Embed Size (px)
Citation preview

J Clin Epidemiol Vol. 45, No. 6, pp. 621626, 1992 0895-4356/92 $5.00 + 0.00 Printed in Great Britain. All rights reserved Copyright 0 1992 Pergamon Press Ltd
DO PATIENTS’ CORONARY RISK FACTOR REPORTS PREDICT ACUTE CARDIAC ISCHEMIA IN THE
EMERGENCY DEPARTMENT? A MULTICENTER STUDY
ROBERT L. JAYES JR,“’ JONI R. BESHANSKY,’ RALPH B. D’AGOSTINO’ and HARRY P. SELKER’*
‘Center for Cardiovascular Health Services Research, Divisions of Clinical Decision Making and General Medicine, Department of Medicine, New England Medical Center and Tufts University School of Medicine, Boston, MA 02111 and *Division of General Internal Medicine, George
Washington University Medical Center, Washington, DC, U.S.A.
(Received in revised form 8 January 1992)
Abstract-The objective of the present study was to determine whether the presence of the classical coronary risk factors increases the likelihood of acute cardiac ischemia beyond that expected from clinical presentation and electrocardiogram. Clinical data and reports of classical coronary risk factors were collected prospectively from 1743 patients without clinically obvious coronary disease. Patients were selected from 5773 emergency department patients at 6 hospitals who presented with symptoms suggesting acute ischemia. We used logistic regression to determine the relative risk of each risk factor report for acute ischemia. In women, the presence of classical risk factor reports does not increase the risk of acute ischemia. In men, only diabetes and family history of myocardial infarction significantly increase the risk (p < 0.05). The relative risks are 2.4 and 2.1, respectively, and are small compared to those conferred by chest pain (12. l), an abnormal ST segment (8.7), or an abnormal T wave (5.3). For a patient presenting to the emergency department, the classical coronary risk factors convey minimal risk for acute cardiac ischemia, especially when compared to the overwhelming importance of the chief complaint and the ECG.
Acute cardiac ischemia myocardial infarction
Coronary risk factors Emergency department Acute
INTRODUCTION risk factors [7]. Physicians customarily assess
The Framingham Study [l] and other longitudi- these factors when providing preventive care,
nal studies [2M] have identified risk factors for because they predict the incidence of future
the development of coronary heart disease. Age, coronary disease.
male gender, hypercholesterolemia, diabetes, Physicians also commonly ask emergency
smoking, hypertension, and family history of department patients with chest pain about these
myocardial infarction are the major coronary risk factors. Among these patients, physicians must identify those with acute cardiac ischemia
*All correspondence should be addressed to: Harry P. (i.e. acute myocardial infarction, new-onset
Selker, M.D., M.S.P.H., Center for Cardiovascular angina, or unstable angina) for hospitalization. Health Services Research, Divisions of Clinical Decision Although physicians depend heavily on symp- Making and General Medicine, Department of Medi- tine, New England Medical Center, 750 Washington
toms and electrocardiograms (ECGs) for triage
Street, Box 1031, Boston, MA 021 II, U.S.A. [Tel: (617) of such emergency department patients, they 956-5049; Fax: (617) 350-80231. also commonly assess coronary risk factors to
CE 45,&E 621
622 ROBERT L. JAYFS JR et al.
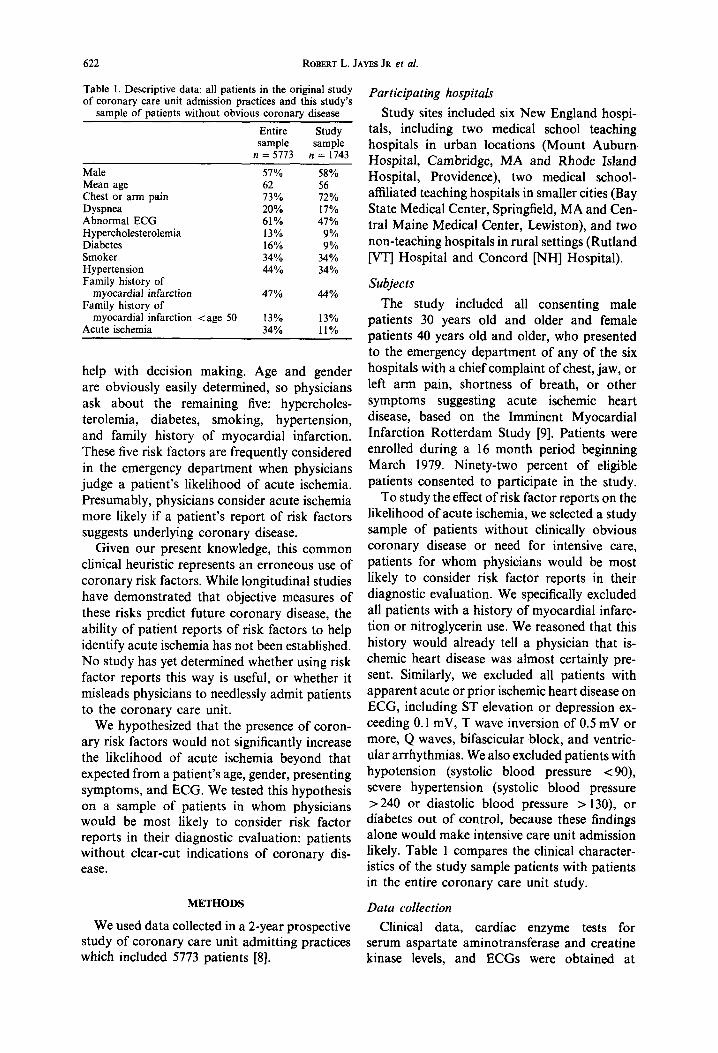
Table 1. Descriptive data: all patients in the original study of coronary care unit admission practices and this study’s
Participating hospitals sample of patients without obvious coronary disease
Entire Study sample sample
n = 5773 n = 1743
Male 51% 58% Mean age 62 56 Chest or arm pain 13% 12% Dyspnea 20% 11% Abnormal ECG 61% 41% Hypercholesterolemia 13% 9% Diabetes 16% 9% Smoker 34% 34% Hypertension 44% 34% Family history of
Study sites included six New England hospi- tals, including two medical school teaching hospitals in urban locations (Mount Auburn. Hospital, Cambridge, MA and Rhode Island Hospital, Providence), two medical school- affiliated teaching hospitals in smaller cities (Bay State Medical Center, Springfield, MA and Cen- tral Maine Medical Center, Lewiston), and two non-teaching hospitals in rural settings (Rutland /VT] Hospital and Concord [NH] Hospital).
myocardial infarction Family history of
47% 44% Subjects
myocardial infarction <age 50 Acute ischemia
13% 13% 34% 11%
help with decision making. Age and gender are obviously easily determined, so physicians ask about the remaining five: hypercholes- terolemia, diabetes, smoking, hypertension, and family history of myocardial infarction. These five risk factors are frequently considered in the emergency department when physicians judge a patient’s likelihood of acute ischemia. Presumably, physicians consider acute ischemia more likely if a patient’s report of risk factors suggests underlying coronary disease.
The study included all consenting male patients 30 years old and older and female patients 40 years old and older, who presented to the emergency department of any of the six hospitals with a chief complaint of chest, jaw, or left arm pain, shortness of breath, or other symptoms suggesting acute ischemic heart disease, based on the Imminent Myocardial Infarction Rotterdam Study [9]. Patients were enrolled during a 16 month period beginning March 1979. Ninety-two percent of eligible patients consented to participate in the study.
Given our present knowledge, this common clinical heuristic represents an erroneous use of coronary risk factors. While longitudinal studies have demonstrated that objective measures of these risks predict future coronary disease, the ability of patient reports of risk factors to help identify acute ischemia has not been established. No study has yet determined whether using risk factor reports this way is useful, or whether it misleads physicians to needlessly admit patients to the coronary care unit.
We hypothesized that the presence of coron- ary risk factors would not significantly increase the likelihood of acute ischemia beyond that expected from a patient’s age, gender, presenting symptoms, and ECG. We tested this hypothesis on a sample of patients in whom physicians would be most likely to consider risk factor reports in their diagnostic evaluation: patients without clear-cut indications of coronary dis- ease.
To study the effect of risk factor reports on the likelihood of acute ischemia, we selected a study sample of patients without clinically obvious coronary disease or need for intensive care, patients for whom physicians would be most likely to consider risk factor reports in their diagnostic evaluation. We specifically excluded all patients with a history of myocardial infarc- tion or nitroglycerin use. We reasoned that this history would already tell a physician that is- chemic heart disease was almost certainly pre- sent. Similarly, we excluded all patients with apparent acute or prior ischemic heart disease on ECG, including ST elevation or depression ex- ceeding 0.1 mV, T wave inversion of 0.5 mV or more, Q waves, bifascicular block, and ventric- ular arrhythmias. We also excluded patients with hypotension (systolic blood pressure < 90), severe hypertension (systolic blood pressure > 240 or diastolic blood pressure > 130), or diabetes out of control, because these findings alone would make intensive care unit admission likely. Table 1 compares the clinical character- istics of the study sample patients with patients in the entire coronary care unit study.
METHODS Data collection We used data collected in a 2-year prospective Clinical data, cardiac enzyme tests for
study of coronary care unit admitting practices serum aspartate aminotransferase and creatine which included 5773 patients [8]. kinase levels, and ECGs were obtained at

Risk Factors in the Emergency Department 623
Table 2. Risk factor questions asked of each emergency department patient by a research assistant
Risk factor
Hypercholesterolemia
Diabetes mellitus
Cigarette smoking
Hypertension
Family history
Question
Prior to your emergency department visit, has a doctor ever told you that you have cholesterol or high level of fat in your blood? Has a doctor ever told you that you have high blood sugar or sugar in your urine or diabetes? Have you ever smoked cigarettes? Are you still smoking cigarettes? How long has it been since you stopped smoking? Has a doctor ever told you that you had high blood pressure? Has anyone in your family ever had a heart attack (father, mother, sister or brother)? Did this member of your family have a heart attack before they were 50 years of age?
the time of entry for all consenting patients. Additional clinical data, including clinical records, follow-up ECGs, and cardiac-enzyme tests, were obtained for both hospitalized and non-hospitalized patients at 48 hours after ad- mission. The follow-up rate was 89% for all study subjects.
During the initial emergency department visit, a research assistant also asked each patient about the five risk factors. using questions simi- lar to the ones used by physicians (Table 2). Response rates were over 98% for each question.
Data analysis
Diagnoses were determined for each patient. We defined acute ischemic heart disease to include acute myocardial infarction, new-onset angina pectoris, and unstable angina pectoris, representing the patients that most physicians would consider as candidates for coronary care unit admission. Final “true diagnoses” (acute myocardial infarction, angina pectoris, or not acute ischemic heart disease) were based on clinical presentation, ECGs, and cardiac enzyme tests, using the World Health Organization [lo] and New York Heart Association [l l] criteria.
We used patients’ reports of coronary risk factors obtained by the research assistant to define six risk factor responses for each patient. A history of hypercholesterolemia, diabetes, or hypertension were marked as yes or no re- sponses. Smoking within the last month was the criterion which established a positive smoking history. There were two questions for family history of myocardial infarction: patients were first asked about any family history, and then about a family history before age 50. We con- sidered the effect of these two responses indepen- dently. The response rates to each risk factor question exceeded 98 %.
Statistical methods
All hypothesis tests were two-tailed. Weighted means over all hospitals for descriptive data include adjustments for each center’s sample size contribution.
To examine whether positive coronary risk factor reports increased the likelihood of acute ischemia given age, gender, chest pain, and the ECG, we used a logistic regression model to obtain estimates of the relative risks, similar to the one used to identify risk factors for the development of coronary disease in the Framingham study [12]. Logistic regression yields the odds ratio, which approxi- mates the relative risk when the dependent variable is of relatively low probability, as in the present case [13]. The dependent variable was acute ischemia. The independent variables included: the ECG variables ST segment elevation or flattening and T wave peaking or inversion, the symptom variable chest or left arm pressure or pain, and reports of coronary risk factors (Table 2). To control for the effect of gender, we performed separate analyses for men and women. We adjusted for age by including age as a continuous variable in each analysis.
Missing reports for risk factor history did not exceed 2% for any factor, and negative responses were assigned to such variables. The results were not changed by deleting cases with missing values or substituting positive responses for missing values.
RESULTS
The study sample included 1743 patients without clinically obvious coronary disease from the 5773 coronary care unit study patients.
624 ROBERT L. JAYES JR et al.
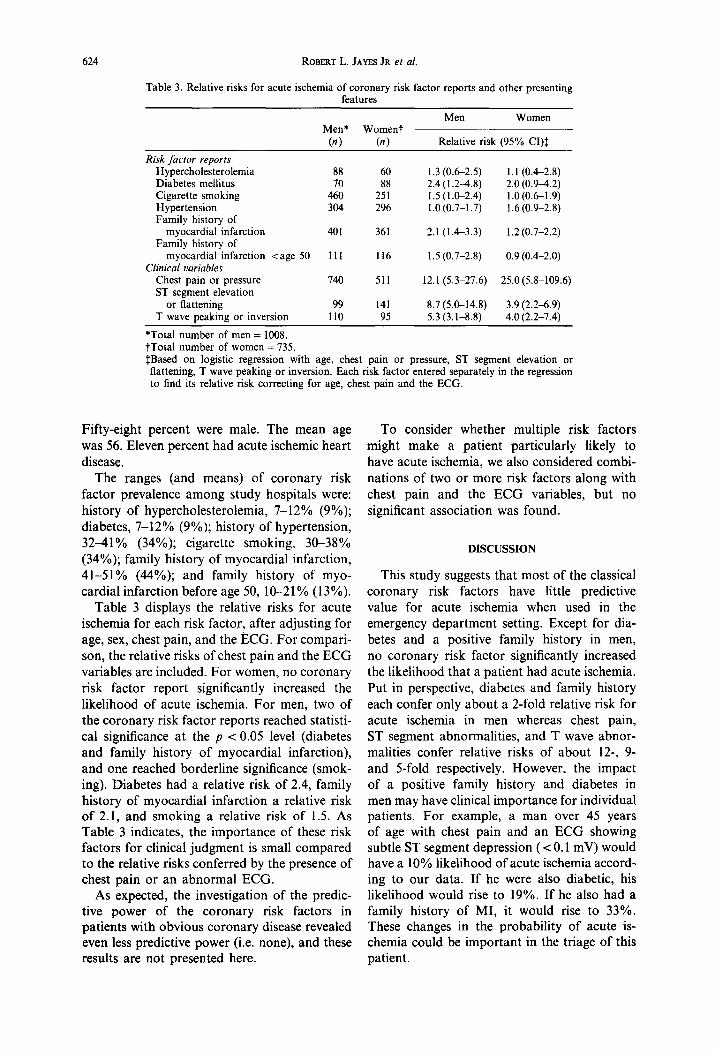
Table 3. Relative risks for acute ischemia of coronary risk factor reports and other presenting features
Men Women Men* Woment
(n) (n) Relative risk (95% CI)$
Risk factor reports Hypercholesterolemia 88 60 1.3 (0.62.5) 1.1 (042.8) Diabetes mellitus 70 88 2.4 (1.2-4.8) 2.0 (0.94.2) Cigarette smoking 460 251 1.5 (l&2.4) l.O(O.61.9) Hypertension 304 296 1.0(0.7-1.7) 1.6 (0.992.8) Family history of
myocardial infarction 401 361 2.1 (143.3) 1.2 (0.7-2.2) Family history of
myocardial infarction <age 50 111 116 1.5 (0.7-2.8) 0.9 (0.42.0) Clinical variables
Chest pain or pressure 740 511 12.1 (5.3-27.6) 25.0 (5.8-109.6) ST segment elevation
or flattening 99 141 8.7 (5.0-14.8) 3.9 (2.269) T wave peaking or inversion 110 95 5.3 (3.1-8.8) 4.0 (2.2-7.4)
*Total number of men = 1008. tTota1 number of women = 735. IBased on logistic regression with age, chest pain or pressure, ST segment elevation or flattening, T wave peaking or inversion. Each risk factor entered separately in the regression to find its relative risk correcting for age, chest pain and the ECG.
Fifty-eight percent were male. The mean age was 56. Eleven percent had acute ischemic heart disease.
The ranges (and means) of coronary risk factor prevalence among study hospitals were: history of hypercholesterolemia, 7-12% (9%); diabetes, 7-12% (9%); history of hypertension, 3241% (34%); cigarette smoking, 3&38% (34%); family history of myocardial infarction, 41-51% (44%); and family history of myo- cardial infarction before age 50, lO--21% (13%).
Table 3 displays the relative risks for acute ischemia for each risk factor, after adjusting for age, sex, chest pain, and the ECG. For compari- son, the relative risks of chest pain and the ECG variables are included. For women, no coronary risk factor report significantly increased the likelihood of acute ischemia. For men, two of the coronary risk factor reports reached statisti- cal significance at the p < 0.05 level (diabetes and family history of myocardial infarction), and one reached borderline significance (smok- ing). Diabetes had a relative risk of 2.4, family history of myocardial infarction a relative risk of 2.1, and smoking a relative risk of 1.5. As Table 3 indicates, the importance of these risk factors for clinical judgment is small compared to the relative risks conferred by the presence of chest pain or an abnormal ECG.
As expected, the investigation of the predic- tive power of the coronary risk factors in patients with obvious coronary disease revealed even less predictive power (i.e. none), and these results are not presented here.
To consider whether multiple risk factors might make a patient particularly likely to have acute ischemia, we also considered combi- nations of two or more risk factors along with chest pain and the ECG variables, but no significant association was found.
DISCUSSION
This study suggests that most of the classical coronary risk factors have little predictive value for acute ischemia when used in the emergency department setting. Except for dia- betes and a positive family history in men, no coronary risk factor significantly increased the likelihood that a patient had acute ischemia. Put in perspective, diabetes and family history each confer only about a 2-fold relative risk for acute ischemia in men whereas chest pain, ST segment abnormalities, and T wave abnor- malities confer relative risks of about 12-, 9- and 5-fold respectively. However, the impact of a positive family history and diabetes in men may have clinical importance for individual patients. For example, a man over 45 years of age with chest pain and an ECG showing subtle ST segment depression ( < 0.1 mV) would have a 10% likelihood of acute ischemia accord- ing to our data. If he were also diabetic, his likelihood would rise to 19%. If he also had a family history of MI, it would rise to 33%. These changes in the probability of acute is- chemia could be important in the triage of this patient.

Risk Factors in the Emergency Department 625
Many studies show that the classical coronary risk factors can predict ischemic heart disease over decades of follow-up. However, physicians in the emergency department need information that will indicate the likelihood of acute disease at that time. Coronary risk factors were not established to provide this information. For example, the Framingham Study showed that hypertension increases the risk of ischemic heart disease 2-fold over 4 years [12], but only a very small portion of this risk applies to the few hours of the emergency department patient’s acute illness. In attempting to use risk factors to identify acute disease, physicians are mis- interpreting the definition of “risk factor” as it was determined from longitudinal studies. Furthermore, coronary risk factor history is subject to all the biases and inaccuracies of a patient’s memory. This history is presumably less reliable than the methods used to assign risk in longitudinal studies.
A potential limitation of our analysis is that physicians may use somewhat different risk factor reports from those we studied, such as reported cholesterol levels or severity of diabetes. Since these data were collected, public awareness of the hazards of hypercholes- terolemia has increased, and patients are now more likely to know their serum cholesterol levels. However, this is unlikely to change our results. Patients who reported elevated levels at the time of this study were likely to have unusually high cholesterol levels, associated with a high long-term risk for coronary disease. Yet this did not increase their likelihood of acute ischemia after accounting for the import- ant clinical variables. Physicians may assess smoking behavior in different ways. We also tested for number of packs smoked per day and “pack-years”, but these did not predict acute ischemia beyond the information provided by the clinical variables. Finally, the history ob- tained by a research assistant might differ from that obtained by a physician. To minimize this possibility, we used standard questions derived from the commonly cited longitudinal studies. It seems unlikely that somewhat different methods of identifying risk factors would produce a significantly different result.
Another potential limitation is our selection of study subjects. We collected data on all patients with symptoms consistent with acute ischemia, but studied only those without clini- cally obvious coronary disease. We chose this group as the one in whom physicians are most
likely to rely on risk factors to diagnose acute ischemia. We guessed that more clear-cut indi- cations of acute ischemia would take precedence over coronary risk factors when triage decisions are made.
We have shown that eliciting patients’ coron- ary risks factors in the emergency department does not improve a physician’s ability to diag- nose acute ischemia. Most positive reports do not increase the likelihood of ischemia beyond what one would expect from the patient’s pre- senting symptoms and ECG. While determining coronary risk factors is part of a complete medical history, physicians in the emergency department should not depend on this history to help judge the risk of acute ischemia.
Because these results run counter to the prevailing clinical wisdom, it is possible that physicians who give risk factor history great weight may inappropriately triage emergency department patients. Whether this potential misuse of the risk factor heuristic has adverse impact on clinical practice remains to be deter- mined.
Acknowledgements-This work was supported by a grant from the Agency for Health Care Policy and Research (formerly National Center for Health Services Research and Technology Assessment) grants ROl HS02068 and ROl HS0554901, and from the National Library of Medicine Medical Information Program training grant LM7044 and Research grant LM4493.
1.
2.
3.
4.
5.
6.
REFERENCES
Gordon T, Sorlie P, Kannel WB. Coronary Heart Disease, Atherothrombotic Brain Infarction, Intermit- tent Claudication-A Multivariate Analysis of Some Factors Related to Their Incidence: Framingham Study, 16 Year Follow-up. Section 27, U.S. Govt. Print. Office; 1971. Snowden CB, McNamara PM, Garrison RJ, Feinleib M, Kannel WB, Epstein FH. Predicting coronary disease in siblings-a multivariate assessment. The Framingham Study. Am J Epidemiol 1982; 115: 217-222. Rosenman RH, Brand RJ, Jenkins D, Freidman M, Straus R, Wurm M. Coronary Heart Disease in the Western Collaborative Group Study. JAMA 1975; 233: 822-827. Brand RJ, Rosenman RH, Sholtz RI, Friedman M. Multivariate prediction of coronary heart disease in the Western Collaborative Group Study compared to the findings of the Framingham Study. Circulation 1976; 53: 348-355. Butler WJ, Ostrander LD, Carmen WJ, Lamphiear DE. Mortality from coronary heart disease in the Tecumseh Study. Long-term effect of diabetes mellitus, glucose tolerance and other risk factors. Am J Epidemiol 1985; 121: 541-547. Yano K, Reed DM, McGee DL. Ten year incidence of coronary heart disease in the Honolulu Heart Program. Relationship to biologic and lifestyle charac- teristics. Am J Epidemiol 1984; 119: 653461.
626 ROBERT L. JAYES JR et al.
7. American Heart Association. Coronary Risk Hand- book: Estimating the Risk of Coronary Heart Disease in Daily Practice. New York: American Heart Associ- ation; 1976.
8. Pozen MW, D’Agostino RB, Selker HP, Sytkowski PA, Hood WB. A predictive instrument to improve coronary-care-unit admission practices in acute is- chemic heart disease: A prospective multicenter clinical trial. N Engl J Med 1984; 310: 1273-1278.
9. Van der Does E, Lubson J, Pool J, Hugenholtz PG, Arntzenius AC. Acute coronary events in general practice: Objectives and design of the Imminent Myo- cardial Infarction Rotterdam Study. Heart Bull 1976; 7: 91-98.
10. Gillum RF, Fortmann SP, Prineas RI, Kottke TE. International diagnostic criteria for acute myocardial infarction and stroke. Am Heart J 1984; 108: 150-158.
11. Criteria Committee of the New York Heart Associ- ation. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, edn 8. New York: New York Heart Association; 1979: 288-290.
12. Truett J, Cornfield J, Kannel W. A multivariate analy- sis of the risk of coronary heart disease in Framing- ham. J Cbron Dis 1967; 20: 511-524.
13. Lemeshow S, Hosmer DW. Estimating odds ratios with categorically scaled covariates in multiple logistic regression analysis. Am J Epidemiol 1984; 119: 147-151.















![The value of exercise SPET for the detection of coronary ...ble prognosis compared to vein grafts [1-2]. Myocardial ischemia after coronary artery bypass grafting (CABG) surgery can](https://img.pdfslide.net/doc/110x75/5ea506f39b89a50fe80fabd8/the-value-of-exercise-spet-for-the-detection-of-coronary-ble-prognosis-compared.jpg)













