Embed Size (px)
Citation preview
463
DUPUYTREN'S CONTRACTUREBy J. S. R. GOLDING, F.R.C.S.
Senior Registrar, Department of Plastic Surgery, The Middlesex Hospital
Astley Cooper recognized a contracture of thepalmar fascia in the hand and described its treat-ment by subcutaneous fasciotomy (I822), but itwas Dupuytren (1834) who clearly differentiated,from a mass of other conditions causing clawing ofthe fingers, the peculiar condition to which hisname has been given.The contracture usually starts as a slightly
tender nodule, later becoming hard and painless,in the palm proximal to the ring finger. The skinbecomes attached to the nodule and a small, pit-like' pucker' develops. The thickening graduallyprogresses and nodules appear in the finger itself,which becomes progressively more flexed atthe metacarpo-phalangeal and proximal inter-phalangeal joints, and extended at the distal joint.
Since the time of Astley Cooper many attempts
have been made to devise a satisfactory treatmentfor the condition, but with so little success thatsignificant published results have been extremelyfew until recent years, when a firmer grasp of thepathology and anatomy of the condition has en-abled a satisfactory technique of treatment to beevolved, giving excellent results in over 80 per cent..of cases (Skoog, I948).AnatomyThe palmar fascia is morphologically the ter-
mination of the palmaris longus muscle, which isprimitively the flexor of the metacarpo-phalangealjoints and is present in about 90 per cent. ofpeople. It is noteworthy, however, that Dupuy-tren's contracture can occur in the absence of apalmaris longus.
INTERFASCIALSEPTUM
SKIN
PALMAR FASCIANEUROVASCUL AR R A I
.-- - FIBRCUS PULLEY-AROUNDt d SYNOVIAL SHEATH AND
LUMBRICAL FLEXOR TENDOIS
2'P PALMAR \ ·ASCIA COVERINGINTEROS-SEIMETACARPAL
A R TE RY 3'?
3Ro DORSAL 2 Pt. PALMARIN TE ROSSE US IN TEROSSE1 S
DIAGRAM TO SHOW THE PALMAR FASCIA AND INTERFASCIAL SEPTA
JUST PROXIMAL TO THE HEAD OF THE 4TMHMETACARPAL BONE.
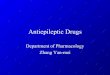
FIc. 1.-Diagram to show the palmar fascia and the interfascial septa immediately proximalto the head of the fourth metacarpal bone.
Protected by copyright.
on February 25, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.311.463 on 1 S
eptember 1951. D
ownloaded from
464 POSTGRADUATE MEDICAL JOURNAL September I951
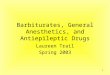
FIG. 2.-Diagram of a metacarpal bone and phalanges,to show the attachment of the palmar fascial slipsto the sides of the phalanges.
The palmar fascia binds the palmar skin to themetacarpal bones. It adheres to the skin intimatelybut is not attached to the neurovascular bundles orto the tendon sheaths. It is thicker on the ulnarthan on the radial side of the hand and is con-tinuous at its margins with the fascia over thethenar and hypothenar eminences. In the distalthird of the palm, longitudinal septa pass down oneither side of the tendons to be attached, with thefascia over the interossei, to the sides of the meta-carpal bones. Within these tunnels run thetendons which are separated by the septa from theneurovascular bundles and lumbrical muscles.These septa are attached to the transverse meta-carpal ligament and capsule of the joints. Thereis also a thin fibrous sheath covering the tendonswhich, in the region of the heads of the metacarpalbones, is thickened to form a ' pulley' preventingthe tendons from 'bow-stringing' across themetacarpo-phalangeal joints. This fibrous sheathis distinct from and is not affected by the contrac-tion of the fascia (Fig. i).
Distally the fascia divides into a strip for eachfinger, which passes down to be attached to thesides of the proximal phalanx and to the proximalhalf of the middle phalanx (Fig. 2).The digital nerve to the fifth finger may be
anomalous and may divide to the radial side of itsweb, to run obliquely behind the palmar fascia toreach the ulnar side of the finger. The nervepasses obliquely over the tendon sheath and behindthe palmar fascia in any position between thedistal palmar crease and the web. If it is not firstidentified in the neurovascular bundle proximallyand followed distally, it is liable to injury.AetiologyThe condition is more than eight times as
common in males as in females. It usually appearsbetween the ages of 30 and 40 years and progressesat a varying rate. In more than half the cases it isbilateral. In unilateral cases it is twice as commonin the right hand as in the left. Very frequently ahistory of familial incidence can be elicited.The fourth and fifth fingers are those usually
affected. Skoog (I948) reports that in 64 per cent.
of cases the fourth finger and in 53 per cent. ofcases the fifth finger is affected. The thirdfinger is affected in 24 per cent. and the indexfinger in 5 per cent. of cases. The thumb isaffected in only about 3 per cent. of cases.There is no conclusive evidence of any associa-
tion of Dupuytren's contracture with any generaldisease except epilepsy, or with any particularoccupation, although Niederland (I932) reportedthe high incidence of 17.8 per cent. in certaintextile workers using the palms of their hands in aparticularly vigorous manner. However, there issome evidence that the severity of the contractureis greater where heavy manual work has been done.Cases with a strong hereditary factor tend to haveseveral fingers affected (Kanavel, et al., 1929).
There is no doubt that epileptics are particularlyaffected. Lund (I94I) found that about 50 percent. of I90 male epileptics and 25 per cent. offemale epileptics showed the condition. He re-marks that earlier workers did not notice thisassociation, and in fact Fere (quoted by Lund)writing early this century categorically stated thatDupuytren's contracture was rare in epileptics.Lund suggests that the advent of the barbituratesin the treatment of epilepsy may be the true causeof this remarkable association.The histological changes associated with
Dupuytren's contracture are also found on thebacks of the hands, where they are known asknuckle pads, and in the soles of the feet.
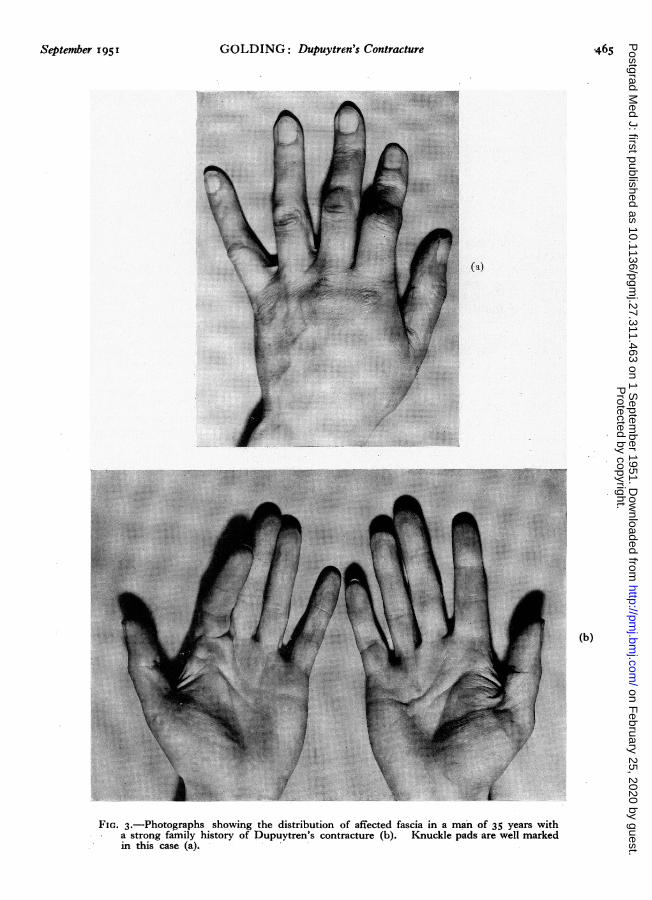
Knuckle Pads (Fig. 3b)These were first described by Paget (1875) in
association with gout. Garrod (1893) noticed theassociation with Dupuytren's contracture. Thepads are situated over the proximal interphalangealjoints and are commonly attached to the overlyingskin (Fig. 3). Microscopically the changes areidentical with those seen in the palm. Lund (I94)noticed knuckle pads in i8 per cent. of epilepticswithout Dupuytren's contracture and in 38 percent. of epileptics with the condition.
Dupuytren's Contracture Affecting the Plantar FasciaThis condition is rare. Bunnell (I944) noticed
Protected by copyright.
on February 25, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.311.463 on 1 S
eptember 1951. D
ownloaded from
September I951 GOLDING: Dupuytren's Contracture 465
MMio
...
tw- I~
...................
,,:i::···I·;::;;.;----R::}...:'..'.:: E-.... .. .....:;...
...!i~. ....!i~-i::i**!!iii ...:, .!-*:1!
* i:.^....:::::::!!::::!!::! !--: .-
......................
........:
....·:: ·· ·· :/·ill
xb
ii iil =i-
--el---
*: ·i;i·:·|i ·· ;?*:;llli:i::::
- ~ " |
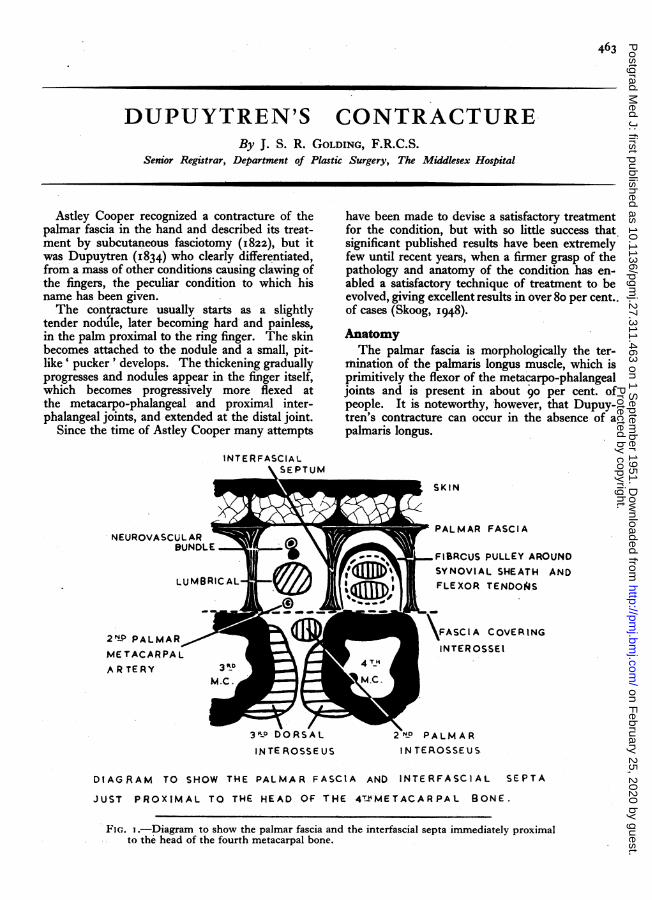
FIG. 3.-Photographs showing the distribution of affected fascia in a man of 35 years witha strong family history of Dupuytren's contracture (b). Knuckle pads are well markedin this case (a).
Protected by copyright.
on February 25, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.311.463 on 1 S
eptember 1951. D
ownloaded from
466 POSTGRADUATE MEDICAL JOURNAL September 1951
it in three of the 87 hand cases he had operated on.Skoog (1948) reported a case where the feet wereaffected before the hands. Considering the con-siderable trauma to which the soles of the feet aresubjected, it would be expected far more fre-quently if the condition had a purely traumaticaetiology.PathologyThe excised fascia shows a dense mass of
hyperplastic and irregular fibrous connectivetissue. In this there are hypercellular areas whichinterrupt the fibres rather than displace them.Iron pigment may be found.Meyerding (I941) believed the process to be a
chronic inflammatory reaction beginning in theinterstitial fibrous tissue of the palm. Horwitz(1942), comparing the tissue with that found innormal hands at autopsy, concluded that theprocess was a' benign fibroplasia ' and stressed thegreat similarity with the histology of keloid scarsand fascial desmoids. However, patients withDupuytren's contracture show no tendency toform either keloids or desmoids.
Skoog (1948) characterizes the condition by:-I. All structures in the palm are normal and
distinct from the contracted fascia.2. Nerves may be displaced but are never in-
filtrated.3. The subcutaneous tissue is displaced be-
cause of its attachment to the contracting cords offibrous tissue.
Skoog believes that the contracture is the resultof multiple partial ruptures occurring in a de-generating palmar aponeurosis which heals byscar formation. The iron pigment is the result ofminute haemorrhages, and the hypercellularregions are recent ruptures in the process of repair.This accounts for the interruption of the fibres.
TreatmentOnce this progressive fibrosis has commenced
we know that it will continue. Nothing less thanexcision of the whole affected tissue will givelasting relief. Operation deferred until capsularchanges have developed in the interphalangealjoints cannot give perfect results. Where bothhands are involved that less affected should betreated first, to lessen the incapacity of the patient.The many methods, such as subcutaneousfasciotomy, which have been used in the past havebeen entirely discarded except in certain cases asan adjunct to excision because recurrence isinevitable.
Recently vitamin ' E' has been tried (Stein-berg, I947) in the early active stage of the disease,but the results have been unsatisfactory (King,
I949). The only effective treatment is completeexcision of the palmar fascia and its septa.Operative Technique
It is essential to perform this delicate procedurein an avascular field. An Esmarch bandage isapplied to the upper arm and above this a blood-pressure cuff is inflated to a pressure of250 mm. Hg. The bandage is then removed. Itis safe to maintain this pressure for an hour. Thecuff is then deflated for lo minutes whilst a swabsoaked in saline is pressed into the wound (Bruner,195I). This procedure should be repeated athalf-hourly intervals.The hand is prepared with cetavlon and spirit;
no coloured antiseptic solution should be used ordifficulty will be encountered in ensuring that theblood flow is sufficient when the pressure dressinghas been applied after operation.
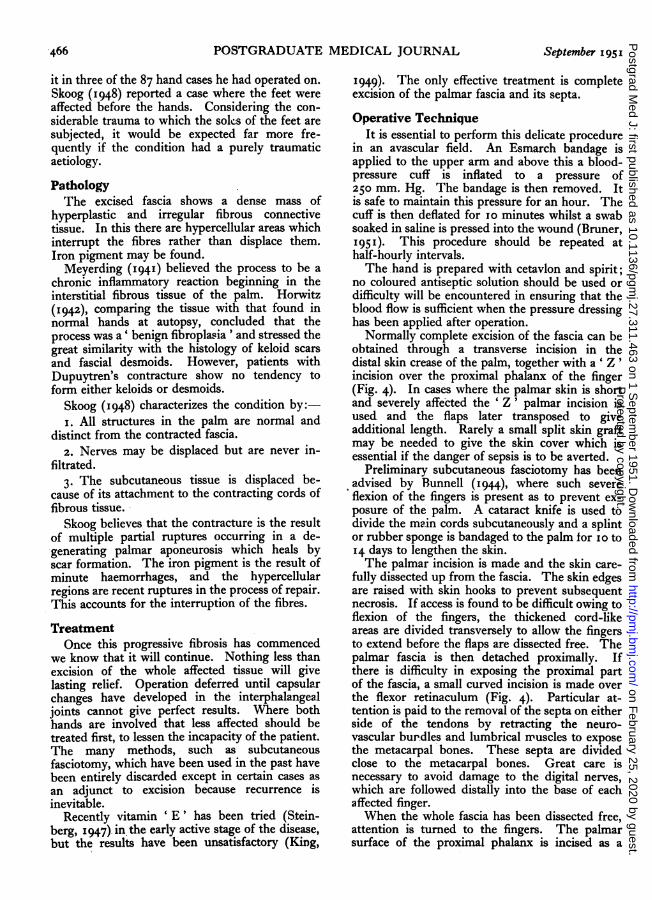
Normally complete excision of the fascia can beobtained through a transverse incision in thedistal skin crease of the palm, together with a ' Z 'incision over the proximal phalanx of the finger(Fig. 4). In cases where the palmar skin is shortand severely affected the 'Z' palmar incision isused and the flaps later transposed to giveadditional length. Rarely a small split skin graftmay be needed to give the skin cover which isessential if the danger of sepsis is to be averted.
Preliminary subcutaneous fasciotomy has beenadvised by Bunnell (I944), where such severeflexion of the fingers is present as to prevent ex-posure of the palm. A cataract knife is used todivide the main cords subcutaneously and a splintor rubber sponge is bandaged to the palm for o0 to14 days to lengthen the skin.The palmar incision is made and the skin care-
fully dissected up from the fascia. The skin edgesare raised with skin hooks to prevent subsequentnecrosis. If access is found to be difficult owing toflexion of the fingers, the thickened cord-likeareas are divided transversely to allow the fingersto extend before the flaps are dissected free. Thepalmar fascia is then detached proximally. Ifthere is difficulty in exposing the proximal partof the fascia, a small curved incision is made overthe flexor retinaculum (Fig. 4). Particular at-tention is paid to the removal of the septa on eitherside of the tendons by retracting the neuro-vascular burdles and lumbrical muscles to exposethe metacarpal bones. These septa are dividedclose to the metacarpal bones. Great care isnecessary to avoid damage to the digital nerves,which are followed distally into the base of eachaffected finger.When the whole fascia has been dissected free,
attention is turned to the fingers. The palmarsurface of the proximal phalanx is incised as a
Protected by copyright.
on February 25, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.311.463 on 1 S
eptember 1951. D
ownloaded from
September I95I GOLDING: Dupuytren's Contracture 467
I I
""
'·' ·.
.:::
r·I r
·. · cIr
.c '·
·.
..
r)·. I.'
.. .·
H.
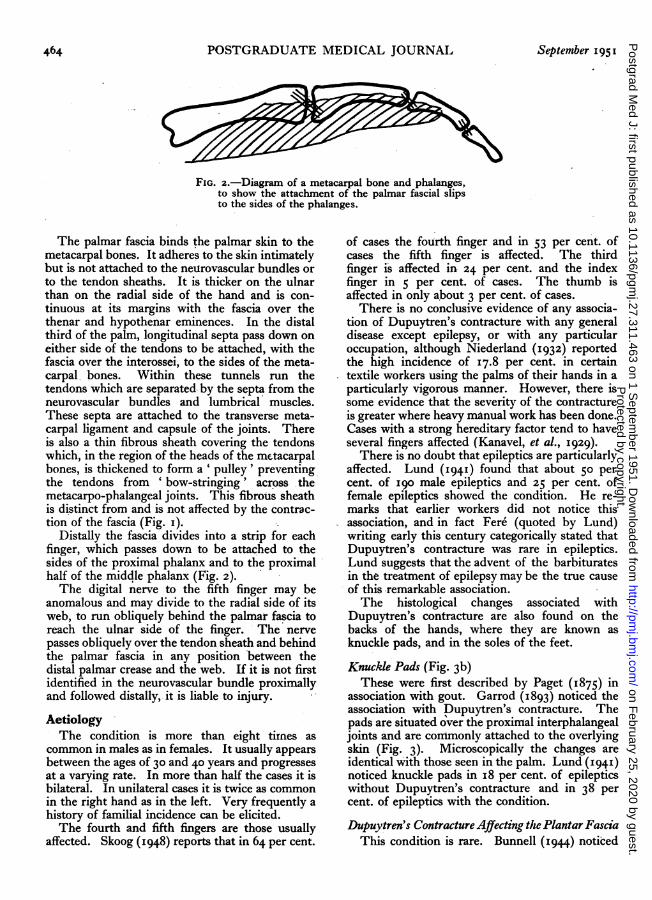
FIG. 4.-A diagram showing the incisions commonlyused. The central part of the fascia is exposedthrough an incision parallel to the distal palmarcrease. The digital extensions are excised throughincisions on the fingers, as shown, whilst the fasciais separated proximally from the flexor retinaculumthrough a small curved incision if this is necessary.
'Z,' and the flaps dissected free. The block offascia previously dissected is divided into a por-tion for each affected finger and the bridge of skinbetween the palm and finger undermined to allowthe fascia to be passed through. This exposes thedigital neuro-vascular bundles which are thenfollowed up from the palm into the finger and thefascia is dissected away from them and detachedfrom the sides of the phalanx. The fascia is fol-lowed up until normal tissue of the middle phalanxis reached and then divided.The two flaps of the finger are transposed,
utilizing the transverse width of skin to give theadditional length which is usually needed. Theflaps are carefully sutured, to avoid damage to the
skin edges. Toothed forceps should not be used.After operation a crepe bandage is applied firmlyover about an inch of cotton wool to give evenpressure. Cotton wool is placed between eachfinger, which makes the hand much more com-fortable. The blood pressure cuff is then releasedand removed and the fingers inspected to ensurethat the pressure bandage has not been applied tootightly.
For the first 24 hours the hand is suspended todiminish swelling. The pressure dressing is leftin place for io days; during this time the cottonwool between the fingers is removed if it is pre-venting the finger movements which are started onthe third post-operative day. Half the stitches areremoved on the tenth day, and the remainder re-tained until the fourteenth day because the palmheals slowly.An intensive course of physiotherapy, including
particularly wax baths and active exercises, iscommenced as soon as the palm is soundly healed.Usually the finger extension is full after four weeks'treatment.
ResultsIn a series of 55 hands operated on in this hospital
during the last five years it is too early to gainexact information about the success of the varioustreatments used. However, in over 75 per cent.of cases the results were considered to be good, andthe patients have not reported with recurrence. Infive cases where fasciotomy was performed, twowere later referred for excision and one was re-ported as being satisfactory; the other two werenot satisfactory but refused further surgery. Twocases treated by radiotherapy were unimproved, aswere seven cases treated with vitamin E.The only failure in the group treated by excision
was due to an exacerbation of rheumatoid ar-thritis which had been quiescent for many years.The ten cases giving only fair results were due todelayed healing interfering with early movementsin four cases and severe capsular changes limitingextension in the remaining six cases.
My thanks are due to Mr. Rainsford Mowlem,whose technique of operation has been described,for his advice and criticism.
.BIBLIOGRAPHY
BRUNER, J. M. (I93I), 7. Bone Jt. Swg., 33, 221.BUNNELL, S. (1944), ' Surgery of the Hand,' Philadelphia.COOPER, A. (822), 'Treatise on Dislocations and Fractures of
the Joints,' London, p. 524.DUPUYTREN, G. (1834), Lancet, ii, 222.GARROD, A. E. (1893), St. Barts. Hosp. Rep., 29, I57.HORWITZ, T. (I942), Arch. Surg., 44, 687.KANI/V;L A B. KOCH, S. L., and MASON, M. L. (1929),
Surg. Gyn. Ob.t., 48, 145.
KING, R. A. (I949), J. Bone Jt. Surg., 31, 443.LUND, M. (x941), Acta. Psychiat. Neurol., x6, 465.MEYERDING, H. W., BLACK, J. R., and BRODERS, A. C.
(x944), Surg. Gyn. Obst., 72, 582.NIEDERLAND, W. (I933), Zbl. Chir., 60, 985. -SKOOG, T. (1948), Acta. Chir. Scand., 46, Supplement 139.STEINBERG C. (r947), N Y St. J. Mled. 47, x679.
H1
Protected by copyright.
on February 25, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.311.463 on 1 S
eptember 1951. D
ownloaded from