Embed Size (px)
Citation preview
GYNECOLOGIC ONCOLOGY 34, 383-388 (1989)
DNA Content as a Prognostic Index in Gestational Trophoblastic Neoplasia’
DAVID A. MARTIN, M.D.,* GREGORY P. SUTTON, M.D., THOMAS M. ULBRIGHT, M.D.,* GEORGE W. SLEDGE, JR., M.D.7 FREDERICK B. STEHMAN, M.D., AND CLARENCE E. EHRLICH, M.D.
Departments of Obstetrics and Gynecology, *Pathology, and ‘/‘Hematology/Oncology, Indiana University School of Medicine, Indianapolis, Indiana 46202
Received November 23, 1988
Hydatidifonn mole will progress to malignant gestational tro- phoblastic neoplasia (GTN) in some cases. Aneuploidy and high proliferative activity are associated with malignant tumors. Molar pregnancy tissue was considered a precursor to malignant GTN, and was studied retrospectively using paraffin-embedded tissue to determine whether aneuploidy or proliferative rates measured on molar tissue could predict a malignant course. Tissues from 51 complete hydatidiform moles were analyzed for nuclear DNA content by flow cytometric techniques. A chart review identified the clinical course after evacuation of the mole. A satisfactory DNA histogram was generated in 40 cases. of the 40 patients, 22 (55%) had spontaneous resolution, and 18 patients (45%) re- quired treatment for persistent GTN. The molar tissue was found to be euploid in 27 cases and aneuploid in 13 cases. Eight of the twenty-seven euploid cases (30%) required treatment after evac- uation, whereas 10 of the 13 aneuploid cases (77%) required treatment after molar evacuation. Proliferative index (PI) was compared with treatment requirements. Average PI was 0.11 2 0.10 for the treatment group and 0.08 f 0.06 for the spontaneous resolution group. The correlation of clinical course with ploidy was significant (P < 0.01). The association with proliferative index was not (P > 0.05). Aneuploidy, therefore, identifies a high-risk group of molar pregnancies, and may represent those that have undergone one stage of malignant transformation. 0 1989 Academic Press, Inc.
INTRODUCTION
Hydatidiform mole develops into persistent tropho- blastic disease for approximately 20% of patients [ 11. Pro- phylactic chemotherapy given after evacuation of hy- datidiform mole has been shown to decrease the inci-
’ Presented at the annual meeting of the Society of Gynecologic Oncologists, Maui, Hawaii, February 5-9, 1989.
* Present address: Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Campus Box 7570, MacNider Building, University of North Carolina, Chapel Hill, NC 27599-7570.
dence of persistent gestational trophoblastic neoplasia (GTN) as well as the incidence of metastatic persistent disease. The regimens vary as to patient tolerance. Pro- phylactic chemotherapy has been advocated as poten- tially less morbid and more successful than treatment required to control recurrent or advanced tumor. Never- theless, prophylactic chemotherapy is not given for most patient populations, for the reason that it subjects all patients to the cost and morbidity of treatment but will likely benefit only 15-20% of those receiving prophy- laxis. The identification of a high-risk group of hydati: diform moles would justify prophylactic chemotherapy if the majority of those treated stand to benefit.
Since the report of Curry et al. [ 11, we can identify the patients at increased risk for persistent GTN by their clinical characteristics at the time of mole evacuation. The characteristics with the greatest predictive value are the combination of uterine size large-for-dates and theta lutein cysts. In this clinical setting 57% of patients de- velop postmolar malignant GTN. These clinical corre- lates identifying a high-risk mole have not had sufficient predictive value to justify prophylactic chemotherapy [2- 41.
Compared with other malignancies, GTN has been studied less with regard to tumor aneuploidy and pro- liferative activity. There has been interest in tumor aneu- ploidy for solid tumors in general [5-71 and for prema- lignant lesions @-lo] as a predictor of biological behavior. Cytogenetic studies reveal that benign tumors and normal tissue are uniformly diploid or polyploid, whereas malignant tumors often contain aneuploid cell populations. This has been confirmed for many tumor types using flow cytometry. Aneuploidy is a better pre- dictor of disease-free interval and survival time than are traditional staging and grading criteria in some types of cancer I1 l-141.
383 0090-825W89 $1 SO
Copyright 0 1989 by Academic Press, Inc. All rights of reproduction in any form reserved.
384 MARTIN ET AL.
Flow cytometry is a rapid and accurate method of measuring cellular aneuploidy. In addition, information about the percentage of cells in various cell cycle com- partments may be obtained, allowing calculation of pro- liferative activity. Proliferative activity also correlates with malignant behavior and clinical prognosis for some malignancies [15,16]. This report presents data on aneu- ploidy and proliferative activity of complete hydatidiform moles, as measured by flow cytometric analysis of tumor obtained from formalin-fixed, paraffin-embedded archi- val blocks. Patient medical records were then reviewed retrospectively, allowing correlation with clinical course and therapy required. This study was undertaken to de- termine whether DNA measurements obtained using flow cytometry could be used to predict trophoblastic seque- lae from molar gestations.
MATERIALS AND METHODS
Patients with hydatidiform mole were identified by dis- charge diagnoses and by chart review at the Indiana University Medical Center. Many of the patients iden- tified were referred for treatment with a diagnosis of persistent or metastatic GTN. In these cases, the ante- cedent molar gestation had been evacuated at a referring hospital. All patients with GTN from 1974 to 1987 were noted for possible inclusion in the study. Study inclusion criteria were as follows: paraffin block availability; clin- ical diagnosis of hydatidiform mole; confirmation of the diagnosis of complete hydatidiform mole by histologic review at the time of the study; and availability of ad- equate clinical history to determine the postmolar course, including at least 6 months of consecutive neg- ative human chorionic gonadotropin (hCG) titers to de- fine a spontaneous resolution after evacuation of the mole. Patients were excluded who received either pro- phylactic chemotherapy or gravid hysterectomy; those who were identified as partial mole or hydropic abortus on histologic review were also excluded.
All tumor samples were reviewed pathologically by examination of hematoxylin and eosin-stained slides rep- resenting paraffin block sections originally adjacent to those sections sampled by flow cytometry. Partial moles were identified either by histologic review or by verifi- cation of fetus or membranes in the pathology report. Criteria for the pathologic distinction of partial and com- plete moles were those described by Szulman [171.
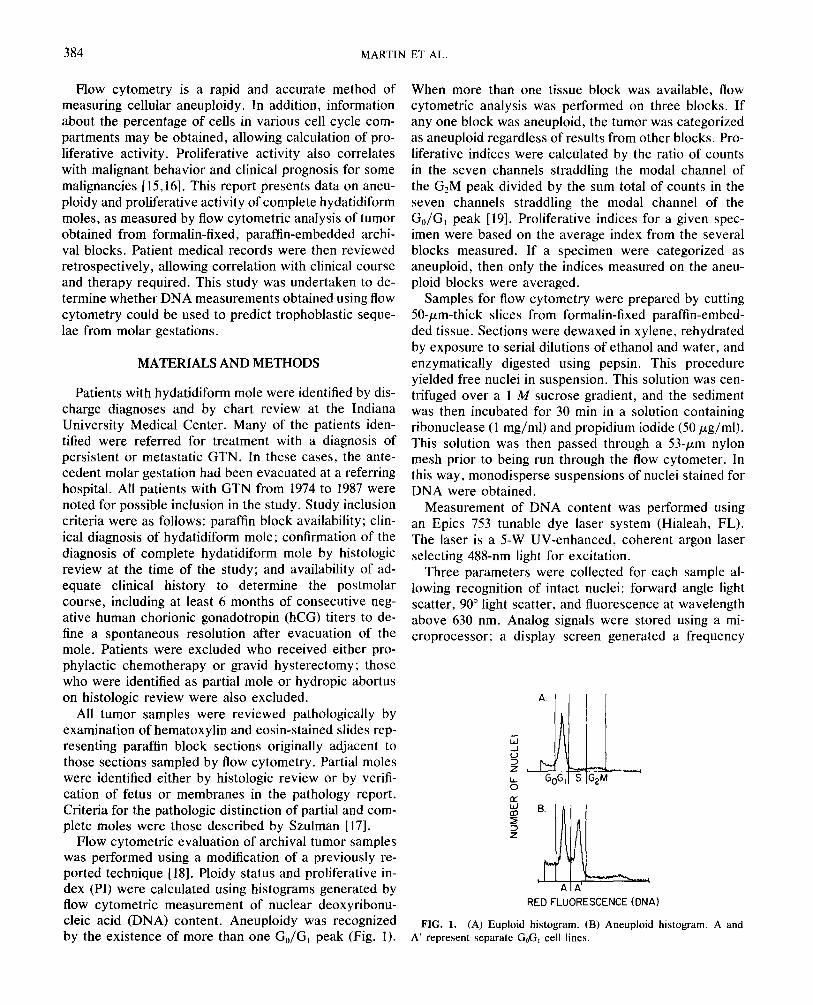
Flow cytometric evaluation of archival tumor samples was performed using a modification of a previously re- ported technique [18]. Ploidy status and proliferative in- dex (PI) were calculated using histograms generated by flow cytometric measurement of nuclear deoxyribonu- cleic acid (DNA) content. Aneuploidy was recognized by the existence of more than one Go/G1 peak (Fig. 1).
When more than one tissue block was available, flow cytometric analysis was performed on three blocks. If any one block was aneuploid, the tumor was categorized as aneuploid regardless of results from other blocks. Pro- liferative indices were calculated by the ratio of counts in the seven channels straddling the modal channel of the G2M peak divided by the sum total of counts in the seven channels straddling the modal channel of the Go/G, peak [19]. Proliferative indices for a given spec- imen were based on the average index from the several blocks measured. If a specimen were categorized as aneuploid, then only the indices measured on the aneu- ploid blocks were averaged.
Samples for flow cytometry were prepared by cutting 50-pm-thick slices from formalin-fixed paraffin-embed- ded tissue. Sections were dewaxed in xylene, rehydrated by exposure to serial dilutions of ethanol and water, and enzymatically digested using pepsin. This procedure yielded free nuclei in suspension. This solution was cen- trifuged over a 1 M sucrose gradient, and the sediment was then incubated for 30 min in a solution containing ribonuclease (1 mg/ml) and propidium iodide (50 pg/ml). This solution was then passed through a 53-pm nylon mesh prior to being run through the flow cytometer. In this way, monodisperse suspensions of nuclei stained for DNA were obtained.
Measurement of DNA content was performed using an Epics 753 tunable dye laser system (Hialeah, FL). The laser is a 5-W UV-enhanced, coherent argon laser selecting 488-nm light for excitation.
Three parameters were collected for each sample al- lowing recognition of intact nuclei: forward angle light scatter, 90” light scatter, and fluorescence at wavelength above 630 nm. Analog signals were stored using a mi- croprocessor; a display screen generated a frequency
A 1 A- CI
RED FLUORESCENCE (DNA)
FIG. 1. (A) Euploid histogram. (B) Aneuploid histogram. A and A’ represent separate G,G, cell lines.
DNA CONTENT IN GESTATIONAL TROPHOBLASTIC NEOPLASIA 385
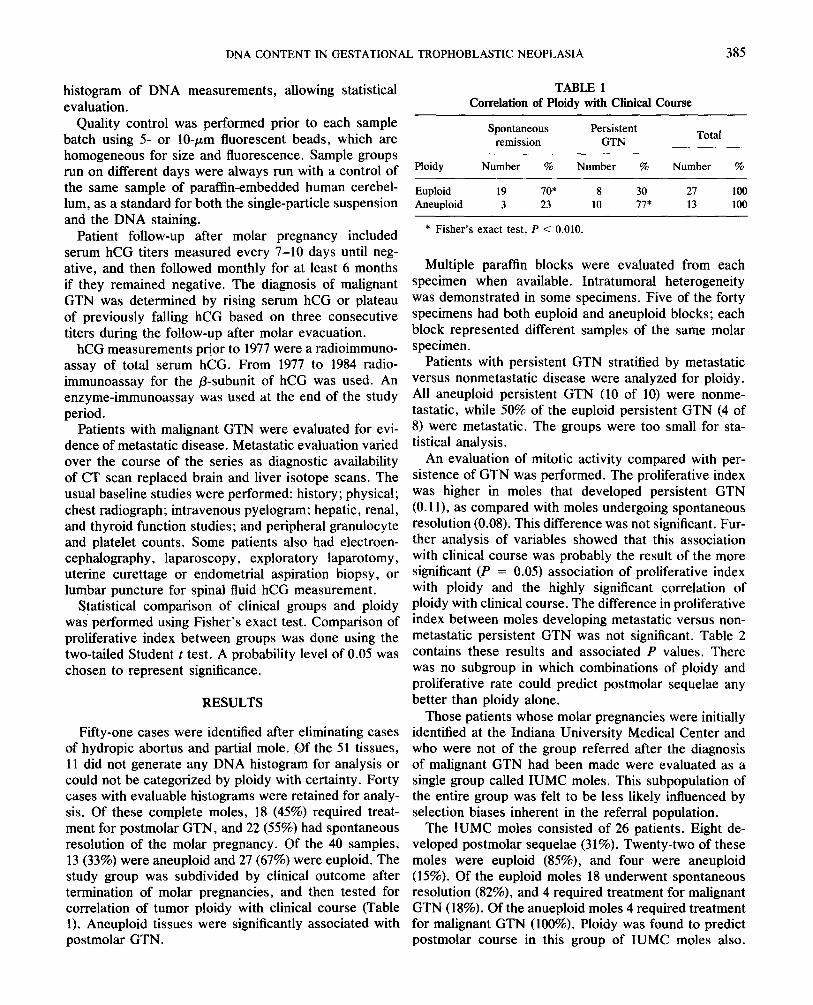
histogram of DNA measurements, allowing statistical TABLE 1
evaluation. Correlation of Ploidy with Clinical Course
Quality control was performed prior to each sample batch using 5- or lo-pm fluorescent beads, which are homogeneous for size and fluorescence. Sample groups run on different days were always run with a control of the same sample of paraffin-embedded human cerebel- lum, as a standard for both the single-particle suspension and the DNA staining.
Spontaneous remission
Persistent GTN Total
Patient follow-up after molar pregnancy included serum hCG titers measured every 7-10 days until neg- ative, and then followed monthly for at least 6 months if they remained negative. The diagnosis of malignant GTN was determined by rising serum hCG or plateau of previously falling hCG based on three consecutive titers during the follow-up after molar evacuation.
Ploidy Number % Number %
Euploid 19 lo* 8 30 Aneuploid 3 23 10 IF
* Fisher’s exact test, P < 0.010.
Number %
21 100 13 100
hCG measurements prior to 1977 were a radioimmuno- assay of total serum hCG. From 1977 to 1984 radio- immunoassay for the p-subunit of hCG was used. An enzyme-immunoassay was used at the end of the study period.
Multiple paraffin blocks were evaluated from each specimen when available. Intratumoral heterogeneity was demonstrated in some specimens. Five of the forty specimens had both euploid and aneuploid blocks; each block represented different samples of the same molar specimen.
Patients with malignant GTN were evaluated for evi- dence of metastatic disease. Metastatic evaluation varied over the course of the series as diagnostic availability of CT scan replaced brain and liver isotope scans. The usual baseline studies were performed: history; physical; chest radiograph; intravenous pyelogram; hepatic, renal, and thyroid function studies; and peripheral granulocyte and platelet counts. Some patients also had electroen- cephalography, laparoscopy, exploratory laparotomy, uterine curettage or endometrial aspiration biopsy, or lumbar puncture for spinal fluid hCG measurement.
Patients with persistent GTN stratified by metastatic versus nonmetastatic disease were analyzed for ploidy. All aneuploid persistent GTN (10 of 10) were nonme- tastatic, while 50% of the euploid persistent GTN (4 of 8) were metastatic. The groups were too small for sta- tistical analysis.
Statistical comparison of clinical groups and ploidy was performed using Fisher’s exact test. Comparison of proliferative index between groups was done using the two-tailed Student t test. A probability level of 0.05 was chosen to represent significance.
RESULTS
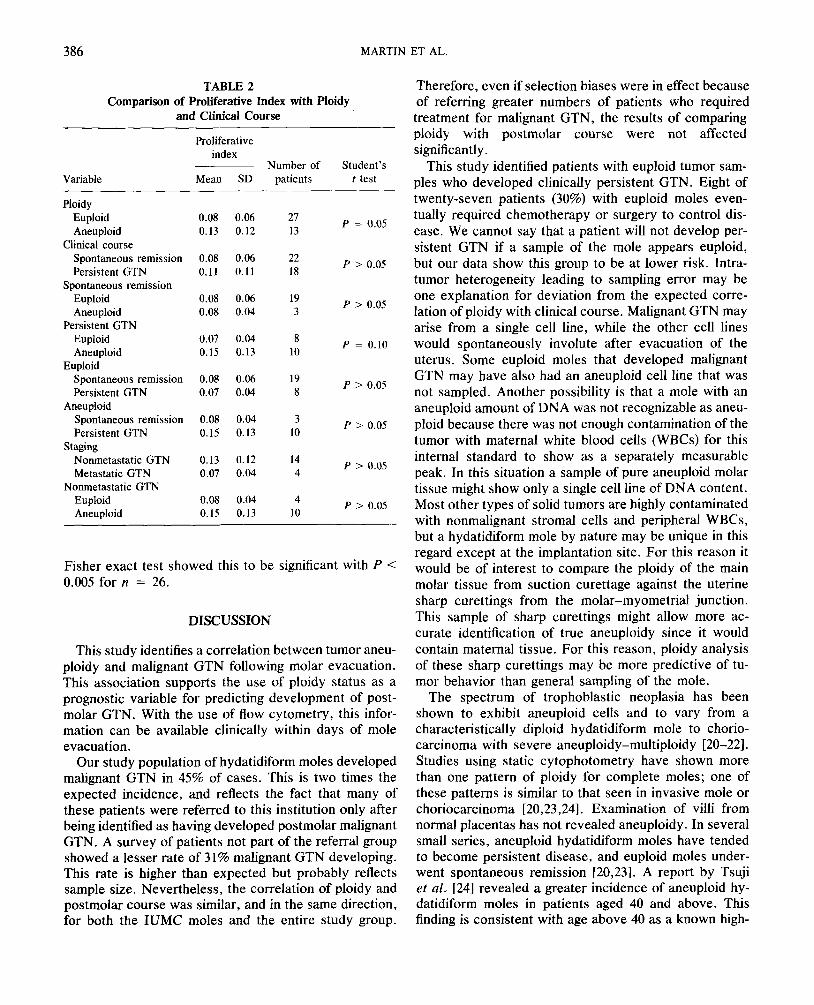
An evaluation of mitotic activity compared with per- sistence of GTN was performed. The proliferative index was higher in moles that developed persistent GTN (0.1 l), as compared with moles undergoing spontaneous resolution (0.08). This difference was not significant. Fur- ther analysis of variables showed that this association with clinical course was probably the result of the more significant (P = 0.05) association of proliferative index with ploidy and the highly significant correlation of ploidy with clinical course. The difference in proliferative index between moles developing metastatic versus non- metastatic persistent GTN was not significant. Table 2 contains these results and associated P values. There was no subgroup in which combinations of ploidy and proliferative rate could predict postmolar sequelae any better than ploidy alone.
Fifty-one cases were identified after eliminating cases of hydropic abortus and partial mole. Of the 51 tissues, 11 did not generate any DNA histogram for analysis or could not be categorized by ploidy with certainty. Forty cases with evaluable histograms were retained for analy- sis. Of these complete moles, 18 (45%) required treat- ment for postmolar GTN, and 22 (55%) had spontaneous resolution of the molar pregnancy. Of the 40 samples, 13 (33%) were aneuploid and 27 (67%) were euploid. The study group was subdivided by clinical outcome after termination of molar pregnancies, and then tested for correlation of tumor ploidy with clinical course (Table 1). Aneuploid tissues were significantly associated with postmolar GTN .
Those patients whose molar pregnancies were initially identified at the Indiana University Medical Center and who were not of the group referred after the diagnosis of malignant GTN had been made were evaluated as a single group called IUMC moles. This subpopulation of the entire group was felt to be less likely influenced by selection biases inherent in the referral population.
The IUMC moles consisted of 26 patients. Eight de- veloped postmolar sequelae (31%). Twenty-two of these moles were euploid (85%), and four were aneuploid (15%). Of the euploid moles 18 underwent spontaneous resolution (82%), and 4 required treatment for malignant GTN (18%). Of the anueploid moles 4 required treatment for malignant GTN (100%). Ploidy was found to predict postmolar course in this group of IUMC moles also.
386 MARTIN ET AL.
TABLE 2 Comparison of Proliferative Index with Ploidy
and Clinical Course
Variable
Proliferative index
Number of Student’s Mean SD patients t test
Ploidy Euploid Aneuploid
Clinical course Spontaneous remission Persistent GTN
Spontaneous remission Euploid Aneuploid
Persistent GTN Euploid Aneuploid
Euploid Spontaneous remission Persistent GTN
Aneuploid Spontaneous remission Persistent GTN
Staging Nonmetastatic GTN Metastatic GTN
Nonmetastatic GTN Euploid Aneuploid
0.08 0.06 0.13 0.12
0.08 0.06 0.11 0.11
0.08 0.06 0.08 0.04
0.07 0.04 0.15 0.13
0.08 0.06 0.07 0.04
0.08 0.04 0.15 0.13
0.13 0.12 0.07 0.04
0.08 0.04 0.15 0.13
27 13
22 18
19 3
8 10
19 8
3 10
14 4
4 10
P = 0.05
P > 0.05
P > 0.05
P = 0.10
P > 0.05
P > 0.05
P > 0.05
P > 0.05
Fisher exact test showed this to be significant with P < 0.005 for n = 26.
DISCUSSION
This study identifies a correlation between tumor aneu- ploidy and malignant GTN following molar evacuation. This association supports the use of ploidy status as a prognostic variable for predicting development of post- molar GTN. With the use of flow cytometry, this infor- mation can be available clinically within days of mole evacuation.
Our study population of hydatidiform moles developed malignant GTN in 45% of cases. This is two times the expected incidence, and reflects the fact that many of these patients were referred to this institution only after being identified as having developed postmolar malignant GTN. A survey of patients not part of the referral group showed a lesser rate of 31% malignant GTN developing. This rate is higher than expected but probably reflects sample size. Nevertheless, the correlation of ploidy and postmolar course was similar, and in the same direction, for both the IUMC moles and the entire study group.
Therefore, even if selection biases were in effect because of referring greater numbers of patients who required treatment for malignant GTN, the results of comparing ploidy with postmolar course were not affected significantly.
This study identified patients with euploid tumor sam- ples who developed clinically persistent GTN. Eight of twenty-seven patients (30%) with euploid moles even- tually required chemotherapy or surgery to control dis- ease. We cannot say that a patient will not develop per- sistent GTN if a sample of the mole appears euploid, but our data show this group to be at lower risk. Intra- tumor heterogeneity leading to sampling error may be one explanation for deviation from the expected corre- lation of ploidy with clinical course. Malignant GTN may arise from a single cell line, while the other cell lines would spontaneously involute after evacuation of the uterus. Some euploid moles that developed malignant GTN may have also had an aneuploid cell line that was not sampled. Another possibility is that a mole with an aneuploid amount of DNA was not recognizable as aneu- ploid because there was not enough contamination of the tumor with maternal white blood cells (WBCs) for this internal standard to show as a separately measurable peak. In this situation a sample of pure aneuploid molar tissue might show only a single cell line of DNA content. Most other types of solid tumors are highly contaminated with nonmalignant stromal cells and peripheral WBCs, but a hydatidiform mole by nature may be unique in this regard except at the implantation site. For this reason it would be of interest to compare the ploidy of the main molar tissue from suction curettage against the uterine sharp curettings from the molar-myometrial junction. This sample of sharp curettings might allow more ac- curate identification of true aneuploidy since it would contain maternal tissue. For this reason, ploidy analysis of these sharp curettings may be more predictive of tu- mor behavior than general sampling of the mole.
The spectrum of trophoblastic neoplasia has been shown to exhibit aneuploid cells and to vary from a characteristically diploid hydatidiform mole to chorio- carcinoma with severe aneuploidy-multiploidy [20-221. Studies using static cytophotometry have shown more than one pattern of ploidy for complete moles; one of these patterns is similar to that seen in invasive mole or choriocarcinoma [20,23,24]. Examination of villi from normal placentas has not revealed aneuploidy. In several small series, aneuploid hydatidiform moles have tended to become persistent disease, and euploid moles under- went spontaneous remission [20,23]. A report by Tsuji et al. [24] revealed a greater incidence of aneuploid hy- datidiform moles in patients aged 40 and above. This finding is consistent with age above 40 as a known high-
DNA CONTENT IN GESTATIONAL TROPHOBLASTIC NEOPLASIA 387
risk marker for postmolar sequelae. It is reasonable then to pursue these tumor-specific variables of ploidy and mitotic activity to evaluate their predictive abilities re- garding trophoblastic sequelae. This report confirms these prior reports and describes a flow cytometric tech- nique whereby the information can be obtained in sec- onds instead of hours.
Our intent was to provide a prognostic variable that could easily be measured in the laboratory, and that would predict need for future therapy of postmolar tro- phoblastic disease. To be of clinical value, a new variable should improve on previously described clinical char- acteristics that predict postmolar GTN. All previously described risk factors for postmolar GTN are only mod- erately predictive. The only safe approach for individual patients has been the serial measure of serum hCG as an early warning of trophoblastic viability. In this con- ventional way, most patients needing treatment for ma- lignant GTN will be identified by 6-8 weeks following termination of a molar pregnancy.
In review of treatment failures of GTN, extensive dis- ease at the time of initial treatment [25] and duration of disease prior to treatment [26,27] are associated with poor outcomes. If a test were available to predict ma- lignant sequelae of a hydatidiform mole at the time of its initial diagnosis, then early treatment might avoid the complications associated with advanced malignancy. In addition, the therapeutic ratio would be markedly im- proved when compared with prior efforts at prophylactic chemotherapy, because only those hydatidiform moles at high risk to progress to malignant GTN would be given early treatment. There would no longer be a need to treat all moles prophylactically to improve the outcome in the 20% predicted to develop malignant GTN. Our data show that aneuploidy may be the variable that pre- dicts postmolar sequelae with sufficient specificity to jus- tify early treatment.
Whether this form of early treatment after evacuation is as effective at decreasing postmolar sequelae as tra- ditional prophylactic chemotherapy must be determined in controlled studies. Traditional chemotherapy, when given prophylactically for hydatidiform mole, is admin- istered for several days before and after evacuation. The early treatment after ploidy determination would be given in entirety after evacuation. It is possible that sur- gical evacuation may decrease the effectiveness of chemo- therapy by interfering with blood supply to the tropho- blasts that remain.
It is hoped that future efforts with prospective studies will confirm this identification of a high-risk mole for which immediate therapy might be indicated. Such ther- apy could reduce tumor progression time by l-2 months in those patients who would otherwise have manifested
trophoblastic malignancy after that interval. If a high enough predictive value could be found in a test, then this treatment would cease to be prophylactic and would be considered early therapy.
I.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
REFERENCES
Curry, S. L., Hammond, C. B., Tyrey, L., et al. Hydatidiform mole diagnosis, management, and long-term followup of 347 pa- tients, Obstet. Gynecol. 45, l-8 (1975). Fasoli, M., Ratti, E., Franceschi, S., et al. Management of ges- tational trophoblastic disease: Results of a cooperative study, Ob- stet. Gynecol. 60, 205-209 (1982). Kim, D. S., Moon, N., Kim, K. T., et al. Effects of prophylactic chemotherapy for persistent trophoblastic disease in patients with complete hydatidiform mole, Obstet. Gynecol. 67, 690-694 (1986). Kashimura, Y., Kashimura, M., Sugimori, H., et al. Prophylactic chemotherapy for hydatidiform mole, Cancer 58, 624-629 (1986). Friedlander, M. L., Hedley, D. W., and Taylor, I. W. Clinical and biological significance of aneuploidy in human tumours, J. Clin. Z’athol. 37, 961-974 (1984). Barlogie, B., Drewinko, B., Schumann, J., et al. Cellular DNA content as a marker of neoplasia in man, Amer. J. Med. 69, 195- 203 (1980). Barlogie, B., Raber, M. N., Schumann, J., et al. Flow cytometry in clinical cancer research, Cancer Res. 43, 3982-3997 (1983). Wagner, D., Richart, R. M., and Temer, J. Y. Deoxyribonucleic acid content of presumed precursors of endometrial carcinoma, Cancer 20, 2067-2077 (1967). Wagner, D., Sprenger, E., and Blank, M. H. DNA content of dysplastic cells of the uterine cervix, Acta Ctyol. 16, 517-522 (1972). Dudzinski, M. R., Haskill, S. J., Fowler, W. C., et al. DNA con- tent in cervical neoplasia and its relations to prognosis, Obstet. Gynecol. 69, 373-377 (1987). Ewers, S.-B., Sangstrom, E., Baldetorp, B., et al. Flow-cytometric DNA analysis in primary breast carcinomas and clinicopathological correlations, Cytometry, 5, 408-419 (1984). Kokal, W., Sheibani, K., Terz, J., et al. Tumor DNA content in the prognosis of colorectal carcinoma, J. Amer. Med. Assoc. 255, 3123-3127 (1986). Iversen, 0. E. Flow cytometric deoxyribonucleic acid index: A prognostic factor in endometrial carcinoma, Amer. J. Obstet. Gy- necol. 155, 770-776 (1986). Friedlander, M. L., Hedley, D. W., Taylor, I. W., et al. Influence of cellular DNA content on survival in advanced ovarian cancer, Cancer Res. 44, 397-400 (1984).
15. Schmidt, D., Wiedemann, B., Keil, W., et al. Flow cytometric analysis of nephroblastomas and related neoplasms, Cancer 58, 2494-2500 (1986).
16. McGuire, W. L., and Dressier, L. G. Emerging impact of flow cytometry in predicting recurrence and survival in breast cancer patients, J. Natl. Cancer Inst. 75, 405-410 (1985).
17. Szulman, A. E. Trophoblastic disease: Complete and partial hy- datidiform moles, in Pathology ofthe placenta (E. V. D. K. Perrin, Ed.), Churchill Livingstone, New York, pp. 183-197 (1984).
18. Hedley, D. W., Friedlander, M. L., Taylor, J. W., et al. Methods for analysis of cellular DNA content of paraffin-embedded path-

388 MARTIN ET AL.
ological material using flow cytometry, J. Histochem. Cytochem. 31, 1333-1335 (1983).
19. Naus, G. J., et al. Predictive value of flow cytometric DNA content analysis of paraffin-embedded tissue in renal cell carcinoma, Lab. Invest. 52, 47a (1985).
20. Sugimori, H., Kashimura, Y., Kashimura, M., et al. Nuclear DNA content of trophoblastic tumors, Acta Cytol. 22, 542-545 (1978).
21. Goldfarb, S., Richart, R. M., and Okagaki, T. A cytophotometric study of nuclear DNA content of cyto- and syncytiotrophoblast in trophoblastic disease, Cancer 27, 83-92 (1971).
22. Kashimura, Y. A quantitative study of nuclear DNA of tropho- blastic cells: Proliferation kinetics, Gynecol. Oncol. 16, 374-382 (1983).
23. Nishiya, I., Moriya, S., Yamashita, K., et al. Cytophotometric
DNA determination of trophoblastic neoplasia, Gynecol. Oncol. 5, 103-108 (1977).
24. Tsuji, K., Yagi, S., and Nakano, R. Increased risk of malignant transformation of hydatidiform moles in older gravidas: A cyto- genetic study, Obstet. Gynecol. 58, 351-355 (1981).
25. Lurain, J. R., Brewer, J. I., Mazur, M. T., et al. Fatal gestational trophoblastic disease: An analysis of treatment failures, Amer. J. Obstet. Gynecol. 144, 391-395 (1982).
26. Ross, G. T., Goldstein, D. P., Hartz, R., et al. Sequential use of methotrexate and actinomycin D in the treatment of metastatic choriocarcinoma and related trophoblastic diseases in women, Amer. J. Obstet. Gynecol. 93, 223-229 (1965).
27. Bagshawe, K. D. Risk and prognostic factors in trophoblastic neo- plasia, Cancer 38, 1373-1385 (1976).