-
8/18/2019 don't kick me out
1/14
http://ccs.sagepub.com/ Clinical Case Studies
http://ccs.sagepub.com/content/9/1/28The online version of
this article can be found at:
DOI: 10.1177/1534650109349293 2010 9: 28 originally
published online 14 October 2009Clinical Case Studies
Raymond V. Burke, Brett R. Kuhn, Jane L. Peterson, Roger W.
Peterson and Amy S. Badura BrackBehavior Problems
''Don't Kick Me Out!'': Day Treatment for Two Preschool Children
With Severe
Published by:
http://www.sagepublications.com
can be found at:Clinical Case Studies Additional
services and information for
http://ccs.sagepub.com/cgi/alertsEmail Alerts:
http://ccs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://ccs.sagepub.com/content/9/1/28.refs.htmlCitations:
What is This?
- Oct 14, 2009Proof
- Jan 14, 2010Version of Record>>
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/content/9/1/28http://ccs.sagepub.com/content/9/1/28http://ccs.sagepub.com/content/9/1/28http://www.sagepublications.com/http://www.sagepublications.com/http://ccs.sagepub.com/cgi/alertshttp://ccs.sagepub.com/cgi/alertshttp://ccs.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsPermissions.navhttp://ccs.sagepub.com/content/9/1/28.refs.htmlhttp://ccs.sagepub.com/content/9/1/28.refs.htmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://ccs.sagepub.com/content/early/2009/10/14/1534650109349293.full.pdfhttp://ccs.sagepub.com/content/9/1/28.full.pdfhttp://ccs.sagepub.com/content/9/1/28.full.pdfhttp://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://ccs.sagepub.com/content/early/2009/10/14/1534650109349293.full.pdfhttp://ccs.sagepub.com/content/9/1/28.full.pdfhttp://ccs.sagepub.com/content/9/1/28.refs.htmlhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://ccs.sagepub.com/subscriptionshttp://ccs.sagepub.com/cgi/alertshttp://www.sagepublications.com/http://ccs.sagepub.com/content/9/1/28http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
2/14
Clinical Case Studies9(1) 28 –40
© The Author(s) 2010
Reprints and permission:
http://www.sagepub.com/journalsPermissions.nav
DOI: 10.1177/1534650109349293http://ccs.sagepub.com
“Don’t Kick Me Out!”: DayTreatment for Two PreschoolChildren
With Severe Behavior
Problems
Raymond V. Burke,1,2 Brett R. Kuhn,3 Jane L.
Peterson,1
Roger W. Peterson,1 and Amy S. Badura Brack 4
Abstract
Parents of young children with severe emotional and behavior
problems have few services from
which to choose if their child is expelled from preschool for
aggressive and disruptive behavior.Two case studies provide an
overview of a multicomponent, intensive, day-treatment programfor
children with moderate to severe behavior disorders. Proximal and
distal program goals are
to eliminate presenting problem behaviors and increase social
competencies and to reintegratechildren back to their school,
preschool, or daycare, respectively. The cases presented in
thisstudy provide preliminary evidence that day treatment can be a
viable option for young children
with disruptive behavior disorders.
Keywordsbehavior disorders, day treatment, young children,
behavior therapy
1 Theoretical and Research Basis
Recent estimates suggest that 10% to 20% of preschool children
exhibit severe behavior prob-
lems that place them at risk for social and academic difficulty
throughout their school years
(National Scientific Council on the Developing Child, 2008;
Powell, Fixsen, & Dunlap, 2003).
These rates are consistent with previous reports that between
16% and 22% of children and ado-
lescents have mental disorders and emotional and behavioral
problems (Costello et al., 1996;
Roberts, Attkisson, & Rosenblatt, 1998). Early onset
behavior problems have resulted in anincreasing number of young
children being “kicked out” of preschools. Nationally, the
preschool
expulsion rate is more than three times the rate found among
K-12 students (Gilliam, 2005) with
some individual states reporting preschool expulsion rates that
are more than 13 times K-12 rates
(Gilliam & Shahar, 2006).
Without intervention, children’s behavior problems remain fairly
stable over time or escalate
and increase the likelihood that as older students, they will
require alternative educational place-
ment, special education services, or drop out of school
altogether (Koertering & Braziel, 1999;
1Behave’n, Omaha, NE2University of Nebraska, Lincoln
3University of Nebraska Medical Center, Omaha, NE4Creighton
University, Omaha, NE
Corresponding Author:
Raymond V. Burke, 8922 Cuming Street, Omaha, NE 68114
Email: [email protected]
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
3/14
Burke et al. 29
Olsen & Hoza, 1993; Raver & Knitzer, 2002; Snyder,
2001). Children who receive special edu-
cation services, that is, identified as learning disabled or
seriously emotionally disturbed, are
overrepresented among those expelled from school (Morrison &
D’Incau, 1997).
To reduce expulsions and dropouts, prevention and intervention
efforts must effectively
address children’s social behavior and academic deficits.
Despite a number of well-documentedstudies of primary prevention
school-based programs (see Berryhill & Prinz, 2003; Brock,
Laza-
rus, & Jimerson, 2002), there are few published studies and
no randomized controlled trials with
day treatment programs for young children with disruptive
behavior disorders (Tse, 2006). How-
ever, a meta-analysis of published primary prevention programs
for young children found that
behavioral and cognitive behavioral interventions were
twice as effective as nonbehavioral inter-
ventions (Durlak & Wells, 1997).
Behavioral treatment program. Well-researched theories
provide the basis for the program
described in this article. Traditional behavioral theories
including operant conditioning (Skinner,
1953) and social learning theory (Bandura, 1969) are employed
through the use of reinforcement
and a discipline hierarchy. The program focuses on building
social competencies through a
combination of verbal reinforcement (Maag, 2001), modeling
(Bandura & McDonald, 1963), problem solving and social
skill instruction (Gresham, Sugai, & Horner, 2001), and a
contin-
gency based point system (Axelrod, 1971; Christophersen, Arnold,
Hill, & Quilitch, 1972; Wolf,
Giles, & Hall, 1968).
Positive reinforcement includes the use of tokens paired with
verbal praise and social rein-
forcement (e.g., signs of affection such as a hug or high-five).
Verbal praise is provided contingent
on children’s demonstration of prosocial behaviors and when they
practice social skills related to
individualized treatment plan (ITP) goals. Initially, staff
members use a fixed continuous rein-
forcement schedule for children’s newly developing skills and
behavior. After skill competency
is demonstrated, reinforcement is faded using an intermittent
schedule to enhance resistance to
extinction. Staff provides children with tokens throughout the
day. The frequency with whichthis exchange occurs varies by child
and is based on ITP goals, developmental level, and sched-
ule of reinforcement. Once a child earns the predetermined
number of tokens, they can be
exchanged for activities (e.g., play with toys, a piggy back
ride, special time with staff) and
prizes (e.g., stickers, Kazdin, 1977). Throughout the day,
children also may exchange tokens to
purchase special trinkets (e.g., stickers, pencils, small
toys, tops, hats).
Another theoretical foundation is social interactional theory
(Patterson, Reid, & Dishion,
1992), emphasizing the influence of adult and peer interactions
on children’s socialization and
establishing the basis for changing adults’ social interactions
to influence children’s social
behavior. Social skill instruction for all children is a
critical program component and begins with
skills of accepting negative and positive consequences and
continues with teaching of adaptivereplacement skills. Additional
skill instruction is based on skill deficits specified by the
parent in
each child’s ITP. For example, a child with problems spitting
and screaming when frustrated may
be taught how to calm herself, ask adults for help, or
walk away from the problem. A child who
is aggressive and frequently hits children and staff may be
taught how to ask other children for
toys, how to wait patiently (e.g., for toys or staff attention),
and how to find toys with which no
one else is playing.
Negative consequences target problem behaviors and are
integrated into the contingent use of
a four-level disciplinary response hierarchy (Larzelere &
Kuhn, 2005) beginning with (a) a
verbal request to stop the inappropriate behavior, (b) use of a
brief time-out (approximately 10
seconds where the child sits on floor and counts to 10), (c) use
of a time-out chair at a distance
of 2′ to 5′ from the desired activity for
approximately 10 seconds, and (d) use of a backup time-
out room with an open door for a maximum of 30 seconds (Peterson
& Peterson, 2006). Time-out
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
4/14
30 Clinical Case Studies 9(1)
procedures involve restricting access to positive
reinforcement to reduce the likelihood that the
target behavior will be strengthened (Wolery, Bailey, &
Sugai, 1988).
The purpose of this case study is to provide an overview of a
multicomponent, intensive
day treatment program (Behave’n Day Center; BDC) for two
children with moderate to
severe behavior disorders. We present two children’s cases and
describe components of the program including staff training,
treatment strategies, participant characteristics, parent
involvement, and outcome assessment. We chose a case study
design because this report rep-
resents an initial evaluation of a previously untested
intervention (Drotar, La Greca, Lemanek,
& Kazak, 1995).
2 Case Presentation
Liam (all names are pseudonyms). Liam is a 4-year-old Caucasian
male who lived with his bio-
logical mother, an 8-year-old brother, a 6-year-old brother, and
15-month-old step-sister. Liam’s
biological father lives in another state; his involvement
in Liam’s life is limited to sending a box
of clothes at unpredictable times once each year. Liam’s mother
had a boyfriend who is father ofLiam’s step-sister. The boyfriend
lived with the family until 2 months prior to Liam’s enrollment
in the day treatment program. The boyfriend was abusive to
Liam’s mother on several occasions
before she decided to move the family back to her parents’
home.
Keisha. Keisha is a 4-year-old African American female who
resided with her parents, new-
born sister, and grandmother. At admission, her father was
unemployed and her mother was on
maternity leave. They had been living with the grandmother for
approximately one year because
of financial strain.
3 Presenting complaintsLiam. Liam was described by his mother as
aggressive, having language and developmental
delays, and unwilling to share with others. Liam’s mother
reported that Liam’s 15-month-old
sister had language and compliance skills that surpassed Liam’s
abilities. During the admission
interview Liam’s mother indicated that he kicked, hit, and bit
his siblings on a daily basis and
aggressively spit food and drink “all day.” Liam’s mother
unsuccessfully attempted to teach
Liam how to use sign language and the Picture Exchange
Communication System (Bondy &
Frost, 2004) to communicate. Liam was not toilet trained prior
to BDC enrollment.
Keisha. At admission, Keisha’s mother reported that Keisha
consistently demonstrated
“aggressive and hyperactive behavior” such as hitting, biting,
spitting, throwing objects, and
pinching her mother and peers in day care. The aggressive
episodes occurred two to three timesdaily at day care and 6 to 10
times per evening at home. In addition, Keisha had one to three
tantrums per evening during which she threw herself face first
on the floor or onto toys, and
kicked, screamed, and banged her head on the floor.
4 History
Liam. Prior to enrollment in BDC, Liam attended a local public
school’s preschool for children
with developmental disabilities. His mother withdrew Liam from
the preschool program after 6
months, citing a lack of improvement in behavior and vocabulary.
Liam’s limited communica-
tion strategies included nonverbal (primarily waving and
pointing) and verbal (one-word
utterances) attempts to get his needs met by those in his
environment. When faced with unwanted
requests or correction, Liam intensely resisted complying by
shouting and shaking his head “no,”
crossing his arms, stamping his feet, hitting, kicking, and
biting those in his vicinity.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
5/14
Burke et al. 31
Keisha. Keisha had been expelled from five daycares for
aggressive behavior toward class-
mates and staff prior to coming to the day treatment program. At
home, Keisha’s mother reported
that Keisha yelled at her, refused to sit still, and hit other
children in the neighborhood. During a
recent tantrum at home, Keisha broke the kitchen table by
jumping from the kitchen counter onto
the table. Shortly after that tantrum, Keisha’s mother saw a
television news report about the BDC program, contacted BDC,
and enrolled Keisha in the program.
5 Assessment
Measurement of Progress
Data from parent-completed measures and staff observations of
target behaviors are used to
evaluate interventions and monitor children’s progress on ITPs.
BDC staff and parents also par-
ticipate in monthly reviews of children’s ITP goals, progress at
home and at BDC, and the need
for additional target areas when specific ITP goals are met.
Parent-completed measures. Parents complete the Child
Behavior Checklist (CBCL; Achen- bach, 1991a) prior to
admission and at departure from BDC. The CBCL, the most widely
used
measure of children and adolescents’ behavior problems, is
available for children 1.5 to 5 years
(Achenbach & Rescorla, 2000). Two broadband scales related
to internalizing and externalizing
behavior problems are included in an overall Total Problem
score. T -scores of 60 to 63 for Inter-
nalizing, Externalizing, and Total Problem scales place a child
in the borderline clinical range
while T -scores greater than 63 place the child in the
clinical range (Achenbach, 1991a). The
CBCL has strong psychometric properties that have been
well-established during more than 20
years of use in published studies (Achenbach, 1991b).
Staff observations. Children attending BDC work to improve
one or two target behaviors at a
time. Baseline data are collected during the first day at BDC.
Target behaviors and goals areoperationally defined, for example,
when given an instruction, Edward will say “Okay” and
perform the task within 5 seconds 80% of the time. A
primary staff person is assigned to each
child at enrollment. Once each week, each child’s primary staff
records the estimated percentage
of time that the target behavior occurred based on the overall
number of opportunities for occur-
rence of the target behavior during that week. The clinical
therapist and supervisor meet weekly
to review the child’s progress.
Individualized treatment plan reviews. A review of
children’s behavior and related goals occurs
during monthly 1-hour ITP meetings with a BDC therapist, a BDC
supervisor, and a child’s
parent(s) or legal guardian. Participants discuss whether
goals are met at home and at BDC, are
in need of revision, or require more time for treatment effects
to occur.
6 Case Conceptualization
The individualized treatment plan. Within the first week
after BDC enrollment, the BDC thera-
pist and parents meet to develop an ITP for each child.
During the ITP meeting, the parent
identifies approximately five target areas for the child.
Current behavior patterns related to each
target area are discussed, interventions for each target area
are proposed, goal behaviors are
specified, and individuals responsible for implementing each
intervention are identified. Center-
based interventions are implemented with one or two target
behaviors at a time. Once the ITP is
established, BDC staff work with the parent(s) to develop
competency with home-based inter-
vention strategies.
Liam. Liam’s speech and language patterns were consistent with
those of a 16-month-old.
Liam’s admission mental status exam indicated a diagnosis of
Mild Mental Retardation and
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
6/14
32 Clinical Case Studies 9(1)
Mixed Receptive-Expressive Language Disorder and an Axis I
diagnosis of Oppositional Defi-
ant Disorder. His T -scores on the CBCL placed him in the
borderline clinical range for the Total
and Internalizing broadband scales, as well as on the Withdrawn
and Attention Problem sub-
scales. His CBCL T -score of 70 placed him in the clinical
range on the Pervasive Developmental
Problems subscale (Table 1).
On the preadmission questionnaire, Liam’s mother identified his
strengths as “fine motor
skills” and “likes to draw.” Liam’s weakness was “speech” and
her target behavioral issues were
“compliance, spiting [sic].” During the initial ITP meeting, the
BDC team, including Liam’smother, identified compliance with adult
instructions and successfully completing time-outs as
primary target areas for Liam. Four additional target
areas were identified at that meeting: “not
asking to go into the kitchen,” “temper tantrums,” “spitting
food and drink,” and “taking things
from his sister.” While the focus was on encouraging prosocial
behaviors, staff used the time-out
continuum to address misbehaviors related to the additional
target areas.
Reinforcement of positive replacement behaviors included use of
verbal praise, tokens, stars,
and high-fives for socially appropriate behaviors. Redirection
included the use of brief time-outs
and full time-outs in an identified chair at BDC and in an
identified time-out room at home. In
addition, BDC staff used positive practice to give Liam multiple
opportunities to complete brief
and full time-outs. During practice, staff used sign language
paired with verbal instructions toindicate that they were going to
practice how to complete time-outs. Then, staff verbally
reminded
Liam to sit quietly on the floor with his legs crossed and his
hands in his lap for 3 seconds. Verbal
praise and stars were provided when Liam completed the
practice to criteria. Additional practice
followed unsuccessful attempts.
Keisha. Keisha came to treatment with a diagnosis of Attention
Deficit Hyperactivity Disor-
der (ADHD) for which she was prescribed Adderall. CBCL broadband
scores for Internalizing,
Externalizing, and Total Problems were all in the clinical range
at admission despite medication.
Aggressive Behavior, Attention Problems, Emotionally Reactive,
and Anxious/Depressed syn-
drome scales on the CBCL also were in the clinical range at
admission (Table 1).
Keisha’s services included 4 months of day treatment, 1 hour of
family therapy per week, and
15 hours of parent education per month. Keisha’s mother and BDC
staff initially identified three
ITP target areas of (a) listening (e.g., compliance with adult
instructions), (b) attending the day
treatment center without complaining on the way, and (c) playing
without hitting other children.
Table 1. Significant Changes in Child Behavior Checklist
T -Scores
Liam Keisha
Pre Post Pre Post
Internalizing 63a 37 66b 45Emotionally reactive 67a 51
Anxious/depressed 69a 51
Withdrawn 67a 51
Externalizing 59 40 82b 52Attention problems 67a 50 73b
57Aggressive behavior 84b 51
Total 60a 41 77b 47Pervasive developmental problems 70b 51
a. Borderline clinical range.
b. Clinical range.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
7/14
Burke et al. 33
As Keisha made improvements in her initial target areas, her
mother added two additional ITP
target areas (“following directions in public places” and
“staying in bed all night”).The mother was encouraged to use the
time-out hierarchy for misbehavior related to the target
areas (i.e., a verbal request to stop the behavior, a brief
10-second time-out, a brief 10-second
time-out in a chair, and time-out in a chair up to a maximum of
30 seconds). BDC staff encour-
aged the mother to use brief, one- to four-word corrective
responses (up to one word per year of
life; Peterson & Peterson, 2006) when Keisha misbehaved to
avoid lecturing and inadvertent
reinforcement of inappropriate behavior.
Day treatment center staff primarily focused on teaching Keisha
to follow instructions. Base-
line data indicated that Keisha said “Okay” following an
instruction on 10% of the occasions
while compliance with the instruction occurred 50% of the time.
The treatment goal was for
Keisha to say “Okay” and follow the instruction 80% of the time.
Contingent verbal praise, highfives, and stars that could be
exchanged for desired activities and tangible rewards were used
to
reinforce Keisha when she complied with instructions. Stars were
provided for each behavior
rehearsal that Keisha completed, with up to 15 opportunities to
practice each day. When instruc-
tions were not followed, staff used the continuum of time-out
responses followed by the
opportunity to respond appropriately to the original
instruction.
7 Course of Treatment and Assessment of Progress
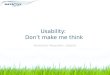
Liam. During the 3 months that Liam was enrolled at BDC, he
improved substantially in his two
primary target areas. During the first 4 weeks
post-baseline, Liam completed time-outs and fol-lowed adult
instructions, on average, 74% and 59% of the time, respectively.
The average
percentage of completed time-outs and instructions
increased to 100% and 74% during the final
4 weeks of his stay at BDC (Figure 1).
At program graduation, Liam’s Internalizing and Total Problem
T -scores were in the normal
range as was his T -score for the Pervasive Developmental
Problems (Table 1). His vocabulary
score had increased 34 points. At the conclusion of Liam’s
treatment, his mother reported that he
was toilet trained, had only infrequent temper tantrums that
were developmentally appropriate,
was eating and drinking without spitting, and played for
extended periods without aggressive
behavior toward his siblings. Liam’s mother reported that
he had increased his vocabulary and
his spontaneous use of sign language at home.
Keisha. Keisha’s mother indicated that Keisha met her goals for
the target areas of not attend-
ing without complaining and playing without hitting peers by the
end of the first month in the
BDC program. Compliance with instructions remained a target area
while a target area of
0
25
50
75
100
Baseline 1 2 3 4 5 6 7 8 9 10 11 12 13
Week
P e
r c e n t
Completes T. O.
Follows instructions
Figure 1. Liam: Weekly progress with two target areas
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
8/14
34 Clinical Case Studies 9(1)
“following directions in public places” was added during the
1-month ITP meeting. After 2
months of attending the day treatment center, Keisha had met the
“following directions in public places” goal; compliance with
instructions remained a target area; and the goal of staying in
bed
all night was added. While noting improvements with compliance
during the third month of
treatment, this target area remained on the list during Keisha’s
ITP review. Her mother indicated
that Keisha met the goal of “staying in bed all night” during
that third month. No additional target
area was identified. By the end of the fourth month of
treatment, Keisha’s mother indicated that
Keisha had reached all home ITP goals.
Keisha steadily improved on her primary treatment goal of
following instructions. By the end
of the second month of treatment, Keisha was verbally responding
with “Okay” and completion
of the instruction on 80% of the occasions at BDC. She
maintained or exceeded that level
throughout the remaining 5 weeks for all but 1 week, when
compliance dipped to 70% (Figure2). During the second month at BDC,
Keisha’s parents, with approval of the physician, decided
to discontinue the Adderall. She continued her BDC placement
medication-free until program
graduation.
Keisha’s post-CBCL T -scores on subscales and syndrome
scales were in the normal range
(Table 1). At the start of the school year, Keisha was enrolled
in a general education kindergarten
class at a neighborhood school.
8 Complicating Factors
In many communities, parents of young children with severe
emotional and behavior problemshave few services from which to
choose once their child is expelled from preschool for aggres-
sive and disruptive behavior (Powell et al., 2003). It is
estimated that only one-third to one-half
of children identified with emotional and behavior disorders
receive services (Kazdin, 1990;
U.S. Public Health Service, 2000) and those who do, receive low
rates of service or only part of
their recommended level of service (Powell et al., 2003). Lack
of services can result in a loss of
parent employment and increased financial stress, social
and emotional isolation for parents and
children, and an increased risk for child physical abuse and
neglect (Taylor-Richardson,
Heflinger, & Brown, 2006). Interventions are needed that
help behaviorally challenged children
improve their social and academic skills in preparation for a
successful transition to elementary
school (Eckert, McGoey, & DuPaul, 1996).
During the 2-years surrounding Liam and Keisha’s treatment,
Behave’n’s central city pro-
gram served 174 children, ages 2 to 7 years, 73% of whom had a
mental health diagnosis.
Thirty-four percent of referred children had prenatal exposure
to alcohol, tobacco, or drugs; 76%
0
20
40
60
80
100
Baseline 1 2 3 4 5 6 7 8 9 10 11 12 13
Week
P e
r c e n t
Comply 2 secSay "Okay"
Figure 2. Keisha: Weekly progress with two target areas
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
9/14
Burke et al. 35
of parents reported a family history of substance abuse.
Thirty-five percent of children had a his-
tory of one or more types of maltreatment. Prior to BDC
referral, more than half of the children
had participated in treatment with a psychiatrist (25%) or
therapist (26%), 12% had multiple
home placements, and 9% had been prescribed psychotropic
medication.
Despite complicating factors for Liam (i.e., unsuccessful
history of interventions for com-munication and other developmental
delays) and Keisha (i.e., inconsistency in living and school
arrangements, financial stress within the family, consistent
history of previously uncontrolled
aggressive behaviors), their cases strongly suggest that day
treatment is beneficial for young
children with disruptive behavior disorders.
9 Managed Care Considerations
Funding for BDC is provided by federal, state, local, and
private sources. Seventy-seven percent
of referred children are funded from Medicaid (45%) or some
combination of Medicaid and
Child Welfare (30%) or Medicaid and public school (2%) sources.
The remaining children are
funded from sole sources such as a private payee (16%), Child
Welfare (6%), and schools (1%).Although treatment is costly,
especially for private payees, there are several factors that
con-
tribute to the assessment of program costs and benefits
including reduced costs for the treatment
of children in the educational or juvenile justice systems,
reduced costs for social and mental
health services for the child and family, and increased parent
earnings due, for example, to
improved workplace attendance (Small, Reynolds, O’Connor, &
Cooney, 2005). Assessment of
long term benefits for the BDC program is difficult because we
lack multiple years of follow-up
data on BDC participants. However, the large percentage of
children whose parents reported reli-
able, meaningful improvements after placement and the follow-up
reports from parents in the
two case studies suggest that immediate and long-term benefits
may be expected. For the pur-
poses of this brief cost-benefits analysis, we compared
program costs with locally availablealternative placements for
children who have been expelled from preschool, school, and
child
care programs.
The BDC day treatment and family therapy programs cost US$112.00
per child per day. The
majority of parents considering BDC enrollment has exhausted
typical community resources for child
care and preschool. If their children were not enrolled in BDC,
they would likely be placed with a
one-to-one para-educator in a preschool or elementary school
classroom (an estimated US$143.00
per day) or enrolled in one of the local alternative
schools (US$130.00 to US$230.00 per day).
The average length of treatment at BDC is slightly less than 57
days for an average cost of
US$6,384.00. The school-based alternatives to BDC involve
services for the entire school year
with costs that range from US$23,400.00 (US$130.00 per day×
180 school days) to US$41,400.00(US$230.00 per day
× 180 school days). The BDC program represents a potential
annual savings
of US$17,016.00 to US$35,016 per child per school year or a
return on every US$1.00 invested
of US$3.67 to US$6.48 per child (Small et al., 2005). While we
do not have long-term results for
program graduates, if the current results are maintained
over time, then the savings and return on
investment have the potential of increasing for each year that
the child continues in school with-
out the need for additional services. This return on investment
is conservative and does not
include a host of other possible benefits such as reductions in
the need for social and mental
health services, juvenile justice services, and other remedial
educational services.
10 Follow-UpLiam. Two years post departure, Liam was attending
second grade in a general education public
school and, according to his mother, continued to make
impressive gains in his ability to speak.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
10/14
36 Clinical Case Studies 9(1)
He reportedly was using full sentences, asking questions, and
playing well with his peers and
siblings.
Keisha. After 4.5 months at BDC, Keisha graduated and returned
to a community day care
near her home. At one-year post-graduation, Keisha remained
medication-free. Keisha’s mother
described her as “a typical child” and indicated that she was
doing well in public school. Sheattended a general education
classroom with no student support services in the classroom.
11 Treatment Implications of the Case
Students are expelled from school due to repeated or serious
verbally or physically aggressive
behavior (Gilliam, 2005). These behavior problems are
evident early in children’s lives. Without
effective intervention, these children are likely to experience
academic deficits throughout their
school years (Reid, Gonzalez, Nordness, Trout, & Epstein,
2004) and are at risk for developing
antisocial patterns that persist into adulthood (Patterson et
al., 1992). However, in most commu-
nities, there is limited access to and availability of these
services (Powell et al., 2003). The BDC
program holds promise for addressing this shortage of
community-based services.The Behave’n Day Center is an
independently owned, for-profit, multicomponent day treat-
ment program designed to reduce childhood behavior problems and
improve mental health and
academic success. The Behave’n Day Center is accredited by the
Commission on Accreditation
of Rehabilitative Facilities—Day Treatment: Family Services
(Children and Adolescents) and is
a state-licensed child care program for children, ages 2 to 13
years; however, services are pro-
vided for children ages 2 to 7 years. The BDC service components
include family therapy and a
day treatment center with emphasis on three key program
components: (a) behaviorally focused
interventions, (b) staff training and data driven implementation
of the intervention, and (c) direct
training of parents in the intervention with the opportunity to
practice learned skills in the child
care setting. Proximal and distal program goals are to eliminate
presenting problem behaviorsand increase social competencies, and
to reintegrate children back to their school, preschool,
or
daycare, respectively.
Liam’s and Keisha’s cases, representative of typical
improvements seen at BDC, suggest that
these goals are being met. An examination of program-wide
results on the (CBCL; Achenbach,
1991a, 1991b) support results from the two case studies.
Pre-post CBCL scores were available
for 105 of the 174 (60%) children enrolled in the BDC program
during the 2 year period sur-
rounding Liam and Keisha’s time in treatment. BDC population
mean scores at admission
indicated that enrolled children had T -scores in the
borderline clinical range for Internalizing,
and in the clinical range for Externalizing and Total Problem
scales (Table 2). Mean T -scores at
departure from the BDC program were in the normal range
( p<
. 01; Table 2). We used the Reli-able Change Index (RCI;
Jacobson & Truax, 1991) as an indicator of clinically
significant change
within the population. A change of 8 T -score points on the
CBCL was used to indicate a meaning-
ful, reliable change on the CBCL (Thompson, Ruma, Brewster,
Besetsney, & Burke, 1997) from
BDC program enrollment to departure. Approximately two-thirds of
children had reliable change
on CBCL Internalizing (62%), Externalizing (70%), and Total
Problem (69%) scales during their
stay at BDC (Table 2). This compares favorably with other
studies that have used the RCI to
assess improvements. For example, 19% to 31% of parents who
completed a parent training
program reported reliable improvements in child behavior
and parents’ potential for child physi-
cal abuse (Thompson et al., 1997). Consistent with the majority
of children completing BDC,
Liam and Keisha demonstrated reliable change on all CBCL
broadband and subscale scores
(Table 1).
A limitation of the current BDC assessments is that no BDC
assessors of intervention out-
come (e.g., staff and parents) are blind to the intervention.
Findings would be stronger if some
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
11/14
Burke et al. 37
outcome measures were completed by an informant not aware of
treatment status, or greater
attention were paid to the reliability and training of staff
observers of the child’s behavior while
at BDC, school, or home. In addition, results should be
interpreted with caution given limited
long-term follow-up data.
12 Recommendations to Clinicians and Students
The current article summarizes two case studies and provides an
initial description of a multi-
component, intensive day treatment program (Behave’n Day Center)
for children with moderate
to severe behavior disorders. The pieces of the BDC puzzle are
comprised primarily of widely
disseminated, validated intervention components (Powell, Dunlap,
& Fox, 2006). However, the
entire puzzle paints a unique picture of a novel day treatment
center that serves “at risk” children
and families by infusing behaviorally focused interventions,
staff training and a data-driven
approach to implementing those interventions, and parent
training in the use of interventions sothat the child can be
reintegrated back into the home, school, or community daycare.
Preliminary
outcome data suggest that the treatment center has been
successful and highly sought after by
parents and referring professionals in the community.
While follow-up reports from parents indicated that both Liam
and Keisha were successfully
enrolled in public elementary school or a neighborhood child
care center, more rigorous evalua-
tion of those outcomes is necessary to assess the durability of
BDC effects with all children
enrolled at BDC. A recent review of early intervention programs
for preschool children with
ADHD found few published studies with this population (McGoey,
Eckert, & DuPaul, 2002),
most of which were conducted in clinical settings and lacked
assessment of generalizability in
preschool or day treatment programs. Our experiences
support Tse’s (2006) recommendations to(a) increase utilization of
evidence-based interventions in day treatment programs, (b)
prevent
elementary school problems by improving access to services for
young children with disruptive
behavior disorders, (c) emphasize social skills training
to provide socialization opportunities that
many children are missing with their current experiences, and
(d) engage parents and caretakers
when children enroll in day treatment programs so that treatment
is optimized and benefits main-
tain at home and school over time.
The challenge for day treatment programs and similar services is
to demonstrate program
fidelity and effectiveness within a service-oriented
organization. Key aspects of the program
include behaviorally focused interventions offered through
well-trained staff, data-driven imple-
mentation of interventions, and the direct training of parents
in the interventions with an
opportunity to practice in the child care setting. A
well-articulated program and close attention to
staff development and intervention implementation with parents
and children appears to contrib-
ute to positive outcomes for children.
Table 2. Pre-post CBCL Subscale T -Scores and Percent
Making Reliable Changea
Enrollment Departure Percent w/ Reliable Change
Internalizing 59.64b 50.40* 62%Externalizing 70.94c 57.40*
70%
Total problem 66.68c 54.57* 69%
CBCL = child behavior checklist.a. n = 105.b. Borderline
clinical range.c. Clinical range.*p
-
8/18/2019 don't kick me out
12/14
38 Clinical Case Studies 9(1)
Declaration of Conflicting Interests
The first, third, and fourth authors are directly involved in
the day treatment services described in this
manuscript. This could be perceived as a conflict of interest.
The second and fifth authors are employed
full-time by universities not affiliated with the day treatment
program.
Funding
The authors received no financial support for the research
and/or authorship of this article.
Note
1. DSM-IV, 312.9 Disruptive Behavior Disorder-NOS, Disruptive
Behavior Disorder NOS (not otherwise
specified) is utilized when there are conduct or
oppositional-defiant behaviors that do not meet diag-
nostic criteria for conduct disorder or oppositional defiant
disorder, but in which there is clinically sig-
nificant impairment. ( Diagnostic and Statistical Manual of
Mental Disorders, Fourth Edition; DSM-IV;
American Psychiatric Association, 1994, p.103).
References
Achenbach, T. M. (1991a). The child behavior
checklist—1991. Burlington, VT: University of Vermont,
Department of Psychiatry.
Achenbach, T. M. (1991b). Manual for the child behavior
checklist/ 4-18 and 1991 profile. Burlington, VT:
University of Vermont, Department of Psychiatry.
Achenbach, T. M., & Rescorla, L. A. (2000). The child
behavior checklist for ages 1½ - 5. Burlington, VT:
ASEBA, University of Vermont.
American Psychiatric Association. (1994). Diagnostic and
statistical manual of mental disorders (4th ed.).
Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and
statistical manual of mental disorders (4th ed.,
text revision). Washington, DC: Author.Axelrod, S. (1971). Token
reinforcement programs in special classes. Exceptional Child,
37 , 371-379.
Bandura, A. (1969). Principles of behavior
modification. New York: Holt, Rinehart, and Winston.
Bandura, A., & McDonald, F. J. (1963). Influence of social
reinforcement and the behavior of models in
shaping children’s moral judgments. Journal of Abnormal and
Social Psychology, 67 , 274-281.
Berryhill, J. C., & Prinz, R. J. (2003). Environmental
interventions to enhance student adjustment: Implica-
tions for prevention. Prevention Science, 4, 65-87.
Bondy, A., & Frost, L. (2004). The picture exchange
communication system. Behavior Modification, 25,
725-744.
Brock, S. E., Lazarus, P. J., & Jimerson, S. R.
(2002). Best practices in school crisis prevention and
inter-
vention. Bethesda, MD: National Association of School
Psychologists.Christophersen, E. R., Arnold, C. M., Hill, D. W.,
& Quilitch, H. R. (1972). The home point system: Token
reinforcement procedures for application by parents of children
with behavior problems. Journal of
Applied Behavior Analysis, 5, 485-497.
Costello, E. J., Angold, A., Burns, B. J., Erkanli, A., Stangl,
D. K., & Tweed, D. L. (1996). Preventing
mental disorder in school-aged children: A review of the
effectiveness of prevention programs. Report
submitted to The Center for Mental Health Services(SAMHSA).
Prevention Research Center, Pennsyl-
vania State University.
Drotar, D., La Greca, A. N., Lemanek, K., & Kazak, A.
(1995). Case reports in pediatric psychology: Uses
and guidelines for authors and reviewers. Journal of
Pediatric Psychology, 20, 549-565.
Durlak, J. A., & Wells, A. M. (1997). Primary prevention
mental health programs for children and adoles-
cents: A meta-analytic review. American Journal of
Community Psychology, 25, 115-152.
Eckert, T. L., McGoey, K. M., & DuPaul, G. J. (1996,
November). Preschool-aged children at-risk for
ADHD: A needs assessment of parents, service providers and
experts. Paper presented at the annual
meeting of the Association for the Advancement of Behavior
Therapy, New York.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
13/14
Burke et al. 39
Gilliam, W. S. (2005). Prekindergarteners left behind:
Expulsion rates in state prekindergarten systems.
New Haven, CT: Yale University Child Study Center.
Gilliam, W. S., & Shahar, G. (2006). Preschool and child
care expulsion and suspension: Rates and predic-
tors in one state. Infants & Young Children, 19,
228-245.
Gresham, F., Sugai, G., & Horner, R. H. (2001). Interpreting
outcomes of social skills training for studentswith high-incidence
disabilities. Exceptional Children, 67 , 331-344.
Jacobson, N. S., & Truax, P. (1991). Clinical significance:
A statistical approach to defining meaningful
change in psychotherapy research. Journal of Consulting and
Clinical Psychology, 59, 12-19.
Kazdin, A. E. (1977). The token economy: A review and
evaluation. New York: Plenum.
Kazdin, A. E. (1990). Psychotherapy for children and
adolescents. Annual Review of Psychology, 41, 21-54.
Koertering, L. J., & Braziel, P. M. (1999). School dropout
from the perspective of former students: Implica-
tions for secondary special education programs. Remedial
& Special Education, 20, 78-83.
Larzelere, R. E., & Kuhn, B. R. (2005). Enhancing behavioral
parent training with an extended discipline
ladder. Behavior Therapist, 28, 105-108.
Maag, J. W. (2001). Rewarded by punishment: Reflections on the
disuse of positive reinforcement in
schools. Exceptional Children, 67 , 173-186.
McGoey, K. E., Eckert, T. L., & DuPaul G. J. (2002). Early
intervention for preschool-age children with
ADHD: A review of the literature. Journal of Emotional and
Behavioral Disorders, 10, 14-28.
Morrison, G., & D’Incau, B. (1997). The web of
zero-tolerance: Characteristics of students who are recom-
mended for expulsion from school. Education & Treatment
of Children, 20, 316-335.
National Scientific Council on the Developing Child.
(2008). Mental health problems in early childhood
can impair learning and behavior for life (Working paper
No. 6.). Available from http://www.develop-
ingchild.net
Olsen, S. L., & Hoza, B. (1993). Preschool developmental
antecedents of conduct problems in children
beginning school. Journal of Clinical Child
Psychology, 22, 60-67.
Patterson, G. R., Reid, J. B., & Dishion, T. J.
(1992). Antisocial boys. Eugene, OR: Castalia
Publishing.Peterson, J., & Peterson, R. (2006). Mini
methods or madness. Omaha, NE: Behave’n Kids Press.
Powell, D., Dunlap, G., & Fox, L. (2006). Prevention and
intervention for the challenging behaviors of tod-
dlers and preschoolers. Infants & Young Children, 19,
25-35.
Powell, D., Fixsen, D., & Dunlap, G. (2003). Pathways
to service utilization: A synthesis of evidence
relevant to young children with challenging
behavior. Tampa: University of South Florida, Center for
Evidence-Based Practice: Young Children with Challenging
Behavior.
Raver, C. C., & Knitzer, J. (2002). Ready to enter:
What research tells policymakers about strategies to
promote social and emotional school readiness among three-
and four-year-olds. New York: National
Center for Children in Poverty.
Reid, R., Gonzalez, J. E., Nordness, P. D., Trout, A., &
Epstein, M. H. (2004). A meta-analysis of the academicstatus of
students with emotional/behavioral disturbance. Journal of
Special Education, 38, 130-143.
Roberts, R. E., Attkisson, C. C., & Rosenblatt, A. (1998).
Prevalence of psychopathology among children
and adolescents. American Journal of Psychiatry, 155,
715-725.
Skinner, B. F. (1953). Science and human behavior. New
York: Free Press.
Small, S. A., Reynolds, A. J., O’Connor, C., & Cooney, S. M.
(2005). What works Wisconsin: What science
tells us about cost-effective programs for juvenile delinquency
prevention. Madison, WI: University of
Wisconsin–Madison.
Snyder, H. (2001). Child delinquents. In R. Loeber & D.
Farrington (Eds.). Risk factors and successful
interventions. Thousand Oaks, CA: SAGE.
Taylor-Richardson, K. D., Heflinger, C. A., & Brown, T. N.
(2006). Experience of strain among types of
caregivers responsible for children with serious emotional and
behavioral disorders. Journal of Emo-
tional & Behavioral Disorders, 14, 157-168.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/18/2019 don't kick me out
14/14
40 Clinical Case Studies 9(1)
Thompson, R. W., Ruma, P. R., Brewster, A. L., Besetsney, L. K.,
& Burke, R. V. (1997). Evaluation of an
air force child physical abuse prevention project using the
reliable change index. Journal of Child and
Family Studies, 6 , 421-434.
Tse, J. (2006). Research on day treatment programs for
preschoolers with disruptive behavior disorders.
Psychiatric Services, 57 , 477-486.U.S. Public Health
Service. (2000). Report of the surgeon general’s conference on
children’s mental health:
A national action agenda. Washington, DC: Department
of Health and Human Services.
Wolery, M., Bailey, D. B., & Sugai, G. M.
(1988). Effective teaching: Principles and procedures of
applied
behavior analysis with exceptional children. Needham, MA:
Allyn and Bacon.
Wolf, M. M., Giles, D. K., & Hall, R. V. (1968). Experiments
with token reinforcement in a remedial class-
room. Behaviour Research and Therapy, 6 , 51-64.
Bios
Ray Burke, Ph.D., is Director of Community Services and
Program Evaluation for Behave'n (a day treat-
ment and mental health clinic for young children with behavior
disorders) and an adjunct faculty member
in the Department of Education and Human Sciences at the
University of Nebraska, Lincoln with research
interests in behavior disorders, treatment fidelity, and
resistance to behavior change.
Brett R. Kuhn, Ph.D. is a licensed psychologist and
Associate Professor of Pediatrics at the University of
Nebraska Medical Center (UNMC). He has served as the
Supervising Practitioner at Behave'n Day Center
since its inception. His clinical and research interests fall in
the areas of children's behavioral health prob-
lems including sleep disorders, elimination problems, and
challenging behavior.
Jane L. Peterson, Nebraska Licensed Mental Health
Practitioner, is co-founder of Behave'n and has co-
authored children's books and books on parenting and family
therapy. Her clinical interests include
replication of programs for young children with mental health
disorders.
Roger W. Peterson, is co-founder of Behave'n, a Licensed
Mental Health Practitioner, co-author of chil-
dren's and parenting books, and has worked with children and
families for over 30 years. He is actively
involved in legislation and practices to improve access to
mental health services for Nebraska's children and
families.
Amy Badura Brack, Ph.D., is an associate professor of
psychology at Creighton University with clinical
research interests in stress reactions and behavioral
disorders.