Embed Size (px)
Citation preview

Distinct barrier integrity phenotypes in filaggrin-related atopiceczema following sequential tape stripping and lipid profiling
Irena Angelova-Fischer1, Anna-Clara Mannheimer1, Anke Hinder2, Andreas Ruether3, Andre Franke3,Reinhard H. H. Neubert2, Tobias W. Fischer1 and Detlef Zillikens1
1Department of Dermatology, University of Lubeck, Germany; 2Institute of Pharmaceutics and Biopharmaceutics, Martin Luther University, Halle-
Wittenberg, Germany; 3Institute for Clinical Molecular Biology, Christian-Albrechts University, Kiel, Germany
Correspondence: Irena Angelova-Fischer, MD, PhD, Department of Dermatology, University of Lubeck, Ratzeburger Allee 160, 23538 Lubeck,
Germany, Tel.: +49 451 500 5729, Fax: +49 451 500 2981, e-mail: [email protected]
Abstract
Background Filaggrin gene (FLG) loss-of-function mutations have
been shown to represent the strongest so far known genetic risk
factor for atopic dermatitis (AD). Whereas the barrier
characteristics in FLG mutation carriers under baseline conditions
have been investigated, there are only limited data on the
permeability barrier function in filaggrin-AD under compromised
conditions.
Aim We investigated: (i) stratum corneum (SC)
integrity ⁄ cohesion; (ii) barrier recovery after controlled
mechanical and irritant-induced barrier abrogation; and (iii) the
lipid composition of the non-lesional and lesional skin of AD
patients harbouring the European R501X, 2282del4, 3702delG,
R2447X or S3247X FLG variants.
Methods Thirty-seven AD patients (14 FLG mutation carriers and
23 non-carriers) and 20 healthy controls participated in the study.
Stratum corneum integrity ⁄ cohesion was assessed by measurement
of transepidermal water loss (TEWL) and amount of removed
protein following sequential tape stripping. Barrier recovery was
monitored by repeated measurements of TEWL and erythema up
to 96 h after barrier abrogation. Samples for lipid analysis were
obtained from non-lesional and lesional skin using the
cyanoacrylate method.
Results Tape stripping revealed distinct genotype-related
impairment of the SC integrity ⁄ cohesion. No differences in the
rate of barrier recovery among the groups were found. The SC
lipid analysis revealed significant differences regarding the
percentage amount of cholesterol, ceramide ⁄ cholesterol ratio and
triglycerides in the uninvolved skin as well as the amounts of free
fatty acids, CER[EOH] and triglycerides in the skin lesions of the
AD FLG mutation carriers.
Conclusions Our results provide evidence for discernible FLG-
related barrier integrity phenotypes in atopic eczema.
Key words: atopic dermatitis – barrier recovery – filaggrin – skin barrier
function – skin lipids
Accepted for publication 11 January 2011
IntroductionPermeability barrier formation results from a tightly regulated
process of terminal differentiation in which keratinocytes undergo
sequential biochemical and structural transformations to form a
layer of cornified cells in a lipid-enriched extracellular matrix as
an elaborate first line of defense to the environment (1,2). The
balance between epidermal proliferation and differentiation in
healthy skin is maintained through complex transcriptional con-
trol; consequently, variations in the genes encoding structural
components of the skin barrier may result in aberrant morphology
and compromised barrier function (3–5). Importantly, the genetic
imprint might be relevant not only for rare congenital disorders
but also play a major role for the manifestation of common dis-
ease phenotypes such as atopic dermatitis (AD).
In 2006, prevalent and rare loss-of-function mutations in the
gene encoding the epidermal differentiation protein filaggrin
(FLG) were identified as the cause of the genodermatosis ichthyo-
sis vulgaris and were additionally reported to be an important
pre-disposing factor for the development of AD (6–8). The associ-
ation has been consistently replicated in multiple case-control and
cross-sectional studies (9,10) as well as across different ancestral
groups (11–13) and to date, the FLG mutations are considered the
strongest genetic risk factor for AD known so far. In view of the
critical role of filaggrin in terminal differentiation and barrier for-
mation as well as the strong line of evidence for compromised
barrier function in AD, there is a need for in-depth analysis of the
contribution of the FLG loss-of-function alleles to the different
aspects of the skin barrier abnormality in atopic eczema.
Whereas previous publications (14–18) focused primarily on
the characterization of the epidermal barrier properties under
baseline conditions, data on the permeability barrier function in
FLG mutation carriers under compromised conditions or upon
external stressors such as mechanically induced barrier damage
have not been reported so far. Furthermore, the stratum corneum
(SC) integrity ⁄ cohesion along with the barrier recovery rate after
experimentally induced barrier abrogation or the lipid composi-
tion of the lesional skin in AD patients harbouring at least one
FLG mutation have not been studied. We aimed to address these
issues and extend the existing body of knowledge by investigating
the above mentioned barrier function parameters in AD patients
carrying at least one of the prevalent European R501X, 2282del4,
3702delG, R2447X or S3247X FLG loss-of-function alleles.
DOI:10.1111/j.1600-0625.2011.01259.x
www.blackwellpublishing.com/EXDOriginal Article
ª 2011 John Wiley & Sons A/S, Experimental Dermatology, 20, 351–356 351

Materials and methodsStudy populationSixty-five AD patients meeting the UK Working Party Criteria
(19) (43 female, 22 male; mean age 29.7 years) and 20 healthy,
non-atopic controls (16 female and 4 male; mean age 34.8 years)
of German origin volunteered for the study. The protocol was
approved by the Ethics Committee of the University of Lubeck
(Nr. 07-207) and all participants gave written informed con-
sent ⁄ assent beforehand. All patients were recruited in acute stage
of disease when medical history and disease severity (SCORAD)
(20) were recorded and additionally, blood samples for total IgE
measurement and genotyping as well as samples for skin lipids
analysis were collected. The patients were asked to contact the
study centre again for assessment of the epidermal barrier func-
tion when free of inflammatory lesions and at least 4 weeks after
discontinuation of any topical or systemic medication or photo-
therapy, except for emollients. Thirty-seven AD patients (27
female and 10 male, mean age 30.8 years) volunteered for assess-
ment of the epidermal barrier function and were thus included in
the final data evaluation.
FLG mutation analysisFor analysis of R501X, 2282del4, 3702delG, R2447X and S3247X
FLG mutations, genomic DNA was extracted from 9 ml EDTA fresh
whole blood samples from patients and controls using an Invisorb�
Blood Universal Kit (Invitek, Berlin, Germany). Genotyping of the
FLG variants was performed using a TaqMan�-based allelic dis-
crimination assay (Applied Biosystems, Foster City, CA, USA). The
primers and PCR settings were as previously described (21).
Dependent on the genotype the AD patients were divided into
subgroups with filaggrin-AD (patients homozygous, heterozygous
or compound heterozygous for R501X, 2282del4, 3702delG,
R2447X or S3247X FLG alleles) and non-filaggrin AD (wild-type).
Assessment of the epidermal barrier function and SC integ-rity ⁄ cohesionFourteen patients with filaggrin-AD (12 female and 2 male, mean
age 35.1 years), 23 patients with non-filaggrin AD (15 female and
8 male; mean age 26.6 years) and 20 healthy controls (as
described) participated in this part of the study. Based on the
genotype, the patients with filaggrin-AD were characterized as
follows: two homozygous carriers of R501X, three homozygous
and five heterozygous carriers of 2282del4, three heterozygous car-
riers of R2447X and one compound heterozygous carrier of R501X
and 2282del4 alleles.
The baseline evaluation of the skin barrier function was per-
formed on the volar surface of the forearm ⁄ arm in the stage of
clinical remission as previously defined. Erythema was measured
using Chromameter CR200 (Minolta, Osaka, Japan) and expressed
in the L*a*b* system. Transepidermal water loss (TEWL) was
measured with the open chamber system (Tewameter TM300) and
skin hydration was assessed by measuring capacitance (Corneome-
ter CM825), both devices from Courage and Khazaka Electronics
(Cologne, Germany). For each parameter, three consecutive mea-
surements per field were performed by the same observer under
controlled environmental conditions (room temperature 20 ± 2�C;
average relative humidity 40–45%) and according to the published
guidelines (22–24).
Stratum corneum integrity was assessed by sequential tape
stripping of a previously marked field on the volar forearm, using
commercially available adhesive tapes (22-mm D-Squame� discs,
CuDerm Corp., Dallas, TX, USA). Thirty consecutive strips per
field ⁄ volunteer were taken following previously standardized pro-
cedure. Barrier integrity was assessed by repeated monitoring of
TEWL at baseline and after 2, 10, 20 and 30 strips as described.
Stratum corneum cohesion was assessed by the amount of
removed protein per tape, measured by infrared densitometry
using a light source with a peak wavelength of 850 nm (Squame-
Scan� 850A, Heiland electronic, Wetzlar, Germany) (25). Visual
scoring of the tape-stripped field and measurement of skin col-
our ⁄ erythema were performed at baseline and after 30 strips as
described. All measurements were performed in duplicate.
Epidermal barrier recoveryTwenty-five AD patients (11 FLG mutation carriers, 14 non-carri-
ers) and 18 healthy controls volunteered for monitoring of the
epidermal barrier recovery after tape stripping and irritant appli-
cation.
Tape stripping was performed on the volar forearm as
described above. TEWL and erythema measured after 30 tapes
were taken as baseline for assessment of the barrier recovery rate
every 24 h up to 96 h.
To assess the recovery after irritant-induced damage, 50 ll 1%
sodium lauryl sulfate solution (SLS; 99% purity, Sigma-Aldrich,
Steinheim, Germany) were applied to the volar forearm using a
large Finn chamber (12 mm, Epitest, Hyrla, Finland). The chamber
was removed after 24 h and the visual score (according to Frosch
and Kligman) (26), chromametry a*-value and TEWL measured
three hours later were taken as baseline for monitoring of the bar-
rier recovery, assessed by repeated measurements of TEWL, ery-
thema and the irritation score up to 72 h post-irritation.
Stratum corneum lipid analysisThe samples for SC lipid analysis were obtained in duplicate from
the non-lesional and lesional skin of the AD patients as well as
from the control group 48 h after the discontinuation of emollient
use, according to a previously established method (16,27). Briefly,
40 ll cyanoacrylate glue were placed on the skin with the help of
a glass slide. After 2 min, the slide was carefully removed and fro-
zen at )80�C until extraction.
The SC lipids were extracted with n-hexane-ethanol 95:5 (v ⁄ v)
under ultrasonication, filtered and dried under nitrogen. The resi-
due was re-dissolved in chloroform ⁄ methanol 1:1 (v ⁄ v) and stored
at )20�C until further analysis.
The separation of the lipid and ceramide fractions was per-
formed by automated multiple development high performance
thin layer chromatography (AMD-HPTLC) according to Farwa-
nah; the protocol has been previously published in detail (28,29).
Statistical analysisStatistical analysis was performed using GraphPrism Version 4
(GraphPad Software Inc, San Diego, CA, USA). The level of sig-
nificance was set at 0.05. Non-parametric (Mann–Whitney) tests
and analysis of variance (ANOVA) were used for comparison
between the patients and controls, respectively the subgroups with
filaggrin-AD, non-filaggrin AD and controls. For P-values less
than 0.05 for ANOVA, a post hoc (Tukey) test was performed. The
barrier recovery parameters (TEWL, chromametry a*-value) were
evaluated by repeated measures ANOVA. Values are presented as
mean and standard error of the mean (SEM) unless otherwise
indicated.
Angelova-Fischer et al.
352 ª 2011 John Wiley & Sons A/S, Experimental Dermatology, 20, 351–356

ResultsTEWL under baseline conditions does not distinguishFLG-dependent alterations in the skin barrier functionThe AD patients carrying at least one FLG mutation had increased
baseline TEWL (9.01 ± 0.69 g ⁄ m2 ⁄ h) compared with non-filaggrin
AD (7.69 ± 0.57 g ⁄ m2 ⁄ h) and the healthy controls
(5.09 ± 0.31 g ⁄ m2 ⁄ h), the difference between filaggrin-AD and the
healthy control group being significant (P < 0.001). No significant
differences in the baseline TEWL values between filaggrin-AD and
non-filaggrin AD were observed.
The baseline capacitance values measured on uninvolved skin
were 27.75 ± 2.21, 30.52 ± 1.49 and 35.25 ± 1.32 AU respectively
for filaggrin-AD, non-filaggrin AD and the healthy controls. The
patients with filaggrin-AD had significantly reduced SC hydration
compared with the control group (P < 0.05), whereas no signifi-
cant differences between filaggrin-AD and non-filaggrin AD or
non-filaggrin AD and controls were registered.
There were no significant differences in the baseline chromame-
try a*-values measured on the non-lesional skin of the patients
with filaggrin-AD, non-filaggrin AD and controls (6.07 ± 0.53,
respectively 6.09 ± 0.38 and 5.72 ± 0.35 AU).
Impaired SC integrity in filaggrin-AD upon controlledapplication of exogenous stressorsThe SC integrity was quantified by repeated TEWL measurements
following sequential tape stripping as described. For each group,
after the application of 2 tapes there was a tendency for increase
in TEWL and after 20 respectively, 30 tapes, TEWL was signifi-
cantly increased compared with baseline.
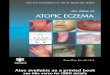
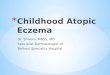
The increase in TEWL after 2, 10, 20 and 30 tapes was greater
in filaggrin-AD compared with non-filaggrin AD and the healthy
controls (Fig. 1a). After 20 strips, the increase in TEWL, assessed
by DTEWL (DTEWL = TEWL after tape stripping ) baseline
TEWL), was significantly higher in the FLG mutation carriers
group (19.02 g ⁄ m2 ⁄ h; P < 0.05) in comparison with both the
wild-type (9.89 g ⁄ m2 ⁄ h) and the healthy control group
(9.5 g ⁄ m2 ⁄ h).
The amount of removed protein measured by infrared densi-
tometry was used to assess SC cohesion. For each group, a ten-
dency for decrease in the removed protein per tape with
increasing number of tapes was observed (Fig. 1b) and the protein
amount upon the respective number of tape was lower in filag-
grin-AD compared with non-filaggrin AD or the healthy controls.
Barrier recovery after tape stripping and irritant damage isnot dependent on the FLG genotypeThe epidermal barrier recovery rate was assessed by repeated mea-
surements of TEWL and chromametry a*-values every 24 h up to
96 h after tape stripping, respectively 72 h after SLS-induced bar-
rier abrogation.
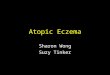
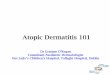
Monitoring of TEWL throughout the observation period
revealed no significant differences among the groups regarding the
rate of barrier recovery after tape stripping (Fig. 2a). Filaggrin-AD
was characterized by higher a*-values up to 72 h post-stripping,
the difference to non-filaggrin AD and the healthy controls how-
ever was not significant (Fig. 2b).
In each group, the 24-h application of 1% SLS under occlusion
resulted in a manifest inflammatory reaction, reflected by signifi-
cant increase in the visual score, chromametry a*-value and TEWL
following the removal of the chamber. Compared with baseline,
3 h post-irritation, filaggrin-AD was characterized by a greater
TEWL and a*-value increase (DTEWL: 34.24 g ⁄ m2 ⁄ h; Da*: 2.78
AU) than non-filaggrin AD or the healthy controls (DTEWL:
31.10 g ⁄ m2 ⁄ h, respectively 24.86 g ⁄ m2 ⁄ h; Da*:1.42 AU, respec-
tively 1.68 AU), the differences among the groups however were
not significant. Throughout the 72-h observation period, there
were no significant differences in the rate of barrier recovery
between the FLG mutation carriers and non-carriers or mutation
carriers and controls (Fig. 2c,d).
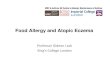
Distinct genotype-related alterations in the lipid composi-tion of the clinically uninvolved skin in filaggrin-ADThe non-lesional skin of the AD FLG mutation carriers was char-
acterized by increased total amount of cholesterol in comparison
to both non-filaggrin AD and the healthy controls as well as sig-
nificantly increased percentage amount of cholesterol (p<0.05)
and decreased triglyceride (TG) levels (p<0.01 and p<0.001 for
respectively, total and percentage amount) compared to the
healthy controls group (Fig.3 a,b). Furthermore, the AD patients
harbouring at least one FLG mutation had lower ceramide ⁄ choles-
terol ratio compared with both the wild-type and the healthy con-
trol group (4.55 ± 0.66, respectively 7.51 ± 1.48 and 8.95 ± 1.33).
No significant differences concerning the total and percentage
amount of ceramides, free fatty acids (FFA) or sterol esters among
the groups were found.
Compared with the healthy controls, the non-lesional skin of
the AD patients was characterized by increased total as well as sig-
nificantly increased percentage amounts of CER[AH ⁄ AP]
(P < 0.001) and significantly reduced amounts of CER[EOH]
(P < 0.001 for both total and percentage composition). The unin-
volved skin of the FLG mutation carriers was characterized by
0
5
10
15
20
25
2 ′ 10 ′ 20 ′ 30 ′Tape number
Prot
ein
(μg/
cm2 )
FLG-AD Non-filaggrin AD Controls(b)
0
10
20
30
40
2 ′ 10 ′ 20 ′ 30 ′Number of tapes
ΔTEW
L (g
/m2 /h
)
FLG-AD Non-filaggrin AD Controls(a)
*
*
Figure 1. (a) Stratum corneum integrity upon tape stripping; DTEWL = TEWLmeasured after the respective number of tapes ) baseline TEWL. (b) Amount ofremoved protein (lg ⁄ cm2). Mean ± SEM; level of significance set at 0.05;*P < 0.05. FLG-AD: filaggrin-AD; non-filaggrin AD: wild-type; controls: healthy,non-atopic controls.
Skin barrier integrity in filaggrin-AD
ª 2011 John Wiley & Sons A/S, Experimental Dermatology, 20, 351–356 353

markedly reduced total amounts of CER[EOH] compared with
both non-filaggrin AD and the control group; however, the differ-
ence was not significant. No significant differences in the ceramide
percentage composition of the uninvolved skin of the AD FLG
mutation carriers compared with the wild-type were observed
(data not shown).
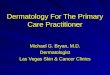
Significantly reduced amounts of free fatty acids, triglyce-rides and CER [EOH] in the lesional skin of the AD FLGmutation carriersIn comparison with non-filaggrin AD, the lesional skin of the
patients with filaggrin-AD was characterized by significantly
reduced total amounts of FFA (P < 0.05) as well as significantly
decreased amounts of TG (P < 0.001 for both total and percentage
amount; Fig. 4a,b). Furthermore, the FLG mutation carriers had
significantly reduced total and percentage amount of CER[EOH]
compared with the wild-type (P < 0.01, respectively P < 0.05;
Fig. 4c,d). Although the total and percentage amounts of CER[EOS]
in the lesional skin of the FLG mutation carriers were reduced,
the difference compared with non-filaggrin AD did not reach
significance.
DiscussionAlthough the association between the FLG loss-of-function alleles
and AD is firmly established, the downstream or functional conse-
quences of the aberrant genotype are incompletely understood so
far (30–32). Previous publications reported decreased levels of the
natural moisturizing factor (NMF) and its components 2-pyrroli-
done-5-carboxylic acid and urocanic acid in FLG mutation carriers
of European ancestry (15,17,33). In contrast to the good agree-
ment between the genotype and NMF levels, no correlation
between the baseline TEWL and the FLG loss-of-function carrier
state could be established so far (14,16,17). TEWL is an objective
and reproducible measure for assessment of the skin barrier integ-
rity and its validity in vivo and ex vivo has been confirmed in both
human and animal studies (34). Importantly, whereas the mea-
surement of baseline TEWL might not suggest differences, moni-
toring of TEWL upon controlled application of exogenous
stressors to the skin might reveal profound alterations in the per-
meability barrier function.
To the best of our knowledge, functional data on the skin bar-
rier integrity upon tape stripping in AD patients carrying the pre-
valent European FLG mutations have not been previously
Tape stripping
0
20
40
60
80
100
120
Time post tape stripping
TEW
L (%
)
FLG-AD Non-filaggrin AD Controls(a)
Tape stripping
020406080
100120140
0 h 24 h 48 h 72 h 96 h
0 h 24 h 48 h 72 h 96 hTime post tape stripping
a*-V
alue
(%)
FLG-AD Non-filaggrin Controls(b)
(c)
(d)
1% SLS
020406080
100120140
3 h 24 h 48 h 72 h
Time after removal of the test chamber
TEW
L (%
)
FLG-AD Non-filaggrin AD controls
1% SLS
020406080
100120140160
3 h 24 h 48 h 72 hTime after removal of the test chamber
a*-V
alue
(%)
FLG-AD Non-filaggrin AD Controls
Figure 2. Barrier recovery after tape stripping (a, b) and 24-h patch testapplication of 1% SLS (c, d), assessed by repeated TEWL and chromametrymeasurements. Mean ± SEM, normalized data. FLG-AD: filaggrin-AD; non-filaggrinAD: wild-type; controls: healthy, non-atopic controls.
Total amount of extracted lipidsNon-lesional skin
0
1
2
3
4
5
To
tal a
mo
un
t o
f lip
ids
(µg
/cm
2 )
FLG-AD Non-filaggrin AD Controls
**
Lipid profile: % of total lipidsNon-lesional skin
01020304050
Ceramides Cholesterol FFA Triglycerides Sterol esters
Ceramides Cholesterol FFA Triglycerides Sterol esters% o
f to
tal l
ipid
s FLG-AD Non-filaggrin AD Controls
* ***
(a)
(b)
Figure 3. Stratum corneum lipid profile of the clinically uninvolved skin presentedas total amount per extraction area (a) and percentage of total lipids (b).Mean ± SEM; level of significance set at 0.05; *P < 0.05, **P < 0.01,***P < 0.001. FLG-AD: filaggrin-AD; non-filaggrin AD: wild-type; controls: healthy,non-atopic controls; FFA: free fatty acids.
Total amount of extracted lipidsLesional skin
0
2
4
6
8
To
tal a
mo
un
t o
f lip
ids
(µg
/cm
2 )
To
tal a
mo
un
t o
f ce
ram
ides
(µ
g/c
m2 )
FLG-AD Non-filaggrin AD
***
*
Lipid profile: % of total lipidsLesional skin
01020304050
% o
f to
tal l
ipid
s FLG-AD Non-filaggrin AD
***
Total amount of recovered ceramidesLesional skin
0
1
2
3 FLG-AD Non-filaggrin AD
**
Ceramide composition: % of totaLesional skin
0102030405060
Ceramides Cholesterol FFA Triglycerides Sterol esters
Ceramides Cholesterol FFA Triglycerides Sterol esters
CER[AH/AP] CER[NH/AS] CER[EOH] CER[NP] CER[NS] CER[EOS]
CER[AH/AP] CER[NH/AS] CER[EOH] CER[NP] CER[NS] CER[EOS]% o
f to
tal c
eram
ides
FLG-AD Non-filaggrin AD
*
(a)
(b)
(c)
(d)
Figure 4. Lesional skin stratum corneum lipid (a, b) and ceramide profile (c, d).Mean ± SEM; level of significance <0.05; *P < 0.05, **P < 0.01, ***P < 0.001.FLG-AD: filaggrin-AD; non-filaggrin AD: wild-type; FFA: free fatty acids.
Angelova-Fischer et al.
354 ª 2011 John Wiley & Sons A/S, Experimental Dermatology, 20, 351–356

reported. The sequential application of adhesive tapes in our study
resulted in greater increase of TEWL (assessed by DTEWL as
described) in filaggrin-AD compared with non-filaggrin AD and
the healthy controls and these findings were consistent indepen-
dently of the number of tapes. Furthermore, the difference in
DTEWL between the AD FLG mutation carriers and non-carriers
or controls reached significance after 20 tapes thus providing evi-
dence for compromised barrier integrity upon mechanical stress in
FLG-related eczema. Tape stripping is an established model for
studying SC cohesion under experimental conditions (35–38). The
lower amount of removed protein per tape in the FLG mutations
carriers in our study make reasonable to hypothesize that the
aberrant genotype might be associated with alterations in SC cohe-
sion. These findings are supported by an earlier report showing
increased SC thickness in carriers of the Japanese p.Ser2554X,
p.Ser2889X, p.Ser3296X or c.3321del FLG loss-of-function variants
(14). Although the above mentioned as well as our results need to
be confirmed, these observations and the previously published evi-
dence for the role of skin surface pH for regulation of protease
activity and integrity ⁄ cohesion point to the need for further inves-
tigation of the link between skin surface pH and possibly abnor-
mal corneocyte cohesion in filaggrin-AD (39–41).
Manifest disease or past history of AD confer enhanced skin
reactivity and inflammatory response upon exposure to common
irritants such as SLS (42–45). Although in our study DTEWL fol-
lowing the 24-h patch test application of 1% SLS was greater in
filaggrin-AD, the difference between the FLG mutation carriers
and the wild-type was not significant and these results are in
agreement with a recently published report (16). As previously
suggested, these observations might be explained by the limited
number of volunteers however, the role of additional factors, such
as the concentration and mode of exposure, should be taken into
consideration for the interpretation of the so far available data.
The composition, organization and biochemical processing of
the SC lipids are important determinants of the permeability bar-
rier homeostasis (46–48). Whereas in a recent study, no differ-
ences regarding the major SC lipid classes in FLG mutation
carriers and non-carriers were found (16), the analysis of the SC
lipid composition in our study population revealed significantly
increased percentage amount of cholesterol and reduced cera-
mide ⁄ cholesterol ratio in the non-lesional skin of the AD patients
carrying at least one FLG loss-of-function variant. Our results are
in agreement with earlier publications reporting alterations in the
ceramide ⁄ cholesterol ratio in atopic skin (49) and might suggest a
link between the genotype and the abnormal lipid composition of
the clinically uninvolved skin of the FLG mutation carriers.
As mentioned, the SC lipid composition of the skin lesions in
AD patients harbouring FLG loss-of-function alleles has not been
characterized so far. Here we provide evidence for significantly
reduced amounts of FFA in the lesional skin of the AD FLG
mutation carriers compared with the non-carriers. In contrast to
our findings, earlier studies found no differences or increased FFA
as well as decreased CER levels in atopic skin (50,51) that could
be further explained by abnormal expression of sphingomyelin-
acylase and deacylase and altered sphingomyelin metabolism in
AD (52,53). The previously published data however refer to
patients with unknown FLG genotype and while genetic variations
may account for the observed differences, the role of confounding
factors such as inflammation should be additionally considered
for the interpretation of our results. In view of the critical role of
FFA for the SC lipid organization (54) and the regulation of key
epidermal barrier functions including SC acidification (55), integ-
rity and repair (56–62), our observations suggest a need for fur-
ther analysis of the underlying pathophysiologic mechanisms and
downstream consequences of the altered lesional skin FFA levels
in filaggrin-AD.
In addition to the reduced amount of FFA, we found signifi-
cant reduction in the amounts of CER[EOH] in the lesional skin
of the AD FLG mutation carriers when compared with the wild-
type. CER[EOH] is omega-hydroxyceramide (x-OH-CER) con-
sisting of a 6-hydroxysphingosine base amide-linked to a very long
chain N-acyl x-hydroxy fatty acid which is esterified to linoleic
acid (47). The esterified x-OH-CERs and their non-esterified,
protein-bound counterparts are unique to the human SC and have
been shown to play a critical role for the formation of the corni-
fied cell envelope, the SC lipid organization and permeability bar-
rier homeostasis (48,63–65). Earlier publications on the levels of
the protein-bound x-OH-CER in AD provide evidence for altera-
tions in de novo synthesis of CER[EOH] along with significant
reduction of the protein-bound x-OH-CER in the clinically unin-
volved as well as lesional skin of atopic eczema patients (66). The
results of our study are in agreement with these findings as well as
with recently published analysis of the ceramide profiles in atopic
skin (67) and suggest that genetic variations might, at least to a
certain extent, contribute to the x-OH-CER deficiency in AD.
Interestingly, the non-lesional as well as the lesional skin of the
AD patients carrying FLG mutations in our study was characterized
by decreased amounts of TG when compared with non-filaggrin AD
or the healthy controls. Triglycerides are synthesized in the epider-
mis and sebaceous glands; however, their role for permeability bar-
rier homeostasis is incompletely understood so far (57,68,69).
Animal studies provide evidence for reduced SC hydration in seba-
ceous glands deficient (asebia) mice and previous investigations in
human skin suggest that skin hydration correlates with both sebum
production and SC glycerol content (70,71). Earlier studies examin-
ing the role of sebaceous gland-derived lipids in the pathogenesis of
AD have yielded partly inconsistent results and although one study
found slightly (but not significantly) increased TG levels, most of
the so far available data, and our results, suggest that atopic skin is
characterized by reduced skin surface lipids amount (50,72,73). The
biochemical pathways leading to decreased TG levels in the non-
lesional and lesional skin of the AD FLG mutation carriers remain
unknown and further investigations of the pathophysiologic rele-
vance of our findings might prove important for understanding the
relationship between reduced skin surface lipids and dry skin in AD.
In conclusion, our results provide distinct phenotype correla-
tions and new supportive evidence for compromised barrier func-
tion and skin lipid composition in AD carriers of the prevalent
European FLG loss-of-function alleles. Further elucidation of the
causalities in filaggrin-AD is of crucial importance for understand-
ing the interplay of the individual factors involved in the initiation
and chronicity of disease. Such an approach will contribute to
translation of the scientific knowledge into optimized skin care
modalities, potential novel diagnostic approaches for at risk indi-
viduals and development of pharmacologic agents specifically tar-
geting the relevant pathophysiologic mechanisms.
Skin barrier integrity in filaggrin-AD
ª 2011 John Wiley & Sons A/S, Experimental Dermatology, 20, 351–356 355

AcknowledgementsThe project was supported by a research grant no. E19-2007 (IAF) from the
University of Lubeck and the European COST Network ‘Skin barrier in
atopic disease; (BM0903; ACM). We would like to thank all volunteers who
participated in the study as well as Dr Simon Wilkinson (Medical Toxicology
Centre, Newcastle University, UK) for critical reading of the manuscript.
References1 Segre J A. J Clin Invest 2006: 5: 1150–1158.2 Elias P M. J Invest Dermatol 2005: 125: 183–
200.3 McGrath J A. Austral J Dermato 2008: 49: 67–
74.4 Richard G. Am J Med Genet C Semin Med
Genet 2004:15:131C(1):32–44.5 Hoffjan S, Stemmler S. Br J Dermatol 2007: 157:
441–49.6 Smith F, Irvine A, Terron-Kwiatkowski A et al.
Nat Genet 2006: 38: 337–342.7 Sandilands A, O’Regan G, Liao H et al. J Invest
Dermatol 2006: 126: 1770–1775.8 Sandilands A, Terron-Kwiatkowski A, Hull P et al.
Nat Genet 2007: 39: 650–654.9 Baurecht H, Irvine A D, Novak N et al. J Allergy
Clin Immunol 2007: 120: 1406–1412.10 Rodrıguez E, Baurecht H, Herberich E et al.
J Allergy Clin Immunol 2009: 123: 1361–1370.11 Nomura T, Sandilands A, Akiyama M et al.
J Allergy Clin Immunol 2007: 119: 434–440.12 Nomura T, Akiyama M, Sandilands A et al.
J Invest Dermatol 2008: 128: 1436–1441.13 Chen H, Ho J, Sandilands A et al. Exp Dermatol
2008: 128: 1669–1975.14 Nemoto-Hasebe I, Akiyama M, Nomura T et al.
J Invest Dermatol 2009: 129: 682–689.15 Kezic S, Kemperman P M, Koster E S et al.
J Invest Dermatol 2008: 128: 2117–2119.16 Jungersted J M, Scheer H, Mempel M et al.
Allergy 2010: 65: 911–918.17 O’Regan G M, Kemperman P M, Sandilands A
et al. J Allergy Clin Immunol 2010: 126: 574–580.
18 Jakasa I, Koster E, Calkoen F et al. J Invest Der-matol 2011:131:540–542.
19 Williams H, Burney P G J, Hay R J. Br J Dermatol1994: 131: 383–396.
20 European Task Force on Atopic Dermatitis. Der-matology 1993: 186: 23–31.
21 Ruther A, Stoll M, Schwarz T et al. Br J Dermatol2006: 154: 1093–1094.
22 Rogiers V. Skin Pharmacol Appl Skin Physiol2001: 14: 117–128.
23 Pinnagoda J, Tupker R A, Agner T et al. ContactDermatitis 1990: 22: 164–178.
24 Fullerton A, Fischer T, Lahti A et al. Contact Der-matitis 1996: 35: 1–10.
25 Voegeli R, Heiland J, Doppler S et al. Skin ResTechnol 2007: 13: 242–251.
26 Frosch P J, Kligman A M. J Am Acad Dermatol1979: 1: 35–41.
27 Imokawa G, Abe A, Jin K et al. J Invest Dermatol1991: 96: 523–526.
28 Farwanah H, Neubert R, Zellmer S et al. J Chro-matogr B Analyt Technol Biomed Life Sci 2002:780: 443–450.
29 Farwanah H, Raith K, Neubert R H et al. ArchDermatol Res 2005: 296: 514–521.
30 Bos J, Brenninkmeyer E, Schram M et al. ExpDermatol 2010: 19: 325–331.
31 Mildner M, Jin J, Eckhart L et al. J Invest Derma-tol 2010: 130: 2286–2294.
32 O’Reagan G M, Irvine A D. Clin Exp Allergy2010: 40: 965–972.
33 Kezic S, Kammeyer A, Calkoen F et al. Br J Der-matol 2009: 161: 1098–1104.
34 Fluhr J W, Feingold K R, Elias P M. Exp Dermatol2006: 15: 483–492.
35 Breternitz M, Flach M, Praßler J et al. Br J Der-matol 2007: 156: 231–240.
36 Pinkus H. J Invest Dermatol 1951: 16: 383–386.37 Loeffler H, Dreher F, Maibach H I. Br J Dermatol
2004: 151: 746–752.38 Pinkus H. G Ital Dermatol Minerva Dermatol
1966: 107: 1115–1126.39 Hatano Y, Man M Q, Uchida Y et al. J Invest
Dermatol 2009: 129: 1824–1835.40 Hachem J P, Crumrine D, Fluhr J W et al. J Invest
Dermatol 2003: 121: 345–353.41 Voegeli R, Rawlings A V, Breternitz M et al. Br J
Dermatol 2009: 161: 70–77.42 Agner T. Contact Dermatitis 1991: 25: 108–114.43 van der Valk P G, Kruis-de Vries M H, Nater J P
et al. Clin Exp Dermatol 1985: 10: 185–193.44 Agner T. Acta Derm Venereol 1992: 173: 1–26.45 Tupker R A, Pinnagoda J, Coenraads P J et al. Br
J Dermatol 1990: 123: 199–205.46 Proksch E, Jensen J M, Elias P M. Clin Dermatol
2003: 21: 134–144.47 Holleran W M, Takagi Y, Uchida Y. FEBS Lett
2006: 580: 5456–5466.48 Bouwstra J A, Gooris G S, Dubbelaar F E et al.
J Lipid Res 1998: 39: 186–196.49 Di Nardo A, Wertz P, Giannetti A et al. Acta
Derm Venereol 1998: 78: 27–30.
50 Yamamoto A, Serizawa S, Ito M et al. Arch Der-matol Res 1991: 283: 219–223.
51 Bleck O, Abeck D, Ring J et al. J Invest Dermatol1999: 113: 894–900.
52 Hara J, Higuchi K, Okamoto R et al. J Invest Der-matol 2000: 115: 406–413.
53 Murata Y, Ogata J, Higaki Y et al. J Invest Der-matol 1996: 106: 1242–1249.
54 Bouwstra J A, Gooris G S, Dubbelaar F E et al.J Invest Dermatol Symp Proc 1998: 3: 69–74.
55 Fluhr J W, Kao J, Jain M et al. J Invest Dermatol2001: 117: 44–51.
56 Man M Q, Elias P M, Feingold K. J Clin Invest1993: 92: 791–798.
57 Feingold K. J Lipid Res 2007: 48: 2531–2546.58 Grubauer G, Feingold K, Elias P M. J Lipid Res
1987: 28: 746–752.59 Ottey K A, Wood L C, Grundfeld C et al. J Invest
Dermatol 1995: 104: 401–4.60 Proksch E, Holleran W, Menon G K et al. Br J
Dermatol 1993: 128: 473–82.61 Man M Q, Feingold K R, Jain M et al. J Lipid Res
1995: 36: 1925–1935.62 Man M Q, Jain M, Feingold K R et al. J Invest
Dermatol 1996: 106: 57–63.63 Uchida Y, Holleran W M. J Dermatol Sci 2008:
51: 77–87.64 Doering T, Holleran W M, Potratz A et al. J Biol
Chem 1999: 274: 11038–11045.65 Behne M, Uchida Y, Seki T et al. J Invest Derma-
tol 2000: 114: 185–192.66 Macheleidt O, Kaiser H W, Sandhoff K. J Invest
Dermatol 2002: 119: 166–173.67 Ishikawa J, Narita H, Kondo N et al. J Invest Der-
matol 2010: 130: 2511–2513.68 Nicolaides N. Science 1974: 186: 19–26.69 Schurer N Y, Elias P M. Adv Lipid Res 1991: 24:
27–56.70 Fluhr J W, Mao-Qiang M, Brown B et al. J Invest
Dermatol 2003: 120: 728–737.71 Choi E H, Man M Q, Wang F et al. J Invest Der-
matol 2005: 125: 288–293.72 Abe T, Ohkido M, Yamamoto K. J Dermatol
(Tokyo) 1978: 5: 223–229.73 Sator P G, Schmidt J, Honigsmann H. J Am Acad
Dermatol 2003: 48: 352–358.
Angelova-Fischer et al.
356 ª 2011 John Wiley & Sons A/S, Experimental Dermatology, 20, 351–356