Embed Size (px)
Citation preview
DEMENTIA
A.R.ALEHASHEMI MD
ASSISTANT PROFESSOR OF NEUROLOGY
MSHDIAU
2016 dec

A radical claim…..
Learn to think…..
…….Think to learn
TITELS
CONSCIOUSSNESS
COGNITION
DEMENTIA
DEFINITION
CLASSFICATION
TREATABLE CAUSES
CONSCIOUSSNESS
Awareness of self & the environment
Consciousness
Two components of conscious behavior
– Arousal- appearance of wakefulness
– Content- the sum of cognitive and affective function
Level of consciousness
Requires NL function of either:
– Bilateral hemispheres
– Reticular activating system (RAS) in the brain stem
Content of Consciousness (COGNITION)
Cerebral cortex
– Emotions
– Memory
– Attention
– Reasoning
– Self-awareness
– Spatial relationships
– …
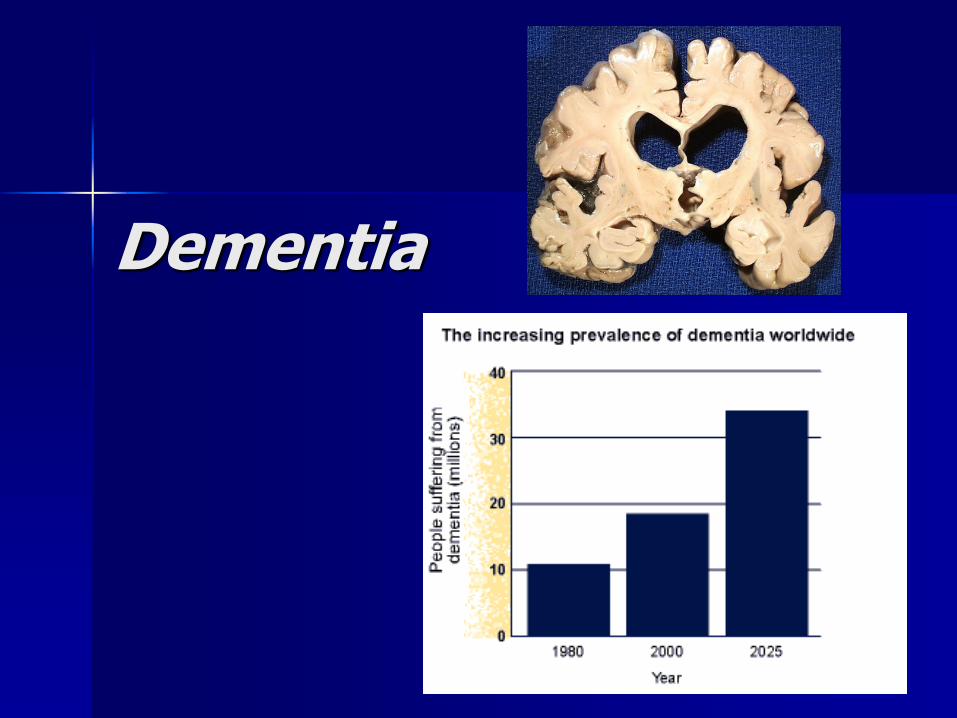
Dementia
DEMENTIA
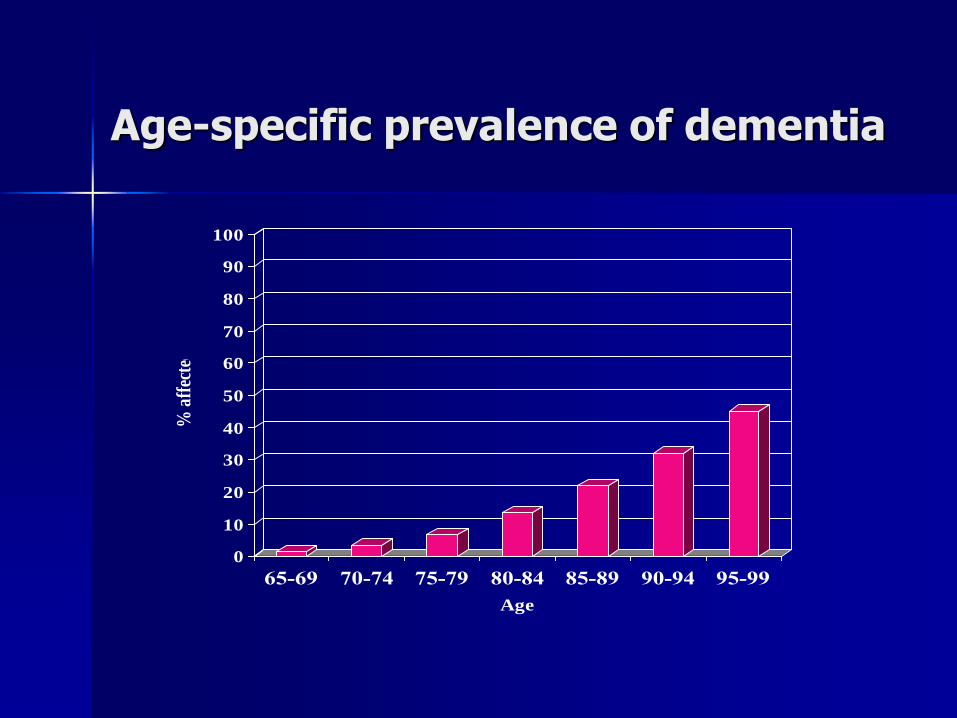
Age-specific prevalence of dementia
0
10
20
30
40
50
60
70
80
90
100
% a
ffec
ted
65-69 70-74 75-79 80-84 85-89 90-94 95-99
Age
Definition
Acquired generalized and often progressive impairment of cognitive function that affects the content, but not the level, of consciousness.
Two types of Dementia
Cortical Disorder affecting the cortex, the outer portion or layers of the brain.
Alzheimer’s and Creutzfeldt-Jakob are two forms of cortical dementia
Memory and language difficulties(Aphasia) most pronounced symptoms.
Two types of Dementia
Subcortical
Dysfunction in parts of the brain that are beneath the cortex.
Memory loss & language difficulties not present or less severe than cortical.
Huntington’s disease and AIDS dementia complex.
Changes in their personality and attention span.
Thinking slows down.
DSM-V Criteria for Dementia:
1. The gradual onset and continuing decline of cognitive function from a previously higher level, resulting in impairment in social or occupational function
DSM-V Criteria for Dementia:(cont.)
2. Impairment of recent memory (the inability to learn new information), and at least one of the following:
a) Language (word-finding difficulties) b) Disturbances of praxis (inability to execute skilled motor activities in the absence of weakness)
c) Disturbances of visual processing (visual agnosia and constructional disturbances)
d) Disturbances of executive function (including abstract reasoning and concentration)
DSM-V Criteria for Dementia:(cont.)
3. The cognitive deficits are not due to other psychiatric disease, neurologic diseases, or systemic diseases, and the deficits do not exclusively occur in the setting of delirium
Minimental status exam
ORIENTATION
REGISTRATION
ATTENTION & CALCULATION
RECALL
LANGUAGE
CONSTRUCTION
TOTAL 30
Mild Cognitive Impairment
MMSE 24-28 Problem with recollection Does not meet dementia criteria
Mild cognitive impairment (MCI)
MCI is a relatively recent term, used to describe people who have some problems with their memory but do not actually have dementia.
Some people (80%?) will be in the early stages of Alzheimer’s disease or another dementia. Others, however, will have MCI as a result of stress, anxiety, depression, physical illness or just an ‘off day’.
It is estimated that 15% of the population may be experiencing MCI.
Currently extensive research on MCI is ongoing.
At the moment there is not enough evidence to recommend any specific treatments.
Differential Diagnosis:
1. Alzheimer Disease (pure ~40%, + mixed~70%)
2. Vascular Disease, MID (5-20%)
3. Drugs , Depression
4. Ethanol
5. Medical / Metabolic Systems
6. Endocrine (thyroid, diabetes)
7. Neurologic , Nutritional (other primary degenerations, etc.)
8. Tumor, Toxin, Trauma
9. Infection
10. Amnesia, Autoimmune
TREATABLE OR REVERSIBLE CAUSES
~ 15% -20 of causes
NPH
IC mass lesion (Tumor, SDH)
B12 def.
Hypothyroidism
Syphilis
Depression(PSEDUDEMENTIA)
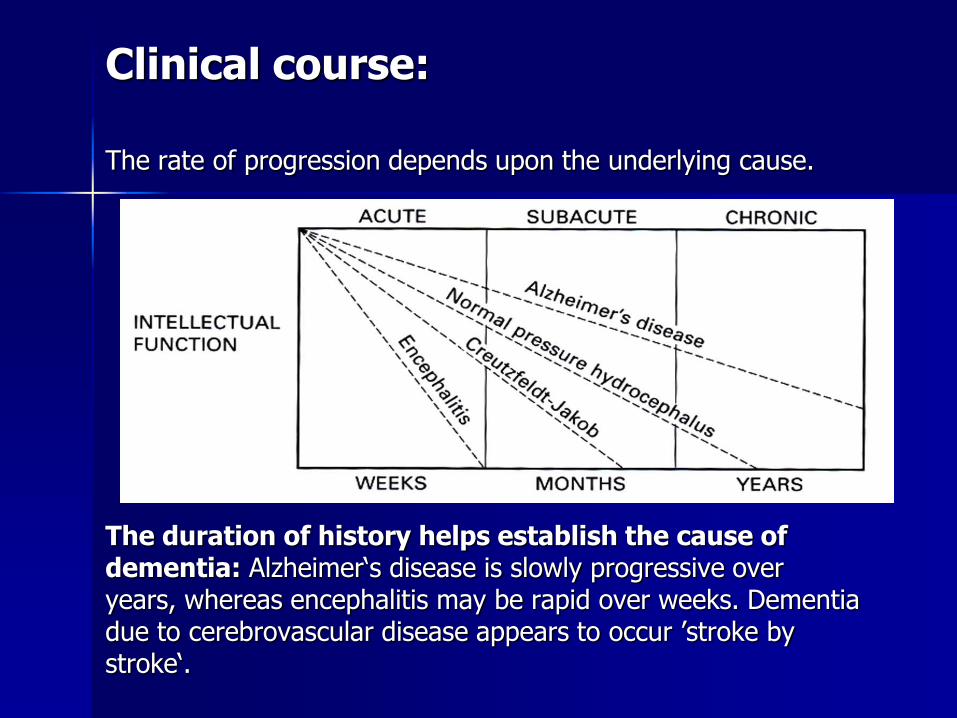
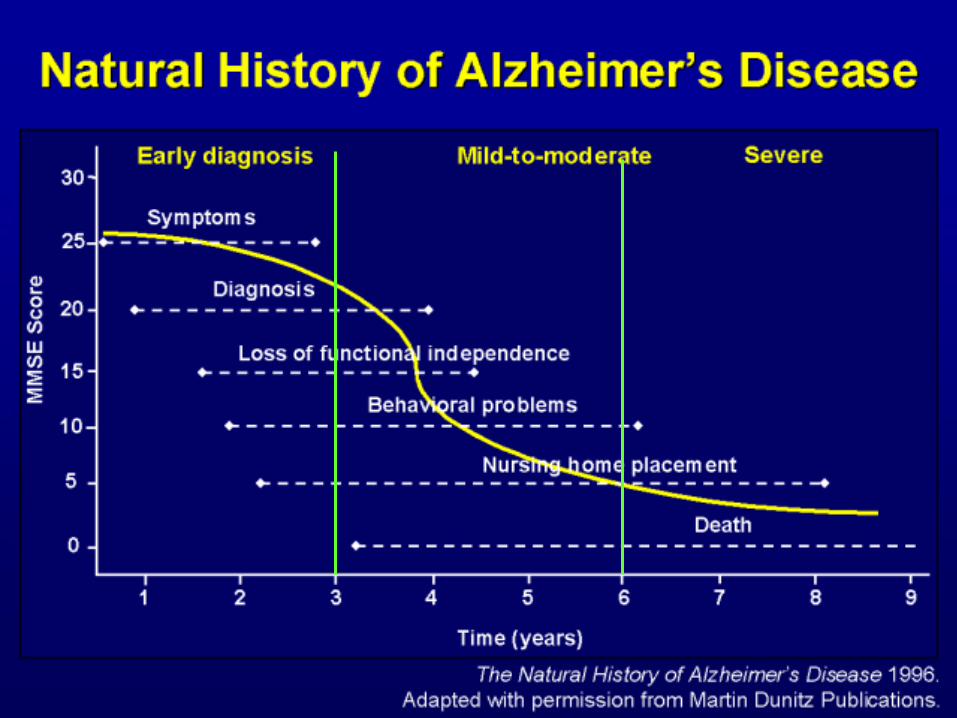
Clinical course:
The rate of progression depends upon the underlying cause.
The duration of history helps establish the cause of dementia: Alzheimer‘s disease is slowly progressive over years, whereas encephalitis may be rapid over weeks. Dementia due to cerebrovascular disease appears to occur ’stroke by stroke‘.
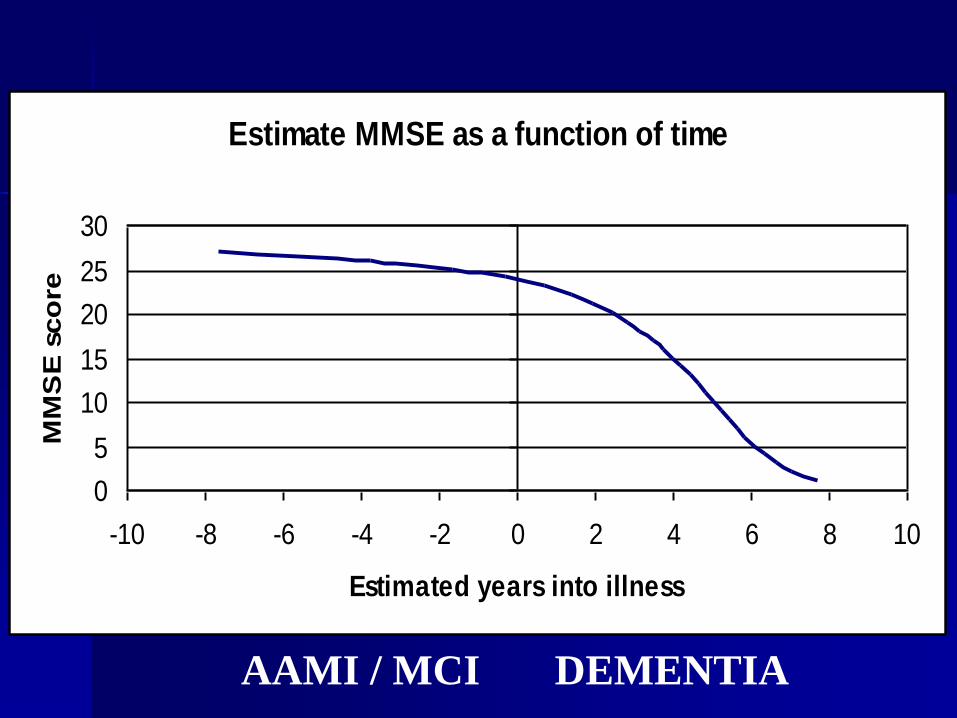
Estimate MMSE as a function of time
0
5
10
15
20
25
30
-10 -8 -6 -4 -2 0 2 4 6 8 10
Estimated years into illness
MM
SE
sco
re
AAMI / MCI DEMENTIA
Alzheimer’s Disease (AD)
Alzheimer’s Disease (AD)
Alzheimer’s Disease (AD)
Epidemiology
– Most common degenerative disease of the brain
– 10% of people over age 65 years have AD
– 20% of persons > 80 years
– 30% of > 90 years old
– Male = Female
Histopathology:
Macroscopic: – Atrophy, mostly temporoparietal and frontal
Microscopic – Loss of neurones and synapses – Neurofibrillary tangles (NFTs) – amyloid plaques ( Neurotic plaques) – Granulovsacular degeneration
Chemistry – loss of neurotransmitters, especially
acetylcholine (ACh)
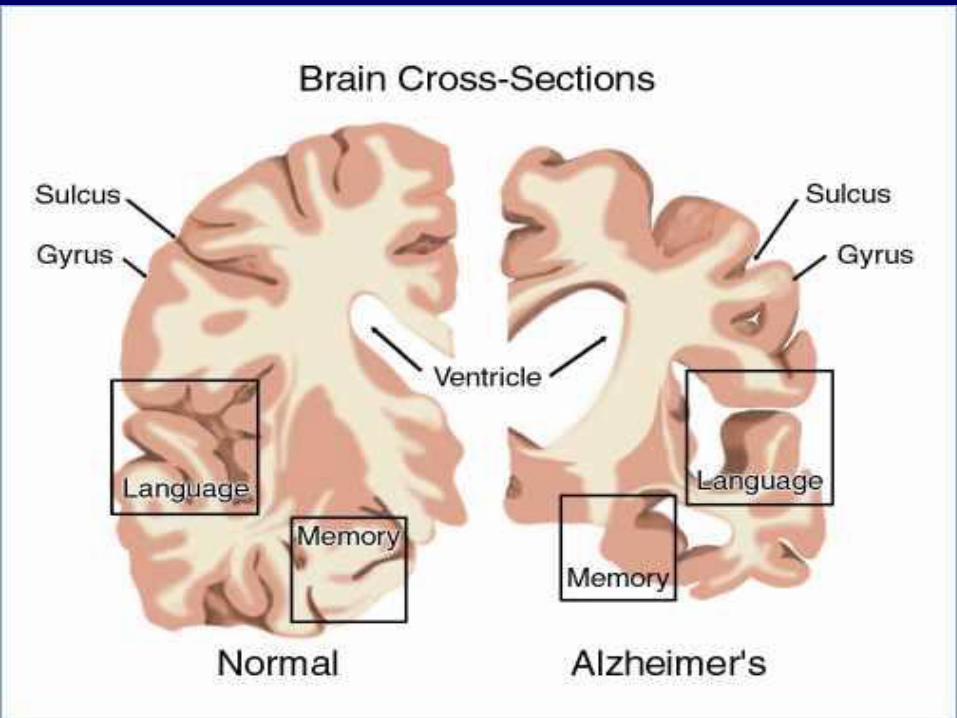
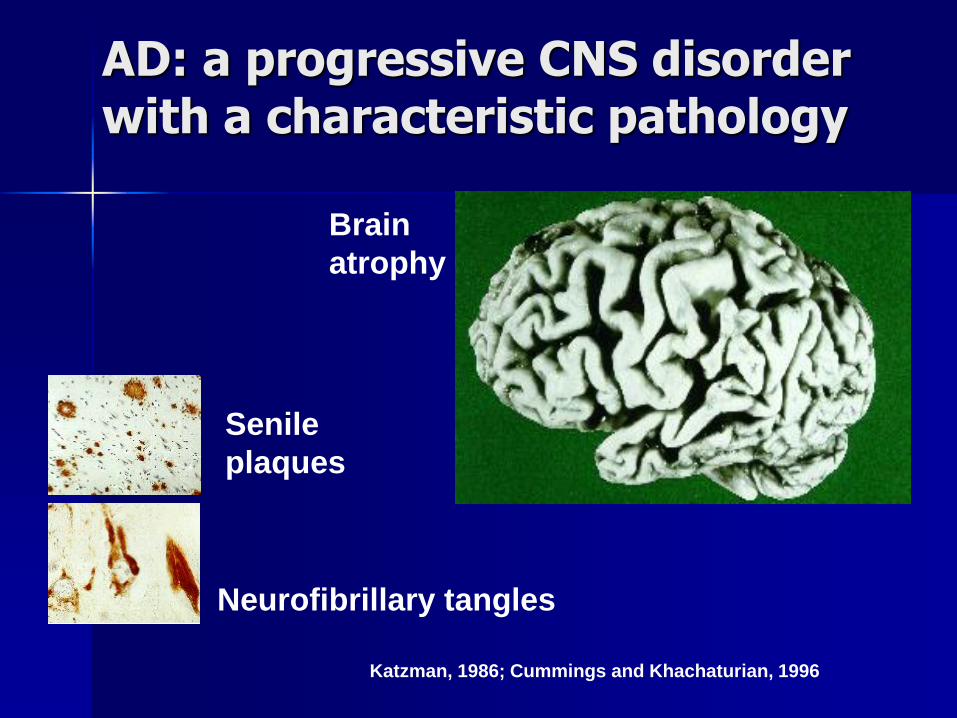
AD: a progressive CNS disorder with a characteristic pathology
Brain
atrophy
Senile
plaques
Neurofibrillary tangles
Katzman, 1986; Cummings and Khachaturian, 1996

Risk factors for AD:
Down’s
syndrome
Strong risk factors for AD*
Age
Down’s syndrome
Family history
Certain genes associated with increased risk but do not cause AD e.g. ApoE4
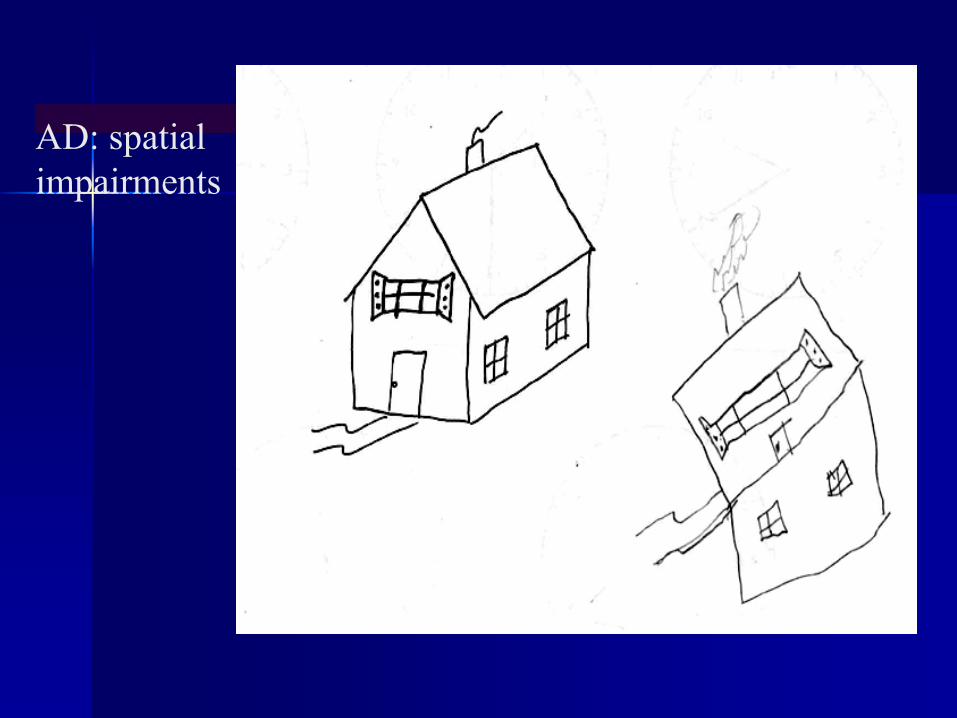
AD: spatial
impairments
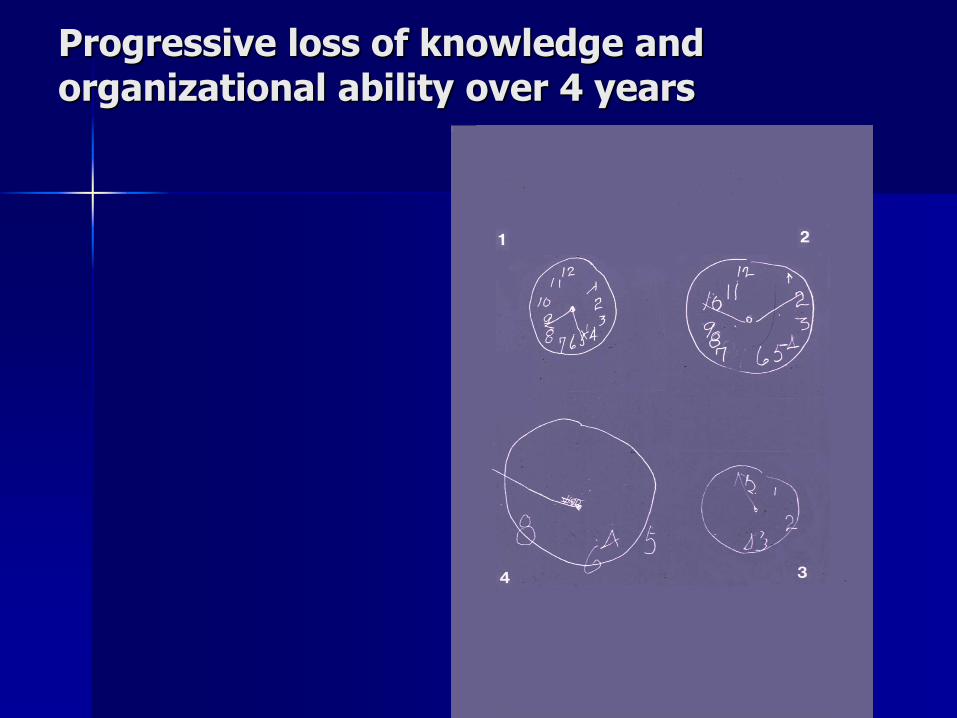
Progressive loss of knowledge and organizational ability over 4 years
Dementia with Lewy bodies
Up to 20% of dementias
Lewy bodies diffusely through cortex
Markedly fluctuating cognitive impairment
Visual and/or auditory hallucinations
Paranoid delusions
Falls
Extrapyramidal features: rigidity & bradykinesia
Neuroleptic sensitivity: extrapyramidal S/Es
Dementia with Lewy bodies

Vascular dementia
Vascular dementia
Also called multi-infarct dementia (MID)
About 15-20%
Decline can be linear or step-wise
Vascular dementia
Step-wise decline - uneven steps, varying plateau
Earlier onset than AD and M > F
Sudden onset, stepwise deterioration
Hx of high BP, strokes
Evidence associated arteriosclerosis, eg coronary artery disease
Focal neurological symptoms and signs
Focal pathology on brain imaging
VAD -vs.- AD
Fronto-temporal dementia Pick’s disease
Creutzfeldt-Jakob disease
Creutzfeldt-Jakob disease
Transmissible: cornea transplants, intracerebral recording electrode implants, growth hormone
Rapidly progressive dementia
Etiologic agent: proteinaceous infectious particle (prion)
Creutzfeldt-Jakob disease (cont.)
Dementia
Psychiatric symptoms
Myoclonus
Extrapyramidal signs
Cranial nerve palsies
New Variant: bovine spongiform encephalopathy – Earlier onset (mean age, about 30 years)
– More prolonged course (median duration over 1 year)
– Prominent early psychiatric abnormalities, including depression and personality changes.
NORMAL-PRESSURE HYDROCEPHALUS
NPH
NORMAL-PRESSURE HYDROCEPHALUS
Sometimes called communicating (lateral, 3rd, 4th ventricles remain in communication) or nonobstructive hydrocephalus
Triad
– Dementia
– Gait apraxia
– Incontinence
Idiopathic or secondary (meningitis, SAH)
Memory defects, but rarely aphasia and agnosia
NORMAL-PRESSURE HYDROCEPHALUS (cont.)
Weeks-months Gait apraxia early, with weight bearing Pyramidal signs Urinary incontinence
Lp: normal or low opening pressure – Remove 30-50 cc; prognostication
CT scan or MRI: enlarged lateral ventricles without increased prominence of cortical sulci
Cisternography: delayed clearance
Rx: CSF shunting; VA,VP,LP
قدری اندیشه گاه میتواند ره آوردی بس بزرگ به
ارمغان بیاورد ،
شاید بسیار بیشتر از عمری تلاش
شاد باشید و سرفراز