-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
1/60
DISEASES of THYROID and
PARATHYROID GLANDBy:
Shalimar C. Cortez, M.D. FPSGS, FPCSSurgical Oncology
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
2/60
OBJECTIVES-To review the anatomy of Thyroidand Parathyroid
gland.
- To review Thyroid and Parathyroid
gland physiology
- To discuss the different diseases andits pathophysiology
-To discuss the different treatmentoptions.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
3/60
Thyroid Gland
Arises as an outpouching of the primitive
foregut during 3rdweek of pregnancy.
Originates at the base of the tongue in the
foramen ceacum.
Descends in the neck anteriorly.
Follicles are apparent by 8 weeks and colloidformation begins at
11 weeks of pregnancy.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
4/60
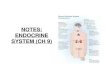
Thyroid Physiology
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
5/60
Iodine Metabolism
Average daily requirement is 0.1 mg.
Iodine is converted to iodide in the stomach
and jejunum.
Iodide is actively transported into follicular
cells.
Thyroid is major storage site for 90% of iodinein the body.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
6/60
Iodine transport
Na+/I-symport proteincontrols serum I-uptake
Based on Na+
/K+
antiport potential
Stimulated by TSH
Inhibited by Perchlorate
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
7/60
Thyroid hormone formation
Iodide trapping: transport of iodide intothyrocyte through Na/I
symport.
Oxidation of iodide and Iodination of
tyrosine residues on thyroglobulinforming MITs and DITs.
Coupling: DIT+DIT = T4 (thyroxine); MIT +
DIT = T3 (triiodothyronine). Hydrolysis to release T3 and T4
hormone.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
8/60
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
9/60
Thyroid Hormone
T4 is produced and released entirely by
the thyroid gland.
Thyroid gland produced 20% of T3 (morepotent).
Thyroid hormones are bounded by
thyroxine-binding globulin, thyroxinebinding pre albumin, and
albumin.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
10/60
Thyroid Hormone Control
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
11/60
Thyroid Hormone Function
Affects almost every system in the body. Important for fetal
brain development and
skeletal maturation.
Increases oxygen consumption, basalmetabolic rate and heat
production.
Positive inotropic and chronotropic effect on
the heart. Increase gastrointestinal motility; bone and
protein turnover; speed of muscle contraction
and relaxation.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
12/60
Thyroid Function Evaluation
TRH TSH
Total T3, T4
Free T3, T4
Thyroglobulin
Antibodies: Anti-Tg; anti-TPO;TSI(thyroid stimulating Ig)
Thyroid Imaging (Radionuclide Imaging;
Ultrasound; CT/MRI)
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
13/60
Thyroid Evaluation
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
14/60
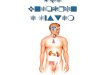
Iodine states
Normal Thyroid
Inactive Thyroid
Hyperactive Thyroid
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
15/60
Common Thyroid Disorders
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
16/60
GOITER (guttur)
Recognized since 2700 B.C.
In 1619, recognized that goiter arose from the
thyroid gland.
As ductless gland with functions ranging fromlubrication of the
larynx; reservoir for blood;
beautifying womens neck.
In 1170, first account of thyroid surgery (RogerFrugardi)
In 1909, physiology, pathology, and surgery of
the thyroid gland were recognized.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
17/60
Goiter Goiter: Chronic enlargement of the thyroid gland not
due to neoplasm Endemic goiter
Areas where > 5% of children 6-12 years of age havegoiter
Common in China and central Africa Sporadic goiter
Areas where < 5% of children 6-12 years of age havegoiter
Multinodulargoiterin sporatic areas often denotesthe presence of
multiple nodules rather than grossgland enlargement
Familial
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
18/60
Goiter Etiology
Hashimotos thyroiditis
Early stages only, late stages show atrophicchanges
May present with hypo, hyper, or euthyroid states
Graves disease Due to chronic stimulation of TSH receptor
Diet Brassica (cabbage, turnips, cauliflower, broccoli)
Cassava
Chronic Iodine excess Iodine excess leads to increased colloid
formation and can
prevent hormone release If a patient does not develop iodine
leak, excess iodine can
lead to goiter
Medications Lithium prevents release of hormone, causes goiter
in 6% of
chronic users Neo lasm
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
19/60
Goiter Pathogenesis
Iodine deficient areas Heterogeneous response to TSH
Chronic stimulation leads to multiple nodules
Iodine replete areas Thyroid follicles are heterogeneous in
their growth and activity
potential
Autopsy series show MNG >30%.
Thyroid function evaluation TSH, T4, T3
Overt hyperthyroidism (TSH low, T3/T4 high)
Subclinical hyperthyroidism (TSH low, T3/T4 normal)
Determination of thyroid state is key in determining
treatment
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
20/60
Non-Toxic Goiter Cancer screening in non-toxic MNG
Longstanding MNG has a risk of malignancy identical tosolitary
nodules ( 4cm should be
excised No FNA needed due to poor sensitivity Incidence of
cancer (up to 40%)
FNA in MNG Sensitivity 85% - 95% Specificity 95% Negative FNA
can be followed with annual US Insufficient FNAs should be repeated
Inconclusive FNA or papillary cytology warrants
excision Hyperfunctioning nodules may mimic follicular
neoplasm
on FNA
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
21/60
Non-Toxic GoiterTreatment options (no compressive symptoms)
US follow-up to monitor for progression
Thyroid suppression therapy
May be used for progressive growth May reduce gland volume up to
50%
Goiter regrowth occurs rapidly following therapycessation
Surgery Suspicious neck lymphadenopathy
History of radiation to the cervical region
Rapid enlargement of nodules
Papillary histology
Microfollicular histology (?)
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
22/60
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
23/60
Toxic Goiter Evaluate for
Graves disease
Clinical findings (Pretibial myxedema, Opthalmopathy)
Anti-TSH receptor Ab
High RAUI
Thyroiditis
Clinical findings (painful thyroid in Subacute thyroiditis) Low
RAUI
Recent Iodine administration
Amiodarone
IV contrast
Change in diet
FNA evaluation Not indicated in hyperthyroid nodules due to low
incidence of
malignancy
FNA of hyperthyroid nodules can mimic follicular neoplasms
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
24/60
Toxic Goiter
Risks of hyperthyroidism
Atrial fibrillation
Congestive Heart Failure
Loss of bone mineral density
Risks exist for both clinical or subclinical disease
Toxic Goiter
Toxicity is usually longstanding
Acute toxicity may occur in hyperthyroid states (JodBasedow
effect) with
Relocation to iodine replete area
Contrast administration
Amiodarone (37% iodine)
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
25/60
Toxic Goiter Treatment for Toxic MNG
Thionamide medications Not indicated for long-term use due to
complications
May be used for symptomatic individuals until
definitivetreatment.
Radioiodine
Primary treatment for toxic MNG Small goiters
Absence of pressure symptoms
Disorders which preclude surgery
Refusal of an operation Surgery
Used for compressive symptoms
Hypothyroidism occurs in up to 70% of subtotalthyroidectomy
patients
Pre-surgical stabilization with thionamide medications
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
26/60
Graves Disease Most common cause of thyrotoxicosis in the
industrialized
world. Autoimmune condition with thyroid stimulating
antibodies
with female preponderance; peak at ages 40 and 60.
-Postpartum state, iodine excess, lithium therapy, infections
as
possible triggers. Diagnosis
TSH, T4, T3to establish thyrotoxicosis; diffuse goiter;
extrathyroidalconditions( ophthalmopathy;dermopathy..)
RAIU in Hyperthyroid StatesHigh Uptake Low Uptake
Graves Subacute Thyroiditis
Toxic MNG Iodine Toxicosis
Toxic Adenoma Thyrotoxicosis factitia
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
27/60
Graves Disease
Treatment Beta blockers for symptoms Thionamide medications
May re-establish euthyroidism in 6-8 weeks
40% - 60% incidence of disease remission
20% incidence of allergy (rash, itching) 0.5% incidence of
potentially fatal agranulocytosis
Radioiodine ablation 10% incidence of hypothyroidism at 1
year
55% - 75% incidence of hypothyroidism at 10 years
Avoid RAI in children and pregnancy. Surgery
Large goiters not amenable to RAI
Compressive symptoms
Children, pregnancy
Relapse after drug therapy Intractable side effects/ failure of
compliance
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
28/60
Toxic Adenoma
Thyrotoxicosis Hyperfunctioning nodules 3 cm.
Treatment Indications Post-menopausal female
Due to increased risk of bone loss
Patients over 60 Due to high risk of atrial fibrillation
Adenomas greater than 3 cm (?)
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
29/60
Toxic Adenoma Treatments
Antithyroid medications Not used due to complications of
long-term treatment
Radioiodine Cure rate > 80% (20 mCi I131)
Hypothyroidism risk 5% - 10%
Second dose of I131 needed in 10% - 20%
Patients who are symptomatically toxic may require control
withthionamide medications before RAI to reduce risk of
worseningtoxicity.
Surgery
Preferred for children and adolescents Preferred for very large
nodules when high I131 doses needed
Low risk of hypothyroidism
Ethanol Injection Rarely done in the US
May achieve cure in 80%
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
30/60
Hypothyroidism
Symptomsfatigability, coldness, weight gain,constipation, low
voice
SignsCool skin, dry skin, swelling of face/hands/legs,
slow reflexes, myxedema NewbornRetardation, short stature,
swelling of
face/hands, possible deafness Types of Hypothyroidism
PrimaryThyroid gland failureSecondaryPituitary
failureTertiaryHypothalamic failurePeripheral resistance
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
31/60
Hypothyroidism
Cause is determined by geography Hashimotos in industrialized
countries
May be due to iodine excess in some costal areas
Diagnosis Low FT4, High TSH (Primary, check for antibodies)
Low FT4, Low TSH (Secondary or Tertiary, TRH
stimulation test, MRI)
Treatment Levothyroxine (T4) due to longer half life
Treatment prevents bone loss, cardiomyopathy,myxedema
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
32/60
Hypothyroidism
Agenesis
Thyroid destruction Hashimotos thyroiditis
Surgery
I131ablation
Infiltrative diseases
Post-laryngectomy
Inhibition of function Iodine deficiency
Iodine administration
Anti-thyroid medications (PTU, Methimazole, Lithium,
Interferon)
Inherited defects
Transient Postpartum
Thyroiditis
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
33/60
Thyroiditis
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
34/60
Hashimotos Thyroiditis Most common cause of goiter and
hypothyroidism in the U.S.
Physical Painless diffuse goiter
Lab studies
Hypothyroidism
Anti TPO antibodies (90%)
Anti Thyroglobulin antibodies (20-50%)
Acute Hyperthyroidism (5%)
Treatment
Levothyroxine if hypothyroid
Triiodothyronine (for myxedema coma)
Thyroid suppression (levothyroxine) to decrease goitersize
Stop therapy if no resolution noted
Surgery for compression or pain.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
35/60
Silent ThyroiditisPost-partum Thyroiditis
Silent thyroiditis is termed post-partum thyroiditis if it
occurs withinone year of delivery.
Clinical
Hyperthyroid symptoms at presentation
Progression to euthyroidism followed by hypothyroidism for upto
1 year.
Hypothyroidism generally resolves
Diagnosis
May be confused with post-partum Gravesrelapse
Treatment
Beta blockers during toxic phase No anti-thyroid medication
indicated
Iopanoic acid (Telopaque) for severe hyperthyroidism
Thyroid hormone during hypothyroid phase. Must withdraw in6
months to check for resolution.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
36/60
Subacute ThyroiditisDeQuervains, Granulomatous
Most common cause ofpainful thyroiditis
Often follows a URI
FNA may revealmultinuleated giant cells orgranulomatous
change.
Course
Pain and thyrotoxicosis(3-6 weeks)
Asymptomatic
euthyroidism Hypothyroid period
(weeks to months)
Recovery (complete in95% after 4-6 months)
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
37/60
Subacute ThyroiditisDeQuervains, Granulomatous
Diagnosis Elevated ESR
Anemia (normochromic, normocytic)
Low TSH, Elevated T4 > T3, Low anti-TPO/Tgb
Low RAI uptake (same as silent thyroiditis)
Treatment NSAIDs and salicylates.
Oral steroids in severe cases
Beta blockers for symptoms of hyperthyroidism, Iopanoic acid
for
severe symptoms PTU not indicated since excess hormone results
from leak instead of
hyperfunction
Symptoms can recur requiring repeat treatment
Gravesdisease may occasionally develop as a late sequellae
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
38/60
Acute Thyroiditis
Causes 68% Bacterial (S. aureus, S. pyogenes)
15% Fungal
9% Mycobacterial
May occur secondary to Pyriform sinus fistulae
Pharyngeal space infections
Persistent Thyroglossal remnants Thyroid surgery wound
infections (rare)
More common in HIV
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
39/60
Acute Thyroiditis
Diagnosis Warm, tender, enlarged thyroid
FNA to drain abscess, obtain culture
RAIU normal (versus decreased in DeQuervains)
CT or US if infected
Treatment High mortality without prompt treatment
IV Antibiotics Nafcillin / Gentamycin or Rocephin for empiric
therapy
Search for pyriform fistulae (BA swallow, endoscopy)
Recovery is usually complete
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
40/60
Riedels Thyroiditis
Rare disease involving fibrosis of the thyroid gland
Diagnosis Thyroid antibodies are present in 2/3
Painless goiter woody
Open biopsy often needed to diagnose
Associated with focal sclerosis syndromes
(retroperitoneal,mediastinal, retroorbital, and sclerosing
cholangitis)
Treatment Resection for compressive symptoms
Chemotherapy with Tamoxifen, Methotrexate, or steroidsmay be
effective
Thyroid hormone only for symptoms of hypothyroidism
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
41/60
ThyroidCancer
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
42/60
Leading Cancer Sites in 2005, Philippines
1. Bronchus,lung 17,238 16.1%
2. Breast 14,043 13.1%
3. Colon/Rectum 8,585 8.0 %
4. Liver 7,629 7.1%
5. Cervix,uteri 7,277 6.8%
6. Prostate 4,254 4.0%
7. Leukemia 4,202 3.9%
8. Stomach 3,932 3.7%
9. Thyroid 3,521 3.3%
10. Ovary 3,283 3.1%
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
43/60
Leading Cancer Sites in 2005, Philippines
11. Oral Cavity 3,054 2.9 %
12.Nasopharynx 2,793 2.6 %
13.Non-Hodgkin lymphom 2,492 2.3 %
14.Pancreas 1,681 2.4 %15.Pancreas 1,873 1.8 %
16.Corpus uteri 1,777 1.7 %
17.Larynx 1,723 1.6 %
18.Kidney 1,518 1.4 %
19.Brain, nervous system 1,509 1.4 %
19.Bladder 1,360 1.3 %
20.Other pharynx 1,059 1.0 %
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
44/60
Incidence of thyroid cancer
9thmost common for both sexes combined(3.3%), 15thleading site
in men ( 1.5%) and6thamong females (5%)
In 2005, estimated 3,521 new cases, 755 inmales and 2,766 in
females.
There will be 1,012 deaths, 245 in males and767 in females.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
45/60
Most common cancer of women at ages 15-
24
Incidence among female residents in the
Philippines is among the highest observed
worldwide
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
46/60
Histologic Variants
PAPILLARYmost common form (60 -70%) withstrong association with
radiation to the head andneck.
FOLLICULARaccount for 25% of cases with
female preponderance. More aggressive thanpapillary with
tendency to spread viahematogenous route.
MEDULLARYneuroendocrine carcinoma (5-
10%). UNDIFFERENTIATED - accounts for 10 -15% of
cases with extensive local invasion.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
47/60
PARATHYROID GLAND
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
48/60
Anatomy
Precise location is variable but tends to be
symmetrical.
Size is 1mm x 3mm x 5 mm; weighs 30 mg.
Blood supply for both pairs is from inferior
thyroid gland.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
49/60
Cellular Structre
Chief cellsmanufacture and secrete
parathyroid hormone
Oxophil cellsfunction is poorly understood.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
50/60
Parathormone
- Stimulation of the activity of osteoclast in
bone.
- Enhancement of the absorption of calcium
from the gut into the bloodstream.
- Increase in the reabsorption of calcium by the
renal tubules.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
51/60
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
52/60
PARATHYROID CARCINOMA
Condition is very, with invasion of local tissues and
recurrenceafter excision.
Metastasis is uncommon
Death is caused hypercalcemia.
The criteria that should alert the clinician to the possibility
of
this diagnosis can be divided into preoperative,intraoperative,
and histopathologic findings.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
53/60
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
54/60
PARATHYROID CARCINOMA
Preoperative Findings
2. Markedly abnormal biochemistry
- the biochemical parameters used for thediagnosis of
hyperparathyroidism are highlyabnormal.
- Mean serum calcium levels usually aregreater than 13.0 mg/dL
(normal range is 8.9to 10.1 mg/dL), parathyroid hormone levelsare
elevated tenfold, and alkaline phosphatase
levels are elevated threefold.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
55/60
PARATHYROID CARCINOMA
Preoperative Findings
3. Complications of hyperparathyroidism
- Bone disease, renal insufficiency, andnephrolithiasis occurred
in 91 percent, 84percent, and 56 percent, respectively, ofpatients
with parathyroid carcinoma, which
are considerably higher than the rates foundin nonmalignant
hyperparathyroidism.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
56/60
PARATHYROID CARCINOMA
Intraoperative Findings
- parathyroid mass that is firmer than the usual
soft, friable, nonmalignant parathyroid gland.
- when a gland has been transformed from the
normal bean shape and kidney color to an irregular,pale white
and is adherent to any of the surrounding
structures, the diagnosis of malignancy is almostcertain.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
57/60
PARATHYROID CARCINOMA
Histopathologic Findings
- Most weigh more than 2000 mg
- The hallmark of malignancy histologically are the presenceof a
thick, fibrous capsule, fibrous septa interdigitatingthroughout the
tumor, and the enlargement, hyperchromasia,and variation of nuclear
size.
- Clear-cut invasion through the capsule to involve
adiposetissue, nerves, thyroid gland, or surrounding muscle usually
ispresent.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
58/60
PARATHYROID CARCINOMA
Treatment :
- treatment of choice is en bloc surgical resection of thetumor
and the involved surrounding structures.
- This treatment usually involves a total thyroid lobectomy
onthe affected side.
- Regional nodal metastases are uncommon, but lymph nodes
should be assessed and, if involved, surgically treated
byappropriate resection, which may include a modified radicalneck
dissection.
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
59/60
-
8/13/2019 Diseases of Thyroid and Parathyroid Gland
60/60
PARATHYROID CARCINOMA
Treatment :
- When recurrent disease is seemingly localized,
repeat surgical resection.- Nonsurgical treatment modalities are
inadequate.
-the 3-year and 5-year survival rates were 84 and 69
percent, respectively.
- the cause of death often was attributed to the
metabolic consequences of hypercalcemia and not to
the local effects of malignancy.