empirically discouraged for 3-6 months. It may be administered to children, if clinically indicated. Long-term safety data in children are not available. Worsening of the hyperthyroid state may occur after radioiodine therapy due to release of prestored hormone. Gland tenderness and swelling is uncommon and may be treated with nonsteroidal anti-inflammatory drugs (NSAIDs) (not aspirin), and they rarely require steroid administration. Radioiodine administration has been associated with worsening or progression of symptomatic ophthalmopathy. Either radioiodine is avoided in very symptomatic individuals or corticosteroids (prednisone 0.5 mg/kg) are used beginning the day after the radioiodine administration for 1-3 months, or they are administered if any worsening of the ophthalmopathy occurs after radioiodine administration. Cessation of smoking and avoidance of hypothyroidism also help the course of ophthalmopathy. The return to the euthyroid state, regardless of therapy, is best monitored by serum free thyroxin, or its equivalent, because the pituitary is suppressed and TSH secretion may remain low for some time after a normal or hypothyroid state occurs. Relapse from a euthyroid state to hyperthyroidism is first monitored by new suppression of the serum TSH, and often the serum T3 then increases above normal before the serum T4 increases above normal.
Pregnancy and breastfeedingPregnancy often has an effect on improving the immunologic disease state during the pregnancy and then often relapses following delivery. The treatment of choice is PTU, which has less placental transfer than MTZ. Rare congenital anomalies reported with MTX (eg, aplasia cutis) are even less associated with PTU. Overall, the congenital abnormality rate with these drugs is similar to background normal rate. MTZ may be used if a problem exists with PTU. The goal is to keep the free thyroxin in the upper part of normal to minimize fetal drug exposure. Monthly monitoring of serum free thyroxin usually allows the dose of PTU to be decreased and often discontinued in the
third trimester. Both PTU and MTZ may be used in breastfeeding mothers. A small amount of drug does enter the milk, but neonatal thyroid levels generally remain normal. PTU and MTZ are not contraindicated in pregnancy or lactation.
Antithyroid agentsClass SummaryThese agents may either inhibit hormonogenesis within the thyroid gland or inhibit release of thyroid hormone from the gland.
Propylthiouracil (PTU)Actively transported into the thyroid gland and inhibits incorporation of iodine to thyroid hormones, and inhibits peripheral conversion of T4 to T3. Drug recommended in pregnancy and lactation with dose adjustment to minimum needed. Laboratory monitoring of free T4 to adjust dose therapy. The serum TSH may lag behind the changes in free T4. Long-term experience with this drug.
Methimazole (Tapazole)Actively transported in thyroid gland and inhibits thyroid synthesis by preventing oxidation of trapped iodine. Ten times more potent than PTU, and once-a-day dose is effective. Euthyroid state is achieved in 4-6 wk, and maintenance treatment continued for 12-24 mo. Relapse may be observed 1-6 mo after stopping therapy, occasionally later. Less desirable than propylthiouracil in pregnancy and lactation but may be used if propylthiouracil cannot be used.
Potassium iodide (Pima, Thyro-Block)Inhibits thyroid hormone secretion. Contains 8 mg of iodide per gtt. May be mixed with juice or water for intake. May decrease thyroid gland secretion and vascularity for a short time, such as 2 wk; may be used in severe cases of hyperthyroidism, such as thyroid storm, or to prepare patient for thyroidectomy
Supersaturated potassium iodide (SSKI)Contains 50 mg of iodide per drop. May be mixed with juice or water for ingestion. Inhibits thyroid hormone release.
CorticosteroidsClass SummaryThese agents have profound and varied metabolic effects.
Dexamethasone (Decadron)Steroids block peripheral conversion of T4 to T3. Used as adjunct in management of thyroid storm and symptomatic progressive Graves ophthalmopathy.
RadiopharmaceuticalsClass SummaryThese agents are used to destroy thyroid cells.
Radioiodine (I-131)Agent of choice because it is selectively taken up by the thyroid gland. Causes dysfunction or death of thyroid cells over time. Long-term experience suggests good safety profile.
Beta-adrenergic receptor blockersClass Summary
Relief of adrenergic symptoms, especially cardiac and neurologic. Propranolol blocks peripheral conversion of T4 to T3, but this is of unknown clinical significance.
Propanolol (Inderal)Nonselective beta-adrenergic receptor blocker. Also blocks peripheral conversion of T4 to T3. Used along with antithyroid drugs, before and after radioiodine treatment. Useful in thyroid crisis/storm, or in cardiac complications such as atrial fibrillation. Oral or intravenous use controls cardiac and psychomotor manifestations within minutes. Continue until euthyroid state is achieved.
GOITERBackgroundIn 1656, Thomas Wharton described the distinct nature of what he termed the thyroid gland, distinguishing it from the larynx, as this structure had been considered a laryngeal gland from the time of Andreas Vesalius in the 16th century. It was nearly 200 more years before the function of the thyroid was elucidated. The normal adult thyroid gland weighs 10-25 g and has 2 lobes connected by an isthmus. Nearly 50% of thyroid glands exhibit a pyramidal lobe arising from the center of the isthmus. Longitudinal dimensions of the lobes of the thyroid range up to 5 cm, as shown in the image below.
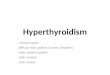
Thyroid nuclear scan of a patient with a euthyroid goiter showing different projections. A goiter is an enlarged thyroid gland, and it may be diffuse or nodular. A goiter may extend into the retrosternal space, with or without substantial anterior enlargement. Because of the anatomic relationship of the thyroid gland to the trachea, larynx, superior and inferior laryngeal nerves, and esophagus, abnormal growth may cause a variety of compressive syndromes. Thyroid function may be normal (nontoxic goiter), overactive (toxic goiter), or underactive (hypothyroid goiter).
PathophysiologyThe thyroid gland is controlled by thyroid-stimulating hormone (TSH; also known as thyrotropin), secreted from the pituitary gland, which in turn is influenced by the thyrotropin-releasing hormone (TRH) from the hypothalamus. TSH permits growth, cellular differentiation, and thyroid hormone production and secretion by the thyroid gland. Thyrotropin acts on TSH receptors located on the thyroid gland. Serum thyroid hormones levothyroxine and triiodothyronine feed back to the pituitary, regulating TSH production. Interference with this TRH-TSH thyroid hormone axis causes changes in the function and structure of the thyroid gland. Stimulation of the TSH receptors of the thyroid by TSH, TSH-receptor antibodies, or TSH receptor agonists, such as chorionic gonadotropin, may result in a diffuse goiter. When a small group of thyroid cells, inflammatory cells, or malignant cells metastatic to the thyroid is involved, a thyroid nodule may develop. A deficiency in thyroid hormone synthesis or intake leads to increased TSH production. Increased TSH causes increased cellularity and hyperplasia of the thyroid gland in an attempt to normalize thyroid hormone levels. If this process is sustained, a goiter is established. Causes of thyroid hormone deficiency include inborn errors of thyroid hormone synthesis, iodine deficiency, and goitrogens.
A goiter may result from a number of TSH receptor agonists. TSH receptor stimulators include TSH receptor antibodies, pituitary resistance to thyroid hormone, adenomas of the hypothalamus or pituitary gland, and tumors producing human chorionic gonadotropin.
EpidemiologyFrequencyUnited States Autopsy studies suggest a frequency of greater than 50% for thyroid nodules; with high-resolution ultrasonography, the value approaches 40% of patients with nonthyroidal illness. In the Wickham study from the United Kingdom, 16% of the population had a goiter. In the Framingham study, ultrasonography revealed that 3% of men older than 60 years had thyroid nodules, while 36% of women aged 49-58 years had thyroid nodules. In the United States, most goiters are due to autoimmune thyroiditis (ie, Hashimoto disease). International Worldwide, the most common cause of goiter is iodine deficiency. It is estimated that goiters affect as many as 200 million of the 800 million people who have a diet deficient in iodine. In a German study, 635 people underwent ultrasonographic thyroid screening, as well as basal TSH measurement, during a preventive-health checkup. Thyroid nodules were detected in 432 (68%) of the persons screened; in a previous German study, ultrasonographic screening of more than 90,000 people detected thyroid nodules in 33% of the normal population. The authors of the latter report attributed this difference to the fact that patients in their study were screened using 13 MHz ultrasonographic scanners, which were more sensitive than the 7.5 MHz scanners used in the previous study. According to the investigators, their results indicated that the question of routine iodine supplementation requires renewed attention.
Mortality/MorbidityMost goiters are benign, causing only cosmetic disfigurement. Morbidity or mortality may result from compression of surrounding structures, thyroid cancer, hyperthyroidism, or hypothyroidism.
RaceNo racial predilection exists.
SexThe female-to-male ratio is 4:1. ; ; In the Wickham study, 26% of women had a goiter, compared to 7% of men. Thyroid nodules are less frequent in men than in women, but when found, they are more likely to be malignant.
AgeThe frequency of goiters decreases with advancing age. The decrease in frequency differs from the incidence of thyroid nodules, which increases with advancing age.
HistoryA goiter may present in various ways, including the following: ; ; ; ; ; ; Incidentally, as a swelling in the neck discovered by the patient or on routine physical examination A finding on imaging studies performed for a related or unrelated medical evaluation Local compression causing dysphagia, dyspnea, stridor, plethora or hoarseness Pain due to hemorrhage, inflammation, necrosis, or malignant transformation Signs and symptoms of hyperthyroidism or hypothyroidism Thyroid cancer with or without metastases
Physical
The general examination for hyperthyroidism, hypothyroidism, and autoimmune stigmata is followed by systematic examination of the goiter. A retrosternal goiter may not be evident on physical examination. Examination of the goiter is best performed with the patient upright, sitting or standing. Inspection from the side may better outline the thyroid profile, as shown below. Asking the patient to take a sip of water facilitates inspection. The thyroid should move upon swallowing. See the image below.
Patient with a goiter. Prominent side-view outline. Palpation of the goiter is performed either facing the patient or from behind the patient, with the neck relaxed and not hyperextended. Palpation of the goiter rules out a pseudogoiter, which is a prominent thyroid seen in individuals who are thin. Each lobe is palpated for size, consistency, nodules, and tenderness. Cervical lymph nodes are then palpated. The oropharynx is visualized for the presence of lingular thyroid tissue. The size of each lobe is measured in 2 dimensions using a tape measure. Some examiners make tracings on a sheet of paper, which is placed in the patient's chart. Suitable landmarks are used and documented to ensure consistent measurement of the thyroid gland. The pyramidal lobe often is enlarged in Graves disease. A firm rubbery thyroid gland suggests Hashimoto thyroiditis, and a hard thyroid gland suggests malignancy or Riedel struma. Multiple nodules may suggest a multinodular goiter or Hashimoto thyroiditis. A solitary hard nodule suggests malignancy, whereas a solitary firm nodule may be a thyroid cyst. Diffuse thyroid tenderness suggests subacute thyroiditis, and local thyroid tenderness suggests intranodal hemorrhage or necrosis. Cervical lymph glands are palpated for signs of metastatic thyroid cancer. Auscultation of a soft bruit over the inferior thyroidal artery may be appreciated in a toxic goiter. Palpation of a toxic goiter may reveal a thrill in the profoundly hyperthyroid patient. Goiters are described in a variety of ways, including the following: ; Toxic goiter: A goiter that is associated with hyperthyroidism is described as a toxic goiter. Examples of toxic goiters include diffuse toxic goiter (Graves disease), toxic multinodular goiter, and toxic adenoma (Plummer disease). Nontoxic goiter: A goiter without hyperthyroidism or hypothyroidism is described as a nontoxic goiter. It may be diffuse or multinodular, but a diffuse goiter often evolves into a nodular goiter. Examination of the thyroid may not reveal small or posterior nodules. Examples of nontoxic goiters include chronic lymphocytic thyroiditis (Hashimoto disease), goiter identified in early Graves disease, endemic goiter, sporadic goiter, congenital goiter, and physiologic goiter that occurs during puberty.
;
Autonomously functioning nodules may present with inability to palpate the contralateral lobe. Unilobar agenesis may also present like a single thyroid nodule with hyperplasia of the remaining lobe. The Pemberton maneuver raises a goiter into the thoracic inlet when the patient elevates the arms. This may cause shortness of breath, stridor, or distention of neck veins.
CausesThe different etiologic mechanisms that can cause a goiter include the following: ; ; ; Iodine deficiency[ Autoimmune thyroiditis - Hashimoto or postpartum thyroiditis Excess iodine (Wolff-Chaikoff effect) or lithium ingestion, which decrease release of thyroid hormone
; ; ; ; ; ; ; ; ; ;
Goitrogens Stimulation of TSH receptors by TSH from pituitary tumors, pituitary thyroid hormone resistance, gonadotropins, and/or thyroid-stimulating immunoglobulins Inborn errors of metabolism causing defects in biosynthesis of thyroid hormones Exposure to radiation Deposition diseases Thyroid hormone resistance Subacute thyroiditis (de Quervain thyroiditis) Silent thyroiditis Riedel thyroiditis Infectious agents o o Acute suppurative - Bacterial Chronic - Mycobacteria, fungal, and parasitic
; ; ;
Granulomatous disease Thyroid malignancy Low selenium levels: This may be associated with goiter prevalence.
Laboratory Studies; Initial screening should include TSH. Given the sensitive third-generation assays in the absence of symptoms of hyper or hypothyroidism further testing is not required. An assessment of free thyroxine index or direct measurement of free thyroxine would be the next step in the evaluation. Further laboratory testing is based on presentation and results of screening studies and may include thyroid antibodies (antithyroid peroxidase formerly the antimicrosomal antibodies and antithyroglobulin), thyroglobulin, sedimentation rate and calcitonin in an individual at high risk for medullary carcinoma of the thyroid.
;
Imaging StudiesUltrasonographyEstablish and follow goiter size, consistency, and nodularity. Localize nodules for ultrasonographically guided biopsy.
RoentgenographyRoentgenography is used to assess extent of a goiter and presence of calcification. Ultrasonography has replaced this modality. Roentgenography is used to visualize calcifications within a goiter and regional lymph glands.
Computed tomography (CT) scanningCT scanning is more precise than roentgenography. CT scanning can be used to delineate size and goiter extent. Due to the superficial placement of the thyroid gland, ultrasonography is more useful in following size. CT scanning does a much better job of determining the effect of the thyroid gland on nearby structures. It also may be useful in the follow-up of patients with thyroid cancer that shows evidence of recurrence. CT scanning can be used to guide biopsy of the thyroid.
MRIMagnetic resonance imaging has the same indications as CT scanning (see above). Radionuclide uptake and radionuclide scanning are used to assess thyroid function and anatomy in hyperthyroidism, as shown below. Additionally, thyroid scanning may be useful in the patient with neck or
superior mediastinal masses. Radionuclide scanning allows determination of the function of a nodule. Function of a thyroid nodule has value both diagnostically and therapeutically. See the image below.
Thyroid nuclear scan of a patient with a euthyroid goiter showing different projections.
OtherBarium swallow is used to assess esophageal obstruction. Spirometry: The flow-volume loop is useful in determining the functional significance of compressive goiters. Perchlorate discharge test is used in individuals with inborn errors of thyroid hormone synthesis. It is used rarely today to determine the ability to trap and organify iodine.
Procedures; Fine-needle aspiration biopsy is used for cytologic diagnosis.[7] Fine-needle aspiration of the thyroid is used to determine the cause of an enlarged gland. In general, the procedure is not used in the workup of autonomously functioning nodules. The procedure has little morbidity and can be tailored to the situation. Core biopsy, or large-needle biopsy, of the thyroid uses a larger gauge needle providing a fragment of tissue. This procedure also carries with it a higher morbidity. Core biopsy has the advantage of more complete sampling. Partial thyroidectomy may be used as a first-line procedure for patients with a high probability of cancer. It is reserved mostly if the result of a fine-needle aspiration is suspicious or if the patient/physician prefers it. Total thyroidectomy is performed for malignant goiters.
;
;
;
Histologic FindingsSimple nontoxic goiters show hyperplasia, colloid accumulation, and nodularity. Nodular hyperplasia is commonly seen in multinodular goiter. Cytologic findings include benign appearing follicular cells, abundant colloid, macrophages, and, sometimes, Hrthle cells. Inflammatory disorders of the thyroid, such as chronic lymphocytic (Hashimoto) thyroiditis, contain a mixed population of lymphocytes mixed with benign appearing follicular cells. Malignant nodules may be follicular cell in origin, ie, papillary (most common), follicular, Hrthle cell, or anaplastic. They also may be from parafollicular cells, medullary carcinoma or lymphoma, or other categories.
Medical CareSmall benign euthyroid goiters do not require treatment. The effectiveness of medical treatment using thyroid hormone for benign goiters is controversial. Large and complicated goiters may require medical and surgical treatment. Malignant goiters require medical and surgical treatment. ; The size of a benign euthyroid goiter may be reduced with levothyroxine suppressive therapy. The patient is monitored to keep serum TSH in a low but detectable range to avoid hyperthyroidism, cardiac arrhythmias, and osteoporosis. The patient has to be compliant with monitoring. Some authorities suggest suppressive treatment for a definite time period instead of indefinite therapy. Patients with Hashimoto thyroiditis respond better. Treatment of hypothyroidism or hyperthyroidism often reduces the size of a goiter. Thyroid hormone replacement is often required following surgical and radiation treatment of a goiter. Use of radioactive iodine for the therapy of nontoxic goiter has been disappointing and is controversial.
; ;
; ;
Medical therapy of autonomous nodules with thyroid hormone is not indicated. Ethanol infusion into benign thyroid nodules has not been approved in the United States, but it is used elsewhere.
Surgical CareSurgery is reserved for the following situations: ; ; ; Large goiters with compression Malignancy When other forms of therapy are not practical or ineffective
ConsultationsAn endocrinologist should assess a patient at least once, and assessment should be even more frequent if the goiter is complicated by thyroid dysfunction or malignancy or if the patient is being considered for surgical management.
DietNutrition plays a role in the development of endemic goiters. Dietary factors include iodine deficiency, goitrogens, protein malnutrition, and energy malnutrition. Often these factors occur concurrently. ; Iodine: If it is practical, treat endemic goiters in iodine-deficient regions with iodine supplementation in the diet and avoidance of goitrogens. Treatment with iodine supplementation or levothyroxine may reduce goiter size. Goitrogens: Cyanoglucosides are naturally occurring goitrogens that are digested to release cyanide, which is converted to thiocyanate. Thiocyanate inhibits iodide transport in the thyroid and, at higher levels, inhibits organification. Foods that contain cyanoglucosides include cassava, lima beans, maize, bamboo shoots, and sweet potatoes. Thioglucosides are natural goitrogens found in the Cruciferae family of vegetables and weeds eaten by animals. When digested, they release thiocyanate and isothiocyanate, which have thionamidelike properties and are passed to humans via milk ingestion.
;
GRAVE DISEASEBackgroundGraves disease, named after Robert J. Graves, MD, circa 1830s, is an autoimmune disease characterized by hyperthyroidism due to circulating autoantibodies. Thyroid-stimulating immunoglobulins (TSIs) bind to and activate thyrotropin receptors, causing the thyroid gland to grow and the thyroid follicles to increase synthesis of thyroid hormone. Graves disease, along with Hashimoto thyroiditis, is classified as an autoimmune thyroid disorder.
Recent studiesBoelaert et al investigated the prevalences of and relative risks for coexisting autoimmune diseases in patients with Graves disease (2791 patients) or Hashimoto thyroiditis (495 patients). The authors found coexisting disorders in 9.7% of patients with Graves disease and in 14.3% of those with Hashimoto thyroiditis, with rheumatoid arthritis being the most common of these (prevalence = 3.15% and 4.24% in Graves disease and Hashimoto thyroiditis, respectively). Relative risks of greater than 10 were found for pernicious anemia, systemic lupus erythematosus, Addison disease, celiac disease, and vitiligo. The authors also reported a tendency for parents of patients with Graves disease or Hashimoto thyroiditis to have a history of hyperthyroidism or hypothyroidism, respectively.
PathophysiologyIn Graves disease, B and T lymphocyte-mediated autoimmunity are known to be directed at 4 well-known thyroid antigens: thyroglobulin, thyroid peroxidase, sodium-iodide symporter, and the thyrotropin receptor. However, the thyrotropin receptor itself is the primary autoantigen of Graves disease and is responsible for the
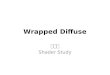
manifestation of hyperthyroidism. In this disease, the antibody and cell-mediated thyroid antigen-specific immune responses are well defined. Direct proof of an autoimmune disorder that is mediated by autoantibodies is the development of hyperthyroidism in healthy subjects by transferring thyrotropin receptor antibodies in serum from patients with Graves disease and the passive transfer of thyrotropin receptor antibodies to the fetus in pregnant women. The thyroid gland is under continuous stimulation by circulating autoantibodies against the thyrotropin receptor, and pituitary thyrotropin secretion is suppressed because of the increased production of thyroid hormones. The stimulating activity of thyrotropin receptor antibodies is found mostly in the immunoglobulin G1 subclass. These thyroid-stimulating antibodies cause release of thyroid hormone and thyroglobulin that is mediated by 3,'5'-cyclic adenosine monophosphate (cyclic AMP), and they also stimulate iodine uptake, protein synthesis, and thyroid gland growth. The anti-sodium-iodide symporter, antithyroglobulin, and antithyroid peroxidase antibodies appear to have little role in the etiology of hyperthyroidism in Graves disease. However, they are markers of autoimmune disease against the thyroid. Intrathyroidal lymphocytic infiltration is the initial histologic abnormality in persons with autoimmune thyroid disease and can be correlated with the titer of thyroid antibodies. Besides being the source of autoantigens, the thyroid cells express molecules that mediate T cell adhesion and complement regulation (Fas and cytokines) that participate and interact with the immune system. In these patients, the proportion of CD4 lymphocytes is lower in the thyroid than in the peripheral blood. The increased Fas expression in intrathyroidal CD4 T lymphocytes may be the cause of CD4 lymphocyte reduction in these individuals. Several autoimmune thyroid disease susceptibility genes have been identified: CD40, CTLA-4, thyroglobulin, TSH receptor, and PTPN22. Some of these susceptibility genes are specific to either Graves disease or Hashimoto thyroiditis, while others confer susceptibility to both conditions. The genetic predisposition to thyroid autoimmunity may interact with environmental factors or events to precipitate the onset of Graves disease. Two new susceptibility loci were found: the RNASET2-FGFR1OP-CCR6 region at 6q27 and an intergenic region at 4p14. Moreover, strong associations of thyroid-stimulating hormone receptor and major histocompatibility complex class II variants with persistently thyroid stimulating hormone receptor autoantibodies (TRAb)-positive Graves disease were found. Graves disease patients a have higher rate of peripheral blood mononuclear cell conversion into CD34+ fibrocytes compared with healthy controls. These cells may contribute to the pathophysiology of ophthalmopathy by accumulating in orbital tissues and producing inflammatory cytokines, including TNF-alpha and IL-6. Pathophysiologic mechanisms are shown in the image below.
Pathophysiologic mechanisms of Graves disease relating thyroid-stimulating immunoglobulins to hyperthyroidism and ophthalmopathy. T4 is levothyroxine. T3 is triiodothyronine.
Epidemiology
FrequencyUnited States Graves disease is the most common cause of hyperthyroidism in the United States. A study conducted in Olmstead County, Minnesota estimated the incidence to be approximately 30 cases per 100,000 persons per year. The prevalence of maternal thyrotoxicosis is approximately 1 case per 500 persons, with maternal Graves disease being the most common etiology. Commonly, patients have a family history involving a wide spectrum of autoimmune thyroid diseases, such as Graves disease, Hashimoto thyroiditis, or postpartum thyroiditis, among others. International Among the causes of spontaneous thyrotoxicosis, Graves disease is the most common. Graves disease represents 60-90% of all causes of thyrotoxicosis in different regions of the world. In the Wickham Study in the United Kingdom, the incidence was reported to be 100-200 cases per 100,000 population per year. The incidence in women in the UK has been reported to be 80 cases 100,000 per year.
Mortality/MorbidityIf left untreated, Graves disease can cause severe thyrotoxicosis. A life-threatening thyrotoxic crisis (ie, thyroid storm) can occur. Long-standing severe thyrotoxicosis leads to severe weight loss with catabolism of bone and muscle. Cardiac complications and psychocognitive complications can cause significant morbidity. Graves disease is also associated with ophthalmopathy, dermopathy, and acropachy. ; Thyroid storm is an exaggerated state of thyrotoxicosis. It occurs in patients who have unrecognized or inadequately treated thyrotoxicosis and a superimposed precipitating event such as thyroid surgery, nonthyroidal surgery, infection, or trauma. When thyroid storm was first described, the acute mortality rate was nearly 100%. In current practice, with aggressive therapy and early recognition of the syndrome, the mortality rate is approximately 20%. Long-term excess of thyroid hormone can lead to osteoporosis in men and women. The effect can be particularly devastating in women, in whom the disease may compound the bone loss secondary to chronic anovulation or menopause. Bone loss is accelerated in patients with hyperthyroidism. The increase in bone loss can be demonstrated by increased urinary pyridinoline cross-link excretion. Serum calcium and phosphate, plasma FGF-23 were significantly higher in the patients with Graves disease than in healthy control subjects, suggesting that FGF-23 is physiologically related to serum phosphate homeostasis in untreated Graves disease. Hyperthyroidism increases muscular energy expenditure and muscle protein breakdown. These abnormalities may explain the sarcopenia and myopathy observed in patients with hyperthyroid Graves disease. Cardiac hypertrophy has been reported in thyrotoxicosis of different etiologies. Rhythm disturbances such as extrasystolic arrhythmia, atrial fibrillation, and flutter are common. Cardiomyopathy and congestive heart failure can occur. Psychiatric manifestations such as mood and anxiety disorders are common. Subjective cognitive dysfunction is often reported by Graves disease patients and may be due to affective and somatic manifestations of thyrotoxicosis, which remit after treatment of Graves thyrotoxicosis. Nonpitting edema is the most prevalent form of dermopathy (about 40%) and are primarily in the pretibial area. The nearly all (>95%) patients with dermopathy had ophthalmopathy. Advanced forms of dermopathy are elephantiasis or thyroid acropachy. Severe acropachy can be disabling and can lead to total loss of hand function. Progression of ophthalmopathy can lead to compromised vision and blindness. Visual loss due to corneal lesions or optic nerve compression can be seen in severe Graves ophthalmopathy. Maternal Graves disease can lead to neonatal hyperthyroidism by transplacental transfer of thyroidstimulating antibodies. Approximately 1-5% of children of mothers with Graves disease (usually with high TSI titer) are affected. Usually, the TSI titer falls during pregnancy. Elderly individuals may develop apathetic hyperthyroidism, and the only presenting features may be unexplained weight loss or cardiac symptoms such as atrial fibrillation and congestive heart failure.
;
;
;
;
;
; ;
;
Race; In whites, autoimmune thyroid diseases are, based on linkage analysis, linked with the following loci: AITD1, CTLA4, GD1, GD2, GD3, HT1, and HT2. Different loci have been reported to be linked with autoimmune thyroid diseases in persons of other races. Susceptibility is influenced by genes in the human leukocyte antigen (HLA) region on chromosome 6 and in CTLA4 on band 2q33. Association with specific HLA haplotypes has been observed and is found to vary with ethnicity. As with most autoimmune diseases, susceptibility is increased in females. Hyperthyroidism due to Graves disease has a female-to-male ratio of 7-8:1. The female-to-male ratio for pretibial myxedema is 3.5:1. Only 7% of patients with localized myxedema have thyroid acropachy. Unlike the other manifestations of Graves disease, the female-to-male ratio for thyroid acropachy is 1:1. Typically, Graves disease is a disease of young women, but it may occur in persons of any age. The typical age range is 20-40 years. Most affected women are aged 30-60 years.
;
Sex; ; ;
Age; ; ;
HistoryBecause Graves disease is an autoimmune disorder that also affects other organ systems, taking a careful patient history is essential to establishing the diagnosis. In some cases, the history might suggest a triggering factor such as trauma to the thyroid, including surgery of the thyroid gland, percutaneous injection of ethanol, and infarction of a thyroid adenoma. Other factors might include interferon (eg, interferon beta-1b) or interleukin (IL-4) therapy. Patients usually present with symptoms typical of thyrotoxicosis. Hyperthyroidism is characterized by both increased sympathetic and decreased vagal modulation. Tachycardia and palpitation are very common symptoms. Not all patients present with such classic features. In fact, a subset of patients with euthyroid Graves disease is described. In elderly individuals, fewer symptoms are apparent to the patient. Clues may include unexplained weight loss, hyperhidrosis, or rapid heart beat. Young adults of Southeast Asian descent may complain of sudden paralysis thought to be related to thyrotoxic periodic paralysis. There is an association of polymorphisms of the calcium channel alpha1-subunit gene with thyrotoxic periodic paralysis. One third of patients with thyrotoxic hypokalemic periodic paralysis were found to have mutations in the inwardly rectifying potassium channel. The symptoms of Graves disease, organized by systems, are as follows: ; ; ; ; ; ; ; ; General - Fatigue, general weakness Dermatologic - Warm, moist, fine skin; sweating; fine hair; onycholysis; vitiligo; alopecia; pretibial myxedema Neuromuscular - Tremors, proximal muscle weakness, easy fatigability, periodic paralysis in persons of susceptible ethnic groups Skeletal - Back pain, increased risk for fractures Cardiovascular - Palpitations, dyspnea on exertion, chest pain, edema Respiratory - Dyspnea Gastrointestinal - Increased bowel motility with increased frequency of bowel movements Ophthalmologic - Tearing, gritty sensation in the eye, photophobia, eye pain, protruding eye, diplopia, visual loss
; ; ; ; ;
Renal - Polyuria, polydipsia Hematologic - Easy bruising Metabolic - Heat intolerance, weight loss despite increase or similar appetite, worsening diabetes control Endocrine/reproductive - Irregular menstrual periods, decreased menstrual volume, gynecomastia, impotence Psychiatric - Restlessness, anxiety, irritability, insomnia
PhysicalMost of the physical findings are related to thyrotoxicosis. Physical findings that are unique to Graves disease but not associated with other causes of hyperthyroidism include ophthalmopathy and dermopathy. Myxedematous changes of the skin (usually in the pretibial areas) are described as resembling an orange peel in color and texture. Onycholysis can be seen usually in the fourth and fifth fingernails. The presence of a diffusely enlarged thyroid gland, thyrotoxic signs and symptoms, together with evidence of ophthalmopathy or dermopathy, can establish the diagnosis. Common physical findings, organized by anatomic regions, are as follows: ; ; ; General - Increased basal metabolic rate, weight loss despite increase or similar appetite Skin - Warm, most, fine skin; increased sweating; fine hair; vitiligo; alopecia; pretibial myxedema Head, eyes, ears, nose, and throat - Chemosis, conjunctival irritation, widening of the palpebral fissures, lid lag, lid retraction, proptosis, impairment of extraocular motion, visual loss in severe optic nerve involvement, periorbital edema Neck - Upon careful examination, the thyroid gland generally is diffusely enlarged and smooth; a welldelineated pyramidal lobe may be appreciated upon careful palpation; thyroid bruits and, rarely, thrills may be appreciated; thyroid nodules may be palpable. Chest - Gynecomastia, tachypnea, tachycardia, murmur, hyperdynamic precordium, S3, S4 heart sounds, ectopic beats, irregular heart rate and rhythm Abdomen - Hyperactive bowel sound Extremities - Edema, acropachy, onycholysis Neurologic - Hand tremor (fine and usually bilateral), hyperactive deep tendon reflexes Musculoskeletal - Kyphosis, lordosis, loss of height, proximal muscle weakness, hypokalemic periodic paralysis in persons of susceptible ethnic groups Psychiatric - Restlessness, anxiety, irritability, insomnia, depression
;
; ; ; ; ; ;
Ophthalmopathy is a hallmark of Graves disease. Approximately 25-30% of patients with Graves disease have clinical evidence of Graves ophthalmopathy. Thyrotropin receptor is highly expressed in the fat and connective tissue of patients with Graves ophthalmopathy. Measuring diplopia fields, eyelid fissures, range of extraocular muscles, visual acuity, and proptosis provides quantitative assessment to follow the course of ophthalmopathy. Signs of corneal or conjunctival irritation include conjunctival injection and chemosis. A complete ophthalmologic examination, including retinal examination and slit-lamp examination by an ophthalmologist, is indicated if the patient is symptomatic. Although thyroid nodule(s) may be present, excluding multinodular toxic goiter (especially in older patients) as the cause of thyrotoxicosis is essential. The approach to treatment may be different. Excluding thyroid neoplasia is also important in these patients because reports have indicated that differentiated thyroid cancer is probably more common in patients with Graves disease and may also have a more aggressive course in these patients.
CausesGraves disease is autoimmune in etiology, and the immune mechanisms involved may be one of the following: ; Expression of a viral antigen (self-antigen) or a previously hidden antigen
; ; ;
The specificity crossover between different cell antigens with an infectious agent or a superantigen Alteration of the T cell repertoire, idiotypic antibodies becoming pathogenic antibodies New expression of HLA class II antigens on thyroid epithelial cells (eg, HLA-DR antigen)
The autoimmune process in Graves disease is influenced by a combination of environmental and genetic factors. Several autoimmune thyroid disease susceptibility genes have been identified: CD40, CTLA-4, thyroglobulin, TSH receptor, and PTPN22. Some of these susceptibility genes are specific to either Graves disease or Hashimoto thyroiditis, while others confer susceptibility to both conditions. HLA-DRB1 and HLA-DQB1 also appear to be associated with Graves disease susceptibility. Genetic factors contribute approximately 20-30% of overall disease susceptibility. ; Cytotoxic T lymphocyte-associated molecule-4 (CTLA4) is a major thyroid autoantibody susceptibility gene, and it is a negative regulator of T-cell activation and may play an important role in the pathogenesis of Graves disease. The G allele of exon1 +49 A/G single nucleotide polymorphism (SNP) of the CTLA4 gene influences higher TPOAb and TgAb production in patients who are newly diagnosed with Graves disease. This SNP of the CTLA4 gene can also predict recurrence of Graves disease after cessation of thionamide treatment. There is an association of a C/T SNP in the Kozak sequence of CD40 with Graves disease. The association of SNPs in PTPN22 varies among autoimmune diseases individually or as part of a haplotype, and the mechanisms by which PTPN22 confers susceptibility to Graves disease may differ from other autoimmune diseases. Alleles of intron 7 of the thyrotropin receptor gene (TSHR) have also been shown to contribute to susceptibility to Graves disease
; ;
;
Environmental factors associated with susceptibility are largely unproven. Other factors include infection, iodide intake, stress, female sex, steroids, and toxins. Smoking has been implicated in the worsening of Graves ophthalmopathy. ; Graves disease has been associated with a variety of infectious agents such as Yersinia enterocolitica and Borrelia burgdorferi. Homologies have been shown between proteins of these organisms and thyroid autoantigens. Stress can be a factor for thyroid autoimmunity. Acute stress-induced immunosuppression may be followed by immune system hyperactivity, which could precipitate autoimmune thyroid disease. This may occur during the postpartum period, in which Graves disease may occur 3-9 months after delivery. Estrogen may influence the immune system, particularly the B-cell repertoire. Both T- and B-cell function are diminished during pregnancy, and the rebound from this immunosuppression is thought to contribute to the development of postpartum thyroid syndrome. Interferon beta-1b and interleukin-4, when used therapeutically, may cause Graves disease. Trauma to the thyroid has also been reported to be associated with Graves disease. This may include surgery of the thyroid gland, percutaneous injection of ethanol, and infarction of a thyroid adenoma.
;
; ;
Laboratory StudiesUltrasensitive (third-generation) thyrotropin assays remain the best screening test for thyroid disorders. ; ; With the exception of thyrotropin-induced hyperthyroidism, subnormal or suppressed thyrotropin levels are seen in most patients with thyrotoxicosis. Free T4 levels or the free T4 index is usually elevated, as is the free T3 level or free T3 index. Subclinical hyperthyroidism, defined as a free T4 or free T3 level within the reference range with suppressed thyrotropin, also can be seen. On occasion, only the free T3 level is elevated, a syndrome known as T3 toxicosis. This may be associated with toxic nodular goiter or the ingestion of T3. Assays for thyrotropin-receptor antibodies (particularly TSIs) almost always are positive. Detection of TSIs is diagnostic for Graves disease.
; ; ;
; ; ; ;
The presence of TSIs is particularly useful in reaching the diagnosis in pregnant women, in whom the use of radioisotopes is contraindicated. Other markers of thyroid autoimmunity, such as antithyroglobulin antibodies or antithyroidal peroxidase antibodies, are usually present. Other autoantibodies that may be present include thyrotropin receptorblocking antibodies and anti sodium-iodide symporter antibody. The presence of these antibodies supports the diagnosis of an autoimmune thyroid disease.
Liver function test results should be obtained to monitor for liver toxicity caused by thioamides (antithyroid medications). A CBC count with differential should be obtained at baseline and with the development of fever or symptoms of infection. Graves disease may be associated with normocytic anemia, low-normal to slightly depressed total WBC count with relative lymphocytosis and monocytosis, low-normal to slightly depressed platelet count. Thionamides may rarely cause severe hematologic side effects, but routine screening for these rare events is not cost-effective. Investigation of gynecomastia associated with Graves disease may reveal increased sex hormonebinding globulin levels and decreased free testosterone levels. Graves disease may worsen diabetes control and may be reflected by an increase in hemoglobin A1C in diabetic patients. A fasting lipid profile may show decreased total cholesterol levels and decreased triglyceride levels. Thyrotropin-releasing hormone testing has largely been replaced by third-generation thyrotropin assays. A high titer of serum antibodies to collagen XIII is associated with active Graves ophthalmopathy.
Imaging StudiesRadioactive iodine scanning and measurements of iodine uptake are useful in differentiating the causes of hyperthyroidism. In Graves disease, the radioactive iodine uptake is increased and the uptake is diffusely distributed over the entire gland. Ultrasounds with color-Doppler evaluation have been found to be cost-effective in hyperthyroid patients. A prospective trial showed that thyroid ultrasound findings are predictive of radioiodine treatment outcome, and, in patients with Graves disease, normoechogenic and large glands are associated with increased radioresistance. Computed tomography scanning or magnetic resonance imaging (of the orbits) may be necessary in the evaluation of proptosis. If routinely performed, most patients have evidence of orbitopathy, such as an increased volume of extraocular muscles and/or retrobulbar connective tissue. These techniques are useful to monitor changes over time or to ascertain the effects of treatment. Careful monitoring is required after using iodinated contrast agents as they may affect ongoing treatment plans.
Histologic FindingsIn select cases in which thyroidectomy was performed for the treatment of severe hyperthyroidism, the thyroid glands from patients with Graves disease show lymphocytic infiltrates and follicular hypertrophy, with little colloid present.
Medical CareTreatment involves alleviation of symptoms and correction of the thyrotoxic state. Adrenergic hyperfunction is treated with beta-adrenergic blockade. Correcting the high thyroid hormone levels can be achieved with antithyroid medications that block the synthesis of thyroid hormones or by treatment with radioactive iodine.
Radioactive iodineThe most commonly used therapy for Graves disease is radioactive iodine. Indications for radioactive iodine over antithyroid agents include a large thyroid gland, multiple symptoms of thyrotoxicosis, high levels of thyroxine, and high titers of TSI. Information and guidelines are as follows: ; Many physicians in the United States prefer to use radioactive iodine as first-line therapy, especially in younger patients, because of the high relapse rate (>50%) associated with antithyroid therapy.
; ;
Radioiodine treatment can be performed in an outpatient setting. The usual dose ranges from 5-15 mCi, determined either by using various formulas that take into account the estimated thyroid weight and radioiodine uptake or by using fixed dosages of iodine I 131; detailed kinetic studies of131 I are not essential and do not lead to better treatment results. A fixed dose of 7 mCi has been advocated by some researchers as the first empirical dose in the treatment of hyperthyroidism. In general, higher dosages are required for patients who have large goiters, have low radioiodine uptake, or who have been pretreated with antithyroid drugs. Patients currently taking antithyroid drugs must discontinue the medication at least 2 days prior to taking the radiopharmaceutical. In one study, withholding antithyroid drugs for just over 2 weeks before radioiodine treatment resulted in the lowest failure rate. Pretreatment with thioanmides reduces the cure rate of radioiodine therapy in hyperthyroid diseases. Thyroid function test results generally improve within 6-8 weeks of therapy, but this can be highly variable. With radioactive iodine, the desired result is hypothyroidism due to destruction of the gland, which usually occurs 2-3 months after administration. Following up with the patient and monitoring thyroid function monthly or as the clinical condition dictates is important. When patients become hypothyroid, they require lifelong replacement with thyroid hormone. The possibility exists that radioactive iodine can precipitate thyroid storm by releasing thyroid hormones. This risk is higher in elderly and debilitated patients. This problem can be addressed by pretherapy administration with antithyroidal medication such as propylthiouracil (PTU) or methimazole, but antithyroid medication also may decrease the effectiveness of radioiodine, as discussed above. If thyroid function does not normalize within 6-12 months of treatment, a second course at a similar or higher dose can be given. Third courses are rarely needed. Hypothyroidism may ensue in the first year in up to 90% of patients given higher doses of radioiodine. Approximately one third of patients develop transient hypothyroidism. Unless a patient is highly symptomatic, thyroxine replacement may be withheld if hypothyroidism occurs within the first 2 months of therapy. If it persists for longer than 2 months, permanent hypothyroidism is likely and replacement with T4 should be initiated. Radiation thyroiditis is rare, but it may occur and exacerbate thyrotoxicosis. Long-term follow-up is mandatory for all patients. One concern with the use of radioiodine in persons with Graves disease is its controversial potential for exacerbating existing Graves ophthalmopathy. However, the presence of ophthalmopathy should not influence the choice of therapy for hyperthyroidism. If possible in patients with mild progressive ophthalmopathy, institute a course of steroids (prednisone up to 1 mg/kg) for 2-3 months, tapering a few days before radioiodine therapy. For those with no obvious ophthalmopathy, the chances of exacerbation are much lower. In patients with severe Graves ophthalmopathy, treatment of hyperthyroidism and ophthalmopathy should proceed concurrently and independently of each other. The absolute contraindication for radioiodine is pregnancy. No evidence of germ-line mutations has been demonstrated from gonadal exposure. The incidence of birth defects or abnormal pregnancies has not increased after radioiodine treatments. After radioiodine therapy, germinal epithelium and Leydig cell function may change marginally, which may have some clinical significance in male patients with preexisting fertility impairment. Because it is known that low-dose thyroid radiation exposure in children increases the risk of thyroid cancer later in life, larger doses of131 I are recommended for children. If patients are aged 6-10 years, ablative doses of131 I (100-150 mCi/g of thyroid tissue) may be used to prevent the survival of thyroid cells that may be transformed later into malignant cells.
;
; ; ; ; ;
; ; ;
; ; ;
;
;
Graves ophthalmopathyGraves ophthalmopathy can be divided into 2 clinical phases: the inflammatory stage and the fibrotic stage. The inflammatory stage is marked by edema and deposition of glycosaminoglycan in the extraocular muscles. This
results in the clinical manifestations of orbital swelling, stare, diplopia, periorbital edema, and at times, pain. The fibrotic stage is a convalescent phase and may result in further diplopia and lid retraction. It improves spontaneously in 64% of patients. Approximately 10-20% of patients have gradual progression of disease over many years, followed by clinical stability. Approximately 2-5% have progressive worsening of the disease, with visual impairment in some. Correction of both hyperthyroidism and hypothyroidism is important for the ophthalmopathy. Antithyroid drugs and thyroidectomy do not influence the course of the ophthalmopathy, whereas radioiodine treatment may exacerbate preexisting ophthalmopathy but can be prevented by glucocorticoids. In the long term, thyroid ablation may be beneficial for ophthalmopathy because of the decrease in antigens shared by the thyroid and the orbit in the autoimmune reactions. In general, treatment of hyperthyroidism is associated with an improvement of ophthalmopathy, but hypothyroidism must be avoided because it worsens ophthalmopathy. For mild-to-moderate ophthalmopathy, local therapeutic measures (eg, artificial tears and ointments, sunglasses, eye patches, nocturnal taping of the eyes, prisms, elevating the head at night) can control symptoms and signs. If the disease is active, the mainstays of therapy are (1) high-dose glucocorticoids, (2) orbital radiotherapy, (3) both, or (4) orbital decompression. For severe or progressive disease, glucocorticoids at 40 mg/d (usual dose) may be tried. The drug should be continued until evidence of improvement and disease stability is observed. The dosage is then tapered over 4-12 weeks. High-dose pulse glucocorticoid therapy has also been used with good results. A study by Liao and Huang evaluated the correlation of retrobulbar volume change, resected orbital fat volume, and proptosis reduction after surgical decompression in patients with Graves ophthalmopathy. Decompression by resecting orbital fat was found to reduce proptosis in patients with disfiguring Graves ophthalmopathy. If no response to therapy occurs in the inflammatory phase, orbital radiotherapy with or without steroids may be tried. Orbital radiotherapy does not increase the risk for radiation-induced tumors, cataract, and retinopathy, except in patients with diabetes with possible or definite retinopathy. Diuretics have a limited effect on the edema caused by venous engorgement of the orbit. Gamma knife surgery has been attempted with success in a limited number of patients, but further studies are needed to validate this approach. Surgical management is generally performed in the fibrotic phase, when the patient is euthyroid. See Surgical Care. Novel treatments such as somatostatin analogs or intravenous immunoglobulins are under evaluation. Studies with octreotide LAR (long-acting, repeatable) show conflicting or marginal therapeutic benefit for patients with Graves ophthalmopathy. Infliximab, an anti-tumour necrosis factor alpha (TNF-) antibody, has been reported to successfully treat a case of sightthreatening Graves ophthalmopathy. Rituximab, anti-CD20 monoclonal antibody, may transiently deplete Blymphocytes and potentially suppress the active inflammatory phase of Graves ophthalmopathy. A multicentered prospective pilot study suggests that periocular injection of triamcinolone may reduce diplopia and the size of extraocular muscles in patients with Graves ophthalmopathy of recent onset. In a prospective randomized trial, pentoxifylline improved symptoms and proptosis in the inactive phase of Graves ophthalmopathy.
Pretibial myxedemaSome degree of pretibial (localized dermopathy) myxedema is observed in 5-10% of patients, with 1-2% having cosmetically significant lesions. Affected patients tend to have more severe ophthalmopathy than those who are not affected. It usually manifests as elevated, firm, nonpitting, localized thickening over the lateral aspect of the lower leg, with bilateral involvement. It also may involve the upper extremities. Milder cases do not require therapy other than treatment of the thyrotoxicosis. Therapy with topical steroids applied under an occlusive plastic dressing film (eg, Saran Wrap) for 3-10 weeks has been helpful. In severe cases, pulse glucocorticoid therapy may be tried.
AcropachyClubbing of fingers with osteoarthropathy, including periosteal new bone formation, may occur. This almost always occurs in association with ophthalmopathy and dermopathy. No therapy has been proven to be effective.
Surgical CareIndications and outcomes are as follows: ; Thyroidectomy is no longer the recommended first-line therapy for hyperthyroid Graves disease. However, a retrospective cohort study showed that one-third of all patients electing surgery as definitive management did so without a specific indication, and the patient satisfaction with the decision for surgery as definitive management of Graves disease was high. Surgery is a safe alternative therapeutic option in patients who are noncompliant with or cannot tolerate antithyroid drugs, have moderate-tosevere ophthalmopathy, have large goiters, or refuse or cannot undergo radioiodine therapy. Thyroidectomy may be appropriate in the presence of a thyroid nodule that is suggestive of carcinoma. In certain cases (eg, in pregnant patients with severe hyperthyroidism), thyroidectomy may be indicated because radioactive iodine and antithyroid medications may be contraindicated. It generally is reserved for patients with large goiters with or without compressive symptoms. It also may be indicated in patients who refuse radioiodine as definitive therapy or in those in whom the use of antithyroid drugs and/or radioiodine does not control hyperthyroidism. Surgery provides rapid treatment of Graves disease and permanent cure of hyperthyroidism in most patients, and it has "negligible mortality and acceptable morbidity" by experienced surgeons. Preoperative preparation to render the patient euthyroid is essential in order to prevent thyrotoxic crisis (thyroid storm). The hyperthyroid state can be rapidly corrected using a combination of iopanoic acid, dexamethasone, beta-blockers, and thionamides. This can be accomplished with the use of antithyroid drugs for approximately 6 weeks, with or without concomitant beta-blockade. Most surgeons administer iodine (as Lugol solution or saturated solution of potassium iodide to provide 30 mg of iodine/d) for 10 days before surgery to decrease thyroid gland vascularity, the rate of blood flow, and intraoperative blood loss during thyroidectomy. With experienced surgeons, vocal cord paralysis due to superior or recurrent laryngeal nerve injury and hypoparathyroidism are rare adverse events, occurring in less than 1% of patients. Subtotal thyroidectomy is usually used with the intention of leaving enough thyroid remnants behind to avoid hypothyroidism. Importantly, keep in mind that the risk of recurrent hyperthyroidism potentially increases with larger remnant sizes. However, many studies have shown that the size of the remnant is not the only determinant of the risk of recurrence. Iodine uptake and immunologic activity (eg, level of TSI) are just 2 of the other factors that influence the risk of recurrent hyperthyroidism. If the goal of surgery is to avoid recurrent hyperthyroidism, near-total thyroidectomy has been advocated as the procedure of choice. Regardless of the extent of surgery, all patients require long-term follow-up. Near-total thyroidectomy has little, if any, effect on the course of ophthalmopathy. If ophthalmopathy is severe but inactive, orbital decompression may be performed. Reducing proptosis and decompressing the optic nerve can be achieved by transantral orbital decompression. A study by Alsuhaibani et al found that the change in the volume of the medial rectus muscle may help explain the variability in the proptosis reduction following orbital decompression. The major adverse effect is postoperative diplopia, which may necessitate a second surgery on the extraocular muscles to correct the problem. Rehabilitative (extraocular muscle or eyelid) surgery is often needed. Eyelid surgery (eg, severance of the Mller muscle, scleral or palatal graft insertion) can be performed to improve exposure keratitis.
; ; ; ; ;
Procedures and preparations are as follows: ;
; ;
; ; ;
; ; ; ; ;
Ophthalmopathy is as follows:
; ;
ConsultationsConsultation with an endocrinologist may be necessary for the management and regulation of thyroid hormone levels in atypical presentations, as follows: ; ; ; Graves disease in pregnancy Neonatal Graves disease management Graves disease complicated by a nodular thyroid gland unresponsive to usual medical therapy or in older adults Unilateral or bilateral proptosis Workup of other etiologies for eye findings besides Graves disease Follow-up of visual acuity, corneal disease prevention, and eye muscle function
Consultation with an ophthalmologist may be needed in the following situations: ; ; ;
Consultation with a dermatologist may be needed in patients with localized myxedema that is unresponsive to topical corticosteroids.
DietThe amount of iodine in the diet can influence the hormone synthesis activity in the thyroid gland. Iodine-containing food has different effects on thyroid uptake of131 I and technetium Tc 99m. Iodine-rich food decreases131 I uptake but increases99m Tc in most patients. However, the diagnostic value of a radioiodine uptake test to differentiate Graves disease and silent thyroiditis is not affected by dietary iodine intake. Iodine restriction before a radioiodine uptake test is unnecessary. Dietary iodine intake may influence the remission rate after antithyroid drug therapy. This is based on the observation that the outcome of antithyroid therapy in the older literature showed lower remission rates than it did in later studies and that the average dietary iodine content has been decreasing over the years. However, a direct causal relationship has not been established by clinical trials.
ActivityGiven the high-output state of the heart, strenuous exercise may be detrimental. The patient should be advised to avoid severe fatigue from exercise. Patients can use their pulse as a guide to activity.
HIPERTIROIDISMEPractice EssentialsHyperthyroidism is a set of disorders that involve excess synthesis and secretion of thyroid hormones by the thyroid gland, which leads to the hypermetabolic condition of thyrotoxicosis. The most common forms of hyperthyroidism include diffuse toxic goiter (Graves disease), toxic multinodular goiter (Plummer disease), and toxic adenoma.
Signs and symptomsCommon symptoms of thyrotoxicosis include the following: ; ; ; ; ; ; ; Nervousness Anxiety Increased perspiration Heat intolerance Hyperactivity Palpitations Tachycardia or atrial arrhythmia
Common signs of thyrotoxicosis include the following:
; ; ; ; ; ; ; ; ; ; ; ;
Systolic hypertension Warm, moist, smooth skin Lid lag Stare Hand tremor Muscle weakness Weight loss despite increased appetite Reduction in menstrual flow or oligomenorrhea Younger patients tend to exhibit symptoms of sympathetic activation (eg, anxiety, hyperactivity, tremor) Older patients have more cardiovascular symptoms (eg, dyspnea, atrial fibrillation) and unexplained weight loss Patients with Graves disease often have more marked symptoms than patients with thyrotoxicosis from other causes Ophthalmopathy (eg, periorbital edema, diplopia, or proptosis) suggests Graves disease
Presentation of thyrotoxicosis varies, as follows
DiagnosisThyroid function tests for hyperthyroidism are as follows: ; ; ; ; ; ; ; ; ; ; ; ; Thyroid-stimulating hormone (TSH) Free thyroxine (FT4) or free thyroxine index (FTItotal T4 multiplied by the correction for thyroid hormone binding) Total triiodothyronine (T3) Thyrotoxicosis is marked by suppressed TSH levels and elevated T3 and T4 levels Patients with milder thyrotoxicosis may have elevation of T3 levels only Subclinical hyperthyroidism features decreased TSH and normal T3 and T4 levels Anti thyroid peroxidase (anti-TPO) antibody Thyroid-stimulating immunoglobulin (TSI) Graves disease Significantly elevated anti-TPO, elevated TSI Toxic multinodular goiter- Low or absent anti-TPO Toxic adenoma Low or absent anti-TPO Patients without active thyroid disease may have mildly positive anti-TPO
Thyroid function study results in hyperthyroidism are as follows:
Autoantibody tests for hyperthyroidism are as follows:
Autoantibody titers in hyperthyroidism are as follows:
If the etiology of thyrotoxicosis is not clear after physical examination and other laboratory tests, it can be confirmed by scintigraphy: the degree and pattern of isotope uptake indicates the type of thyroid disorder. Findings are as follows: ; ; ; Graves disease Diffuse enlargement of both thyroid lobes, with uniform uptake of isotope and elevated radioactive iodine uptake Toxic multinodular goiter -- Irregular areas of relatively diminished and occasionally increased uptake; overall radioactive iodine uptake is mildly to moderately increased Subacute thyroiditis Very low radioactive iodine uptake
Management
Treatment of hyperthyroidism includes symptom relief, as well as therapy with antithyroid medications, radioactive iodine-131 (131 I), or thyroidectomy. Symptomatic treatment is as follows: ; ; ; ; Oral rehydration for dehydrated patients Beta-blockers for relief of neurologic and cardiovascular symptoms For mild ophthalmopathy, saline eye drops as needed and tight-fitting sunglasses for outdoors For vision-threatening ophthalmopathy, high-dose glucocorticoids, with consideration for orbital decompression surgery and ocular radiation therapy Used for long-term control of hyperthyroidism in children, adolescents, and pregnant women In adult men and nonpregnant women, used to control hyperthyroidism before definitive therapy with radioactive iodine Methimazole is more potent and longer-acting than propylthiouracil Propylthiouracil is reserved for use in thyroid storm, first trimester of pregnancy, and methimazole allergy or intolerance Antithyroid drug doses are titrated every 4 weeks until thyroid functions normalize Patients with Graves disease may experience remission after treatment for 12-18 months, but recurrences are common within the following year Toxic multinodular goiter and toxic adenoma will not go into remission Preferred therapy for hyperthyroidism Administered orally as a single dose in capsule or liquid form Causes fibrosis and destruction of the thyroid over weeks to many months Hypothyroidism is expected Pregnancy, breast feeding, and recent lactation are contraindications Radioactive iodine should be avoided in children younger than 5 years Radioactive iodine is usually not given to patients with severe ophthalmopathy Severe hyperthyroidism in children Pregnant women who are noncompliant with or intolerant of antithyroid medication Patients with very large goiters or severe ophthalmopathy Patients who refuse radioactive iodine therapy Refractory amiodarone-induced hyperthyroidism Patients who require normalization of thyroid functions quickly, such as pregnant women, women who desire pregnancy in the next 6 months, or patients with unstable cardiac conditions
Antithyroid drug treatment is as follows: ; ; ; ; ; ; ; ; ; ; ; ; ; ; ; ; ; ; ; ;
Radioactive iodine treatment is as follows:
Thyroidectomy is reserved for special circumstances, including the following:
BackgroundHyperthyroidism is a set of disorders that involve excess synthesis and secretion of thyroid hormones by the thyroid gland. The resulting elevation in levels of FT4, free triiodothyronine (FT3), or both leads to the hypermetabolic condition of thyrotoxicosis. Thus, although many clinicians (endocrinologists excluded) use the terms hyperthyroidism and thyrotoxicosis interchangeably, the 2 words have distinct meanings. For example, both exogenous thyroid hormone intake and subacute thyroiditis can cause thyrotoxicosis, but neither constitutes hyperthyroidism, because the conditions are not associated with new hormone production. The most common forms of hyperthyroidism include diffuse toxic goiter (Graves disease), toxic multinodular goiter (Plummer disease), and toxic adenoma (see Etiology). Together with subacute thyroiditis, these conditions constitute 85-90% of all causes of thyrotoxicosis.
The most reliable screening measure of thyroid function in the healthy ambulatory adult population is the TSH level. The degree of thyrotoxicosis is determined by measurement of thyroid hormone levels. Autoantibody testing, and nuclear thyroid scintigraphy in some cases, can provide useful etiologic information. (See Workup.) Treatment of hyperthyroidism includes symptom relief, as well as therapy with antithyroid medications, radioactive iodine, or thyroidectomy. However, antithyroid medications are not effective in thyrotoxicosis from subacute thyroiditis, because these cases result from release of preformed thyroid hormone. (See Treatment.)
PathophysiologyNormally, the secretion of thyroid hormone is controlled by a complex feedback mechanism involving the interaction of stimulatory and inhibitory factors (see the image below). Thyrotropin-releasing hormone (TRH) from the hypothalamus stimulates the pituitary to release TSH.
Hypothalamic-pituitary-thyroid axis feedback. Schematic representation of negative feedback system that regulates thyroid hormone levels. TRH = thyrotropin-releasing hormone; TSH = thyroid-stimulating hormone. Binding of TSH to receptors on the thyroid gland leads to the release of thyroid hormonesprimarily T4 and to a lesser extent T3. In turn, elevated levels of these hormones act on the hypothalamus to decrease TRH secretion and thus the synthesis of TSH. Synthesis of thyroid hormone requires iodine. Dietary inorganic iodide is transported into the gland by an iodide transporter, converted to iodine, and bound to thyroglobulin by the enzyme thyroid peroxidase through a process called organification. This results in the formation of monoiodotyrosine (MIT) and diiodotyrosine (DIT), which are coupled to form T3 and T4; these are then stored with thyroglobulin in the thyroids follicular lumen. The thyroid contains a large supply of its preformed hormones. Thyroi