Embed Size (px)
Citation preview

Probiotics in Inflammatory Bowel Disorder (IBD)
Dr. Neelam MohanDNB(Pediatrics), FPGH(UK),FIMSA,FACG(USA), FIAPDirector - Department of Pediatric Gastroenterology, Hepatology and Liver Transplantation Medanta Medicity – Gurgaon ( Delhi NCR)
Pioneer in liver transplant program in India & heads the busiest Pediatric Liver Transplant Centre.Pioneer in Endoscopy in neonates. Set up first IAP fellowship program in Pediatric Gastroenterology & Hepatology in India. National Coordinator of diarrhea module 2012 – in IndiaSecretary – Indian Society of Gastroenterology, Hepatology & Nutrition (ISPGHAN)Honored with “Zee swasth Bharat Samman” Award by the health Minister of India & “DMA Centenary Award - 2014” by Hon’ble Health Minister Harsh Vardhan & Hon’ble Finance Minister Arun Jaitley.
Probiotics from Bench to Community ; 7-8 March 2015, The Grand , New Delhi

My Presentation
2
Role of Microbiome in the pathogenesis of IBD
Role of Probiotics in Ulcerative Coltitis• Acute inflammation • Maintenance treatment• Pouchitis
Role of Probiotics in Crohn’s disease
Adults & children

Charaka Samhita (supposed to be written in 1000 BC), a treatise on Ayurveda medicine “Jataragni” (fire in stomach) – Beneficial
microbial flora of GI tract &“Takra” i.e., fermented milk, as “Amrita” or
elixir.
3

Interesting facts
• The human gut normally hosts roughly 1014 bacterial organisms of up to 1000 different species; this bacterial community can add up to 1-2 kg.
• In total, the number of intestinal bacteria is approximately ten times the number of cells constituting the human body
• The collective bacterial genome, also referred to as the microbiome, contains 100-fold more genes than the entire human genome.
4Wehkamp J et al. Germany: Falk Foundation e.V., 2013Stephani J et al. Arch Immunol Ther Exp (Warsz) 2011; 59: 161-177

Fact
5
Gut Microbiota
Common to all
Individualised

Role of Microbiome in the pathogenesis of IBD
6

Intestinal Microbiota & IBD
• There is plenty of evidence supporting the hypothesis of the involvement of intestinal microbiota in IBD pathogenesis.
• Crohn’s disease (CD) and ulcerative colitis (UC) tend to occur in the colon and distal ileum, which contain the highest intestinal bacterial concentrations.
• A pathogenic role of luminal constituents is suggested by the prevention and treatment of Crohn’s disease by the diversion of fecal stream and reactivation of inflammation within one week following reinfusion of ileostomy contents.
Sartor RB et al. Gastroenterology 2008; 134: 577-594D’Haens GR et al Gastroenterology 1998; 114: 262-267

Intestinal Microbiota in Pathogenesis of IBD
• Similarly, Ulcerative Colitis patients who undergo ileal pouch-anastomosis surgery develop mucosal inflammation after bacterial colonization of the pouch.
• Furthermore, there are many studies on animal models supporting the role of gut microbiota in the development of IBD.
• In experimental animal models of IBD, genetically- engineered animals developed spontaneous colitis under standard laboratory conditions, but remained colitis-free when they were raised in a sterile, germ-free environment, thus indicating that bacterial exposure and colonization are essential for the development of colitis.
8Harper PH et al Gut 1985; 26: 279-284
de Silva HJ et al Gut 1991; 32: 1166-1169Taurog JD et al. J Exp Med 1994; 180:2359-2364

Intestinal Microbiota in Pathogenesis of IBD
• The majority of genes found to be associated with an increased risk for the development of IBD are those encoding proteins that act to preserve the mucosal barrier and/or regulate the host immune system.
• A major breakthrough in understanding the linkage between genetic predisposition and IBD development was the discovery of the NOD2/CARD15 gene, which encodes a protein responsible for microbial recognition, induction of antimicrobial genes, and control of the host adaptive immune response.
9

Intestinal Microbiota in Pathogenesis of IBD
• Patients with CD have increased intestinal permeability, which could reflect mucosal barrier defects that promote bacterial translocation through the intestinal mucosa.
• The intestinal mucus barrier is significantly altered in UC patients, particularly in terms of mucus composition and phospholipid concentration.
10

Intestinal Microbiota in Pathogenesis of IBD
• Interaction between Intestinal Microbes and mucosa of susceptible individuals Triggers a cascade of reactions.
11
+ Th1 / Th2
Mucosal damage

Machanism of Action of Probiotics
12
Pathogens Probiotics
Produce antimicrobial
substance
Stimulation of immunity
Compete for nutrients
Competition for receptors
Receptors on intestinal walls where pathogens attached
Degradation of toxin pathogen receptors
Mucin secretion
Block receptors

Role of Probiotics in Ulcerative Colitis
13

Probiotics in Ulcerative Colitis
Probiotics in treatment of Active Inflammation
in Ulcerative Colitis

Randomized Trails of Probiotics as therapy of Active UC
15
Participants / Treated (Yr of Study)
Trial Design
Probiotic (Strains) Trial Length (weeks )
Results
20 (10) (2004)
EBRPC Blend Probiotic (Yakult™) + 5ASA
Placebo + 5ASA
12Pr - 40%, Placebo 30%, [OR 0.64 (95% CI 0.10 to 4.10)]
90 (30) (2004)
R Blend Probiotic (VSL#3™) + Balasalazide
Placebo + Balasalazide
8 Pr - 80% Placebo 70%, [OR 0.58 (95% CI 0.18 to 1.91)]
102 (52) (1999)
DBRDD Single strain (E. coli Nissle) + Steriods Mesalazine + steroids
12 Pr- 68.4%, mesalazine 74.6%, OR 1.35 (95% CI 0.6 to 3.04).
EBRPC: Endoscopy blinded, randomized, placebo-controlled; R: Randomized; DBRDD: Double-blind, randomized, double-dummy.
Dosing (CFU/day) 1 × 1010
9 × 1011
1 × 1011
Mallon et al. concluded that addition of a probiotic to conventional therapy did not improve overall remission rates in patients with mild to moderate ulcerative colitis but the addition of probiotics may reduce disease activity.

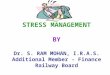
Probiotics in Ulcerative Colitis (Mod. to Sev. ) in Children
16
Corticosteroid dose (1 mg/kg/day to a maximum of 40 mg/day) and Mesalamine (50 mg/kg/day) dose (n=14)
+ +
Probiotic VSL#3 Placebo
Remission 13/14 (92.8%)
Remission4/15 (36.4%)
P < 0.001
Miele E et al. Am J Gastroenterol. 2009;104:437–443.

Probiotics in Ulcerative Colitis (UC) in Children – Recent Trial
• 31 children with mild to moderate ulcerative proctitis / proctosigmoiditis with mild to moderate disease activity
• Study duration 8 weeks
17
Mesalazine + Enema solution with L. reuteri ATCC 55730.
Mesalazine + Placebo
• Clinical and endoscopic improvements better in the probiotic group. • Histological score significantly decreased in the L. reuteri group (P<0.01). • A significant increase in the mucosal expression levels of IL-10 and a significant decrease in the levels of IL-1b, TNFa, and IL-8 mucosal expression levels (P\0.01) were documented only in the L. reuteri group.
Oliva S. et al . Aliment Pharmacol Ther. 2012; 35(3):p. 327–34.

Probiotics / Prebiotics / Both in Active UC
18
Fujimori, S. et al. Nutrition 2009, 25, 520–525
Patients on stable doses of aminosalicylates and/or prednisolone for at least 4 weeks in remission or had mildly active UC
Prebiotics Probiotics B longum
Prebiotics + Probiotics B longum
Only those patients taking a combination of a Prebiotic and B. longum had an improvement (p = 0.03)

Probiotic in Adults UC in India
• Multicenter, randomized, double blind, placebo-controlled trial from India.
• VSL#3 in adults with mild-to- moderate UC. • Dose - 3.6 × 1012 CFU VSL#3 (N = 77) or placebo (n = 70) twice
daily for 12 weeks.
19
Sood et al. Clin. Gastroenterol. Hepatol. 2009, 7, 1202–1209
Probiotic Placebo p Value
Primary end point (50% decrease in *UCDAI ) at 6 weeks
32.5% 10% 0.001
Secondary end points - 12 weeks 42.9% 15.7% 0.001
*UC disease activity index

Probiotics in Ulcerative Colitis
Maintenance of Remission

Probiotics in Maintenance of Remission UC
21J Clin Gastroenterol. Volume 45, supp.3, Nov./ Dec. 2011
DB, double-blind;

Probiotics in Maintenance of Remission UC
22
J Clin Gastroenterol. Volume 45, supp.3, Nov./ Dec. 2011
Children
• It is not the probiotic and the dose alone but also the specific strain of probiotic that matters.

Probiotics in Ulcerative Colitis
Treatment of Pouchitis
Proctocolectomy with ileal pouch-anal anastomosis may be required in some UC patients because their disease was medically intractable or they developed secondary dysplasia or cancer. Pouchitis or inflammation of the ileal reservoir created during the procedure may develop in between 15 and 50% in patients. It is the most common complication of the surgery and although the exact etiology is not clear host genetic factors, local pouch issues and the microbiota contained within the pouch are thought to be involved.

Probiotics in Pouchitis
24J Clin Gastroenterol. Volume 45, supp.3, Nov./ Dec. 2011

Summary of Probiotics in UC
25
• Over the past 3 years we have seen a more robust efficacy of probiotics, such as VSL#3, to induce remission in mild-to-moderately active UC
• The efficacy of probiotics as an “ADJUNCT” therapy for patients who fail standard therapy and who otherwise have to step up to steroids and/or immunosuppressives is an important contribution to the clinical field.
• This beneficial effect was also reported in children with UC, a group in which we would like to avoid the use of steroids that could lead to further growth retardation.

Summary of Probiotics in UC
Probiotics Strains Evidence
Inductions of Remission VSL#3 Level A
Maintenance of Remission VSL#3
E coli Nissle 1917
Level A
Level B
Pouchitis VSL#3 Level A
26

Role of Probiotics in Crohn’s Disease (CD)
27

Maintenance of Remission – Adults
28J Clin Gastroenterol. Volume 45, supp.3, Nov./ Dec. 2011

Probiotic - S. Boulardii in CD – Adults
First Author Date
Design duration
Probiotic Concomitant Therapy
Results
Vilela et al ;
Scand J Gastroenterol.2008
DB, R, C 3mo S. Boulardii (4108 CFU) n=15
Mesalamine,AzathioprinePrednisone, metronidazol/thalidomide
Improved permeability(P=0.0005) andmaintenance of remission
Bourreille A, et al
Clin Gastroenterol Hepatol. 2013
RCT, 1 yr S. Boulardii Frequency of relapses -Saccharomyces boulardii group - (47.5 %)Placebo - (53.2 %)
Time to relapse was also notstatistically different
29

Probiotics in CD in Children
30

Gupta P et al. J Pediatr Gastroenterol Nutr 2000;31:453Y7.

Probiotic Lactobacillus GG in Pediatric CD
32
Multi centric , USA, n=75 children (5-21 yrs)
Groups
LGG (n=39) Placebo (n=36)
• No difference in adverse events in the 2 groups. • Median time to relapse was same in 2 groups

Summary Probiotics in CD
• There is no evidence of efficacy for any used strain in pediatric / adult CD unlike UC.
• The pathogenesis of UC and CD, especially the role of microbes-host interaction, is different between these 2 disease entities .
• Given the array of genotype & phenotype of CD, we need to identify the specific Probiotic that may be beneficial.
33

CAPGAN 2015 : 2 -4 Oct. Online Registration Open
Conference Secretariat:-Dr. Neelam Mohan
DirectorDepartment of Pediatric Gastroenterology, Hepatology
& Liver TransplantationMedanta-The Medicity Hospital, Gurgaon – India
Email – [email protected]
Dr. Neelam MohanOrganising Secretary
www.capgan2015.com

35




• Probiotics (Yakult™) + 5-ASA had similar effectiveness to placebo + 5-ASA for induction of remission [28]: probiotic 40%, placebo 30%, OR 0.64 (95% CI 0.10 to 4.10).
• Probiotics (VSL#3™) + balsalazide had similar effectiveness to placebo + balsalazide for induction of remission [30]: probiotic 80%, placebo 70%, OR 0.58 (95% CI 0.18 to 1.91).
• Probiotics (E. coli Nissle 1917) + steroids had similar effectiveness to mesalazine + steroids for induction of remission [31]: probiotic 68.4%, mesalazine 74.6%, OR 1.35 (95% CI 0.6 to 3.04).

Blend Probiotic (VSL#3). Dose-1 × 1011/kg
• N=29 (14), DBRPC
• In a trial in children with moderate-to-severe disease VSL#3™ or placebo was administered along with corticosteroids and mesalamine.
• The corticosteroid dose (1 mg/kg/day to a maximum of 40 mg/day) and mesalamine (50 mg/kg/day) dose were those commonly used.
• The corticosteroids were tapered after a month if subjects were in remission.
• In this study, remission was achieved in 13 of 14 participants (92.8%) treated with VSL#3™ and IBD therapy and in 4 of 15 patients (36.4%) treated with placebo and IBD therapy (p < 0.001).
• This result must be taken in context the response rate to corticosteroids and mesalamine in the placebo treated group.
Miele, E et al. Am. J. Gastroenterol. 2009, 104, 437–443.