Embed Size (px)
Citation preview

Douglas Woelkers, MD Associate Professor Maternal Fetal Medicine University of California, San Diego

Differences in preeclampsia between
Early preterm
Late preterm
Term preeclampsia
Fetal risks Maternal risks Constructing rational delivery plan Risk stratification by biomarkers

Stage II - Maternal Endothelial dysfunction Vasospasm
Hypertension Capillary leak
Edema Proteinuria
Stage I - Placental Poor implantation Defective remodeling Perfusion mismatch Hypoxia, inflammation
“Toxins”
•Nulliparity • In Vitro IVF •Preeclampsia •Multiples
•Chronic Hypertension •Renal disease • Lupus
•Age •Dyslipidemia •Diabetes •Obesity
Risk Factors


*Lain, et al. JAMA 2002
0%
5%
10%
15%
20%
20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43
Gestational Age
% Births
% PET
2009 Natality Statistics, CDC
% of all births
% preeclampsia births per week
65% 10% 25%
Early Preterm Late Preterm
Term

Higher prevalence of placental pathology
0
10
20
30
40
50
60
70
80
90
< 28 28-32 33-37 > 37
% P
reva
len
ce
Gestational Age
Placental Pathology in Preeclampsia
arteriopathy
infarction
hypermaturity
Moldenhauer, et al. AJOG 2003

Higher proportion of severe disease
0%
20%
40%
60%
80%
100%
24-28 28-34 34-37 >37
% o
f ca
ses
Gestational age (weeks)
265 Cases of Preeclampsia by Gestational Age
Mild
Severe
Lai, et al. SMFM 2007

Higher maternal mortality
0
5
10
15
20
25
>3733-3629-32< 28
Ris
k R
ati
o
Gestational Age (weeks)
Maternal Mortality Risk
MacKay, et al. Obstet Gynecol, 2001

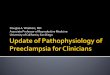
Impact of preeclampsia and gestational hypertension on birth weight (n = 87,798), Alberta, Canada, 1991–1996.
Xiong X et al. Am. J. Epidemiol. 2002;155:203-209
Smaller Same Larger
Greater fetal growth delay

Gestational Age Morbidity in 8523 Neonates, 1997–1998

Lung maturity is not advanced in preeclampsia
Schiff, et al. AJOG 1993
0%
20%
40%
60%
80%
100%
PET CON PET CON PET CON PET CON
29-31 31-33 33-35 35-37
Mature Amnio Rate
ns
ns
ns
ns

RDS is not reduced in preeclampsia
Chang, et al. Obstet Gynecol 2004
Preeclampsia
Normotensive
RDS Incidence by Gestational Age
Per
cen
t R
DS

Deliver
For maternal benefit
For fetal benefit
Expectant management
For fetal benefit
Maternal risk
Depends on gestational age and outcomes

1st Trial (Sibai, 1984)
Unselected cohort, N=60
Severe preeclampsia
17 to 28 weeks
No steroids
Offered expectant management
Minimal monitoring
Complication N Percent
Abruption 13 22%
Eclampsia 10 17%
Coagulopathy 5 8%
Renal Failure 3 5%
Hypertensive Encephalopathy 2 3%
Hepatic Rupture 1 2%
Fetal Demise 21 35%
Neonatal Demise 31 52%
Neonatal Survival 8 12%

2nd Trial (Sibai, 1990)
Selected cohort
Maternal & fetal monitoring
Steroids, magnesium, anti-hypertensives
N=109
19-27 weeks
GA < 24 (n=25) Offered termination
Expectant (15) 1 survivor
Termination (10)
GA 24-27 (84) Steroids given
Delivery (30)
Expectant (54)
Outcomes Deliver (n=30)
Expectant (n=54)
Eclampsians 3.3% 5.6%
Abruptionns 6.7% 5.6%
HELLPns 13% 13%
Latency* 2 d 13.2 d
Gest age 26.3 wk 28.0 wk
Birth weight 709 gm 800 gm
Perinatal mortality*
64% 24%

Summary Outcomes of Previable Preeclampsia, <24 weeks
Author N Perinatal Death (%)
Maternal Complications (%)
Sibai, 1990 15 93 27
Moodley, 1993 10 100 50
Visser, 1995 25 84 NR
Gaugler-Seden, 2006 26 82 65
Hall, 2001 8 88 36
Budden, 2006 31 71 71

Fetal outcomes are poor Maternal risks are high Delivery should be considered with severe
preeclampsia before viability

Sibai, 1994
Severe preeclampsia
28-32 weeks ▪ Delivery 48 hrs after
steroids vs.
▪ Expectant management
Intensive maternal and fetal monitoring
Outcome Deliver (n=46)
Expectant (n=49)
Eclampsia ns 0 0
Abruption ns 2 2
HELLP ns 1 2
Latency * 2.3 d 15.4 d
GA delivery * 30.8 wks 32.9 wks
IUFD, NND ns 0 0
RDS * 50% 22.4%
NEC * 10.9% 0
ICH ns 6.5% 2%

Author GA (wks) N Latency (d)
Sibai 28-32 46 15 (3-32)
Odendaal 26-34 18 7.1
Sibai 24-27 54 13 (2-26)
Olah 24-32 28 9.5 (2-26)
Visser 26-31 229 14 (0-16)
Hall 26-34 340 10.3 (1-47)
Chammas 24-33 47 6 (1.5-28)
Vigil-DeGracia 24-34 129 8.5 (3-30)
Haddad 24-34 239 5 (2-35)
Oettle 23-34 131 11.6 (1-89)
Shear 24-34 155 5.3 (1-27)
Ganzevoort 24-34 216 11 (2-44)

No worsening of outcomes at earlier age
Maternal Outcomes of Expectant Management with Preeclampsia
by Gestational Age, N (%)
24-28
n=110
28-32
n=97
32-34
n=32
HELLP Syndrome 17 (16) 13 (13) 4 (13)
Abruption 7 (6.4) 5 (5) 2 (6)
D I C 3 (3) 0 0
Renal Insufficiency 6 (5) 5 (5) 2 (6)
Haddad, et al. AJOG 2004

Perinatal Outcomes of Expectant Management with Preeclampsia
by Gestational Age
24-28
(n=110)
28-32
(n=97)
32-34
(n=32)
Latency (d) * 6 (2-35) 4 (2-32) 4 (2-12)
IUGR * 28 (25) 27 (27) 3 (9)
Neonatal Mortality * 7 (7) 0 0
Ventilation (d) * 3 (0-60) 0 (0-17) 0 (0-4)
RDS * 69 (66) 36 (37) 1 (3)
BPD * 34 (33) 6 (6) 0
IVH * 6 (6) 0 0
NEC * 6 (6) 1 (1) 0
NICU (d)* 22.5 (0-100) 8 (0-57) 5 (0-18) Haddad, et al. AJOG 2004

RDS (%) 43 57 42
IVH (%) 14 10 7
NEC (%) 4.5 3.4 0
BPD (%) 16 22 7
Perinatal death (%) 14 0 0
Expectant Management with IUGR
Complication <5th % (n=44)
5-10th % (n=52)
> 10th % (n=59)
Liver injury 18 (41) 22(42) 19 (32)
Thrombocytopenia 13 (30) 10 (19) 19 (33)
Eclampsia 2 (4.5) 1 (2.1) 0 (0)
Abruption 6 (13.6) 3 (5.8) 0 (0)
Pulmonary edema 4 (9) 2 (3.8) 0 (0)
Shear, et al. AJOG 2005

Higher rates of
Abruption
Pulmonary edema
Perinatal death
Consider expectant management only if < 28 weeks
Shear, et al. AJOG 2005

Very high risk endeavor
3 series of expectant management true HELLP ▪ Latency 3 to 7 days
▪ 3 liver rupture, 1 maternal death
▪ No improvement neonatal outcome vs delivery
Recommend active or intermediate delivery option
Chamas, et al. 2000 Van Pampus, et al. 1998 Van Runnard, et al. 2006

Variable Indication
Maternal Persistent severe headache or visual changes; eclampsia
Shortness of breath or chest tightness with rales and/or pulse oximetry of < 94% on room air; or pulmonary edema
Epigastric/right upper quadrant pain with AST or ALT > 2x the ULN
Oliguria (<500 mL/24 hr) or creatinine of >1.5 mg/dL
Persistent platelet count < 100,000
Suspected abruptio, labor, rupture of membranes
Fetal Severe growth restriction (<5%)
Persistent severe oligo (AFI < 5 or absent 2 x 2 pocket)
Repetitive variable or late decelerations
Biophysical profile (BPP) ≤ 2; or = 4 on two occasions
Reversed umbilical artery diastolic fow
Fetal death

Expectant management of severe preeclampsia remote from term
Requires expert management in tertiary center
Appropriate in selected cases
Yields comparable maternal outcomes to delivery
▪ Except eclampsia, abruption, HELLP, renal failure
Is associated with improved neonatal outcomes
▪ RDS, IVH, NEC
▪ Survival, IUGR

34 to 37 weeks
15-25% of preeclampsia
#1 indication for late preterm delivery
Optimal management is not defined
Neonatal morbidities decreasing…
But not absent
%

Outcomes (%) Gestational Age
340-6 350-6 360-6
Hyperbilirubinemia 22 15 12
NEC 1.2 0.4 0.1
O2 support 21 13 6.5
RDS 6.7 3.2 0.5
TTN 7.2 5.5 3.6
ICH 0.7 0.2 0.5
Convulsions 0.0 0.5 0.6
• Persistent neonatal risks 34 to 37 weeks
• Review of 1,864 cases of LP Preeclampsia
Langeveld, et al. 2011

Hypertensive vs normotensive infants Lower birth weights at 35-36 weeks
Greater need oxygen support (O2S) at 37 weeks
Greater NICU admit and length of stay at all ages
0%
10%
20%
30%
40%
50%
60%
SGA O2S NICU SGA O2S NICU SGA O2S NICU
35 36 37
Normotensive
Hypertensive*
* *
*
*
*
Habli, et al. AOG 2007

Severe preeclampsia, HELLP Syndrome Expedited delivery
Preeclampsia with co-morbidity (ie diabetes, CHTN) Delivery in 36-37th week
Non-severe preeclampsia Expectant management until 37 weeks
Risks of Expectant Management Incidence
Severe hypertension 10-15%
Eclampsia 0.2-0.5%
HELLP 1-2%
Abruption 0.5-2%
Growth restriction 10-20%
Fetal death 0.2-0.5% Sibai, et al. Semin Perinat 2011

Is amniocentesis useful?
34 to 37 weeks
51 patients with mature amnio ▪ Stable mild preeclampsia
Compared to 51 with no amnio ▪ Indicated delivery or labor
Same rate of RDS
Amnio has 10% false negative rate
9.8% 9.8%
0%
2%
4%
6%
8%
10%
12%
Mature amnio,elective delivery
No amnio,indicateddelivery
Ra
te o
f R
DS
Lewis, et al. 2009

No trials comparing options
HYPITAT Trial supports delivery over expectant management at 36 to 41 weeks ▪ For gestational hypertension (DBP >95) or preeclampsia
HYPITAT II (34+0 to 36+6) in progress
Expert opinion says…
Indications for delivery in LP Preeclampsia
Severe hypertension Preterm labor or ROM
Vaginal bleeding Growth restriction (<5%)
Oligohydramnios Recurrent FHR decelerations
Absent or reverse umbilical artery flow BPP ≤ 6
Sibai, et al. 2011

---- cut-off levels (5th centile)
100% sensitivity 96% specificity
Early Onset Preeclampsia Fetal Growth Restriction
100% sensitivity 86% specificity
---- cut-off levels (5th centile)
Placental IUGR Preeclampsia
Case-Control Cohort
Benton J, et al. Am J Obstet Gynecol 206(2); 2011

PELICAN Study (2012 UK)
649 subjects with suspected preeclampsia
▪ 278 subjects < 35 weeks (mean 31.0)
▪ PlGF determined at presentation
▪ Managed according to provider
▪ Final diagnosis determined after delivery
1Knudsen, et al. Pregnancy Hyperten 2;2012 In Press Circulation

Preeclampsia requiring delivery within 14 days
Sensitivity 67/71 0.94 0.86 – 0.98
Specificity 116/207 0.56 0.49 – 0.63
NPV 116/120 0.97 0.92 – 0.99
PPV 67/158 0.42 0.35 – 0.51
Preeclampsia requiring preterm delivery
Sensitivity 102/114 0.90 0.82 – 0.94
Specificity 108/164 0.66 0.58 – 0.73
NPV 108/120 0.90 0.83 – 0.95
PPV 102/158 0.65 0.57 – 0.72
GA < 35+0 using 5 %tile cutoffs

Preeclampsia requiring delivery within 14 days
Positive likelihood ratio 2.15
Negative likelihood ratio 0.10
Application of test into practice
Prior odds: 71 cases, 207 non-cases 0.33
Pre-test probability: 26%
If test positive: posterior odds: 0.74
Post-test probability: 43%
If test negative: posterior odds: 0.034
Post-test probability 3.3%

20 25 30 35 40 450
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Gestational Age
Pro
po
rtio
n o
f W
om
en
Un
de
live
red
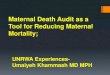
Length of Pregnancy, Sample GA < 35+0 (N=278)
PlGF High (n=120)
PlGF Med (n=93)PlGF Low (n=65)
Hazard Ratio for Time-To-Delivery* PlGF Med 2.31 (1.68-3.18) PlGF Low (<12 pg/ml) 10.61 (7.09- 15.89)
*adjusted for gestational age at sampling and final diagnosis.
All patients tested before 35 weeks (N=278)
High
Low
Med

38 not for print or distribution
Receiver Operator Curve (ROC) analysis
Endpoint is preterm pre-eclampsia delivering within 14 days
PlGF outperforms all other tests (AUC 0.88)
PlGF sensitivity for the endpoint is 96% (73/76)*
PlGF NPV for the endpoint is 98% (118/121)*
Standard tests individually or in combination (AUC 0.69) have poor discrimination
*cutoff 100pg/mL
SBP = Systolic BP, DBP = Diastolic BP, ALT =Alanine transaminase
0.00
0.25
0.50
0.75
1.00
Sensitiv
ity
0.00 0.25 0.50 0.75 1.00
1-Specificity
Test: ROC area (SE)
PlGF: 0.88 (0.03)
SBP: 0.65 (0.04)
DBP: 0.65 (0.05)
Urate: 0.68 (0.05)
ALT: 0.58 (0.05)
PlGF is superior to other tests for diagnosis of preterm pre-eclampsia delivering in 14 days

39 not for print or distribution
SBP = Systolic BP, DBP = Diastolic BP, ALT =Alanine transaminase, Uric Acid uses a GA-dependent cutoff. Cutoffs are based on PRECOGII Guideline. BMJ 2009;339:b3129
<35w GA % Sens % Spec % PPV % NPV OR
PlGF <100 pg/mL 96.1 55.9 44.0 97.5 30.87
Dipstick ≥2+ 66.7 81.0 52.6 88.4 8.50
Uric acid* 43.6 88.0 60.0 79.1 5.66
SBP ≥170 mmHG 26.7 86.3 40.8 76.8 2.28
DBP ≥110 mmHg 17.3 85.8 30.2 74.5 1.27
ALT ≥32 IU/L 11.3 88.7 28.6 71.4 1.00
PlGF is superior to other tests for diagnosis of preterm pre-eclampsia delivering in 14 days

PlGF n Time to Delivery, d
Median (IQR)
Undetectable < 12 pg/ml 12 9 (6.2 – 10.5)
Low < 5th %tile 22 18 (8.5 – 22.0)
Normal > 5th %tile 14 56 (39.2 – 76.7)
48 cases with 1) hypertension, or 2) proteinuria, but not both

Thank You