Embed Size (px)
Citation preview

Journal of Medical Genetics 1988, 25, 463-472
Dysmorphic syndromes with demonstrablebiochemical abnormalitiesP T CLAYTON AND ELIZABETH THOMPSONFrom the Departments of Child Health and Clinical Genetics, Institute of Child Health, London WC]N IEH.
SUMMARY Many inborn errors of metabolism are associated with dysmorphic manifestations. Inthis review, we have attempted to correlate the dysmorphic features with the underlyingmetabolic defect or its consequences. Most of the defects which we have discussed affect thesynthesis or degradation of macromolecules (for example, collagen, elastin, bone mineral,proteoglycans, glycoproteins, and triglycerides). Such defects may affect either a single enzymeor multiple enzymes in specific organelles, such as lysosomes or peroxisomes, or they may affecthormonal control of synthesis and degradation. Examples are also included of defects affectingthe catabolism of simple molecules when accumulating metabolites have a secondary effect onmacromolecules, as in homocystinuria. In a number of instances, however, the correlationbetween the biochemical abnormality and the dysmorphic features are not understood.Ultimately, all dysmorphic syndromes will be attributable to a biochemical defect or its effects.The aim of this overview is to provide an insight into the relationship between the two at thepresent time.
The study of inborn errors of metabolism has madesubstantial contributions to our understanding ofbiochemistry. It is worthwhile, therefore, to con-sider whether we can learn anything about the bio-chemistry of morphogenesis and dysmorphogenesisfrom studies of those inborn errors which producedysmorphic features. The first conclusion to bedrawn from a survey of inborn errors' 2is that, as ageneral rule, dysmorphic manifestations can beexpected as a result of disorders which affect thesynthesis or early steps in the degradation of thelarge molecules which form the structural frame-work of cells and extracellular matrix. Many of thesemacromolecular reactions are under hormonalcontrol and therefore disorders affecting the syn-thesis and biological action of hormones may alsolead to dysmorphic features. Inborn errors affectingthe metabolism of simple molecules (for example,organic acidaemias) do not usually lead to dysmorphicfeatures unless there are secondary effects onmacromolecules.Major components of the extracellular matrix
include collagen, proteoglycans (95% polysaccharide,5% protein), glycoproteins, elastin, and bonemineral. The architecture of cells is determined bycell membranes and by intracellular structural pro-
Received for publication 5 December 1987.Accepted for publication 10 Decembcr 1987.
teins and also by their content of stored macro-molecules (for example, triglyceride in normaladipocytes or intralysosomal material in lysosomalstorage disorders). Cell membranes are composedlargely of phospholipids (phosphoglycerides, sphingo-myelin, and plasmalogens), glycolipids, and choles-terol. Disorders affecting the metabolism of some ofthe macromolecules listed above are well known;others have only recently been recognised.
Disorders of collagen and elastin metabolism
Collagen is the major fibrous element of skin, bone,tendon, and cartilage and is responsible for theirtensile strength. Bone contains mainly type I col-lagen whereas dermal collafen is approximately80% type I and 20% type III. Elastin is responsiblefor the elastic properties of the skin and of the wallsof blood vessels.
It is now generally accepted that defective syn-thesis of type I collagen can result in weakness of thebones with consequent fractures and deformity:osteogenesis imperfecta (01). A variety of muta-ions in the chains of type I collagen have beendescribed in autosomal dominant and recessiveforms of the disease.3 Type I collagen is a polymer,assembled from al(I) and a2(I) chains in the ratio of2:1. Sykes4 has suggested that mutant a chainswhich become included in the collagen molecule
463
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

P T Clayton and Elizabeth Thompson
may produce more severe phenotypic effects thanthose in which the mutation prevents the a chainfrom being incorporated into the collagen molecule.01 is not always caused by a mutation in one of thestructural genes for type I collagen (COLIAl andCOLIA2); another postulated cause is a recessivelyinherited defect in one of the enzymes required forcollagen production.5 Equally, defective synthesis oftype I collagen does not always produce osteogenesisimperfecta; it may produce severe joint laxity withmultiple dislocations and subluxations: Eblers-Danlos syndrome (EDS) type VII. The commonbiochemical feature in patients with EDS type VIIappears to be impaired removal of the aminoterminal N-propeptides from procollagen. Thedocumented defects include heterozygous structuralalterations of the proal(I) or proal(II) chains whichprevent cleavage of the abnormal chain by pro-collagen N-proteinase.('11 It is possible that asimilar clinical picture may be caused by deficiencyof the proteinase itself, inherited in an autosomalrecessive manner (McKusick 2254111).
Defective synthesis of type III collagen can reducethe tensile strength of the skin and joints and so thiscan also cause Ehlers-Danlos syndrome, in this casethe severe ecchymotic form (EDS type IV).'2 "3The synthesis of both type I and type III collagen
requires post-translational modification of the pro-collagen by conversion of lysine residues to hydroxy-lysine. Lysyl hydroxylase deficiency causes theautosomal recessive ocular-scoliotic form of EDS(type VI).13 14
Impaired synthesis or increased catabolism ofelastin reduces the elasticity of the skin and cantherefore produce cutis laxa. Anderson et al"S havedescribed an autosomal recessive form of cutis laxawith pulmonary emphysema associated with highserum activity of an elastase.'5
Cross links between individual collagen moleculesand between individual elastin molecules are forgedby lysyl oxidase, a copper dependent enzyme. In Xlinked cutis laxa (previously called EDS type IX),Byers et all6 reported low levels of lysyl oxidaseactivity and low serum copper and caeruloplasminlevels. Clinical features included moderate skinlaxity, hyperextensible skin, mild joint laxity, dilata-tions of the urinary tract, and inguinal herniae. InMenkes syndrome,' the disordered copper metabol-ism produces severe disruption of the elastic tissueof blood vessels and emphysema and bladderdiverticula have also been described. Abnormalitiesof skin elastin are detectable on electron micro-scopy: these ultimately lead to cutis laxa and mayperhaps contribute to the pudgy cheeks. In cartilage,irregularity of collagen fibrils has been describedand the bones are osteoporotic. The most striking
dysmorphic feature of Menkes syndrome, the steelyhair, is not attributable to lysyl oxidase deficiency.Danks has suggested that it may be the result ofdeficiency of another copper dependent enzyme thatcross links keratin by forming disulphide bonds.'
In cystathionine synthetase deficiency, accumu-lation of homocysteine impairs the formation of thecross links between lysyl and hydroxylysyl residuesof collagen and this is thought to be responsible forsome of the dysmorphic features, for example,osteoporosis and joint laxity. However, the highlycharacteristic lens dislocation is more likely to resultfrom disruption of the disulphide bonds of anotherfibrous protein as a result of homocysteine accumu-lation. Lens dislocation also occurs in sulphiteoxidase deficiency2 and molybdenum cofactordeficiency'7; in these conditions it is thought to bethe sulphite accumulation which disrupts thedisulphide bonds.
Disorders affecting the bone mineral
Failure to deposit bone mineral in the matrix ofosteoid and epiphyseal cartilage leads to rickets,with beading of the costrochondral junctions, bow-ing of the legs, and widening of the metaphyses ofthe long bones. Such changes can be the result ofinborn errors affecting renal tubular reabsorption ofphosphate, conversion of vitamin D to activemetabolites, or end organ sensitivity to thesemetabolites. ' Failure of mineralisation also occurs inhypophosphatasia,' which is characterised by lowactivities of alkaline phosphatase in bone and serumand by increased urinary excretion of phosphoetha-nolamine and inorganic pyrophosphate. The failureof mineralisation is probably caused by the reducedactivity of alkaline phosphatase in the bone. Thisprevents hydrolysis of pyrophosphate and otherphosphate esters. Hence, the accumulation of in-organic phosphate in matrix vesicles, which wouldnormally lead to the deposition of bone mineral, isimpaired. The dysmorphic features of hypophospha-tasia include not only the signs of rickets but alsoskin dimples and, in some cases, gross craniofacialdysmorphism as a result of premature synostosis ofskull bones. Synostosis occurs because, in theuncalcified osteoid, the fibrous septa that normallyseparate the individual bones fail to develop. Thesame phenomenon occurs in acrocephalosyndactyly,but the cause of delayed calcification of osteoid inApert and related syndromes is not known.Normal bone growth involves remodelling and
therefore catabolism of bone mineral. This process,as well as mobilisation of calcium to restore theplasma calcium concentration, is controlled byparathormone. Pseudohypoparathyroidism' is caused
464
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

Dysmorphic syndromes with demonstrable biochemical abnormalities
by target organ resistance to parathormone. Hypo-calcaemia is usual and there is a reduced urinaryexcretion of cyclic AMP in response to parathormone.Most patients are of short stature and have a roundface with a depressed nasal bridge and multiplediscrete abnormalities in the bones, including shortmetacarpals and metatarsals. The latter defects ariseas a result of premature closure of the epiphysespreceded by a decrease in longitudinal growth.Reduced bone growth is a predictable consequenceof impaired remodelling, but why it should affect thefourth and fifth digits and spare the others is difficultto explain.
Disorders affecting subcutaneous fat
Insulin stimulates synthesis of triglyceride and in-hibits lipolysis in adipocytes. A reduction in theamount of fat in the subcutaneous tissues is re-sponsible for some of the dysmorphic features inleprechaunism, generalised lipodystrophy, and par-tial lipodystrophy. Elsas et all8 have shown thatleprechaunism can occur as the result of a deficiencyof high affinity insulin receptors. In generalisedlipodystrophy, hyperinsulinism and insulin resis-tance may also be found but the cause of thesyndrome is not fully understood. Partial lipo-dystrophy has been recorded in association withfamilial deficiency of the C3 component of comple-ment and loss of adipose tissue may have animmunological basis in this instance.19
Lysosomal storage disorders' 2 20
The lysosomes are the site of catabolism of manystructural macromolecules, including glycosamino-glycans (mucopolysaccharides) derived from proteo-glycans, glycoproteins, sphingolipids (sphingo-myelin and ceramide), and glyco(sphingo)lipids (forexample, gangliosides). In some lysosomal storagedisorders, catabolism of only one type of compoundis impaired, for example, the glycosaminoglycandermatan sulphate in Maroteaux-Lamy disease (arylsulphatase B deficiency). However, some lysosomalenzymes catalyse the hydrolysis of more than onetype of macromolecule and so, for example, ininfantile GM1 gangliosidosis, deficiency of 0i galac-tosidase A leads to reduced catabolism of gang-liosides, glycosaminoglycans, and glycoproteins. Inother lysosomal storage disorders the primary defectleads to reduced activity of more than one enzyme(for example, multiple sulphatase deficiency, I celldisease). Finally, the distension of lysosomes withundigested macromolecules may lead to secondaryeffects on the catabolism of other macromolecules.Nevertheless, it is possible to dissect out the majoreffects of the primary defects.
The effect of a block of sphingolipid or glyco-sphingolipid catabolism depends upon the localisa-tion and function of the lipid. Galactocerebrosidesand their sulphates are lipids of the central nervoussystem and so impaired degradation leads to neuro-logical disease rather than dysmorphic features (forexample, Krabbe disease, metachromatic leuco-dystrophy). Gangliosides are also found mainly inthe CNS and in GM2 gangliosidoses (Tay Sachsdisease and Sandhoff disease) CNS symptoms pre-dominate. However, accumulation of gangliosidesand gliosis can lead to macrocephaly and, inaddition, many patients have doll-like facies withpale translucent skin, long eyelashes, fine hair, anddelicate pink colouring. Whether these dysmorphicfeatures are caused by ganglioside accumulation isuncertain; histochemical techniques reveal onlylimited lipid storage outside the CNS. GM1 gang-liosidosis can occur as a neurological disease withoutobvious dysmorphic features but this is not the casefor the infantile form (see below). Glucocerebrosides,neutral glycosphingolipids, sphingomyelin, andceramide are widely distributed outside the CNS asconstituents of cell membranes. Accumulation ofglucocerebrosides can produce bony deformity(Gaucher disease), accumulation of neutral glyco-sphingolipids (in particular trihexosylceramide) pro-duces corneal dystrophy, cataracts, and angiokera-toma corporis diffusum (Fabry disease), and accumu-lation of ceramide causes a tissue reaction whichleads to swollen joints and periarticular nodules(Farber disease).The effect of a block in the pathway for degrada-
tion of one of the glycosaminoglycans depends uponthe function of the parent proteoglycan. Proteogly-cans containing keratan sulphate are importantconstituents of the extracellular matrix of cartilageand the cornea. Remodelling of bones and jointsduring growth is dependent upon turnover of thecartilage matrix. Impaired degradation of keratansulphate in Morquio disease (types A and B) isassociated with severe dysostosis multiplex, growthretardation, joint laxity, and corneal clouding.
Proteoglycans containing dermatan sulphate areimportant constituents of the extracellular matrix ofinterstitial connective tissue. Impaired degradationof dermatan sulphate in Maroteaux-Lamy disease,Hurler disease, and Hunter disease is associatedwith thickening of subcutaneous tissues producing acoarse facies, thick lips and gum ridges, and herniae.Increased stiffness of ligaments and other connec-tive tissues leads to deformities of joints such as clawhand. Dermatan sulphate is not a major componentof cartilage and yet chondrocytes do becomevacuolated and irregularly arranged in the growingareas of bones and this is probably the basis of the
465
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

P T Clayton and Elizabeth Thompson
dysostosis multiplex (which is milder than that ofMorquio disease). In the cornea, dermatan sulphateoccurs as a mixed chondroitin-dermatan sulphateproteoglycan. Degradation of this proteoglycanrequires a-L-iduronidase and arylsulphatase B but ismuch less dependent upon iduronate sulphatase,either because of undersulphation or because of aneasier bypass of the block by hyaluronidase. Hence,corneal clouding occurs in Hurler disease (iduroni-dase deficiency) and Maroteaux-Lamy disease (aryl-sulphatase B deficiency), but not in Hunter disease(iduronate sulphatase deficiency).Proteoglycans containing heparan sulphate are
not components of the extracellular matrix; they arecomponents of cell membranes including the limit-ing membranes of synaptosomes in the CNS. Im-paired degradation of heparan sulphate is thecommon feature in patients with Sanfilippo diseasetypes A to D. These disorders are characterised bymental retardation and regression but only milddysmorphic features (coarse facies and dysostosismultiplex).
Glycoproteins occur widely within cells, on thecell surface, and extracellularly both within andwithout the CNS. The effects of impaired glycopro-tein catabolism can be identified in a mannosidosisand aspartylglycosaminuria. (In other glyco-proteinoses there is also impaired degradation ofglycolipids and perhaps glycosaminoglycans.) Inboth a mannosidosis and aspartylglycosaminuria,facial coarsening, herniae, opacities of the lens orcornea or both, and a variable degree of dysostosismultiplex occur. Thus, the dysmorphic effects ofimpaired glycoprotein catabolism appear to besimilar to those of impaired dermatan sulphatecatabolism. In fucosidosis type 2 and sialidosis type2 (juvenile type'), these dysmorphic features occurtogether with angiokeratomata, similar to thoseseen in Fabry disease. In fucosidosis this can beexplained by the defect in glycolipid catabolismwhich leads to the accumulation of a pentaglycosyl-ceramide which is closely related to the glycosyl-ceramides that accumulate in Fabry disease. Earlyreports of human I mannosidosis21 suggest thatcoarse features and skeletal abnormalities do notoccur, but angiokeratomata can. This is verydifficult to explain as the defect should affectglycoprotein degradation rather than glycolipid de-gradation! One patient who was deficient in both ,mannosidase and heparan-N-sulphatase (the en-zyme which is deficient in Sanfilippo disease type A)did have both coarse features and bonyabnormalities.22
In infantile GM1 gangliosidosis, catabolism ofgangliosides, keratan sulphate, and glycoproteinsare all severely impaired as a result of a defect of PI
galactosidase A. Hence, severe neurological diseasecoexists with major skeletal abnormalities andcoarse features. In I cell disease and pseudo-Hurlerpolydystrophy, there is a defect in the post-trans-lational modification of a number of lysosomal acidhydrolases. The mannose residues of these glyco-protein enzymes are not phosphorylated normally,which impairs translocation into the lysosomes andleads to further glycosylation of the enzymes. Thephenotypic expression of these disorders appears tobe affected by the fact that impaired lysosomalfunction, as indicated by their distension (presumablywith undigested macromolecules), occurs largely inconnective tissue cells. The dysmorphic featuresresemble those seen in disorders of dermatansulphate or glycoprotein degradation, but there is nocorneal clouding. In multiple sulphatase deficiencythere is impaired catabolism of keratan sulphate anddermatan sulphate and consequent dysostosis multi-plex and coarse features. In addition, however,there is ichthyosis as a result of steroid sulphatasedeficiency.The above survey indicates that in the lysosomal
storage disorders, dysmorphic features occur largelyas a result of impaired turnover of structuralmacromolecules within cells and in the extracellularmatrix. This results in progressive distortion of thetissue and may provoke a tissue reaction such asgranuloma formation or gliosis. In many cases thedysmorphic features are not present at birth butbecome evident during childhood.The investigations which may be helpful in a
patient who has or is developing coarse facialfeatures are shown in table 1. There are a number ofinborn errors of metabolism affecting either thesynthesis of thyroid hormones or their effect ontarget organs' and the hypothyroidism which resultsmay produce coarsening of facial features, beakingof lumbar vertebrae, and epiphyseal dysgenesis;thyroid hormones are essential for the normalturnover of the extracellular matrix.
Peroxisomal disorders
Peroxisomes are round or ovoid subcellularorganelles slightly smaller than mitochondria andwith a single limiting membrane and no cristae.They can be shown histochemically by making use oftheir peroxidase activity. Over the last few years thenumber of genetic disorders attributable to malfunc-tioning of peroxisomal enzyme systems has beenincreasing steadily.2--36 In peroxisomal disorders,the dysmorphic features are well established at birthand thus the biochemical abnormalities must beexerting their influence in utero. Peroxisomal de-fects vary from those in which a single peroxisomal
466
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

Dysmorphic syndromes with demonstrable biochemical abnormalities
enzyme is deficient to those in which the wholeorganelle is absent. Thus, it is possible to build up apicture of the consequences of a single metabolicblock and of combinations of interrupted pathways.The investigations which can be used to define thenature of a peroxisomal disorder are summarised intable 2. Some of the reactions occurring within theperoxisome are concerned with the catabolism ofsmall molecules, for example, hydrogen peroxide23and glyoxylate,24 and inborn errors of metabolism
TABLE 1 Investigations which may aid in the diagnosis of apatient who has or is developing coarse facial features.
UrineGlycosaminoglycansOligosaccharidesN-AspartylglycosamineSialiac acidBloodThyroid function testsWhite cell histochemistry (vacuoles and metachromatic granules)I cell screen (eg plasma aryl sulphatase A)White cell enzymes (as indicated by above results)
a-L-lduronidase (Hurler, Scheie)Sulphoiduronate sulphatase (Hunter)Aryl sulphatase B (Maroteaux-Lamy)Heparan N-sulphatase (Sanfilippo A)N-Acetyl-a-glucosaminidase (Sanfilippo B)Acetyl CoA: a-glucosaminide N-acctyltransfcrase (Sanfilippo C)N-Acetylglucosamine 6-sulphate sulphatase (Sanfilippo D)13 Glucuronidase (Sly)3 Galactosidase A (GMI gangliosidosis. variaint Morquio)o Mannosidase (mannosidosis)a-L-Fucosidase (fucosidosis)I-Aspartamido-1-N-acetylglucosaminc amidohydrolasc
(aspartylglycosaminuria)a Neuraminidase (sialidosis)
X ravsSkeletal survey for dysostosis multiplex
TABLE 2 Investigations used to delineate the nature of a
peroxisomopathy.
Demonstration of reduced numbers of peroxisomesElectron microscopy of liver biopsyHistochemistry of liver biopsy (staining for catalase activity)Fibroblast catalase latency test (release of catalase using digitonin)
Peroxisome morphologyElectron microscopy of liver biopsy
Demonstration of impaired peroxisomal 13 oxidationPlasma very long chain fatty acids (VLCFA)C27 bile acids in bile plasma or urineFibroblast oxidation of 14C-VLCFA
Localisation of the defect in peroxisomal oxidationAbsence of a peroxisomal oxidation protein in the liver (immunoblotting)Fibroblast acyl-CoA oxidase activity?C-27 bile acid pattern
Demonstration of impaired plasmalogen synthesisErythrocyte plasmalogensFibroblast/platelet dihydroxyacetonephosphate acyl transferaseFibroblast de novo plasmalogen synthesis (hexadecanol incorporation into
plasmalogens)Demonstration of other biochemical abnormalitiesPlasma phytanic acid/oxidation of phytanic acid by fibroblastsUrinary pipecolic acidHepatic D amino acid oxidase activityHepatic L-a-hydroxy acid oxidase activity
affecting these reactions do not produce dysmorphicfeatures. However, peroxisomes are also responsiblefor synthesis of certain phospholipids (plasmalogens)and for the i oxidation of fatty acids. Plasmalogensare important constituents of cell membranes andthe acetyl-CoA generated by peroxisomal j3 oxidationis used in the synthesis of cholesterol and for othersyntheses involving acetylation reactions. 25The peroxisomal pathway for 0 oxidation of
coenzyme A esters of fatty acids involves, sequen-tially, acyl-CoA oxidase, a bifunctional protein withenoyl-CoA hydratase and 3-hydroxyacyl-CoAoxidase activities, and 3-oxoacyl-CoA thiolase. Inaddition, oxidation of very long chain fatty acids(VLCFA) requires a VLCFA-CoA synthetase. De-ficiency of the peroxisomal VLCFA-CoA synthetaseproduces X linked adrenoleucodystrophy and itsvariants.26 27 These patients have no dysmorphicfeatures despite the fact that accumulation ofVLCFA can be shown in the fetus; adrenal atrophyand demyelination first produce symptoms at sevento eight years. Patients with a deficiency of one ofthe PI oxidation enzymes (acyl-CoA oxidase28 or3-oxoacyl-CoA thiolase29-31 ) do not have strikingdysmorphic features either; the mild dysmorphicfeatures can probably be attributed to the severehypotonia of prenatal onset (expressionless face,tented mouth, high arched palate, bell shaped chest,single transverse palmar creases) and delayedosseous maturation (large fontanelle). However,there are developmental anomalies in these patients.The hypotonia is in part the result of abnormalitiesof the cerebellum which shows demyelination andgliosis but also neuronal heterotopias, indicatingdefective neuronal migration. Renal cortical cystsmay also be present. Thus, deficiency of a singleperoxisomal i oxidation enzyme can cause abnor-malities of organogenesis.
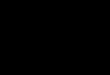
Defects in the peroxisomal pathway for thesynthesis of either phospholipids (plasmalogens)have been described in both rhizomelic chondrodys-plasia Bunctata32 and Conradi-Hunermann syn-drome 3 The enzyme catalysing the first step,dihydroxyacetone phosphate acyl transferase(DHAPAT), is deficient in skin fibroblasts in bothconditions. Thus, it is tempting to postulate thatdeficient plasmalogen synthesis can give rise topunctate epiphyseal mineralisation with associatedlimb shortening and joint contractures, a prominentforehead, a low, flat nasal bridge, a short nose withanteverted nostrils, malar hypoplasia, cataracts, ashort neck, and ichthyosis (fig 1). In rhizomelicchondrodysplasia punctata, which is inherited as anautosomal recessive trait, all cells express the defectso that the abnormalities are severe and symmetrical.In the X linked dominant form of Conradi-
467
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

P T Clayton and Elizabeth Thompson
FIG 1 Craniofacial dysmorphismin two infants with reduced activityof dihydroxyacetonephosphateacyl transferase but normal
* peroxisomal A3 oxidation.(a) Patient 1 has X linkeddominant Conradi-Hunermann
~. syndrome and (b) patient 2 hasI..: rhizomelic chondrodysplasia
punctata.U
(diI/) I
Hunermann syndrome the patchy nature of the skinlesions and the asymmetry of the skeletal changescould be explained by Lyonisation.34 The cranio-facial features in rhizomelic chondrodysplasiapunctata are also affected by the extent to whichCNS involvement leads to microcephaly.
Patients with Zellweger syndrome, 'mild Zell-weger variants', and patients with infantile Refsumdisease have a defect in the biogenesis of peroxi-somes; the organelles are absent or virtually absentfrom all cells. Cell fusion studies indicate that thedefect in infantile Refsum disease may be at thesame gene locus as the defect in Zellweger syn-drome.35 As a result of the absence of peroxisomes,the activity of DHAPAT (an enzyme which isnormally bound to the peroxisomal membrane) isdepressed and peroxisomal P oxidation is impaired.The clinical features reflect to a considerable extenta summation of those found in defects of peroxi-somal I6 oxidation and those found in patients withchondrodysplasia punctata, but there is a widespectrum in the expression of all of the features.Patients with classical Zellweger syndrome havevery obvious dysmorphic features; the mild variantswho survive into the second decade of life and thosewith infantile Refsum disease may have very subtledysmorphology (fig 2). Whether the variability is areflection of the ability of some patients to assemblea few peroxisomes or whether the effect of absentperoxisomes can be modified by other genetic orenvironmental factors remains uncertain.
Patients with neonatal adrenoleucodystrophy also
have a defect in the biogenesis of peroxisomes. Cellfusion studies indicate that this is not identical to thedefect in Zellweger patients. Kelley et a137 havesuggested that the effect on peroxisomal P oxidationmay be different; whereas Zellweger fibroblastsshow marked accumulation of saturated very longchain fatty acids and some accumulation of unsatu-rated VLCFA, neonatal ALD fibroblasts accumulateless saturated VLCFA and considerably less unsatu-rated VLCFA. A similar phenomenon is seen in theplasma of these patients. This fits to some extentwith the postulated effects of impaired peroxisomal
oxidation; neonatal ALD patients are less likelythan Zellweger patients to show a retarded bone ageand large fontanelle or cystic kidneys. However,both groups of patients show marked truncal hypo-tonia and defects of neuronal migration, particularlyin the region of the brainstem and cerebellum. Theimpairment of plasmalogen synthesis may also beless marked in neonatal ALD than in Zellwegersyndrome. This could explain the absence ofchondral calcification and less obvious craniofacialdysmorphism in neonatal ALD.
Although in the above discussion we have drawnattention to the association between reduced plas-malogen synthesis and punctate epiphyseal calcifica-tion, Gilbert et a138 have listed a number of otherconditions in which such calcification can occur, butin which impaired plasmalogen synthesis has notbeen found, for example, warfarin embryopathy.We could add to this list f glucuronidase deficiency(R M Winter, P T Clayton, unpublished obser-
468
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

Dysmorphic syndromes with demonstrable biochemical abnormalities
I ^~ ~~~~~~~~~e .AA..*, rv 1-
()
I(c)
(d)FIG 2 The spectrum of craniofacial dysmorphism in patients with absent peroxisomes. Patients I (a) and 2 (b) had classicalZellweger syndrome and patient 3 (c) had most ofthe features of classical ZS (see reference 36, patient A P) but has moresubtle dysmorphic features. Patient 4 (d) and his brother have many features ofZS but have survived beyond the age oftwoand 10 years respectively ('mild Zellweger variants'). (e) PatientS (CB-6) had infantile Refsum disease.
vations), idiopathic neonatal hepatitis (E Naughten,1987, personal communication), and a defect ofperoxisomal Pi oxidation (P T Clayton et al, un-published data). One possible unifying explanationwould be haemorrhage into the cartilage in uteroperhaps because of hypoprothrombinaemia; hypo-
prothrombinaemia could result from liver disease,from peroxisomal dysfunction, or from maternalwarfarin therapy. Punctate epiphyseal calcificationcan also occur when the normal actions of thyroidhormone are prevented, for example, in familialresistance to thyroid hormone.'
469
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

P T Clayton and Elizabeth Thompson
A disorder of cholesterol and nonsterol isoprenesynthesis: mevalonic aciduria39 40
Cholesterol is an important constituent of cellmembranes. The body's needs are supplied in partby the diet and partly by synthesis from acetyl-CoAvia 3-hydroxy-3-methylglutaryl-CoA and mevalonicacid. This pathway also supplies cells with nonsterolisoprenes, including ubiquinone and haem A (com-ponents of the respiratory chain), dolichol (whichparticipates in the synthesis of glycoproteins), andisopentenyl adenine (a precursor of isopentenyltRNA which participates in DNA replication).The first patient described with mevalonate
kinase deficiency had microcephaly, cataracts, alarge anterior and posterior fontanelle, and widesagittal and metopic sutures. He was dolichocephalicand had a triangular face, downward slantingpalpebral fissures, and large, posteriorly rotatedears. He showed severe failure to thrive and washypotonic but hyperreflexic. Radiology revealed aseverely retarded bone age and a CT scan showedgeneralised atrophy of the brain. It is not possible tosay whether the dysmorphic features in this patientwere a consequence of impaired synthesis ofcholesterol and nonsterol isoprenes.
Disorders of pathways of metabolism of simplemolecules which do produce dysmorphic features
3-Hydroxyisobutyryl CoA deacylase deficiency4l isan inborn error which only affects one step in thecatabolism of an amino acid (valine). Nevertheless,the one reported case of this disorder had multiplecongenital malformations. Details of the dysmor-phic facial features were not given, but the otherabnormalities included multiple vertebral anoma-lies, tetralogy of Fallot, and agenesis of the corpuscallosum. It has been postulated that the inbornerror of valine metabolism leads to the accumulationof ethylacrylyl-CoA, that this compound can formconjugates with compounds containing free sulphy-dryl groups, and that this is the cause of themalformations. Methylacrylyl esters have been shownto be potent teratogens in the rat.42Nyhan and Sakati4" have suggested that
patients with methylmalonic acidaemia all have asimilar facial appearance; this is not our impressionfrom the 15 cases seen at The Hospital for SickChildren, Great Ormond Street. Some patients witha deficiency of the pyruvate dehydrogenase complexhave had a high bossed forehead, anteverted nose,large ears, and dislocated hips with external rotationof the legs.40The dysmorphic features of cystathionine syn-
thetase deficiency, sulphite oxidase deficiency, and
molybdenum cofactor deficiency have already beenmentioned. Thus, we have described a number ofexceptions to the general rule that defects in thecatabolism of small molecules do not producedysmorphic features. Accumulating metabolites canoften affect important macromolecules in the fetus ifthey are not dealt with by the placenta and maternalmetabolism. A graphic illustration of this is seen inphenylketonuria. A fetus with (homozygous) phenyl-ketonuria born to a normal (heterozygous) motherhas no dysmorphic features or congenital malforma-ions because the mother rapidly metabolises theexcess phenylalanine and metabolites from thefetus. However, a non-phenylketonuric (heterozy-gous) fetus born to a mother with (homozygous)phenylketonuria can have microcephaly, a faciessimilar to the fetal alcohol syndrome, and congenitalheart disease as a result of the toxic effects ofmaternal metabolites on the fetus.43
Dysmorphic syndromes with biochemicalabnormalities in which the precise metabolic defect isunknown
Some patients with glutaric aciduria type II havedysmorphic features. The first such patient4"1 44 hada large head, a large fontanelle, and widely spacedsutures. The ears were low set, the palpebral fissuressmall, and the inner canthal distance increased. Theforehead was high and the nasal bridge low. Thenose was short, the nares upturned, and the phil-trum long. The hands showed bilateral simiancreases and dysplastic nails. The infant had poly-cystic kidneys. Lehnert et a145 and Bohm et a146described a patient with wide set eyes, prominentepicanthic folds, large, low set ears, a flattenednose, and a receding chin. The facial features of hissib were not commented upon, but both brothershad warty dysplasia of the cerebral cortex, poly-cystic kidneys, and intrahepatic biliary hypoplasia.The pattern of organic acids excreted in glutaricaciduria type II suggests that the defect affectsflavine adenine dinucleotide (FAD) containingenzymes. In the non-dysmorphic patients, accu-mulation of sarcosine suggested a defect affect-ing the transfer of electrons from mitochondrialFAD dependent dehydrogenases to coenzyme Q inthe respiratory chain. The cause of dysmorphic GAII has not yet been fully elucidated. Sarcosineaccumulation does not appear to occur. Thus, it ispossible that the defect in this case affects glutarylCoA and acyl CoA oxidases in the peroxisomesrather than the corresponding dehydrogenases inthe mitochondria. Peroxisomal oxidases appear tobe FAD dependent but it is thought that theelectrons from the FADH2 are transferred tomolecular oxygen (producing hydrogen peroxide)
470
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

Dysmorphic syndromes with demonstrable biochemical abnormalities
rather than to coenzyme Q.47 There are certainlysimilarities between the dysmorphic features of GAII and those of the peroxisomal defects.
Recently, Patton et a148 have described raisedplasma and urinary 2-oxoglutarate levels in threepatients with the DOOR syndrome (deafness,onycho-osteodystrophy, and mental retardation).Further studies will be needed before we can start toexplain the relationship between the biochemicalabnormality and the dysmorphic features in thisinstance.The cause of hypercalcaemia in Williams syn-
drome also remains obscure; detailed studies havefailed to show any definite abnormality of vitamin Dmetabolism49 but impaired calcitonin secretion hasbeen reported in five children.5t
Future research
It is clear that we have much to learn about thebiochemistry of dysmorphism. The reactions whichare likely to produce the most severe dysmorphicfeatures (and may prove the most difficult to study)are those relating to the metabolism and mode ofaction of the substances that induce organogenesisin the embryo, the morphogens. The first vertebratemorphogen was identified in 1987: all-trans-retinoicacid is produced in posterior limb bud tissue in thechick and its concentration gradient induces thecorrect sequence of digits in the developing limb.5'Retinoic acid is a hydrophobic compound of re-latively low molecular mass, characteristics whichmay allow it to pass from cell to cell without gapjunctions or specialised receptors.52 It may beworthwhile to investigate the mrtabolism of thistype of compound in patients with gross limbreduction defects.
Identification of an inborn error by metabolicstudies sometimes makes it possible to localise thegene defect. Take, for example, hypophosphatasia.It is reasonable to assume that this disorder is causedby a mutation in the structural gene for alkalinephosphatase. Recently, the structural gene for theliver/bone/kidney form of alkaline phosphatase(ALPL) has been mapped to chromosomelp34-p36-1.53 Since the ALPL cDNA detects arestriction fragment length polymorphism with therestriction endonuclease Bcll, it will be possible toundertake linkage studies in families with morethan one child with hypophosphatasia to test thehypothesis that the mutation is at this site.
We thank Drs J V Leonard, D G Atherton, D BGrant, J Wilson, and E Brett for allowing us topublish photographs of the patients and we thankthe families themselves. We are grateful to Profes-sor Marcus Pembrey for his helpful comments.
Note added in proof
Further clues concerning the link between hypo-prothrombinaemia and stippled epiphyses haveemerged from studies on a boy with a coagulo?athyand the phenotype of warfarin embryopathy.5 It isnow well established that glutaric aciduria type II isusually the result of an inherited defect of electrontransport flavoprotein (ETF) or ETF:ubiquinoneoxidoreductase but that the dysmorphic patients donot have this defect.55
References
Stanbury JB, Wyngaarden JB, Fredrickson DS, Goldstein JL,Brown MS. eds. The metabolic basis of inherited disease. 5th ed.New York: McGraw-Hill, 1983.
2 Benson PF, Fensom AH. Genetic biochemical disorders. Oxford:Oxford University Press, 1985.Cheah KSE. Collagen genes and inherited connective tissuedisease. Biochem J 1985;229:287-303.Sykes B. The molecular genetics of collagen. BioEssays 1985;3:112-7.Aitchison K, Ogilvie D, Honeyman M, Thompson E, Sykes B.Homozygous osteogenesis imperfecta unlinked to collagen Igenes. Hum Genet 1988;78:233-6.
" Steinmann B, Tuderman L, Peltonen L, Martin GR, McKusickVA, Prockop DJ. Evidence for a structural mutation ofprocollagen type I in a patient with Ehlers-Danlos syndrometype VII. J Biol Chem 1980;255:8887-93.
7 Prockop DJ, Kivirikko KI. Heritable diseases of collagen. NEngl J Med 1984;311:376-86.Eyre DR, Shapiro FD, Aldridge JF. A heterozygous collagendefect in a variant of Ehlers-Danlos syndrome type VII. J BiolChem 1985;260:11322-9.Cole WG, Chan D, Chambers GW, Walker ID, Bateman JF.Deletion of 24 amino acids from the pro-al(I) chain of type Iprocollagen in a patient with Ehlers-Danlos syndrome type VII.J Biol Chem 1986;261:5496-503.
II Cole WG, Evans R, Sillence DO. The clinical features ofEhlers-Danlos syndrome type VII due to a deletion of 24 aminoacids from the pro al(I) chain of type I procollagen. J MedGenet 1987;24:698-701.McKusick VA. Mendelian inheritance in man. Catalogs ofautosomal dominant, autosomal recessive and X-linked pheno-types. (No 22541). 7th ed. Baltimore: Johns Hopkins UniversityPress, 1986.
12 Pope FM, Martin GR, Lichtenstein JR, et al. Patients withEhlers Danlos syndrome type IV lack type III collagen. ProcNatl Acad Sci USA 1975;72:1314-7.
13 Pope FM, Nicholls AC, Dorling J, Webb J. Molecular abnorma-lities of collagen: a review. J R Soc Med 1983;76:1050-62.
14 Pinnell SR, Krane SM, Kenzora JE, Glimcher MJ. Heritabledisorder with hydroxylysine-deficient collagen. Hydroxylysine-deficient collagen disease. N Engl J Med 1972;286:1013-20.
'1 Anderson LL, Oikarinen AJ, Ryhanen L, Anderson CE, UittoJ. Characterisation and partial purification of a neutral proteasefrom the serum of a patient with autosomal recessive pulmonaryemphysema and cutis laxa. J Lab Clin Med 1985;105:537-46.
16 Byers PH, Siegel RC, Holbrook KA, Narayanan AS, BornsteinP, Hall JG. X-linked cutis laxa. Defective cross-link formationin collagen due to decreased lysyl oxidase activity. N Engl J Med1980;303:61-5.
'7 Wadman SK, Duran M, Beemer FA, et al. Absence of hepaticmolybdenum cofactor: an inborn error of metabolism leading toa combined deficiency of sulphite oxidase and xanthine dehyd-rogenase. J Inherited Metab Dis 1983;6(suppl 1):78-83.
Ix Elsas LU, Endo F, Strumlauf E, Elders J, Priest JH. Lep-
471
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from

P T Clayton and Elizabeth Thompson
rechaunism: an inherited defcct in a high-affinity insulinreceptor. Am J Hum Genet 1985;37:73-88.
19 McLcan RH, Hoefnagcl D. Partial lipodystrophy and familialC3 deficiency. Hum Hered 1980:30:149-54.
201 Watts RWE, Gibbs DA. Lysosomal storage diseases. London:Taylor and Francis, 1986.
21 Coopcr A, Sardarwalla IB, Roberts MM. Human -
mannosidasc dcficicncy. N Engl J Med 1986;315:1231.22 Wenger DA, Sujansky E, Fennessey PV, Thompson JN.
Human ,B-mannosidasc deficiency. N Enigi J Med 1986;315:1201-5.
23 Schutgens RBH, Heymans HSA, Wanders RJA, van den BoschH, Tager JM. Peroxisomal disorders: a newly recognised group
of genetic diseases. Eur J Pediatr 1986;144:430-40.24 Danpure CJ, Jennings PR, Watts RWE. Enzymological diagno-
sis of primary hyperoxaluria type 1 by measurement of hepaticalanine:glyoxylate aminotransferase activity. Lancet 1987;i:289-91.
25 Lazarow PB. The rolc of peroxisomes in mammalian ccllularmetabolism. J Inherited Metab Dis 1987;10(suppl 1):11-22.
26 Wanders RJA, van Roermund CWT, van Wijland MJA, et al.Peroxisomal fatty acid ,B-oxidation in relation to the accumula-tion of very long chain fatty acids in cultured skin fibroblastsfrom patients with Zellweger syndrome and other peroxisomaldisorders. J Clin Invest 1987;80:1778-83.
27 Moser HW, Moser AE, Singh I, O'Neill BP. Adrenoleukody-strophy: survey of 303 cases: biochemistry, diagnosis andtherapy. Ann Neurol 1984:16:628-41.
28 Poll-The BT, Roels F, Ogier F, et al. Pseudo-neonatal adreno-leukodystrophy: a new peroxisomal disorder with giant peroxi-somes and a specific defect of acyl-CoA oxidase. Am J HumGenet (in press).
29 Goldfischer S, Collins J, Rapin 1, et al. Pseudo-Zellwegersyndrome: deficiencies in sevcral peroxisomal oxidative activi-ties. J Pediatr 1986;108:25-32.
3" Schram AW, Goldfischer S, Van Roermund CWT, et al. Humanperoxisomal 3-oxoacyl-cocnzyme A thiolase deficiency. ProcNatl Acad Sci USA 1987;84:2494-6.
-' Clayton PT, Lake BD, Hjelm M, et al. Bile acid analyses inpseudo-Zellweger syndrome: clucs to the defect in peroxisomalfl-oxidation. J Inherited Metab Dis 1988;11(suppl 2) (in press).
32 Hcymans HSA, Oorthuys JWE, Nelck G, Wanders RJA,Schutgens RBH. Rhizomelic chondrodysplasia punctata:another peroxisomal disorder. N Eng! J Med 1985;313:187-8.
33 Holmes RD, Wilson GN, Hajra AK. Peroxisomal enzymedeficicncy in the Conradi-Hunermann form of chondrodysplasiapunctata. N Enigl J Med 1987;316:1608.
34 Mueller RF, Crowlc PM, Jones RAK, Davison BCC. X-linkeddominant chondrodysplasia punctata: a case report and familystudies. Am J Med Genet 1985;20:137-44.
35 Wanders RJA, Saclman D, Heymans HSA, et al. Geneticrelation between the Zellwegcr syndrome, infantile Refsum'sdiseasc and rhizomelic chondrodysplasia punctata. N Enigl JMed 1986;314:787-8.
31 Clayton PT, Lake BD, Hall NA, Shortland DB, Carruthers RA,Lawson AM. Plasma bile acids in paticnts with peroxisomaldysfunction syndromes: analysis by capillary gas chroma-tography-mass spectrometry. Eur J Pediatr 1987;146:166-73.
37 Kelley RI, Datta NS, Dobyns WB, et al. Nconatal adre-noleukodystrophy: ncw cases. biochemical studies and dif-ferentiation from Zellweger and related peroxisomal poly-dystrophy syndromcs. Am J Med Genet 1986;23:869-901.
36 Gilbert EF, Opitz JM, Spranger JW, Langer LO, Wolfson JJ,Viseskull C. Chondrodysplasia punctata-rhizomelic form. Patho-logical and radiological studies of three infants. Eur J Pediatr1976;123:89-109.
3' Hoffmann G, Gibson KM, Brandt IK, Bader PI, Wappner RS,Swectman L. Mevalonic aciduria-an inborn error of choles-terol and nonsterol isoprene biosynthesis. N Engl J Med1986;314: 161t-4.
40 Nyhan WL, Sakati NA. Diagnostic recogniition of geneticdisease. Philadelphia: Lea & Febiger, 1987.
4' Brown GK, Hunt SM, Scholem R, et al. fi-HydroxyisobutyrylCoA deacylase deficiency: a defcct in valine metabolismassociated with physical malformations. Pediatrics 1982;70:532-8.
42 Singh AR, Lawrcnce WH, Autian J. Embryonic-fetal toxicityand teratogenic effects of a group of methacrylate esters in rats.J Dent Res 1972;51:1632-8.
43 Lipson A, Yu JS, O'Halloran MI, Williams R. Alcohol andphenylketonuria. Lancet 1981;i:717-8.
44 Sweetman L, Nyhan WL, Trauner DA, Merritt TA, Singh M.Glutaric aciduria type II. J Pediatr 1980;96:1020-6.
4 Lehnert W, Wendel U, Lindenmaier S, Bohm N. Multiple acyl-CoA dehydrogenation dcficiency (glutaric aciduria type 11),congenital polycystic kidneys, and symmetric warty dysplasia ofthe cerebral cortex in two brothers. 1. Clinical, metabolic andbiochemical findings. Eur J Pediatr 1982;139:56-9.
4' Bohm N, Uy J, Kiessling M, Lehnert W. Multiple acyl-CoAdehydrogcnation deficiency (glutaric aciduria type II), con-
gcnital polycystic kidneys, and symmetric warty dysplasia of thecerebral cortex in two newborn brothers. II. Morphology andpathogenesis. Eur J Pediatr 1982;139:60-5.
47 Vamccq J, Van Hoof F. Implications of a peroxisomal enzymein the catabolism of glutaryl-CoA. Biochem J 1984:221:203-11.
48 Patton MA, Krywawych S, Winter RM, Brenton DB, BaraitserM. DOOR syndrome (deafness, onycho-osteodystrophy andmental rctardation): elevated plasma and urinary 2-oxoglutaratein three unrelatcd patients. Ain J Med Gentet 1987;26:207-15.
49 Martin NDT, Snodgrass GJAI, Cohen RD, et al. Vitamin Dmetabolites in idiopathic infantile hypercalcaemia. Arch DisChild 1985;60:1140-3.
50 Culler FL, Jones KL, Dcftos U. Impaircd calcitonin secretionin paticnts with Williams syndrome. J Pediatr 1985;107:720-3.
5' Thaller C, Eichele G. Identification and spatial distribution ofretinoids in the developing chick limb bud. Nature 1987;327:625-8.
52 Slack JMW. We have a morphogen! Nature 1987;327:553-4.,3 Weiss M, Smith M, Griffin C, et al. Assignment of the gene
encoding the liver/bone/kidney form of alkaline phosphataseALPL to the region lp34-p36-1. HGM9. Cytogenet Cell Genet(in press).
54 Pauli RM, Lian JB, Mosher DF, Suttie JW. Association ofcongenital deficiency of multiple vitamin K-dependent coagu-lation factors and the phenotype of the warfarin embryopathy.Am J Hum Genet 1987;41:566-83.
5 Goodman S1, Frerman FE, Loehr JP. Recent progress inunderstanding glutaric acidemias. Enzyme 1987:38:76-79.
Correspondence and requests for reprints to Dr E MThompson, Mothercare Department of PaediatricGenetics, Institute of Child Health, 30 GuilfordStreet, London WC1N 1EH.
472
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.25.7.463 on 1 July 1988. Dow
nloaded from