Embed Size (px)
Citation preview
District Health Board Serious Adverse Events
1 July 2012 to 30 June 2013
District health boards have summarised on their websites the serious adverse events reported during 2012-13.
The document below has been copied from the DHB summaries and placed into one document.
It is recommended that the DHB website is primarily accessed for this information, as DHBs have provided more detail about the quality activities underway at each.
1
Auckland DHB
Auckland District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.adhb.govt.nz/
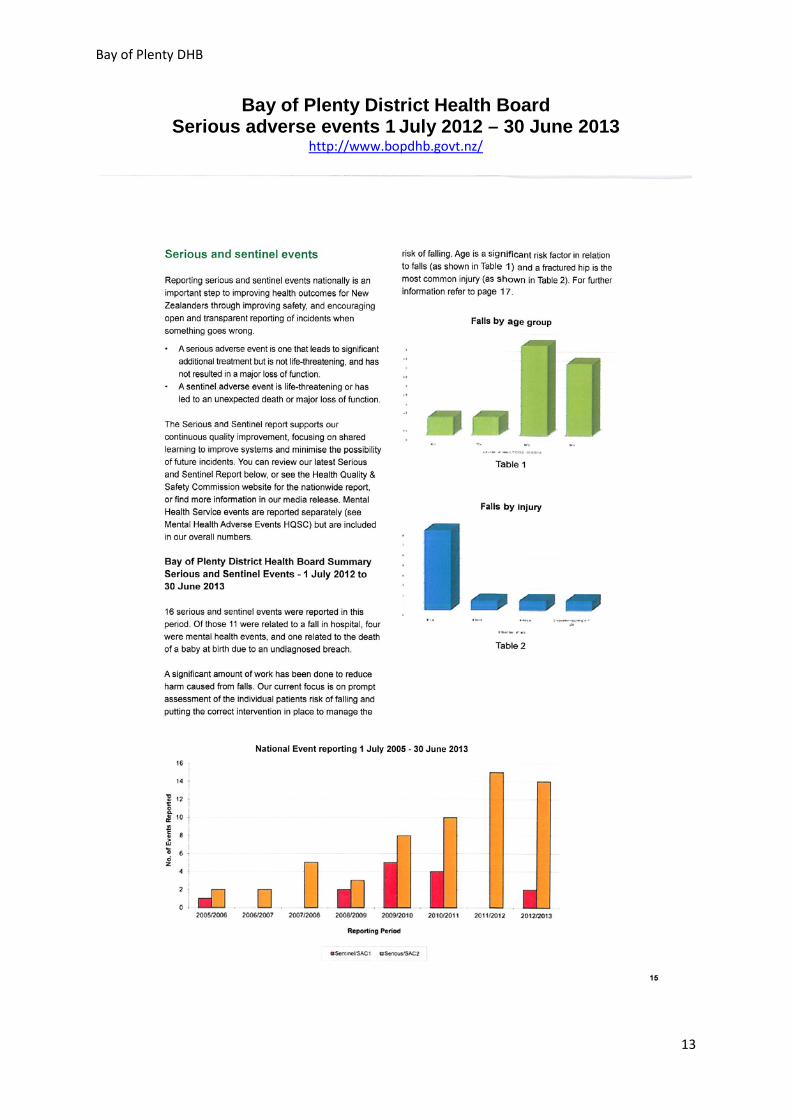
There were 67 serious adverse events reported by ADHB in the July 2012 to June 2013 year.
Adverse events identified as serious receive an in-depth investigation by a team of clinicians and quality department staff who are independent from the event. The reports are reviewed by a committee of senior management and senior clinical staff for robustness and for issues which may need to be addressed at an organisational level. The recommendations from the reports are tracked to ensure that follow-up and implementation occurs.
The table and report below outlines a summary of events, findings and recommendations of the events which have occurred. The events have been classified into eight specific themes:
• Delay in escalation of treatment
• Wrong procedure
• Patient misidentification
• Procedural injury
• Medication error
• Delay/failure in follow up or treatment
• Pressure injuries
• Falls
• Other
2
Auckland DHB
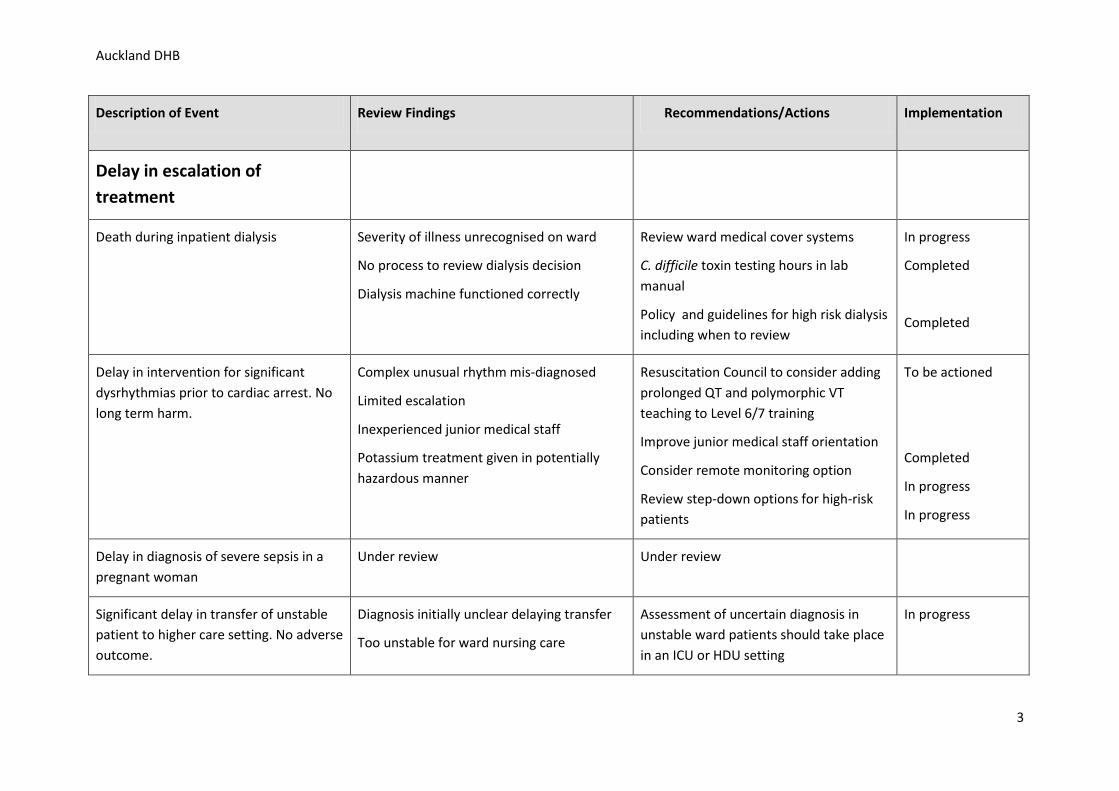
Description of Event Review Findings Recommendations/Actions Implementation
Delay in escalation of treatment
Death during inpatient dialysis Severity of illness unrecognised on ward
No process to review dialysis decision
Dialysis machine functioned correctly
Review ward medical cover systems
C. difficile toxin testing hours in lab manual
Policy and guidelines for high risk dialysis including when to review
In progress
Completed
Completed
Delay in intervention for significant dysrhythmias prior to cardiac arrest. No long term harm.
Complex unusual rhythm mis-diagnosed
Limited escalation
Inexperienced junior medical staff
Potassium treatment given in potentially hazardous manner
Resuscitation Council to consider adding prolonged QT and polymorphic VT teaching to Level 6/7 training
Improve junior medical staff orientation
Consider remote monitoring option
Review step-down options for high-risk patients
To be actioned
Completed
In progress
In progress
Delay in diagnosis of severe sepsis in a pregnant woman
Under review Under review
Significant delay in transfer of unstable patient to higher care setting. No adverse outcome.
Diagnosis initially unclear delaying transfer
Too unstable for ward nursing care
Assessment of uncertain diagnosis in unstable ward patients should take place in an ICU or HDU setting
In progress
3
Auckland DHB
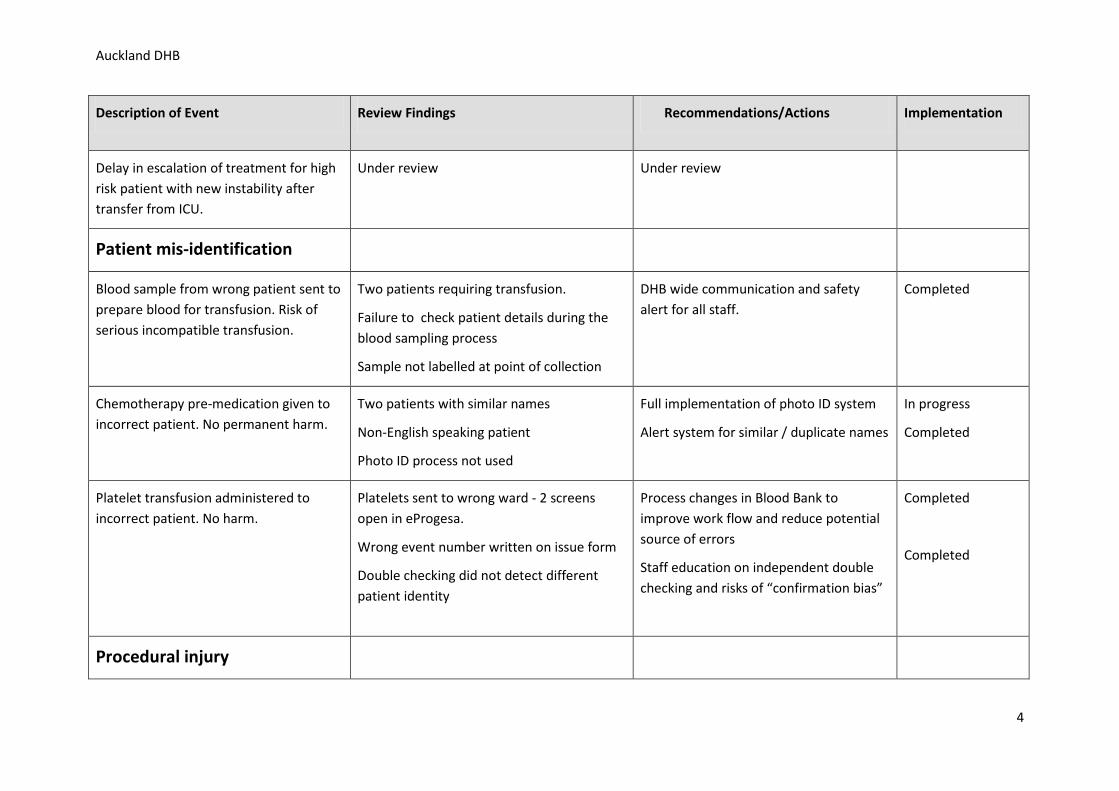
Description of Event Review Findings Recommendations/Actions Implementation
Delay in escalation of treatment for high risk patient with new instability after transfer from ICU.
Under review Under review
Patient mis-identification
Blood sample from wrong patient sent to prepare blood for transfusion. Risk of serious incompatible transfusion.
Two patients requiring transfusion.
Failure to check patient details during the blood sampling process
Sample not labelled at point of collection
DHB wide communication and safety alert for all staff.
Completed
Chemotherapy pre-medication given to incorrect patient. No permanent harm.
Two patients with similar names
Non-English speaking patient
Photo ID process not used
Full implementation of photo ID system
Alert system for similar / duplicate names
In progress
Completed
Platelet transfusion administered to incorrect patient. No harm.
Platelets sent to wrong ward - 2 screens open in eProgesa.
Wrong event number written on issue form
Double checking did not detect different patient identity
Process changes in Blood Bank to improve work flow and reduce potential source of errors
Staff education on independent double checking and risks of “confirmation bias”
Completed
Completed
Procedural injury
4
Auckland DHB
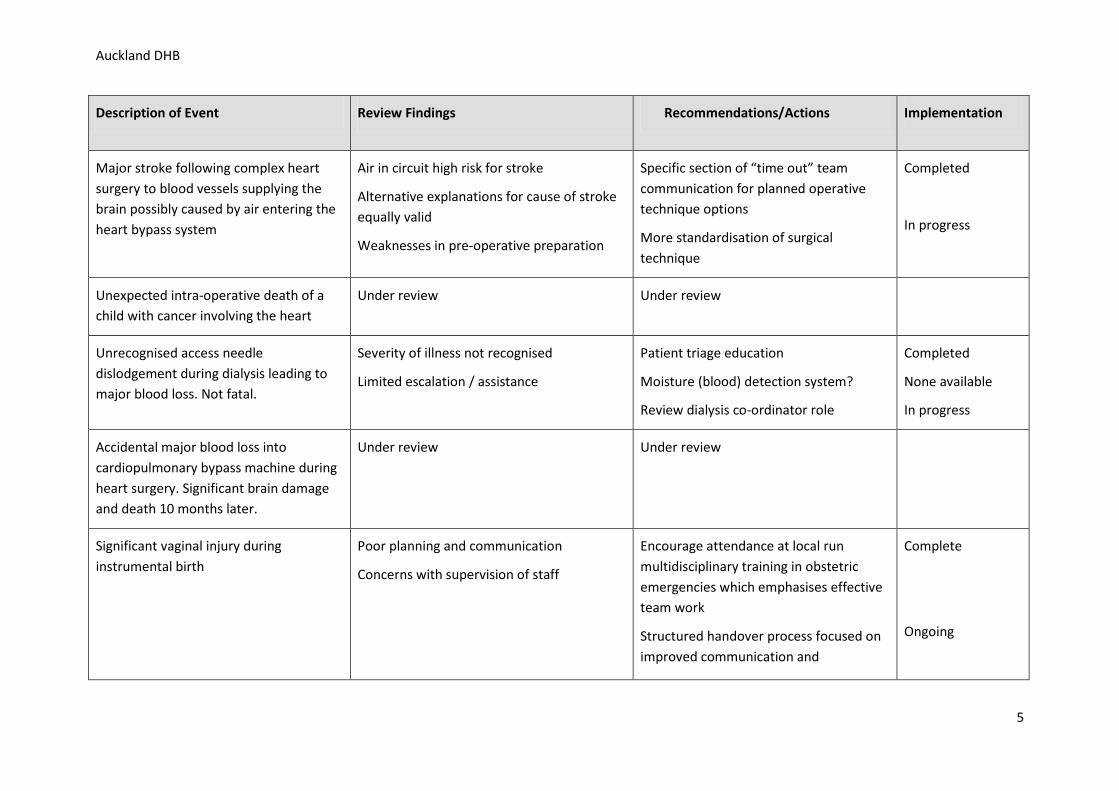
Description of Event Review Findings Recommendations/Actions Implementation
Major stroke following complex heart surgery to blood vessels supplying the brain possibly caused by air entering the heart bypass system
Air in circuit high risk for stroke
Alternative explanations for cause of stroke equally valid
Weaknesses in pre-operative preparation
Specific section of “time out” team communication for planned operative technique options
More standardisation of surgical technique
Completed
In progress
Unexpected intra-operative death of a child with cancer involving the heart
Under review Under review
Unrecognised access needle dislodgement during dialysis leading to major blood loss. Not fatal.
Severity of illness not recognised
Limited escalation / assistance
Patient triage education
Moisture (blood) detection system?
Review dialysis co-ordinator role
Completed
None available
In progress
Accidental major blood loss into cardiopulmonary bypass machine during heart surgery. Significant brain damage and death 10 months later.
Under review Under review
Significant vaginal injury during instrumental birth
Poor planning and communication
Concerns with supervision of staff
Encourage attendance at local run multidisciplinary training in obstetric emergencies which emphasises effective team work
Structured handover process focused on improved communication and
Complete
Ongoing
5
Auckland DHB
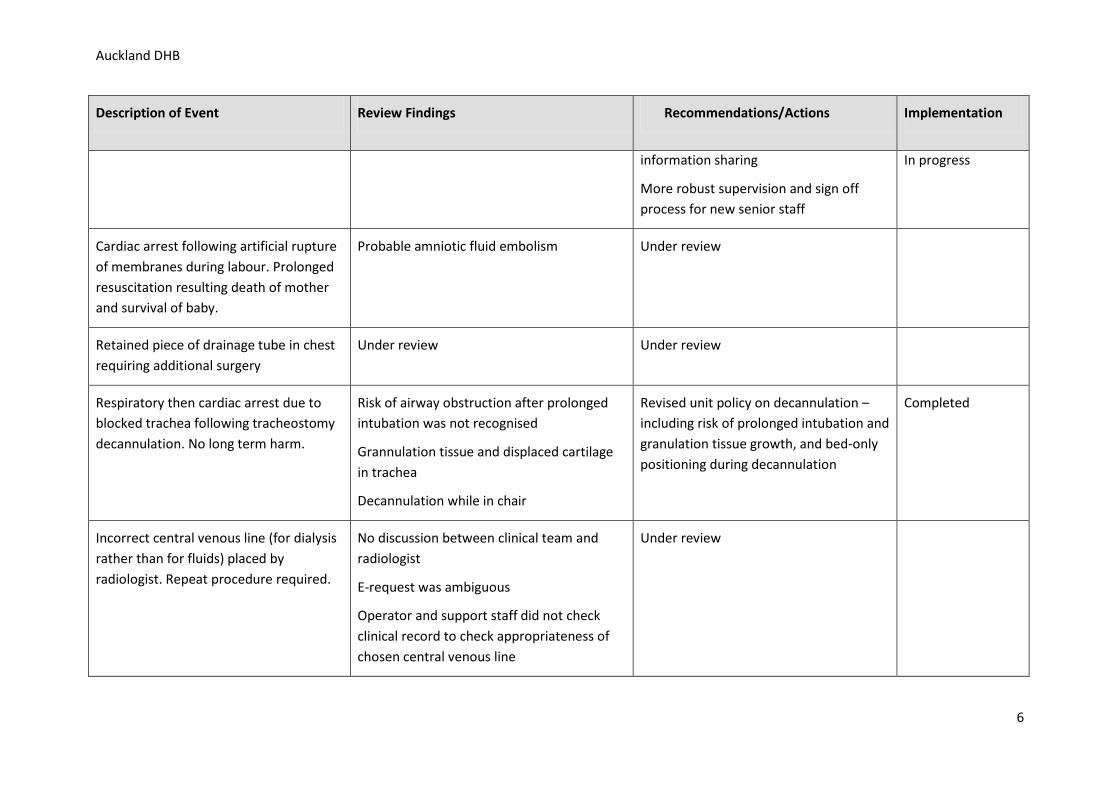
Description of Event Review Findings Recommendations/Actions Implementation
information sharing
More robust supervision and sign off process for new senior staff
In progress
Cardiac arrest following artificial rupture of membranes during labour. Prolonged resuscitation resulting death of mother and survival of baby.
Probable amniotic fluid embolism
Under review
Retained piece of drainage tube in chest requiring additional surgery
Under review Under review
Respiratory then cardiac arrest due to blocked trachea following tracheostomy decannulation. No long term harm.
Risk of airway obstruction after prolonged intubation was not recognised
Grannulation tissue and displaced cartilage in trachea
Decannulation while in chair
Revised unit policy on decannulation – including risk of prolonged intubation and granulation tissue growth, and bed-only positioning during decannulation
Completed
Incorrect central venous line (for dialysis rather than for fluids) placed by radiologist. Repeat procedure required.
No discussion between clinical team and radiologist
E-request was ambiguous
Operator and support staff did not check clinical record to check appropriateness of chosen central venous line
Under review
6
Auckland DHB
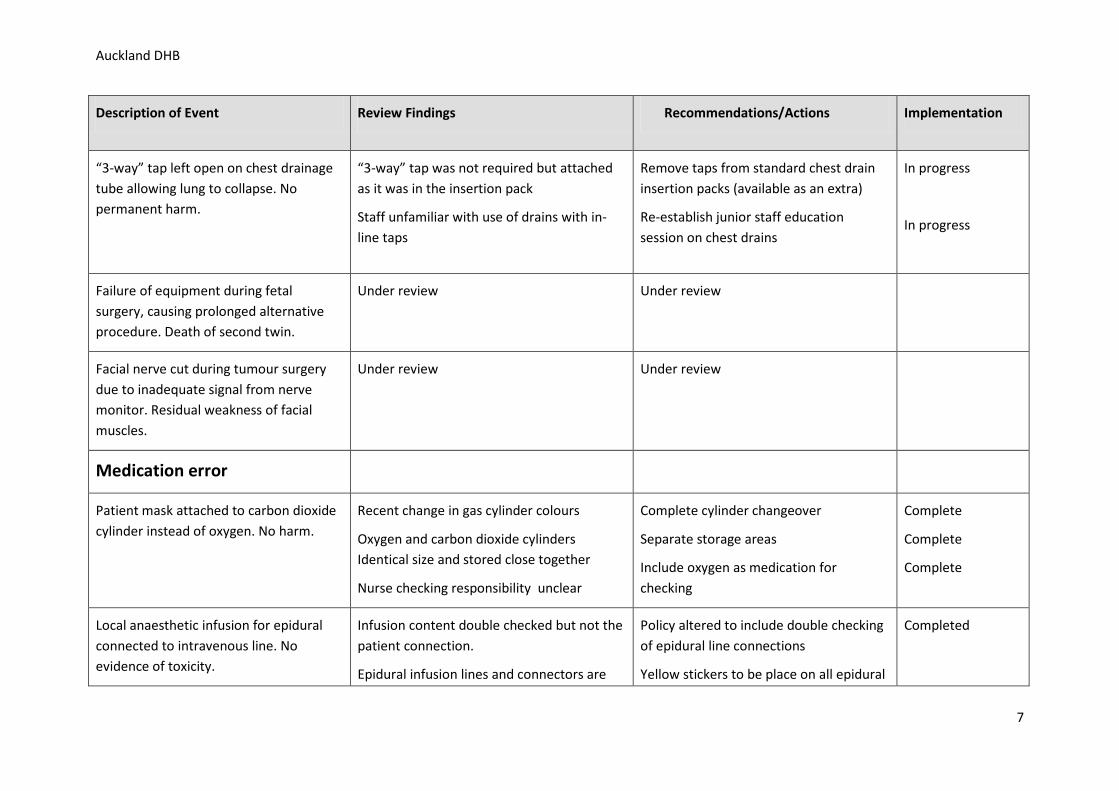
Description of Event Review Findings Recommendations/Actions Implementation
“3-way” tap left open on chest drainage tube allowing lung to collapse. No permanent harm.
“3-way” tap was not required but attached as it was in the insertion pack
Staff unfamiliar with use of drains with in-line taps
Remove taps from standard chest drain insertion packs (available as an extra)
Re-establish junior staff education session on chest drains
In progress
In progress
Failure of equipment during fetal surgery, causing prolonged alternative procedure. Death of second twin.
Under review Under review
Facial nerve cut during tumour surgery due to inadequate signal from nerve monitor. Residual weakness of facial muscles.
Under review Under review
Medication error
Patient mask attached to carbon dioxide cylinder instead of oxygen. No harm.
Recent change in gas cylinder colours
Oxygen and carbon dioxide cylinders Identical size and stored close together
Nurse checking responsibility unclear
Complete cylinder changeover
Separate storage areas
Include oxygen as medication for checking
Complete
Complete
Complete
Local anaesthetic infusion for epidural connected to intravenous line. No evidence of toxicity.
Infusion content double checked but not the patient connection.
Epidural infusion lines and connectors are
Policy altered to include double checking of epidural line connections
Yellow stickers to be place on all epidural
Completed
7
Auckland DHB
Description of Event Review Findings Recommendations/Actions Implementation
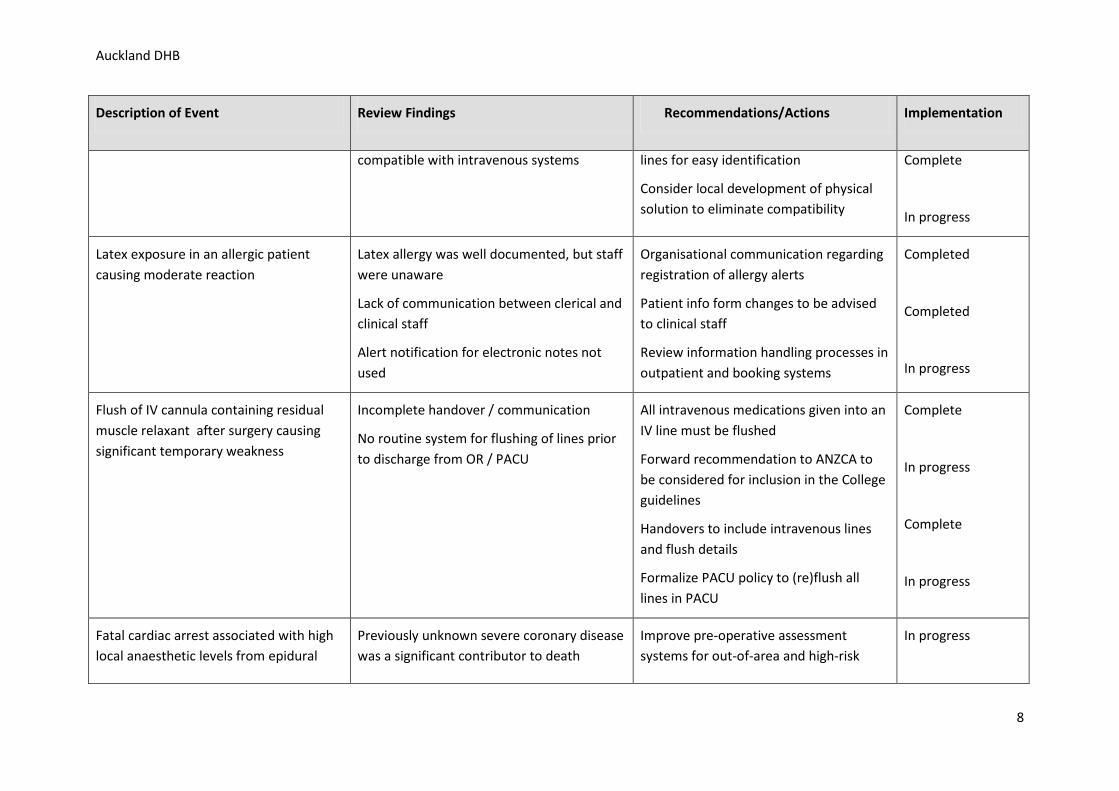
compatible with intravenous systems lines for easy identification
Consider local development of physical solution to eliminate compatibility
Complete
In progress
Latex exposure in an allergic patient causing moderate reaction
Latex allergy was well documented, but staff were unaware
Lack of communication between clerical and clinical staff
Alert notification for electronic notes not used
Organisational communication regarding registration of allergy alerts
Patient info form changes to be advised to clinical staff
Review information handling processes in outpatient and booking systems
Completed
Completed
In progress
Flush of IV cannula containing residual muscle relaxant after surgery causing significant temporary weakness
Incomplete handover / communication
No routine system for flushing of lines prior to discharge from OR / PACU
All intravenous medications given into an IV line must be flushed
Forward recommendation to ANZCA to be considered for inclusion in the College guidelines
Handovers to include intravenous lines and flush details
Formalize PACU policy to (re)flush all lines in PACU
Complete
In progress
Complete
In progress
Fatal cardiac arrest associated with high local anaesthetic levels from epidural
Previously unknown severe coronary disease was a significant contributor to death
Improve pre-operative assessment systems for out-of-area and high-risk
In progress
8
Auckland DHB
Description of Event Review Findings Recommendations/Actions Implementation
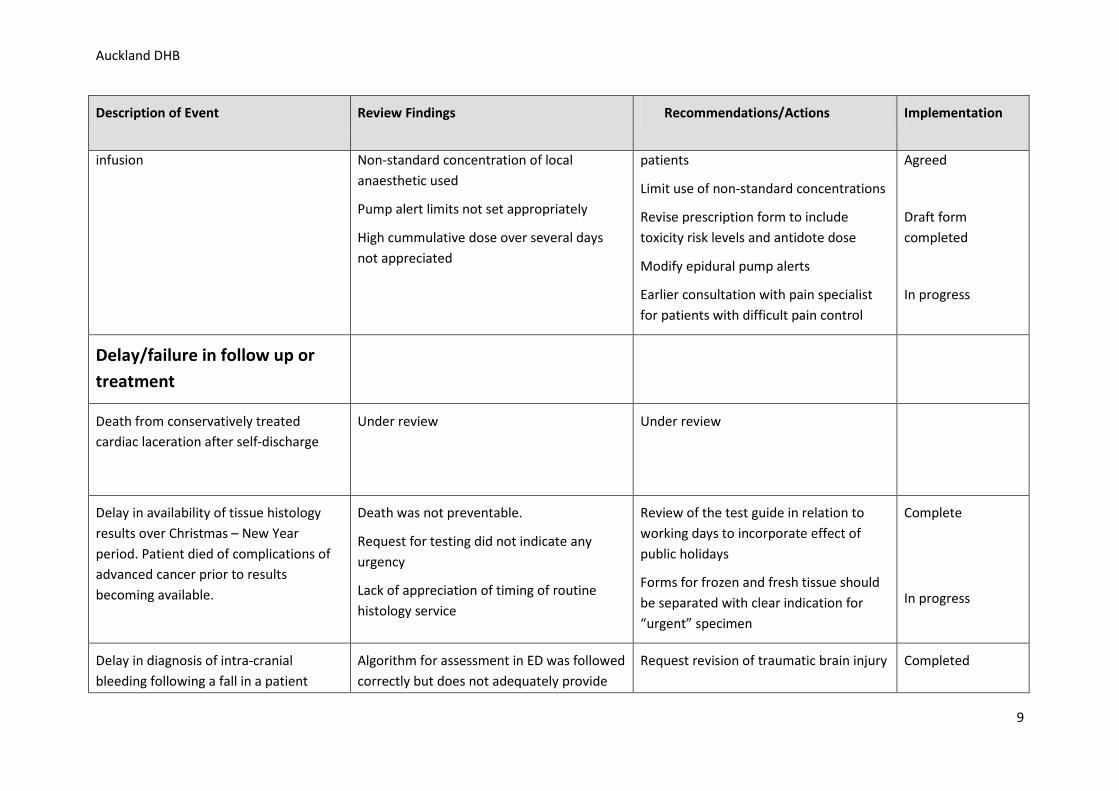
infusion Non-standard concentration of local anaesthetic used
Pump alert limits not set appropriately
High cummulative dose over several days not appreciated
patients
Limit use of non-standard concentrations
Revise prescription form to include toxicity risk levels and antidote dose
Modify epidural pump alerts
Earlier consultation with pain specialist for patients with difficult pain control
Agreed
Draft form completed
In progress
Delay/failure in follow up or treatment
Death from conservatively treated cardiac laceration after self-discharge
Under review Under review
Delay in availability of tissue histology results over Christmas – New Year period. Patient died of complications of advanced cancer prior to results becoming available.
Death was not preventable.
Request for testing did not indicate any urgency
Lack of appreciation of timing of routine histology service
Review of the test guide in relation to working days to incorporate effect of public holidays
Forms for frozen and fresh tissue should be separated with clear indication for “urgent” specimen
Complete
In progress
Delay in diagnosis of intra-cranial bleeding following a fall in a patient
Algorithm for assessment in ED was followed correctly but does not adequately provide
Request revision of traumatic brain injury Completed
9
Auckland DHB
Description of Event Review Findings Recommendations/Actions Implementation
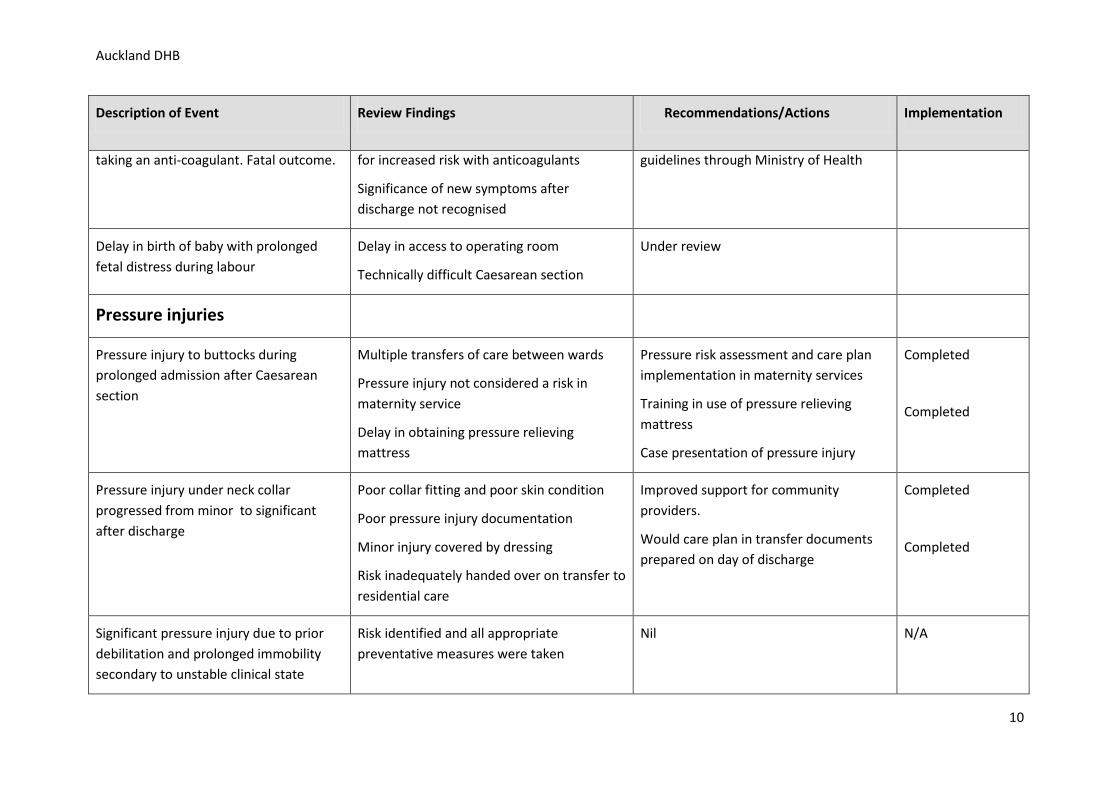
taking an anti-coagulant. Fatal outcome. for increased risk with anticoagulants
Significance of new symptoms after discharge not recognised
guidelines through Ministry of Health
Delay in birth of baby with prolonged fetal distress during labour
Delay in access to operating room
Technically difficult Caesarean section
Under review
Pressure injuries
Pressure injury to buttocks during prolonged admission after Caesarean section
Multiple transfers of care between wards
Pressure injury not considered a risk in maternity service
Delay in obtaining pressure relieving mattress
Pressure risk assessment and care plan implementation in maternity services
Training in use of pressure relieving mattress
Case presentation of pressure injury
Completed
Completed
Pressure injury under neck collar progressed from minor to significant after discharge
Poor collar fitting and poor skin condition
Poor pressure injury documentation
Minor injury covered by dressing
Risk inadequately handed over on transfer to residential care
Improved support for community providers.
Would care plan in transfer documents prepared on day of discharge
Completed
Completed
Significant pressure injury due to prior debilitation and prolonged immobility secondary to unstable clinical state
Risk identified and all appropriate preventative measures were taken
Nil N/A
10
Auckland DHB
Description of Event Review Findings Recommendations/Actions Implementation
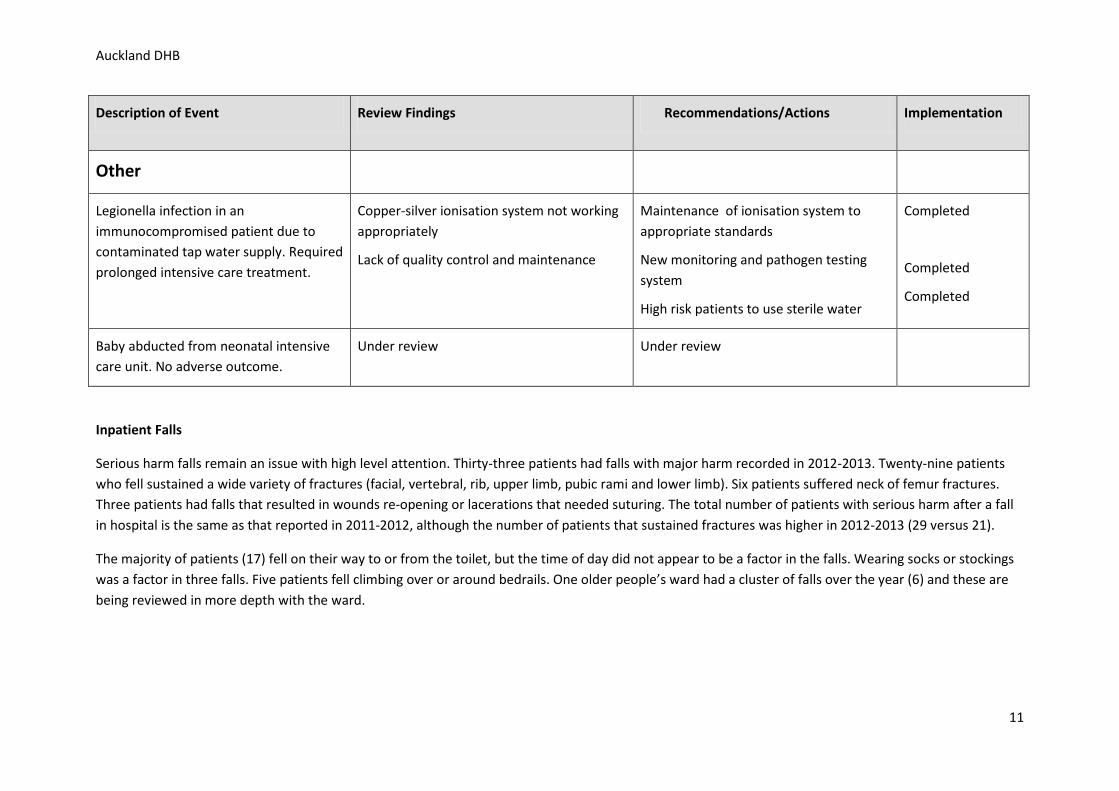
Other
Legionella infection in an immunocompromised patient due to contaminated tap water supply. Required prolonged intensive care treatment.
Copper-silver ionisation system not working appropriately
Lack of quality control and maintenance
Maintenance of ionisation system to appropriate standards
New monitoring and pathogen testing system
High risk patients to use sterile water
Completed
Completed
Completed
Baby abducted from neonatal intensive care unit. No adverse outcome.
Under review Under review
Inpatient Falls
Serious harm falls remain an issue with high level attention. Thirty-three patients had falls with major harm recorded in 2012-2013. Twenty-nine patients who fell sustained a wide variety of fractures (facial, vertebral, rib, upper limb, pubic rami and lower limb). Six patients suffered neck of femur fractures. Three patients had falls that resulted in wounds re-opening or lacerations that needed suturing. The total number of patients with serious harm after a fall in hospital is the same as that reported in 2011-2012, although the number of patients that sustained fractures was higher in 2012-2013 (29 versus 21).
The majority of patients (17) fell on their way to or from the toilet, but the time of day did not appear to be a factor in the falls. Wearing socks or stockings was a factor in three falls. Five patients fell climbing over or around bedrails. One older people’s ward had a cluster of falls over the year (6) and these are being reviewed in more depth with the ward.
11
Auckland DHB
A multidisciplinary falls and pressure injury steering group oversees improvement work and has been in place for two years. Across ADHB the following actions have been implemented in 2012-2013:
• Accurate identification processes using checking of coding databases to identify all patients who suffer serious harm falls. This process was changed from a quarterly check to a monthly check in March 2013.
• Standardised risk assessment with an intervention package for adult areas in ADHB. Implementation was completed in February/March 2013. • Intentional rounding has been implemented in older people’s and general medical wards with the aim to implement in all adult wards. Intentional
rounding involves patients being asked every hour if there is anything the staff member can do for the patient (in addition to normal clinical contact). Such an approach helps address comfort and toileting needs.
• “Sticky socks” have been made available for patients to wear over stockings or if the patient does not have hard soled foot wear available. Implementation started in September 2013.
• Case review of all serious harm falls by the Nurse Advisor Quality & Safety to identify lessons for the organisation. • Monthly random audit of falls risk assessment and care planning. Initiated in April 2013, with feedback reports from the Chief Nursing Officer circulated
to all wards showing each ward’s compliance with the HQSC criteria for falls risk assessment and the ward position with respect to compliance compared to other wards.
Issues for further attention
The appropriate use of bedrails has received increased focus as bedrails can both prevent harm and cause harm, and five patients suffered a serious injury climbing over or around bedrails. A workgroup involving restraint and falls experts has been convened, cause and effect workshops held, and areas for attention identified with implementation expected in the beginning of 2014. This work is aligned with work in behaviours of concern to ensure patients have the right interventions matched to their ongoing level of need.
Case review for each serious harm fall is undertaken by the charge health professional in the area the fall occurred to identify and remedy local factors leading to or associated with the fall. However, serious harms falls in each clinical area are a rare event for that area. Reviewing each serious harm fall in isolation from other such falls (with respect to that area and over time) means that clinical areas may struggle to identify lessons. Thus the process and type of review requires further development at ADHB.
12
Bay of Plenty DHB
Bay of Plenty District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.bopdhb.govt.nz/
13
Bay of Plenty DHB
14
Bay of Plenty DHB
15
Canterbury DHB
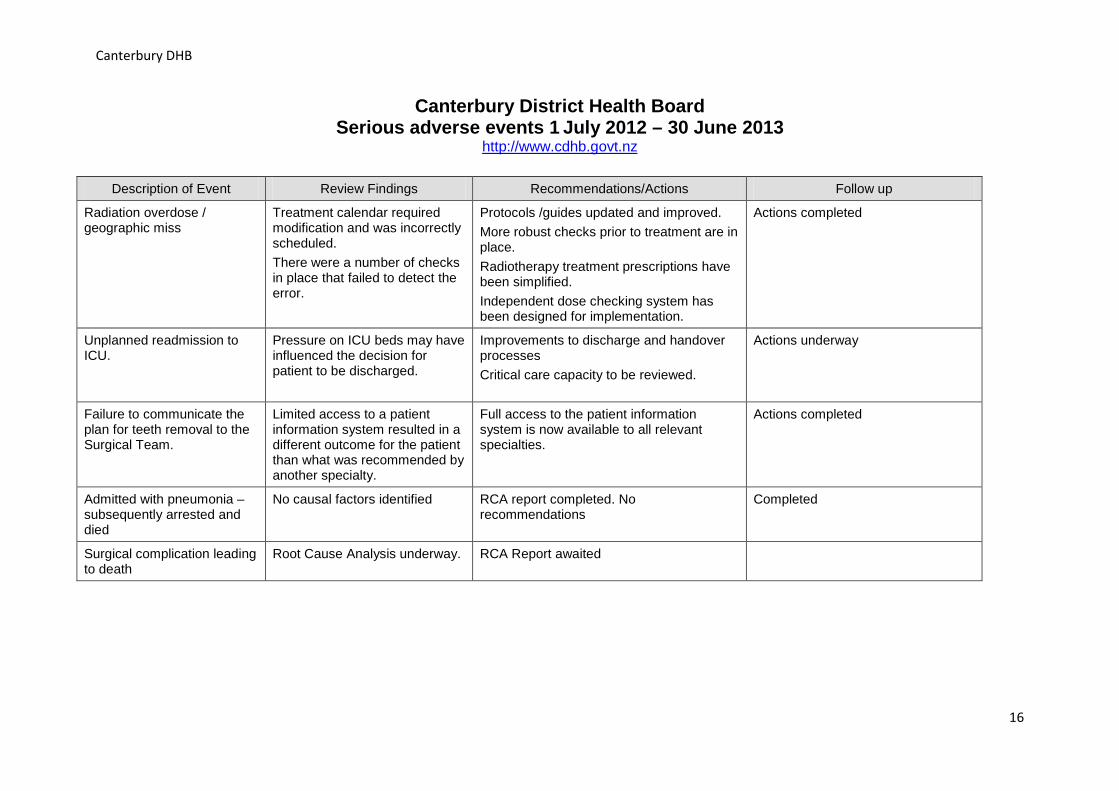
Canterbury District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.cdhb.govt.nz
Description of Event Review Findings Recommendations/Actions Follow up
Radiation overdose / geographic miss
Treatment calendar required modification and was incorrectly scheduled. There were a number of checks in place that failed to detect the error.
Protocols /guides updated and improved. More robust checks prior to treatment are in place. Radiotherapy treatment prescriptions have been simplified. Independent dose checking system has been designed for implementation.
Actions completed
Unplanned readmission to ICU.
Pressure on ICU beds may have influenced the decision for patient to be discharged.
Improvements to discharge and handover processes Critical care capacity to be reviewed.
Actions underway
Failure to communicate the plan for teeth removal to the Surgical Team.
Limited access to a patient information system resulted in a different outcome for the patient than what was recommended by another specialty.
Full access to the patient information system is now available to all relevant specialties.
Actions completed
Admitted with pneumonia – subsequently arrested and died
No causal factors identified RCA report completed. No recommendations
Completed
Surgical complication leading to death
Root Cause Analysis underway. RCA Report awaited
16
Canterbury DHB
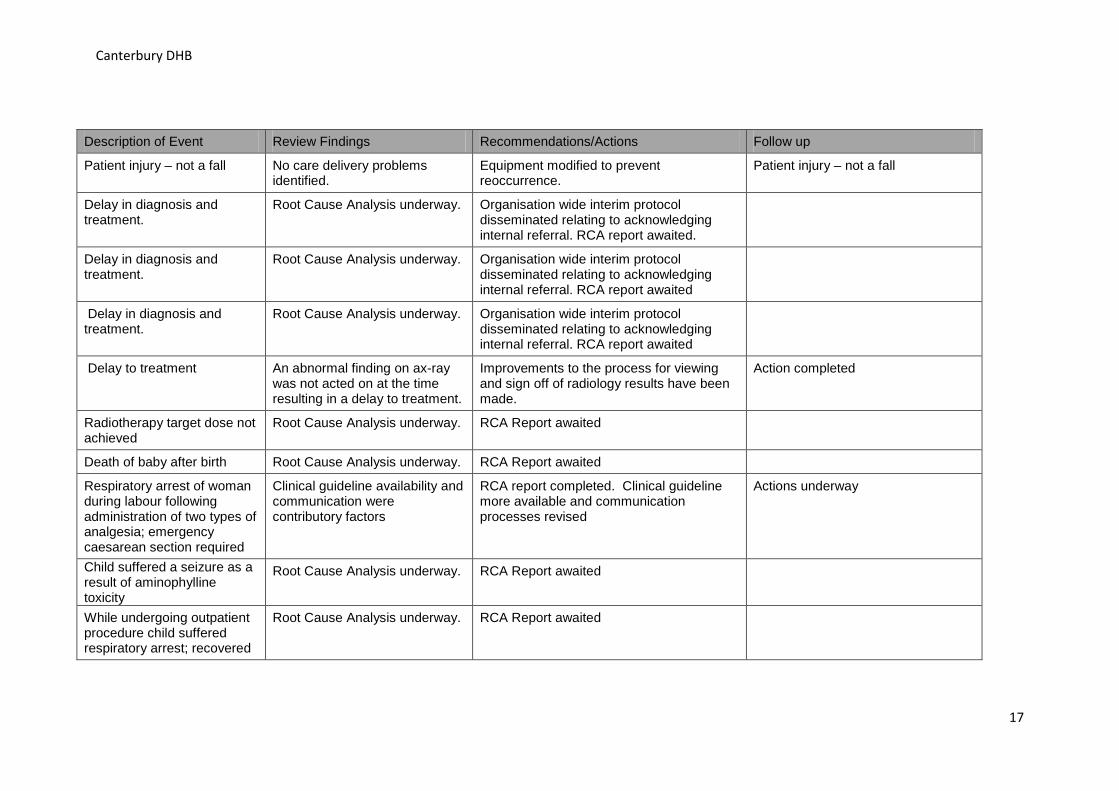
Description of Event Review Findings Recommendations/Actions Follow up
Patient injury – not a fall No care delivery problems identified.
Equipment modified to prevent reoccurrence.
Patient injury – not a fall
Delay in diagnosis and treatment.
Root Cause Analysis underway. Organisation wide interim protocol disseminated relating to acknowledging internal referral. RCA report awaited.
Delay in diagnosis and treatment.
Root Cause Analysis underway. Organisation wide interim protocol disseminated relating to acknowledging internal referral. RCA report awaited
Delay in diagnosis and treatment.
Root Cause Analysis underway. Organisation wide interim protocol disseminated relating to acknowledging internal referral. RCA report awaited
Delay to treatment An abnormal finding on ax-ray was not acted on at the time resulting in a delay to treatment.
Improvements to the process for viewing and sign off of radiology results have been made.
Action completed
Radiotherapy target dose not achieved
Root Cause Analysis underway. RCA Report awaited
Death of baby after birth Root Cause Analysis underway. RCA Report awaited
Respiratory arrest of woman during labour following administration of two types of analgesia; emergency caesarean section required
Clinical guideline availability and communication were contributory factors
RCA report completed. Clinical guideline more available and communication processes revised
Actions underway
Child suffered a seizure as a result of aminophylline toxicity
Root Cause Analysis underway. RCA Report awaited
While undergoing outpatient procedure child suffered respiratory arrest; recovered
Root Cause Analysis underway. RCA Report awaited
17
Canterbury DHB
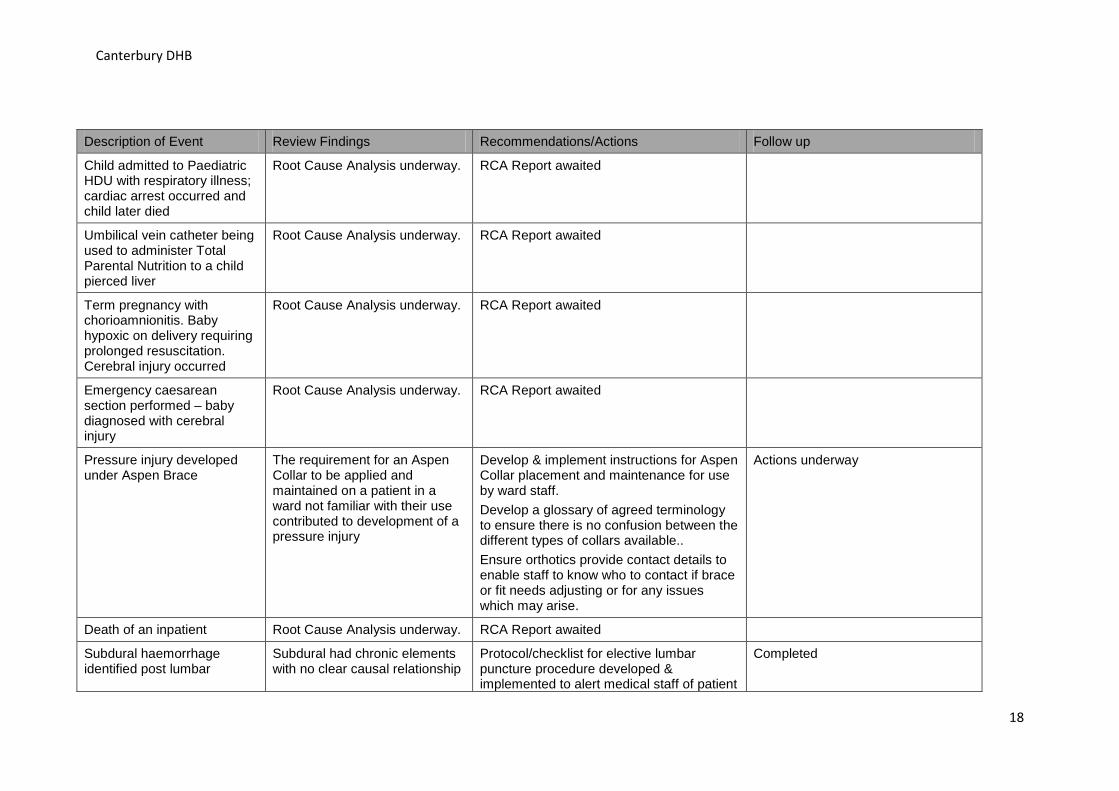
Description of Event Review Findings Recommendations/Actions Follow up
Child admitted to Paediatric HDU with respiratory illness; cardiac arrest occurred and child later died
Root Cause Analysis underway. RCA Report awaited
Umbilical vein catheter being used to administer Total Parental Nutrition to a child pierced liver
Root Cause Analysis underway. RCA Report awaited
Term pregnancy with chorioamnionitis. Baby hypoxic on delivery requiring prolonged resuscitation. Cerebral injury occurred
Root Cause Analysis underway. RCA Report awaited
Emergency caesarean section performed – baby diagnosed with cerebral injury
Root Cause Analysis underway. RCA Report awaited
Pressure injury developed under Aspen Brace
The requirement for an Aspen Collar to be applied and maintained on a patient in a ward not familiar with their use contributed to development of a pressure injury
Develop & implement instructions for Aspen Collar placement and maintenance for use by ward staff. Develop a glossary of agreed terminology to ensure there is no confusion between the different types of collars available.. Ensure orthotics provide contact details to enable staff to know who to contact if brace or fit needs adjusting or for any issues which may arise.
Actions underway
Death of an inpatient Root Cause Analysis underway. RCA Report awaited
Subdural haemorrhage identified post lumbar
Subdural had chronic elements with no clear causal relationship
Protocol/checklist for elective lumbar puncture procedure developed & implemented to alert medical staff of patient
Completed
18
Canterbury DHB
puncture procedure. to the lumbar puncture. contraindications.
19
Canterbury DHB
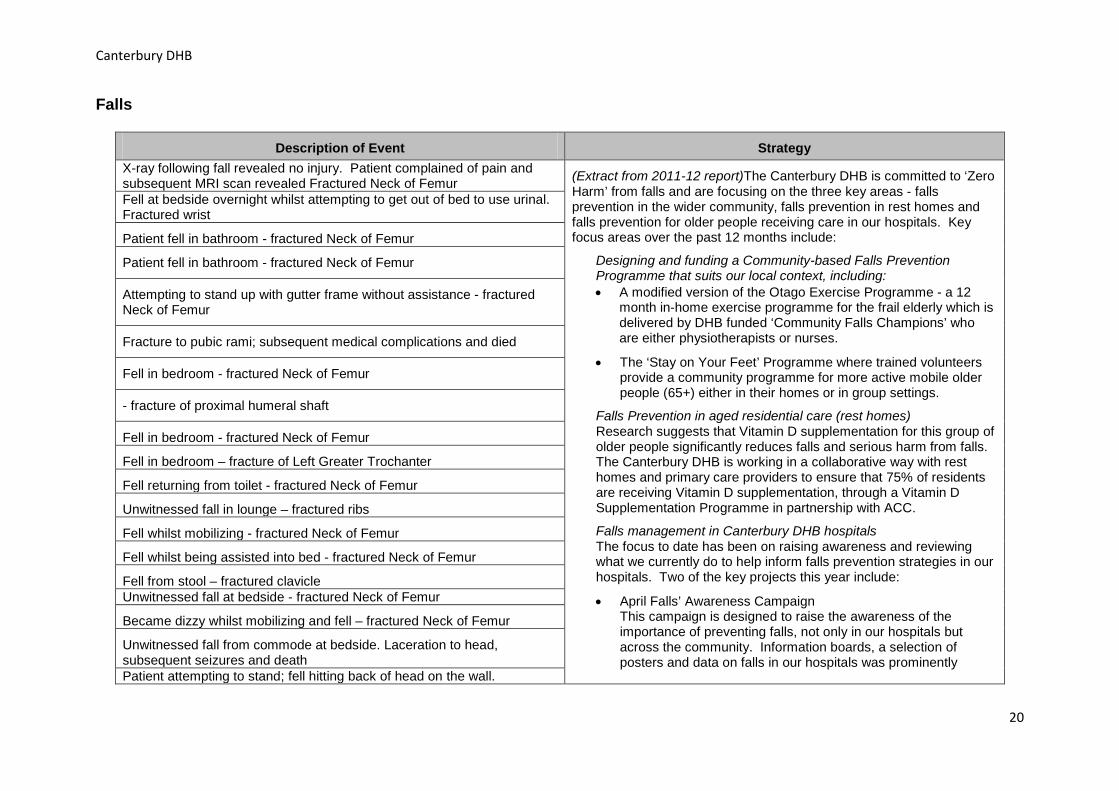
Falls
Description of Event Strategy X-ray following fall revealed no injury. Patient complained of pain and subsequent MRI scan revealed Fractured Neck of Femur (Extract from 2011-12 report)The Canterbury DHB is committed to ‘Zero
Harm’ from falls and are focusing on the three key areas - falls prevention in the wider community, falls prevention in rest homes and falls prevention for older people receiving care in our hospitals. Key focus areas over the past 12 months include:
Designing and funding a Community-based Falls Prevention Programme that suits our local context, including: • A modified version of the Otago Exercise Programme - a 12
month in-home exercise programme for the frail elderly which is delivered by DHB funded ‘Community Falls Champions’ who are either physiotherapists or nurses.
• The ‘Stay on Your Feet’ Programme where trained volunteers provide a community programme for more active mobile older people (65+) either in their homes or in group settings.
Falls Prevention in aged residential care (rest homes) Research suggests that Vitamin D supplementation for this group of older people significantly reduces falls and serious harm from falls. The Canterbury DHB is working in a collaborative way with rest homes and primary care providers to ensure that 75% of residents are receiving Vitamin D supplementation, through a Vitamin D Supplementation Programme in partnership with ACC.
Falls management in Canterbury DHB hospitals The focus to date has been on raising awareness and reviewing what we currently do to help inform falls prevention strategies in our hospitals. Two of the key projects this year include:
• April Falls’ Awareness Campaign This campaign is designed to raise the awareness of the importance of preventing falls, not only in our hospitals but across the community. Information boards, a selection of posters and data on falls in our hospitals was prominently
Fell at bedside overnight whilst attempting to get out of bed to use urinal. Fractured wrist
Patient fell in bathroom - fractured Neck of Femur
Patient fell in bathroom - fractured Neck of Femur
Attempting to stand up with gutter frame without assistance - fractured Neck of Femur
Fracture to pubic rami; subsequent medical complications and died
Fell in bedroom - fractured Neck of Femur
- fracture of proximal humeral shaft
Fell in bedroom - fractured Neck of Femur
Fell in bedroom – fracture of Left Greater Trochanter
Fell returning from toilet - fractured Neck of Femur
Unwitnessed fall in lounge – fractured ribs
Fell whilst mobilizing - fractured Neck of Femur
Fell whilst being assisted into bed - fractured Neck of Femur
Fell from stool – fractured clavicle Unwitnessed fall at bedside - fractured Neck of Femur
Became dizzy whilst mobilizing and fell – fractured Neck of Femur
Unwitnessed fall from commode at bedside. Laceration to head, subsequent seizures and death Patient attempting to stand; fell hitting back of head on the wall.
20
Canterbury DHB
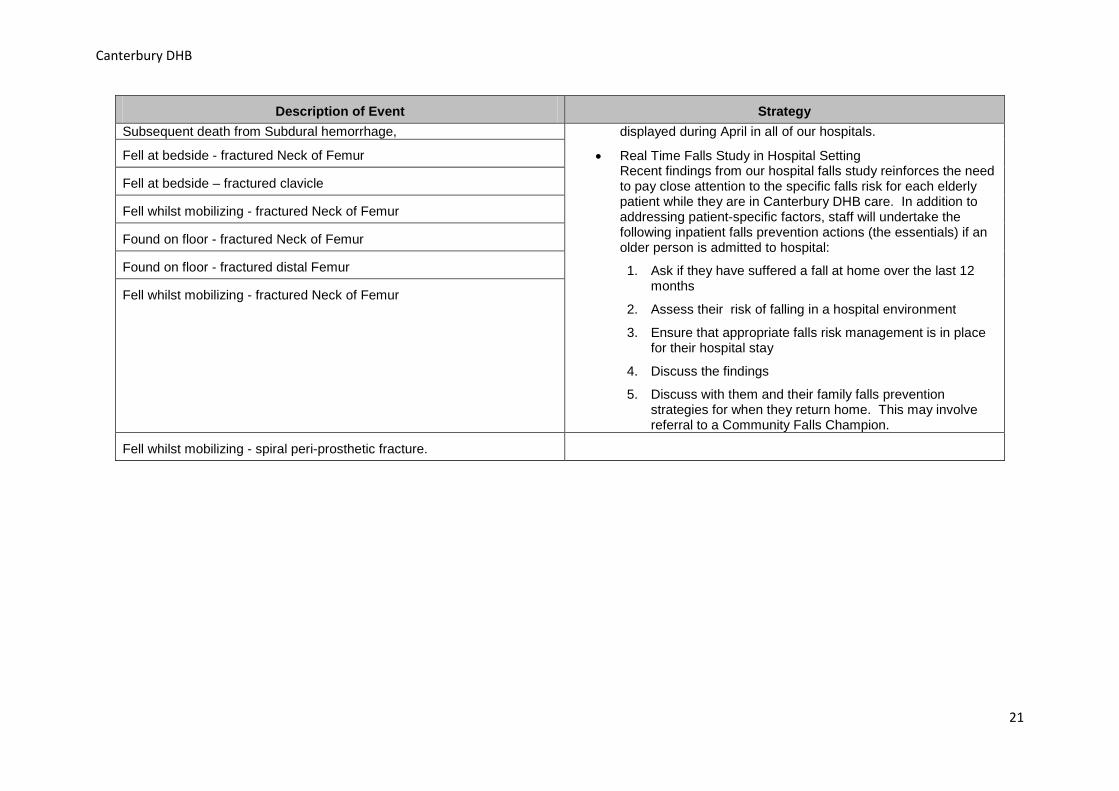
Description of Event Strategy Subsequent death from Subdural hemorrhage, displayed during April in all of our hospitals.
• Real Time Falls Study in Hospital Setting Recent findings from our hospital falls study reinforces the need to pay close attention to the specific falls risk for each elderly patient while they are in Canterbury DHB care. In addition to addressing patient-specific factors, staff will undertake the following inpatient falls prevention actions (the essentials) if an older person is admitted to hospital:
1. Ask if they have suffered a fall at home over the last 12 months
2. Assess their risk of falling in a hospital environment
3. Ensure that appropriate falls risk management is in place for their hospital stay
4. Discuss the findings
5. Discuss with them and their family falls prevention strategies for when they return home. This may involve referral to a Community Falls Champion.
Fell at bedside - fractured Neck of Femur
Fell at bedside – fractured clavicle
Fell whilst mobilizing - fractured Neck of Femur
Found on floor - fractured Neck of Femur
Found on floor - fractured distal Femur
Fell whilst mobilizing - fractured Neck of Femur
Fell whilst mobilizing - spiral peri-prosthetic fracture.
21
Counties Manukau DHB
Counties Manukau District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.countiesmanukau.health.nz/
Introduction
This report is released in conjunction with the Health Quality & Safety Commission (HQSC) National Report on Serious and Sentinel Events.
http://www.hqsc.govt.nz/our-programmes/reportable-events/serious-and-sentinel-event-reports/
In the 2012-2013 year Counties Manukau Health (CMH) reported forty five events that have caused serious harm or death. Thirty three of these events related to falls.
Because of the complex nature of health care, adverse events causing serious unintended harm to patients do occur and are truly regrettable. In reviewing each of these events, the focus is always on what we can learn and how we can improve care to prevent the likelihood of a similar event recurring.
What is a serious adverse event?
A serious adverse event has resulted in serious lasting disability or death, not related to the natural course of the patient’s illness or underlying condition.
As part of Counties Manukau Health’s commitment to providing safer care for patients, we have in place a process for reviewing serious adverse events that occur in our organisation. The purpose of reviewing these is to determine the underlying causes of the event so that improvements can be made to the systems of care to reduce the likelihood of such events occurring again.
Serious adverse event reviews at CMH are undertaken according to the following principles:
• Establish the facts: what happened, to whom, when, where, how and why • To look for improvements in the system of care rather than apportion blame to individuals • To establish how recurrence may be reduced or eliminated • To formulate recommendations and an action plan • To provide a report as a record of the review process
• To provide a means of sharing learning from the incident
22
Counties Manukau DHB
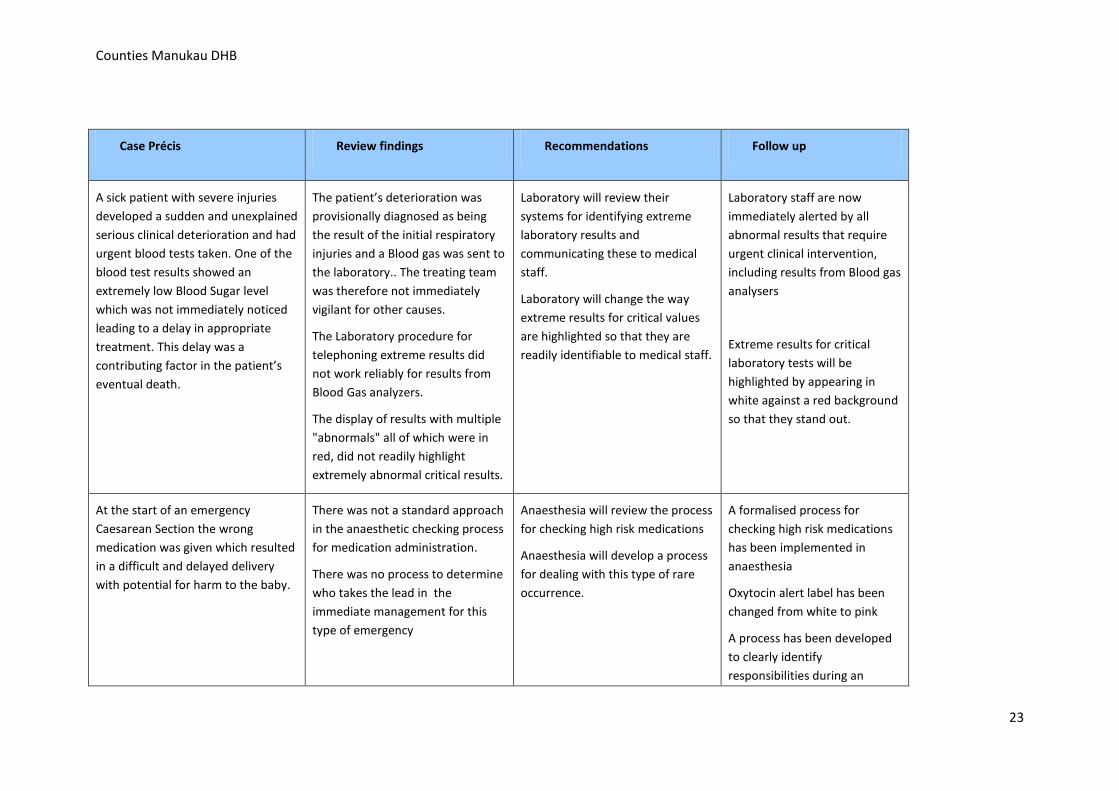
Case Précis Review findings Recommendations Follow up
A sick patient with severe injuries developed a sudden and unexplained serious clinical deterioration and had urgent blood tests taken. One of the blood test results showed an extremely low Blood Sugar level which was not immediately noticed leading to a delay in appropriate treatment. This delay was a contributing factor in the patient’s eventual death.
The patient’s deterioration was provisionally diagnosed as being the result of the initial respiratory injuries and a Blood gas was sent to the laboratory.. The treating team was therefore not immediately vigilant for other causes.
The Laboratory procedure for telephoning extreme results did not work reliably for results from Blood Gas analyzers.
The display of results with multiple "abnormals" all of which were in red, did not readily highlight extremely abnormal critical results.
Laboratory will review their systems for identifying extreme laboratory results and communicating these to medical staff.
Laboratory will change the way extreme results for critical values are highlighted so that they are readily identifiable to medical staff.
Laboratory staff are now immediately alerted by all abnormal results that require urgent clinical intervention, including results from Blood gas analysers
Extreme results for critical laboratory tests will be highlighted by appearing in white against a red background so that they stand out.
At the start of an emergency Caesarean Section the wrong medication was given which resulted in a difficult and delayed delivery with potential for harm to the baby.
There was not a standard approach in the anaesthetic checking process for medication administration.
There was no process to determine who takes the lead in the immediate management for this type of emergency
Anaesthesia will review the process for checking high risk medications
Anaesthesia will develop a process for dealing with this type of rare occurrence.
A formalised process for checking high risk medications has been implemented in anaesthesia
Oxytocin alert label has been changed from white to pink
A process has been developed to clearly identify responsibilities during an
23
Counties Manukau DHB
emergency
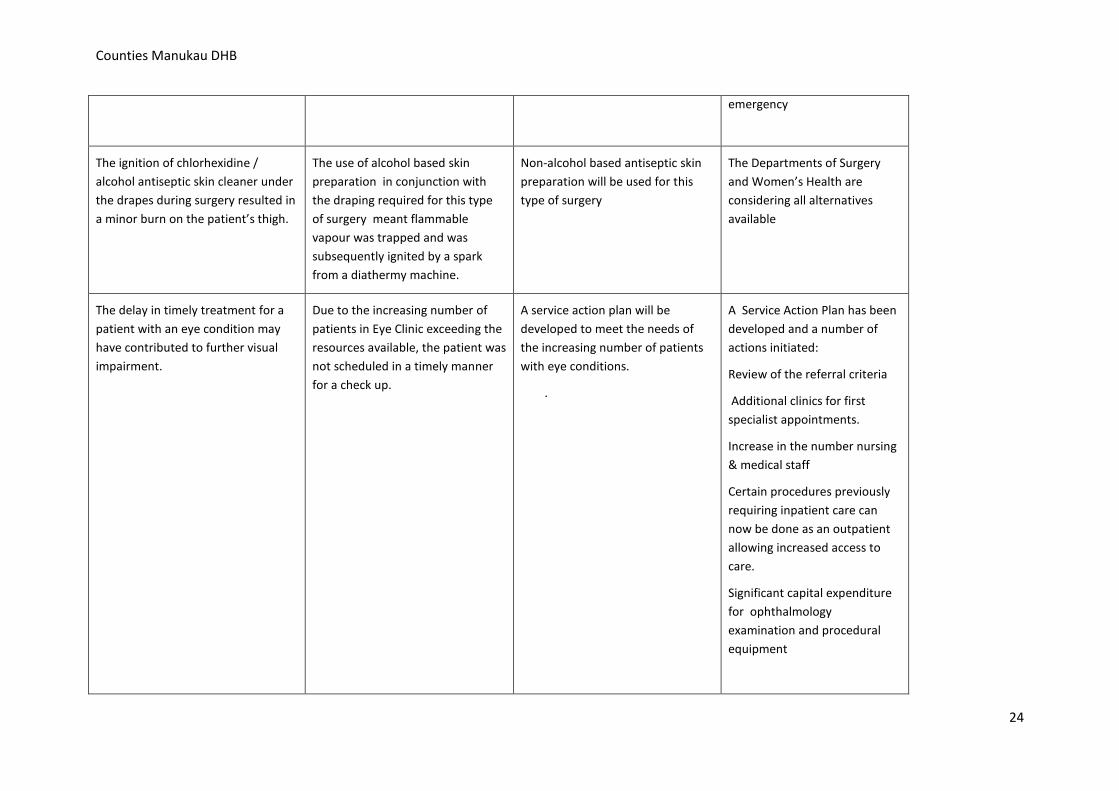
The ignition of chlorhexidine / alcohol antiseptic skin cleaner under the drapes during surgery resulted in a minor burn on the patient’s thigh.
The use of alcohol based skin preparation in conjunction with the draping required for this type of surgery meant flammable vapour was trapped and was subsequently ignited by a spark from a diathermy machine.
Non-alcohol based antiseptic skin preparation will be used for this type of surgery
The Departments of Surgery and Women’s Health are considering all alternatives available
The delay in timely treatment for a patient with an eye condition may have contributed to further visual impairment.
Due to the increasing number of patients in Eye Clinic exceeding the resources available, the patient was not scheduled in a timely manner for a check up.
A service action plan will be developed to meet the needs of the increasing number of patients with eye conditions.
.
A Service Action Plan has been developed and a number of actions initiated:
Review of the referral criteria
Additional clinics for first specialist appointments.
Increase in the number nursing & medical staff
Certain procedures previously requiring inpatient care can now be done as an outpatient allowing increased access to care.
Significant capital expenditure for ophthalmology examination and procedural equipment
24
Counties Manukau DHB
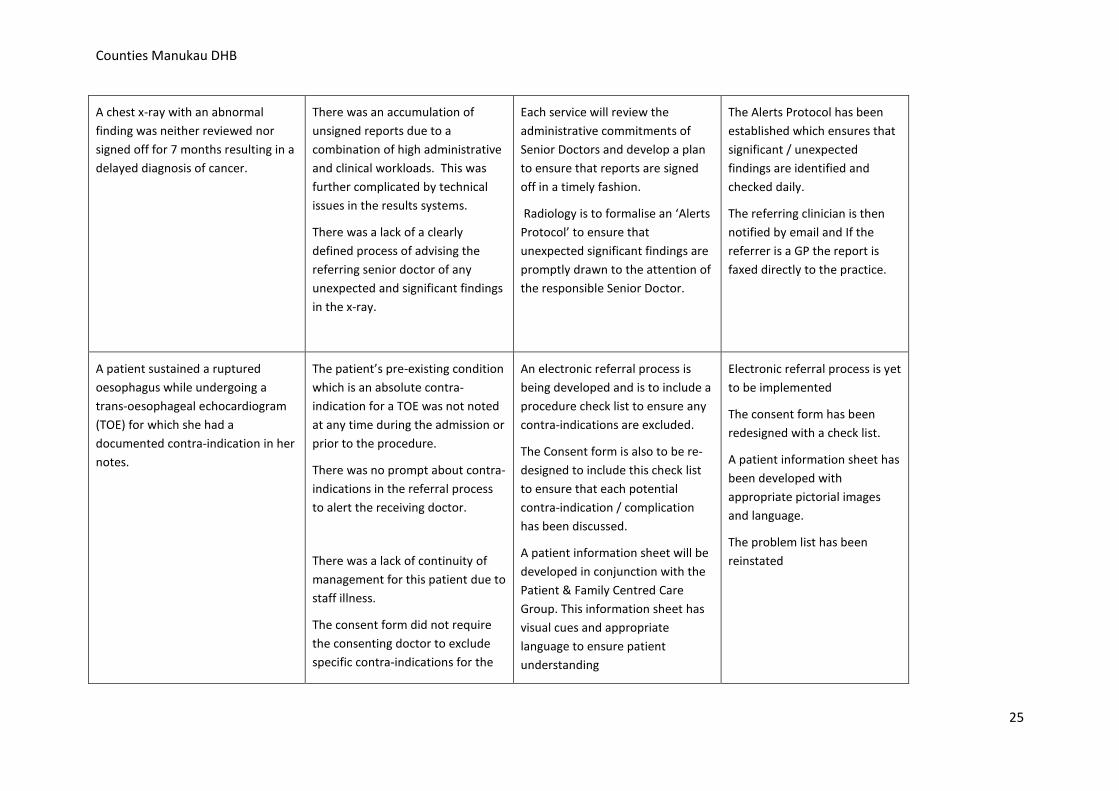
A chest x-ray with an abnormal finding was neither reviewed nor signed off for 7 months resulting in a delayed diagnosis of cancer.
There was an accumulation of unsigned reports due to a combination of high administrative and clinical workloads. This was further complicated by technical issues in the results systems.
There was a lack of a clearly defined process of advising the referring senior doctor of any unexpected and significant findings in the x-ray.
Each service will review the administrative commitments of Senior Doctors and develop a plan to ensure that reports are signed off in a timely fashion.
Radiology is to formalise an ‘Alerts Protocol’ to ensure that unexpected significant findings are promptly drawn to the attention of the responsible Senior Doctor.
The Alerts Protocol has been established which ensures that significant / unexpected findings are identified and checked daily.
The referring clinician is then notified by email and If the referrer is a GP the report is faxed directly to the practice.
A patient sustained a ruptured oesophagus while undergoing a trans-oesophageal echocardiogram (TOE) for which she had a documented contra-indication in her notes.
The patient’s pre-existing condition which is an absolute contra-indication for a TOE was not noted at any time during the admission or prior to the procedure.
There was no prompt about contra-indications in the referral process to alert the receiving doctor.
There was a lack of continuity of management for this patient due to staff illness.
The consent form did not require the consenting doctor to exclude specific contra-indications for the
An electronic referral process is being developed and is to include a procedure check list to ensure any contra-indications are excluded.
The Consent form is also to be re-designed to include this check list to ensure that each potential contra-indication / complication has been discussed.
A patient information sheet will be developed in conjunction with the Patient & Family Centred Care Group. This information sheet has visual cues and appropriate language to ensure patient understanding
Electronic referral process is yet to be implemented
The consent form has been redesigned with a check list.
A patient information sheet has been developed with appropriate pictorial images and language.
The problem list has been reinstated
25
Counties Manukau DHB
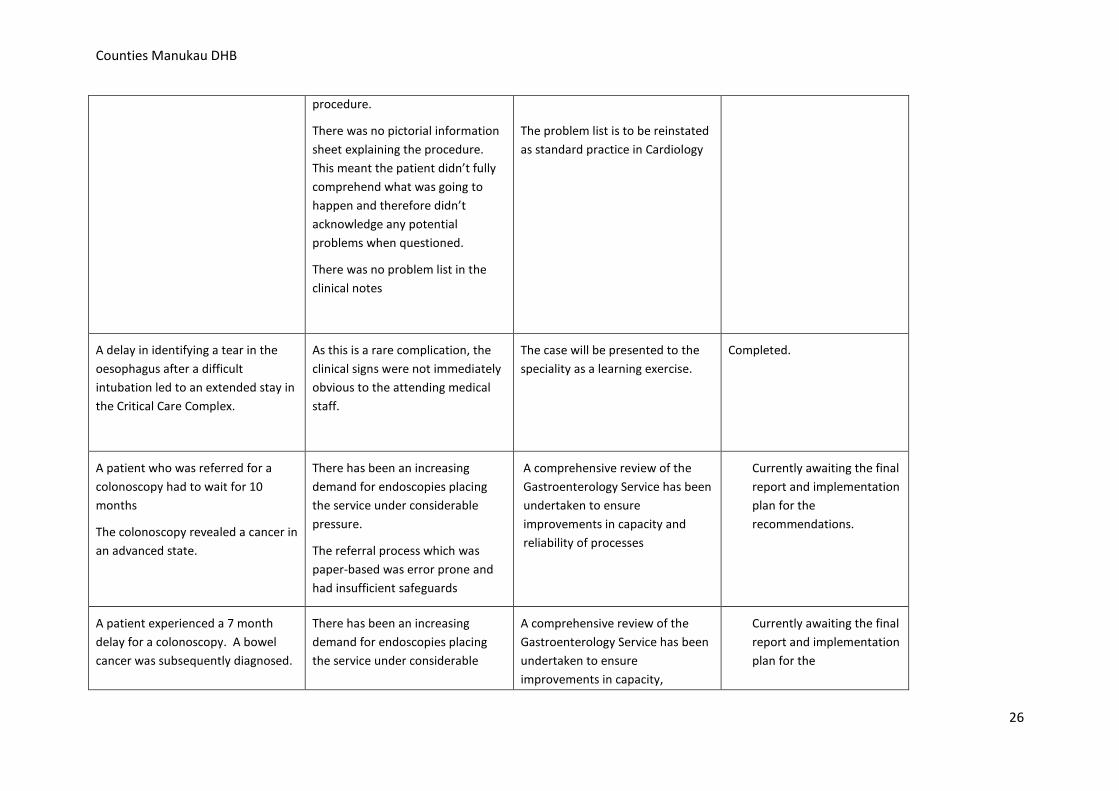
procedure.
There was no pictorial information sheet explaining the procedure. This meant the patient didn’t fully comprehend what was going to happen and therefore didn’t acknowledge any potential problems when questioned.
There was no problem list in the clinical notes
The problem list is to be reinstated as standard practice in Cardiology
A delay in identifying a tear in the oesophagus after a difficult intubation led to an extended stay in the Critical Care Complex.
As this is a rare complication, the clinical signs were not immediately obvious to the attending medical staff.
The case will be presented to the speciality as a learning exercise.
Completed.
A patient who was referred for a colonoscopy had to wait for 10 months
The colonoscopy revealed a cancer in an advanced state.
There has been an increasing demand for endoscopies placing the service under considerable pressure.
The referral process which was paper-based was error prone and had insufficient safeguards
A comprehensive review of the Gastroenterology Service has been undertaken to ensure improvements in capacity and reliability of processes
Currently awaiting the final report and implementation plan for the recommendations.
A patient experienced a 7 month delay for a colonoscopy. A bowel cancer was subsequently diagnosed.
There has been an increasing demand for endoscopies placing the service under considerable
A comprehensive review of the Gastroenterology Service has been undertaken to ensure improvements in capacity,
Currently awaiting the final report and implementation plan for the
26
Counties Manukau DHB
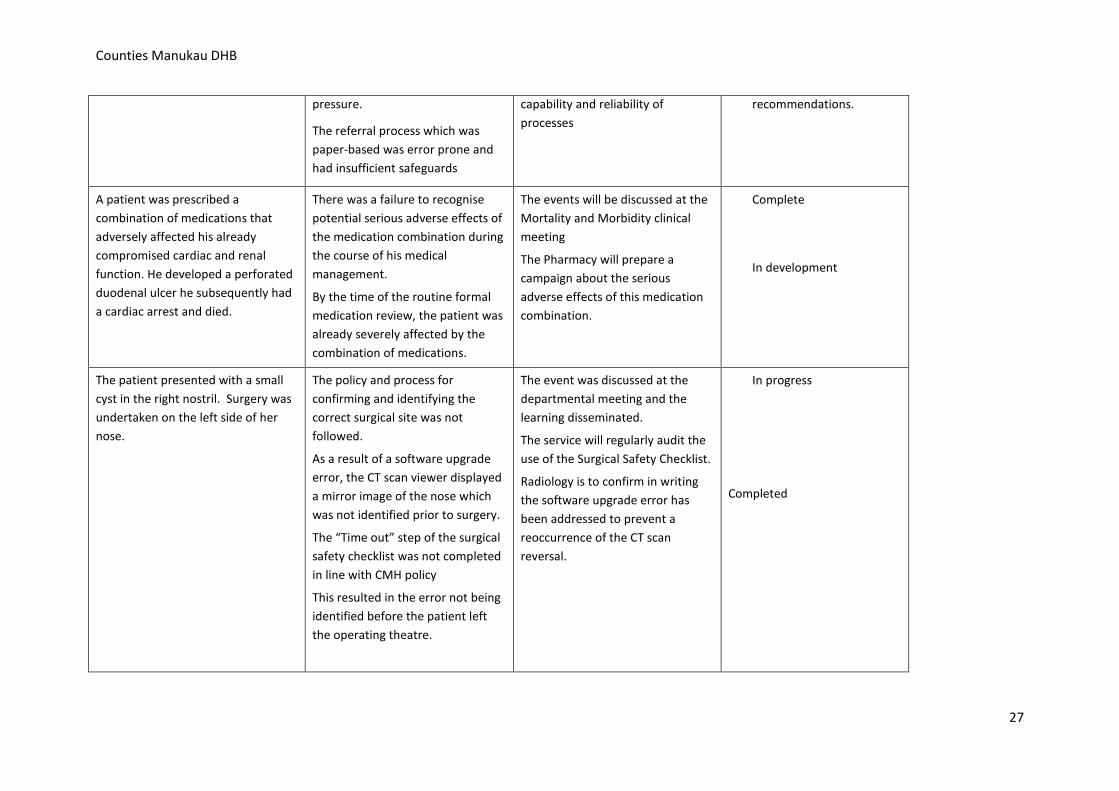
pressure.
The referral process which was paper-based was error prone and had insufficient safeguards
capability and reliability of processes
recommendations.
A patient was prescribed a combination of medications that adversely affected his already compromised cardiac and renal function. He developed a perforated duodenal ulcer he subsequently had a cardiac arrest and died.
There was a failure to recognise potential serious adverse effects of the medication combination during the course of his medical management.
By the time of the routine formal medication review, the patient was already severely affected by the combination of medications.
The events will be discussed at the Mortality and Morbidity clinical meeting
The Pharmacy will prepare a campaign about the serious adverse effects of this medication combination.
Complete
In development
The patient presented with a small cyst in the right nostril. Surgery was undertaken on the left side of her nose.
The policy and process for confirming and identifying the correct surgical site was not followed.
As a result of a software upgrade error, the CT scan viewer displayed a mirror image of the nose which was not identified prior to surgery.
The “Time out” step of the surgical safety checklist was not completed in line with CMH policy
This resulted in the error not being identified before the patient left the operating theatre.
The event was discussed at the departmental meeting and the learning disseminated.
The service will regularly audit the use of the Surgical Safety Checklist.
Radiology is to confirm in writing the software upgrade error has been addressed to prevent a reoccurrence of the CT scan reversal.
In progress
Completed
27
Counties Manukau DHB
A cotton swab was left in place in situ after an assisted delivery which resulted in an infection.
The routine formal swab count that occurred after the delivery was incorrect.
The formal count process will be reviewed.
A third level of checking the swabs has been instigated.
Summary of Falls causing patient harm
Of the 45 serious adverse events reported to the Health Quality & Safety Commission for the 2012-2013 year, thirty three were related to falls. In three of these events, the fall contributed to the patient’s death.
This year CMH has reported more falls than for the 2011-2012 year, however in this year’s total we have included six falls that resulted in lacerations that required sutures that would not have previously been reported.
The remaining falls which resulted in fractures included:
• five fractures involving the upper limb,
• five involving the spine, pelvis or ribs
• two involving the lower thigh or leg.
• 10 patients had a fractured hip - one of the patients died following surgery to repair the fracture.
• 5 patients had a cerebral haemorrhage - two of these died.
The Falls prevention programme is continuing with the following strategies to reduce the risk of serious harm from a fall. Over the next year the focus will be on testing and improving the reliability of the following interventions across the whole organisation:
• All patients to have a falls risk assessment completed within 6 hours of admission to the ward. • Ensuring appropriate interventions are put in place according to the assessed risk, including: • Provision of non-slip socks • Falls alert on room door • Frequent nurse rounds (up to hourly)
28
Counties Manukau DHB
• Nursed on low bed • Walking frames and other stability supports • Medication review to decrease use of medications likely to increase risk of falling • Hip-protectors • Ensuring every patient is reassessed regularly or when their condition changes • Developing an organisational clinical equipment management system that allows wards to quickly and efficiently access falls prevention equipment
(example alarms, Invisi-beams, high low beds as required by patients)
29
Hawke’s Bay DHB
Hawke’s Bay District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.hawkesbay.health.nz
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
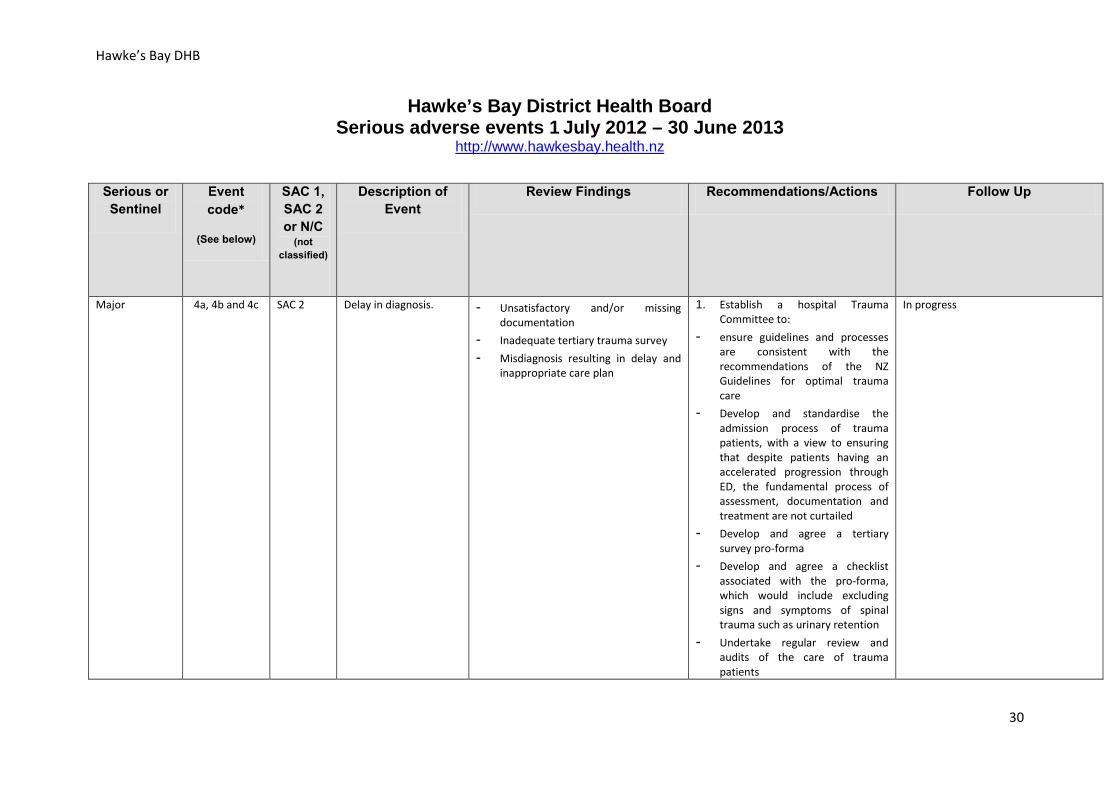
Major
4a, 4b and 4c SAC 2 Delay in diagnosis.
- Unsatisfactory and/or missing documentation
- Inadequate tertiary trauma survey - Misdiagnosis resulting in delay and
inappropriate care plan
1. Establish a hospital Trauma Committee to:
- ensure guidelines and processes are consistent with the recommendations of the NZ Guidelines for optimal trauma care
- Develop and standardise the admission process of trauma patients, with a view to ensuring that despite patients having an accelerated progression through ED, the fundamental process of assessment, documentation and treatment are not curtailed
- Develop and agree a tertiary survey pro-forma
- Develop and agree a checklist associated with the pro-forma, which would include excluding signs and symptoms of spinal trauma such as urinary retention
- Undertake regular review and audits of the care of trauma patients
In progress
30
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
- Oversee trauma training requirements for medical and nursing staff
2. Review the process for management of documents relating to patients transferring from ED to the inpatient wards.
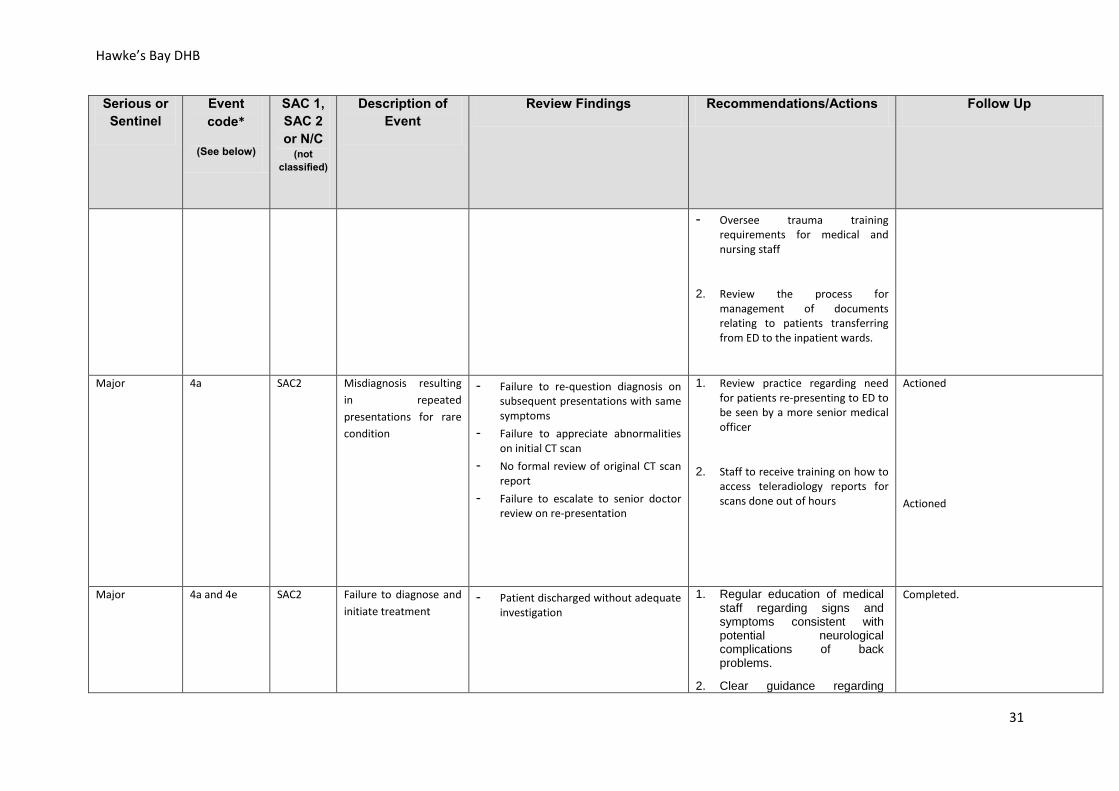
Major
4a SAC2 Misdiagnosis resulting in repeated presentations for rare condition
- Failure to re-question diagnosis on subsequent presentations with same symptoms
- Failure to appreciate abnormalities on initial CT scan
- No formal review of original CT scan report
- Failure to escalate to senior doctor review on re-presentation
1. Review practice regarding need for patients re-presenting to ED to be seen by a more senior medical officer
2. Staff to receive training on how to access teleradiology reports for scans done out of hours
Actioned
Actioned
Major
4a and 4e SAC2 Failure to diagnose and initiate treatment
- Patient discharged without adequate investigation
1. Regular education of medical staff regarding signs and symptoms consistent with potential neurological complications of back problems.
2. Clear guidance regarding
Completed.
31
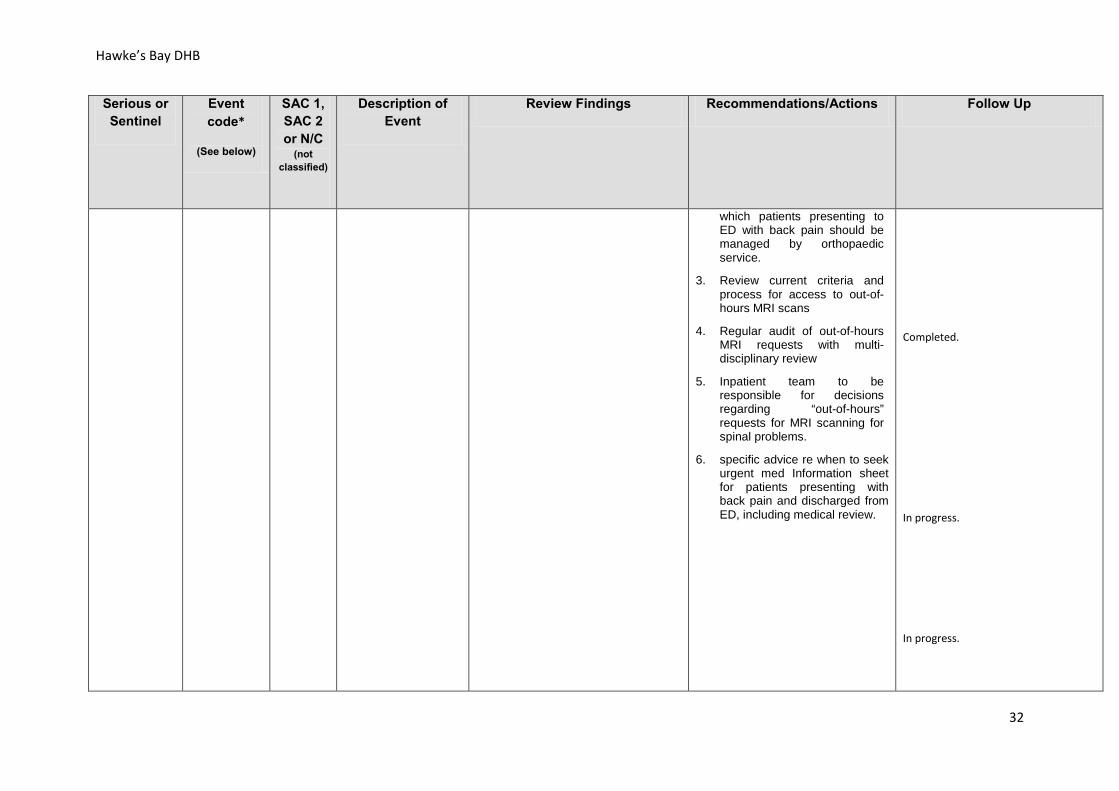
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
which patients presenting to ED with back pain should be managed by orthopaedic service.
3. Review current criteria and
process for access to out-of-hours MRI scans
4. Regular audit of out-of-hours
MRI requests with multi-disciplinary review
5. Inpatient team to be
responsible for decisions regarding “out-of-hours” requests for MRI scanning for spinal problems.
6. specific advice re when to seek
urgent med Information sheet for patients presenting with back pain and discharged from ED, including medical review.
Completed.
In progress.
In progress.
32
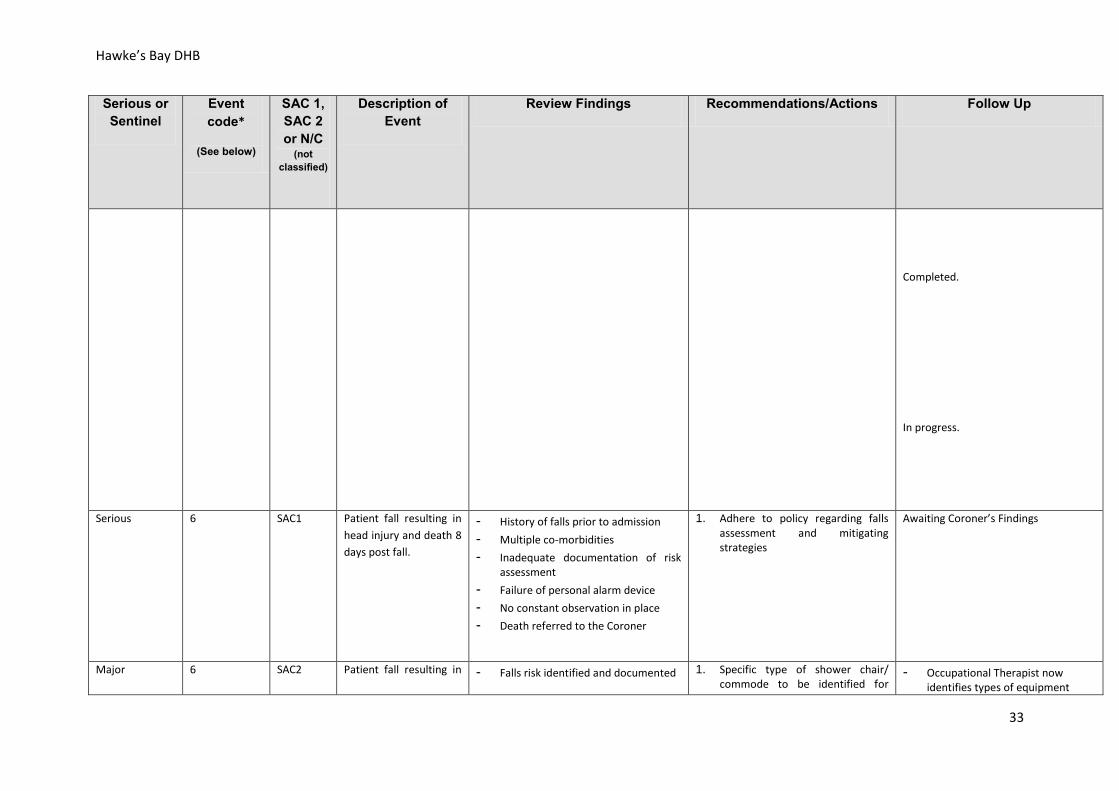
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
Completed.
In progress.
Serious
6 SAC1 Patient fall resulting in head injury and death 8 days post fall.
- History of falls prior to admission - Multiple co-morbidities - Inadequate documentation of risk
assessment - Failure of personal alarm device - No constant observation in place - Death referred to the Coroner
1. Adhere to policy regarding falls assessment and mitigating strategies
Awaiting Coroner’s Findings
Major 6 SAC2 Patient fall resulting in - Falls risk identified and documented 1. Specific type of shower chair/ commode to be identified for
- Occupational Therapist now identifies types of equipment
33
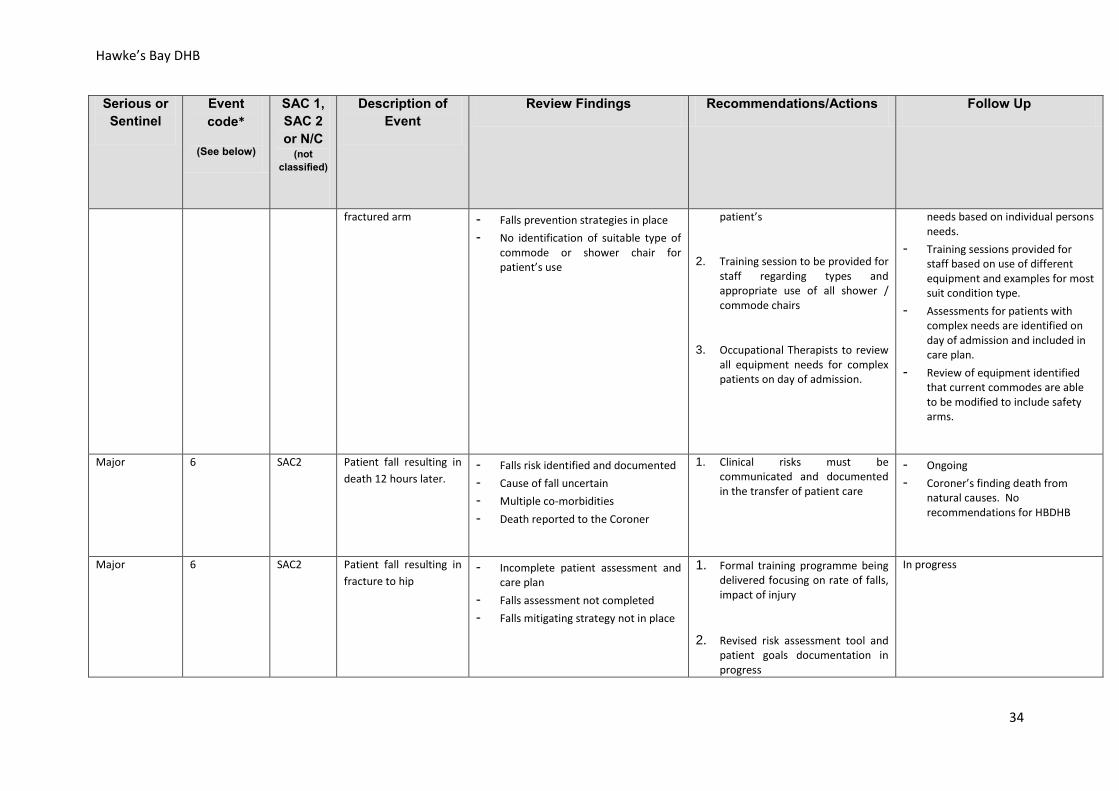
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
fractured arm - Falls prevention strategies in place - No identification of suitable type of
commode or shower chair for patient’s use
patient’s
2. Training session to be provided for staff regarding types and appropriate use of all shower / commode chairs
3. Occupational Therapists to review all equipment needs for complex patients on day of admission.
needs based on individual persons needs.
- Training sessions provided for staff based on use of different equipment and examples for most suit condition type.
- Assessments for patients with complex needs are identified on day of admission and included in care plan.
- Review of equipment identified that current commodes are able to be modified to include safety arms.
Major
6 SAC2 Patient fall resulting in death 12 hours later.
- Falls risk identified and documented - Cause of fall uncertain - Multiple co-morbidities - Death reported to the Coroner
1. Clinical risks must be communicated and documented in the transfer of patient care
- Ongoing - Coroner’s finding death from
natural causes. No recommendations for HBDHB
Major
6 SAC2 Patient fall resulting in fracture to hip
- Incomplete patient assessment and care plan
- Falls assessment not completed - Falls mitigating strategy not in place
1. Formal training programme being delivered focusing on rate of falls, impact of injury
2. Revised risk assessment tool and patient goals documentation in progress
In progress
34
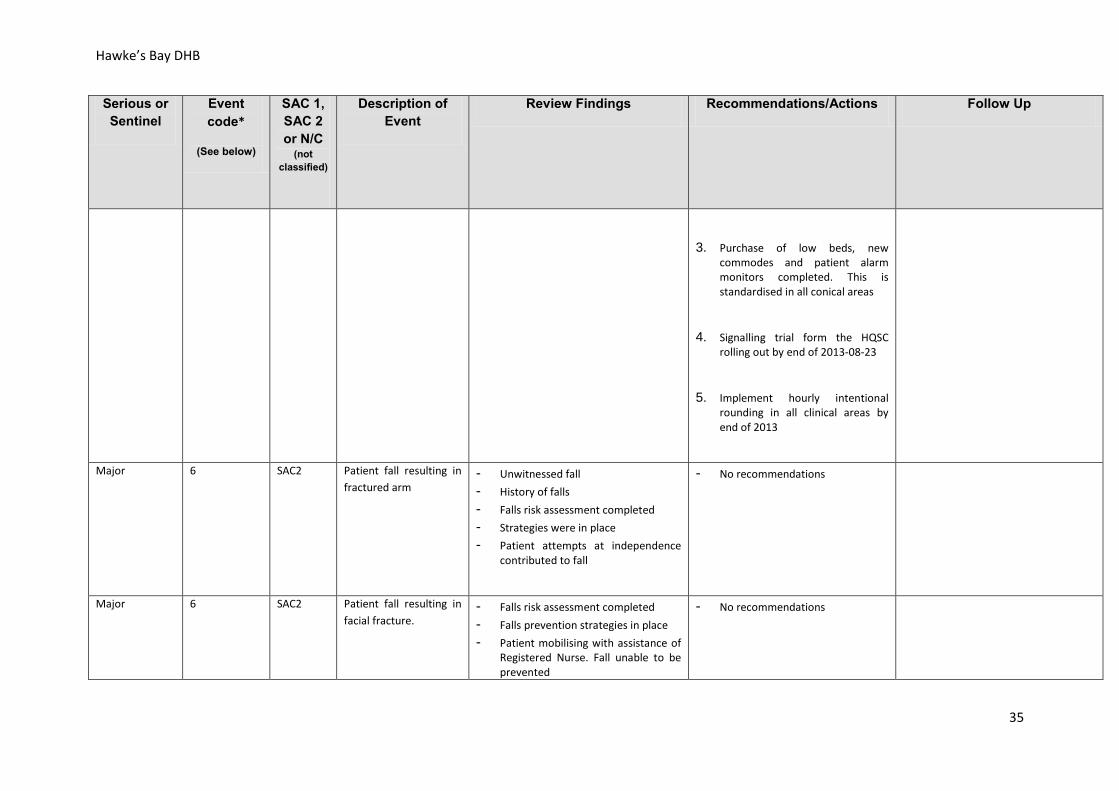
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
3. Purchase of low beds, new commodes and patient alarm monitors completed. This is standardised in all conical areas
4. Signalling trial form the HQSC rolling out by end of 2013-08-23
5. Implement hourly intentional rounding in all clinical areas by end of 2013
Major
6 SAC2 Patient fall resulting in fractured arm
- Unwitnessed fall - History of falls - Falls risk assessment completed - Strategies were in place - Patient attempts at independence
contributed to fall
- No recommendations
Major
6 SAC2 Patient fall resulting in facial fracture.
- Falls risk assessment completed - Falls prevention strategies in place - Patient mobilising with assistance of
Registered Nurse. Fall unable to be prevented
- No recommendations
35
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
- Fall likely to have been caused by increasing medical condition
- Multiple medical conditions
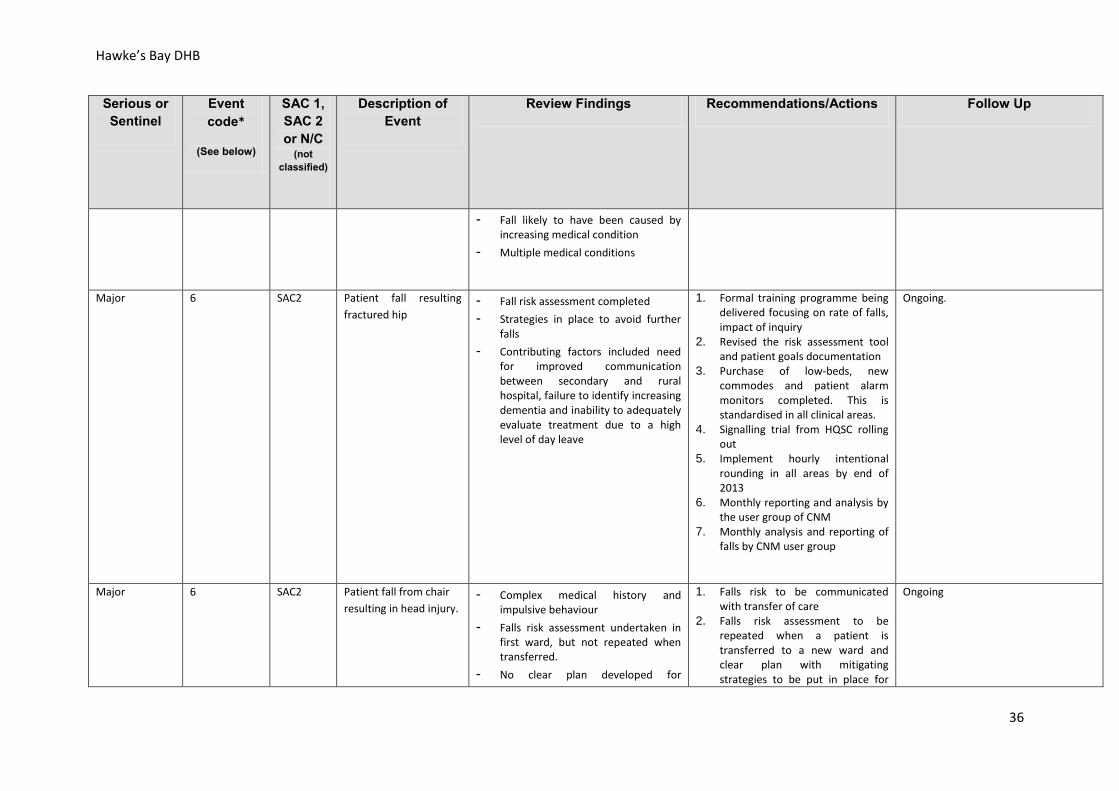
Major
6 SAC2 Patient fall resulting fractured hip
- Fall risk assessment completed - Strategies in place to avoid further
falls - Contributing factors included need
for improved communication between secondary and rural hospital, failure to identify increasing dementia and inability to adequately evaluate treatment due to a high level of day leave
1. Formal training programme being delivered focusing on rate of falls, impact of inquiry
2. Revised the risk assessment tool and patient goals documentation
3. Purchase of low-beds, new commodes and patient alarm monitors completed. This is standardised in all clinical areas.
4. Signalling trial from HQSC rolling out
5. Implement hourly intentional rounding in all areas by end of 2013
6. Monthly reporting and analysis by the user group of CNM
7. Monthly analysis and reporting of falls by CNM user group
Ongoing.
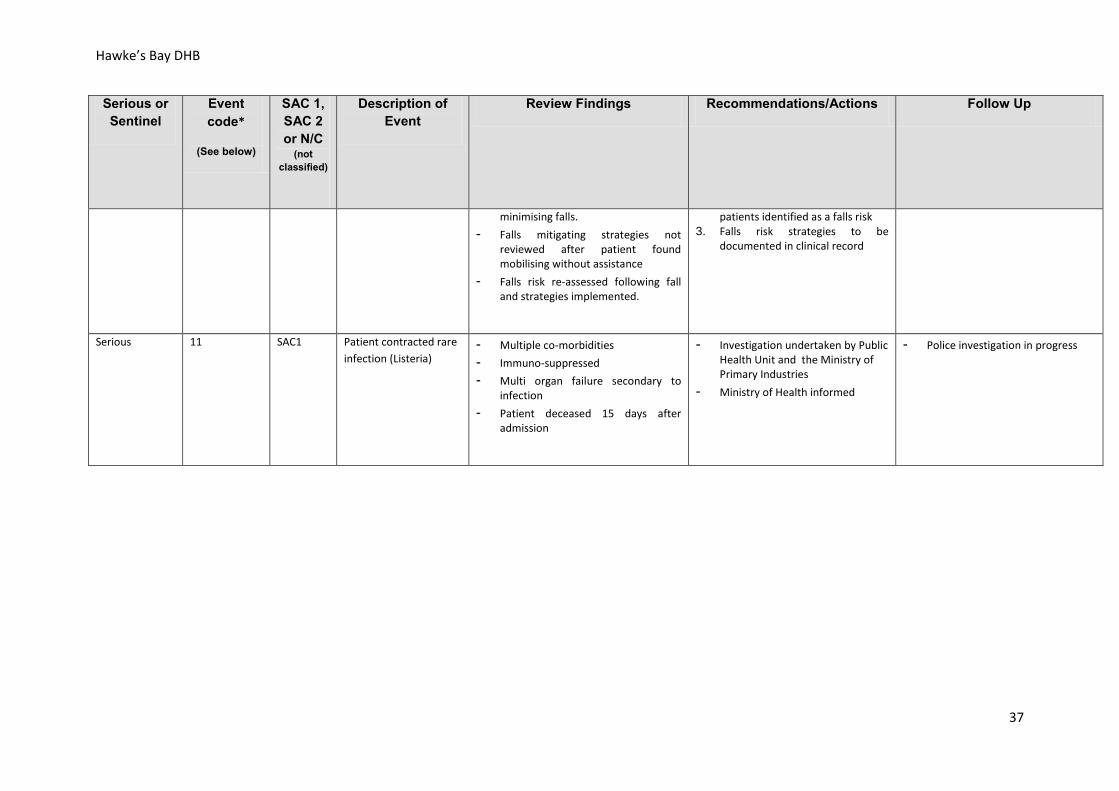
Major
6 SAC2 Patient fall from chair resulting in head injury.
- Complex medical history and impulsive behaviour
- Falls risk assessment undertaken in first ward, but not repeated when transferred.
- No clear plan developed for
1. Falls risk to be communicated with transfer of care
2. Falls risk assessment to be repeated when a patient is transferred to a new ward and clear plan with mitigating strategies to be put in place for
Ongoing
36
Hawke’s Bay DHB
Serious or Sentinel
Event code*
(See below)
SAC 1, SAC 2 or N/C
(not classified)
Description of Event
Review Findings Recommendations/Actions Follow Up
minimising falls. - Falls mitigating strategies not
reviewed after patient found mobilising without assistance
- Falls risk re-assessed following fall and strategies implemented.
patients identified as a falls risk 3. Falls risk strategies to be
documented in clinical record
Serious 11 SAC1 Patient contracted rare infection (Listeria)
- Multiple co-morbidities - Immuno-suppressed - Multi organ failure secondary to
infection - Patient deceased 15 days after
admission
- Investigation undertaken by Public Health Unit and the Ministry of Primary Industries
- Ministry of Health informed
- Police investigation in progress
37
Wairarapa, Hutt Valley and Capital and Coast DHBs
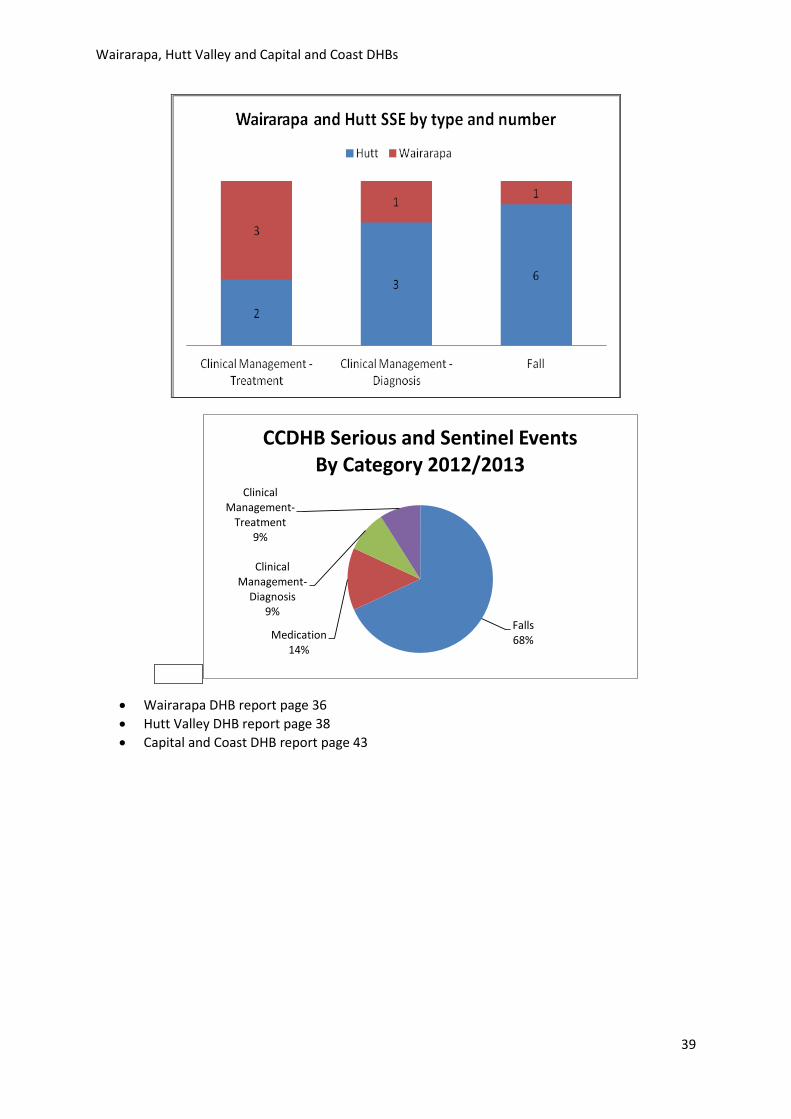
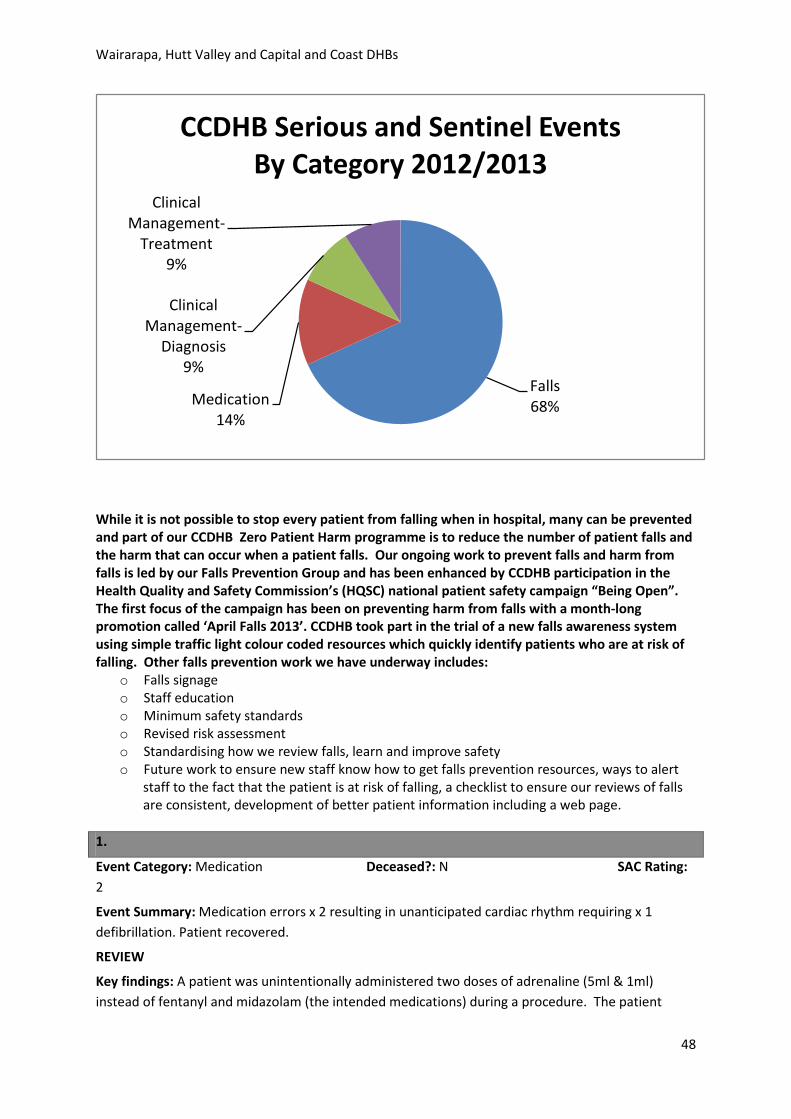
Wairarapa, Hutt Valley and Capital & Coast District Health Boards Serious and Sentinel Events Report: 2012 -2013 Wairarapa and Hutt Valley DHBs have reported 16 serious and sentinel events (SSEs) and Capital & Coast District Health Board (CCDHB) has reported 22. These SSEs occurred in our hospitals and health services during the period 1 July 2012 to 30 June 2013. These SSEs were reported to the Health Quality and Safety Commission as per national Reportable Events policy requirements and include one joint DHB community pharmacy event.
Each of the reported SSE events involves a patient suffering harm or death while in our care.
We consider one event is one too many, and apologise unreservedly to the patients and families involved. We acknowledge the distress and grief that result when things go wrong in healthcare.
We always seek to learn from these incidents and improve safety. We can’t do this if we don’t know about them happening. A strong safety culture means that patients and their families, other health providers like family doctors, primary health nurses, and our own staff tell us when an incident has occurred and raise concerns so that we can look into what happened.
Continually strengthening our culture of patient safety and quality is a top priority for the three DHBs. We are committed to working with patients and families when things go wrong to ensure that their concerns and needs are addressed and supported, and that they are included in the process of the review.
Our practice is to communicate openly with patients and families at all times including when adverse events occur, to acknowledge what has happened and to apologise where we have got things wrong. We will listen to concerns, provide support, involve patients and families to the degree they prefer, and where possible answer their questions and address any concerns that they have.
When reviews result in recommendations for changes and action, we ensure that these are followed up and implemented. In this way we aim to achieve both:
• The CCDHB goal of Zero Patient Harm, which forms part of our overall quality improvement and patient safety programme of work, and
• The Wairarapa and Hutt Valley strategic quality direction, our three objectives being:
• Improving the Healthcare Experience • Improving Healthcare Outcomes (effectiveness) • Improving Healthcare Safety
38
Wairarapa, Hutt Valley and Capital and Coast DHBs
Falls68%Medication
14%
Clinical Management-
Diagnosis9%
Clinical Management-
Treatment9%
CCDHB Serious and Sentinel EventsBy Category 2012/2013
• Wairarapa DHB report page 36 • Hutt Valley DHB report page 38 • Capital and Coast DHB report page 43
39
Wairarapa, Hutt Valley and Capital and Coast DHBs
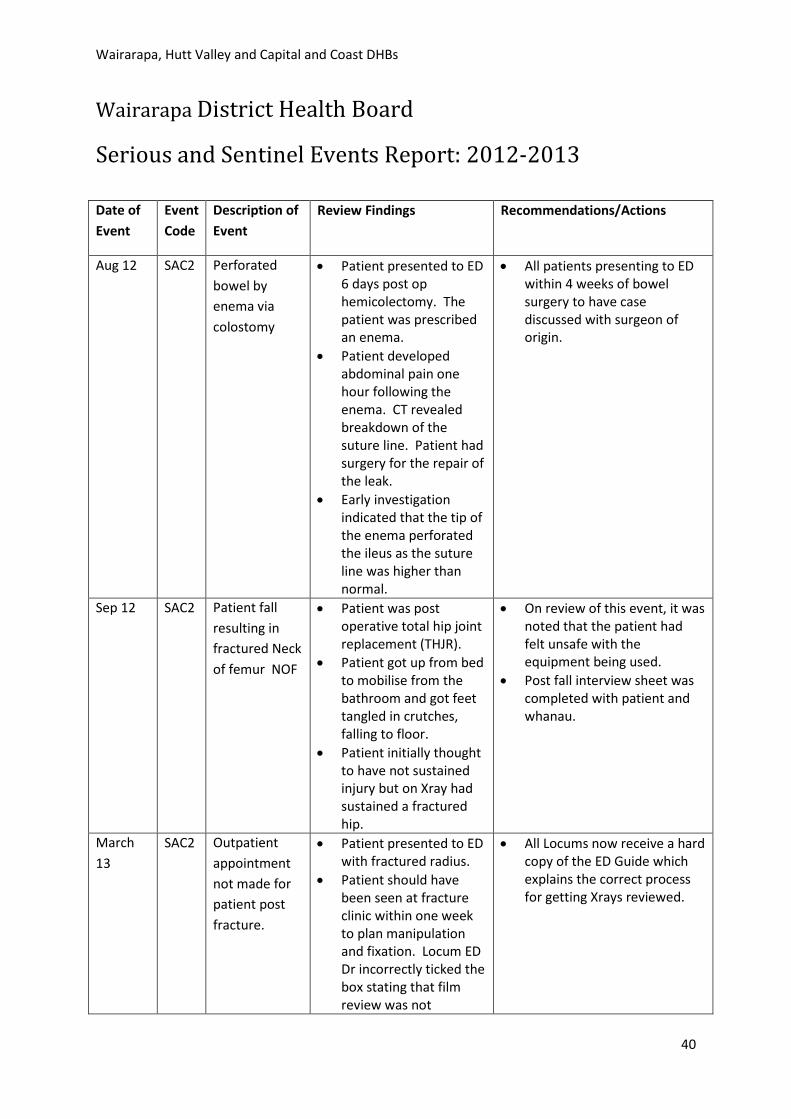
Wairarapa District Health Board
Serious and Sentinel Events Report: 2012-2013
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
Aug 12 SAC2 Perforated bowel by enema via colostomy
• Patient presented to ED 6 days post op hemicolectomy. The patient was prescribed an enema.
• Patient developed abdominal pain one hour following the enema. CT revealed breakdown of the suture line. Patient had surgery for the repair of the leak.
• Early investigation indicated that the tip of the enema perforated the ileus as the suture line was higher than normal.
• All patients presenting to ED within 4 weeks of bowel surgery to have case discussed with surgeon of origin.
Sep 12 SAC2 Patient fall resulting in fractured Neck of femur NOF
• Patient was post operative total hip joint replacement (THJR).
• Patient got up from bed to mobilise from the bathroom and got feet tangled in crutches, falling to floor.
• Patient initially thought to have not sustained injury but on Xray had sustained a fractured hip.
• On review of this event, it was noted that the patient had felt unsafe with the equipment being used.
• Post fall interview sheet was completed with patient and whanau.
March 13
SAC2 Outpatient appointment not made for patient post fracture.
• Patient presented to ED with fractured radius.
• Patient should have been seen at fracture clinic within one week to plan manipulation and fixation. Locum ED Dr incorrectly ticked the box stating that film review was not
• All Locums now receive a hard copy of the ED Guide which explains the correct process for getting Xrays reviewed.
40
Wairarapa, Hutt Valley and Capital and Coast DHBs
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
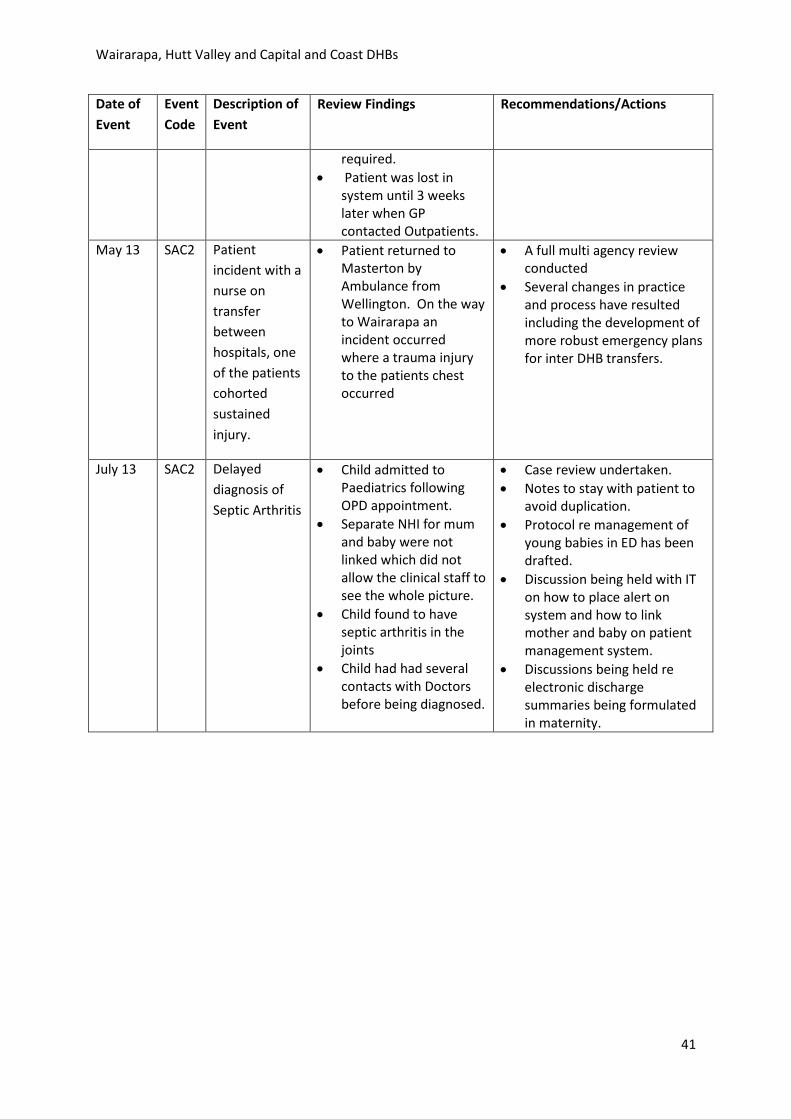
required. • Patient was lost in
system until 3 weeks later when GP contacted Outpatients.
May 13 SAC2 Patient incident with a nurse on transfer between hospitals, one of the patients cohorted sustained injury.
• Patient returned to Masterton by Ambulance from Wellington. On the way to Wairarapa an incident occurred where a trauma injury to the patients chest occurred
• A full multi agency review conducted
• Several changes in practice and process have resulted including the development of more robust emergency plans for inter DHB transfers.
July 13 SAC2 Delayed diagnosis of Septic Arthritis
• Child admitted to Paediatrics following OPD appointment.
• Separate NHI for mum and baby were not linked which did not allow the clinical staff to see the whole picture.
• Child found to have septic arthritis in the joints
• Child had had several contacts with Doctors before being diagnosed.
• Case review undertaken. • Notes to stay with patient to
avoid duplication. • Protocol re management of
young babies in ED has been drafted.
• Discussion being held with IT on how to place alert on system and how to link mother and baby on patient management system.
• Discussions being held re electronic discharge summaries being formulated in maternity.
41
Wairarapa, Hutt Valley and Capital and Coast DHBs
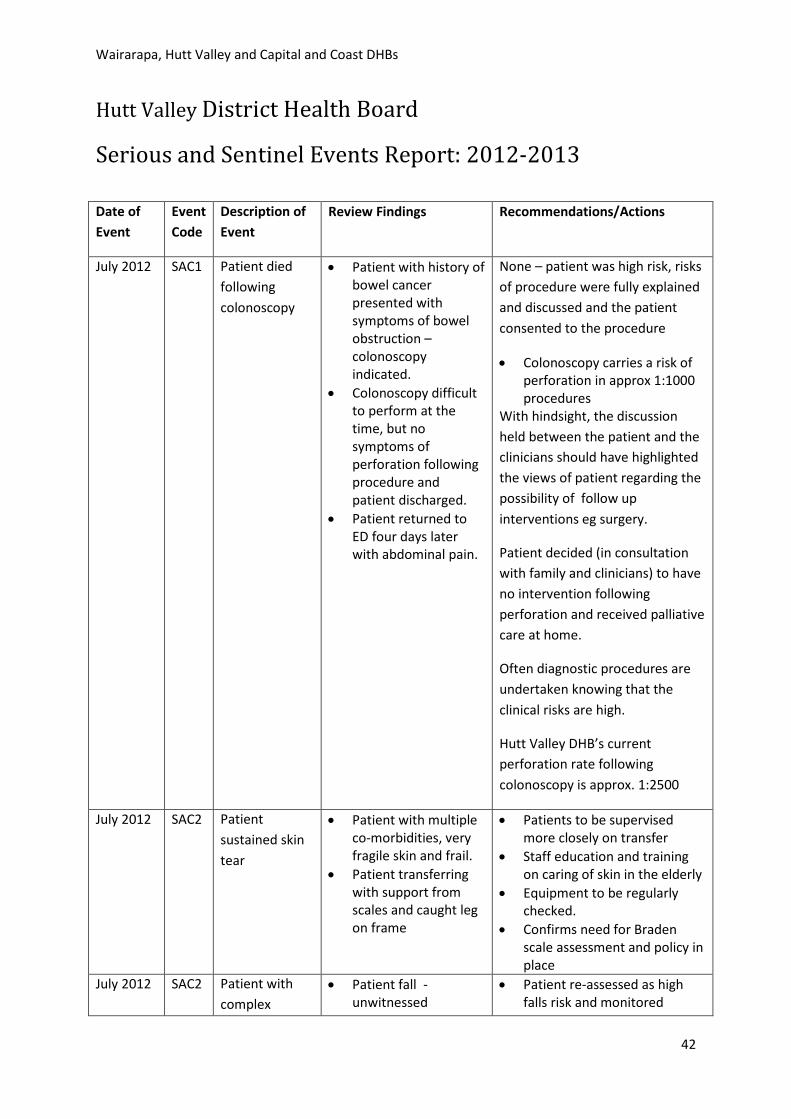
Hutt Valley District Health Board
Serious and Sentinel Events Report: 2012-2013
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
July 2012 SAC1 Patient died following colonoscopy
• Patient with history of bowel cancer presented with symptoms of bowel obstruction – colonoscopy indicated.
• Colonoscopy difficult to perform at the time, but no symptoms of perforation following procedure and patient discharged.
• Patient returned to ED four days later with abdominal pain.
None – patient was high risk, risks of procedure were fully explained and discussed and the patient consented to the procedure
• Colonoscopy carries a risk of perforation in approx 1:1000 procedures
With hindsight, the discussion held between the patient and the clinicians should have highlighted the views of patient regarding the possibility of follow up interventions eg surgery.
Patient decided (in consultation with family and clinicians) to have no intervention following perforation and received palliative care at home.
Often diagnostic procedures are undertaken knowing that the clinical risks are high.
Hutt Valley DHB’s current perforation rate following colonoscopy is approx. 1:2500
July 2012 SAC2 Patient sustained skin tear
• Patient with multiple co-morbidities, very fragile skin and frail.
• Patient transferring with support from scales and caught leg on frame
• Patients to be supervised more closely on transfer
• Staff education and training on caring of skin in the elderly
• Equipment to be regularly checked.
• Confirms need for Braden scale assessment and policy in place
July 2012 SAC2 Patient with complex
• Patient fall - unwitnessed
• Patient re-assessed as high falls risk and monitored
42
Wairarapa, Hutt Valley and Capital and Coast DHBs
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
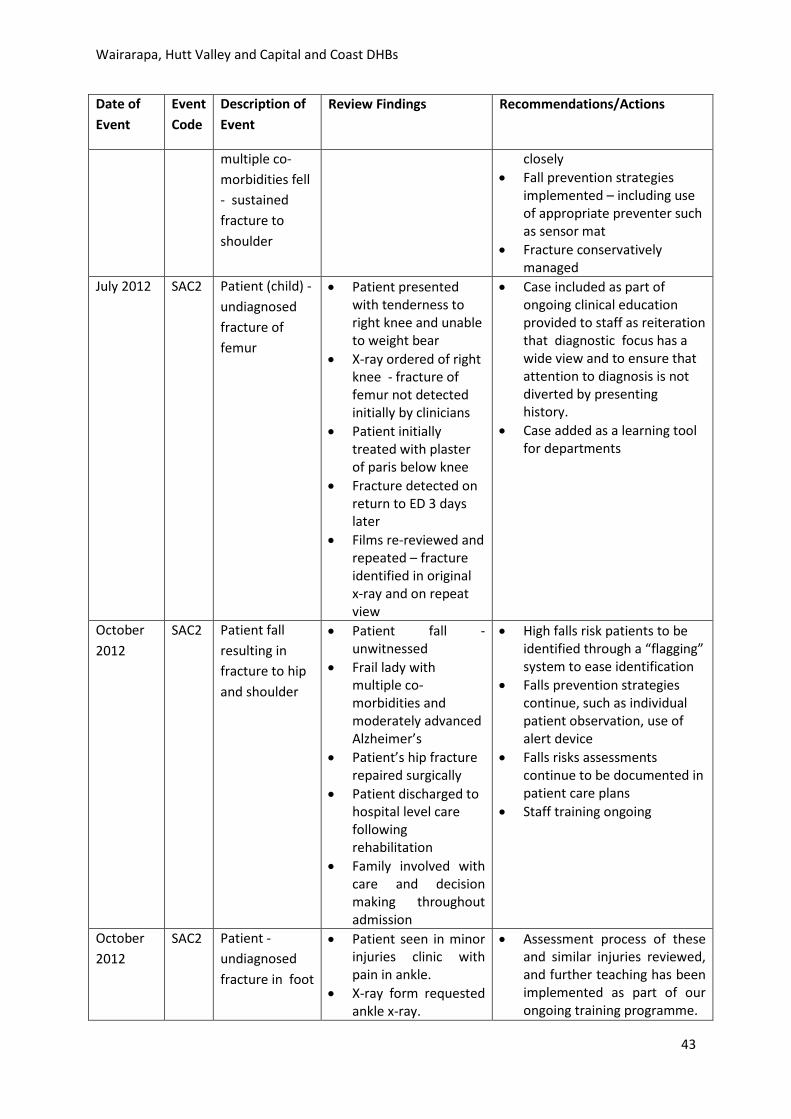
multiple co-morbidities fell - sustained fracture to shoulder
closely • Fall prevention strategies
implemented – including use of appropriate preventer such as sensor mat
• Fracture conservatively managed
July 2012 SAC2
Patient (child) - undiagnosed fracture of femur
• Patient presented with tenderness to right knee and unable to weight bear
• X-ray ordered of right knee - fracture of femur not detected initially by clinicians
• Patient initially treated with plaster of paris below knee
• Fracture detected on return to ED 3 days later
• Films re-reviewed and repeated – fracture identified in original x-ray and on repeat view
• Case included as part of ongoing clinical education provided to staff as reiteration that diagnostic focus has a wide view and to ensure that attention to diagnosis is not diverted by presenting history.
• Case added as a learning tool for departments
October 2012
SAC2 Patient fall resulting in fracture to hip and shoulder
• Patient fall - unwitnessed
• Frail lady with multiple co-morbidities and moderately advanced Alzheimer’s
• Patient’s hip fracture repaired surgically
• Patient discharged to hospital level care following rehabilitation
• Family involved with care and decision making throughout admission
• High falls risk patients to be identified through a “flagging” system to ease identification
• Falls prevention strategies continue, such as individual patient observation, use of alert device
• Falls risks assessments continue to be documented in patient care plans
• Staff training ongoing
October 2012
SAC2 Patient - undiagnosed fracture in foot
• Patient seen in minor injuries clinic with pain in ankle.
• X-ray form requested ankle x-ray.
• Assessment process of these and similar injuries reviewed, and further teaching has been implemented as part of our ongoing training programme.
43
Wairarapa, Hutt Valley and Capital and Coast DHBs
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
• Whilst in x-ray patient reported that pain was in her foot – due to communication breakdown between staff this was not reported back to ED and was not followed up. Patient discharged – diagnosis ankle sprain.
• Patient attended GP one week later was x-rayed privately - fracture of foot identified.
• Original x-ray reviewed and fracture present – This fracture was not picked up by the Clinical Nurse Specialist at the time, or the radiologist on reviewing the films the next day.
• Breakdown in the passing on of information has now been addressed between the Emergency Department and Radiology staff so that information is now passed on appropriately; if patients identify problems other than those initially identified on the X-Ray form, the radiology staff will contact the requestor to clarify.
• Missed identification of fracture – the advent of electronic x-ray makes requests clearer to reduce the likelihood of this happening again.
• The imaging and medical staff use a preliminary read system which reduces the risk. The sticky note information placed in the report helps identify significant errors when picked up by the reporting radiologist.
December 2012
SAC2 Patient – fell and sustained fracture to hip
• Patient fell in bathroom post surgery
• Patient independently mobilising
• Building services reviewed bathroom floor – no changes required regarding the floor or the environment
• Case presented at audit meeting
• High falls risk patients to be identified through a “flagging” system to ease identification
• Falls prevention strategies continue, such as individual patient observation, use of alert device
• Falls risks assessments continue to be documented in patient care plans
• Staff training ongoing December 2012
SAC2 Patient fell and sustained fracture to elbow
• Patient fell whilst attempting to mobilise
• Patient was disoriented following waking
• High falls risk patients to be identified through a “flagging” system to ease identification
• Falls prevention strategies continue, such as individual patient observation, use of alert device
• Falls risks assessments
44
Wairarapa, Hutt Valley and Capital and Coast DHBs
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
continue to be documented in patient care plans
• Staff training ongoing
December
2012
SAC2 Patient fell and sustained fracture to hip
• Patient lost balance and fell
• Patient independently mobilising with a stick.
• No indication that patient was unwell prior to fall
• Case presented at Mortality & Morbidity meeting
• High falls risk patients to be identified through a “flagging” system to ease identification
• Falls prevention strategies continue, such as individual patient observation, use of alert devices
• Falls risks assessments continue to be documented in patient care plans
• Staff training ongoing. Feb 2013 SAC2 Delay in cancer
diagnosis Patient referral for
procedure was prioritised as a “B”, and letter sent to patient advising that would be seen within 6 months. Patient waited 9 months for procedure.
An external review found that:
• “In general terms delays over six months in the institution of treatment of colorectal cancer are thought to be associated with worse outcomes although the evidence base is poor. There is little evidence that delays of less than six months are associated with worse outcomes.”
• Waiting lists continue to be monitored to ensure patients are seen within the required times
• Resources increased to reduce waiting times
April 2013 SAC 2 Patient fall resulting in fractured to hip.
• Patient with multiple co-morbidities and English as a second language
• Assessed on admission as high falls risk.
• Appropriate preventative measures in place - including location near to the nurses
• No recommendations as fall deemed unavoidable
45
Wairarapa, Hutt Valley and Capital and Coast DHBs
Date of Event
Event Code
Description of Event
Review Findings Recommendations/Actions
station, falls flags placed outside the room, cot sides raised and frequent checks.
• Patient attempted to get out of bed and catheter disconnected. Nurse lowered the bed rail to sit the patient up on the side of the bed. Patient put feet to the floor, slipped on spilt urine and fell to floor.
46
Wairarapa, Hutt Valley and Capital and Coast DHBs
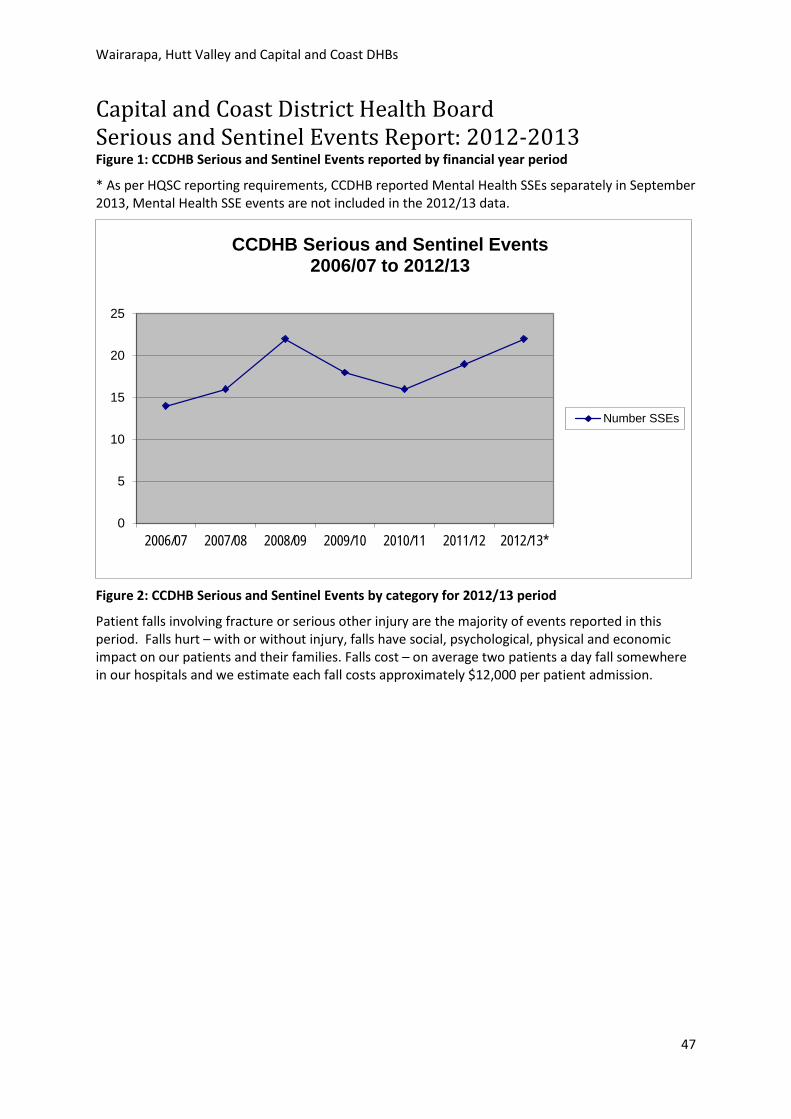
Capital and Coast District Health Board Serious and Sentinel Events Report: 2012-2013 Figure 1: CCDHB Serious and Sentinel Events reported by financial year period
* As per HQSC reporting requirements, CCDHB reported Mental Health SSEs separately in September 2013, Mental Health SSE events are not included in the 2012/13 data.
0
5
10
15
20
25
2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13*
CCDHB Serious and Sentinel Events2006/07 to 2012/13
Number SSEs
Figure 2: CCDHB Serious and Sentinel Events by category for 2012/13 period
Patient falls involving fracture or serious other injury are the majority of events reported in this period. Falls hurt – with or without injury, falls have social, psychological, physical and economic impact on our patients and their families. Falls cost – on average two patients a day fall somewhere in our hospitals and we estimate each fall costs approximately $12,000 per patient admission.
47
Wairarapa, Hutt Valley and Capital and Coast DHBs
Falls68%Medication
14%
Clinical Management-
Diagnosis9%
Clinical Management-
Treatment9%
CCDHB Serious and Sentinel EventsBy Category 2012/2013
While it is not possible to stop every patient from falling when in hospital, many can be prevented and part of our CCDHB Zero Patient Harm programme is to reduce the number of patient falls and the harm that can occur when a patient falls. Our ongoing work to prevent falls and harm from falls is led by our Falls Prevention Group and has been enhanced by CCDHB participation in the Health Quality and Safety Commission’s (HQSC) national patient safety campaign “Being Open”. The first focus of the campaign has been on preventing harm from falls with a month-long promotion called ‘April Falls 2013’. CCDHB took part in the trial of a new falls awareness system using simple traffic light colour coded resources which quickly identify patients who are at risk of falling. Other falls prevention work we have underway includes:
o Falls signage o Staff education o Minimum safety standards o Revised risk assessment o Standardising how we review falls, learn and improve safety o Future work to ensure new staff know how to get falls prevention resources, ways to alert
staff to the fact that the patient is at risk of falling, a checklist to ensure our reviews of falls are consistent, development of better patient information including a web page.
1.
Event Category: Medication Deceased?: N SAC Rating: 2
Event Summary: Medication errors x 2 resulting in unanticipated cardiac rhythm requiring x 1 defibrillation. Patient recovered.
REVIEW
Key findings: A patient was unintentionally administered two doses of adrenaline (5ml & 1ml) instead of fentanyl and midazolam (the intended medications) during a procedure. The patient
48
Wairarapa, Hutt Valley and Capital and Coast DHBs
required one defibrillation shock for the resulting ventricular arrhythmia to restore normal sinus rhythm. The review team identified five key causal factors: 1. Normal yellow container used for emergency medications not available, this led to use of a clear container for the emergency medications 2. Use of the same clear containers for both the emergency and sedation medications, led to a selection error. The wrong container was selected, a second subsequent selection error was then predisposed and occurred when subsequently, the wrong medication (adrenaline) was used. 3. Use of the same syringes (size) for emergency and sedation medications increased the risk of the medication selection error occurring 4. The placement of the emergency and sedation containers on the same bench increased the risk of container selection error occurring 5. The absence of a clear process to check medication prior to administration increased the risk of a medication error not being detected and averted. 6. The error occurred twice before it was fully realised.
Recommendations: The review team notes that the service implemented the following risk controls immediately as a result of this incident:
o Closed lid visibly different containers have been implemented for all emergency medications that are required to be drawn up as part of pre procedure preparation.
o A requirement for the circulating and scrub nurse to double check medication prior to administration has been instigated.
o Noting the above changes have already been implemented, the review team recommended: Consideration, in consultation with the specialist team, is given to keeping emergency medications in an area separate from other routine medications given during the procedure.
Recommendations progress ie. action plan: Visibly different containers have been implemented and are now placed in a separate area from sedation drugs that is accessible. Verbal checks have been implemented prior to administration. All actions completed.
2.
Event Category: Clinical management-diagnosis Deceased?: N SAC Rating: 2
Event Summary: Unreported finding on CT scan (chest) leading to possible delayed diagnosis of metastatic cancer REVIEW
Key findings: The review team were unable to specifically identify the reason the metastatic cancer was not reported on the chest CT scan. The most likely cause of the error was a combination of factors;
o review of multiple imaging, o focus was on diagnosis of abdominal imaging related to the primary problem o there was a delay over the weekend between the preliminary report written by the registrar
being sent by the registrar for review and sign off by the consultant. o Subsequent opportunity for the error to be detected during Multidisciplinary Team (MDT)
meetings, was also missed due to a number of factors including; o late addition of the patient to the MDT list, leaving no preparation time to review all imaging o focus was on abdominal imaging related to the primary problem and differentiating between
disease process and cancer during the MDT. The review team noted that:
49
Wairarapa, Hutt Valley and Capital and Coast DHBs
o MDT preparation time is not protected nor is there a clear provision for leave cover o there is no guideline for the role and responsibilities of the radiologist attending the MDT there are currently no protocols to guide staging and restaging of each tumour stream prior to radical treatment.
Recommendations: The review team recommended that: 1. The Executive Clinical Director formally apologise to the patient, provide a copy of the review report and offer to meet and explain the findings.
2. Radiology review and standardise processes for review, 2nd reporting and sign off of Registrar reports by radiology consultants.
3. Radiology undertake job sizing of Radiology Consultants roles to include protected time for preparing and participating in MDT, cover for leave and to ensure adequate Consultant resource is available for the reporting requirement associated with the CT scan workload.
4. The MDT meetings should have an identified timeframe to register patients that allows for adequate radiology preparation and develop terms of reference to define roles, responsibilities and resource requirements
5. Directorate Services develop protocols for staging and restaging of each tumour stream prior to radical treatment (staging means measuring the growth of tumours by taking scans over time).
Recommendations progress ie. action plan: An apology to the family has been sent. Standardisation of workflow processes indicated has commenced. Actions relating to job-sizing have commenced. Discussion re MDT roles and responsibilities has been identified to strategic clinical governance. Tumour stream staging requirements in progress.
3.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall on inpatient ward. Subsequent X-ray confirmed fractured neck of femur. January 2013 – Incident notified to DHB as not yet reported nationally as a SAC 2 – review initiated at this point.
REVIEW
Key findings: Preliminary event review identified that:
o A reportable event was completed severity 4 minor at the time. Subsequent X-Ray confirmed fractured neck of femur. The reportable event should have been upgraded to a higher severity-SAC 2.
o Falls risk assessment completed on day of admission. Indicated patient was at risk of falls. Appropriate falls prevention strategies implemented at that time (patient watch in place).
o Patient transferred to rehabilitation ward. Placed in single room with close observation from the nurse’s station. New care plan started including falls risk assessment and interventions. Patient able to walk around the ward.
o The patient had a minor fall 5 days before this incident. No evidence of injury, reportable event form completed. Falls risk and the patient admission to discharge planner updated. Patient walking with a frame and supervision the following day.
o Two days before the fall a patient watch was in place. o Fall occurred when patient was accompanied to toilet by watch, patient at basin, pulled away
from watch and slipped sideways. Watch tried to prevent the fall. Patient able to stand with
50
Wairarapa, Hutt Valley and Capital and Coast DHBs
assistance and transfer to bed. Observations stable. Subsequent X-ray confirmed fractured neck of femur.
Recommendations:.
o CCDHB notify the Health Quality and Safety Commission (HQSC) of the incident as a SAC 2. o Review findings be tabled at Directorate Quality Forums to share learning related to both the
Reportable events process and the prevention of harm from falls. o CCDHB continue ongoing falls improvement working group activity and continue to audit the
completion of patient admission to discharge planner and compliance with falls risk assessment and risk controls requirements, and ensure strategies are in place to assist with compliance.
Recommendations progress ie. action plan:. Health Quality and Safety Commission (HQSC) notified of event. Event presented to Clinical Governance and service level areas. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
4.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall on inpatient ward. Subsequent X-ray confirmed fractured neck of femur. January 2013 – Incident notified to DHB as not yet reported nationally as a SAC 2 – review initiated at this point.
REVIEW
Key findings: Preliminary event review identified that:
o A reportable event was completed severity 4 minor at the time. Subsequent X-Ray confirmed fractured neck of femur. The reportable event was rated SAC 3 on review. It does not appear the severity was upgraded after the fracture was identified.
o In 2011 the timeframe for a falls assessment to be completed was within 24 hours of admission. There was no documented falls assessment completed. The patient was admitted via Emergency Department (ED) and the Medical Assessment and Planning Unit (MAPU) to an acute Medical ward.
o The patient fall occurred approximately 8 hours after admission. o Clinical notes indicate that the patient was extremely confused and disorientated, was verbally
and physically aggressive, (had required police intervention at home prior to admission) would not allow observations to be taken and refused medication.
o The patient was to be transferred to a bed in the safe care bay in the medical ward however this did not occur prior to the fall.
o The patient had a watch in ED and MAPU. Documentation does not specify if the watch remained in place after transfer to the Medical ward. Notes record a security orderly assisting the patient after the fall.
o The patient tried to run away and slipped and fell. Recommendations:
o CCDHB notify the Health Quality and Safety Commission (HQSC) of the incident as a SAC 2. o Review findings be tabled at Directorate Quality Forums to share learning related to both the
Reportable events process and the prevention of harm from falls. o CCDHB continue ongoing falls improvement working group activity and continue to audit the
completion of patient admission to discharge planner and compliance with falls risk assessment and risk controls requirements, and ensure strategies are in place to assist with compliance.
51
Wairarapa, Hutt Valley and Capital and Coast DHBs
Recommendations progress ie. action plan: HQSC notified of event. Event presented to Clinical Governance and service level areas. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
5.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Feb 2012 - Patient fall on inpatient ward (night duty). X-ray later that day confirmed fractured neck of femur. Jan 2013 – Incident notified to DHB as not yet reported nationally as SAC 2 – review initiated at this point.
REVIEW
Key findings: Preliminary event review identified that:
o The patient had got out of bed, walked to the toilet without usual aids, call bell not used (unwitnessed fall-night duty).
o Reportable event recorded severity minimal. Post fall patient alert and oriented, no injury evident. Medical review noted no immediate action indicated, for possible X-ray in morning.
o The need to update the reportable event when the fracture was diagnosed the following day was overlooked. At this time a SAC 2 or 3 rating would apply depending on likelihood.
o Falls risk assessment was completed two days post admission (standard = completion within one hour of admission). Indicated the patient was at risk of falls. Appropriate falls prevention strategies were implemented at that time. Patient alert and oriented and shown call bell system.
o The day after the falls risk assessment was completed, the patient suffered a minor fall and was transferred to the Safe Care Bay (SCB) for closer monitoring.
o While patient admission to discharge planner, and falls risk assessments were not completed within specified timeframes, appropriate falls prevention strategies were in place.
o Although the patient was transferred to the SCB for increased monitoring this did not prevent the fall from occurring.
o It was determined no further review was indicated. Recommendations:
o CCDHB notify the Health Quality and Safety Commission (HQSC) of the incident as a SAC 2. o Review findings be tabled at Directorate Quality Forums to share learning related to both the
Reportable events process and the prevention of harm from falls. o CCDHB continue ongoing falls improvement working group activity and continue to audit the
completion of patient admission to discharge planner and compliance with falls risk assessment and risk controls requirements, and ensure strategies are in place to assist with compliance.
Recommendations progress ie. action plan: HQSC notified of event. Event presented to Clinical Governance and service level areas. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
6.
Event Category: Clinical management-diagnosis Deceased?: Y
Event Summary: Patient had two separate Hepatitis B positive serology reports and an abnormal liver CT scan report. Appears no follow up for same.
52
Wairarapa, Hutt Valley and Capital and Coast DHBs
REVIEW
Key findings: Review found that:
o The patient had pre op hepatitis serology testing (2010-prior to cardiothoracic procedure) reported positive for Hepatitis B. No record of follow up. A month later the patient was admitted with chest pain. During admission a CT scan was reported abnormal, showing possible early liver cancer. No record of follow up. Six months later the patient was admitted for orthopaedic surgery and required a cardiothoracic procedure for which pre op hepatitis serology testing was ordered and reported positive for Hepatitis B. No record of follow up. On this admission the CT report from six months previous was noted as not having been followed up.
o A number of failures contributed to both the failure to follow up the patient’s Hepatitis B status once reported positive, and the failure to follow up the patient’s CT scan report which was indicative of cancer. As a result, there was a 21 month delay in the diagnoses being acted upon (hepatitis) or confirmed (liver cancer).
o The review team note that while the outcome for the patient may not have been different, the patient was not informed of the diagnoses and his options at that time, and by the time the diagnoses were acted upon he was not considered a candidate for more than palliative care.
o The failures related to lack of a formal process to sign off on receipt of results, lack of a formal results management process for tests requested, and failure of issues noted for follow up to be formally recorded in either a problem list and actioned, or referred to the appropriate specialty for investigation.
Recommendations:. Review recommended: C&C DHB formally apologise to the patient’s family, provide them with a copy of the review report and the opportunity to meet and discuss as desired. The review team recommend that the DHB complete implementation of a system for electronic sign off of results, that an electronic ‘problem list’ be considered for implementation and that services review their processes for the requesting and follow up of hepatitis serology results as part of pre-operative testing.
Recommendations progress ie. action plan: Apology sent to family. Electronic sign off project implemented and in place at CCDHB. Electronic problem list option on Concerto to be actioned. Cardiology reviewed process prior to E sign off implementation; E sign off now actioned.
7.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall on inpatient ward. Subsequent X-ray confirmed fractured neck of femur. January 2013 – Incident notified to DHB as not yet reported nationally as a SAC 2 – review initiated at this point.
REVIEW
Key findings:: Preliminary event review identified that:
o A reportable event was completed severity 4 minor at the time. Subsequent X-Ray the following day confirmed fractured neck of femur. The severity was not upgraded after the fracture was identified.
o Falls assessment not completed on admission but documented in notes high falls risk and supervision and assistance recommended for all transferring and mobility.
o Appropriate falls prevention strategies in place, patient alert and oriented, shown call bell system. Call bell was in reach and commode beside bed.
53
Wairarapa, Hutt Valley and Capital and Coast DHBs
o Patient had earlier un-witnessed fall beside bed on morning of same day. Medical review-no obvious injuries found, patient alert and no concerns.
o Patient reminded to ring bell if needed to go to toilet, supervised with personal cares and assisted to the toilet throughout the day. For supervision and assistance for all transferring and mobility.
o The second fall (which resulted in the fracture) occurred in the evening. The patient attempted to mobilise from bed to the bathroom without staff noticing, and fell.
Recommendations:
o CCDHB notify the Health Quality and Safety Commission (HQSC) of the incident as a SAC 2. o Review findings be tabled at Directorate Quality Forums to share learning related to both the
Reportable events process and the prevention of harm from falls. o CCDHB continue ongoing falls improvement working group activity and continue to audit the
completion of patient admission to discharge planner and compliance with falls risk assessment and risk controls requirements, and ensure strategies are in place to assist with compliance.
Recommendations progress ie. action plan: HQSC notified of event. Event presented to Clinical Governance and service level areas. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
8.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall resulting in fractured neck of femur (hip).
REVIEW
Key findings:: The review found that the Patient Admission to Discharge Plan (PADP) which includes falls risk assessment was not completed during admission to the assessment unit but was completed on transfer to the ward half an hour before the fall. Review found that appropriate falls prevention strategies were in place for this patient at the time of the fall.
Recommendations:
o Regular audit and reporting of Patient Admission to Discharge Planner completion at organisation and directorate level with specific focus on falls risk assessment.
o Findings to be fed back to ward staff and directorate clinical governance o Staff education o Purchase of falls resources. Recommendations progress ie. action plan: Regular audits of PADP conducted as per project plan and development of PADP. Falls risk safety group established. Findings presented to Clinical Governance and ward staff. Staff education completed on ward.
9.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall resulting in peri prosthetic fracture right femur shaft.
REVIEW
Key findings:: The review found that all falls prevention strategies were in place at time of fall, green wrist band insitu, patient orientated to the environment (patient had previously been on the ward
54
Wairarapa, Hutt Valley and Capital and Coast DHBs
for 6 weeks), except optimal visibility to staff – patient in room not able to be directly visualised from nursing station.
Recommendations: The review recommended:
o Continue with falls prevention forum –two monthly with nursing staff and Clinical Nurse Educator and Charge Nurse Manager.
o De-clutter 6 bedded cubicles, remove 2 unused beds and store in basement o Nursing staff to ensure when mobilising patients to reflect physiotherapist recommendations. o Nursing staff complete falls risk assessments on admission and change of plan, treatment, fall. o Implementation of prevention strategies. o Multidisciplinary teams update care plans. Recommendations progress ie. action plan: Falls safety group established. Bed spaces de-cluttered. Education given regard mobilising patients. PADP education ongoing and audited as per CCDHB wide policy. Falls prevention mitigation strategies implemented as per falls safety group. MDT's educated on contribution to PADP and discussed at clinical governance.
10.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Voluntary patient admitted intoxicated, left ward, on returning further intoxicated, fell resulting in fracture left femur.
REVIEW
Key findings:: The preliminary event review found that the patient’s actions were not predictable, and that falls prevention strategies would not have prevented this incident. No further review indicated.
Recommendations: Nil.
Recommendations progress ie. action plan: Not applicable.
11.
Event Category: Medication Deceased?: N SAC Rating:
Event Summary: Dispensing community pharmacist changed usual liquid morphine concentration, patient's family informed. Appears patient took usual volume of higher concentration resulting in unintended overdose. Hypoxic brain injury resulted..
REVIEW
Key findings:: Review found that during routine review of an oncology patient, dehydration and significant pain issues were identified. In addition to fentanyl patches the patient was taking very small doses of morphine elixir 2.5 mg (in a 1 mg/ml solution) for breakthrough pain relief. Prescription increasing the patient’s morphine dose was given. The patient and spouse were informed about the change in dose and the possible side effects. The new dose was administered while the patient was in the oncology day unit, on two occasions, with good effect and no side effects. The patient returned home on this new regime.
55
Wairarapa, Hutt Valley and Capital and Coast DHBs
Later that day the patient’s spouse took the prescription to a community pharmacy the pharmacist dispensed 10mg/ml strength of morphine. This was an appropriate formulation perceived to be more convenient for the patient to swallow, i.e. 1 ml for each dose. The pharmacist informed the patient’s spouse that the patient was to take 1ml each time up to 5 times a day. Later that day the visiting community nurse noted the change of medication dose and discussed this with the patient and her spouse. The patient was noted to be comfortable.
The following day the patient attended the oncology unit with her spouse. It was noted pain had improved. No concerns, side effects or significant issues were noted.
The following day the patient was admitted to the Emergency Department and Intensive Care Unit with hypoxic brain injury, acute hepatitis and acute kidney failure. It was noted that it appeared the patient had self administered the usual volume thereby giving a cumulative overdose of morphine due to the higher concentration dispensed (10 mg/ml compared with 1 mg/ml).
The review team found that several efforts were made to provide information about the change in dose and formulation to the patient and spouse by both the DHB and the community pharmacy. Despite this an overdose occurred. An incidental finding was that there was no evidence of communicating the oral morphine dose to the patient’s General Practitioner (GP). The most likely factor that contributed to event was confusion about the volume of oral morphine to be taken after the change in dose prescribed. This occurred despite information being provided on several occasions by both C&C DHB and the community pharmacy, within the two days prior to the accidental overdose taking place.
Recommendations:
o Community pharmacies consider how and when adjunct written information should be given to patients, particularly with a change of dose and or formulation, and while this may not guarantee that the information provided is understood and/or acted upon it would be an additional source of information that could be referred to by the patient and her carer.
o The review team also notes that daily dispensing of liquid morphine can reduce the chances of the patient being in possession of an excessive or toxic dose of the drug. This technique is used in pain services and in the opiate treatment service. However, daily pick up would in its own right pose problems of access and may lead to distress for the patient and carer and would therefore need to be considered on a case by case basis.
o Community pharmacies consider provision of a syringe to reduce the risk of taking or being given an excessive volume of medication when small volumes of high risk such as opiate liquid medication are dispensed.
o The DHB Medicines Committee chair communicate to all prescribers, the need to provide adjunct written information to patients/carers, particularly with a change of dose and/or formulation. While this may not guarantee that the information provided is understood and/or acted upon it would be an additional source of information that could be referred to by the patients/carers.
o The DHB Medicines Committee considers the value of requiring that a copy of the controlled drug script is made and kept in the patient record.
Recommendations progress ie. action plan: Community Pharmacy recommendations approved by Community Pharmacy involved in review. Recommendations relating to Community Pharmacy presented to Primary Secondary Clinical Governance Group for discussion and actioning. PSO to produce national alert regard this event. Medicines Review Committee actioning communication
56
Wairarapa, Hutt Valley and Capital and Coast DHBs
and provision of adjunct information. MRC have communicated with National Medicines group regard fourth copy of Controlled Drugs prescription.
12.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall resulting in fracture right neck of femur (hip).
REVIEW
Key findings:: The preliminary event review identified that the patient had been identified as a falls risk and appropriate falls risk mitigation strategies were in place at the time of the fall in particular use of a walking frame and supervision. No further review indicated.
Recommendations:
o No specific recommendations from this incident. All appropriate strategies were in place. o Findings will be used in general education and awareness for staff and tabled at appropriate
forums. Recommendations progress ie. action plan: Nil specific. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
13.
Event Category: Fall Deceased?: Y SAC Rating: 2
Event Summary: Patient fall resulting in fracture right neck of femur (hip). Decision to provide palliative care. Patient deceased.
REVIEW
Key findings:: The review found that:
o The Patient Admission to Discharge Planner (PADP) was initially completed appropriately (including falls risk assessment/mobility assessment and falls strategies) however, on transfer to the rehabilitation ward, no re-assessments were formally completed.
o Appropriate falls prevention strategies were in place for the patient however these did not prevent the patient falling.
Recommendations:
o Formal apology, meeting with and provision of report to patient’s family o Regular audit and reporting of Patient Admission to Discharge Planner (PADP) completion at
organisation and directorate level with specific focus on falls risk assessment. o The requirement for new PADP forms for patient’s transferring between wards be revised to a
requirement for completion of the “Patient Plan” section as soon as practicable on arrival of the patient in order to reflect any changes to the status/risk of the patient and the changed environment
Recommendations progress ie. action plan: Regular auditing of PADP and reporting of same to HHS Clinical Governance ongoing. Apology to family completed. Requirement for completion of 'Patient Plan' on transfer to Kenepuru Hospital in place.
57
Wairarapa, Hutt Valley and Capital and Coast DHBs
14.
Event Category: Fall Deceased?: Y SAC Rating: 2
Event Summary: Patient fall resulting in fracture right neck of femur (hip).
REVIEW
Key findings::The preliminary review identified that a falls risk assessment was completed and that appropriate falls prevention strategies in place. Findings related to incomplete documentation are being addressed through recommendations from other recent falls reviews. No further review indicated.
Recommendations:
o Recommend letter of apology and findings of preliminary event review be provided to patient’s family with offer to meet as required.
o Recommend no further review indicated above actions will address findings from this preliminary event review.
Recommendations progress ie. action plan: Nil specific. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
15.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall resulting in fracture shaft of femur.
REVIEW
Key findings: Review found that the patient was admitted to the assessment unit for headache.
o The Patient Admission to Discharge Planner was completed including assessment for falls risk soon after admission. The patient was noted as being at risk of falling and appropriate falls risk prevention strategies in place. The patient was advised to wait for staff assistance to mobilise to toilet to empty catheter bag.
o The patient mobilised independently to toilet, attempted to drain catheter bag and appears to have slipped on spill on the floor.
o All appropriate actions taken to assess injury and provide care to patient subsequent to fall. Patient suffered spiral fracture proximal shaft of femur. Surgical repair.
Recommendations:
o No specific recommendations from this incident. All appropriate strategies were in place. o Findings will be used in general education and awareness for staff and tabled at appropriate
forums. Recommendations progress ie. action plan: Nil specific. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
16.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall on inpatient ward resulting in a mid shaft spiral fracture of R) femur.
REVIEW
58
Wairarapa, Hutt Valley and Capital and Coast DHBs
Key findings: Reportable event recorded at time of event – no apparent injury - severity rated minimal. X-Ray imaging later the same day confirmed a fractured neck of femur. The reportable event was referred to the Quality Manager. Preliminary event review identified that:
o Patient admitted to orthopaedic ward after a fall at home, had surgery for a post revision of right Total Knee Joint Replacement, patient later transferred to rehabilitation ward the day before the fall.
o The Patient Admission to Discharge Planner (PADP) falls risk assessment and interventions were commenced on the orthopaedic ward. PADP updates were documented every two to three days on both wards. Falls risk assessment indicated that the patient was at risk of falls-green wrist band on to signify the falls risk.
o Night staff investigated a noise and found the patient lying on the floor beside the bed. Side rails were up and call bell in reach. Patient had been reluctant to call for assistance and tried to get out of bed and fell.
o X-ray later the same day confirmed peri- prosthetic fracture spinal mid shaft femur.. Recommendations:
o That this preliminary event review be tabled at the appropriate Quality forums for MCC. o That this event be notified to the Health Quality and Safety Commission (HQSC) by way of a
Reportable Event Brief as a SAC 2 rated event. o That CCDHB continue the ongoing projects already underway in order to help reduce the
incidence of falls. o That CCDHB continue to audit the timeliness of completion of the new PADP and ensure
strategies are in place to assist with compliance.. Recommendations progress ie. action plan: Review presented to Clinical Governance and service level areas. HQSC notified of event. Incorporated into DHB Patient Safety Programme - zero patient harm - falls prevention workplan.
17.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall from bed resulting in a right periprosthetic distal spiral femur fracture.
REVIEW
Key findings:
o The patient was an acute admission due to chronically infected right hip joint replacement. Complex history including diabetes – insulin dependent. Revision surgery the following day, multiple subsequent dislocations, managed in traction until 2nd stage revision – 3 days later. An episode of delirium post-operatively - CT showed no abnormalities, improved with reduced opiates. Multiple blood transfusions.
o Transferred to a rehabilitation ward 12 days post admission. Care plan updated on admission – continued from admitting ward. Patient identified as high falls risk, fall minimisation strategies put in place. Care plan regularly updated.
o Two weeks after transfer to the rehabilitation ward the patient was medically reviewed due to concerns re wound, minimal food or fluid intake, low mood and energy. Blood sugar levels unstable. Low haemoglobin and high potassium levels noted. Two units of red blood cells transfused the following day.
o In the early hours of the following morning the patient was found sitting on the floor beside the bed having “dreamt she was walking”. Medical review completed. Patient transferred to
59
Wairarapa, Hutt Valley and Capital and Coast DHBs
orthopaedic ward. X-ray showed periprosthetic fracture of the R femur. Subsequent surgery open reduction and internal fixation of fracture. Patient later transferred to rehabilitation ward.
o A reportable event was recorded by nursing staff- Severity 2. Preliminary event review showed falls risk assessment and risk controls were in place for this patient. Concerns about the patient’s condition were notified and responded to appropriately.
o The patient was unwell with post surgery problems, wound concerns, extended hospitalisation, unstable blood sugars and recent blood transfusion. All appropriate actions were taken when the fall occurred. It was noted incidentally that it was not documented whether the patient was wearing a green falls risk wrist band - the review team note that the wrist band’s presence or absence would not have been material in preventing such a fall.
Recommendations: The findings of the review will be incorporated into the Ward, Directorate and DHB preventing harm from falls programme. No further review indicated
Recommendations progress ie. action plan: No further review indicated. CLOSED.
18.
Event Category: Clinical management-treatment Deceased?: Y
Event Summary: Patient deceased in community on same day as attended 4 week post op orthopaedic clinic follow-up appointment. Interim post mortem indicates Pulmonary Embolism (clot in lungs) secondary to Deep Vein Thrombosis (DVT-clot).
REVIEW
Key findings: The review found that the patient received appropriate care, the sudden death from a clot was not predictable from the signs, symptoms or history and that the clinical team carefully reviewed the patient’s care at each outpatient appointment. Review noted CCDHB is finalising a Venous Thromboembolism (VTE) Prophylaxis (prevention) guideline including Orthopaedic Risk Assessment Form, that the patient received prophylaxis consistent with the draft guideline and greater than the American College of Chest Physicians guidelines currently recommend.
Recommendations: Review recommended:
o Provision of the report to the patient’s family and an offer to meet o Completion of the VTE prophylaxis (clot prevention) guideline as soon as practicable including
consideration of inclusion of an information leaflet for patients o Orthopaedic services to further research the efficacy of oral anticoagulant agents, consent
information and clarification of information for patients and families. Recommendations progress ie. action plan: Note: Family advised of review and report provided. The family chose not to meet formally. The action plan is still in progress:
o A research project re "aspirin versus rivaroxaban in below knee casts for Achilles Tendon and non-weight bearing follow fracture" has been submitted for a feasibility grant,
o The Orthopaedic Services Consent checklist and updated Achilles Tendon Rupture forms are being updated presently.
o The organisation guideline for prevention of venous thromboembolism (VTE-clots) has been completed and implemented.
o 19.
60
Wairarapa, Hutt Valley and Capital and Coast DHBs
Event Category: Clinical management-treatment Deceased?: N
Event Summary: Non-reassuring fetal heart rate tracing-during labour. Proceeded to emergency caesarean section-full thickness uterine rupture identified. Woman retained uterus, prolonged stay, baby spent several days in Neonatal Intensive Care Unit (NICU).
REVIEW
Key findings: The review found that a number of factors resulted in a situation where trial of labour was allowed to continue and the opportunity to delivery prior to uterine rupture was missed. The number of clinicians involved in the planning and care coupled with unclear communication at times meant that clarity for all involved and uniform expectations of intervention did not occur.
Recommendations: Review recommended:
o An apology to the patient’s family, provision of the report and an offer to meet o Letter to all medical staff assess for vaginal birth after caesarean section highlighting the
importance of clearly documenting the management plan agreed with the Lead Maternity Carer and woman/couple
o Memo to all Women’s Health clinicians re importance of attending handover o Audit of documentation re options and consent for VBAC o Registrar teaching o Registrar assessments of level of competence regularly discussed. Recommendations progress ie. action plan: Note: Woman and family advised of review, report provided and meeting held with the family. The action plan is now complete.
20.
Event Category: Medication Deceased?: N SAC Rating: 2
Event Summary: Concern re prescription of opiate medication for patient with history of chronic renal failure. Patient required admission to ICU for haemodialysis-acute on chronic renal failure, acidosis, anuria and opiate overdose.
REVIEW
Key findings: The draft review report is awaiting staff feedback before being finalised.
Recommendations: NA
Recommendations progress ie. action plan: Family to be provided with report when complete.
21.
Event Category: Fall Deceased?: Y SAC Rating: 2
Event Summary: Patient admitted with mild delirium secondary to urinary tract infection with consideration for confusion and social situation. Three days later in the early hours of the morning the patient fell. Oblique fracture through the surgical neck of the humerus diagnosed. Subsequent deterioration agreed not for active resuscitation in discussion with family. Care transferred to Internal Medicine. Three days later the patient transferred to rehabilitation. A further nine days later the patient deceased having developed pneumonia and a palliative approach taken. Coroner advised including of fall. Coroner satisfied with information.
61
Wairarapa, Hutt Valley and Capital and Coast DHBs
REVIEW
Key findings: The draft review report is awaiting staff feedback before being finalised.
Recommendations: NA
Recommendations progress ie. action plan: Family to be provided with report when complete.
22.
Event Category: Fall Deceased?: N SAC Rating: 2
Event Summary: Patient fall. Initial assessment appeared no injury. Subsequent CT Scan showed small acute on chronic sub dural bleed, no midline shift. 5 days later developed seizures, required intensive care admission. A further 5 days later required burr holes. Later transferred to rehabilitation.
REVIEW
Key findings: The review is in progress and due to be completed in November 2013.
Recommendations: NA
Recommendations progress ie. action plan: Family to be provided with report when complete.
62
Lakes DHB
Lakes District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.lakesdhb.govt.nz
Serious Adverse Events @ Lakes DHB Hospitals 2012-13 year – onto QUALITY and RISK – under Serious Adverse Events
The last financial year Lakes DHB reported 18 adverse events to the Health Quality and Safety Commission. A total of 17 are reported for Lakes in the national HQSC report, with the difference being the result of a timing issue in finalising the level of harm for one case. The 2012-13 events are an increase from the seven of the previous financial year.
As noted throughout the country, increased reporting is thought to be due to the New Zealand health sector’s move towards a culture of no blame. This is to be encouraged as along with allowing Lakes DHB to learn from the mistakes, it allows for the outcomes of the improvements to be shared with all other health providers in New Zealand.
The make up of our reported events are:
Falls with harm 5
Medication error 3
Delay in diagnosis and treatment 3
Pressure sores 2
Death of a baby during or following child birth 2
Patient behaviour causing harm 1
Inappropriate transport 1
Discharged home with no known cause for clinical presentation. 1
Five of the patients who were affected by these events died as a result of the event.
Of this year’s events two were what are termed near misses - incidents that occur that could have had a serious outcome but did not.
All these events are investigated using a root cause analysis methodology, which results in identifying system errors and develops recommendations for improvements.
Falls are identified as the major risk for our patients when they are admitted to hospital. A change of environment for the elderly and confused adds to the likelihood of a fall so staff have a predetermined tool to assess the falls risk and a number of strategies to put in place to minimise that risk. Working with the other regional DHBs, Taranaki, Waikato, Bay of Plenty and Tarawhiti, Lakes DHB has embraced the OPEN for BETTER CARE CAMPAIGN and the six-month programme of falls prevention.
63
Lakes DHB
The prevention of falls will be a continuing part of the safety programme at Lakes and the next steps of the campaign will see us working with community health care providers, families and whanau to help prevent such accidents.
Medication errors are an international event and Lakes has three major errors this financial year. One of these errors resulted in death, due to inadequate monitoring of the side effects of the drug in the community.
The root cause analyses for drug errors have resulted in a number of improvement actions.
One incidental finding from these reviews found a patient who had a complex medication regime who took a over the counter cough mixture lead to her death. As a result of this finding the DHB has published information for patients in the community who are taking very strong pain relief warning them of the dangers of adding other medications to the mix.
Delay in diagnosis or treatment resulted in three serious adverse events. Two of these prolonged the patients’ treatment and delayed recovery. One had no serious harm but was reported and investigated as another result from the delay could have caused harm.
Hospital acquired pressure ulcers can be debilitating and cause loss of limb. The two cases reported by Lakes DHB were caused through a mechanical device used to prevent deep vein thrombosis following surgery. Through a hospital-wide project on the prevention of venous thrombosis the decision was made for mechanical foot pumps to no longer be used, with risk assessment and the use of preventative medication now used in place of the foot pumps. The best means of preventing this complication is ensuring patients are as fit as possible for surgery, with as short a time in theatre as possible along with getting the patient out of bed and walking on the same day or morning after surgery. A project underway in the DHB is Early Recovery After Surgery (ERAS) which looks at a number of ways to prevent complications and reduce recovery times.
The loss of a mother or baby during child birth or as a result of child birth is a very distressing event. Lakes DHB reports two unexpected baby deaths this year. While both these babies succumbed to difficulties during the labour there were lessons to be learned about the observations and actions taken during the time in labour. A heart monitor was purchased for theatre, guidelines were established regarding criteria for performing an emergency caesarean section, and there has been a change in protocol of managing a baby delivered unwell with the immediate involvement of a doctor.
Lakes DHB did experience a fire in a patient area due to a patient’s behaviour. A full review of the circumstances, clinical care and a review with the fire service revealed a number of improvements in monitoring equipment, checking possessions brought into hospital, and the need to advise relatives and friends about not bringing certain things into patients. The report on this event was shared with all DHBs and with the Department of Corrections as a learning.
64
Lakes DHB
Transportation between health centres can be a cause for concern and this incident was a near miss that was investigated to prevent a serious event from occurring. Work continues with staff to recognise appropriate streams of intervention, transferring quickly or stabilising the patient with the staff available and the support of a secondary or tertiary hospital. Support can be provided by tele and video links and this is to be enhanced in the near future at Lakes DHB.
Please click here to view the Lakes DHB Quality Account for the period 1 July 2012-30 June 2013. This document details some of the many quality improvements undertaken at Lakes DHB to enhance safety and the care delivered to our community.
Media release: Serious Adverse Events 2012-2013
Lakes DHB Quality and Risk Manager Lesley Yule says Lakes DHB regrets any harm caused to patients during their care.
“Our staff are mindful of the patients and families involved in these incidents and we encourage families and patients to contact us to alert us to any issues that are noticed so we can act to prevent harm,” said Lesley Yule.
Lakes DHB serves a population of just over 100,000 people and had 68,001 contacts of hospital admissions and outpatients in the last year ended June 2013. (Comprised of: in-patients 25,636, and specialist outpatient attendances 42,365).
Reporting incidents is a voluntary process within the Lakes DHB. This is a method of collecting incidents and near misses that have or have the potential to cause harm to our patients. Our review into each incident assesses the seriousness and indicates the appropriate level of investigation to be undertaken, and our process is looking for accountability without blame. This process is one of the fundamental tools in the health sector to improve safety, process and quality.
The last financial year Lakes DHB reported 18 adverse events to the Health Quality and Safety Commission. A total of 17 are reported for Lakes in the national HQSC report, with the difference being the result of a timing issue in finalising the level of harm for one case. The 2012-13 events are an increase from the seven of the previous financial year.
As noted throughout the country, increased reporting is thought to be due to the New Zealand health sector’s move towards a culture of no blame. This is to be encouraged as along with allowing Lakes DHB to learn from the mistakes, it allows for the outcomes of the improvements to be shared with all other health providers in New Zealand.
65
Lakes DHB
The make up of reported events in Lakes is as follows:
Falls with harm 5
Medication error 3
Delay in diagnosis and treatment 3
Pressure sores 2
Death of a baby during or following child birth 2
Patient behaviour causing harm 1
Inappropriate transport 1
Discharged home with no known cause for clinical presentation. 1
Five of the patients who were affected by these events died as a result of the event.
Of this year’s events two were what are termed near misses - incidents that occur that could have had a serious outcome but did not.
All these events are investigated using a root cause analysis methodology, which results in identifying system errors and develops recommendations for improvements.
Falls are identified as the major risk for our patients when they are admitted to hospital. A change of environment for the elderly and confused adds to the likelihood of a fall so staff have a predetermined tool to assess the falls risk and a number of strategies to put in place to minimise that risk. Working with the other regional DHBs, Taranaki, Waikato, Bay of Plenty and Tairawhiti, Lakes DHB has embraced the Open for Better Care campaign and the six-month programme of falls prevention.
The prevention of falls will be a continuing part of the safety programme at Lakes and the next steps of the campaign will see us working with community health care providers, families and whanau to help prevent such accidents.
Medication errors are an international event and Lakes has three major errors this financial year. One of these errors resulted in death, due to inadequate monitoring of the side effects of the drug in the community.
The root cause analyses for drug errors have resulted in a number of improvement actions.
One incidental finding from these reviews found a patient who had a complex medication regime who took a over the counter cough mixture lead to her death. As a result of this finding the DHB has published information for patients in the community who are taking very strong pain relief warning them of the dangers of adding other medications to the mix.
66
Lakes DHB
Click here to see the brochure on Opioid Pain Relief.
Delay in diagnosis or treatment resulted in three serious adverse events. Two of these prolonged the patients’ treatment and delayed recovery. One had no serious harm but was reported and investigated as another result from the delay could have caused harm.
Hospital acquired pressure ulcers can be debilitating and cause loss of limb. The two cases reported by Lakes DHB were caused through a mechanical device used to prevent deep vein thrombosis following surgery. Through a hospital-wide project on the prevention of venous thrombosis the decision was made for mechanical foot pumps to no longer be used, with risk assessment and the use of preventative medication now used in place of the foot pumps. The best means of preventing this complication is ensuring patients are as fit as possible for surgery, with as short a time in theatre as possible along with getting the patient out of bed and walking on the same day or morning after surgery. A project underway in the DHB is Early Recovery After Surgery (ERAS) which looks at a number of ways to prevent complications and reduce recovery times.
The loss of a mother or baby during child birth or as a result of child birth is a very distressing event. Lakes DHB reports two unexpected baby deaths this year. While both these babies succumbed to difficulties during the labour there were lessons to be learned about the observations and actions taken during the time in labour. A heart monitor was purchased for theatre, guidelines were established regarding criteria for performing an emergency caesarean section, and there has been a change in protocol of managing a baby delivered unwell with the immediate involvement of a doctor.
Lakes DHB did experience a fire in a patient area due to a patient’s behaviour. A full review of the circumstances, clinical care and a review with the fire service revealed a number of improvements in monitoring equipment, checking possessions brought into hospital, and the need to advise relatives and friends about not bringing certain things into patients. The report on this event was shared with all DHBs and with the Department of Corrections as a learning.
Transportation between health centres can be a cause for concern and this incident was a near miss that was investigated to prevent a serious event from occurring. Work continues with staff to recognise appropriate streams of intervention, transferring quickly or stabilising the patient with the staff available and the support of a secondary or tertiary hospital. Support can be provided by tele and video links and this is to be enhanced in the near future at Lakes DHB.
67
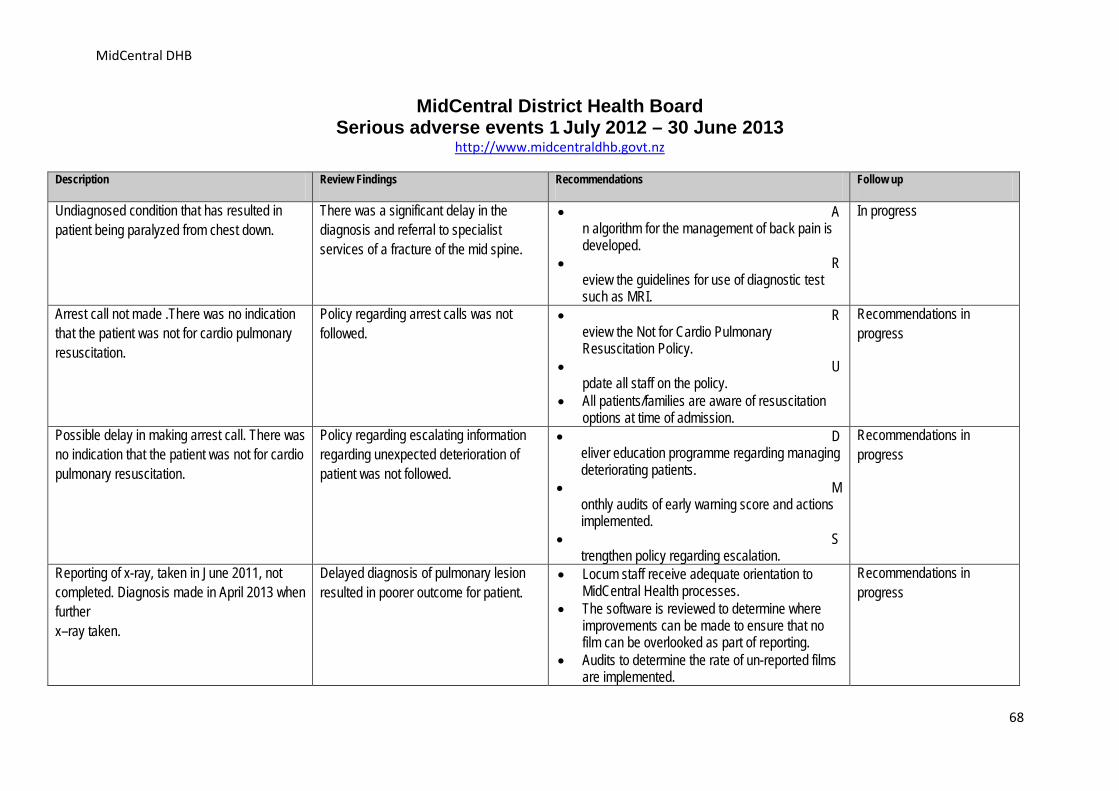
MidCentral DHB
MidCentral District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.midcentraldhb.govt.nz
Description Review Findings Recommendations Follow up
Undiagnosed condition that has resulted in patient being paralyzed from chest down.
There was a significant delay in the diagnosis and referral to specialist services of a fracture of the mid spine.
• An algorithm for the management of back pain is developed.
• Review the guidelines for use of diagnostic test such as MRI.
In progress
Arrest call not made .There was no indication that the patient was not for cardio pulmonary resuscitation.
Policy regarding arrest calls was not followed.
• Review the Not for Cardio Pulmonary Resuscitation Policy.
• Update all staff on the policy.
• All patients/families are aware of resuscitation options at time of admission.
Recommendations in progress
Possible delay in making arrest call. There was no indication that the patient was not for cardio pulmonary resuscitation.
Policy regarding escalating information regarding unexpected deterioration of patient was not followed.
• Deliver education programme regarding managing deteriorating patients.
• Monthly audits of early warning score and actions implemented.
• Strengthen policy regarding escalation.
Recommendations in progress
Reporting of x-ray, taken in June 2011, not completed. Diagnosis made in April 2013 when further x–ray taken.
Delayed diagnosis of pulmonary lesion resulted in poorer outcome for patient.
• Locum staff receive adequate orientation to MidCentral Health processes.
• The software is reviewed to determine where improvements can be made to ensure that no film can be overlooked as part of reporting.
• Audits to determine the rate of un-reported films are implemented.
Recommendations in progress
68
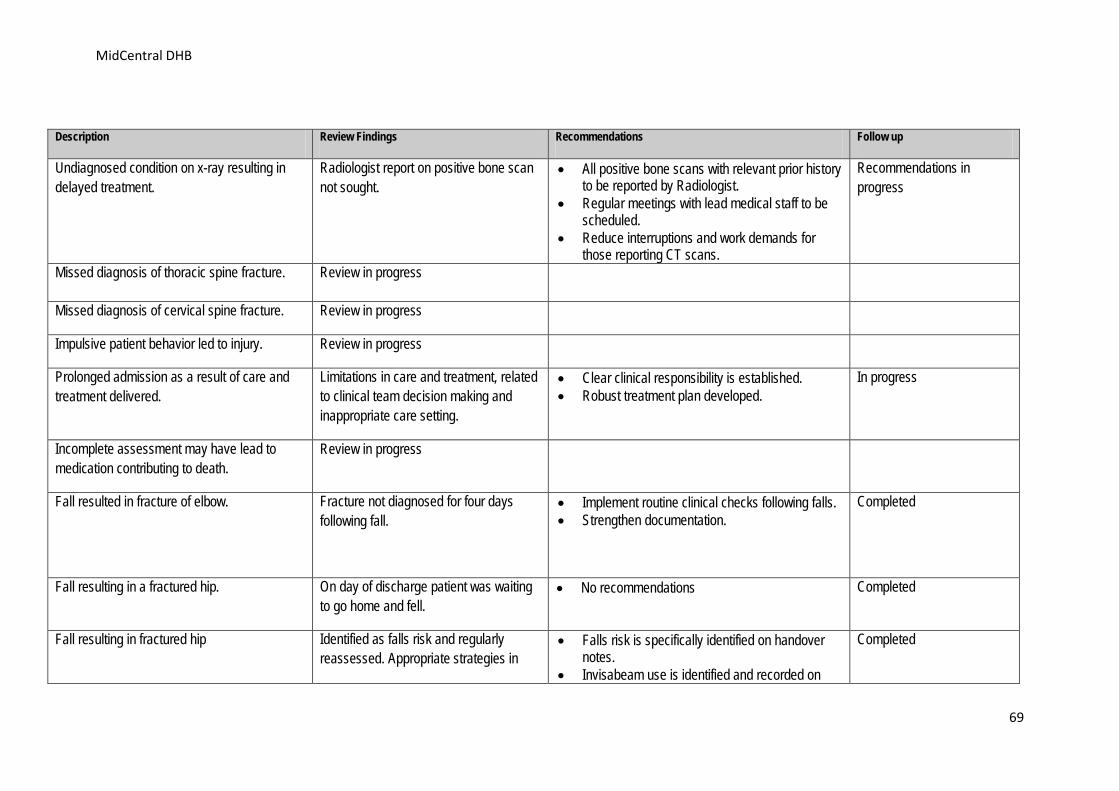
MidCentral DHB
Description Review Findings Recommendations Follow up
Undiagnosed condition on x-ray resulting in delayed treatment.
Radiologist report on positive bone scan not sought.
• All positive bone scans with relevant prior history to be reported by Radiologist.
• Regular meetings with lead medical staff to be scheduled.
• Reduce interruptions and work demands for those reporting CT scans.
Recommendations in progress
Missed diagnosis of thoracic spine fracture. Review in progress
Missed diagnosis of cervical spine fracture. Review in progress
Impulsive patient behavior led to injury. Review in progress
Prolonged admission as a result of care and treatment delivered.
Limitations in care and treatment, related to clinical team decision making and inappropriate care setting.
• Clear clinical responsibility is established. • Robust treatment plan developed.
In progress
Incomplete assessment may have lead to medication contributing to death.
Review in progress
Fall resulted in fracture of elbow. Fracture not diagnosed for four days following fall.
• Implement routine clinical checks following falls. • Strengthen documentation.
Completed
Fall resulting in a fractured hip. On day of discharge patient was waiting to go home and fell.
• No recommendations Completed
Fall resulting in fractured hip Identified as falls risk and regularly reassessed. Appropriate strategies in
• Falls risk is specifically identified on handover notes.
• Invisabeam use is identified and recorded on
Completed
69
MidCentral DHB
Description Review Findings Recommendations Follow up
place. nursing care plan.
70
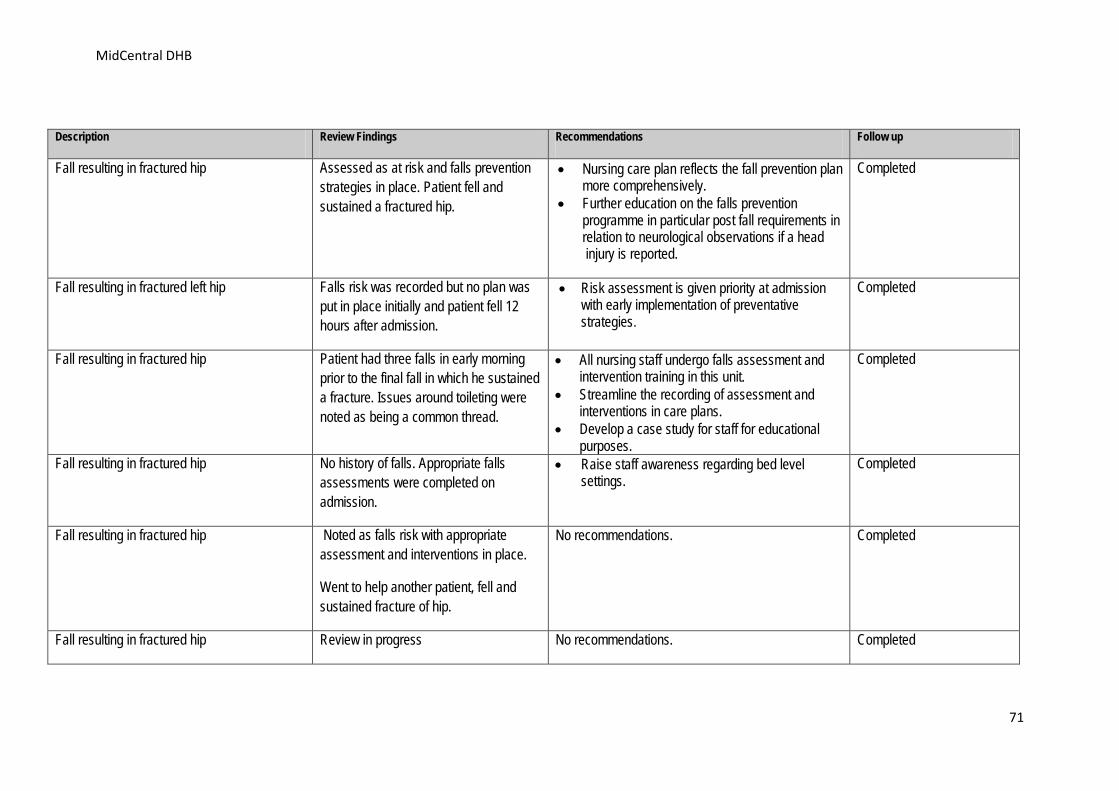
MidCentral DHB
Description Review Findings Recommendations Follow up
Fall resulting in fractured hip Assessed as at risk and falls prevention strategies in place. Patient fell and sustained a fractured hip.
• Nursing care plan reflects the fall prevention plan more comprehensively.
• Further education on the falls prevention programme in particular post fall requirements in relation to neurological observations if a head injury is reported.
Completed
Fall resulting in fractured left hip Falls risk was recorded but no plan was put in place initially and patient fell 12 hours after admission.
• Risk assessment is given priority at admission with early implementation of preventative strategies.
Completed
Fall resulting in fractured hip Patient had three falls in early morning prior to the final fall in which he sustained a fracture. Issues around toileting were noted as being a common thread.
• All nursing staff undergo falls assessment and intervention training in this unit.
• Streamline the recording of assessment and interventions in care plans.
• Develop a case study for staff for educational purposes.
Completed
Fall resulting in fractured hip No history of falls. Appropriate falls assessments were completed on admission.
• Raise staff awareness regarding bed level settings.
Completed
Fall resulting in fractured hip Noted as falls risk with appropriate assessment and interventions in place.
Went to help another patient, fell and sustained fracture of hip.
No recommendations. Completed
Fall resulting in fractured hip Review in progress No recommendations. Completed
71
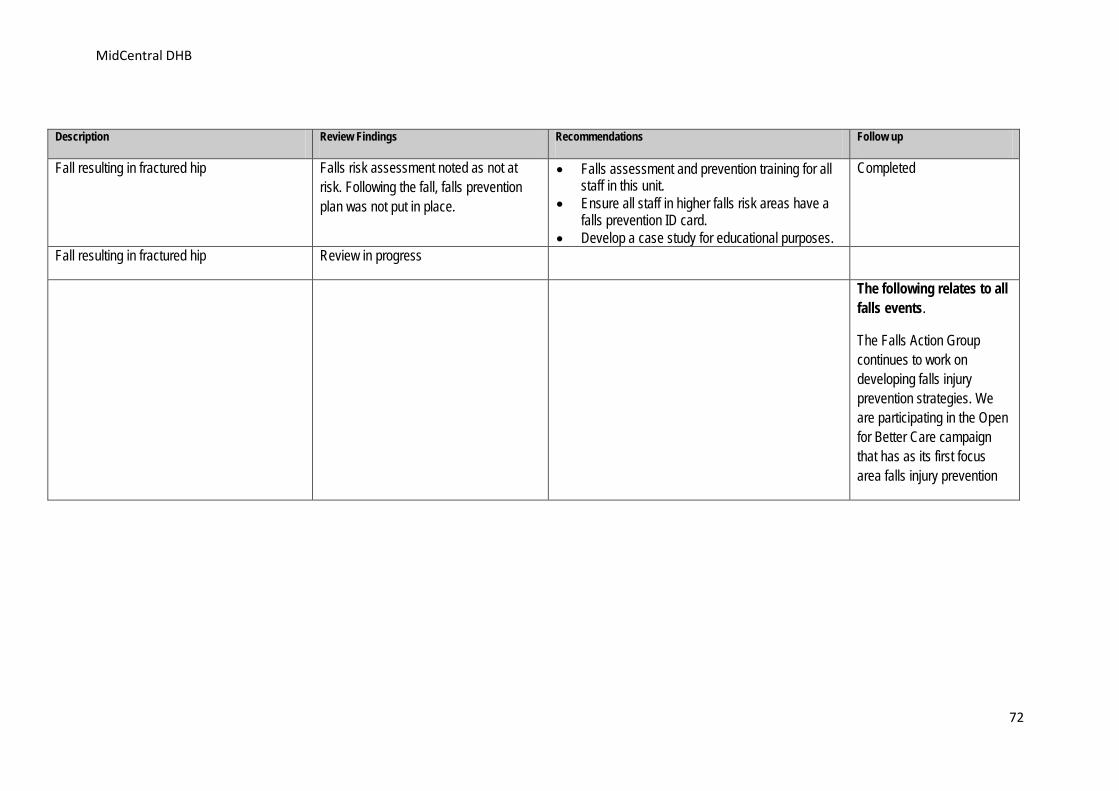
MidCentral DHB
Description Review Findings Recommendations Follow up
Fall resulting in fractured hip Falls risk assessment noted as not at risk. Following the fall, falls prevention plan was not put in place.
• Falls assessment and prevention training for all staff in this unit.
• Ensure all staff in higher falls risk areas have a falls prevention ID card.
• Develop a case study for educational purposes.
Completed
Fall resulting in fractured hip Review in progress
The following relates to all falls events.
The Falls Action Group continues to work on developing falls injury prevention strategies. We are participating in the Open for Better Care campaign that has as its first focus area falls injury prevention
72
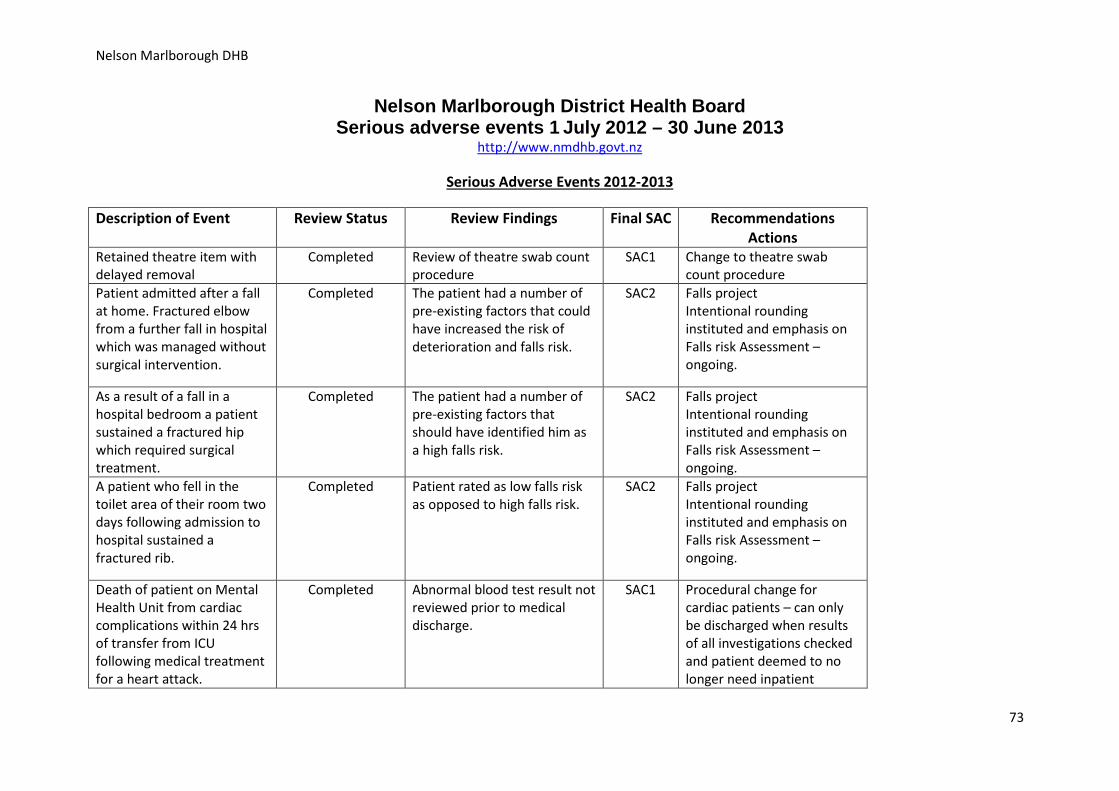
Nelson Marlborough DHB
Nelson Marlborough District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.nmdhb.govt.nz
Serious Adverse Events 2012-2013
Description of Event Review Status Review Findings Final SAC Recommendations Actions
Retained theatre item with delayed removal
Completed Review of theatre swab count procedure
SAC1 Change to theatre swab count procedure
Patient admitted after a fall at home. Fractured elbow from a further fall in hospital which was managed without surgical intervention.
Completed The patient had a number of pre-existing factors that could have increased the risk of deterioration and falls risk.
SAC2 Falls project Intentional rounding instituted and emphasis on Falls risk Assessment – ongoing.
As a result of a fall in a hospital bedroom a patient sustained a fractured hip which required surgical treatment.
Completed The patient had a number of pre-existing factors that should have identified him as a high falls risk.
SAC2 Falls project Intentional rounding instituted and emphasis on Falls risk Assessment – ongoing.
A patient who fell in the toilet area of their room two days following admission to hospital sustained a fractured rib.
Completed Patient rated as low falls risk as opposed to high falls risk.
SAC2 Falls project Intentional rounding instituted and emphasis on Falls risk Assessment – ongoing.
Death of patient on Mental Health Unit from cardiac complications within 24 hrs of transfer from ICU following medical treatment for a heart attack.
Completed Abnormal blood test result not reviewed prior to medical discharge.
SAC1 Procedural change for cardiac patients – can only be discharged when results of all investigations checked and patient deemed to no longer need inpatient
73
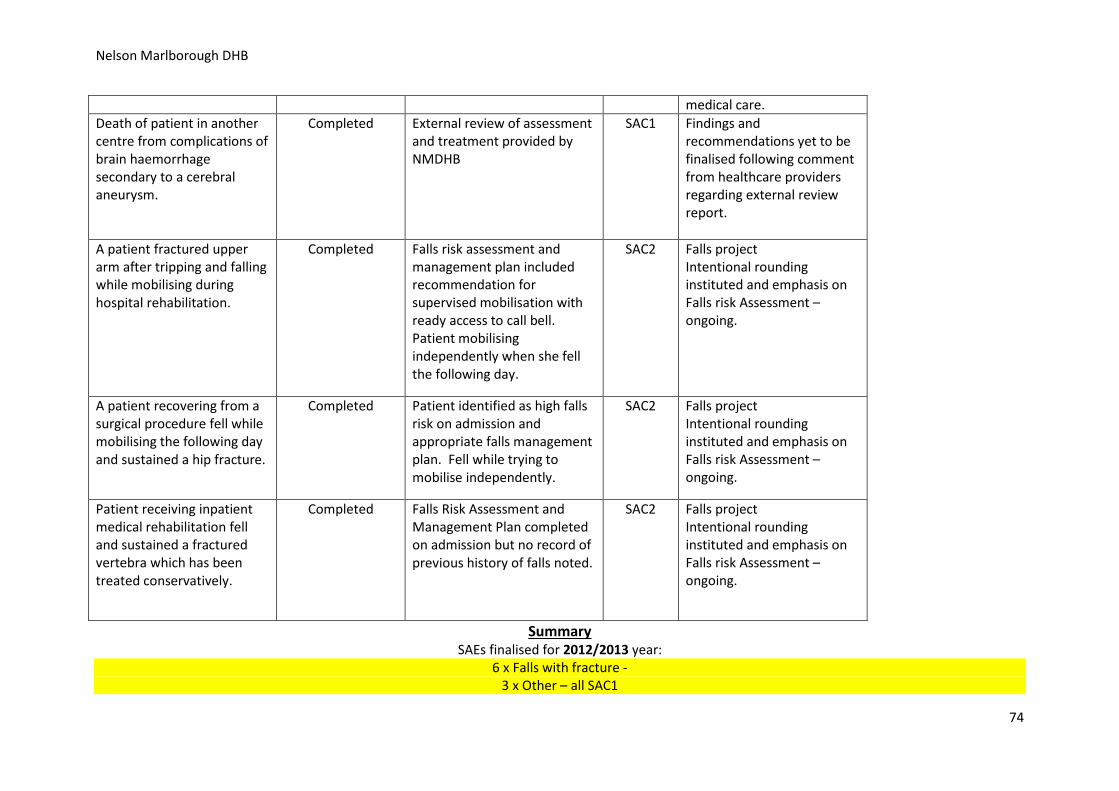
Nelson Marlborough DHB
medical care. Death of patient in another centre from complications of brain haemorrhage secondary to a cerebral aneurysm.
Completed External review of assessment and treatment provided by NMDHB
SAC1 Findings and recommendations yet to be finalised following comment from healthcare providers regarding external review report.
A patient fractured upper arm after tripping and falling while mobilising during hospital rehabilitation.
Completed Falls risk assessment and management plan included recommendation for supervised mobilisation with ready access to call bell. Patient mobilising independently when she fell the following day.
SAC2 Falls project Intentional rounding instituted and emphasis on Falls risk Assessment – ongoing.
A patient recovering from a surgical procedure fell while mobilising the following day and sustained a hip fracture.
Completed Patient identified as high falls risk on admission and appropriate falls management plan. Fell while trying to mobilise independently.
SAC2 Falls project Intentional rounding instituted and emphasis on Falls risk Assessment – ongoing.
Patient receiving inpatient medical rehabilitation fell and sustained a fractured vertebra which has been treated conservatively.
Completed Falls Risk Assessment and Management Plan completed on admission but no record of previous history of falls noted.
SAC2 Falls project Intentional rounding instituted and emphasis on Falls risk Assessment – ongoing.
Summary SAEs finalised for 2012/2013 year:
6 x Falls with fracture - 3 x Other – all SAC1
74
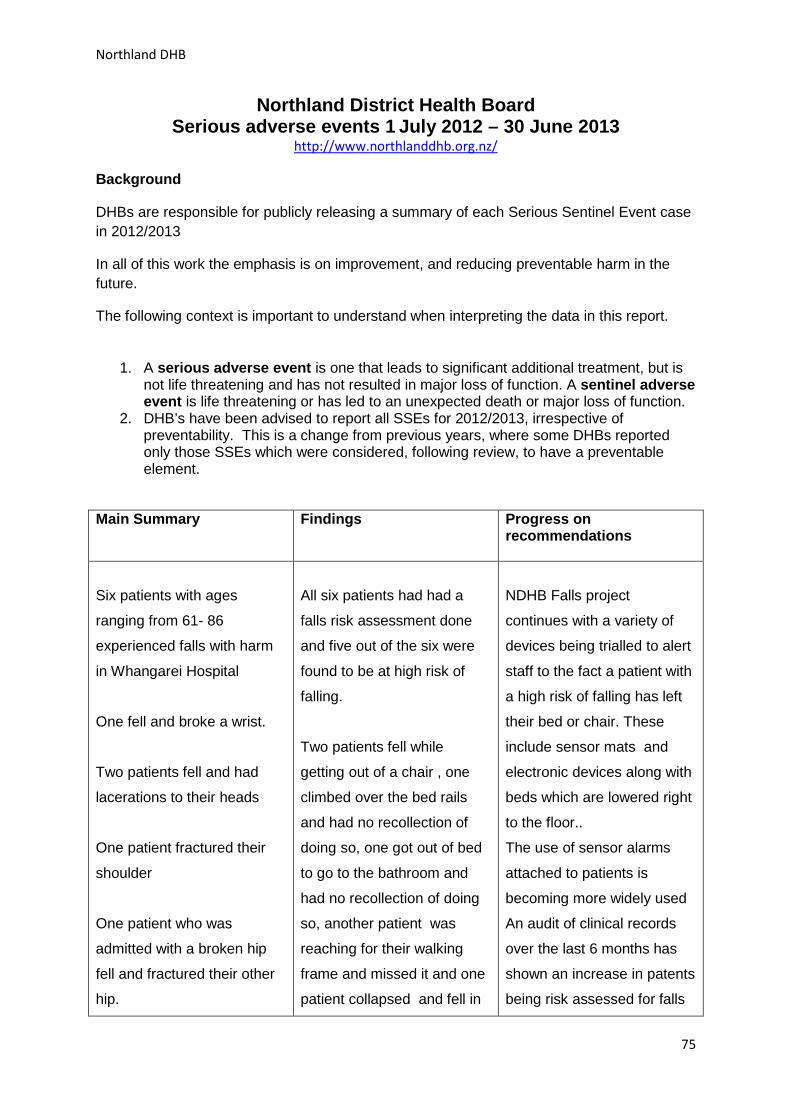
Northland DHB
Northland District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.northlanddhb.org.nz/
Background
DHBs are responsible for publicly releasing a summary of each Serious Sentinel Event case in 2012/2013
In all of this work the emphasis is on improvement, and reducing preventable harm in the future.
The following context is important to understand when interpreting the data in this report.
1. A serious adverse event is one that leads to significant additional treatment, but is not life threatening and has not resulted in major loss of function. A sentinel adverse event is life threatening or has led to an unexpected death or major loss of function.
2. DHB’s have been advised to report all SSEs for 2012/2013, irrespective of preventability. This is a change from previous years, where some DHBs reported only those SSEs which were considered, following review, to have a preventable element.
Main Summary
Findings
Progress on recommendations
Six patients with ages
ranging from 61- 86
experienced falls with harm
in Whangarei Hospital
One fell and broke a wrist.
Two patients fell and had
lacerations to their heads
One patient fractured their
shoulder
One patient who was
admitted with a broken hip
fell and fractured their other
hip.
All six patients had had a
falls risk assessment done
and five out of the six were
found to be at high risk of
falling.
Two patients fell while
getting out of a chair , one
climbed over the bed rails
and had no recollection of
doing so, one got out of bed
to go to the bathroom and
had no recollection of doing
so, another patient was
reaching for their walking
frame and missed it and one
patient collapsed and fell in
NDHB Falls project
continues with a variety of
devices being trialled to alert
staff to the fact a patient with
a high risk of falling has left
their bed or chair. These
include sensor mats and
electronic devices along with
beds which are lowered right
to the floor..
The use of sensor alarms
attached to patients is
becoming more widely used
An audit of clinical records
over the last 6 months has
shown an increase in patents
being risk assessed for falls
75
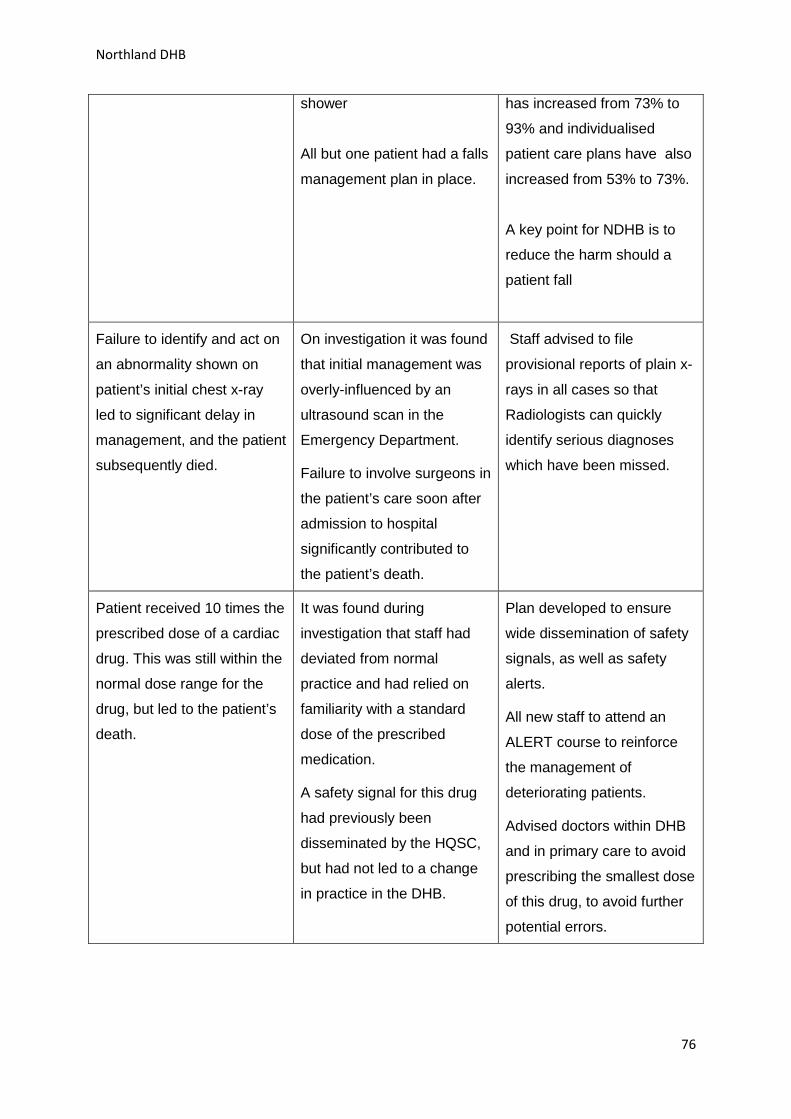
Northland DHB
shower
All but one patient had a falls
management plan in place.
has increased from 73% to
93% and individualised
patient care plans have also
increased from 53% to 73%.
A key point for NDHB is to
reduce the harm should a
patient fall
Failure to identify and act on
an abnormality shown on
patient’s initial chest x-ray
led to significant delay in
management, and the patient
subsequently died.
On investigation it was found
that initial management was
overly-influenced by an
ultrasound scan in the
Emergency Department.
Failure to involve surgeons in
the patient’s care soon after
admission to hospital
significantly contributed to
the patient’s death.
Staff advised to file
provisional reports of plain x-
rays in all cases so that
Radiologists can quickly
identify serious diagnoses
which have been missed.
Patient received 10 times the
prescribed dose of a cardiac
drug. This was still within the
normal dose range for the
drug, but led to the patient’s
death.
It was found during
investigation that staff had
deviated from normal
practice and had relied on
familiarity with a standard
dose of the prescribed
medication.
A safety signal for this drug
had previously been
disseminated by the HQSC,
but had not led to a change
in practice in the DHB.
Plan developed to ensure
wide dissemination of safety
signals, as well as safety
alerts.
All new staff to attend an
ALERT course to reinforce
the management of
deteriorating patients.
Advised doctors within DHB
and in primary care to avoid
prescribing the smallest dose
of this drug, to avoid further
potential errors.
76
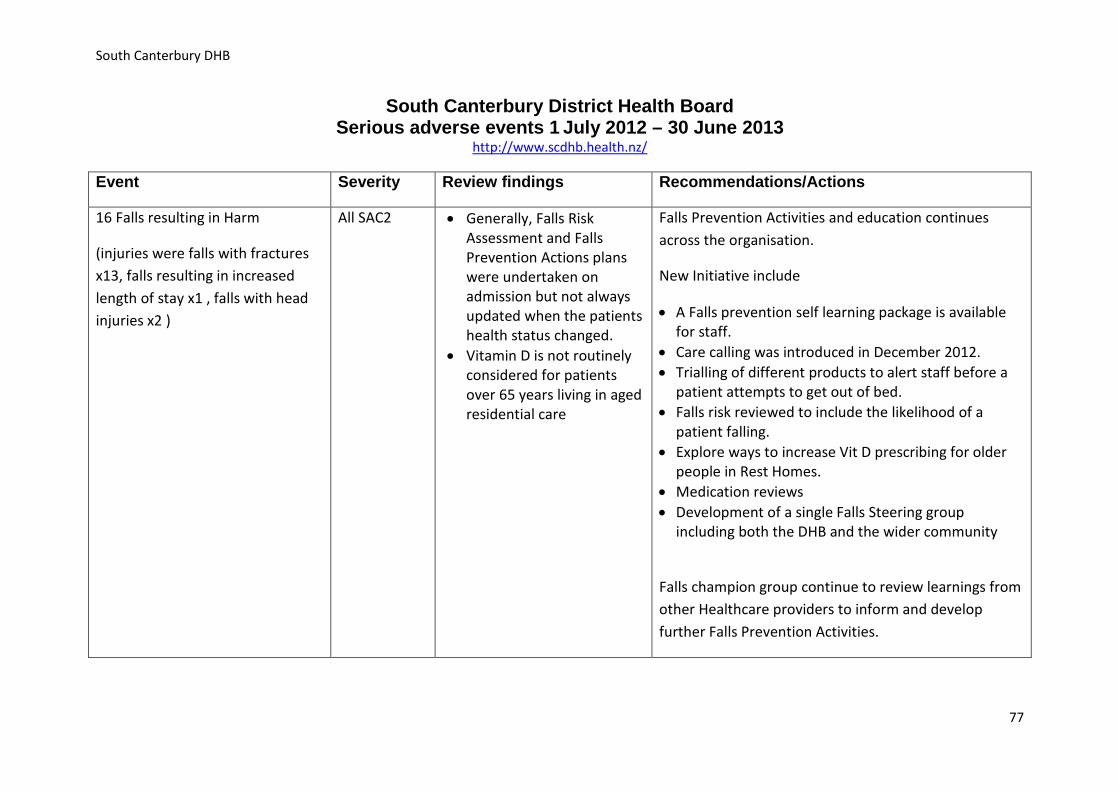
South Canterbury DHB
South Canterbury District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.scdhb.health.nz/
Event Severity Review findings Recommendations/Actions
16 Falls resulting in Harm
(injuries were falls with fractures x13, falls resulting in increased length of stay x1 , falls with head injuries x2 )
All SAC2 • Generally, Falls Risk Assessment and Falls Prevention Actions plans were undertaken on admission but not always updated when the patients health status changed.
• Vitamin D is not routinely considered for patients over 65 years living in aged residential care
Falls Prevention Activities and education continues across the organisation.
New Initiative include
• A Falls prevention self learning package is available for staff.
• Care calling was introduced in December 2012. • Trialling of different products to alert staff before a
patient attempts to get out of bed. • Falls risk reviewed to include the likelihood of a
patient falling. • Explore ways to increase Vit D prescribing for older
people in Rest Homes. • Medication reviews • Development of a single Falls Steering group
including both the DHB and the wider community
Falls champion group continue to review learnings from other Healthcare providers to inform and develop further Falls Prevention Activities.
77
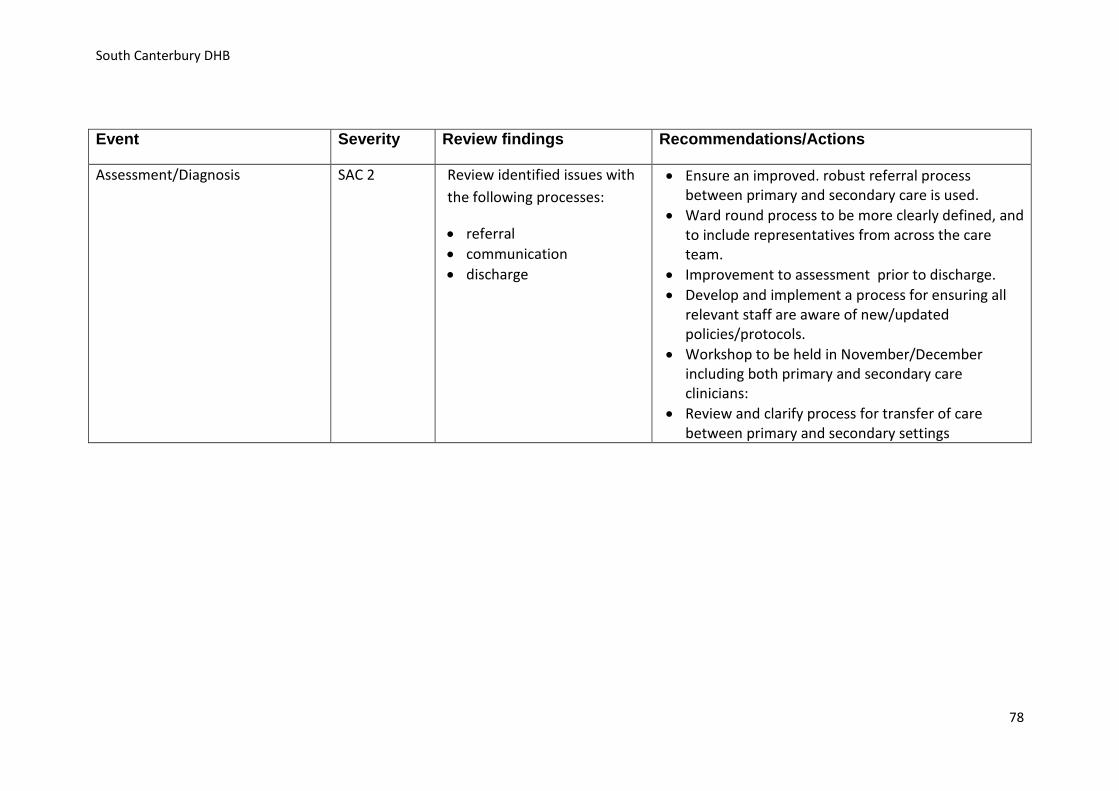
South Canterbury DHB
Event Severity Review findings Recommendations/Actions
Assessment/Diagnosis SAC 2 Review identified issues with the following processes:
• referral • communication • discharge
• Ensure an improved. robust referral process between primary and secondary care is used.
• Ward round process to be more clearly defined, and to include representatives from across the care team.
• Improvement to assessment prior to discharge. • Develop and implement a process for ensuring all
relevant staff are aware of new/updated policies/protocols.
• Workshop to be held in November/December including both primary and secondary care clinicians:
• Review and clarify process for transfer of care between primary and secondary settings
78
Southern DHB
Southern District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.southerndhb.govt.nz/
Serious Adverse Events 2012- 2013
Welcome to the serious adverse event release for 1 July 2012 - 30 June 2013 from the Southern District Health Board.
It is recognised worldwide that health care is a complex process, has associated risks and that patients may become harmed when receiving care intended to help them. This report provides details of the serious adverse events that have occurred within the Southern District Health Board (SDHB), the recommendations to make improvements to the care we provide and our progress.
The report is released in conjunction with the Health Quality & Safety Commission (HQSC) National Report on Serious Adverse Events
http://www.hqsc.govt.nz
For the 2012-2013 financial year, SDHB has reported 33 events that have caused serious harm or death and 2 events that nearly caused serious harm; with a total of 35 events.
What is a serious adverse event?
Serious adverse events are events which have resulted in serious harm to patients. This harm may have led to significant additional treatment, have been life threatening or led to a major loss of function or unexpected death.
District Health Boards classify the severity of adverse events or incidents using the Severity Assessment Code (SAC). The two major SAC classifications, SAC1 and SAC2 are called serious adverse events which is one that is life threatening or has led to an unexpected death or major loss of function – and is classified as a SAC 1 and one that requires significant additional treatment, but is not life threatening and has not resulted in a major loss of function – and is classified as a SAC 2.
As a provider of health services we are required to review these events and report them to the Health Quality and Safety Commission.
79
Southern DHB
You may notice that some incidents have not had their investigation completed at the time of release of this report. This means that the incident is still under investigation or that the recommendations are in the process of being finalised.
Using Serious Adverse Events to promote Patient Safety & Prevent Harm
All serious adverse events are investigated to try to determine the major cause, or causes, that led to the event. When these causes are known, interventions are recommended to try to prevent the recurrence of the same or similar adverse event in the future. The aim is therefore to enhance patient safety by learning from adverse events and near misses that occur in health and disability services and not to blame individuals who are involved in the event.
We have provided graphs to summarise the incidents that have occurred within the Southern DHB. The rise and fall in the number of incidents can indicate a number of factors including better reporting as well as the actual frequency of incidents.
The Southern DHB is committed to the Open For Better Care campaign developed through HQSC; this forms part of the transparent process of identifying harm and working to learn and improve our patient safety.
In the July 1, 2012 to June 30, 2013 year, 35 serious adverse events took place in the Southern District Health Board (see Graph A).
80
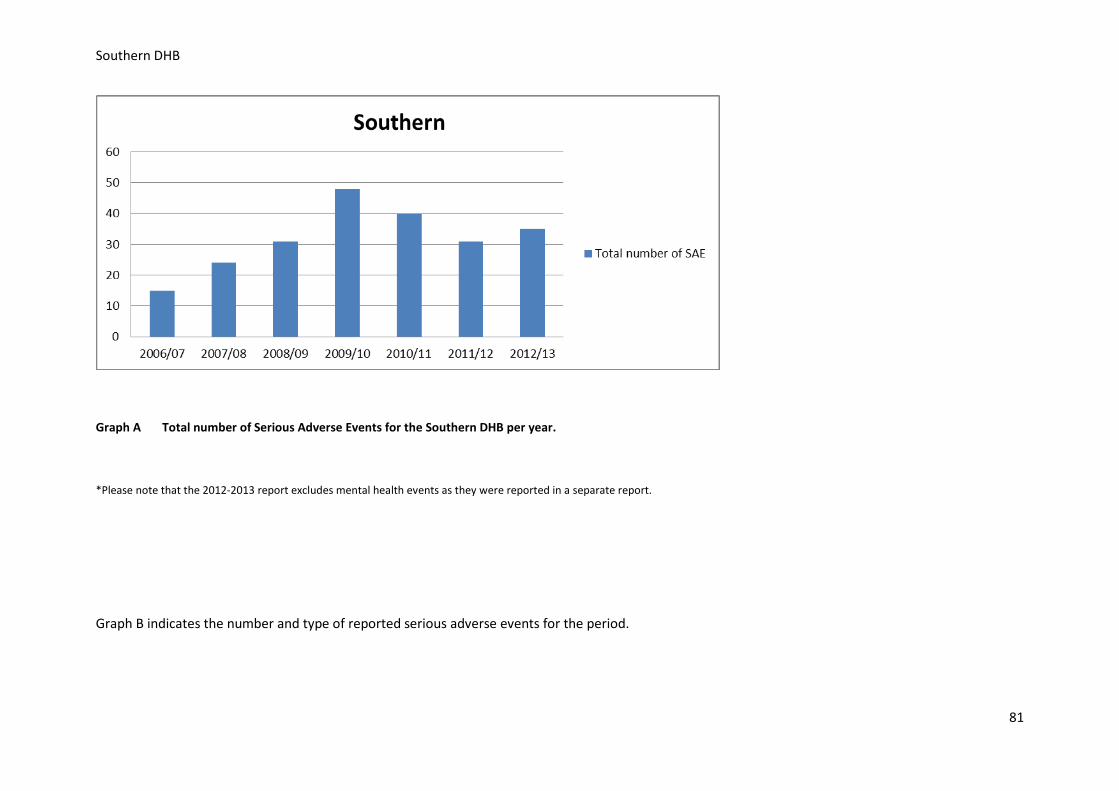
Southern DHB
Graph A Total number of Serious Adverse Events for the Southern DHB per year.
*Please note that the 2012-2013 report excludes mental health events as they were reported in a separate report.
Graph B indicates the number and type of reported serious adverse events for the period.
81
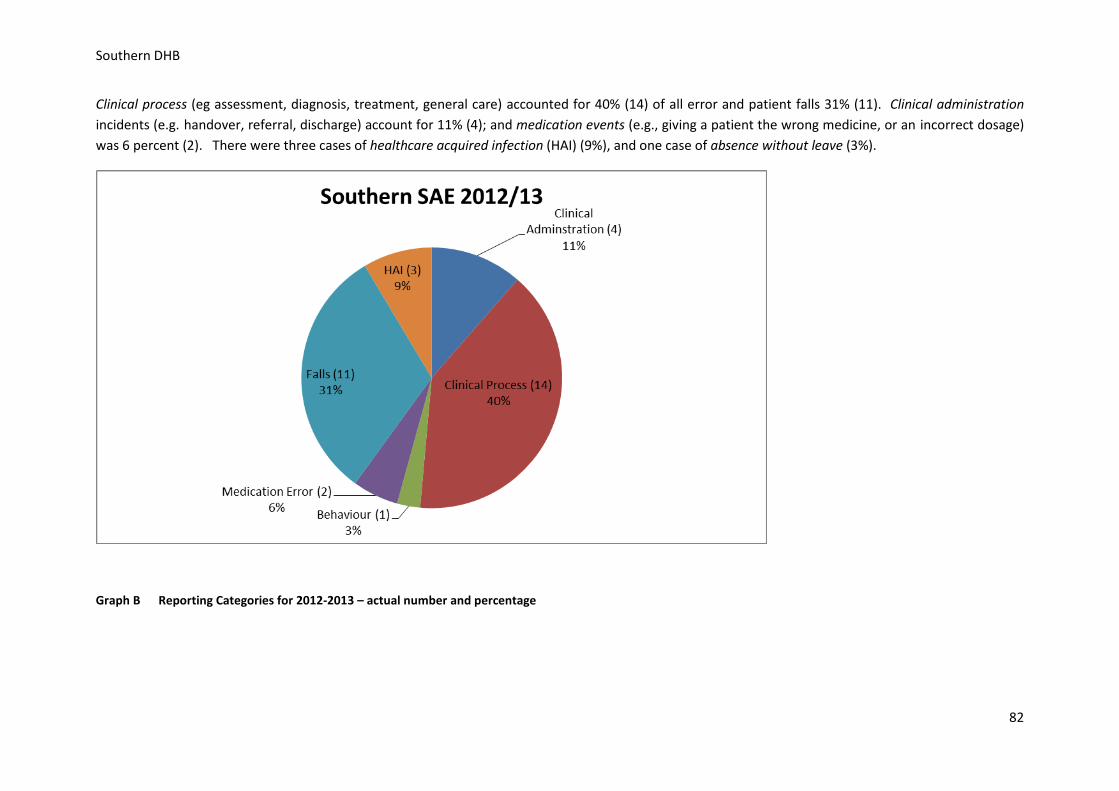
Southern DHB
Clinical process (eg assessment, diagnosis, treatment, general care) accounted for 40% (14) of all error and patient falls 31% (11). Clinical administration incidents (e.g. handover, referral, discharge) account for 11% (4); and medication events (e.g., giving a patient the wrong medicine, or an incorrect dosage) was 6 percent (2). There were three cases of healthcare acquired infection (HAI) (9%), and one case of absence without leave (3%).
Graph B Reporting Categories for 2012-2013 – actual number and percentage
82
Southern DHB
Lexie O'Shea Mr Richard Bunton Executive Director Patient Service/Deputy CEO. Medical Director of Patient Services.
Leanne Samuel Lynda McCutcheon Executive Director of Nursing & Midwifery. Executive Director - Allied Health, Scientific & Technical.
83
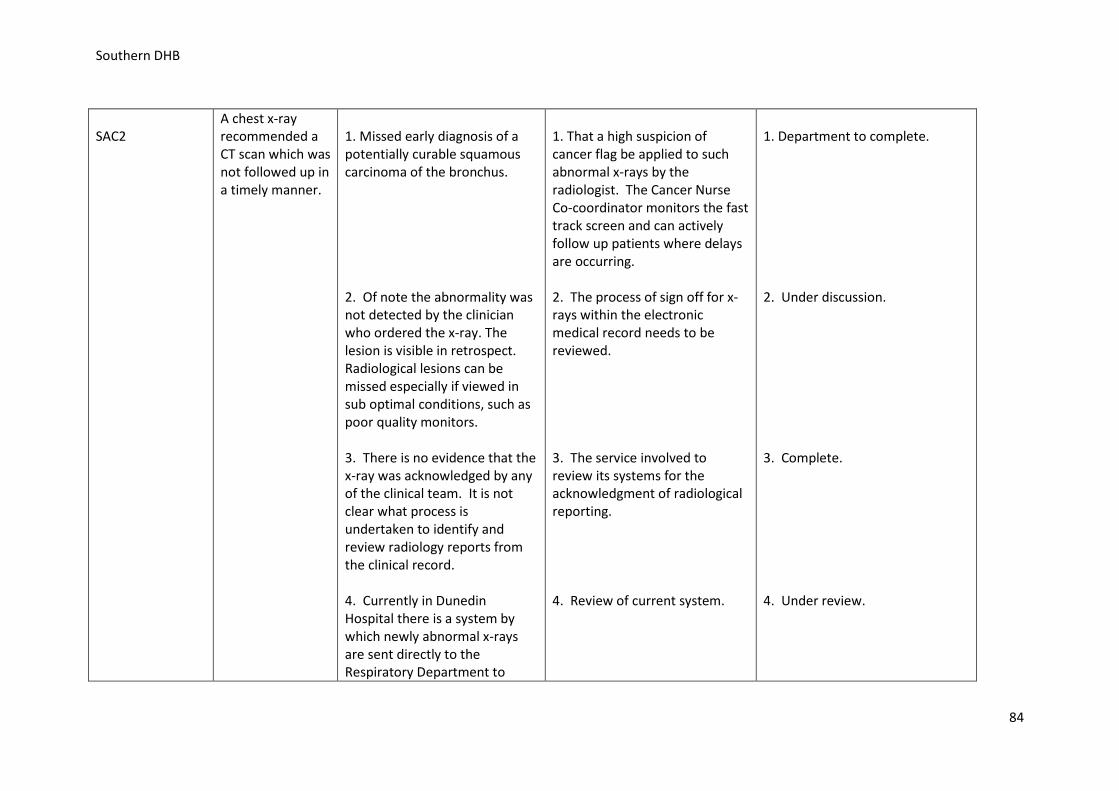
Southern DHB
SAC2
A chest x-ray recommended a CT scan which was not followed up in a timely manner.
1. Missed early diagnosis of a potentially curable squamous carcinoma of the bronchus. 2. Of note the abnormality was not detected by the clinician who ordered the x-ray. The lesion is visible in retrospect. Radiological lesions can be missed especially if viewed in sub optimal conditions, such as poor quality monitors. 3. There is no evidence that the x-ray was acknowledged by any of the clinical team. It is not clear what process is undertaken to identify and review radiology reports from the clinical record. 4. Currently in Dunedin Hospital there is a system by which newly abnormal x-rays are sent directly to the Respiratory Department to
1. That a high suspicion of cancer flag be applied to such abnormal x-rays by the radiologist. The Cancer Nurse Co-coordinator monitors the fast track screen and can actively follow up patients where delays are occurring. 2. The process of sign off for x-rays within the electronic medical record needs to be reviewed. 3. The service involved to review its systems for the acknowledgment of radiological reporting. 4. Review of current system.
1. Department to complete.
2. Under discussion. 3. Complete. 4. Under review.
84
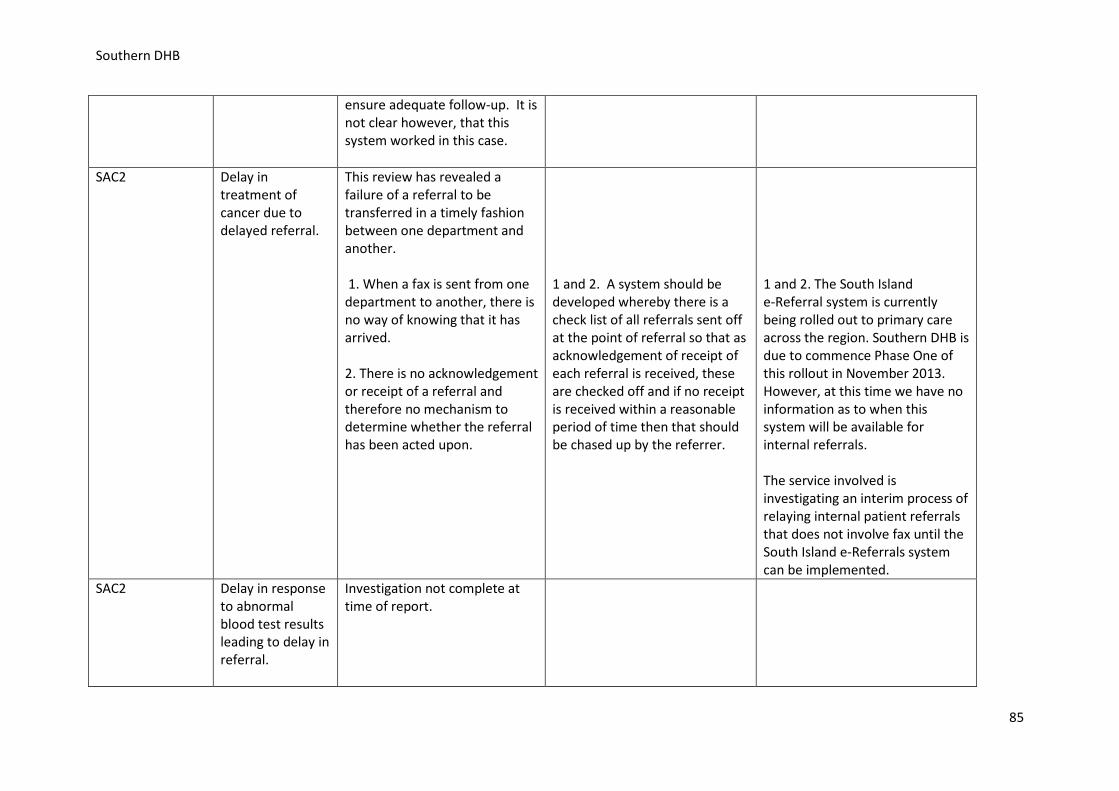
Southern DHB
ensure adequate follow-up. It is not clear however, that this system worked in this case.
SAC2 Delay in treatment of cancer due to delayed referral.
This review has revealed a failure of a referral to be transferred in a timely fashion between one department and another. 1. When a fax is sent from one department to another, there is no way of knowing that it has arrived. 2. There is no acknowledgement or receipt of a referral and therefore no mechanism to determine whether the referral has been acted upon.
1 and 2. A system should be developed whereby there is a check list of all referrals sent off at the point of referral so that as acknowledgement of receipt of each referral is received, these are checked off and if no receipt is received within a reasonable period of time then that should be chased up by the referrer.
1 and 2. The South Island e-Referral system is currently being rolled out to primary care across the region. Southern DHB is due to commence Phase One of this rollout in November 2013. However, at this time we have no information as to when this system will be available for internal referrals. The service involved is investigating an interim process of relaying internal patient referrals that does not involve fax until the South Island e-Referrals system can be implemented.
SAC2 Delay in response to abnormal blood test results leading to delay in referral.
Investigation not complete at time of report.
85
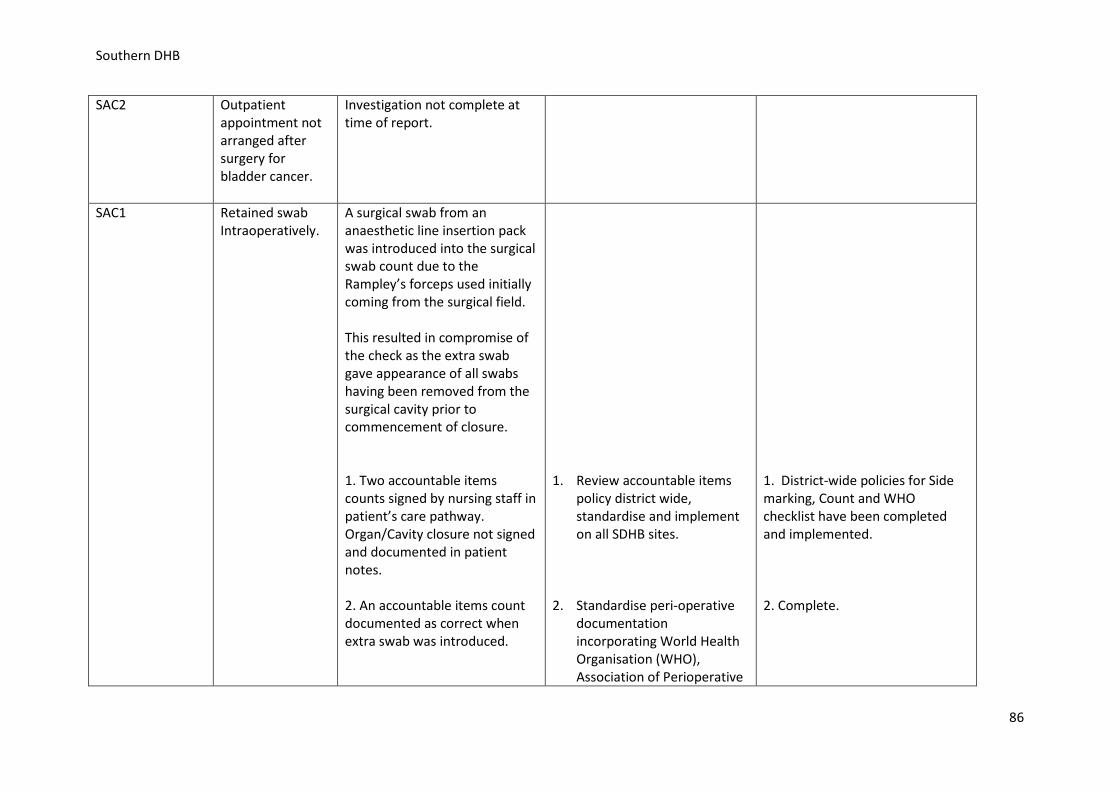
Southern DHB
SAC2 Outpatient appointment not arranged after surgery for bladder cancer.
Investigation not complete at time of report.
SAC1 Retained swab Intraoperatively.
A surgical swab from an anaesthetic line insertion pack was introduced into the surgical swab count due to the Rampley’s forceps used initially coming from the surgical field. This resulted in compromise of the check as the extra swab gave appearance of all swabs having been removed from the surgical cavity prior to commencement of closure. 1. Two accountable items counts signed by nursing staff in patient’s care pathway. Organ/Cavity closure not signed and documented in patient notes. 2. An accountable items count documented as correct when extra swab was introduced.
1. Review accountable items
policy district wide, standardise and implement on all SDHB sites.
2. Standardise peri-operative
documentation incorporating World Health Organisation (WHO), Association of Perioperative
1. District-wide policies for Side marking, Count and WHO checklist have been completed and implemented. 2. Complete.
86
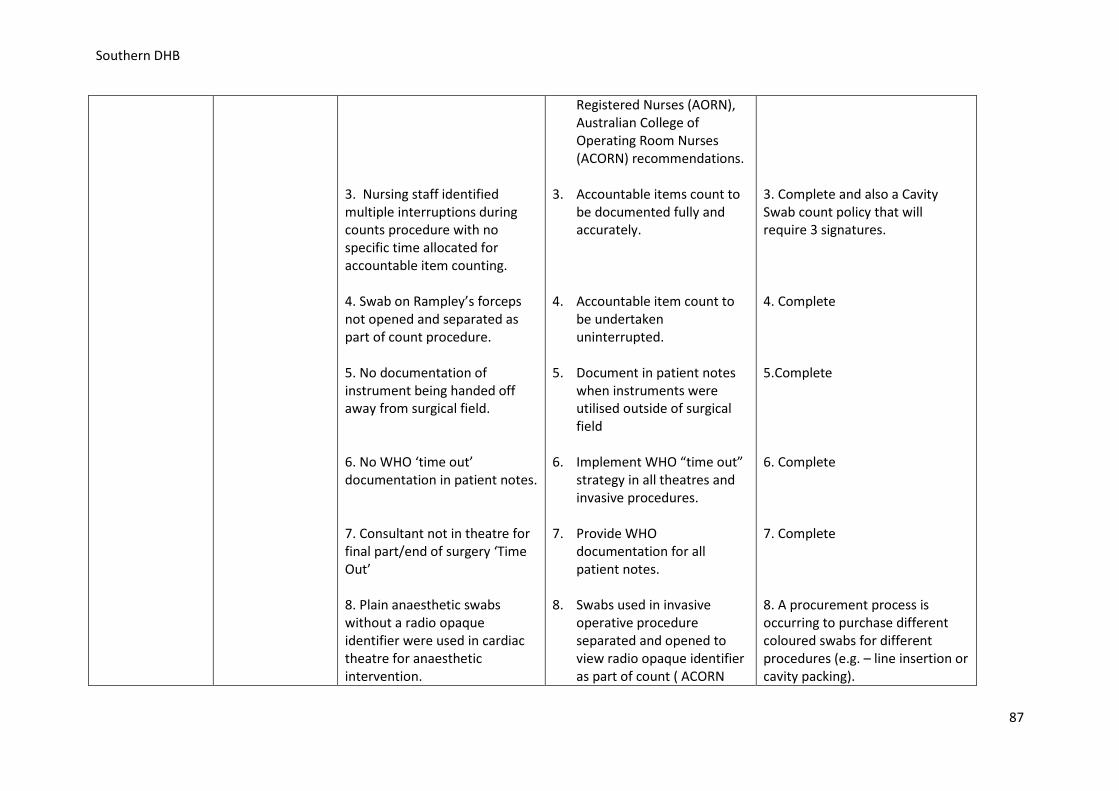
Southern DHB
3. Nursing staff identified multiple interruptions during counts procedure with no specific time allocated for accountable item counting. 4. Swab on Rampley’s forceps not opened and separated as part of count procedure. 5. No documentation of instrument being handed off away from surgical field. 6. No WHO ‘time out’ documentation in patient notes. 7. Consultant not in theatre for final part/end of surgery ‘Time Out’ 8. Plain anaesthetic swabs without a radio opaque identifier were used in cardiac theatre for anaesthetic intervention.
Registered Nurses (AORN), Australian College of Operating Room Nurses (ACORN) recommendations.
3. Accountable items count to
be documented fully and accurately.
4. Accountable item count to
be undertaken uninterrupted.
5. Document in patient notes
when instruments were utilised outside of surgical field
6. Implement WHO “time out”
strategy in all theatres and invasive procedures.
7. Provide WHO
documentation for all patient notes.
8. Swabs used in invasive
operative procedure separated and opened to view radio opaque identifier as part of count ( ACORN
3. Complete and also a Cavity Swab count policy that will require 3 signatures. 4. Complete 5.Complete 6. Complete 7. Complete 8. A procurement process is occurring to purchase different coloured swabs for different procedures (e.g. – line insertion or cavity packing).
87
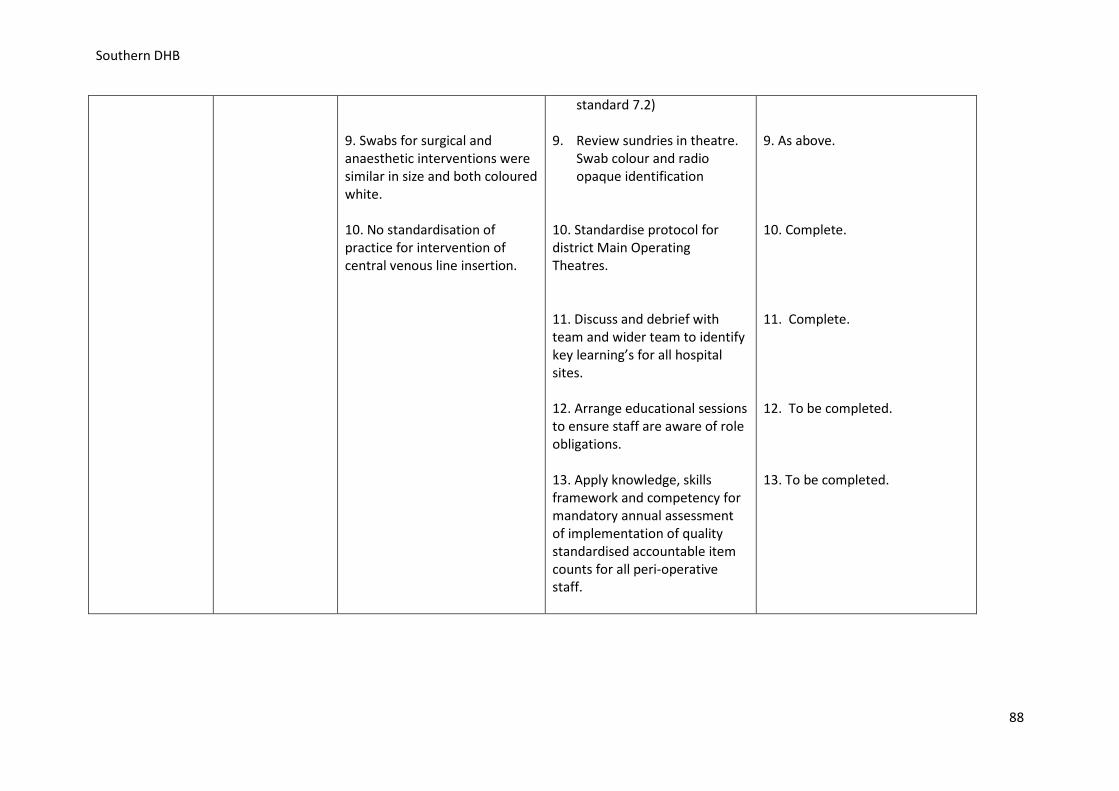
Southern DHB
9. Swabs for surgical and anaesthetic interventions were similar in size and both coloured white. 10. No standardisation of practice for intervention of central venous line insertion.
standard 7.2) 9. Review sundries in theatre.
Swab colour and radio opaque identification
10. Standardise protocol for district Main Operating Theatres. 11. Discuss and debrief with team and wider team to identify key learning’s for all hospital sites. 12. Arrange educational sessions to ensure staff are aware of role obligations. 13. Apply knowledge, skills framework and competency for mandatory annual assessment of implementation of quality standardised accountable item counts for all peri-operative staff.
9. As above. 10. Complete. 11. Complete. 12. To be completed. 13. To be completed.
88
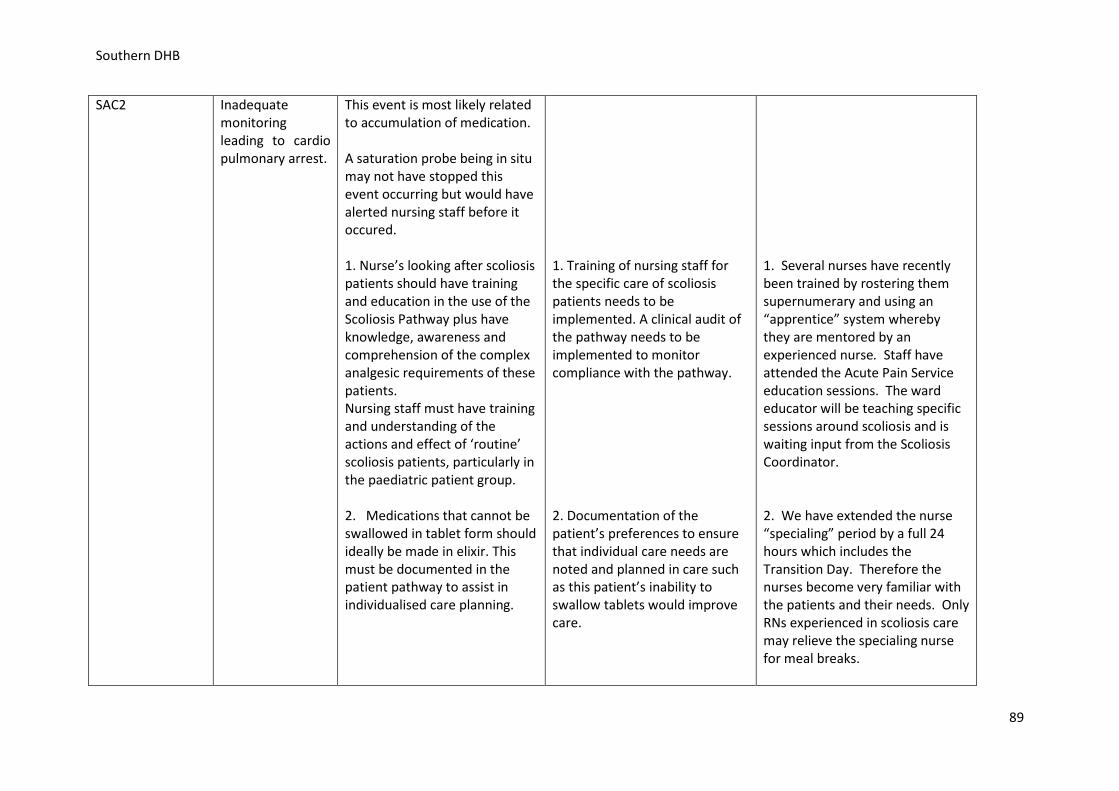
Southern DHB
SAC2
Inadequate monitoring leading to cardio pulmonary arrest.
This event is most likely related to accumulation of medication. A saturation probe being in situ may not have stopped this event occurring but would have alerted nursing staff before it occured. 1. Nurse’s looking after scoliosis patients should have training and education in the use of the Scoliosis Pathway plus have knowledge, awareness and comprehension of the complex analgesic requirements of these patients. Nursing staff must have training and understanding of the actions and effect of ‘routine’ scoliosis patients, particularly in the paediatric patient group. 2. Medications that cannot be swallowed in tablet form should ideally be made in elixir. This must be documented in the patient pathway to assist in individualised care planning.
1. Training of nursing staff for the specific care of scoliosis patients needs to be implemented. A clinical audit of the pathway needs to be implemented to monitor compliance with the pathway. 2. Documentation of the patient’s preferences to ensure that individual care needs are noted and planned in care such as this patient’s inability to swallow tablets would improve care.
1. Several nurses have recently been trained by rostering them supernumerary and using an “apprentice” system whereby they are mentored by an experienced nurse. Staff have attended the Acute Pain Service education sessions. The ward educator will be teaching specific sessions around scoliosis and is waiting input from the Scoliosis Coordinator. 2. We have extended the nurse “specialing” period by a full 24 hours which includes the Transition Day. Therefore the nurses become very familiar with the patients and their needs. Only RNs experienced in scoliosis care may relieve the specialing nurse for meal breaks.
89
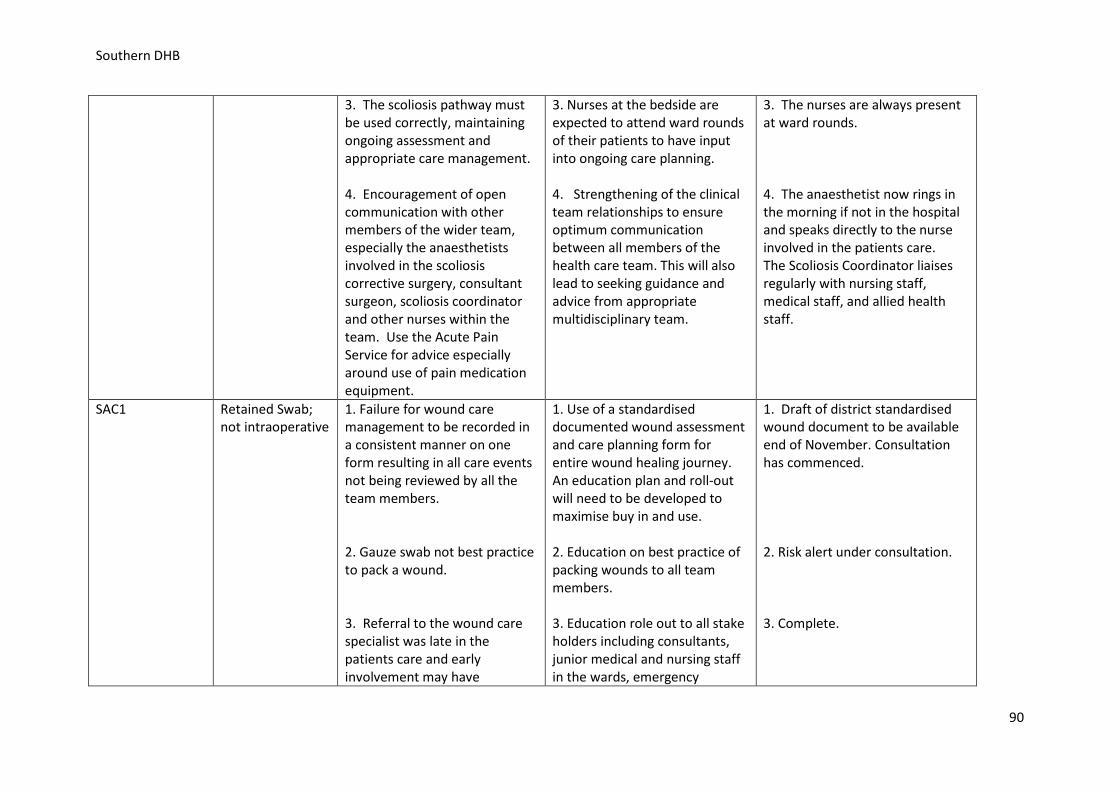
Southern DHB
3. The scoliosis pathway must be used correctly, maintaining ongoing assessment and appropriate care management. 4. Encouragement of open communication with other members of the wider team, especially the anaesthetists involved in the scoliosis corrective surgery, consultant surgeon, scoliosis coordinator and other nurses within the team. Use the Acute Pain Service for advice especially around use of pain medication equipment.
3. Nurses at the bedside are expected to attend ward rounds of their patients to have input into ongoing care planning. 4. Strengthening of the clinical team relationships to ensure optimum communication between all members of the health care team. This will also lead to seeking guidance and advice from appropriate multidisciplinary team.
3. The nurses are always present at ward rounds. 4. The anaesthetist now rings in the morning if not in the hospital and speaks directly to the nurse involved in the patients care. The Scoliosis Coordinator liaises regularly with nursing staff, medical staff, and allied health staff.
SAC1 Retained Swab; not intraoperative
1. Failure for wound care management to be recorded in a consistent manner on one form resulting in all care events not being reviewed by all the team members. 2. Gauze swab not best practice to pack a wound. 3. Referral to the wound care specialist was late in the patients care and early involvement may have
1. Use of a standardised documented wound assessment and care planning form for entire wound healing journey. An education plan and roll-out will need to be developed to maximise buy in and use.
2. Education on best practice of packing wounds to all team members. 3. Education role out to all stake holders including consultants, junior medical and nursing staff in the wards, emergency
1. Draft of district standardised wound document to be available end of November. Consultation has commenced. 2. Risk alert under consultation. 3. Complete.
90
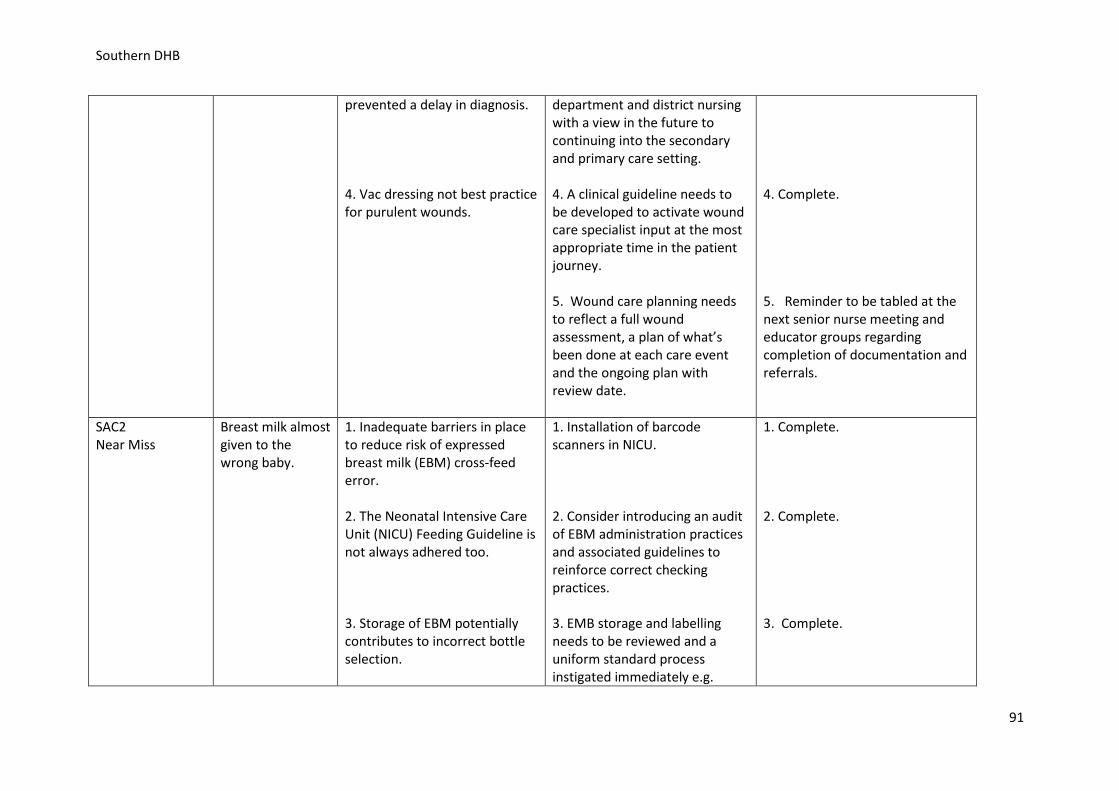
Southern DHB
prevented a delay in diagnosis. 4. Vac dressing not best practice for purulent wounds.
department and district nursing with a view in the future to continuing into the secondary and primary care setting. 4. A clinical guideline needs to be developed to activate wound care specialist input at the most appropriate time in the patient journey. 5. Wound care planning needs to reflect a full wound assessment, a plan of what’s been done at each care event and the ongoing plan with review date.
4. Complete. 5. Reminder to be tabled at the next senior nurse meeting and educator groups regarding completion of documentation and referrals.
SAC2 Near Miss
Breast milk almost given to the wrong baby.
1. Inadequate barriers in place to reduce risk of expressed breast milk (EBM) cross-feed error. 2. The Neonatal Intensive Care Unit (NICU) Feeding Guideline is not always adhered too. 3. Storage of EBM potentially contributes to incorrect bottle selection.
1. Installation of barcode scanners in NICU. 2. Consider introducing an audit of EBM administration practices and associated guidelines to reinforce correct checking practices. 3. EMB storage and labelling needs to be reviewed and a uniform standard process instigated immediately e.g.
1. Complete. 2. Complete. 3. Complete.
91
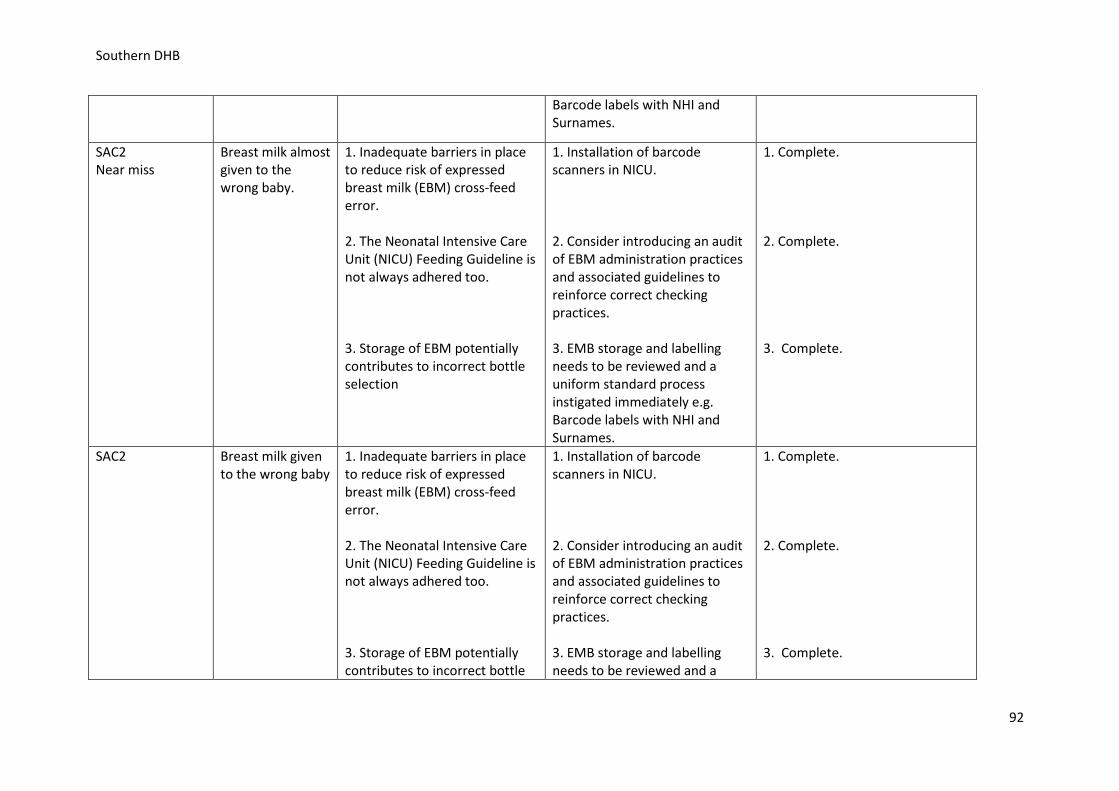
Southern DHB
Barcode labels with NHI and Surnames.
SAC2 Near miss
Breast milk almost given to the wrong baby.
1. Inadequate barriers in place to reduce risk of expressed breast milk (EBM) cross-feed error. 2. The Neonatal Intensive Care Unit (NICU) Feeding Guideline is not always adhered too. 3. Storage of EBM potentially contributes to incorrect bottle selection
1. Installation of barcode scanners in NICU. 2. Consider introducing an audit of EBM administration practices and associated guidelines to reinforce correct checking practices. 3. EMB storage and labelling needs to be reviewed and a uniform standard process instigated immediately e.g. Barcode labels with NHI and Surnames.
1. Complete. 2. Complete. 3. Complete.
SAC2
Breast milk given to the wrong baby
1. Inadequate barriers in place to reduce risk of expressed breast milk (EBM) cross-feed error. 2. The Neonatal Intensive Care Unit (NICU) Feeding Guideline is not always adhered too. 3. Storage of EBM potentially contributes to incorrect bottle
1. Installation of barcode scanners in NICU. 2. Consider introducing an audit of EBM administration practices and associated guidelines to reinforce correct checking practices. 3. EMB storage and labelling needs to be reviewed and a
1. Complete. 2. Complete. 3. Complete.
92
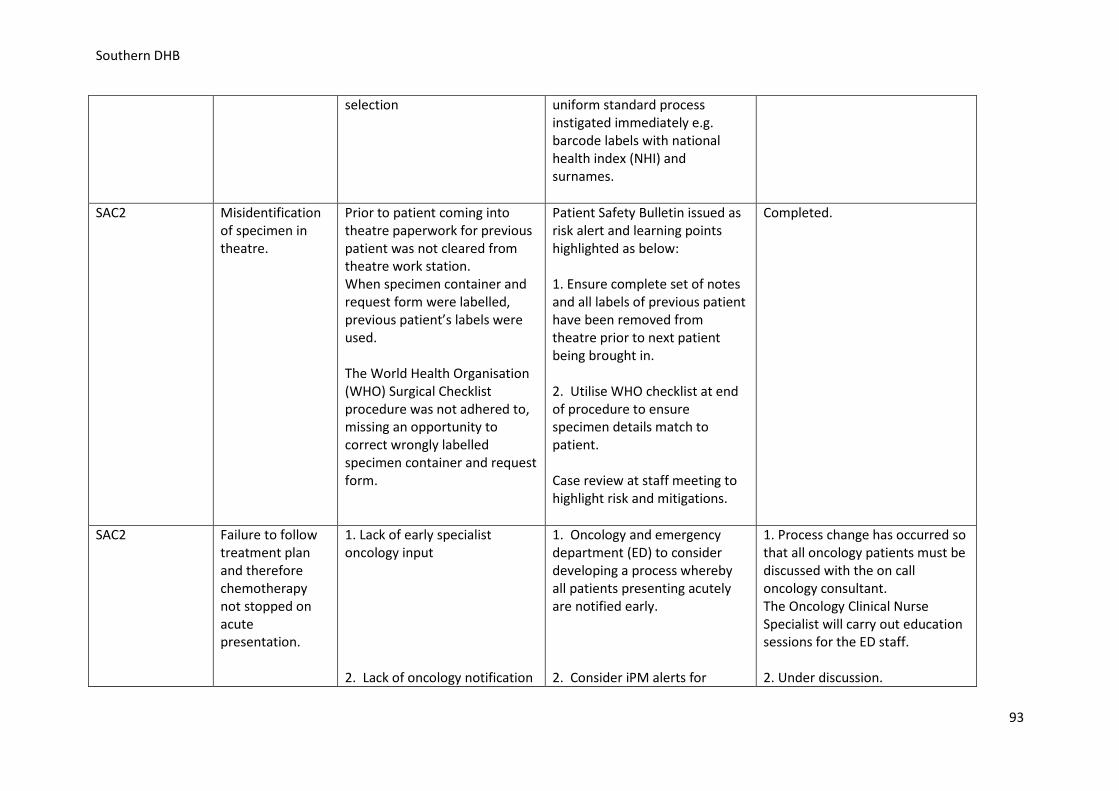
Southern DHB
selection
uniform standard process instigated immediately e.g. barcode labels with national health index (NHI) and surnames.
SAC2 Misidentification of specimen in theatre.
Prior to patient coming into theatre paperwork for previous patient was not cleared from theatre work station. When specimen container and request form were labelled, previous patient’s labels were used. The World Health Organisation (WHO) Surgical Checklist procedure was not adhered to, missing an opportunity to correct wrongly labelled specimen container and request form.
Patient Safety Bulletin issued as risk alert and learning points highlighted as below: 1. Ensure complete set of notes and all labels of previous patient have been removed from theatre prior to next patient being brought in. 2. Utilise WHO checklist at end of procedure to ensure specimen details match to patient. Case review at staff meeting to highlight risk and mitigations.
Completed.
SAC2
Failure to follow treatment plan and therefore chemotherapy not stopped on acute presentation.
1. Lack of early specialist oncology input 2. Lack of oncology notification
1. Oncology and emergency department (ED) to consider developing a process whereby all patients presenting acutely are notified early. 2. Consider iPM alerts for
1. Process change has occurred so that all oncology patients must be discussed with the on call oncology consultant. The Oncology Clinical Nurse Specialist will carry out education sessions for the ED staff. 2. Under discussion.
93
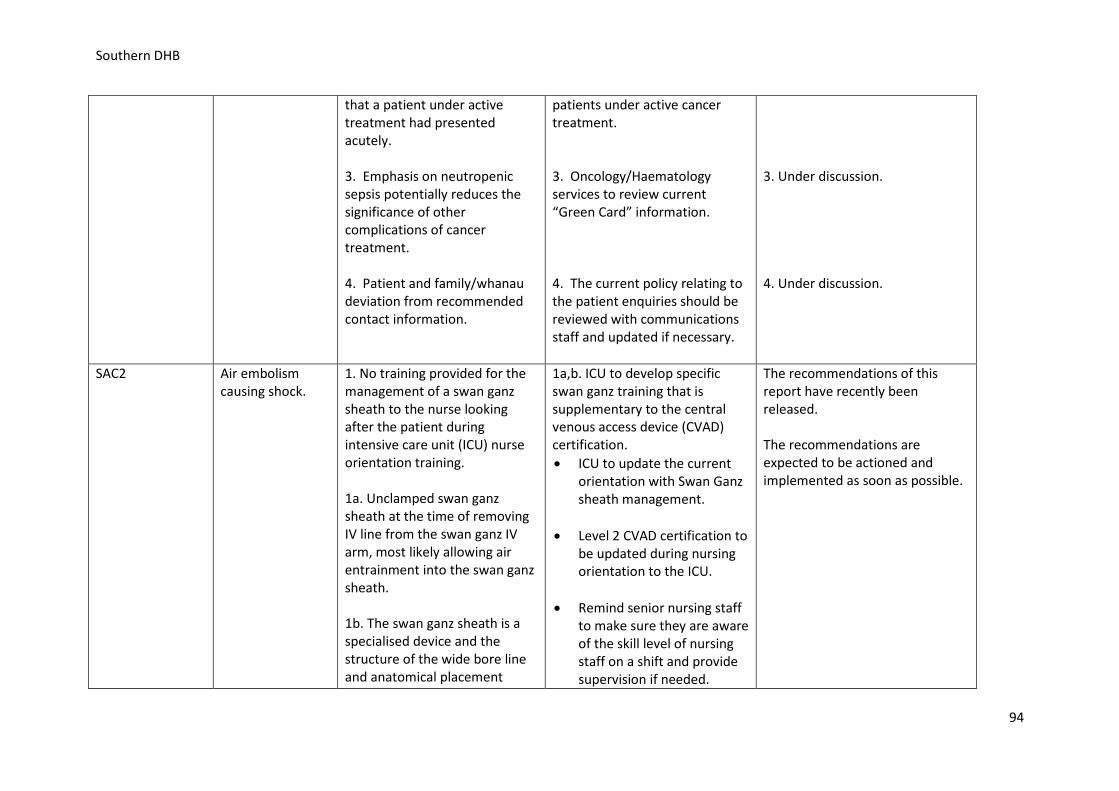
Southern DHB
that a patient under active treatment had presented acutely. 3. Emphasis on neutropenic sepsis potentially reduces the significance of other complications of cancer treatment. 4. Patient and family/whanau deviation from recommended contact information.
patients under active cancer treatment. 3. Oncology/Haematology services to review current “Green Card” information. 4. The current policy relating to the patient enquiries should be reviewed with communications staff and updated if necessary.
3. Under discussion. 4. Under discussion.
SAC2 Air embolism causing shock.
1. No training provided for the management of a swan ganz sheath to the nurse looking after the patient during intensive care unit (ICU) nurse orientation training. 1a. Unclamped swan ganz sheath at the time of removing IV line from the swan ganz IV arm, most likely allowing air entrainment into the swan ganz sheath. 1b. The swan ganz sheath is a specialised device and the structure of the wide bore line and anatomical placement
1a,b. ICU to develop specific swan ganz training that is supplementary to the central venous access device (CVAD) certification. • ICU to update the current
orientation with Swan Ganz sheath management.
• Level 2 CVAD certification to be updated during nursing orientation to the ICU.
• Remind senior nursing staff
to make sure they are aware of the skill level of nursing staff on a shift and provide supervision if needed.
The recommendations of this report have recently been released. The recommendations are expected to be actioned and implemented as soon as possible.
94
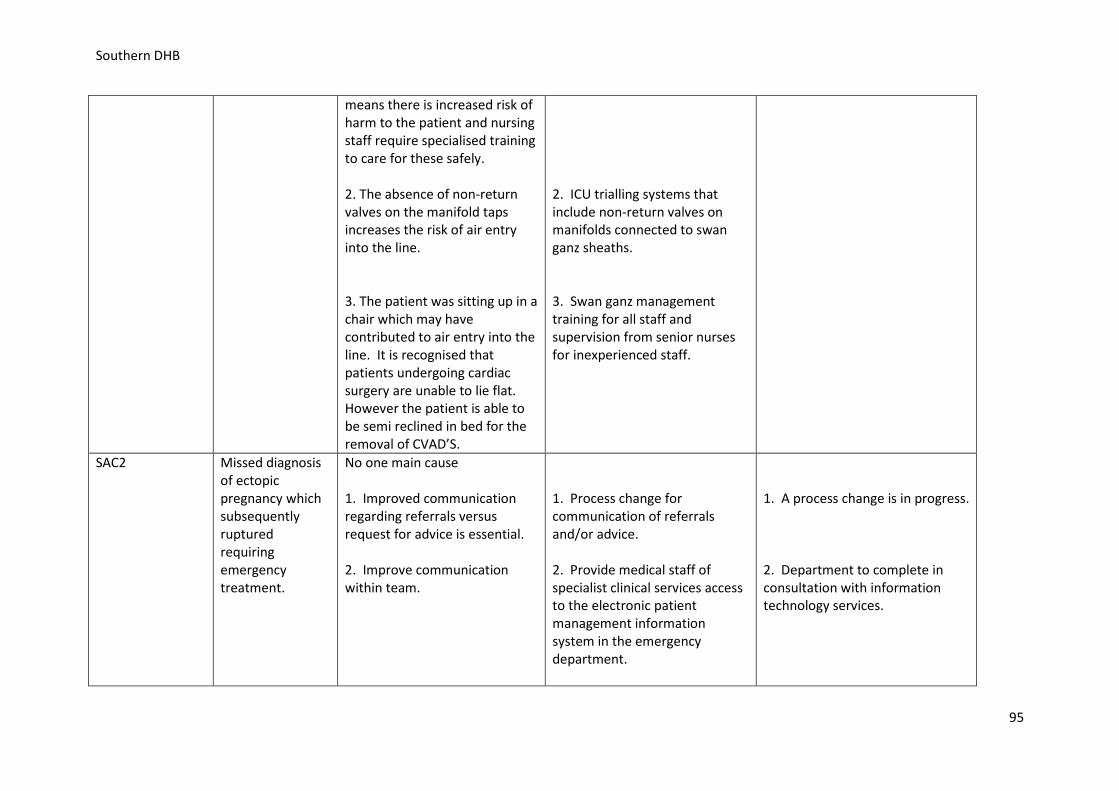
Southern DHB
means there is increased risk of harm to the patient and nursing staff require specialised training to care for these safely. 2. The absence of non-return valves on the manifold taps increases the risk of air entry into the line. 3. The patient was sitting up in a chair which may have contributed to air entry into the line. It is recognised that patients undergoing cardiac surgery are unable to lie flat. However the patient is able to be semi reclined in bed for the removal of CVAD’S.
2. ICU trialling systems that include non-return valves on manifolds connected to swan ganz sheaths. 3. Swan ganz management training for all staff and supervision from senior nurses for inexperienced staff.
SAC2
Missed diagnosis of ectopic pregnancy which subsequently ruptured requiring emergency treatment.
No one main cause 1. Improved communication regarding referrals versus request for advice is essential. 2. Improve communication within team.
1. Process change for communication of referrals and/or advice. 2. Provide medical staff of specialist clinical services access to the electronic patient management information system in the emergency department.
1. A process change is in progress. 2. Department to complete in consultation with information technology services.
95
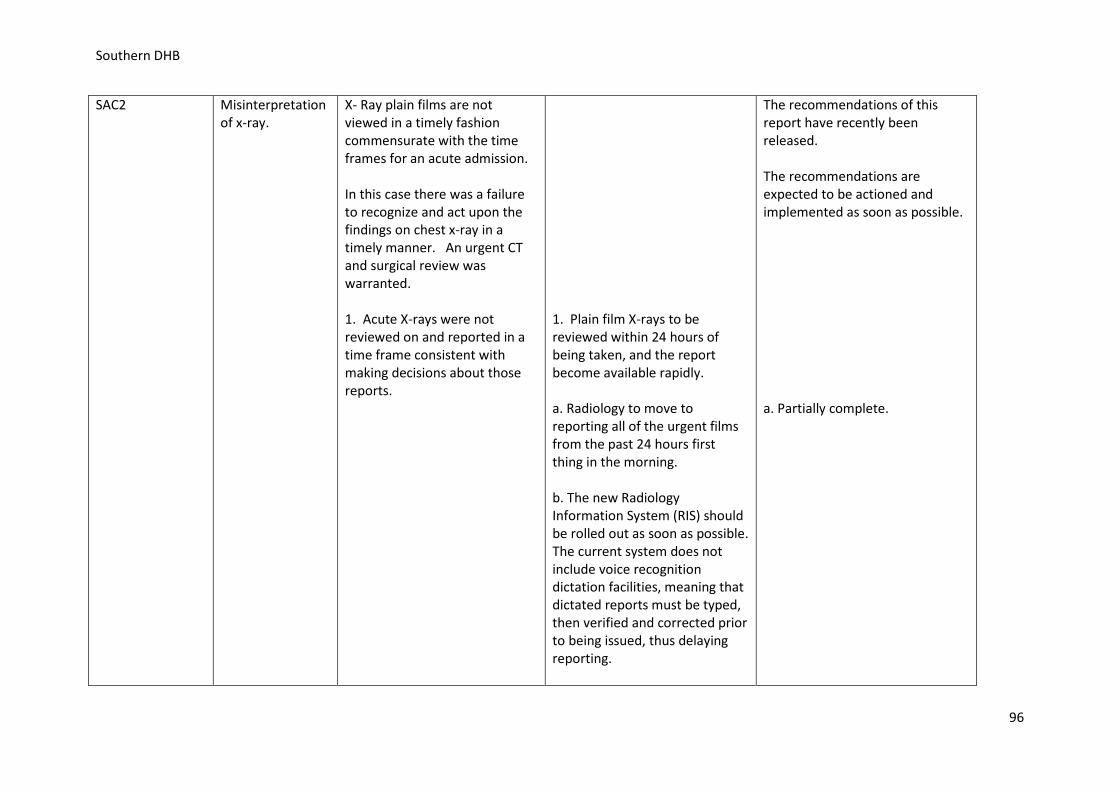
Southern DHB
SAC2 Misinterpretation of x-ray.
X- Ray plain films are not viewed in a timely fashion commensurate with the time frames for an acute admission. In this case there was a failure to recognize and act upon the findings on chest x-ray in a timely manner. An urgent CT and surgical review was warranted. 1. Acute X-rays were not reviewed on and reported in a time frame consistent with making decisions about those reports.
1. Plain film X-rays to be reviewed within 24 hours of being taken, and the report become available rapidly. a. Radiology to move to reporting all of the urgent films from the past 24 hours first thing in the morning. b. The new Radiology Information System (RIS) should be rolled out as soon as possible. The current system does not include voice recognition dictation facilities, meaning that dictated reports must be typed, then verified and corrected prior to being issued, thus delaying reporting.
The recommendations of this report have recently been released. The recommendations are expected to be actioned and implemented as soon as possible. a. Partially complete.
96
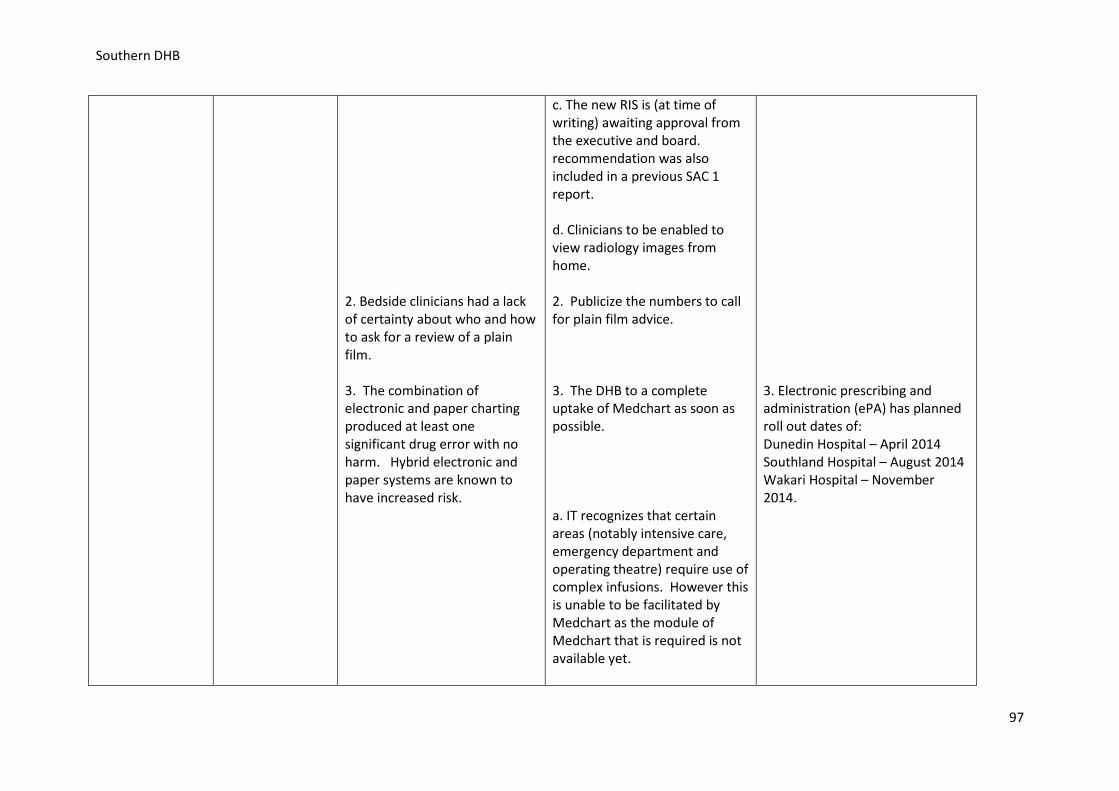
Southern DHB
2. Bedside clinicians had a lack of certainty about who and how to ask for a review of a plain film. 3. The combination of electronic and paper charting produced at least one significant drug error with no harm. Hybrid electronic and paper systems are known to have increased risk.
c. The new RIS is (at time of writing) awaiting approval from the executive and board. recommendation was also included in a previous SAC 1 report. d. Clinicians to be enabled to view radiology images from home. 2. Publicize the numbers to call for plain film advice. 3. The DHB to a complete uptake of Medchart as soon as possible. a. IT recognizes that certain areas (notably intensive care, emergency department and operating theatre) require use of complex infusions. However this is unable to be facilitated by Medchart as the module of Medchart that is required is not available yet.
3. Electronic prescribing and administration (ePA) has planned roll out dates of: Dunedin Hospital – April 2014 Southland Hospital – August 2014 Wakari Hospital – November 2014.
97
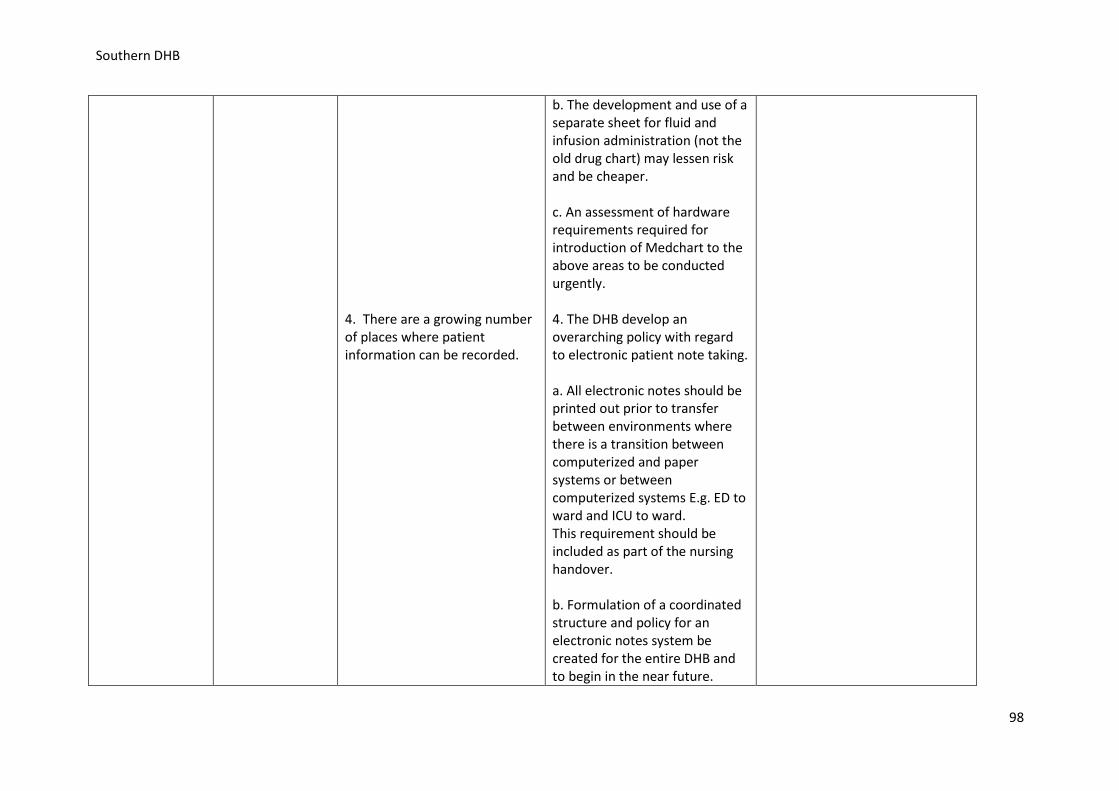
Southern DHB
4. There are a growing number of places where patient information can be recorded.
b. The development and use of a separate sheet for fluid and infusion administration (not the old drug chart) may lessen risk and be cheaper. c. An assessment of hardware requirements required for introduction of Medchart to the above areas to be conducted urgently. 4. The DHB develop an overarching policy with regard to electronic patient note taking. a. All electronic notes should be printed out prior to transfer between environments where there is a transition between computerized and paper systems or between computerized systems E.g. ED to ward and ICU to ward. This requirement should be included as part of the nursing handover. b. Formulation of a coordinated structure and policy for an electronic notes system be created for the entire DHB and to begin in the near future.
98
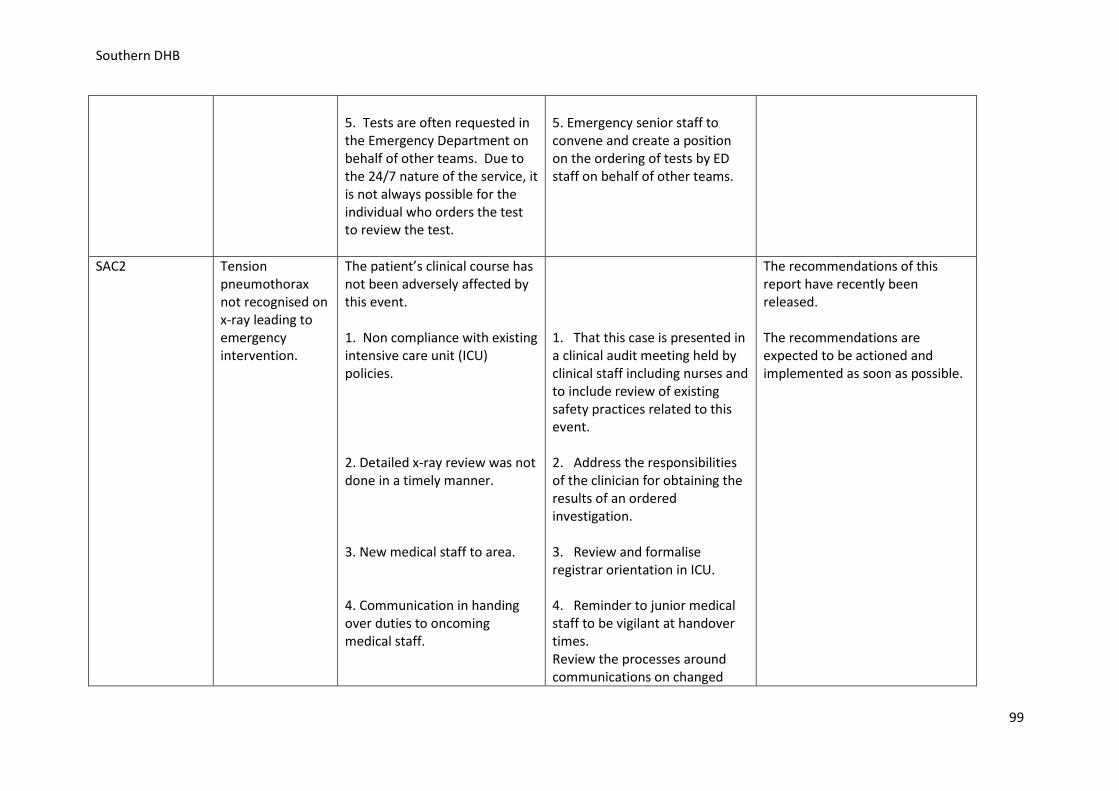
Southern DHB
5. Tests are often requested in the Emergency Department on behalf of other teams. Due to the 24/7 nature of the service, it is not always possible for the individual who orders the test to review the test.
5. Emergency senior staff to convene and create a position on the ordering of tests by ED staff on behalf of other teams.
SAC2
Tension pneumothorax not recognised on x-ray leading to emergency intervention.
The patient’s clinical course has not been adversely affected by this event. 1. Non compliance with existing intensive care unit (ICU) policies. 2. Detailed x-ray review was not done in a timely manner. 3. New medical staff to area. 4. Communication in handing over duties to oncoming medical staff.
1. That this case is presented in a clinical audit meeting held by clinical staff including nurses and to include review of existing safety practices related to this event. 2. Address the responsibilities of the clinician for obtaining the results of an ordered investigation. 3. Review and formalise registrar orientation in ICU. 4. Reminder to junior medical staff to be vigilant at handover times. Review the processes around communications on changed
The recommendations of this report have recently been released. The recommendations are expected to be actioned and implemented as soon as possible.
99
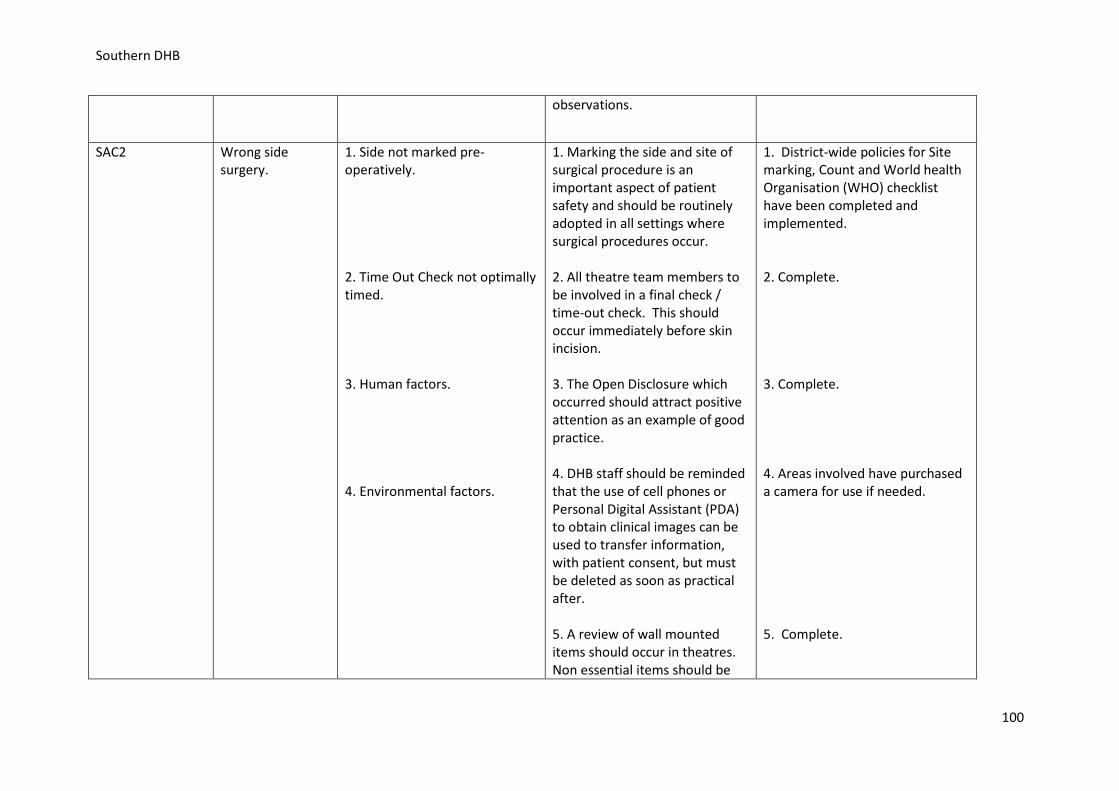
Southern DHB
observations.
SAC2
Wrong side surgery.
1. Side not marked pre-operatively. 2. Time Out Check not optimally timed. 3. Human factors. 4. Environmental factors.
1. Marking the side and site of surgical procedure is an important aspect of patient safety and should be routinely adopted in all settings where surgical procedures occur. 2. All theatre team members to be involved in a final check / time-out check. This should occur immediately before skin incision. 3. The Open Disclosure which occurred should attract positive attention as an example of good practice. 4. DHB staff should be reminded that the use of cell phones or Personal Digital Assistant (PDA) to obtain clinical images can be used to transfer information, with patient consent, but must be deleted as soon as practical after. 5. A review of wall mounted items should occur in theatres. Non essential items should be
1. District-wide policies for Site marking, Count and World health Organisation (WHO) checklist have been completed and implemented. 2. Complete. 3. Complete. 4. Areas involved have purchased a camera for use if needed. 5. Complete.
100
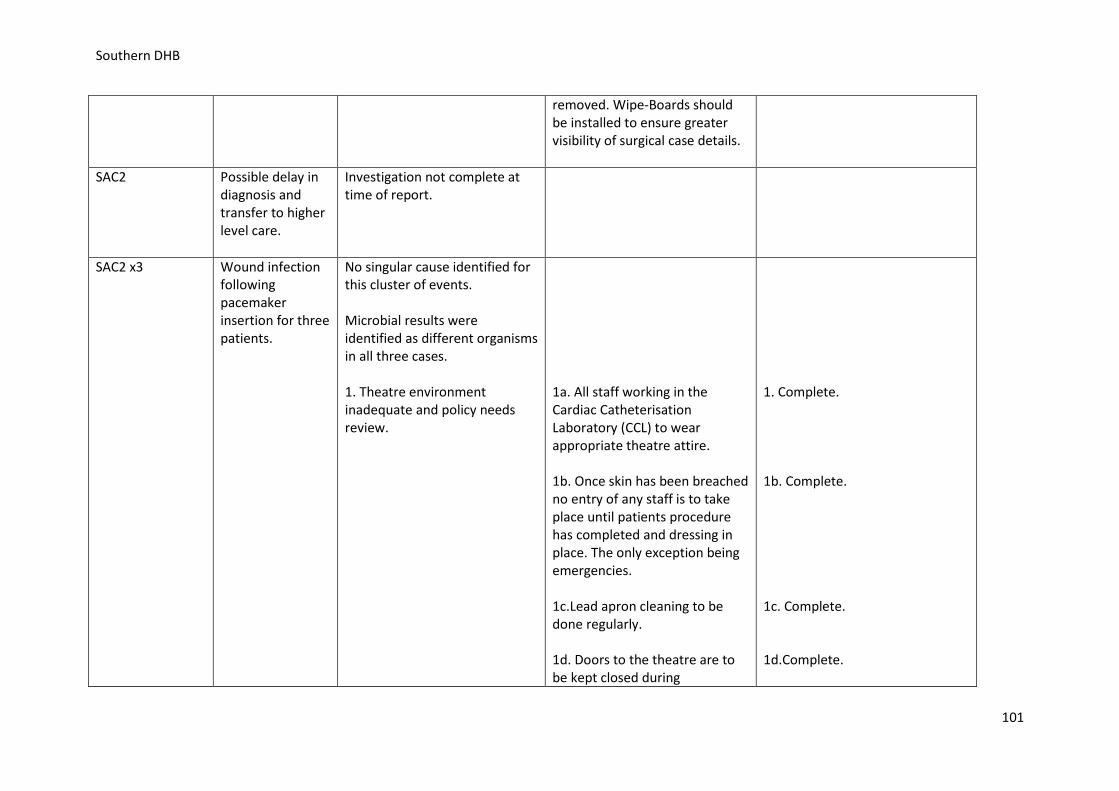
Southern DHB
removed. Wipe-Boards should be installed to ensure greater visibility of surgical case details.
SAC2 Possible delay in diagnosis and transfer to higher level care.
Investigation not complete at time of report.
SAC2 x3
Wound infection following pacemaker insertion for three patients.
No singular cause identified for this cluster of events. Microbial results were identified as different organisms in all three cases. 1. Theatre environment inadequate and policy needs review.
1a. All staff working in the Cardiac Catheterisation Laboratory (CCL) to wear appropriate theatre attire. 1b. Once skin has been breached no entry of any staff is to take place until patients procedure has completed and dressing in place. The only exception being emergencies. 1c.Lead apron cleaning to be done regularly. 1d. Doors to the theatre are to be kept closed during
1. Complete. 1b. Complete. 1c. Complete. 1d.Complete.
101
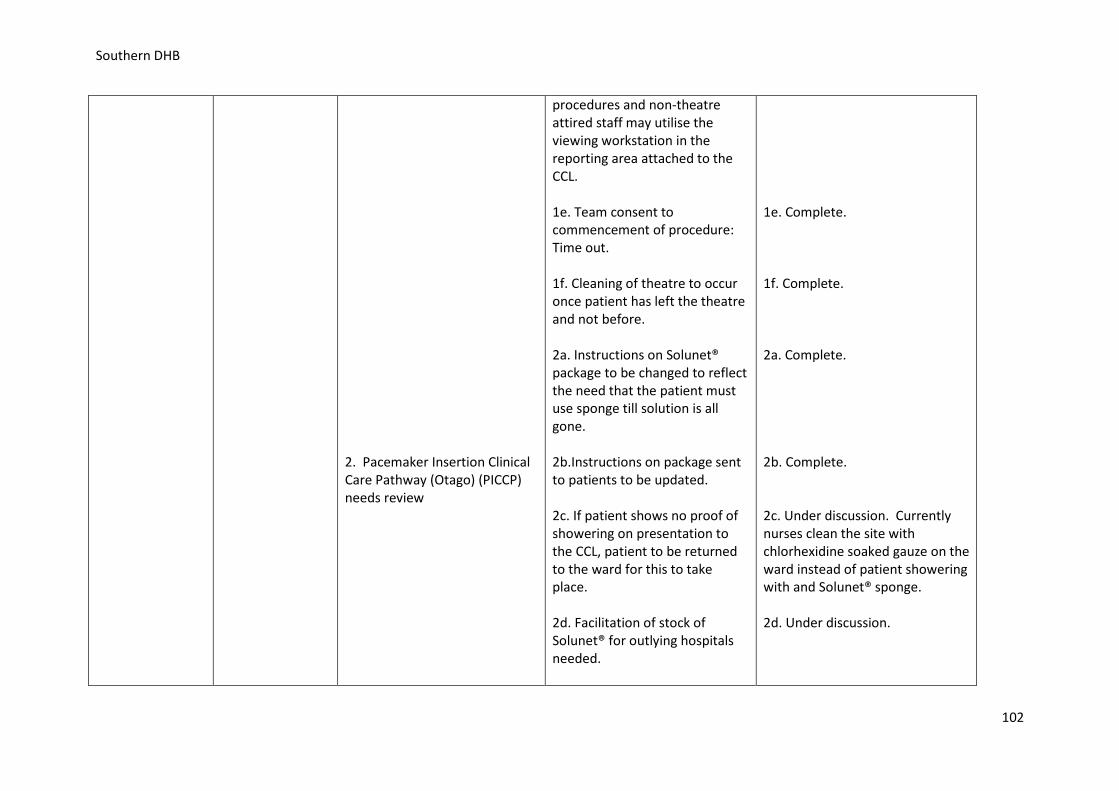
Southern DHB
2. Pacemaker Insertion Clinical Care Pathway (Otago) (PICCP) needs review
procedures and non-theatre attired staff may utilise the viewing workstation in the reporting area attached to the CCL. 1e. Team consent to commencement of procedure: Time out. 1f. Cleaning of theatre to occur once patient has left the theatre and not before. 2a. Instructions on Solunet® package to be changed to reflect the need that the patient must use sponge till solution is all gone. 2b.Instructions on package sent to patients to be updated. 2c. If patient shows no proof of showering on presentation to the CCL, patient to be returned to the ward for this to take place. 2d. Facilitation of stock of Solunet® for outlying hospitals needed.
1e. Complete. 1f. Complete. 2a. Complete. 2b. Complete. 2c. Under discussion. Currently nurses clean the site with chlorhexidine soaked gauze on the ward instead of patient showering with and Solunet® sponge. 2d. Under discussion.
102
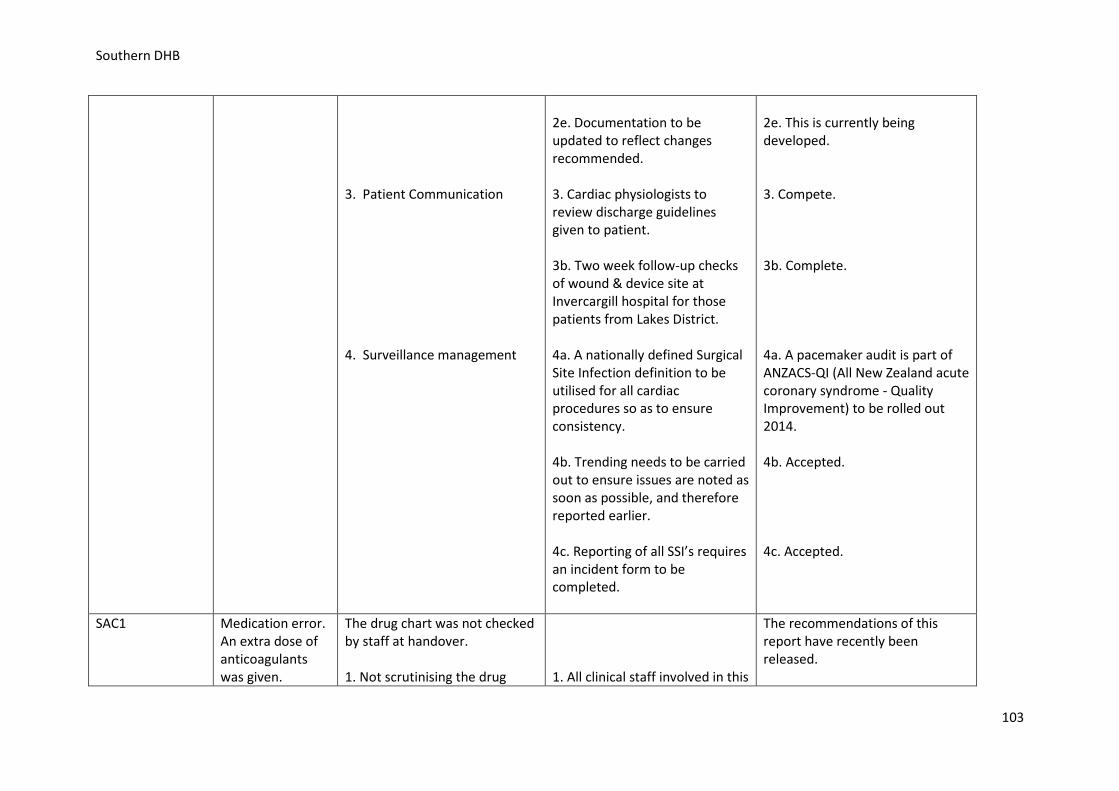
Southern DHB
3. Patient Communication 4. Surveillance management
2e. Documentation to be updated to reflect changes recommended. 3. Cardiac physiologists to review discharge guidelines given to patient. 3b. Two week follow-up checks of wound & device site at Invercargill hospital for those patients from Lakes District. 4a. A nationally defined Surgical Site Infection definition to be utilised for all cardiac procedures so as to ensure consistency. 4b. Trending needs to be carried out to ensure issues are noted as soon as possible, and therefore reported earlier. 4c. Reporting of all SSI’s requires an incident form to be completed.
2e. This is currently being developed. 3. Compete. 3b. Complete. 4a. A pacemaker audit is part of ANZACS-QI (All New Zealand acute coronary syndrome - Quality Improvement) to be rolled out 2014. 4b. Accepted. 4c. Accepted.
SAC1
Medication error. An extra dose of anticoagulants was given.
The drug chart was not checked by staff at handover. 1. Not scrutinising the drug
1. All clinical staff involved in this
The recommendations of this report have recently been released.
103
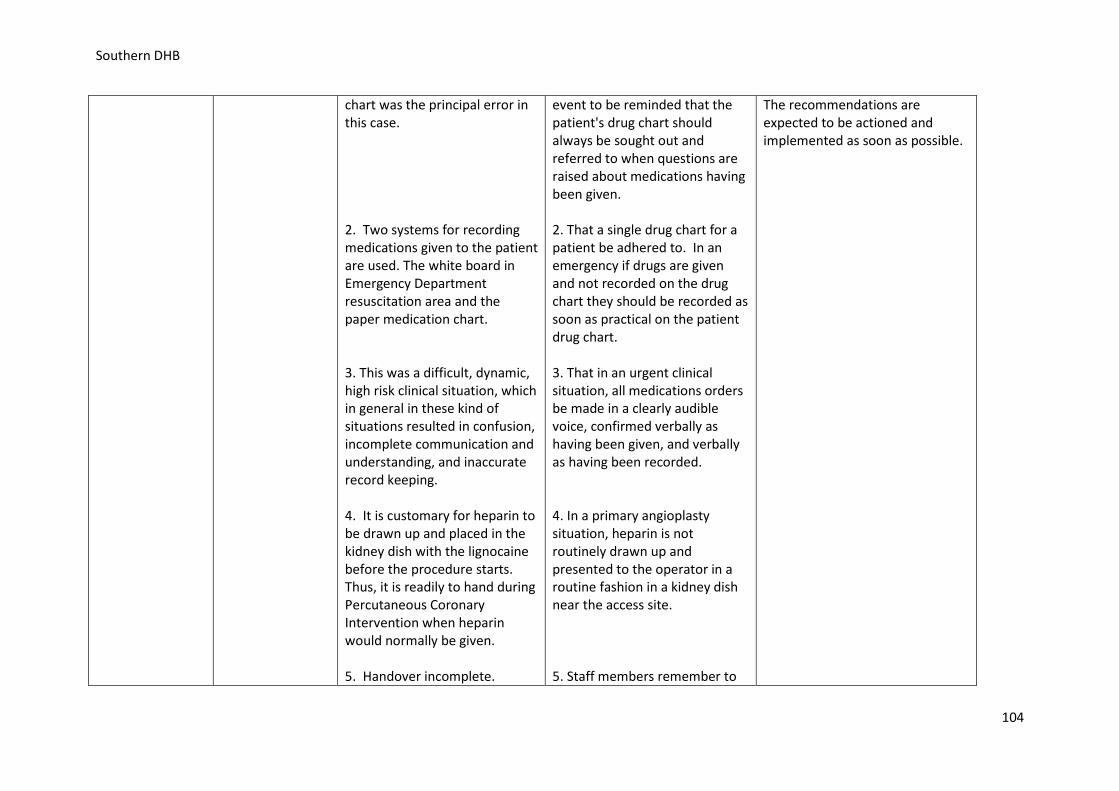
Southern DHB
chart was the principal error in this case. 2. Two systems for recording medications given to the patient are used. The white board in Emergency Department resuscitation area and the paper medication chart. 3. This was a difficult, dynamic, high risk clinical situation, which in general in these kind of situations resulted in confusion, incomplete communication and understanding, and inaccurate record keeping. 4. It is customary for heparin to be drawn up and placed in the kidney dish with the lignocaine before the procedure starts. Thus, it is readily to hand during Percutaneous Coronary Intervention when heparin would normally be given. 5. Handover incomplete.
event to be reminded that the patient's drug chart should always be sought out and referred to when questions are raised about medications having been given. 2. That a single drug chart for a patient be adhered to. In an emergency if drugs are given and not recorded on the drug chart they should be recorded as soon as practical on the patient drug chart. 3. That in an urgent clinical situation, all medications orders be made in a clearly audible voice, confirmed verbally as having been given, and verbally as having been recorded. 4. In a primary angioplasty situation, heparin is not routinely drawn up and presented to the operator in a routine fashion in a kidney dish near the access site. 5. Staff members remember to
The recommendations are expected to be actioned and implemented as soon as possible.
104
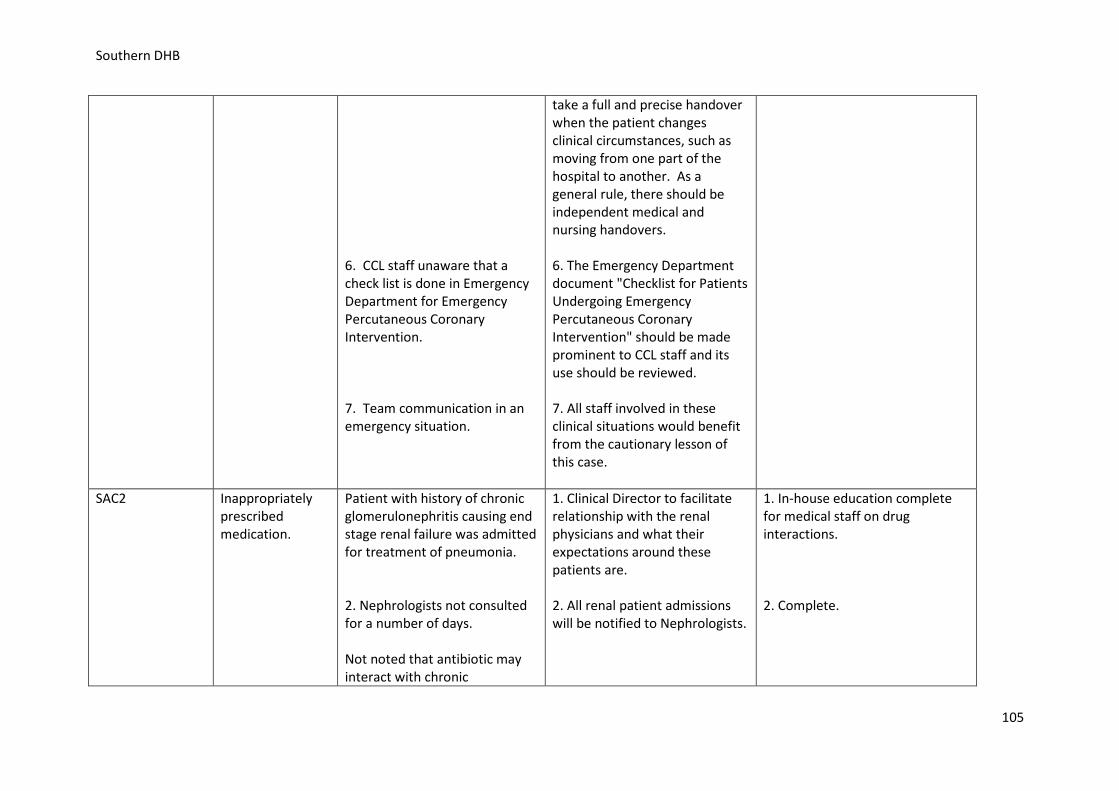
Southern DHB
6. CCL staff unaware that a check list is done in Emergency Department for Emergency Percutaneous Coronary Intervention. 7. Team communication in an emergency situation.
take a full and precise handover when the patient changes clinical circumstances, such as moving from one part of the hospital to another. As a general rule, there should be independent medical and nursing handovers. 6. The Emergency Department document "Checklist for Patients Undergoing Emergency Percutaneous Coronary Intervention" should be made prominent to CCL staff and its use should be reviewed. 7. All staff involved in these clinical situations would benefit from the cautionary lesson of this case.
SAC2 Inappropriately prescribed medication.
Patient with history of chronic glomerulonephritis causing end stage renal failure was admitted for treatment of pneumonia. 2. Nephrologists not consulted for a number of days. Not noted that antibiotic may interact with chronic
1. Clinical Director to facilitate relationship with the renal physicians and what their expectations around these patients are. 2. All renal patient admissions will be notified to Nephrologists.
1. In-house education complete for medical staff on drug interactions. 2. Complete.
105
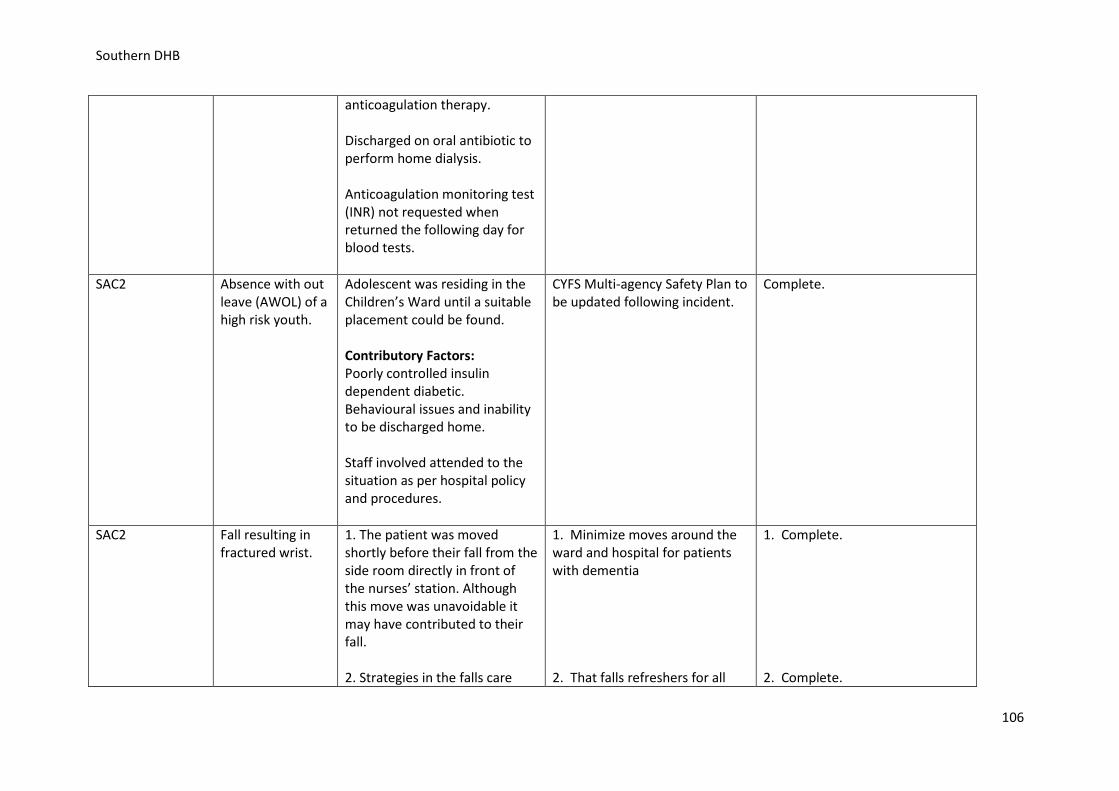
Southern DHB
anticoagulation therapy. Discharged on oral antibiotic to perform home dialysis. Anticoagulation monitoring test (INR) not requested when returned the following day for blood tests.
SAC2
Absence with out leave (AWOL) of a high risk youth.
Adolescent was residing in the Children’s Ward until a suitable placement could be found. Contributory Factors: Poorly controlled insulin dependent diabetic. Behavioural issues and inability to be discharged home. Staff involved attended to the situation as per hospital policy and procedures.
CYFS Multi-agency Safety Plan to be updated following incident.
Complete.
SAC2
Fall resulting in fractured wrist.
1. The patient was moved shortly before their fall from the side room directly in front of the nurses’ station. Although this move was unavoidable it may have contributed to their fall. 2. Strategies in the falls care
1. Minimize moves around the ward and hospital for patients with dementia 2. That falls refreshers for all
1. Complete. 2. Complete.
106
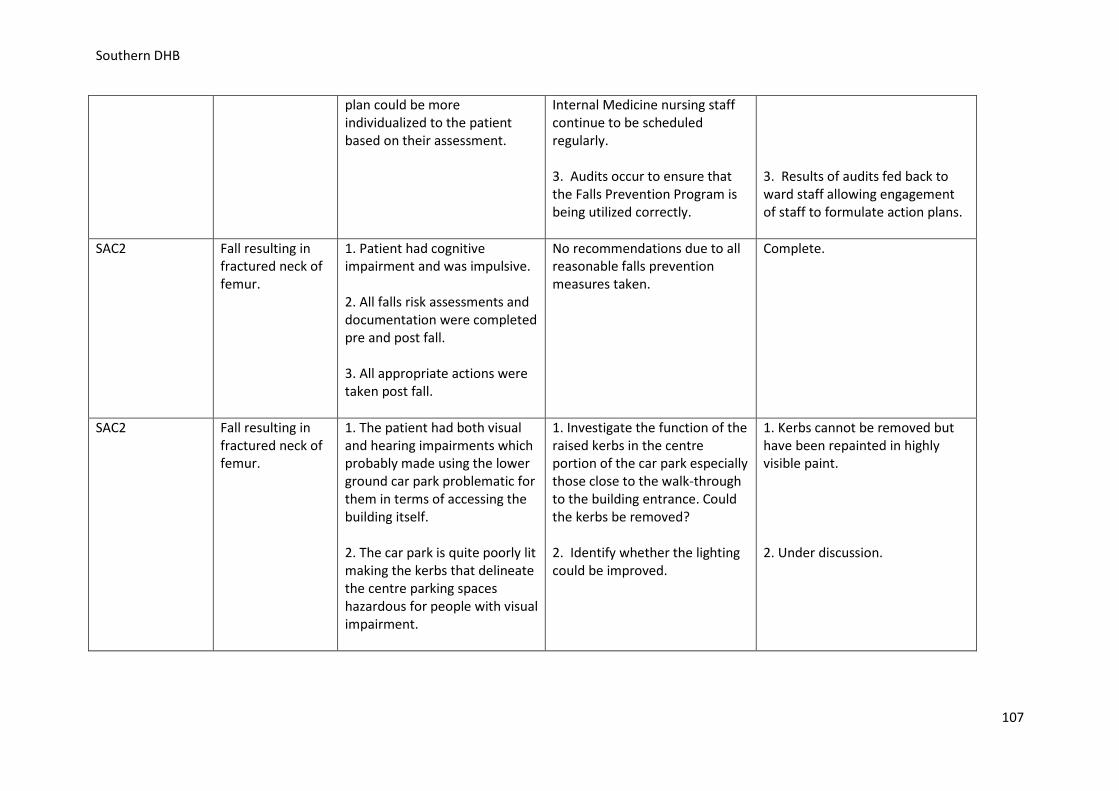
Southern DHB
plan could be more individualized to the patient based on their assessment.
Internal Medicine nursing staff continue to be scheduled regularly. 3. Audits occur to ensure that the Falls Prevention Program is being utilized correctly.
3. Results of audits fed back to ward staff allowing engagement of staff to formulate action plans.
SAC2
Fall resulting in fractured neck of femur.
1. Patient had cognitive impairment and was impulsive. 2. All falls risk assessments and documentation were completed pre and post fall. 3. All appropriate actions were taken post fall.
No recommendations due to all reasonable falls prevention measures taken.
Complete.
SAC2
Fall resulting in fractured neck of femur.
1. The patient had both visual and hearing impairments which probably made using the lower ground car park problematic for them in terms of accessing the building itself. 2. The car park is quite poorly lit making the kerbs that delineate the centre parking spaces hazardous for people with visual impairment.
1. Investigate the function of the raised kerbs in the centre portion of the car park especially those close to the walk-through to the building entrance. Could the kerbs be removed? 2. Identify whether the lighting could be improved.
1. Kerbs cannot be removed but have been repainted in highly visible paint. 2. Under discussion.
107
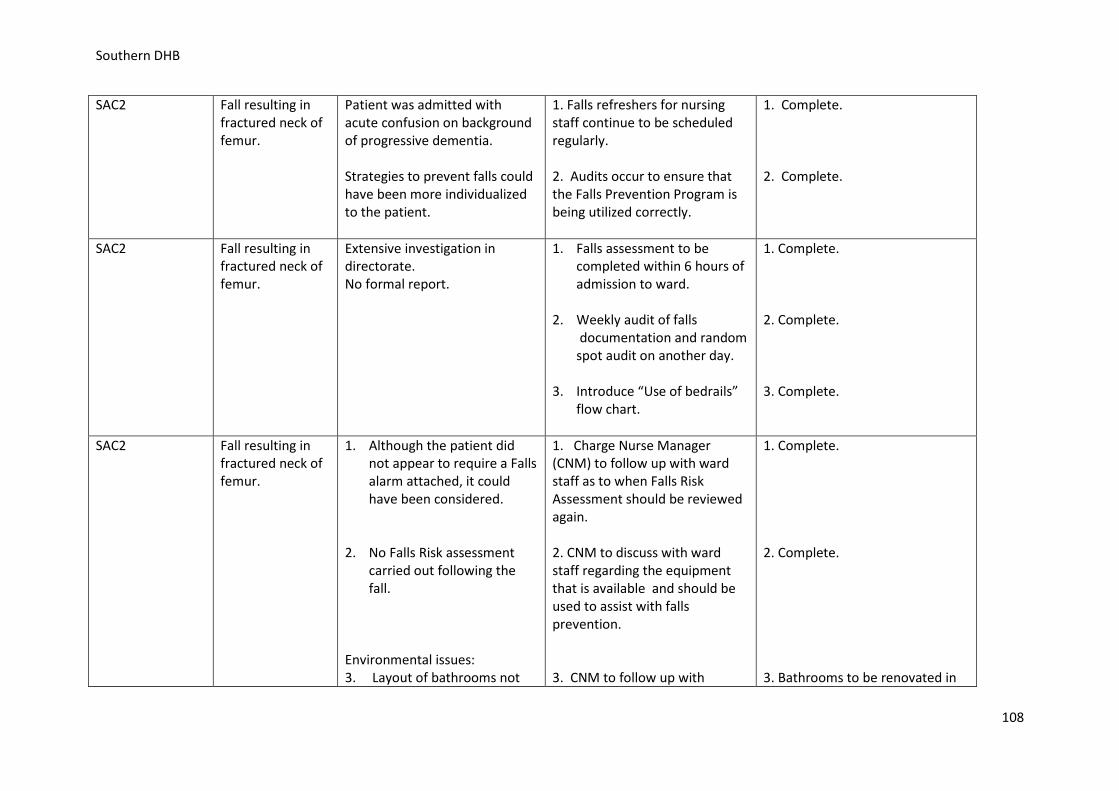
Southern DHB
SAC2
Fall resulting in fractured neck of femur.
Patient was admitted with acute confusion on background of progressive dementia. Strategies to prevent falls could have been more individualized to the patient.
1. Falls refreshers for nursing staff continue to be scheduled regularly. 2. Audits occur to ensure that the Falls Prevention Program is being utilized correctly.
1. Complete. 2. Complete.
SAC2
Fall resulting in fractured neck of femur.
Extensive investigation in directorate. No formal report.
1. Falls assessment to be completed within 6 hours of admission to ward.
2. Weekly audit of falls documentation and random spot audit on another day.
3. Introduce “Use of bedrails” flow chart.
1. Complete. 2. Complete. 3. Complete.
SAC2
Fall resulting in fractured neck of femur.
1. Although the patient did not appear to require a Falls alarm attached, it could have been considered.
2. No Falls Risk assessment carried out following the fall.
Environmental issues: 3. Layout of bathrooms not
1. Charge Nurse Manager (CNM) to follow up with ward staff as to when Falls Risk Assessment should be reviewed again. 2. CNM to discuss with ward staff regarding the equipment that is available and should be used to assist with falls prevention. 3. CNM to follow up with
1. Complete. 2. Complete. 3. Bathrooms to be renovated in
108
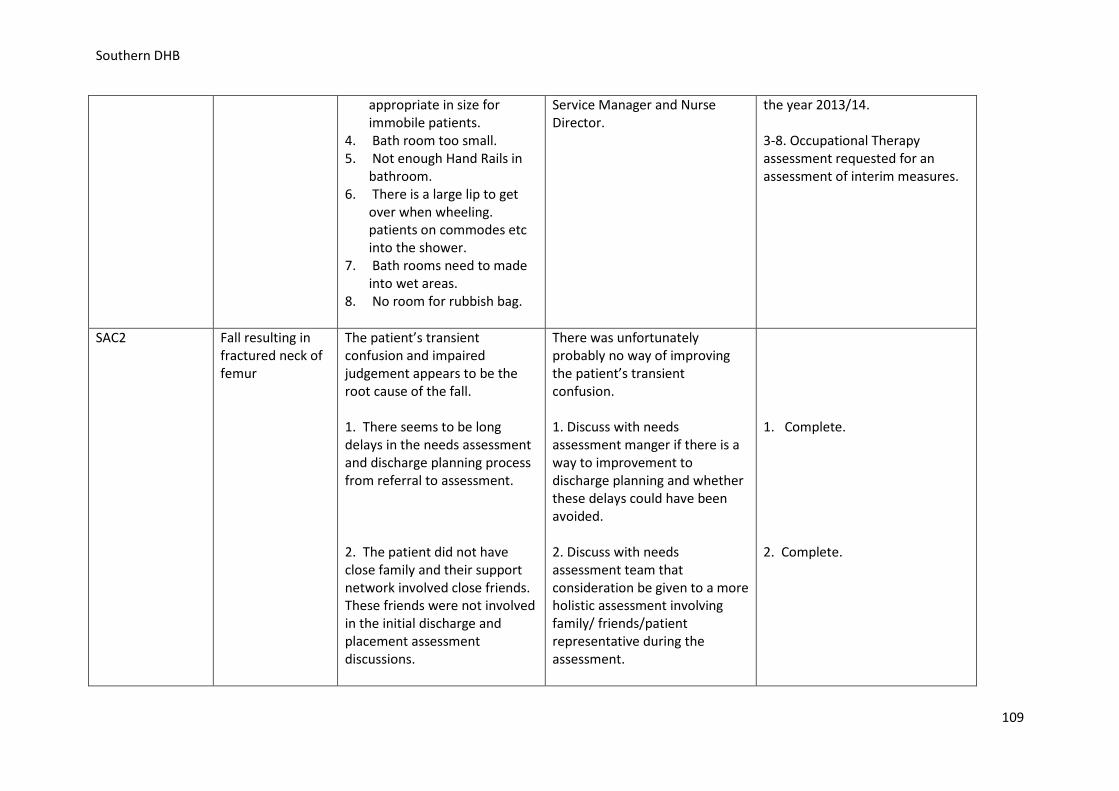
Southern DHB
appropriate in size for immobile patients.
4. Bath room too small. 5. Not enough Hand Rails in
bathroom. 6. There is a large lip to get
over when wheeling. patients on commodes etc into the shower.
7. Bath rooms need to made into wet areas.
8. No room for rubbish bag.
Service Manager and Nurse Director.
the year 2013/14. 3-8. Occupational Therapy assessment requested for an assessment of interim measures.
SAC2
Fall resulting in fractured neck of femur
The patient’s transient confusion and impaired judgement appears to be the root cause of the fall. 1. There seems to be long delays in the needs assessment and discharge planning process from referral to assessment. 2. The patient did not have close family and their support network involved close friends. These friends were not involved in the initial discharge and placement assessment discussions.
There was unfortunately probably no way of improving the patient’s transient confusion. 1. Discuss with needs assessment manger if there is a way to improvement to discharge planning and whether these delays could have been avoided. 2. Discuss with needs assessment team that consideration be given to a more holistic assessment involving family/ friends/patient representative during the assessment.
1. Complete. 2. Complete.
109
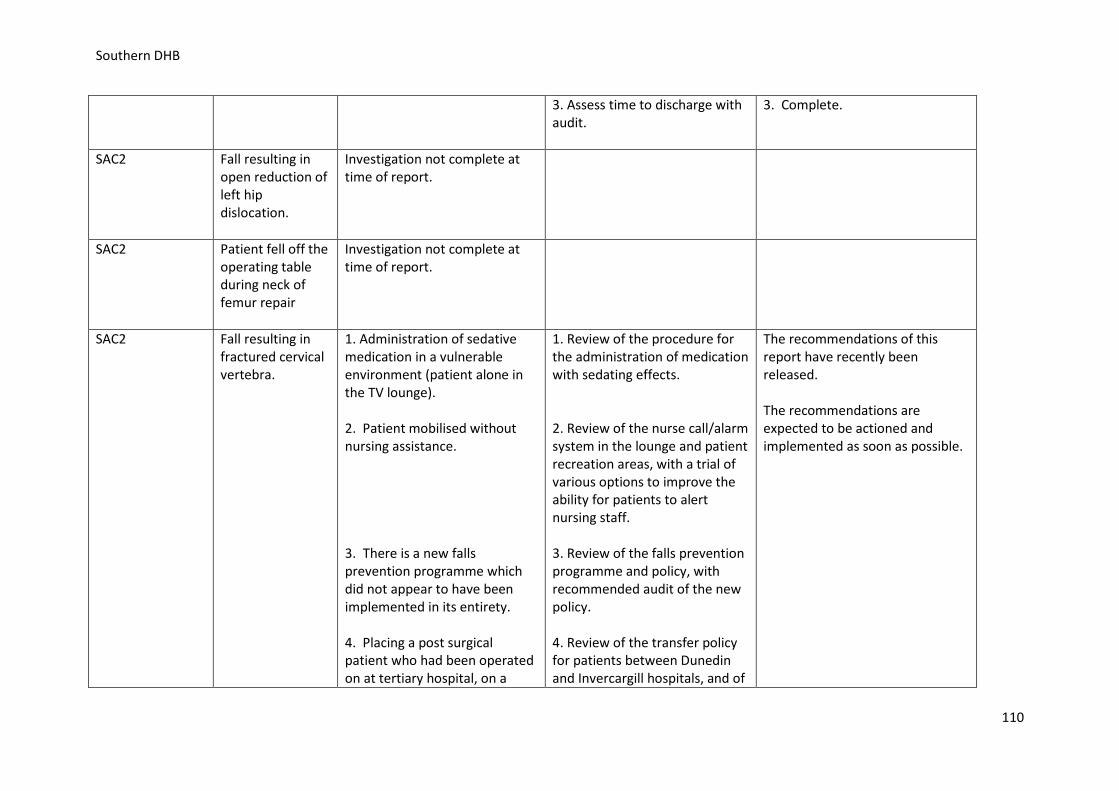
Southern DHB
3. Assess time to discharge with audit.
3. Complete.
SAC2
Fall resulting in open reduction of left hip dislocation.
Investigation not complete at time of report.
SAC2
Patient fell off the operating table during neck of femur repair
Investigation not complete at time of report.
SAC2 Fall resulting in fractured cervical vertebra.
1. Administration of sedative medication in a vulnerable environment (patient alone in the TV lounge). 2. Patient mobilised without nursing assistance. 3. There is a new falls prevention programme which did not appear to have been implemented in its entirety. 4. Placing a post surgical patient who had been operated on at tertiary hospital, on a
1. Review of the procedure for the administration of medication with sedating effects. 2. Review of the nurse call/alarm system in the lounge and patient recreation areas, with a trial of various options to improve the ability for patients to alert nursing staff. 3. Review of the falls prevention programme and policy, with recommended audit of the new policy. 4. Review of the transfer policy for patients between Dunedin and Invercargill hospitals, and of
The recommendations of this report have recently been released. The recommendations are expected to be actioned and implemented as soon as possible.
110
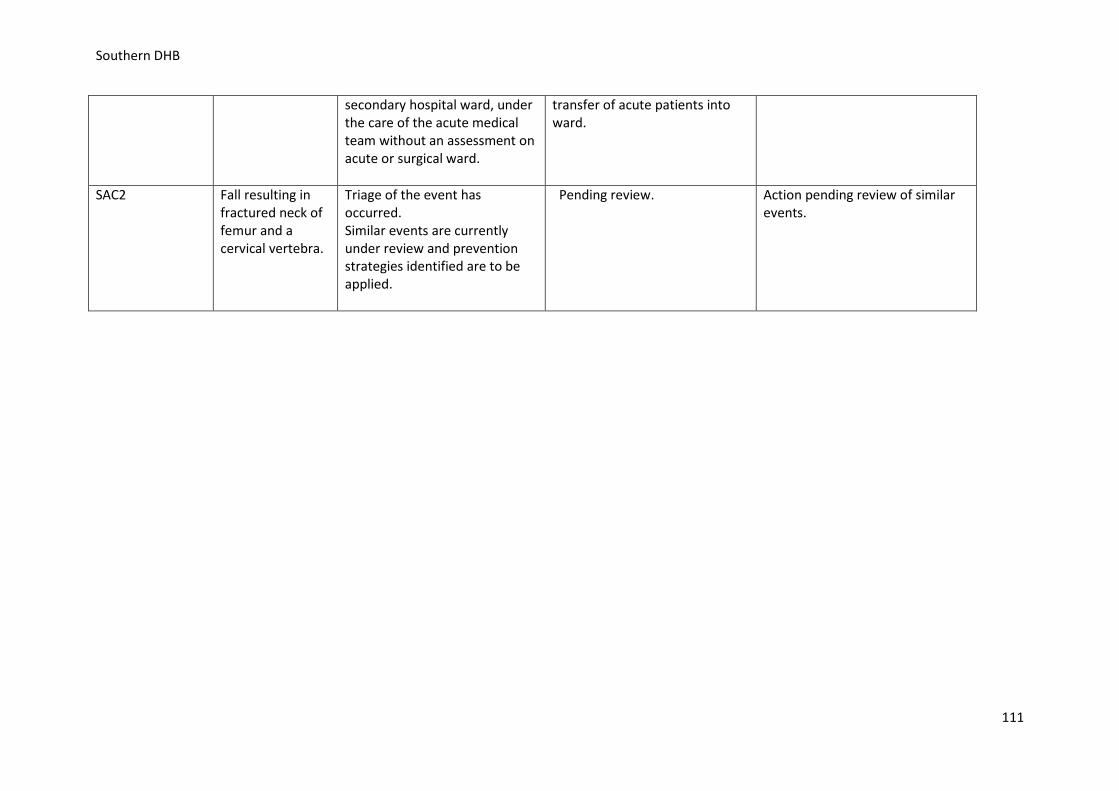
Southern DHB
secondary hospital ward, under the care of the acute medical team without an assessment on acute or surgical ward.
transfer of acute patients into ward.
SAC2 Fall resulting in fractured neck of femur and a cervical vertebra.
Triage of the event has occurred. Similar events are currently under review and prevention strategies identified are to be applied.
Pending review. Action pending review of similar events.
111
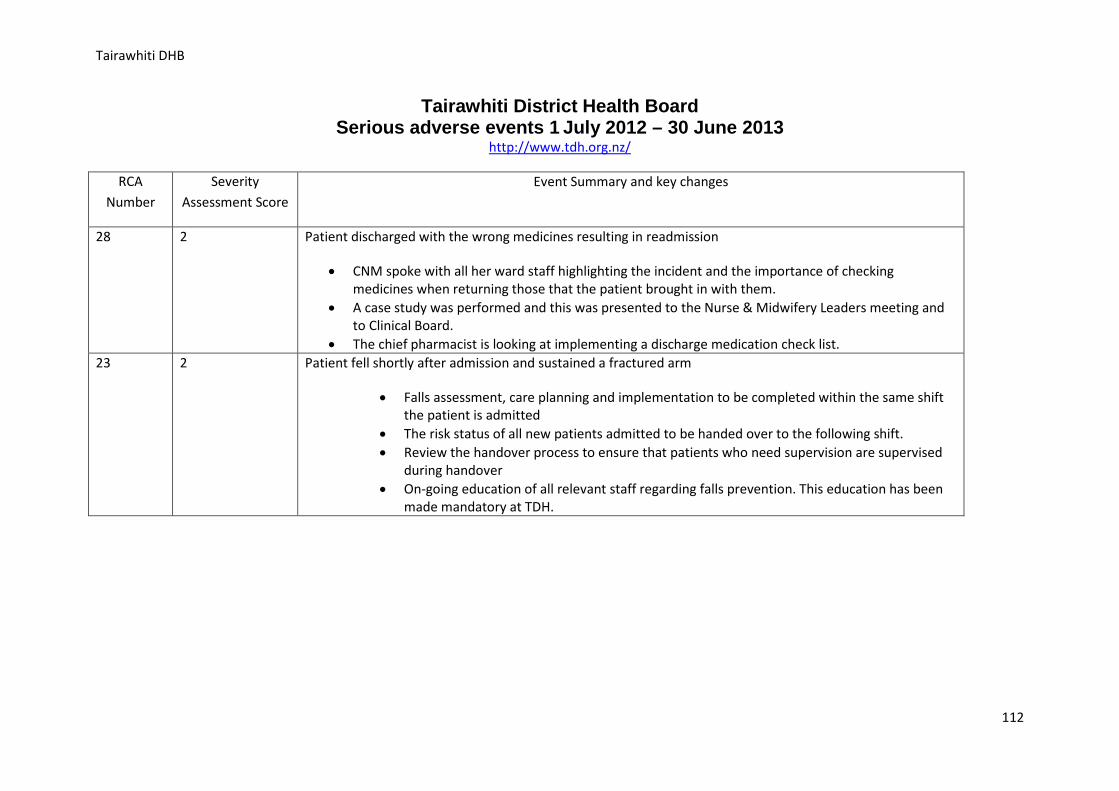
Tairawhiti DHB
Tairawhiti District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.tdh.org.nz/
RCA Number
Severity Assessment Score
Event Summary and key changes
28 2 Patient discharged with the wrong medicines resulting in readmission
• CNM spoke with all her ward staff highlighting the incident and the importance of checking medicines when returning those that the patient brought in with them.
• A case study was performed and this was presented to the Nurse & Midwifery Leaders meeting and to Clinical Board.
• The chief pharmacist is looking at implementing a discharge medication check list. 23 2 Patient fell shortly after admission and sustained a fractured arm
• Falls assessment, care planning and implementation to be completed within the same shift the patient is admitted
• The risk status of all new patients admitted to be handed over to the following shift. • Review the handover process to ensure that patients who need supervision are supervised
during handover • On-going education of all relevant staff regarding falls prevention. This education has been
made mandatory at TDH.
112
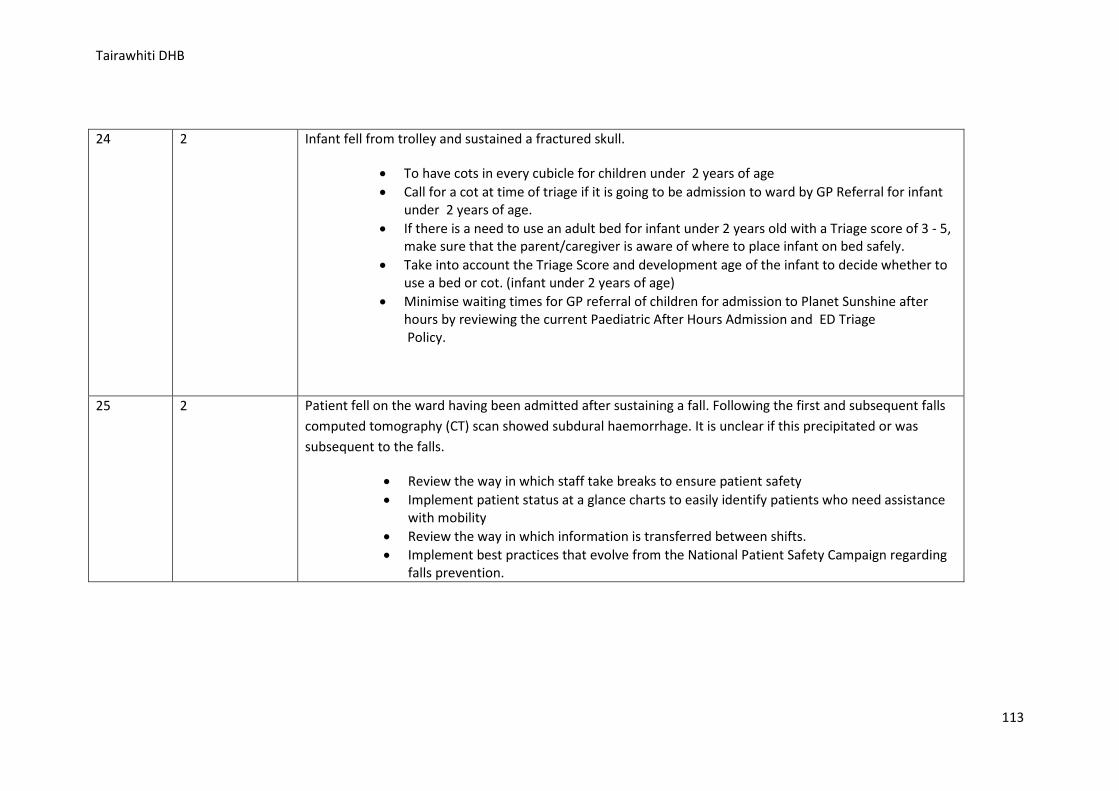
Tairawhiti DHB
24 2 Infant fell from trolley and sustained a fractured skull.
• To have cots in every cubicle for children under 2 years of age • Call for a cot at time of triage if it is going to be admission to ward by GP Referral for infant
under 2 years of age. • If there is a need to use an adult bed for infant under 2 years old with a Triage score of 3 - 5,
make sure that the parent/caregiver is aware of where to place infant on bed safely. • Take into account the Triage Score and development age of the infant to decide whether to
use a bed or cot. (infant under 2 years of age) • Minimise waiting times for GP referral of children for admission to Planet Sunshine after
hours by reviewing the current Paediatric After Hours Admission and ED Triage Policy.
25 2 Patient fell on the ward having been admitted after sustaining a fall. Following the first and subsequent falls computed tomography (CT) scan showed subdural haemorrhage. It is unclear if this precipitated or was subsequent to the falls.
• Review the way in which staff take breaks to ensure patient safety • Implement patient status at a glance charts to easily identify patients who need assistance
with mobility • Review the way in which information is transferred between shifts. • Implement best practices that evolve from the National Patient Safety Campaign regarding
falls prevention.
113
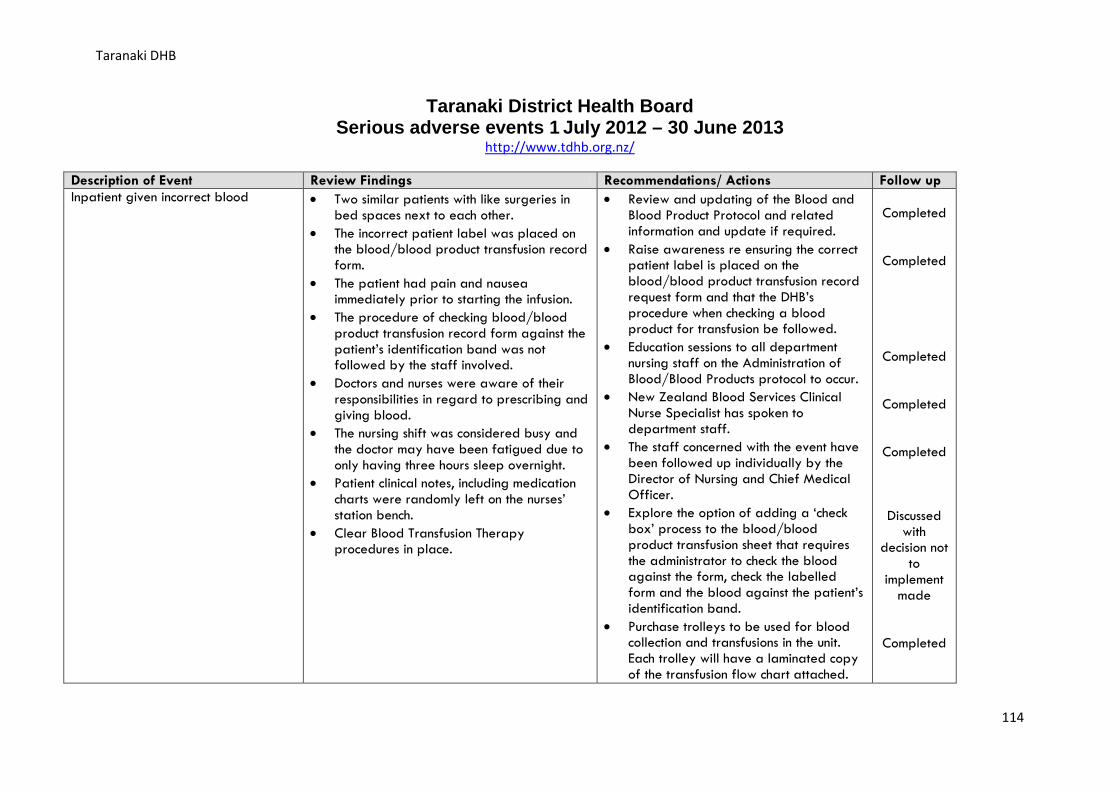
Taranaki DHB
Taranaki District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.tdhb.org.nz/
Description of Event Review Findings Recommendations/ Actions Follow up Inpatient given incorrect blood • Two similar patients with like surgeries in
bed spaces next to each other. • The incorrect patient label was placed on
the blood/blood product transfusion record form.
• The patient had pain and nausea immediately prior to starting the infusion.
• The procedure of checking blood/blood product transfusion record form against the patient’s identification band was not followed by the staff involved.
• Doctors and nurses were aware of their responsibilities in regard to prescribing and giving blood.
• The nursing shift was considered busy and the doctor may have been fatigued due to only having three hours sleep overnight.
• Patient clinical notes, including medication charts were randomly left on the nurses’ station bench.
• Clear Blood Transfusion Therapy procedures in place.
• Review and updating of the Blood and Blood Product Protocol and related information and update if required.
• Raise awareness re ensuring the correct patient label is placed on the blood/blood product transfusion record request form and that the DHB’s procedure when checking a blood product for transfusion be followed.
• Education sessions to all department nursing staff on the Administration of Blood/Blood Products protocol to occur.
• New Zealand Blood Services Clinical Nurse Specialist has spoken to department staff.
• The staff concerned with the event have been followed up individually by the Director of Nursing and Chief Medical Officer.
• Explore the option of adding a ‘check box’ process to the blood/blood product transfusion sheet that requires the administrator to check the blood against the form, check the labelled form and the blood against the patient’s identification band.
• Purchase trolleys to be used for blood collection and transfusions in the unit. Each trolley will have a laminated copy of the transfusion flow chart attached.
Completed
Completed
Completed
Completed
Completed
Discussed with
decision not to
implement made
Completed
114
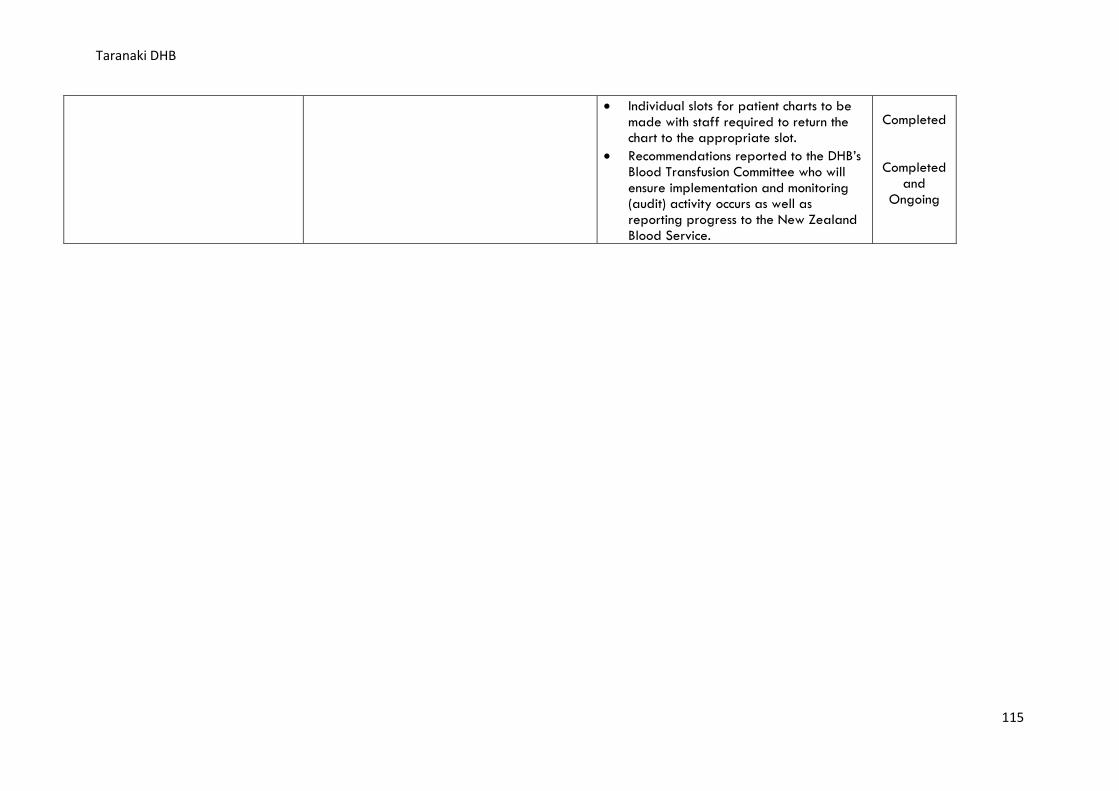
Taranaki DHB
• Individual slots for patient charts to be made with staff required to return the chart to the appropriate slot.
• Recommendations reported to the DHB’s Blood Transfusion Committee who will ensure implementation and monitoring (audit) activity occurs as well as reporting progress to the New Zealand Blood Service.
Completed
Completed and
Ongoing
115
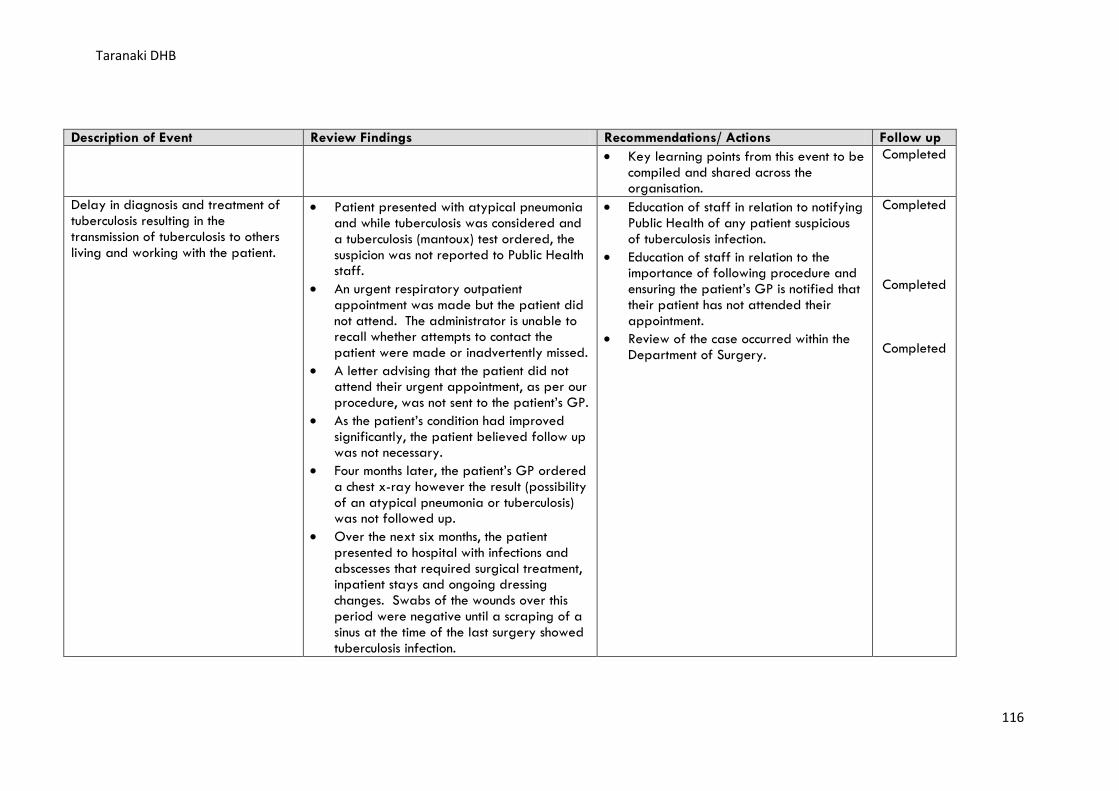
Taranaki DHB
Description of Event Review Findings Recommendations/ Actions Follow up • Key learning points from this event to be
compiled and shared across the organisation.
Completed
Delay in diagnosis and treatment of tuberculosis resulting in the transmission of tuberculosis to others living and working with the patient.
• Patient presented with atypical pneumonia and while tuberculosis was considered and a tuberculosis (mantoux) test ordered, the suspicion was not reported to Public Health staff.
• An urgent respiratory outpatient appointment was made but the patient did not attend. The administrator is unable to recall whether attempts to contact the patient were made or inadvertently missed.
• A letter advising that the patient did not attend their urgent appointment, as per our procedure, was not sent to the patient’s GP.
• As the patient’s condition had improved significantly, the patient believed follow up was not necessary.
• Four months later, the patient’s GP ordered a chest x-ray however the result (possibility of an atypical pneumonia or tuberculosis) was not followed up.
• Over the next six months, the patient presented to hospital with infections and abscesses that required surgical treatment, inpatient stays and ongoing dressing changes. Swabs of the wounds over this period were negative until a scraping of a sinus at the time of the last surgery showed tuberculosis infection.
• Education of staff in relation to notifying Public Health of any patient suspicious of tuberculosis infection.
• Education of staff in relation to the importance of following procedure and ensuring the patient’s GP is notified that their patient has not attended their appointment.
• Review of the case occurred within the Department of Surgery.
Completed
Completed
Completed
116
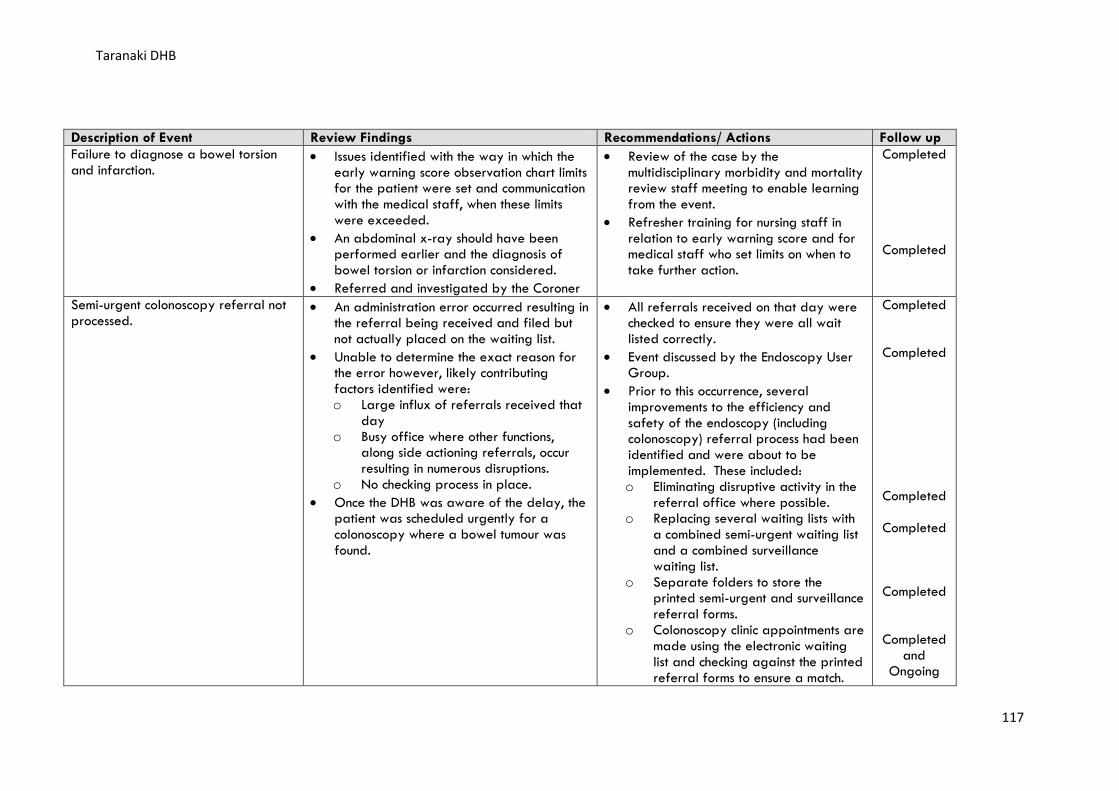
Taranaki DHB
Description of Event Review Findings Recommendations/ Actions Follow up Failure to diagnose a bowel torsion and infarction.
• Issues identified with the way in which the early warning score observation chart limits for the patient were set and communication with the medical staff, when these limits were exceeded.
• An abdominal x-ray should have been performed earlier and the diagnosis of bowel torsion or infarction considered.
• Referred and investigated by the Coroner
• Review of the case by the multidisciplinary morbidity and mortality review staff meeting to enable learning from the event.
• Refresher training for nursing staff in relation to early warning score and for medical staff who set limits on when to take further action.
Completed
Completed
Semi-urgent colonoscopy referral not processed.
• An administration error occurred resulting in the referral being received and filed but not actually placed on the waiting list.
• Unable to determine the exact reason for the error however, likely contributing factors identified were: o Large influx of referrals received that
day o Busy office where other functions,
along side actioning referrals, occur resulting in numerous disruptions.
o No checking process in place. • Once the DHB was aware of the delay, the
patient was scheduled urgently for a colonoscopy where a bowel tumour was found.
• All referrals received on that day were checked to ensure they were all wait listed correctly.
• Event discussed by the Endoscopy User Group.
• Prior to this occurrence, several improvements to the efficiency and safety of the endoscopy (including colonoscopy) referral process had been identified and were about to be implemented. These included: o Eliminating disruptive activity in the
referral office where possible. o Replacing several waiting lists with
a combined semi-urgent waiting list and a combined surveillance waiting list.
o Separate folders to store the printed semi-urgent and surveillance referral forms.
o Colonoscopy clinic appointments are made using the electronic waiting list and checking against the printed referral forms to ensure a match.
Completed
Completed
Completed
Completed
Completed
Completed and
Ongoing
117
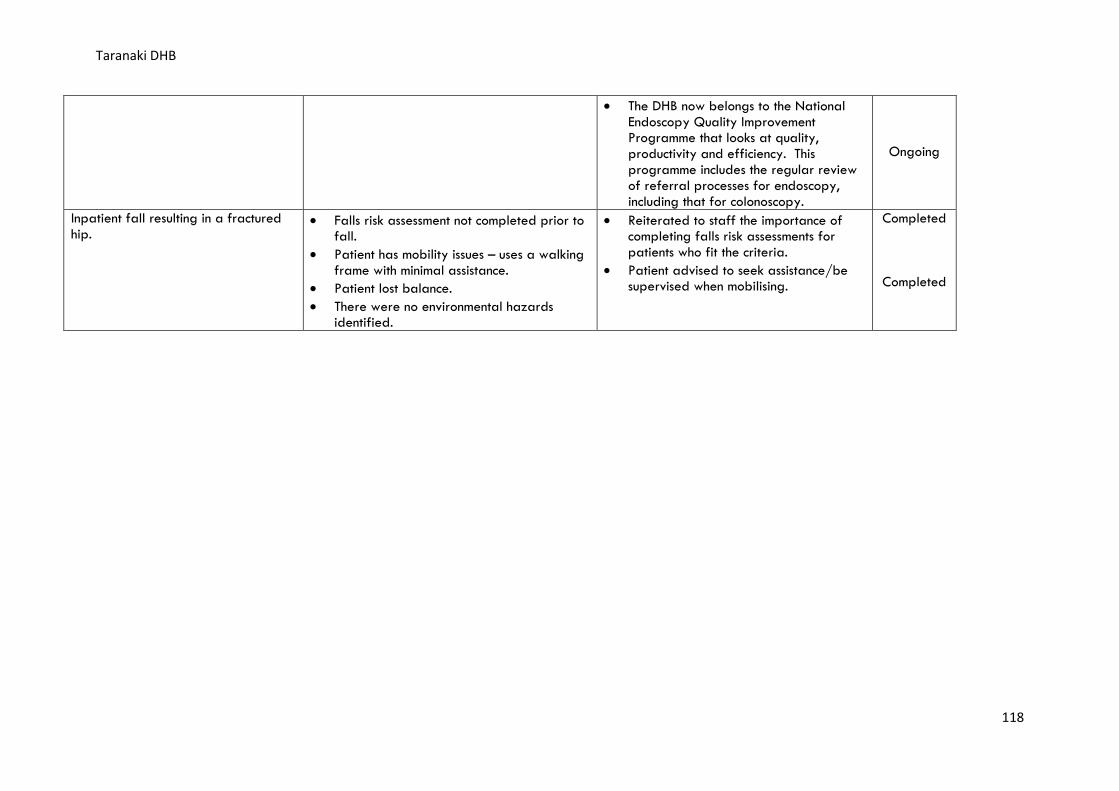
Taranaki DHB
• The DHB now belongs to the National Endoscopy Quality Improvement Programme that looks at quality, productivity and efficiency. This programme includes the regular review of referral processes for endoscopy, including that for colonoscopy.
Ongoing
Inpatient fall resulting in a fractured hip.
• Falls risk assessment not completed prior to fall.
• Patient has mobility issues – uses a walking frame with minimal assistance.
• Patient lost balance. • There were no environmental hazards
identified.
• Reiterated to staff the importance of completing falls risk assessments for patients who fit the criteria.
• Patient advised to seek assistance/be supervised when mobilising.
Completed
Completed
118
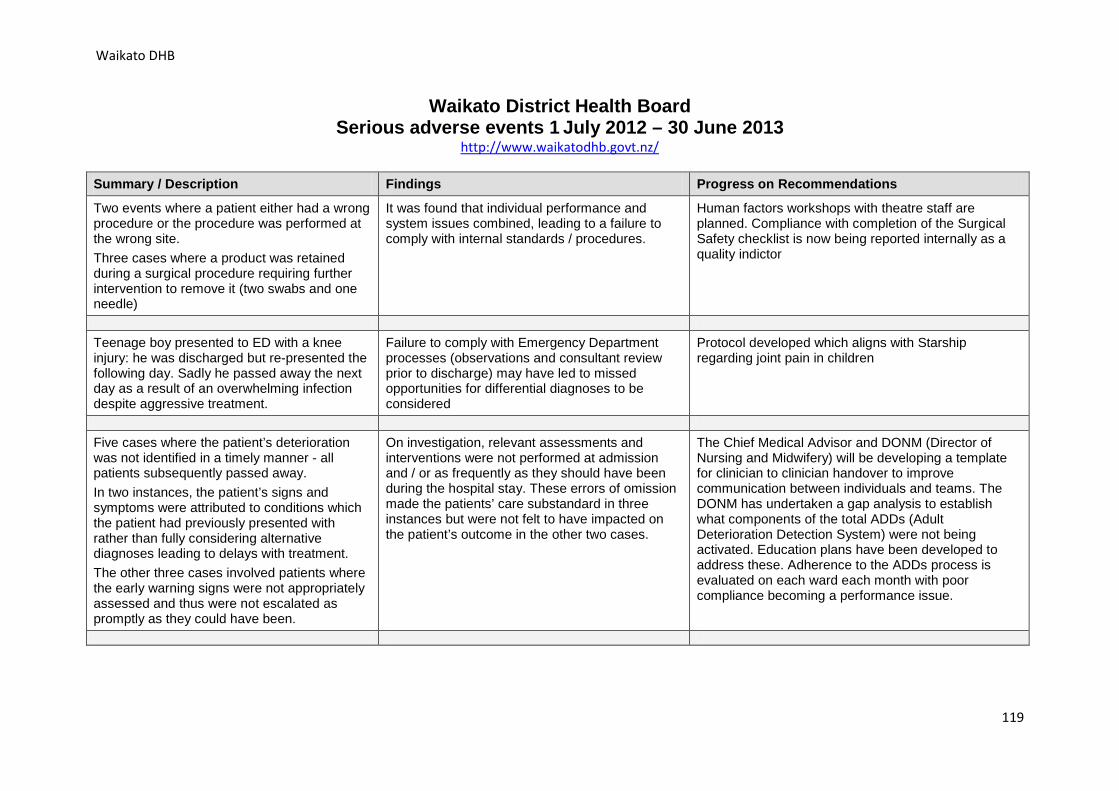
Waikato DHB
Waikato District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.waikatodhb.govt.nz/
Summary / Description Findings Progress on Recommendations
Two events where a patient either had a wrong procedure or the procedure was performed at the wrong site. Three cases where a product was retained during a surgical procedure requiring further intervention to remove it (two swabs and one needle)
It was found that individual performance and system issues combined, leading to a failure to comply with internal standards / procedures.
Human factors workshops with theatre staff are planned. Compliance with completion of the Surgical Safety checklist is now being reported internally as a quality indictor
Teenage boy presented to ED with a knee injury: he was discharged but re-presented the following day. Sadly he passed away the next day as a result of an overwhelming infection despite aggressive treatment.
Failure to comply with Emergency Department processes (observations and consultant review prior to discharge) may have led to missed opportunities for differential diagnoses to be considered
Protocol developed which aligns with Starship regarding joint pain in children
Five cases where the patient’s deterioration was not identified in a timely manner - all patients subsequently passed away. In two instances, the patient’s signs and symptoms were attributed to conditions which the patient had previously presented with rather than fully considering alternative diagnoses leading to delays with treatment. The other three cases involved patients where the early warning signs were not appropriately assessed and thus were not escalated as promptly as they could have been.
On investigation, relevant assessments and interventions were not performed at admission and / or as frequently as they should have been during the hospital stay. These errors of omission made the patients’ care substandard in three instances but were not felt to have impacted on the patient’s outcome in the other two cases.
The Chief Medical Advisor and DONM (Director of Nursing and Midwifery) will be developing a template for clinician to clinician handover to improve communication between individuals and teams. The DONM has undertaken a gap analysis to establish what components of the total ADDs (Adult Deterioration Detection System) were not being activated. Education plans have been developed to address these. Adherence to the ADDs process is evaluated on each ward each month with poor compliance becoming a performance issue.
119
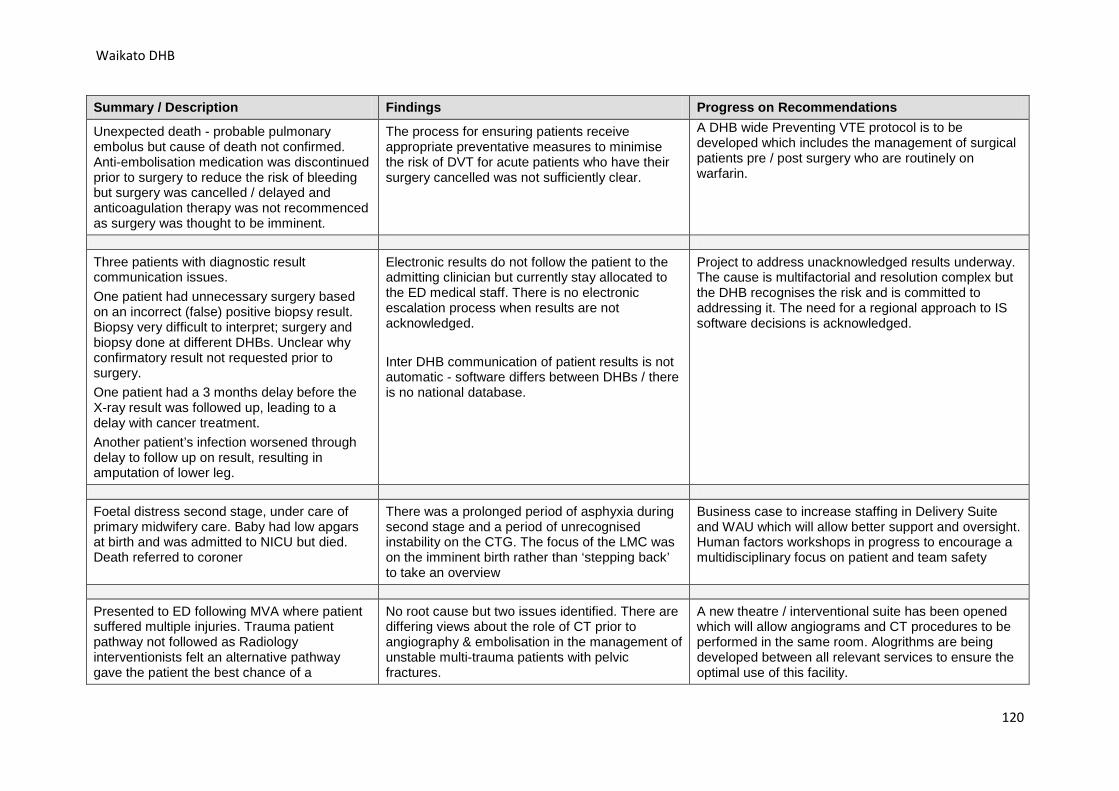
Waikato DHB
Summary / Description Findings Progress on Recommendations
Unexpected death - probable pulmonary embolus but cause of death not confirmed. Anti-embolisation medication was discontinued prior to surgery to reduce the risk of bleeding but surgery was cancelled / delayed and anticoagulation therapy was not recommenced as surgery was thought to be imminent.
The process for ensuring patients receive appropriate preventative measures to minimise the risk of DVT for acute patients who have their surgery cancelled was not sufficiently clear.
A DHB wide Preventing VTE protocol is to be developed which includes the management of surgical patients pre / post surgery who are routinely on warfarin.
Three patients with diagnostic result communication issues. One patient had unnecessary surgery based on an incorrect (false) positive biopsy result. Biopsy very difficult to interpret; surgery and biopsy done at different DHBs. Unclear why confirmatory result not requested prior to surgery. One patient had a 3 months delay before the X-ray result was followed up, leading to a delay with cancer treatment. Another patient’s infection worsened through delay to follow up on result, resulting in amputation of lower leg.
Electronic results do not follow the patient to the admitting clinician but currently stay allocated to the ED medical staff. There is no electronic escalation process when results are not acknowledged. Inter DHB communication of patient results is not automatic - software differs between DHBs / there is no national database.
Project to address unacknowledged results underway. The cause is multifactorial and resolution complex but the DHB recognises the risk and is committed to addressing it. The need for a regional approach to IS software decisions is acknowledged.
Foetal distress second stage, under care of primary midwifery care. Baby had low apgars at birth and was admitted to NICU but died. Death referred to coroner
There was a prolonged period of asphyxia during second stage and a period of unrecognised instability on the CTG. The focus of the LMC was on the imminent birth rather than ‘stepping back’ to take an overview
Business case to increase staffing in Delivery Suite and WAU which will allow better support and oversight. Human factors workshops in progress to encourage a multidisciplinary focus on patient and team safety
Presented to ED following MVA where patient suffered multiple injuries. Trauma patient pathway not followed as Radiology interventionists felt an alternative pathway gave the patient the best chance of a
No root cause but two issues identified. There are differing views about the role of CT prior to angiography & embolisation in the management of unstable multi-trauma patients with pelvic fractures.
A new theatre / interventional suite has been opened which will allow angiograms and CT procedures to be performed in the same room. Alogrithms are being developed between all relevant services to ensure the optimal use of this facility.
120
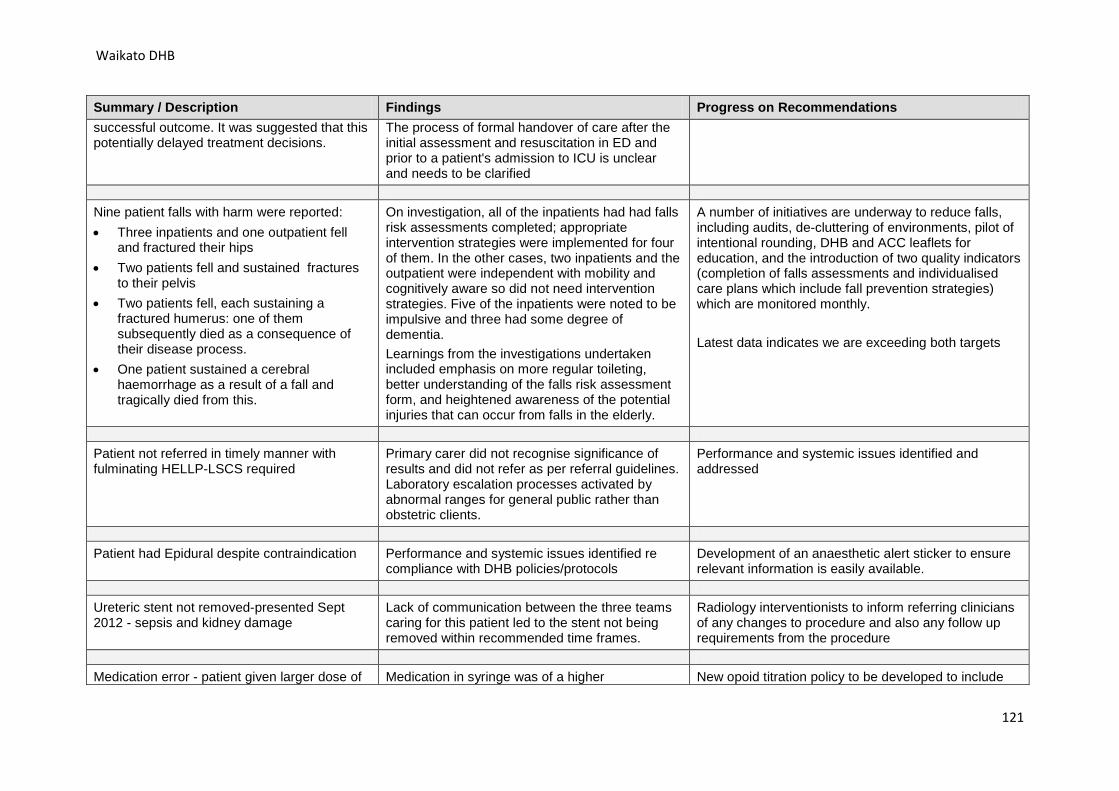
Waikato DHB
Summary / Description Findings Progress on Recommendations successful outcome. It was suggested that this potentially delayed treatment decisions.
The process of formal handover of care after the initial assessment and resuscitation in ED and prior to a patient's admission to ICU is unclear and needs to be clarified
Nine patient falls with harm were reported: • Three inpatients and one outpatient fell
and fractured their hips • Two patients fell and sustained fractures
to their pelvis • Two patients fell, each sustaining a
fractured humerus: one of them subsequently died as a consequence of their disease process.
• One patient sustained a cerebral haemorrhage as a result of a fall and tragically died from this.
On investigation, all of the inpatients had had falls risk assessments completed; appropriate intervention strategies were implemented for four of them. In the other cases, two inpatients and the outpatient were independent with mobility and cognitively aware so did not need intervention strategies. Five of the inpatients were noted to be impulsive and three had some degree of dementia. Learnings from the investigations undertaken included emphasis on more regular toileting, better understanding of the falls risk assessment form, and heightened awareness of the potential injuries that can occur from falls in the elderly.
A number of initiatives are underway to reduce falls, including audits, de-cluttering of environments, pilot of intentional rounding, DHB and ACC leaflets for education, and the introduction of two quality indicators (completion of falls assessments and individualised care plans which include fall prevention strategies) which are monitored monthly. Latest data indicates we are exceeding both targets
Patient not referred in timely manner with fulminating HELLP-LSCS required
Primary carer did not recognise significance of results and did not refer as per referral guidelines. Laboratory escalation processes activated by abnormal ranges for general public rather than obstetric clients.
Performance and systemic issues identified and addressed
Patient had Epidural despite contraindication Performance and systemic issues identified re compliance with DHB policies/protocols
Development of an anaesthetic alert sticker to ensure relevant information is easily available.
Ureteric stent not removed-presented Sept 2012 - sepsis and kidney damage
Lack of communication between the three teams caring for this patient led to the stent not being removed within recommended time frames.
Radiology interventionists to inform referring clinicians of any changes to procedure and also any follow up requirements from the procedure
Medication error - patient given larger dose of Medication in syringe was of a higher New opoid titration policy to be developed to include
121
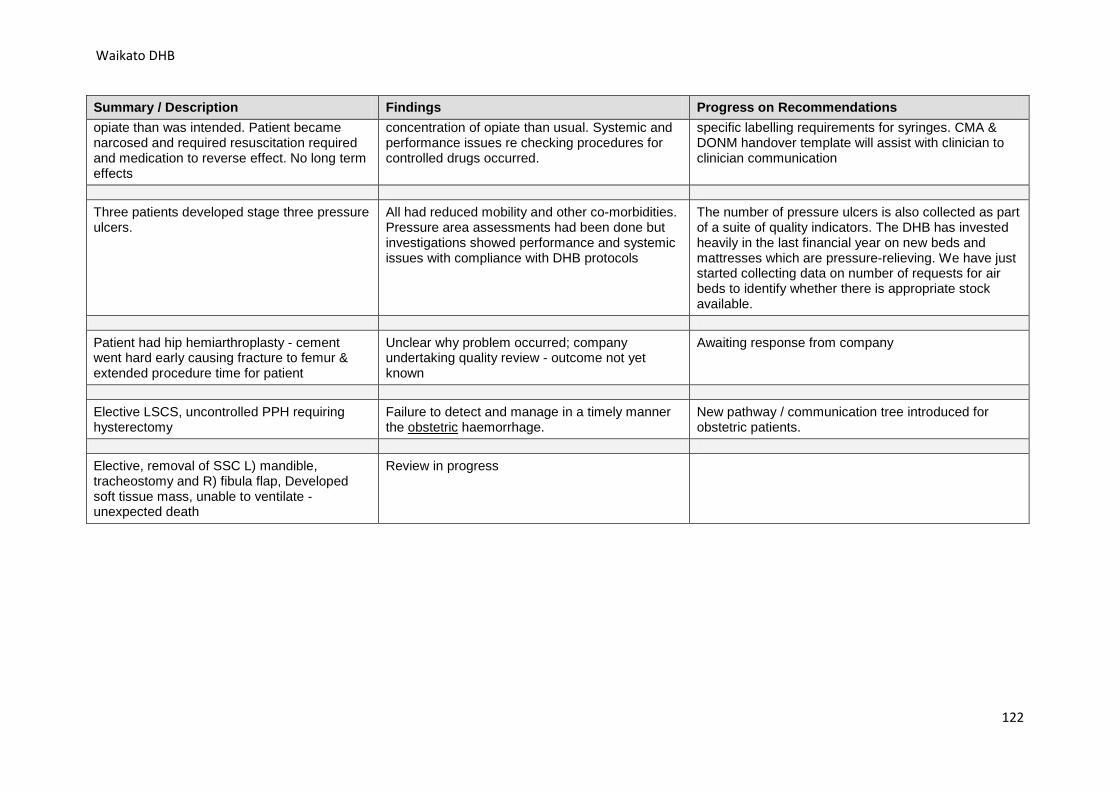
Waikato DHB
Summary / Description Findings Progress on Recommendations opiate than was intended. Patient became narcosed and required resuscitation required and medication to reverse effect. No long term effects
concentration of opiate than usual. Systemic and performance issues re checking procedures for controlled drugs occurred.
specific labelling requirements for syringes. CMA & DONM handover template will assist with clinician to clinician communication
Three patients developed stage three pressure ulcers.
All had reduced mobility and other co-morbidities. Pressure area assessments had been done but investigations showed performance and systemic issues with compliance with DHB protocols
The number of pressure ulcers is also collected as part of a suite of quality indicators. The DHB has invested heavily in the last financial year on new beds and mattresses which are pressure-relieving. We have just started collecting data on number of requests for air beds to identify whether there is appropriate stock available.
Patient had hip hemiarthroplasty - cement went hard early causing fracture to femur & extended procedure time for patient
Unclear why problem occurred; company undertaking quality review - outcome not yet known
Awaiting response from company
Elective LSCS, uncontrolled PPH requiring hysterectomy
Failure to detect and manage in a timely manner the obstetric haemorrhage.
New pathway / communication tree introduced for obstetric patients.
Elective, removal of SSC L) mandible, tracheostomy and R) fibula flap, Developed soft tissue mass, unable to ventilate - unexpected death
Review in progress
122
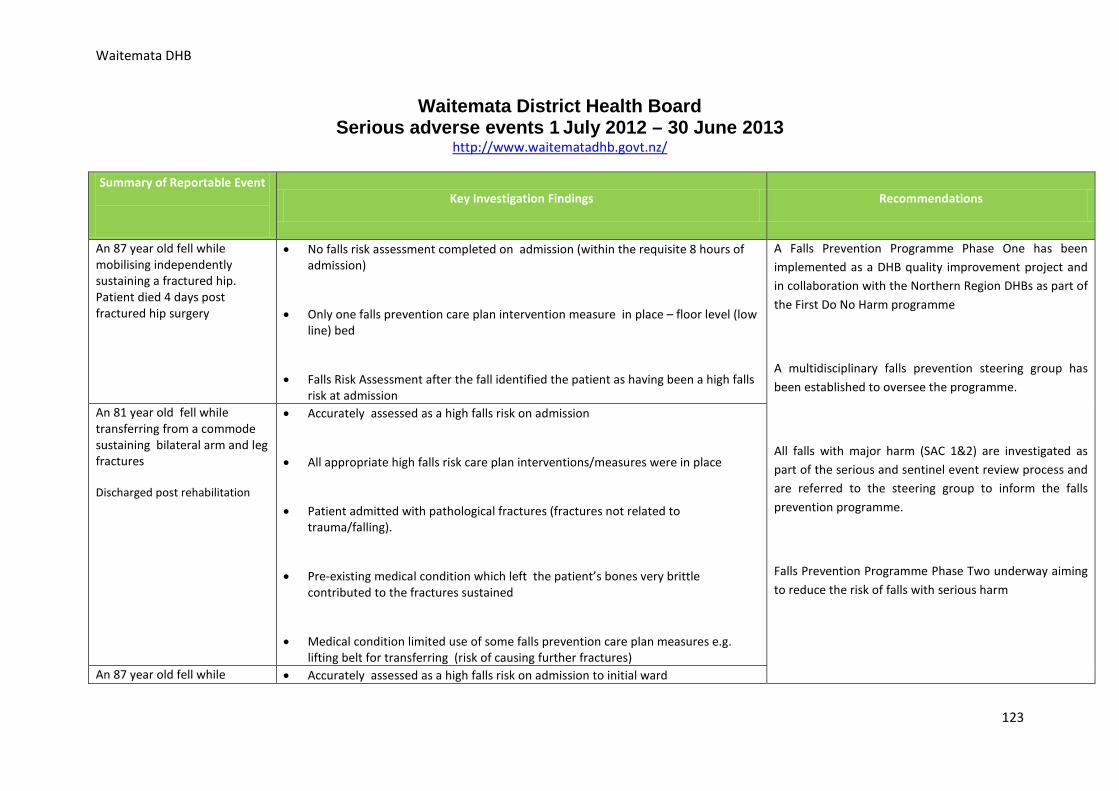
Waitemata DHB
Waitemata District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.waitematadhb.govt.nz/
Summary of Reportable Event
Key Investigation Findings Recommendations
An 87 year old fell while mobilising independently sustaining a fractured hip. Patient died 4 days post fractured hip surgery
• No falls risk assessment completed on admission (within the requisite 8 hours of admission)
• Only one falls prevention care plan intervention measure in place – floor level (low line) bed
• Falls Risk Assessment after the fall identified the patient as having been a high falls risk at admission
A Falls Prevention Programme Phase One has been implemented as a DHB quality improvement project and in collaboration with the Northern Region DHBs as part of the First Do No Harm programme
A multidisciplinary falls prevention steering group has been established to oversee the programme.
All falls with major harm (SAC 1&2) are investigated as part of the serious and sentinel event review process and are referred to the steering group to inform the falls prevention programme.
Falls Prevention Programme Phase Two underway aiming to reduce the risk of falls with serious harm
An 81 year old fell while transferring from a commode sustaining bilateral arm and leg fractures Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk care plan interventions/measures were in place
• Patient admitted with pathological fractures (fractures not related to trauma/falling).
• Pre-existing medical condition which left the patient’s bones very brittle contributed to the fractures sustained
• Medical condition limited use of some falls prevention care plan measures e.g. lifting belt for transferring (risk of causing further fractures)
An 87 year old fell while • Accurately assessed as a high falls risk on admission to initial ward
123
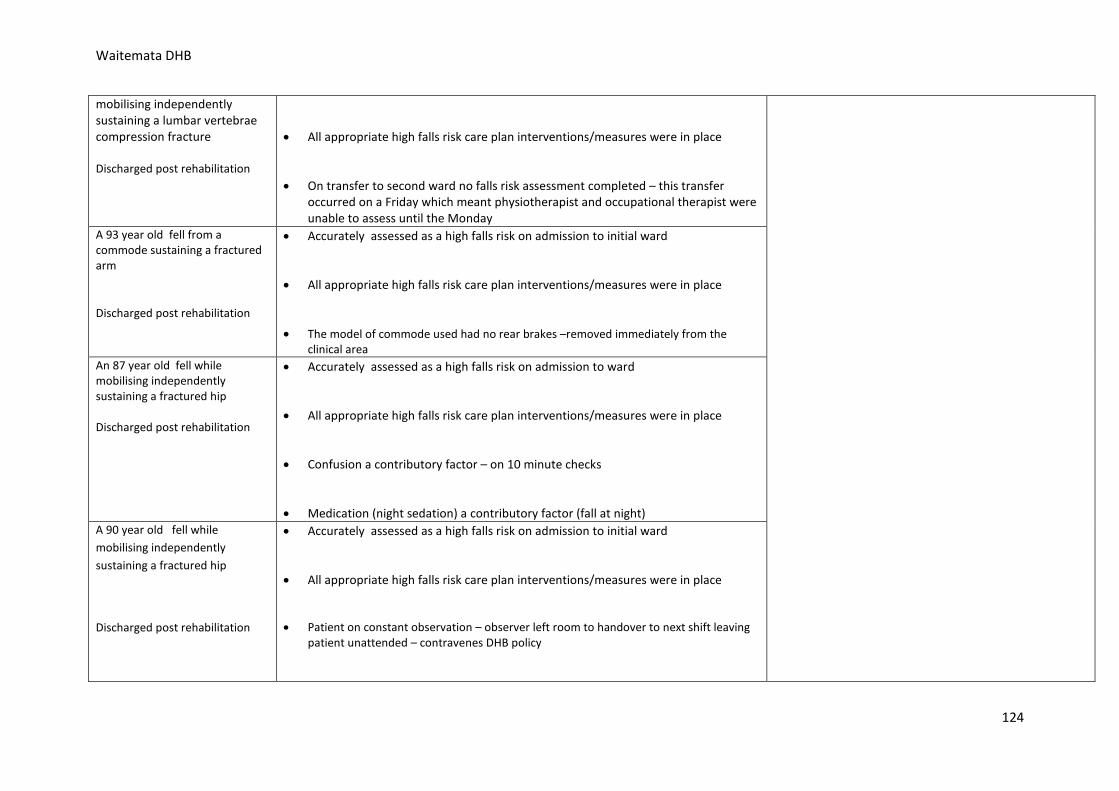
Waitemata DHB
mobilising independently sustaining a lumbar vertebrae compression fracture Discharged post rehabilitation
• All appropriate high falls risk care plan interventions/measures were in place
• On transfer to second ward no falls risk assessment completed – this transfer occurred on a Friday which meant physiotherapist and occupational therapist were unable to assess until the Monday
A 93 year old fell from a commode sustaining a fractured arm
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission to initial ward
• All appropriate high falls risk care plan interventions/measures were in place
• The model of commode used had no rear brakes –removed immediately from the clinical area
An 87 year old fell while mobilising independently sustaining a fractured hip Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission to ward
• All appropriate high falls risk care plan interventions/measures were in place
• Confusion a contributory factor – on 10 minute checks
• Medication (night sedation) a contributory factor (fall at night) A 90 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission to initial ward
• All appropriate high falls risk care plan interventions/measures were in place
• Patient on constant observation – observer left room to handover to next shift leaving patient unattended – contravenes DHB policy
124
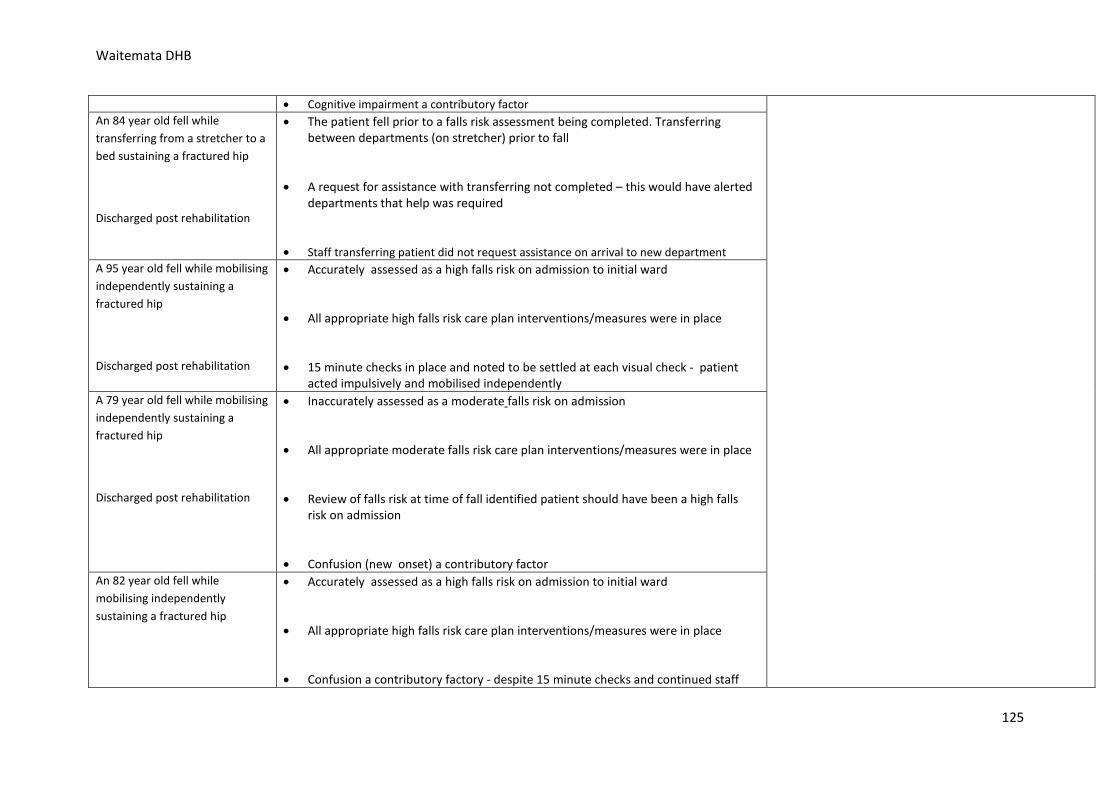
Waitemata DHB
• Cognitive impairment a contributory factor An 84 year old fell while transferring from a stretcher to a bed sustaining a fractured hip
Discharged post rehabilitation
• The patient fell prior to a falls risk assessment being completed. Transferring between departments (on stretcher) prior to fall
• A request for assistance with transferring not completed – this would have alerted departments that help was required
• Staff transferring patient did not request assistance on arrival to new department A 95 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission to initial ward
• All appropriate high falls risk care plan interventions/measures were in place
• 15 minute checks in place and noted to be settled at each visual check - patient acted impulsively and mobilised independently
A 79 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Inaccurately assessed as a moderate falls risk on admission
• All appropriate moderate falls risk care plan interventions/measures were in place
• Review of falls risk at time of fall identified patient should have been a high falls risk on admission
• Confusion (new onset) a contributory factor An 82 year old fell while mobilising independently sustaining a fractured hip
• Accurately assessed as a high falls risk on admission to initial ward
• All appropriate high falls risk care plan interventions/measures were in place
• Confusion a contributory factory - despite 15 minute checks and continued staff
125
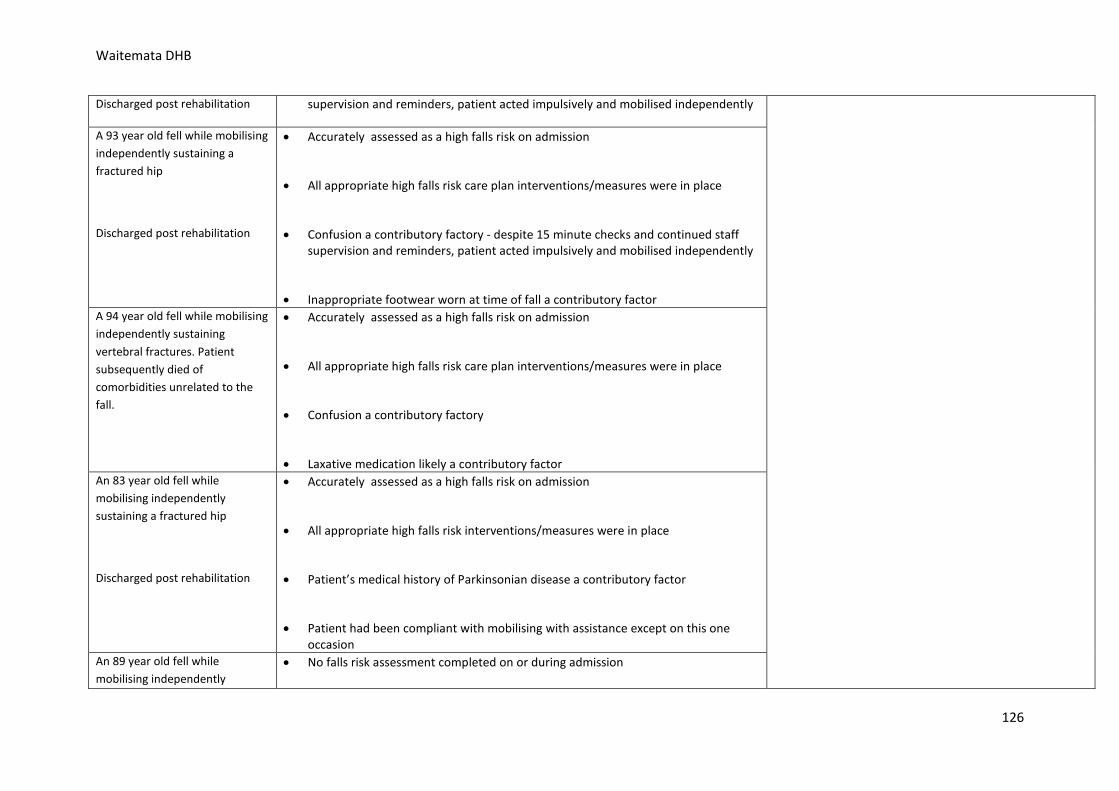
Waitemata DHB
Discharged post rehabilitation supervision and reminders, patient acted impulsively and mobilised independently
A 93 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk care plan interventions/measures were in place
• Confusion a contributory factory - despite 15 minute checks and continued staff supervision and reminders, patient acted impulsively and mobilised independently
• Inappropriate footwear worn at time of fall a contributory factor A 94 year old fell while mobilising independently sustaining vertebral fractures. Patient subsequently died of comorbidities unrelated to the fall.
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk care plan interventions/measures were in place
• Confusion a contributory factory
• Laxative medication likely a contributory factor An 83 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place
• Patient’s medical history of Parkinsonian disease a contributory factor
• Patient had been compliant with mobilising with assistance except on this one occasion
An 89 year old fell while mobilising independently
• No falls risk assessment completed on or during admission
126
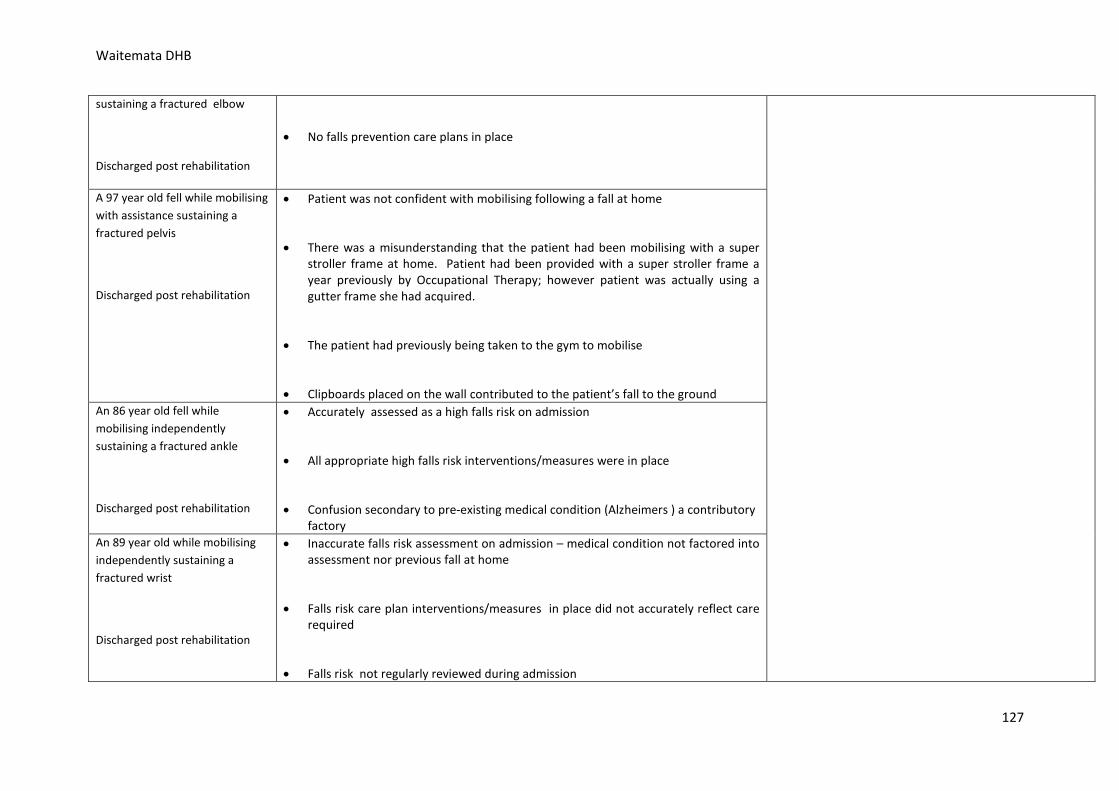
Waitemata DHB
sustaining a fractured elbow
Discharged post rehabilitation
• No falls prevention care plans in place
A 97 year old fell while mobilising with assistance sustaining a fractured pelvis
Discharged post rehabilitation
• Patient was not confident with mobilising following a fall at home
• There was a misunderstanding that the patient had been mobilising with a super stroller frame at home. Patient had been provided with a super stroller frame a year previously by Occupational Therapy; however patient was actually using a gutter frame she had acquired.
• The patient had previously being taken to the gym to mobilise
• Clipboards placed on the wall contributed to the patient’s fall to the ground An 86 year old fell while mobilising independently sustaining a fractured ankle
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place
• Confusion secondary to pre-existing medical condition (Alzheimers ) a contributory factory
An 89 year old while mobilising independently sustaining a fractured wrist
Discharged post rehabilitation
• Inaccurate falls risk assessment on admission – medical condition not factored into assessment nor previous fall at home
• Falls risk care plan interventions/measures in place did not accurately reflect care required
• Falls risk not regularly reviewed during admission
127
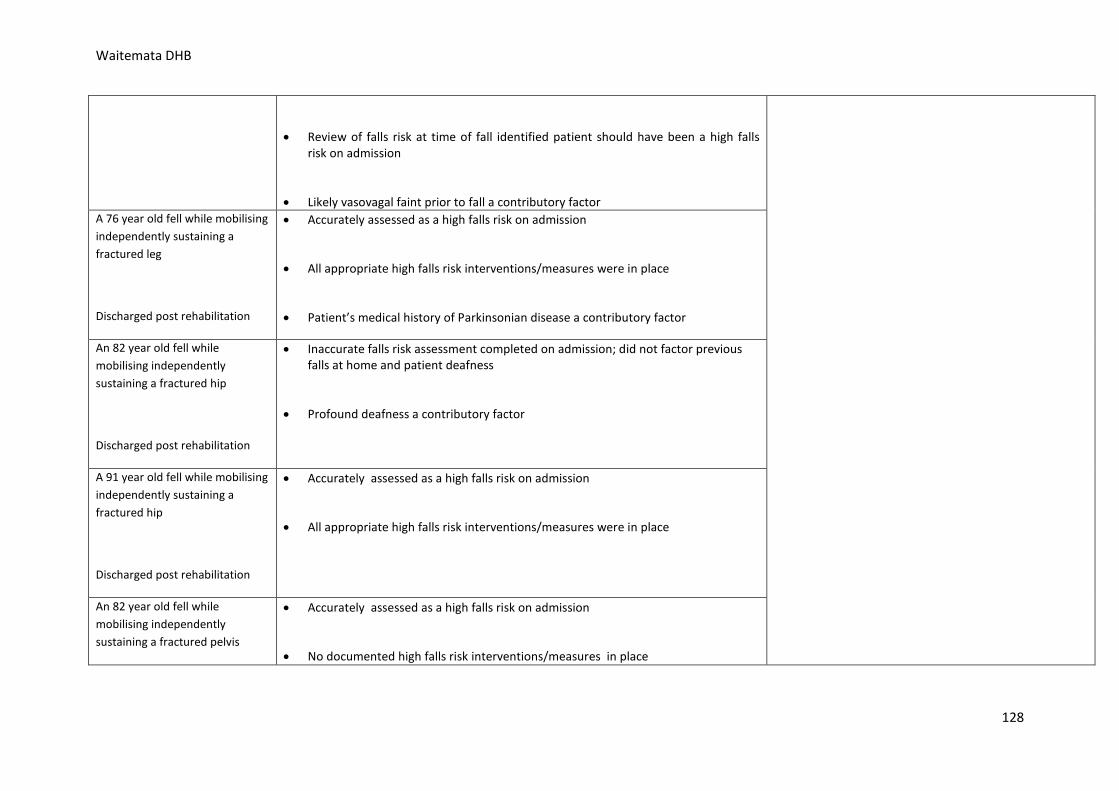
Waitemata DHB
• Review of falls risk at time of fall identified patient should have been a high falls risk on admission
• Likely vasovagal faint prior to fall a contributory factor A 76 year old fell while mobilising independently sustaining a fractured leg
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place
• Patient’s medical history of Parkinsonian disease a contributory factor
An 82 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Inaccurate falls risk assessment completed on admission; did not factor previous falls at home and patient deafness
• Profound deafness a contributory factor
A 91 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place
An 82 year old fell while mobilising independently sustaining a fractured pelvis
• Accurately assessed as a high falls risk on admission
• No documented high falls risk interventions/measures in place
128
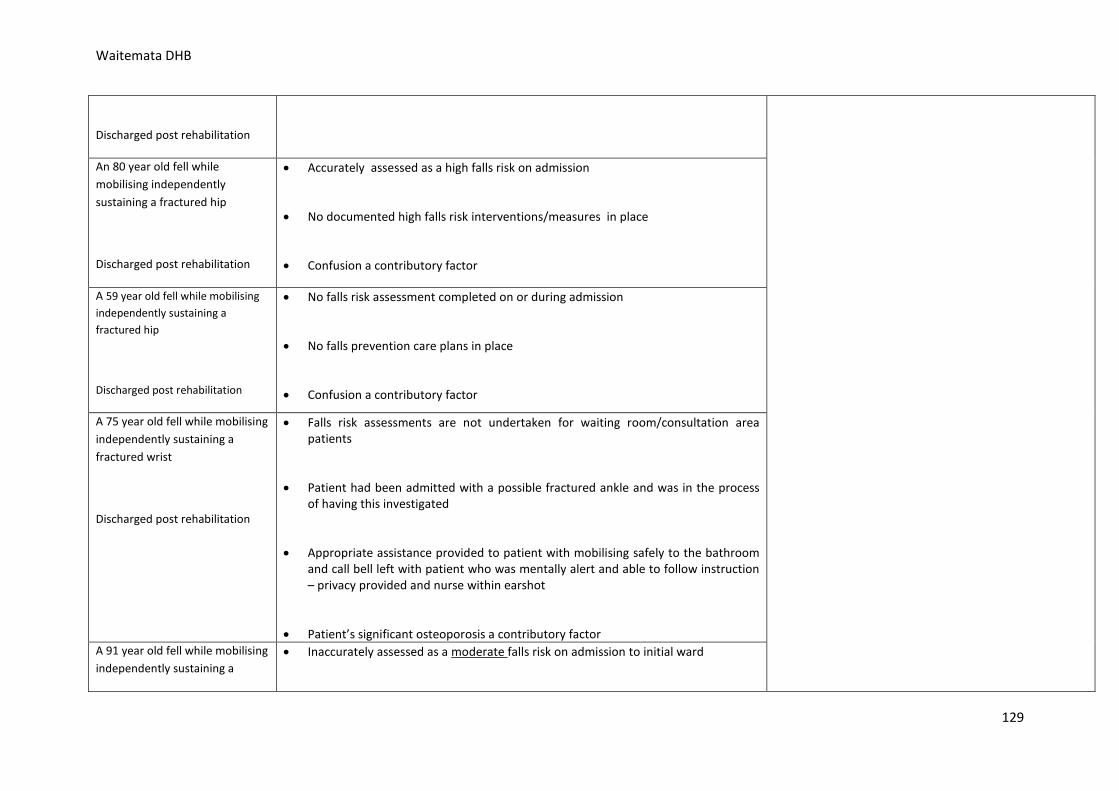
Waitemata DHB
Discharged post rehabilitation
An 80 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• No documented high falls risk interventions/measures in place
• Confusion a contributory factor
A 59 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• No falls risk assessment completed on or during admission
• No falls prevention care plans in place
• Confusion a contributory factor
A 75 year old fell while mobilising independently sustaining a fractured wrist
Discharged post rehabilitation
• Falls risk assessments are not undertaken for waiting room/consultation area patients
• Patient had been admitted with a possible fractured ankle and was in the process of having this investigated
• Appropriate assistance provided to patient with mobilising safely to the bathroom and call bell left with patient who was mentally alert and able to follow instruction – privacy provided and nurse within earshot
• Patient’s significant osteoporosis a contributory factor A 91 year old fell while mobilising independently sustaining a
• Inaccurately assessed as a moderate falls risk on admission to initial ward
129
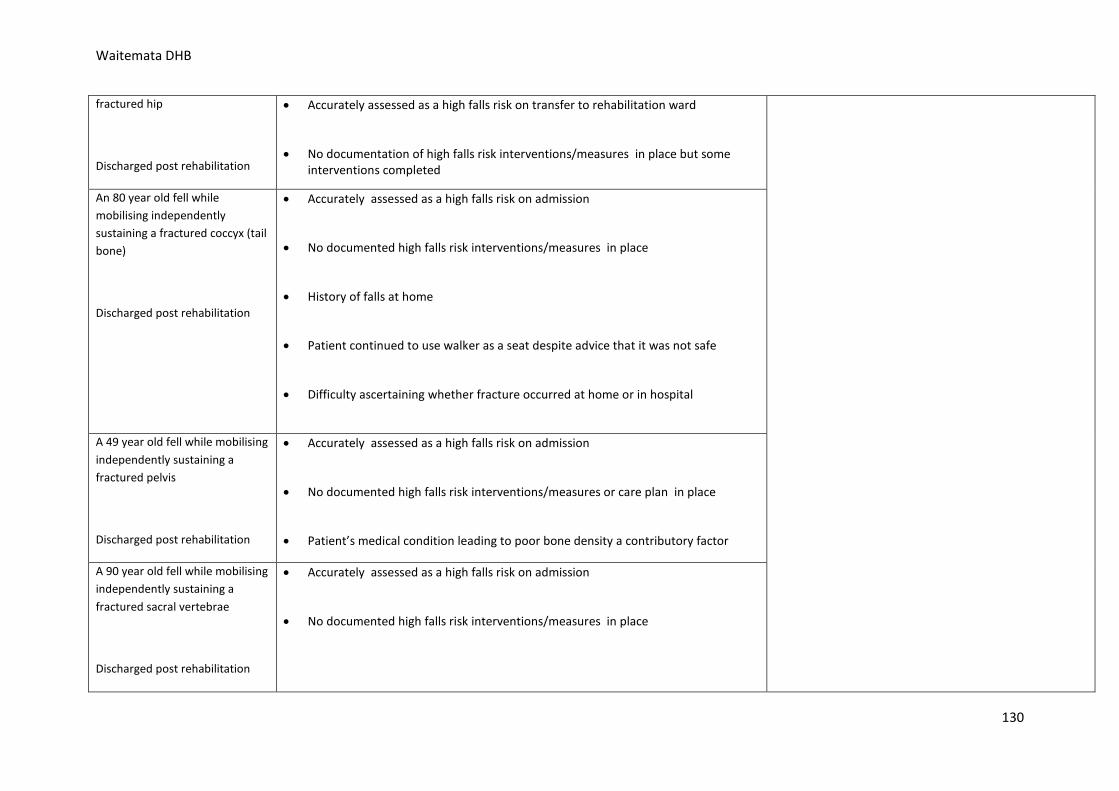
Waitemata DHB
fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on transfer to rehabilitation ward
• No documentation of high falls risk interventions/measures in place but some interventions completed
An 80 year old fell while mobilising independently sustaining a fractured coccyx (tail bone)
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• No documented high falls risk interventions/measures in place
• History of falls at home
• Patient continued to use walker as a seat despite advice that it was not safe
• Difficulty ascertaining whether fracture occurred at home or in hospital
A 49 year old fell while mobilising independently sustaining a fractured pelvis
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• No documented high falls risk interventions/measures or care plan in place
• Patient’s medical condition leading to poor bone density a contributory factor
A 90 year old fell while mobilising independently sustaining a fractured sacral vertebrae
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• No documented high falls risk interventions/measures in place
130
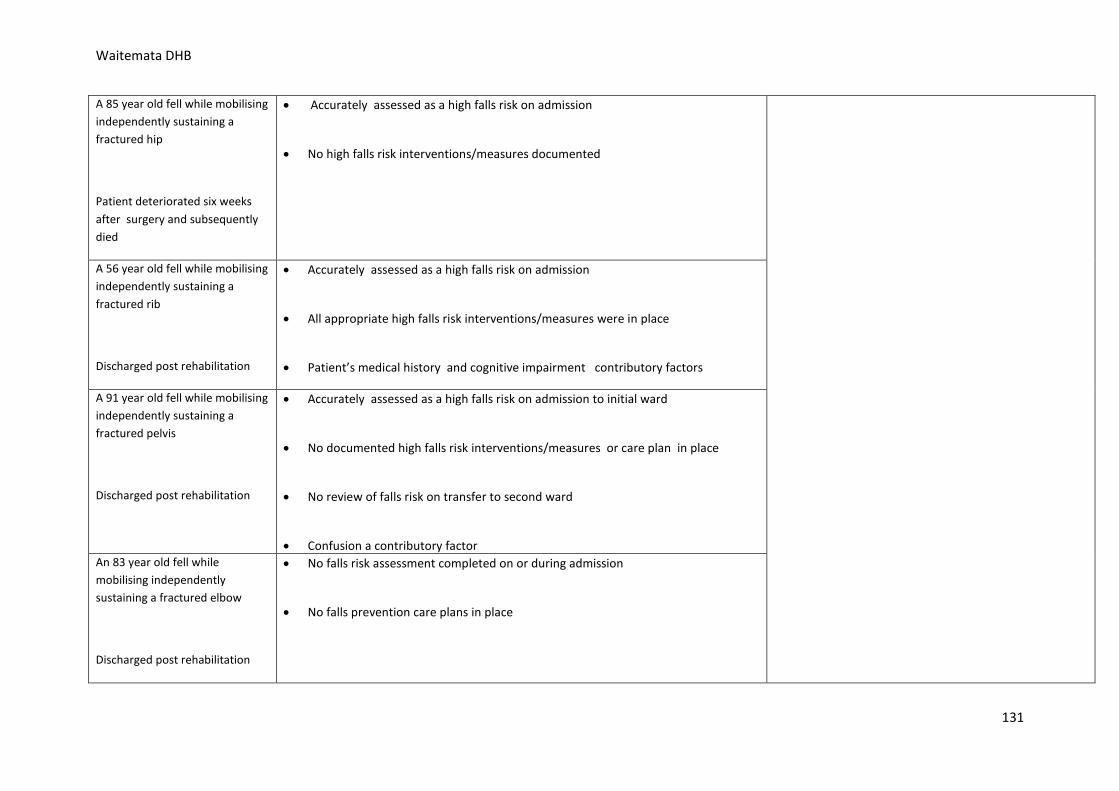
Waitemata DHB
A 85 year old fell while mobilising independently sustaining a fractured hip
Patient deteriorated six weeks after surgery and subsequently died
• Accurately assessed as a high falls risk on admission
• No high falls risk interventions/measures documented
A 56 year old fell while mobilising independently sustaining a fractured rib
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place
• Patient’s medical history and cognitive impairment contributory factors
A 91 year old fell while mobilising independently sustaining a fractured pelvis
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission to initial ward
• No documented high falls risk interventions/measures or care plan in place
• No review of falls risk on transfer to second ward
• Confusion a contributory factor An 83 year old fell while mobilising independently sustaining a fractured elbow
Discharged post rehabilitation
• No falls risk assessment completed on or during admission
• No falls prevention care plans in place
131
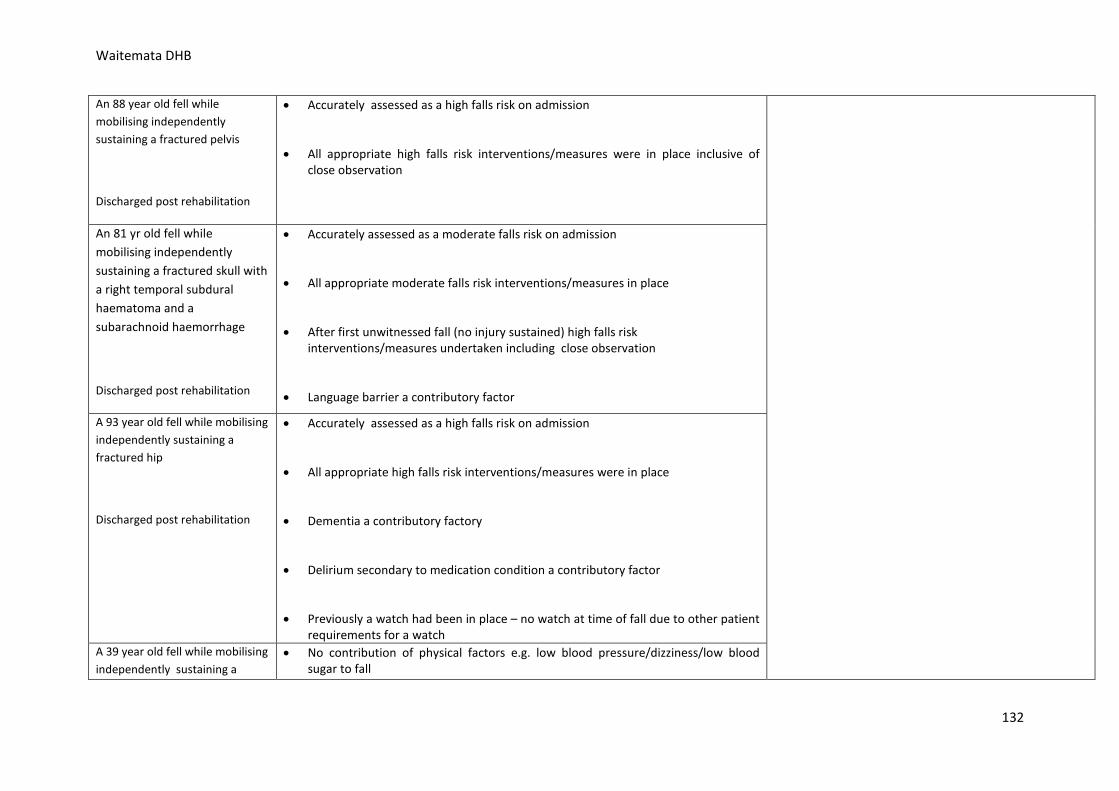
Waitemata DHB
An 88 year old fell while mobilising independently sustaining a fractured pelvis
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place inclusive of close observation
An 81 yr old fell while mobilising independently sustaining a fractured skull with a right temporal subdural haematoma and a subarachnoid haemorrhage
Discharged post rehabilitation
• Accurately assessed as a moderate falls risk on admission
• All appropriate moderate falls risk interventions/measures in place
• After first unwitnessed fall (no injury sustained) high falls risk interventions/measures undertaken including close observation
• Language barrier a contributory factor
A 93 year old fell while mobilising independently sustaining a fractured hip
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission
• All appropriate high falls risk interventions/measures were in place
• Dementia a contributory factory
• Delirium secondary to medication condition a contributory factor
• Previously a watch had been in place – no watch at time of fall due to other patient requirements for a watch
A 39 year old fell while mobilising independently sustaining a
• No contribution of physical factors e.g. low blood pressure/dizziness/low blood sugar to fall
132
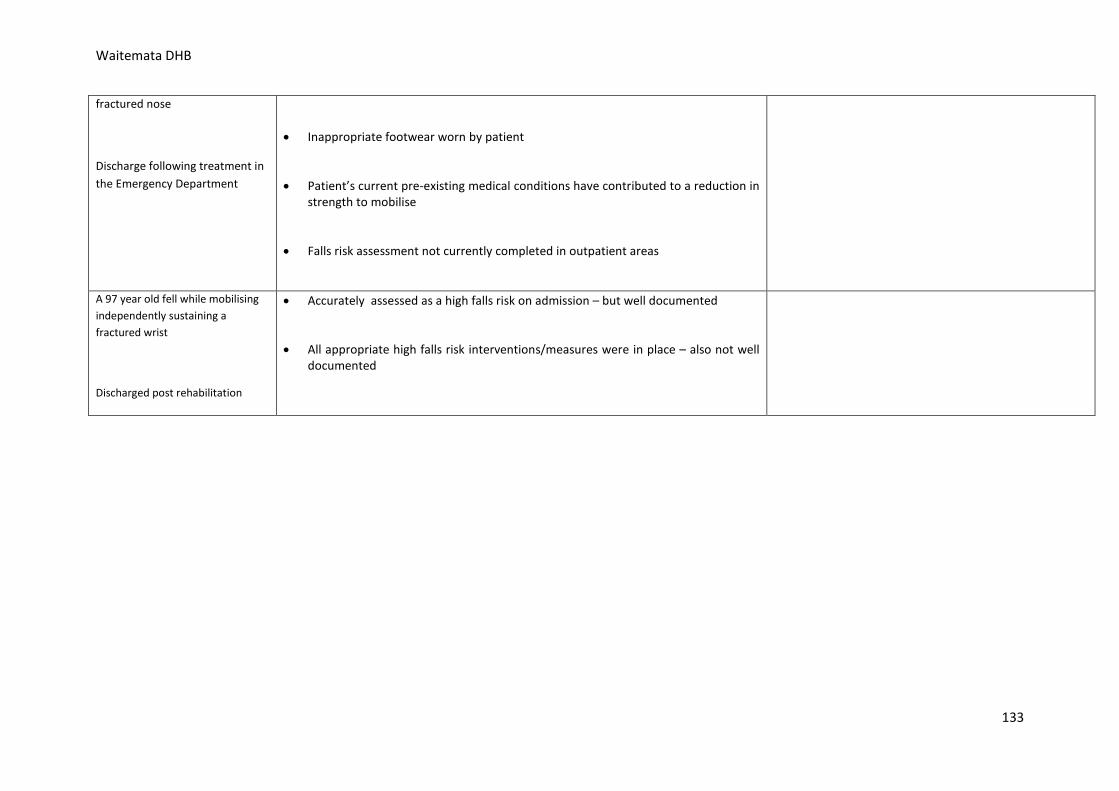
Waitemata DHB
fractured nose
Discharge following treatment in the Emergency Department
• Inappropriate footwear worn by patient
• Patient’s current pre-existing medical conditions have contributed to a reduction in strength to mobilise
• Falls risk assessment not currently completed in outpatient areas
A 97 year old fell while mobilising independently sustaining a fractured wrist
Discharged post rehabilitation
• Accurately assessed as a high falls risk on admission – but well documented
• All appropriate high falls risk interventions/measures were in place – also not well documented
133
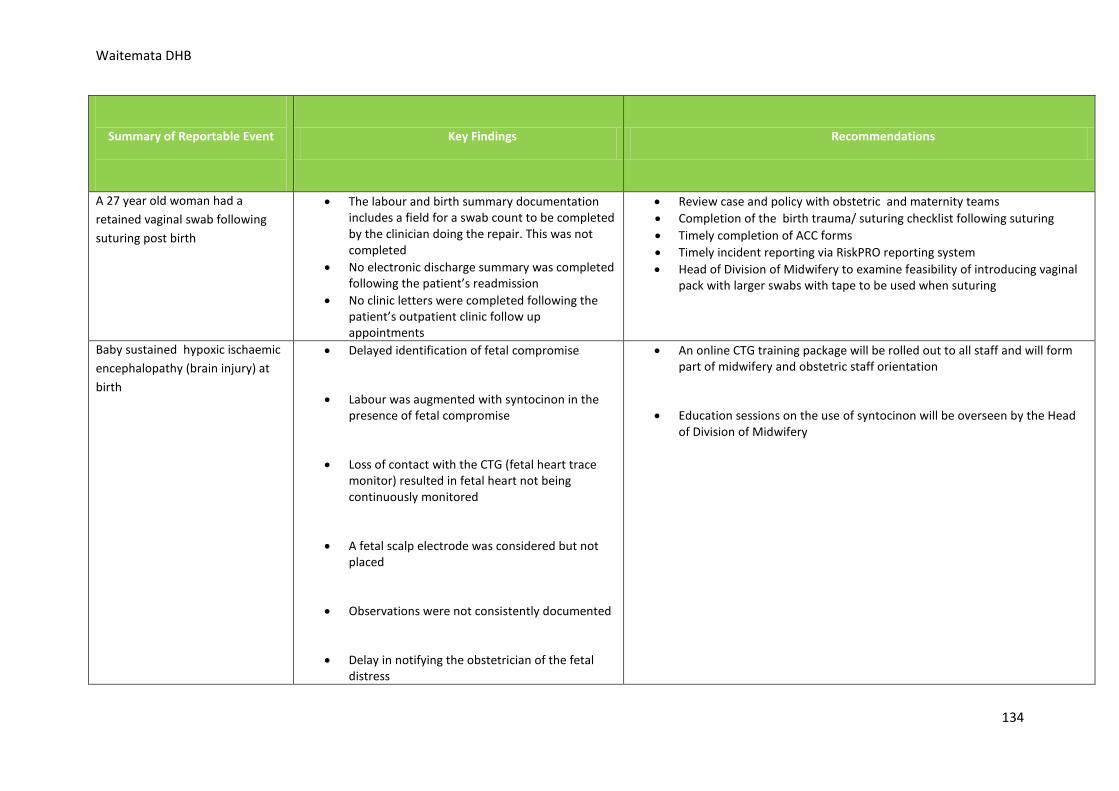
Waitemata DHB
Summary of Reportable Event
Key Findings Recommendations
A 27 year old woman had a retained vaginal swab following suturing post birth
• The labour and birth summary documentation includes a field for a swab count to be completed by the clinician doing the repair. This was not completed
• No electronic discharge summary was completed following the patient’s readmission
• No clinic letters were completed following the patient’s outpatient clinic follow up appointments
• Review case and policy with obstetric and maternity teams • Completion of the birth trauma/ suturing checklist following suturing • Timely completion of ACC forms • Timely incident reporting via RiskPRO reporting system • Head of Division of Midwifery to examine feasibility of introducing vaginal
pack with larger swabs with tape to be used when suturing
Baby sustained hypoxic ischaemic encephalopathy (brain injury) at birth
• Delayed identification of fetal compromise
• Labour was augmented with syntocinon in the presence of fetal compromise
• Loss of contact with the CTG (fetal heart trace monitor) resulted in fetal heart not being continuously monitored
• A fetal scalp electrode was considered but not placed
• Observations were not consistently documented
• Delay in notifying the obstetrician of the fetal distress
• An online CTG training package will be rolled out to all staff and will form part of midwifery and obstetric staff orientation
• Education sessions on the use of syntocinon will be overseen by the Head of Division of Midwifery
134
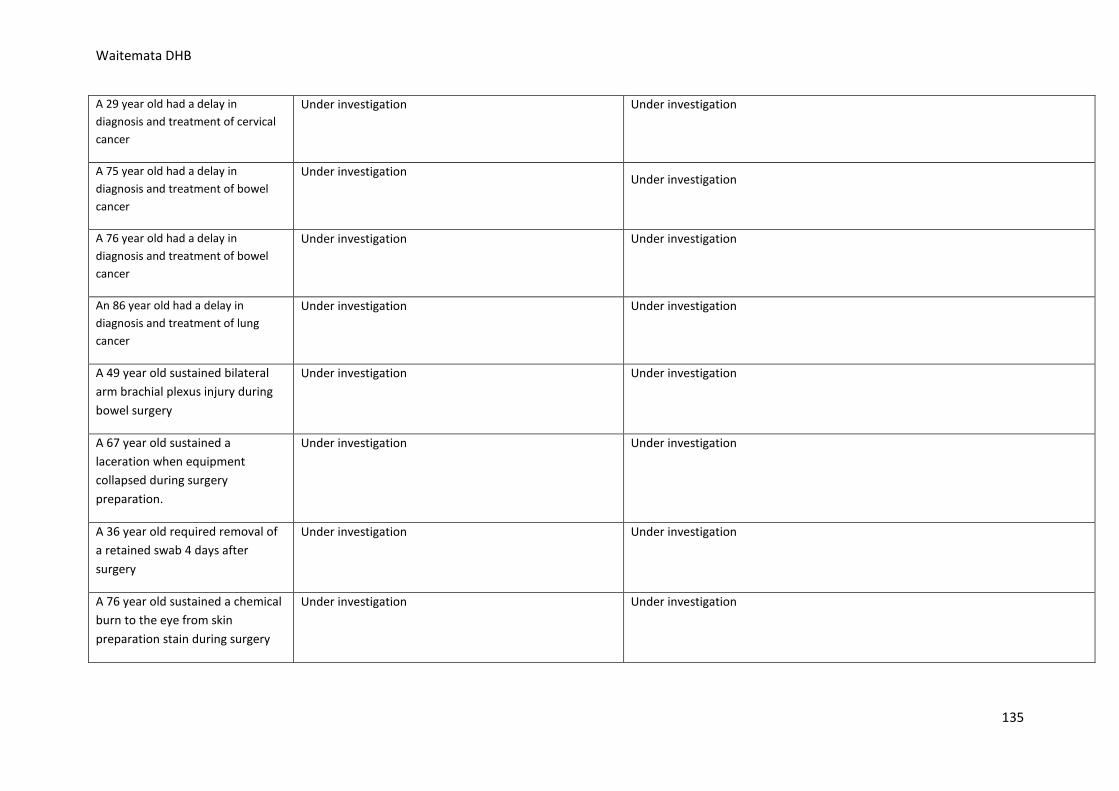
Waitemata DHB
A 29 year old had a delay in diagnosis and treatment of cervical cancer
Under investigation Under investigation
A 75 year old had a delay in diagnosis and treatment of bowel cancer
Under investigation Under investigation
A 76 year old had a delay in diagnosis and treatment of bowel cancer
Under investigation Under investigation
An 86 year old had a delay in diagnosis and treatment of lung cancer
Under investigation Under investigation
A 49 year old sustained bilateral arm brachial plexus injury during bowel surgery
Under investigation Under investigation
A 67 year old sustained a laceration when equipment collapsed during surgery preparation.
Under investigation Under investigation
A 36 year old required removal of a retained swab 4 days after surgery
Under investigation Under investigation
A 76 year old sustained a chemical burn to the eye from skin preparation stain during surgery
Under investigation Under investigation
135
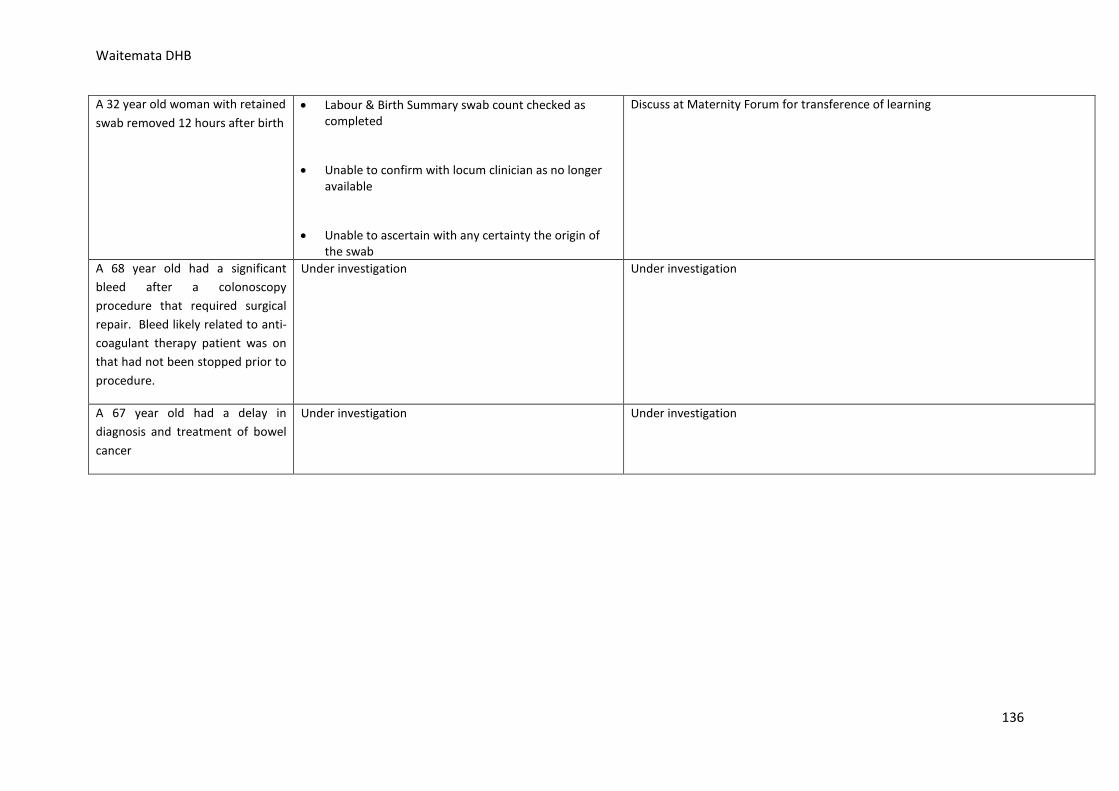
Waitemata DHB
A 32 year old woman with retained swab removed 12 hours after birth
• Labour & Birth Summary swab count checked as completed
• Unable to confirm with locum clinician as no longer available
• Unable to ascertain with any certainty the origin of the swab
Discuss at Maternity Forum for transference of learning
A 68 year old had a significant bleed after a colonoscopy procedure that required surgical repair. Bleed likely related to anti-coagulant therapy patient was on that had not been stopped prior to procedure.
Under investigation Under investigation
A 67 year old had a delay in diagnosis and treatment of bowel cancer
Under investigation Under investigation
136
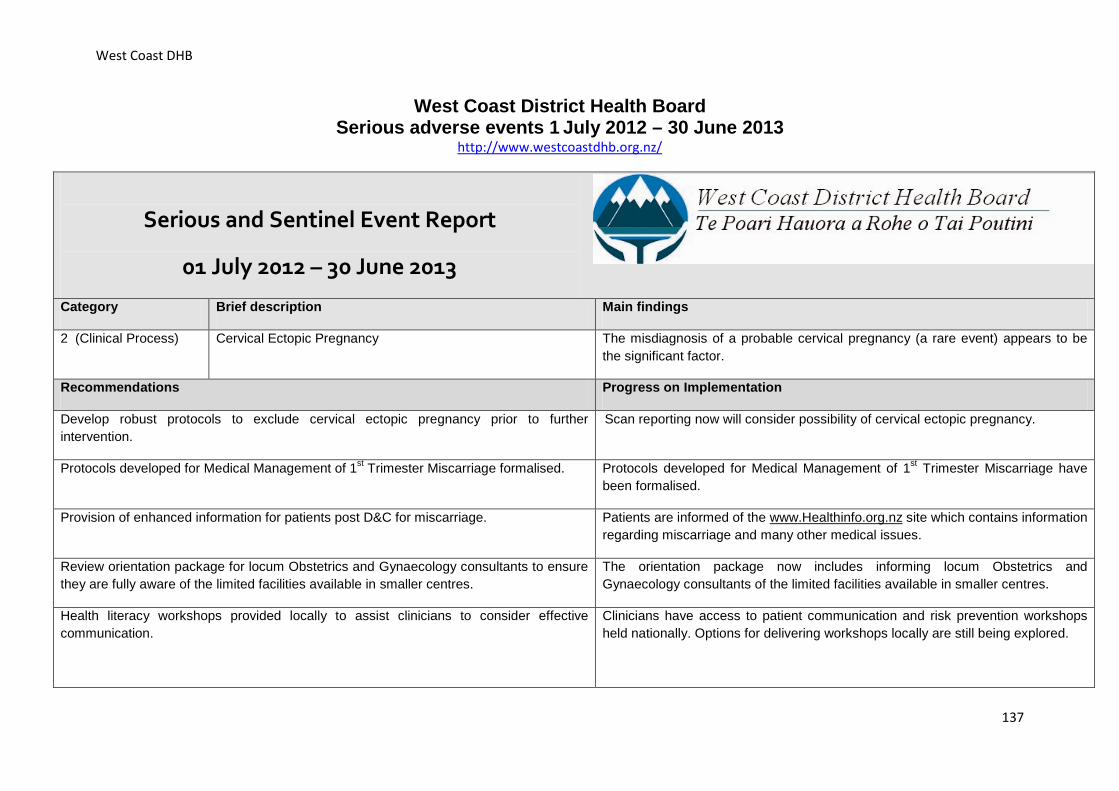
West Coast DHB
West Coast District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.westcoastdhb.org.nz/
Serious and Sentinel Event Report
01 July 2012 – 30 June 2013
Category Brief description Main findings
2 (Clinical Process) Cervical Ectopic Pregnancy The misdiagnosis of a probable cervical pregnancy (a rare event) appears to be the significant factor.
Recommendations Progress on Implementation
Develop robust protocols to exclude cervical ectopic pregnancy prior to further intervention.
Scan reporting now will consider possibility of cervical ectopic pregnancy.
Protocols developed for Medical Management of 1st Trimester Miscarriage formalised. Protocols developed for Medical Management of 1st Trimester Miscarriage have been formalised.
Provision of enhanced information for patients post D&C for miscarriage. Patients are informed of the www.Healthinfo.org.nz site which contains information regarding miscarriage and many other medical issues.
Review orientation package for locum Obstetrics and Gynaecology consultants to ensure they are fully aware of the limited facilities available in smaller centres.
The orientation package now includes informing locum Obstetrics and Gynaecology consultants of the limited facilities available in smaller centres.
Health literacy workshops provided locally to assist clinicians to consider effective communication.
Clinicians have access to patient communication and risk prevention workshops held nationally. Options for delivering workshops locally are still being explored.
137
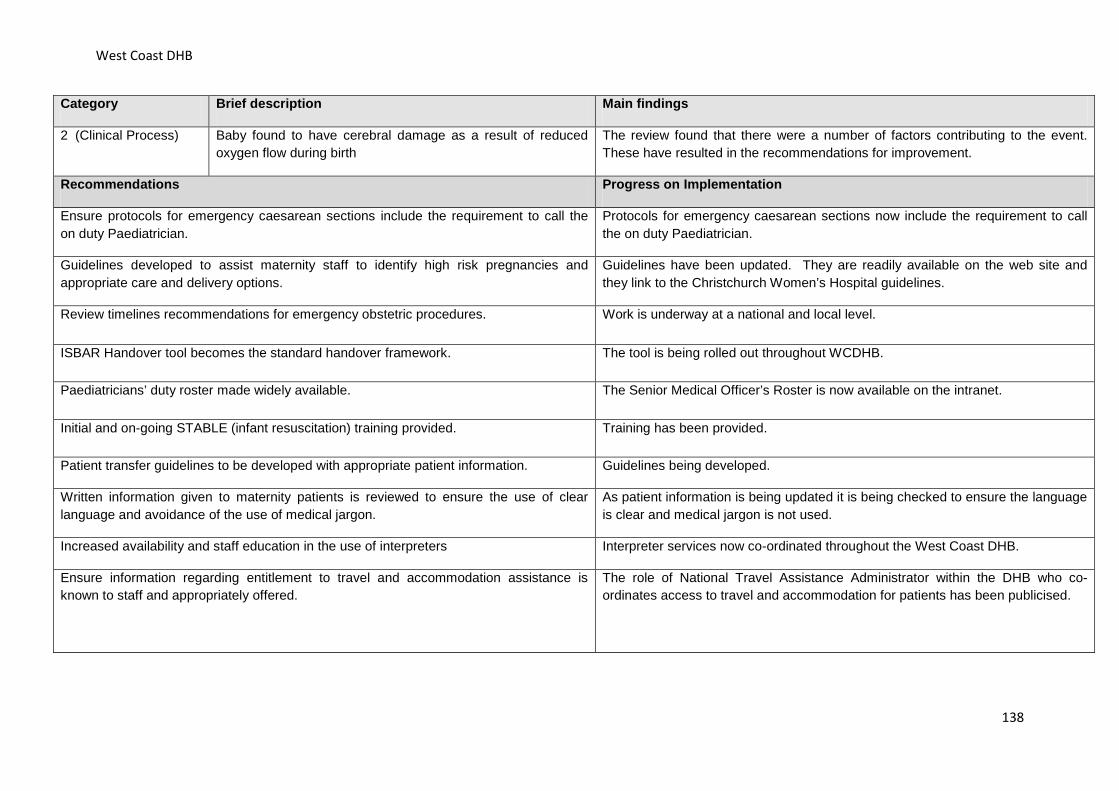
West Coast DHB
Category Brief description Main findings
2 (Clinical Process) Baby found to have cerebral damage as a result of reduced oxygen flow during birth
The review found that there were a number of factors contributing to the event. These have resulted in the recommendations for improvement.
Recommendations Progress on Implementation
Ensure protocols for emergency caesarean sections include the requirement to call the on duty Paediatrician.
Protocols for emergency caesarean sections now include the requirement to call the on duty Paediatrician.
Guidelines developed to assist maternity staff to identify high risk pregnancies and appropriate care and delivery options.
Guidelines have been updated. They are readily available on the web site and they link to the Christchurch Women’s Hospital guidelines.
Review timelines recommendations for emergency obstetric procedures. Work is underway at a national and local level.
ISBAR Handover tool becomes the standard handover framework. The tool is being rolled out throughout WCDHB.
Paediatricians’ duty roster made widely available. The Senior Medical Officer’s Roster is now available on the intranet.
Initial and on-going STABLE (infant resuscitation) training provided. Training has been provided.
Patient transfer guidelines to be developed with appropriate patient information. Guidelines being developed.
Written information given to maternity patients is reviewed to ensure the use of clear language and avoidance of the use of medical jargon.
As patient information is being updated it is being checked to ensure the language is clear and medical jargon is not used.
Increased availability and staff education in the use of interpreters Interpreter services now co-ordinated throughout the West Coast DHB.
Ensure information regarding entitlement to travel and accommodation assistance is known to staff and appropriately offered.
The role of National Travel Assistance Administrator within the DHB who co-ordinates access to travel and accommodation for patients has been publicised.
138
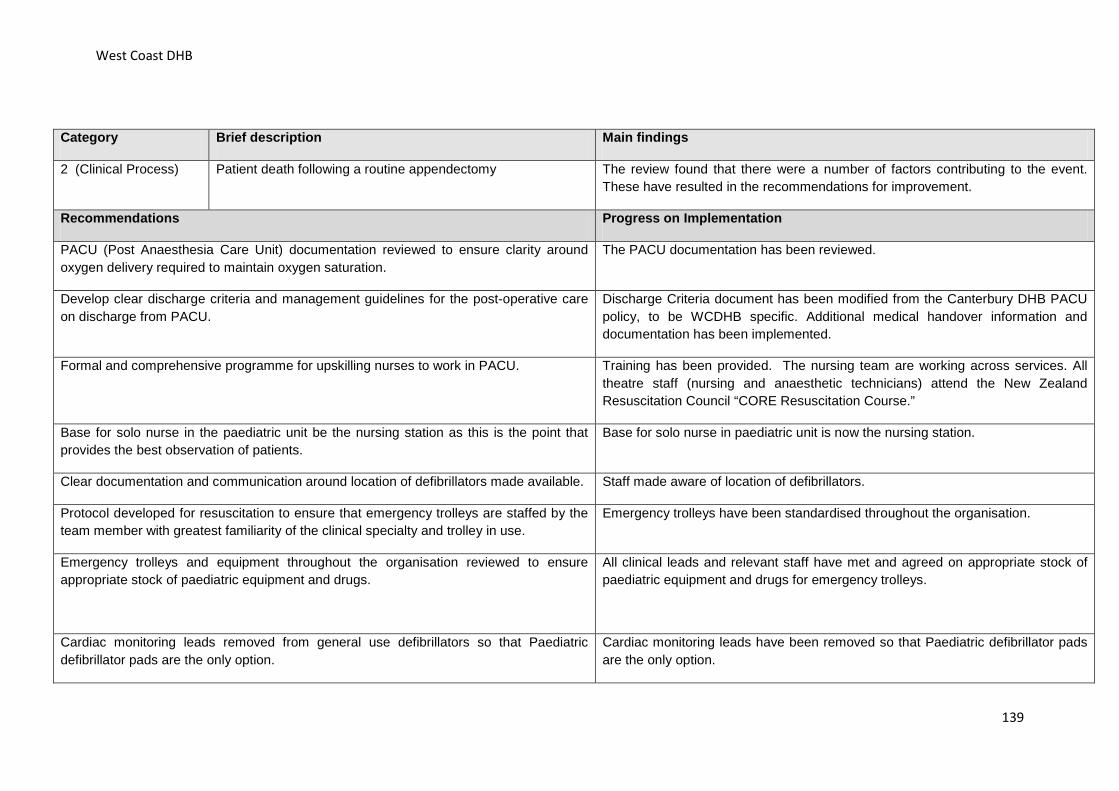
West Coast DHB
Category Brief description Main findings
2 (Clinical Process) Patient death following a routine appendectomy The review found that there were a number of factors contributing to the event. These have resulted in the recommendations for improvement.
Recommendations Progress on Implementation
PACU (Post Anaesthesia Care Unit) documentation reviewed to ensure clarity around oxygen delivery required to maintain oxygen saturation.
The PACU documentation has been reviewed.
Develop clear discharge criteria and management guidelines for the post-operative care on discharge from PACU.
Discharge Criteria document has been modified from the Canterbury DHB PACU policy, to be WCDHB specific. Additional medical handover information and documentation has been implemented.
Formal and comprehensive programme for upskilling nurses to work in PACU. Training has been provided. The nursing team are working across services. All theatre staff (nursing and anaesthetic technicians) attend the New Zealand Resuscitation Council “CORE Resuscitation Course.”
Base for solo nurse in the paediatric unit be the nursing station as this is the point that provides the best observation of patients.
Base for solo nurse in paediatric unit is now the nursing station.
Clear documentation and communication around location of defibrillators made available. Staff made aware of location of defibrillators.
Protocol developed for resuscitation to ensure that emergency trolleys are staffed by the team member with greatest familiarity of the clinical specialty and trolley in use.
Emergency trolleys have been standardised throughout the organisation.
Emergency trolleys and equipment throughout the organisation reviewed to ensure appropriate stock of paediatric equipment and drugs.
All clinical leads and relevant staff have met and agreed on appropriate stock of paediatric equipment and drugs for emergency trolleys.
Cardiac monitoring leads removed from general use defibrillators so that Paediatric defibrillator pads are the only option.
Cardiac monitoring leads have been removed so that Paediatric defibrillator pads are the only option.
139
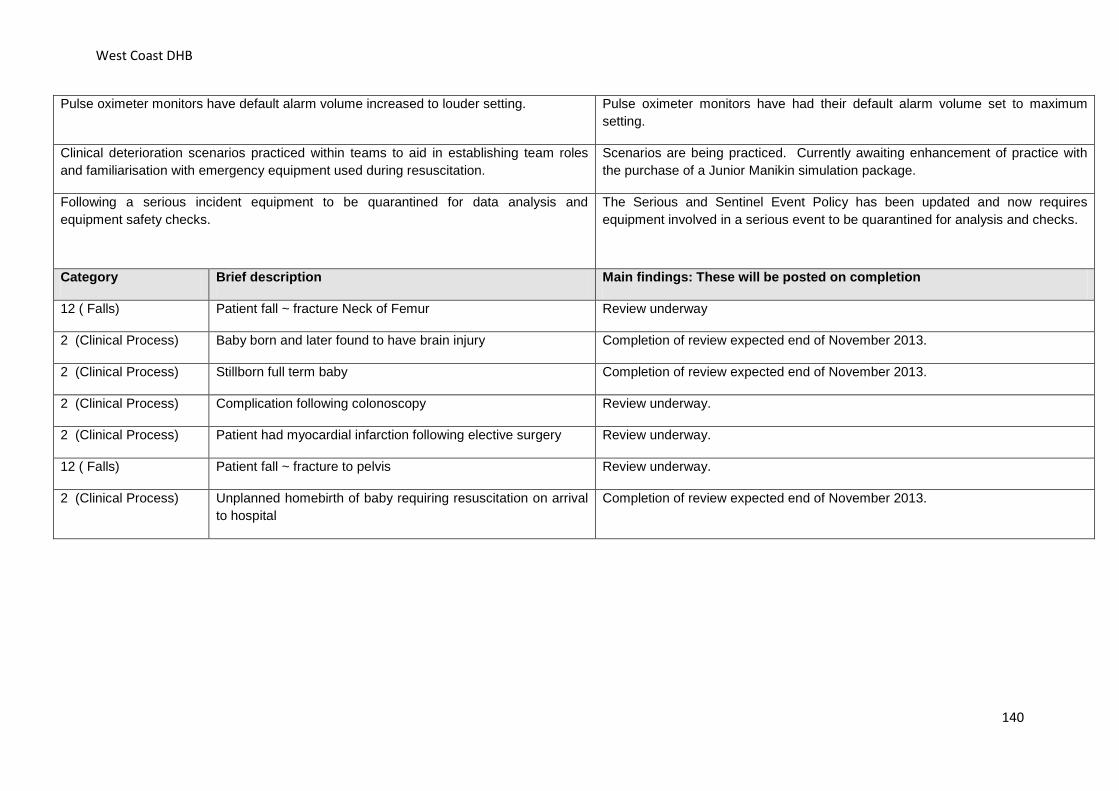
West Coast DHB
Pulse oximeter monitors have default alarm volume increased to louder setting. Pulse oximeter monitors have had their default alarm volume set to maximum setting.
Clinical deterioration scenarios practiced within teams to aid in establishing team roles and familiarisation with emergency equipment used during resuscitation.
Scenarios are being practiced. Currently awaiting enhancement of practice with the purchase of a Junior Manikin simulation package.
Following a serious incident equipment to be quarantined for data analysis and equipment safety checks.
The Serious and Sentinel Event Policy has been updated and now requires equipment involved in a serious event to be quarantined for analysis and checks.
Category Brief description Main findings: These will be posted on completion
12 ( Falls) Patient fall ~ fracture Neck of Femur Review underway
2 (Clinical Process) Baby born and later found to have brain injury Completion of review expected end of November 2013.
2 (Clinical Process) Stillborn full term baby Completion of review expected end of November 2013.
2 (Clinical Process) Complication following colonoscopy Review underway.
2 (Clinical Process) Patient had myocardial infarction following elective surgery Review underway.
12 ( Falls) Patient fall ~ fracture to pelvis Review underway.
2 (Clinical Process) Unplanned homebirth of baby requiring resuscitation on arrival to hospital
Completion of review expected end of November 2013.
140
Whanganui DHB
Whanganui District Health Board Serious adverse events 1 July 2012 – 30 June 2013
http://www.wdhb.org.nz/
The Whanganui District Health Board (WDHB) is committed to keeping patients safe and reducing harm caused by adverse events. When adverse events do occur, the WDHB strives to be open and honest with patients and their families by investigating, learning and making positive changes to prevent a similar event from occurring again.
There were three serious adverse events reported and investigated in the year ending 30 June 2013. Two events resulted from patients falling and fracturing their hips. The third was the unexpected death of a baby.
Serious adverse event one
An 85-year-old male was admitted to Wanganui Hospital after falling at home and fracturing his left hip. There were no complications as a result of the surgery performed to repair his hip and the patient was transferred to the Assessment Treatment and Rehabilitation Ward for rehabilitation.
Unfortunately, prior to going home, the patient fell again and fractured his left leg. Due to his existing medical conditions, no surgical intervention was undertaken.
Our investigation found a need for further education and improvement with managing patients at risk of falling.
Seven recommendations were made as a result of this investigation:
Nursing staff were provided with further education around the monitoring of confused patients
An injury prevention resource person has been appointed Falls risk assessment documentation has been amended The Physiotherapy Department now works with staff to implement individual patient
programmes An algorithm was developed for use with patients identified as a high falls risk Written guidelines were developed to guide staff when a doctor does not respond to their
pager Bell mat usage was reviewed.
Serious event two
When a 78-year-old female admitted to the Medical Ward was identified as a high falls risk, appropriate interventions were implemented. Regrettably, a health care assistant tasked with observing the patient in a four-bed room left the bedside to attend to another patient’s hygiene needs. The woman fell and fractured her right hip. Following surgery she was discharged back to the rest home.
141

Whanganui DHB
Our investigation found that health care assistants needed further education regarding how patients are to be specialled.
Serious event three
A baby born in Wellington with a congenital abdominal wall defect was operated on immediately after birth and made good progress following surgery.
At five weeks old, the baby was admitted to Wanganui Hospital for tests and found to be feeding well. Then sadly, before discharge, the baby became unwell and despite resuscitation attempts, died.
The post mortem found the baby had a bowel obstruction which had occurred very rapidly, giving no time to arrange a transfer to Wellington for emergency surgery.
The investigation into this little baby’s death found no issues with the care provided by the Wanganui Hospital paediatric team which was described by the tertiary paediatric surgeon as exemplary.
142