Embed Size (px)
Citation preview

D
CS
a
AA
KDPS
1
idiasItohupepfdriatflcdi
1d
Respiratory Physiology & Neurobiology 167 (2009) 61–71
Contents lists available at ScienceDirect
Respiratory Physiology & Neurobiology
journa l homepage: www.e lsev ier .com/ locate / resphys io l
yspnea relief: More than just the perception of a decrease in dyspnea
laudine Peiffer ∗
ervice de Physiologie Radio Isotopes, Hôpital Européen Georges Pompidou, 20-40, rue Leblanc, 75908 Paris Cedex 15, France
r t i c l e i n f o
rticle history:ccepted 1 April 2009
eywords:
a b s t r a c t
Like relief in general, relief of dyspnea is the fundamental quite familiar subjective experience associatedwith the offset of, or decrease in an unpleasant stimulus associated most frequently with an emotion ofpleasantness. Dyspnea relief can be experienced in normal daily life, but most often, occurs during recov-ery from the large number of various diseases where dyspnea is frequently the predominant symptom.
yspnea reliefsychological modelsensori-emotional experience
In the present paper, after a brief review of current knowledge of the mechanisms of action of currentlyavailable therapeutic interventions for dyspnea, I shall address more extensively the specificity of reliefin the larger framework of psychological models relative to human perception and emotion. More specif-ically, I show that emerging, albeit preliminary results, including personal work, support the view thatdyspnea relief is a specific sensori-emotional experience involving a characteristic central processing, and
an th
that it is more complex th. Introduction
Dyspnea is a multidimensional subjective experience of breath-ng discomfort encompassing sensory, affective and cognitiveimensions. Furthermore, dyspnea is mostly associated with phys-
ological but also behavioural changes, including avoiding ordaptive strategies. As dyspnea is phylogenetically a very ancientensation, it has presumably provided evolutionary advantages.ndeed, by its unpleasant nature, dyspnea acts as a preventa-ive alarm signal, or at least to minimize harm to the integrityf the body by preserving it from asphyxia. Thereby, dyspneaas, like pain, potentially life-saving properties. The most pop-lar illustration of this fact is that absent or impaired dyspneaerception may lead to severe or even life-threatening asthmaxacerbation (Barnes, 1994). Most frequently however, rather thanroviding any advantage, dyspnea turns out to be a very distress-ul, and most predominant symptom in a large variety of differentiseases and thereby a major cause of suffering. It follows thatelief of dyspnea is a crucial concern in clinical practice, whichn turn has generated an important number of clinical studiesssessing the way of action, but predominantly, the outcome, inerms of decrease in dyspnea scores, of all the numerous dif-erent therapeutic interventions for dyspnea management. Much
ess work has been done on dyspnea relief as such i.e. a spe-ific and highly complex construct. Indeed, like relief in general,yspnea relief encompasses two different components, predom-nantly, the perception of offset of, or at least decrease in its
∗ Tel.: +33 01 56 09 34 88; fax: +33 01 56 09 29 67.E-mail address: [email protected].
569-9048/$ – see front matter © 2009 Published by Elsevier B.V.oi:10.1016/j.resp.2009.04.001
e mere perception of a decrease in dyspnea.© 2009 Published by Elsevier B.V.
underlying inherent unpleasant physical or mental stimulus, butalso a positive valenced emotion i.e. pleasantness or euphoriaand thus the perception of an hedonic switch from unpleasant topleasant. Moreover, unlike for pain, and more recently for dysp-nea, virtually nothing is currently known about central integrationand more specifically, potential consequences of dyspnea relief onbehaviour.
All these different aspects of relief will be addressed in thepresent paper. In the first part, after a brief overview and com-ments concerning current knowledge of the mechanisms of actionof presently available and recognized therapeutic interventions fordyspnea, I shall consider relief in the larger framework of psy-chological models relative to human perception and emotion andcurrent results from imaging studies. More specifically, I supportthe view, in the light of emerging results from specific albeit pre-liminary studies including personal work, that relief is a specificsensori-emotional experience, which basically is more complexthan the mere perception of a decrease in dyspnea and that itinvolves characteristic neural substrates.
2. Dyspnea relief in the clinical context
In the first part of this section, I shall review the numerous andobvious reasons why dyspnea is a major concern, and its man-agement an important challenge in clinical practice. In the secondpart, I present an integrative overview of the general mechanisms
of action and impacts of current treatment strategies for dyspnearather than to detail each of them. Indeed, both traditional andalternative interventions for dyspnea, especially regarding COPD,have been thoroughly addressed in several excellent recent reviews(ATS consensus statement of Dyspnea, 1999; Rabe, 2006; O’Donnell
6 gy & N
eCpr
2o
icipocdpteidvcctattim(efbqit1iipatpcstodur(vdtuatspcItond
2 C. Peiffer / Respiratory Physiolo
t al., 2007) and textbooks (Stuhlbarg et al., 1998, pp. 321–361;arrieri-Kohlman, 2005, pp. 365–396; O’Donnell and Mahler, 2005,p. 283–299; Zuwallack et al., 2005, pp. 301–320; Pan et al., 2000),espectively.
.1. Therapeutic interventions for dyspnea: a major clinicalutcome
As previously mentioned, dyspnea is a predominant symptomn a very large range of different pathological conditions, espe-ially in respiratory and cardiac disorders, but may also be presentn muscle or metabolic disease, in obesity and in special specifichysiological circumstances like heavy physical deconditioningr pregnancy. Moreover, in about 15% of cases, dyspnea is “psy-hogenic” or “medically unexplained” i.e. albeit sometimes veryistressing, it seems not to be, or not fully explained by obvioushysiological abnormalities, thus highlighting additional poten-ially generating and modulating factors of dyspnea factors such asmotional and cognitive processes. In this clinical context dyspneas indeed mostly associated with anxiety disorders, such as panicisorders (reviewed by Nardi et al., in the present issue) or hyper-entilation syndrome (Gardner, 1996). Moreover, in most clinicalonditions, especially in the before-mentioned, dyspnea becomeshronic presumably involving amplification processes. Most impor-antly, in critically ill patients, especially at the end of life, dyspnea ismajor and distressing problem often underestimated and under-
reated by health professionals (Hayes et al., 2006). Moreover, inhis setting, the prevalence of dyspnea is extremely high. Indeed,t concerns up to 80% of patients, and is even considered as the
ost distressing symptom in up to 95% of end-stage COPD patientsSkilbeck et al., 1998) and is as highly ranked as pain (Desbienst al., 1999) and severely impairs quality of life. The clearly harm-ul nature of dyspnea is further evidenced by the fact that it haseen shown to be an independent factor of impaired health-relateduality of life, and most importantly, of severity and bad prognosisn end-stage disease (Cuervo Pinna et al., 2008) and even of mor-ality from all causes in the general population (Carpenter et al.,989). Moreover, there is growing evidence that like for pain, thedeal objective i.e. removal of, or at least, decrease in the underly-ng causes of the corresponding unpleasant sensation is not alwaysossible or fully successful and thus, there is a clear need to man-ge the symptom per se. There is also increasing evidence that forhe large variety of pathological conditions associated with dys-nea, there is often no straightforward relationship between thisardinal symptom and the traditional physiological outcome mea-ures e.g. in the case of respiratory disease, mainly lung functionests and exercise capacity. Thereby, dyspnea management is notnly a crucial outcome for the patient but also an independenteterminant for the assessment of successful management of thenderlying disease. Therefore, there is a growing concern, and cur-ently a fully justified comeback, for a symptom-based evaluationi.e. taking into account the subjective effect) of therapeutic inter-ention as well as for the follow-up of diseases associated withyspnea. Moreover, there is increasing evidence that like for pain,he ideal objective i.e. the removal (or at least, the decrease of thenderlying cause of the corresponding unpleasant sensation) is notlways possible or fully successful and thus there is a clear needo manage the symptom per se. For all the before-mentioned rea-ons, doctors are quite frequently faced with the problem to relieveatients from dyspnea and there is a clear need and challenging out-omes for studies of dyspnea management in the clinical context.
ndeed, this important clinical concern led to an extensive litera-ure of clinical, mostly descriptive reports about the efficacy, andnly recently, studies of the underlying mechanisms of the largeumber of traditional and alternative therapeutic interventions foryspnea.eurobiology 167 (2009) 61–71
2.2. Integrative overview of impact and actions of therapeutic oftherapeutic interventions for dyspnea management
In almost all clinical studies of dyspnea management, impactis legitimately assessed in terms of decrease in dyspnea intensityand referred to as dyspnea relief. However, the sensory experienceof relief and of decrease in dyspnea intensity are slightly differentconstructs and may therefore not be strictly interchangeable. There-fore, for the discussion of clinical studies of dyspnea management, Ishall use the term “decrease in dyspnea” or “dyspnea management”instead of “relief”.
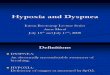
The underlying mechanisms of spontaneous or therapeuticallyinduced dyspnea management are basically the reversion or at leastthe decrease of the various dyspnea-related underlying physio-logical changes. The possible impacts and ways of action of thevarious interventions that may decrease dyspnea are manifold.Thus, a given therapeutic intervention may act at many differentlevels, whereas many different therapeutic interventions may havethe same impact. For example, opioids decrease ventilation andthereby the ventilatory demand, but have also an effect on theperception per se by a direct effect on central processing of dys-pnea. On the other hand, quite different therapeutic managementslike most bronchodilators and exercise training may ultimately (butsometimes by different mechanisms) reduce ventilatory demand.Therefore, there have been several attempts to identify commonunderlying mechanisms of these treatment strategies. A first rele-vant contribution has been provided by Stark (1988) who separatedpharmacological interventions for dyspnea into two categories(types I and II) according to whether the corresponding agentdecreases dyspnea by a concomitant decrease in ventilation (typeI) or without any change in ventilation, therefore supposed to be acentrally acting agent (type II). This led to the current view consider-ing that the impact of dyspnea management may be physiological(peripheral) or central i.e. acting directly on dyspnea perceptionper se. Based on this approach, as well as on current knowledge ofphysiopathology and central processing of dyspnea, an integratedview of dyspnea management may be proposed (Fig. 1). Thus, itmay be considered that the various therapeutic intervention mayact at either individual or both of the two main integration levelsof dyspnea, i.e. level I (sensori-motor integration) corresponding tothe final converging integration of the numerous underlying, pre-dominantly physiological mechanisms of dyspnea generation andemergence (peripheral mechanisms) and/or level II correspond-ing to the final integration and modulation of the sensation bypredominantly central mechanisms. At level I, decrease in dysp-nea may be obtained by different basic mechanisms (listed below)that ultimately decrease the mismatch between the planned andexpected versus the actual respiratory response. The latter resultsfrom an individual or collective action of the following: a decreasein ventilatory demand (that mainly results in a decrease in ven-tilation, which is a major impact, corresponding to Stark’s type Idyspnea treatment), the increase in efficiency of the effector (res-piratory system) and/or the increase in re-afferent signal). At levelII, decrease in dyspnea may be obtained by the modulation of thesensation per se, i.e. by an action on its final central perception inabsence of any – at least currently known – physiological changes(central mechanisms). There is indeed increasing evidence thatdyspnea encompasses affective/cognitive dimensions, including animmediate emotional reaction and a secondary, more sophisticatedreaction to dyspnea, which have a crucial influence on the subjec-tive experience of this symptom. Therefore, much emphasis has
been placed in recent years on the development and testing of theefficacy of strategies acting on modulating factors of dyspnea (levelII, Fig. 1), such as cognitive-behavioural, self-management and cop-ing strategies. This issue highlights the complexity of symptomperception, which is determined altogether by internal and exter-
C. Peiffer / Respiratory Physiology & Neurobiology 167 (2009) 61–71 63
Fig. 1. Integrative view of the possible impact of therapeutic interventions for dyspnea. The various therapeutic intervention may act at either individual or both of the two
main integration levels of dyspnea, i.e. level (sensori-motor integration) corresponding to the final converging integration of the numerous underlying, predominantly
physiological mechanisms of dyspnea generation and emergence (peripheral mechanisms) (large red arrow ), and/or level corresponding to final integration and
modulation of the sensation (predominantly central mechanisms) (large red flash 2). At level , decrease in dyspnea may be obtained by different basic mechanisms
(listed below) that ultimately decrease the mismatch between the planned and expected versus the actual respiratory response (large red arrow ) The latter results froman individual or collective action of the following (small red arrows): a decrease in ventilatory demand (that mainly results in a decrease of ventilation which is a majorimpact, corresponding to Stark’s type I dyspnea treatment), the increase in efficiency of the effector (respiratory system) and/or the increase in re-afferent signal). At level
, decrease in dyspnea may be obtained by the modulation of the sensation per se, i.e. acting on its final central perception in absence of any – at least currently known
– er theo ions, ai ferenca
nioams
3c
3
ifemhbbebipaaua
physiological changes (central mechanisms) (red flash ) by an action on eithn short- or long-term reactions to dyspnea. However, most therapeutic interventnteractions between the two main integration levels. (For interpretation of the rerticle.)
al reference frames, including psychological, social and culturalnfluences, as well as by self-confidence and/or both distractionr attention towards the symptom. It is in this regard noteworthy,s reported by Carrieri-Kohlman (2005), that apparently oppositeanoeuvers like distraction (by music) or attention towards the
ymptom of dyspnea have both been shown to decrease dyspnea.
. Dyspnea relief in the light of current research and newonceptual frameworks
.1. General considerations about relief
Relief, basically the perception of offset of, or at least decreasen, noxious and/or unpleasant physical or mental stimuli, is aundamental quite familiar subjective experience since it may bexperienced in a large variety of different situations such as pain,oral or mental suffering, escape from danger or threat, thirst,
unger, heat or cold, and of course dyspnea. Regarding dyspnea,esides its predominant occurrence in the clinical context, relief cane easily experienced in normal daily life e.g. after stopping heavyxercise but also in a more occasional circumstance, namely afterreaking volitional breath-holding. In addition, and most interest-
ngly, relief is actually a complex construct that in addition to the
erception of offset or decrease in its underlying inherent unpleas-nt stimulus, includes a positive valenced emotion i.e. pleasantness,nd thus encompasses the perception of an hedonic switch fromnpleasantness to pleasantness. The dimension of pleasantness isn intuitively well-known component of relief and is included incontext (determined by affectivo-cognitive, social and/or cultural factors) and/orct simultaneously at different levels. The dotted lines I′ and II′ symbolize possiblees to colour in this figure legend, the reader is referred to the web version of the
several official definitions of relief in current dictionaries (i.e. “afeeling of happiness that something unpleasant (has not/does not)happened or has ended/stops” (Cambridge and Oxford AdvancedLearner’s Dictionaries), “a feeling of cheerfulness that follows theremoval of anxiety, pain or distress” (Collins English Dictionary)).More specifically for dyspnea, the dimension of pleasantness is acommon emotional experience in everyday life (its pleasant to stopheavy exercise), but especially for patients. Indeed, daily clinicalobservation shows that in most subjects, successful managementof dyspnea is associated with a component of pleasure and/orreward, especially in the case of acute dyspnea e.g. during an asthmaexacerbation. In addition, this pleasantness component may con-fer some specificity to the qualitative experience of dyspnea reliefand therefore the perception of relief and the decrease in dyspneaintensity may not be strictly interchangeable constructs. The latterassumption, i.e. the specificity of relief, has indeed been repeat-edly verified for pain, which is a sensori-emotional experience thathas many common characteristics with dyspnea. In the context ofclinical and pharmacological studies of pain, long lasting experi-ence with the use of both pain intensity and relief scales showedthat these two types of scales did indeed reflect slightly differ-ent experiences. Thus, despite an expected overall good correlationbetween scores of relief and pain scales, the corresponding scores
are not identical and relief is more than just a change in pain inten-sity (Jensen, 2003). Differences between both constructs have beenattributed to the fact that relief scores may also include the per-ceived change of other aspects of pain e.g. such as affective andqualitative characteristics and that they may differentially depend
6 gy & N
otoatdapcqpaiaopetrmnnta
3
33csnorctsrlritibrurtitsWpobittsnomsegs
4 C. Peiffer / Respiratory Physiolo
n initial intensity (starting level) of pain (Jensen et al., 2002) andhat they may also differentially reflect the experience of treatmentutcome i.e. being a more relevant marker of treatment satisfactionnd adequacy of analgesia (Jensen, 2003). Moreover, the strength ofhe relationship between pain and relief scores has been shown toecrease over time (Angst et al., 1999; Jensen et al., 2002) presum-bly due to progressive changes in the reference frame regardingreceding sensory experience. Unlike for other types of relief, espe-ially pain, specific aspects of relief such as sensory, emotional andualitative characteristics, mechanisms underlying its intensity andleasantness and most importantly, its neural substrates, have beenddressed only quite recently for dyspnea relief. This may be relatedn part to the fact that, given the clinical importance of inducing andssessing decrease in dyspnea, this is the predominant componentf dyspnea relief that has been taken into account in virtually allrevious clinical and fundamental studies of dyspnea relief. How-ver, there is emerging, albeit preliminary evidence in the favour ofhe view that dyspnea relief is a specific sensori-emotional expe-ience involving a characteristic central processing, and that it isore complex than the mere perception of a decrease in dysp-
ea. Given the fact that this issue has received little attention untilow, most of the presented results come from personal studieshat will be discussed in the light of current research of frontierreas.
.2. Characteristics and specificities of dyspnea relief
.2.1. Sensori-emotional aspects
.2.1.1. Intensity of dyspnea relief and its physiological correlates. Inontrast to studies of clinical pain, to my knowledge specific reliefcales have never been used in long-term clinical studies of dysp-ea. Yet, given the similarities between pain and dyspnea, severalf the findings relative to these scales may also be applicable andelevant for clinical studies of dyspnea management. More specifi-ally, the fact that specific relief scales tend to be more sensitive tohe effects of treatment and to reflect more adequately treatmentatisfaction, they may be helpful for the management of disease-elated dyspnea, i.e. a mostly chronic condition that requires in aong-term treatment. Jensen (2003) reported that relief ratings mayemain positive despite the fact that intensity of pain returned tots baseline level which, as previously mentioned may be relatedo the fact that relief scores tell something more than a decreasen intensity. The before-mentioned specific information obtainedy relief scales may be important for treatment strategies such asehabilitation, which despite its effectiveness in dyspnea, is poorlynderstood with respect to the mechanism action. In contrast, quiteecently we have used specific relief scales for the assessment ofhe acutely load-induced dyspnea relief in 10 healthy volunteersn the context of a functional brain imaging study that addressedhe putative specificity of neural substrates and qualitative andensori-emotional aspects of dyspnea relief (Peiffer et al., 2008).
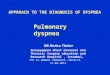
e found that intensity of both moderate and high relief of dys-nea (in terms of group mean scores) was rated as high as thatf the corresponding preceding dyspnea (Fig. 2A, black and emptyars, respectively). This result differs from a recent study of acutely
nduced heat pain by Leknes et al. (2008), who found, accordingo the predictions of a psychological theory (the opponent-processheory) that relief scores were consistently lower than pain inten-ities scores. These differences may be related to those of theature (pain versus dyspnea) and exposure time (3 s versus 40 s)f the underlying unpleasant stimulus. In contrast, as previously
entioned, under certain circumstances, in long-term clinical paintudies, relief scores tended to be higher and more sensitive to theffect of treatment than pain intensity scores (Jensen, 2003), sug-esting that perceived intensity of relief may depend on the contextuch as short versus long-term assessments. In addition, we found
eurobiology 167 (2009) 61–71
a large inter-subject variation for relief intensity scores that waspredominantly related to intensity scores of preceding dyspnea,reflecting the obvious, intrinsic relation of relief with its preced-ing underlying dyspnea (Fig. 2B). This result suggests that, in thecase of relief from acutely induced dyspnea, there may be somesimilarities of individual perceptual profiles i.e. a high or poor per-ceiver of dyspnea is likely to rate also high or low intensity of relief.However, inasmuch dyspnea relief cannot exist independently fromdyspnea, this raises the more theoretical question whether one canconsider the presence of high or poor perception of relief. It mayfurther be argued that what was rated was actually a decrease indyspnea, even if one is asked to rate relief. While this bias cannot beformally ruled out, given the tight causal relationship between bothvariables, we believe it to be unlikely. Indeed, specific relief scaleswere used and the subjects were clearly instructed to rate posi-tive relief instead of a decrease in dyspnea. Therefore, combinedwith the previously mentioned clinical pain studies (Jensen, 2003),one may hypothesize that a decrease in dyspnea and a change inrelief are slightly different constructs and it is legitimate to con-sider that they may involve a differential sensory experience, andconsequently a distinct perceptual profile as well.
As dyspnea relief basically involves the return to normal base-line of the dyspnea-induced respiratory changes, it may be expectedthat relief intensity is primarily determined by the same param-eters. Indeed, in our study, the best physiological predictor ofperceived intensity of relief (explaining 88% of its variance) wasthe decrease in a composite index, the ratio of the amplitude ofmouth pressure swings (�Pm) and the minute ventilation (V̇E)(�Pm/V̇E) reflecting the reversion of the dyspnea-induced increasein the respiratory effort: displacement ratio which itself, indi-rectly reflects reversion of one of the main characteristics of loadedbreathing-induced dyspnea, i.e. neuromechanical uncoupling. Thisresult further suggests that in the context of loaded breathing,the positive or negative valence of respiratory sensation is primar-ily determined by perception of the sense of change (decrease orincrease) of the �Pm/V̇E ratio rather than by its absolute value.
3.2.1.2. Qualitative aspects of dyspnea relief. Since the early workof Simon et al. (1989) on the language of breathlessness, thereis growing interest for the qualitative aspect of dyspnea and itsputative relationship with other characteristics of this sensation,especially its underlying mechanisms. Indeed, qualitative aspectshave been extensively investigated for both experimentally inducedand spontaneous disease-related dyspnea in a large number of dif-ferent pathological and experimental settings. Although there is aless clear-cut relationship between qualitative aspects and the spe-cific underlying afferent pathways for dyspnea than for pain, thereis currently good agreement that dyspnea is made up of severalbasic sensation e.g., increased effort/work of breathing, air hungerand chest tightness rather than a unique sensation (ATS statementon Dyspnea, 1999). Thus, in a given situation, dyspnea is character-ized by a specific set of a varying number and relative contributionof basic sensations, which depend on various degrees on underlyingmechanisms (Elliott et al., 1991) and/or intensity of dyspnea (VonLeupoldt et al., 2007), as well as ethnic and cultural factors (Hardieet al., 2000). However, until quite recently virtually no attentionhas been paid to qualitative aspects of dyspnea relief or more gen-erally, in a context of decrease in dyspnea. This specific issue wasfirst addressed by Moy et al. (1998) who assessed quality of dysp-nea in 25 subjects with acute asthma exacerbation after nebulizedalbuterol by a specific, commonly used and validated set of verbal
descriptors. Repeated assessments, i.e. every 20 min, of both thequantitative and qualitative aspect of decreasing dyspnea, showedthat the choice of the corresponding descriptors reflected the dif-ferential time courses of return to normal baseline of underlyingphysiological mechanisms of dyspnea i.e. the relative contribu-
C. Peiffer / Respiratory Physiology & Neurobiology 167 (2009) 61–71 65
Fig. 2. Sensory and emotional characteristics of dyspnea relief (adapted from Peiffer et al., 2008). (A) Group means (+SD) of perceived intensity (in % of maximal value ofeither Borg or VAS scores) showing that there was no significant difference between the intensity of relief of acutely load-induced dyspnea (black bars) and its correspondingpreceding dyspnea (empty bars), as well as its associated emotion of pleasantness (hatched bars) for the two experimental conditions i.e. high and moderate dyspnea relief(hR and mR), respectively. (B) Relationship between perceived intensity (individual Borg scores) of high and moderate dyspnea relief and of its preceding dyspnea with thedistribution along the identity line (broken line), showing that there was a strong correlation between both sensation intensities. (C) Relationship between individual valuesof perceived intensity (Borg scores) of dyspnea relief and of emotion of breathing-related pleasantness (in % of maximal value of Borg or VAS scores, respectively) for thethree experimental conditions, unloaded control condition, and high and moderate relief of dyspnea. While there was an overall good correlation between both experiencesfor most subjects (thin lines) i.e. pleasantness increases in parallel with relief, there was some discrepancy for three subjects (bold lines) i.e. virtually no pleasantness despitehigh relief (1), high pleasantness even in the absence of any significant relief, during the control condition (2) and decrease in pleasantness between the mR and hR conditionsd breaa een bw ogue s
t“edTrcaacdsssaaocjdcsr
“unrewarded effort” (which is a common and crucial feature ofdyspnea, at least in the context of loaded breathing). Our resultsshowed that qualitative assessment of dyspnea relief involves spe-cific, mostly positive valenced word descriptors. Indeed, only one
Table 1Specific word descriptors for the qualitative assessment of dyspnea relief.
Neutral valenceNeutral (absence of any specific respiratory sensation)Simple return to normal breathing
Positive valenceEasier to breathe (than during normal breathing)More comfortable to breathe (than during normal breathing)
espite constant relief (3). (D) Relationship between individual values of perceivedlong the identity line (broken line), showing again an overall good correlation betwith virtually no pleasantness (corresponding to subjects 1 and 3). VAS: visual anal
ion of the latter at a given time-point. Thus, the sensation ofchest tightness” decreased earlier than the sensation of “breathingffort”, which was directly related to ongoing airway obstruction,espite resolution of overall dyspnea in terms of intensity scores.hese results suggest that besides the commonly used intensityating, qualitative assessment of dyspnea may provide additional,linically relevant information during the recovery from an asthmattack, specifically regarding residual airway obstruction. However,s for most previous studies, the subjective experience of suc-essful dyspnea management has been inferred from decrease inyspnea scores. Therefore, based on our hypothesis relative to thepecificity of dyspnea relief, we assessed qualitative aspects withpecific word descriptors in our recent functional brain imagingtudy (Peiffer et al., 2008). To address this, subjects were asked tossess qualitative aspects of acutely load-induced high and moder-te dyspnea relief by selecting appropriate specific word descriptorsut of a list. The latter has been obtained from spontaneous reportsollected in a preliminary study with a larger number of sub-
ects since, as opposed to dyspnea, no validated list of specificescriptors is currently available for dyspnea relief. The final listonsisted of eight different descriptors, two neutral-valenced, andix positive valenced i.e. with a connotation of pleasantness and/oreward (Table 1). In addition, we submitted a further descriptor tothing-related pleasantness and unpleasantness (VAS scores) with the distributionoth emotion scores but also some discrepancy (encircled) i.e. high unpleasantnesscale; mR: moderate dyspnea relief; hR: high dyspnea relief.
the subjects, the term “hyperrewarded effort” defined as the sen-sory experience of breathing that is easier and/or more rewarded(more ventilation with less effort) than commonly expected dur-ing normal breathing, We decided to add this descriptor to ourfinal list because we considered it as a relevant counterpart to the
“Hyperrewarded” effort (sensation of getting more air with less effort thanduring normal breathing)
Real pleasure to breathe (rather than just neutral, normal breathing)Feeling of respiratory well-being (breathing becomes pleasant and relaxing)Respiratory release (very strong relief, liberation)

6 gy & N
swoprstvifaprbcibiifiictssirmmradmednoieimmomhpWitvwtc
3ci(sbocvpot
6 C. Peiffer / Respiratory Physiolo
ubject of our study population chose exclusively neutral-valencedord descriptors for all relief trials suggesting that, consistent with
ur initial hypothesis, dyspnea relief is not exclusively a neutralerception of return to normal breathing. Furthermore, for globalelief (values of high and moderate relief pooled together for eachubject) as well as for high relief alone, the selection rate of posi-ive valenced descriptors was significantly higher than for neutralalence. Interestingly, our results also showed that with increas-ng intensity of dyspnea relief, there was a parallel increase inrequency of choice of positive valenced word descriptors with
concomitant change in quality of the latter i.e. predominantlyleasantness for moderate relief and reward in terms of hyper-ewarded effort for high relief. This leads to the speculation thatoth the frequency distribution and the valence of selected spe-ific word descriptors of dyspnea relief change according to thentensity of relief, suggesting a certain degree of interdependenceetween the qualitative and quantitative dimensions of relief. This
s consistent with a previous study of exercise-induced dyspnean COPF patients (Von Leupoldt et al., 2007), which reported thatve different clusters of verbal descriptors changed according to
ntensity of dyspnea in different settings i.e. at rest, during exer-ise, walking test and after rehabilitation. More generally, it haso be kept in mind that the relief descriptors we used have beenelected and used in only one center, and due to the fact that ourtudy has been primarily designed for functional brain imaging, itncluded a relatively small number of subjects. Therefore, the cor-esponding results need to be verified and further validated in auch larger study population. Furthermore, we employed a singleethod to induce dyspnea, namely various degrees of an external
esistive load, thereby inducing increased effort of breathing andsmall increase in CO2. However, as previously mentioned, wordescriptors of dyspnea are in part determined by its underlyingechanism (Elliott et al., 1991) even in healthy volunteers (Simon
t al., 1989). It is therefore conceivable that there may also existifferent types of relief according to the main underlying mecha-isms of its preceding dyspnea. In this respect, the high frequencyf choice of the descriptor “hyperrewarded effort” in our studys noteworthy. Indeed, given the fact that increased unrewardedffort is one of the main basic sensory qualities of sensation dur-ng loaded breathing, the word descriptor “hyperrewarded effort”
ay be specific for relief in this setting. Likewise, qualitative assess-ent of dyspnea relief remains to be determined in the context
f disease. Indeed, word descriptors for quality of dyspnea reliefay slightly differ between patients and healthy subjects as it
as been recently shown for exercise-induced dyspnea in COPDatients and age-matched normal subjects (O’Donnell et al., 1997;illiams et al., 2008). Similarly, the short duration of our exper-
mental session due to the functional brain imaging design, andherefore, the lack of repeated relief ratings, did not allow us toerify whether, as in the study of Moy et al. (1998), the choice oford descriptors changed according to the time course of return
o baseline values of the different dyspnea-related respiratoryhanges.
.2.1.3. Pleasantness associated with dyspnea relief. The first andurrent only study of putative underlying mechanisms of thisntriguing characteristic of dyspnea relief is that of Nishino et al.2005). Based on the assumption that the pleasantness dimen-ion of relief, called “respiratory euphoria” by these authors, mighte related to endogenous opioids, they tested the effect of nalox-ne on acutely induced relief from severe dyspnea induced by a
ombination of resistive loading and hypercapnia in 14 healthyolunteers. They found that naloxone had no effect on breathingatterns or dyspnea and that it inhibited relief-related euphorianly to a minor extent, suggesting that the latter was only par-ially related to endogenous opioids. However, they did not ruleeurobiology 167 (2009) 61–71
out a decreased effect of naloxone and thereby an underestimationof the effect of opioids on relief related pleasantness via a partialblockade of vagal afferents from pulmonary stretch receptors by thedyspnea-associated hypercapnia.
As the main objectives of our functional brain imaging studywas dyspnea relief, we assessed emotional specificity of relief,i.e. pleasantness, together with negative valenced emotion, i.e.unpleasantness, and their respective relationship with relief anddyspnea intensity scores and their underlying respiratory changes.Since the subjects were blinded for the experimental sessions i.e.either dyspnea with subsequent relief or dyspnea alone or unloadedcontrol, the subjects were asked to rate emotion for all experimen-tal conditions. Group mean values of pleasantness scores during themoderate and high relief conditions did not differ significantly fromthose of the corresponding intensity scores of relief and of its pre-ceding dyspnea (Fig. 2, part A, black and empty bars, respectively).Likewise, there was an overall positive relationship between pleas-antness and intensity scores, i.e. pleasantness increases in parallelwith relief, for the study group as a whole and for most individualsubjects (Fig. 2, part C, thin lines). This is in line with a study ofacutely induced pain relief that shows there was a significant cor-relation between relief intensity and pleasantness scores (Leknes etal., 2008). However, for a given level of relief, pleasantness scoresdiffered greatly between subjects with three extreme cases, vir-tually no pleasantness despite high relief, high pleasantness evenin the absence of any significant relief during the control condi-tion, and one whose pleasantness decreased between the mR andhR conditions despite constant relief (Fig. 2, part C, bold lines 1,2 and 3, respectively) This result suggests that, like for dyspnea,relief presumably involves a sensory and an emotional component.Indeed, as first demonstrated for dyspnea by Wilson and Jones(1991), intensity and dyspnea-related unpleasantness are actuallytwo distinct and distinguishable components of dyspnea that can beassessed and vary independently (Von Leupoldt et al., 2006). In thisrespect, it is noteworthy that, as reflected by the ratings of two of oursubjects, pleasantness can be experienced without any associatedrelief and likewise, relief can be experienced without any associatedpleasantness, (Fig. 2, part C, bold lines 1 and 2, respectively). How-ever, the prevalence and possible clinical relevance of these extremeperceptual profiles remain to be determined in a much larger num-ber of subjects. Thus in a given subject, although the intensities ofboth components are highly related, there is a large interindividualvariation in the ratio of relief-related pleasantness and intensity.It is conceivable that these inter-subject differences in the inten-sity/pleasantness relationship, by further increasing inter-subjectdifferences in overall perception of relief, increase the complexityof individual global perceptual profiles of the subjective experienceof relief. In addition, this may contribute to determine the final sub-jective experience of treatment outcome for dyspnea similar to thatobtained by pain relief scales (Jensen, 2003).
Finally, it may be speculated that this emotional dimension ofrelief may be an additional or even more relevant determinant ofdisease-related behaviour (i.e. seeking medical help or compliancewith treatment) than the perception of relief intensity. Further-more, for the whole group, there was a reasonably good overallpositive relationship between pleasantness and unpleasantnessscores (Fig. 2, part D). However, similar to the relationship for reliefintensity scores, there was some discrepancy (Fig. 2, part D) encir-cled data points) i.e. subjects experiencing high unpleasantnessand virtually no pleasantness. Thus, there seems to be less congru-ency between experienced pleasantness and unpleasantness than
between intensity scores of the corresponding sensations i.e. reliefand dyspnea (Fig. 2B and D) highlighting a greater inter-subjectvariation in the way associated emotional valence is experienced.Furthermore, overall variance of sensation scores explained byrespiratory parameters was lower in pleasantness than in relief
C. Peiffer / Respiratory Physiology & Neurobiology 167 (2009) 61–71 67
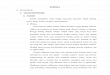
Fig. 3. Neural substrates of acutely induced high dyspnea relief characterized by areas of significant increase in the group average of relative regional cerebral blood flow(rCBF) as compared with the control condition (unloaded, without any respiratory sensation) (left panels A and B) and with acutely induced high dyspnea (panel C) (adaptedfrom Peiffer et al., 2008). Upper left panel (A): activation areas of relief as compared with control represented as “glass brain views” (i.e. projection of statistical parametricmaps of significant rCBF increase in the three dimensions of the standard stereotactic space defined by the atlas of Talairach and Tournoux. For clarity, only the five clusterswith the highest peak activation are labeled: (1) main activation area: left anterior cingulate cortex (BA 32/24); (2) right neocerebellum (inferior semilunar lobule, Crus II);(3) anterior right superior frontal gyrus; (4) right neocerebellum (superior semilunar lobule, Crus I); and (5) midbrain (meso-diencephalic junction, periventricular gray)showing an activation pattern which is different from that of dyspnea except for area in the midbrain (area 5) (see text for further details). Lower panels (B and C): projectionof the most significant activation area of two different contrasts of relief (i.e. versus control (B) and versus dyspnea (C) showing that the main activation peak of the former,a in virta n cent
iniciprstatsv
ataa
3f
sicipwi(
nd the secondary activation peak of the latter comparison (encircled) are locatedrea, at least under our experimental conditions, is the most importantly involved i
ntensity scores, suggesting that the determination of pleasant-ess presumably includes other, non-physiological factors, thereby
ntroducing additional inter-subject variation. In this respect, it isonceivable that according to personality traits and/or philosoph-cal principals, positive and negative valenced emotions may beerceived, integrated, or at least scored, in a different way. In thisespect, it is noteworthy that in a recent functional brain imagingtudy, Lewis et al. (2007) have verified that psychological modelshat predict positive and negative valenced emotions are processeds two independent dimensions and/or as difference from a neu-ral valence by identifying activation in partially distinct braintructures during presentation of affective positive and negativealenced word stimuli.
Although, our study was designed for functional brain imagingnd therefore had a small sample size, it provides the first evidencehat dyspnea relief is a specific construct with a distinct and char-cteristic predominantly positive valenced quality of sensation andconnotation of pleasantness
.2.2. Central integration of dyspnea relief: insights fromunctional brain imaging
Based on the assumption that relief of dyspnea is a specificensori-emotional experience, it might be expected that its centralntegration involves a characteristic, or at least a partially spe-ific neural network, or more specifically, that it would not solely
nvolve decreased activation of brain structures subserving dyspneaerception. We therefore determined brain activation associatedith moderate and high relief of acutely load-induced dyspnean 10 healthy volunteers by use of positron emission tomographyPeiffer et al., 2008). Together with a preliminary report of a fMRI
ually the same area of the left anterior cingulate cortex), thus suggesting that thisral processing of dyspnea relief.
study inducing dyspnea by reduced tidal volume in six mechani-cally ventilated healthy subjects (Binks, A., Vovk, A., unpublished,oral presentation entitled “Cerebral Activity with the Relief of Dys-pnea” presented at the International Dyspnea Symposium in SanDiego, 2005), these are currently the only specific imaging studiesof dyspnea relief. We identified a characteristic distributed brainactivation pattern associated with dyspnea relief, including a mainbrain activation area in the left anterior cingulate cortex (ACC), andadditional activation in the posterior cerebellum, the temporal andprefrontal cortices and the midbrain (Fig. 3A), while for dyspnea,significant activation was located in the right caudate nucleus, theanterior cerebellum, the premotor cortex and the midbrain, anddeactivation occurred in the left prefrontal cortex. Thus, our studyshowed that except for a common activation area in the midbrain,dyspnea relief-associated brain activation was distinct from bothincreased and decreased activation of areas involved in dyspneaperception. These results favour our initial hypothesis, namely thatthe sensory experience of dyspnea relief involves specific centralprocessing and not only a decrease in areas subserving dyspneaperception. In the only other brain imaging study of dyspnea relief,Binks and Vovk (2005) showed that relief of acutely induced airhunger relief was associated with increased activity in the midin-sula, thalamus and the putamen. Although their activation areasdiffered from ours, possibly because of differences in the design(induction of relief) and the imaging technique used, it confirms
that dyspnea relief involves characteristic increase in activationrather than exclusive decrease in dyspnea-related areas. A simi-lar activation pattern i.e. again involving predominantly specificincrease, has been identified for relief-related brain activation ofother unpleasant sensations, like thirst (Parsons et al., 2000) and
6 gy & N
et2vcrttrrtoMb(aaaorss12ndaietnwaaii(tbaa2tcitsTencMtccimbtetstbbp
8 C. Peiffer / Respiratory Physiolo
specially, relief of pain by various mechanisms, such as electros-imulation (Willoch et al., 2003), drugs and placebo (Petrovic et al.,002) and hypnosis (Rainville et al., 1999). The most significant acti-ation area that we identified by the two main contrasts of relief i.e.omparison to the unloaded control condition and to high dyspneaelief, respectively, was located in the same brain structure, namelyhe left anterior cingulate cortex (Fig. 3, panels B and C, respec-ively) suggesting that the latter may play a relevant contributiveole in central processing of the different sensory aspects of dyspneaelief. Activation in this brain structure has been previously showno be associated with pleasant sensory experiences like inhalationf NO2 (Gyulai et al., 1996) and pleasant touch (Rolls et al., 2003).ost interestingly, however, this brain area was also activated by
oth the positive and the negative valence associated with emotionsBush et al., 2000) and affective words (Lewis et al., 2006), as wells with the positive and negative difference between expected andctual pain relief (prediction errors) (Seymour et al., 2005), whichll may be relevant regarding one of the important characteristicsf relief, the hedonic switch from unpleasant to pleasant. In thisespect, it is noteworthy that activation close to our ACC activationite has also been previously identified in all the before-mentionedtudies of relief from other unpleasant sensations (Rainville et al.,999; Parsons et al., 2000; Petrovic et al., 2002; Willoch et al.,003), suggesting this brain structure may be part of a commoneural substrate for central processing of relief per se i.e. indepen-ently from the underlying cause. Interestingly, brain activation inmore rostral part of this cerebral structure has been repeatedly
dentified for acutely induced dyspnea (Corfield et al., 1995; Liottit al., 2001; Evans et al., 2002). It may therefore be hypothesizedhat, like pain (Willoch et al., 2003), the central processing of dysp-ea may involve a caudo-rostral functional segregation in the ACC,ith a caudal area devoted to perceptual processing of dyspnea
nd its associated motor changes, and a rostral modulation area,ssociated with relief, involved in anti-dyspneic regulation. A sim-lar rostro-caudal functional segregation has been demonstratedn the ACC for perception of pain and anti-nociceptive modulationWilloch et al., 2003) and in the nucleus accumbens and the ven-ral striatum for positive and negative valenced emotions (reviewedy Leknes & Tracey, 2008). In this respect, it may be relevant tonalyse this result in the light of an emerging highly innovatingpproach of pain and pleasure (reviewed by Leknes and Tracey,008) which, owing to the currently well-known common charac-eristics of pain and dyspnea, may be highly relevant in the presentontext. Indeed, convergent results from functional brain imaging,n particular from molecular imaging strongly support the view thathese two sensori-emotional experiences, while traditionally con-idered as opposite, in fact strongly interact by mutual inhibition.he latter involves a complex interplay between dopamine andndogenous opioids and share a distributed large set of commoneural substrates, the most important being the anterior cingulateortex, the amygdale, the nucleus accumbens and the pallidum,ost interestingly, ongoing technical progress with a higher spa-
ial resolution showed that rather than being strictly similar, theorresponding activation foci actually correspond to distinct, verylose, albeit partially overlapping cerebral structures correspond-ng to distinct neuronal populations. The only common albeit weak
inor activation area for relief and dyspnea was located in the mid-rain (meso-diencephalic junction, periventricular gray) an areahat has been previously shown to be activated by dyspnea (Banzettt al., 2000) and to be heavily involved in endogenous pain modula-ion (Bingel et al., 2007). Thus, in the light of the above-mentioned
patial relationship of opposed sensations, it may be speculatedhat according to the present preliminary results, ACC and the mid-rain could be part of a neural network involved in the interactionetween pro- and anti-dyspneic modulation. This may open newerspectives towards a better understanding of the modulationeurobiology 167 (2009) 61–71
of central dyspnea processing and possibly, a novel insight intoimpaired or enhanced dyspnea perception. Indeed, there is con-verging evidence from pain studies that an imbalance in pro andanti-nociceptive activity contributes to chronic pain. In this view,it may be speculated that chronic disproportional dyspnea may berelated to an impaired relief-related dyspnea modulation.
The currently available brain imaging results of dyspnea reliefhave to be considered as preliminary, given the small number ofimaging studies, which also provided somewhat different results.Nevertheless, these results suggest that dyspnea relief involvescharacteristic brain activation in areas predominantly distinct fromthose subserving dyspnea perception, which may be part of a mod-ulation network. These studies may be the first step towards theidentification of a “dyspnea-matrix”.
3.3. New conceptual frameworks for the understanding ofdyspnea relief
3.3.1. What may be the role of pleasantness and reward in thecontext of breathing and relief?
As previously outlined, both pleasantness and reward, twohighly related concepts, are hallmarks of dyspnea relief. At a firstsight, however, pleasure and reward are somewhat surprising andunusual in the context of breathing since, except after a sigh, theact of breathing is virtually never associated with positive emotionand in general, is intuitively considered as something neutral andautomatic. In fact, the life-long vital motor act of breathing actu-ally involves a complex regulation by multiple sensory input, that,although very complex, remains most of the time automatic andunconscious at the price of an active context-dependent filtering(Davenport and Vovk, in the present issue). Consequently, respi-ratory sensations that are consciously perceived are likely to berelevant or salient for the integrity of the body and more specifi-cally, the ventilatory status. Thus, when the act of breathing reachesconsciousness, the corresponding sensation is generally unpleasantand distressful in nature, i.e. it consists of dyspnea whose aversivenature can be easily understood with respect to its well-knownfunction as an alarm signal for impending threat e.g. asphyxia,thereby prompting an adaptative change towards return to normal.However, the role of pleasantness seems less intuitive in this con-text and thus leads to the more general question of what may be therole of positive emotional valence of breathing, and more specifi-cally in the context of dyspnea relief. To address this question, I thinkthat dyspnea relief should be considered within the larger frame-work of relief in general since pleasantness is one of its inherentfundamental characteristics
Over recent decades, there has been a progressive trend towardsa conceptual change in the way one considers emotions, namely inthe light of homeostasis i.e. a dynamic ongoing process tendingtowards bodily equilibrium. According to this view, both positiveand negative valenced emotions are powerful behavioural motiva-tors towards the maintenance of homeostasis by the correction ofany imbalance (Cabanac, 1971; Craig, 2003). In this respect, a phys-iological role of pleasure has been proposed by Cabanac since early1970 by suggesting that seeking pleasure and avoiding displeasureare of beneficial to the subject’s physiology and thus, linking plea-sure to usefulness (Cabanac, 1971). It follows that under this view,relief becomes an important determinant for behavioural choices.Moreover, reward value of a stimulus increases with the effec-tiveness of that stimulus in restoring homeostasis, the so-calledalliesthesia. This highly important characteristic, as well as the
very transient nature of pleasure allows a subtle and rapid ongo-ing adaptation to environmental and internal changes. In addition,pleasantness is tightly related to reward, since according to oneof its main definitions, it represents the subjective hedonic valueof reward. Reward expectation is a strong motivator for approach
gy & N
bTbfsrcsta
3
fposthipves(Faoadadii1av(2hchfosdihpotsdhnrhsaatoan(h
C. Peiffer / Respiratory Physiolo
ehaviour and highly subjected to learning (O’Doherty et al., 2003).he before-mentioned views lead to consideration of the possi-le consequences dyspnea relief on behaviour within a broaderramework. Relief may play an adaptive role as additional drive in auffocating condition by adding some reward value to the dyspnea-elated flight reaction in this situation. More specifically, in thelinical setting, beside numerous higher ordered cultural social,ymbolic motivations, the rewarding character of relief may con-ribute to compliance with bronchodilator treatment, especially insthma.
.3.2. Dyspnea relief in the light of the opponent-process theorySince its introduction by Hurvich and Jameson (1957) and
urther development by Solomon and Corbit (1974), the opponent-rocess model has received increasing attention and interest. Thepponent-process theory states that emotions are pairs of oppo-ites, e.g. happiness and sadness, fear and relief, pleasure and pain,hat interact as a linked pair by modulating around a point ofedonic neutrality, and thereby, that one emotion also activates
ts opposite. Thus, when after an affect-arousing stimulus (eitherleasurable or aversive) a corresponding, either positive or negativealenced, primary emotion is experienced, the other one (oppositemotion) is temporarily suppressed. This opposite emotion, i.e. theo-called opponent process, however, is likely to re-emerge stronglyafter-reaction) and may curtail or interact with the initial emotion.urthermore, although it may occasionally be directly induced orctivated by electrical stimulation, conditioning or memory, thepposite emotion is basically a slave process i.e. it can only beroused indirectly via the arousal of the primary emotion and itsuration varies greatly among the different situations (Solomonnd Corbit, 1974). Interestingly, repeated stimulation induces aecrease of the primary emotion, whereas the opposing one is
ncreased, appears earlier, last longer and may change in qual-ty, albeit not in terms of emotional valence (Solomon and Corbit,974). Thus, the opponent-process theory has provided a novelnd elegant explanatory model that applies successfully to a largeariety of different emotional events e.g. sky diving, colour visionBonnardel and Varela, 2003) and drug addiction (Koob and Le Moal,008), even though Solomon and Corbit’s (1974) consideration ofedonic neutrality as an a priori universal aim as well as the appli-ation of their model to higher ordered, complex and multifactorialuman experiences like love and grief, is somewhat questionable
rom a more general philosophical point of view. Subsequently, thepponent-process theory has been further developed to includeubstantial input from theories of learning such as the temporalifference model and by novel insight from recent imaging stud-
es (Seymour et al., 2005). However, to my best knowledge, unlikeeavy exercise (Petruzzello et al., 1997), neither breathing, nor dys-nea, and especially its relief, have been considered in the lightf this model. Yet the opponent-process theory is quite attrac-ive because it elegantly accounts for all the before-mentionedpecificities of dyspnea relief, as for relief in general, i.e. a pre-ominantly pleasurable sensori-emotional experience including aedonic switch from unpleasant to pleasant. In this respect, it isoteworthy that the prediction of the opponent model has beenecently verified for another type of relief that is acutely inducedeat pain (Leknes et al., 2008). Regarding dyspnea, this model con-iders dyspnea relief within a novel conceptual framework, namelys an opponent process associated with pleasantness, triggered byprimary aversive emotion i.e. dyspnea, and thereby sheds fur-
her light on the intrinsic internal relationship between these two
pposed yet inseparable emotions. In addition, this model maylso explain a further intriguing characteristic of dyspnea relief,amely the fact that its time course differs from that of dyspneai.e. offset of relief versus onset of dyspnea). Indeed, at least in ourands, despite a similar time course of induction of both dyspneaeurobiology 167 (2009) 61–71 69
and relief, as well as the corresponding respiratory changes, theduration of decrease of its intensity from maximum (i.e. just afterthe offset of dyspnea) to 0 is consistently shorter than the onseti.e. the duration of increase of intensity of the preceding dyspneafrom 0 to its destination value. Although, we did not specificallymeasure it, we noticed this intriguing difference in both our brainimaging study as well in our preliminary study on a greater num-ber of subjects. Likewise, a similar difference, albeit not specificallydiscussed, appears in the figures of two previous studies of load-induced dyspnea (Minowa et al., 2002; Nishino et al., 2005). Since,according to the opponent-process theory, the opponent emotion,in this case, relief, is expected to start before the end of the pri-mary aversive emotion, this may explain that the offset of reliefwhen counted from the offset of dyspnea, may be shorter. This spe-cific prediction has indeed been verified in the before-mentionedpsychophysical study of acute pain relief (Leknes et al., 2008). How-ever, several of the predicted characteristics of the opponent modeldo not apply to dyspnea relief. First, as previously mentioned, theopponent-process model predicts, that after repeated stimulation,the opposing emotion becomes stronger, with a parallel weak-ening of the primary emotion (Solomon and Corbit, 1974). Theclassical example, in the case of an aversive primary sensation, issky diving where the initial fear tends to decrease progressivelywhile the associated pleasure increases. Transposed to dyspnea,the model would predict that successive asthma attacks woulddecrease in unpleasantness while relief would be increasingly plea-surable. Although this point issue has never been formally tested,common, and especially clinical observation suggest that this is notthe case. Indeed, while temporal adaptation may occur, especiallyin chronic disease, this seems not to be associated with progressiveincrease of relief. This conflicting result may be due to the speci-ficity of dyspnea i.e. its primary crucial function of vital protectivealarm signal that may preclude this specific long-term evolution.Although to my best knowledge, this has never been formally tested,the same probably also applies to pain. In addition, it may also bespeculated that in the case of dyspnea relief, the opponent processcould work the other way round in some subjects, i.e. bronchodila-tors induce pleasurable relief which subsequently, is replaced byan anticipatory fear from impending bronchoconstriction and thusincreased dyspnea. Furthermore, it has to kept in mind that theopponent-process model has mainly be tested for acutely inducedsensori-emotional events, notably for relief of pain (Leknes et al.,2008). Therefore, it remains to be determined for both dyspnea andpain whether the opponent-process model also applies to reliefwith a slower onset i.e. when the offset of the main underlyingmechanisms of both preceding aversive emotions is slower, whichis likely to be the case in most clinical settings. Second, our resultsdid not confirm the prediction relative to intensity of the oppositeemotion i.e. that the latter is supposed to be weaker than the pri-mary aversive emotion, that is dyspnea. Indeed, unlike the resultsof Leknes et al. (2008), we found that intensity of both aspects ofrelief, i.e. the sensory intensity and the magnitude of its relatedpleasantness, were of similar intensity than preceding dyspnea. Ihave no straightforward explanation for this difference other thanthe trivial general consideration that this may be related to someintrinsic differences between pain and dyspnea. Furthermore, I sus-pect that, here again, things may be different in the clinical context,thus requiring further research with relief scales in long-term treat-ment. Two further characteristics of the opponent-process modelmay be relevant for dyspnea relief, namely the facts that the oppo-nent process, while subjected to substantial change by repeated
stimulation, is supposed to be by itself automatic, i.e. its presencedoes not require or imply any active cognitive or learning process,and, as clearly mentioned in the original paper, that the opponent-process model applies to the affective rather than to the sensorycharacteristics of a given stimulus (Solomon and Corbit, 1974).
7 gy & N
otnoe
4
upsriosssta
R
A
A
B
B
B
B
B
CC
C
C
C
C
D
E
E
G
G
H
H
H
0 C. Peiffer / Respiratory Physiolo
Despite several still open questions relative to the validity of thepponent model for dyspnea relief, the latter allows to considerhis intriguing sensori-emotional experience under a novel aspectamely, that its associated pleasantness is not simply the oppositef the aversive emotion associated with dyspnea, but that its merexistence is at the price of prior unpleasantness.
. Concluding remarks
Much work remains to be done towards a more completenderstanding of dyspnea relief, which given the burden of dys-nea, is before all, a major clinical concern. Yet, at the presenttate, new conceptual frameworks and recent, albeit preliminaryesults of current research suggest that dyspnea relief, despite itsnherent and absolute dependence on preceding dyspnea (with-ut dyspnea, no relief), encompasses specificity, both in termsensori-emotional experience and neural substrates. Furthermore,tudies of relief have highlighted the intriguing fact that the oppo-ite side of dyspnea, namely its usefulness as crucial aversive andhereby protective mechanism, is inherently associated with pleas-ntness.
eferences
merican Thoracic Society, 1999. Dyspnea: mechanisms, assessment, and man-agement. A consensus statement. Am. J. Respir. Crit. Care Med. 159,321–340.
ngst, M.S., Brose, W.G., Dyck, J.B., 1999. The relationship between the visual analogpain intensity and pain relief scale changes during analgesic drug studies inchronic pain patients. Anesthesiology 91, 34–41.
anzett, R.B., Mulnier, H.E., Murphy, K., Rosen, S.D., Wise, R.J., Adams, L., 2000. Breath-lessness in humans activates insular cortex. Neuroreport 14, 2117–2120.
arnes, P.J., 1994. Blunted perception and death from asthma. N. Engl. J. Med. 330,1383–1384.
ingel, U., Schoell, E., Büchel, C., 2007. Imaging pain modulation in health and disease.Curr. Opin. Neurol. 20, 424–431 (review).
onnardel, V., Varela, F.J., 2003. Color vision in the comb frequency domain. Biol.Res. 36, 119–134 (review).
ush, G., Luu, P., Posner, M.I., 2000. Cognitive and emotional influences in anteriorcingulate cortex. Trends Cogn. Sci. 4, 215–222.
abanac, M., 1971. Physiological role of pleasure. Science 173, 1103–1107.arpenter, L., Beral, V., Strachan, D., Ebi-Kryston, K.L., Inskip, H., 1989. Respiratory
symptoms as predictors of 27 year mortality in a representative sample of Britishadults. Br. Med. J. 299, 357–361.
arrieri-Kohlman, V., 2005. Coping and self-management strategies for dyspnea. In:Mahler, D.A., O’Donnell, D.E. (Eds.), Dyspnea: Mechanisms, Measurement, andManagement. Marcel Dekker, New York, pp. 365–396.
orfield, D.R., Fink, G.R., Ramsay, S.C., Murphy, K., Harty, H.R., Watson, J.D., Adams,L., Frackowiak, R.S., Guz, A., 1995. Evidence for limbic system activation duringCO2-stimulated breathing in man. J. Physiol. 488, 77–84.
raig, A.D., 2003. A new view of pain as a homeostatic emotion. Trends Neurosci. 26,303–307 (review).
uervo Pinna, M.A., Mota Vargas, R., Redondo Moralo, M.J., Sanchez Correas, M.A.,Pera Blanco, G., 2008. Dyspnea—a bad prognosis symptom at the end of life. Am.J. Hosp. Palliat. Care., December 29, PMID: 19114605.
esbiens, N.A., Mueller-Rizner, N., Connors Jr., A.F., Wenger, N.S., Lynn, J., 1999. Thesymptom burden of seriously ill hospitalized patients. SUPPORT Investigators.Study to understand prognoses and preferences for outcome and risks of treat-ment. J. Pain Symptom Manage. 17, 248–255.
lliott, M.W., Adams, L., Cockcroft, A., MacRae, K.D., Murphy, K., Guz, A., 1991. Thelanguage of breathlessness: use by patients of verbal descriptors. Am. Rev. Respir.Dis. 144, 826–832.
vans, K.C., Banzett, R.B., Adams, L., McKay, L., Frackowiak, R.S., Corfield, D.R., 2002.BOLD fMRI identifies limbic, paralimbic, and cerebellar activation during airhunger. J. Neurophysiol. 88, 1500–1511.
ardner, W.N., 1996. The pathophysiology of hyperventilation disorders. Chest 109,516–534 (review).
yulai, F.E., Firestone, L.L., Mintun, M.A., Winter, P.M., 1996. In vivo imagingof human limbic responses to nitrous oxide inhalation. Anesth. Analg. 83,291–298.
ardie, G.E., Janson, S., Gold, W.M., Carrieri-Kohlman, V., Boushey, H.A., 2000. Eth-nic differences: word descriptors used by African–American and white asthma
patients during induced bronchoconstriction. Chest 117, 935–943.ayes, A.W., Philip, J., Spruyt, O.W., 2006. Patient reporting and doctor recog-nition of dyspnoea in a comprehensive cancer centre. Intern. Med. J. 36,381–384.
urvich, L.M., Jameson, D., 1957. An opponent-process theory of color vision. Psychol.Rev. 64, 384–404.
eurobiology 167 (2009) 61–71
Jensen, M.P., Chen, C., Brugger, A.M., 2002. Postsurgical pain outcome assessment.Pain 99, 101–109.
Jensen, M.P., 2003. The validity and reliability of pain measures in adults with cancer.J. Pain 4, 2–21 (review).
Koob, G.F., Le Moal, M., 2008. Neurobiological mechanisms for opponent motiva-tional processes in addiction. Philos. Trans. R. Soc. Lond. B: Biol. Sci. 363 (1507),3113–3123 (review).
Leknes, S., Brooks, J.C., Wiech, K., Tracey, I., 2008. Pain relief as an opponent process:a psychophysical investigation. Eur. J. Neurosci. 28, 794–801.
Leknes, S., Tracey, I., 2008. A common neurobiology for pain and pleasure. Nat. Rev.Neurosci. 9, 314–320 (review).
Lewis, P.A., Critchley, H.D., Rotshtein, P., Dolan, R.J., 2007. Neural correlatesof processing valence and arousal in affective words. Cereb. Cortex 17,742–748.
Liotti, M., Brannan, S., Egan, G., Shade, R., Madden, L., Abplanalp, B., Robillard, R.,Lancaster, J., Zamarripa, F.E., Fox, P.T., Denton, D., 2001. Brain responses associatedwith consciousness of breathlessness (air hunger). Proc. Natl. Acad. Sci. U.S.A. 98,2035–2040.
Minowa, Y., Ide, T., Nishino, T., 2002. Effects of inhaled furosemide on CO(2) ventila-tory responsiveness in humans. Pulm. Pharmacol. Ther. 15, 363–368.
Moy, M.L., Lantin, M.L., Harver, A., Schwartzstein, R.M., 1998. Language of dyspneain assessment of patients with acute asthma treated with nebulized albuterol.Am. J. Respir. Crit. Care Med. 158, 749–753.
Nishino, T., Isono, S., Shinozuka, N., Ishikawa, T., 2005. Effects of naloxone on respi-ratory sensation before and after a removal of severe respiratory stress. Jpn. J.Physiol. 55, 117–126.
O’Doherty, J.P., Dayan, P., Friston, K., Critchley, H., Dolan, R.J., 2003. Temporal dif-ference models and reward-related learning in the human brain. Neuron 38,329–337.
O’Donnell, D.E., Bertley, J.C., Chau, L.K., Webb, K.A., 1997. Qualitative aspects ofexertional breathlessness in chronic airflow limitation: pathophysiologic mech-anisms. Am. J. Respir. Crit. Care Med. 155, 109–115.
O’Donnell, D.E., Mahler, D.A., 2005. Effect of bronchodilators and inhaled corticos-teroids on dyspnea in COPD. In: Mahler, D.A., O’Donnell, D.E. (Eds.), Dyspnea:Mechanisms, Measurement, and Management. Marcel Dekker, New York, pp.283–299.
O’Donnell, D.E., Banzett, R.B., Carrieri-Kohlman, V., Casaburi, R., Davenport, P.W.,Gandevia, S.C., Gelb, A.F., Mahler, D.A., Webb, K.A., 2007. Pathophysiology of dys-pnea in chronic obstructive pulmonary disease: a roundtable. Proc. Am. Thorac.Soc. 4, 145–168 (review).
Pan, C.X., Morrison, R.S., Ness, J., Fugh-Berman, A., Leipzig, R.M., 2000. Complemen-tary and alternative medicine in the management of pain, dyspnea, and nauseaand vomiting near the end of life. A systematic review. J. Pain Symptom Manage.20, 374–387.
Parsons, L.M., Denton, D., Egan, G., McKinley, M., Shade, R., Lancaster, J., Fox,P.T., 2000. Neuroimaging evidence implicating cerebellum in support of sen-sory/cognitive processes associated with thirst. Proc. Natl. Acad. Sci. U.S.A. 97,2332–2336.
Peiffer, C., Costes, N., Hervé, P., Garcia-Larrea, L., 2008. Relief of dyspnea involves acharacteristic brain activation and a specific quality of sensation. Am. J. Respir.Crit. Care Med. 177, 440–449.
Petrovic, P., Kalso, E., Petersson, K.M., Ingvar, M., 2002. Placebo and opioidanalgesia—imaging a shared neuronal network. Science 295, 1737–1740.
Petruzzello, S.J., Jones, A.C., Tate, A.K., 1997. Affective responses to acute exer-cise: a test of opponent-process theory. J. Sports Med. Phys. Fitness 37,205–212.
Rabe, K.F., 2006. Improving dyspnea in chronic obstructive pulmonary disease: opti-mal treatment strategies. Proc. Am. Thorac. Soc. 3, 270–275 (review).
Rainville, P., Hofbauer, R.K., Paus, T., Duncan, G.H., Bushnell, M.C., Price, D.D., 1999.Cerebral mechanisms of hypnotic induction and suggestion. J. Cogn. Neurosci.11, 110–125.
Rolls, E.T., O’Doherty, J., Kringelbach, M.L., Francis, S., Bowtell, R., McGlone, F., 2003.Representations of pleasant and painful touch in the human orbitofrontal andcingulate cortices. Cereb. Cortex 13, 308–317.
Seymour, B., O’Doherty, J., Koltzenburg, M., Wiech, K., Frackowiak, R., Friston, K.,Dolan, R., 2005. Opponent appetitive–aversive neural processes underlie pre-dictive learning of pain relief. Nat. Neurosci. 8, 1234–1240.
Skilbeck, J., Mott, L., Page, H., Smith, D., Hjelmeland-Ahmedzai, S., Clark, D., 1998.Palliative care in chronic obstructive airways disease: a needs assessment. Palliat.Med. 12, 245–254.
Simon, P.M., Schwartzstein, R.M., Weiss, J.W., Lahive, K., Fencl, V., Teghtsoonian, M.,Weinberger, S.E., 1989. Distinguishable sensations of breathlessness induced innormal volunteers. Am. Rev. Respir. Dis. 140, 1021–1107.
Solomon, R.L., Corbit, J.D., 1974. An opponent-process theory of motivation. I. Tem-poral dynamics of affect. Psychol. Rev. 81, 119–145.
Stark, R.D., 1988. Dyspnoea: assessment and pharmacological manipulation. Eur.Respir. J. 1, 280–287.
Stuhlbarg, M.S., Belman, M.J., Ries, A.L., 1998. Treatment of dyspnea: physical modal-ities, oxygen, and pharmacology. In: Mahler, D.A. (Ed.), Dyspnea. Marcel Dekker,New York, pp. 321–361.
Von Leupoldt, A., Ambruzsova, R., Nordmeyer, S., Jeske, N., Dahme, B., 2006. Sen-sory and affective aspects of dyspnea contribute differentially to the Borg scale’smeasurement of dyspnea. Respiration 73, 762–768.
Von Leupoldt, A., Balewski, S., Petersen, S., Taube, K., Schubert-Heukeshoven, S., Mag-nussen, H., Dahme, B., 2007. Verbal descriptors of dyspnea in patients with COPDat different intensity levels of dyspnea. Chest 132, 141–147.

gy & N
W
W
C. Peiffer / Respiratory Physiolo
illiams, M., Cafarella, P., Olds, T., Petkov, J., Frith, P., 2008. The language of breath-lessness differentiates between patients with COPD and age-matched adults.Chest 134, 489–496.
illoch, F., Gamringer, U., Medele, R., Steude, U., Tölle, T.R., 2003. PET activationstudy. Analgesia by electrostimulation of the trigeminal ganglion in patientswith trigeminopathic pain: a PET activation study. Pain 103, 119–130.
eurobiology 167 (2009) 61–71 71
Wilson, R.C., Jones, P.W., 1991. Differentiation between the intensity of breathless-ness and the distress it evokes in normal subjects during exercise. Clin. Sci.(Lond.) 80, 65–70.
Zuwallack, R., Lareau, S.C., Meek, P., 2005. The effect of pulmonary rehabilitation ondyspnea. In: Mahler, D.A., O’Donnell, D.E. (Eds.), Dyspnea: Mechanisms, Mea-surement, and Management. Marcel Dekker, New York, pp. 301–320.