Upload
ngokhuong
View
228
Download
0
Embed Size (px)
Citation preview
R
D
MJYCGPSKa
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
q
r
s
t
u
a
ARR3AA
KCMWHC
h1
Seminars in Cancer Biology 35 (2015) S129S150
Contents lists available at ScienceDirect
Seminars in Cancer Biology
j o ur na l ho me page: www.elsev ier .com/ locate /semcancer
eview
ysregulated metabolism contributes to oncogenesis
atthew D. Hirscheya,b,c,, Ralph J. DeBerardinisd,1, Anna Mae E. Diehla,1,anice E. Drewe,1, Christian Frezza f,1, Michelle F. Greenb,1, Lee W. Jonesg,1,oung H. Koh,1, Anne Le i,1, Michael A. Lea j,1, Jason W. Locasalec,k,l,1, Valter D. Longom,1,ostas A. Lyssiotisn,1, Eoin McDonnellb,1, Mahya Mehrmohamadi l,1,regory Michelotti a,1, Vinayak Muralidharo,p,1, Michael P. Murphyq,1,eter L. Pedersenr,1, Brad Poore i,1, Lizzia Raffaghellos,1, Jeffrey C. Rathmellb,c,1,haranya Sivanandt,1, Matthew G. Vander Heideno,p,u,1,athryn E. Wellent,1, Target Validation Team2
Department of Medicine, Duke University Medical Center, Durham, NC 27710, USADuke Molecular Physiology Institute, Duke University Medical Center, Durham, NC 27701, USADepartment of Pharmacology & Cancer Biology, Duke University Medical Center, Durham, NC 27710, USAChildrens Medical Center Research Institute, University of Texas Southwestern Medical Center, Dallas, TX 75390, USARowett Institute of Nutrition and Health, University of Aberdeen, Aberdeen, Scotland, United KingdomMRC Cancer Unit, University of Cambridge, Hutchison/MRC Research Centre, Cambridge, United KingdomDepartment of Medicine, Memorial Sloan-Kettering Cancer Center, New York, NY 10065, USAUniversity of Maryland BioPark, KoDiscovery, Baltimore, MD 20201, USAThe Sol Goldman Pancreatic Cancer Research Center, Department of Pathology, Johns Hopkins University School of Medicine, Baltimore, MD 21231, USANew Jersey Medical School, Rutgers University, Newark, NJ 07103, USADivision of Nutritional Sciences, Cornell University, Ithaca, NY 14850, USAField of Genetics, Genomics, and Development, Cornell University, Ithaca, NY 14850, USAAndrus Gerontology Center, Division of Biogerontology, University of Southern California, Los Angeles, CA 90089, USADepartment of Molecular and Integrative Physiology and Department of Internal Medicine, University of Michigan, Ann Arbor 48109, USAKoch Institute for Integrative Cancer Research, Massachusetts Institute of Technology, Cambridge, MA 02139, USAHarvard-MIT Division of Health Sciences and Technology, Harvard Medical School, Boston, MA 02115, USAMRC Mitochondrial Biology Unit, Wellcome Trust-MRC Building, Cambridge, United KingdomDepartment of Biological Chemistry and Department of Oncology, Johns Hopkins University, Baltimore, MD 21205, USALaboratory of Oncology, Istituto Giannina Gaslini, Genoa, ItalyDepartment of Cancer Biology, Abramson Family Cancer Research Institute, University of Pennsylvania, Philadelphia, PA 19104, USADana-Farber Cancer Institute, Boston, MA 02115, USA
r t i c l e i n f o
rticle history:eceived 12 March 2014eceived in revised form0 September 2015ccepted 5 October 2015vailable online 8 October 2015
a b s t r a c t
Cancer is a disease characterized by unrestrained cellular proliferation. In order to sustain growth, can-cer cells undergo a complex metabolic rearrangement characterized by changes in metabolic pathwaysinvolved in energy production and biosynthetic processes. The relevance of the metabolic transformationof cancer cells has been recently included in the updated version of the review Hallmarks of Cancer,where dysregulation of cellular metabolism was included as an emerging hallmark. While several lines of
evidence suggest that metabolic rewiring is orchestrated by the concerted action of oncogenes and tumor
suppressor genes, in some circumstances altered metabolism can play a primary role in oncogenesis.eywords:ancer metabolismitochondriaarburg
ost metabolismancer therapy
Recently, mutations of cytosolic and mitochondrial enzymes involved in key metabolic pathways havebeen associated with hereditary and sporadic forms of cancer. Together, these results demonstrate thataberrant metabolism, once seen just as an epiphenomenon of oncogenic reprogramming, plays a key rolein oncogenesis with the power to control both genetic and epigenetic events in cells. In this review, we
Corresponding author at: Duke Molecular Physiology Institute, 300 N. Duke Street, Durham, NC 27701, USA.E-mail address: [email protected] (M.D. Hirschey).
1 Equal contribution; authors listed alphabetically.2 The complete list of contributing authors on the target validation team are listed alphabetically in the acknowledgements.
ttp://dx.doi.org/10.1016/j.semcancer.2015.10.002044-579X/ 2015 Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
dx.doi.org/10.1016/j.semcancer.2015.10.002http://www.sciencedirect.com/science/journal/1044579Xhttp://www.elsevier.com/locate/semcancerhttp://crossmark.crossref.org/dialog/?doi=10.1016/j.semcancer.2015.10.002&domain=pdfmailto:[email protected]/10.1016/j.semcancer.2015.10.002http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/
S130 M.D. Hirschey et al. / Seminars in Cancer Biology 35 (2015) S129S150
discuss the relationship between metabolism and cancer, as part of a larger effort to identify a broad-spectrum of therapeutic approaches. We focus on major alterations in nutrient metabolism and theemerging link between metabolism and epigenetics. Finally, we discuss potential strategies to manipulatemetabolism in cancer and tradeoffs that should be considered. More research on the suite of metabolicalterations in cancer holds the potential to discover novel approaches to treat it.
evier
1
lwstbgaoac
oaotpcpltctai
mmecuFlbt
2
tWmoowcwlteaiWg
2015 Els
. Introduction
A non-profit organization called Getting to Know Canceraunched an initiative entitled The Halifax Project in 2011, which
as charged with identifying synergistic molecular targets and/ormall molecules for each of the areas that are widely consideredo be hallmarks of cancer [1]. The rationale for this approach isased on the idea that cancers harbor significant genetic hetero-eneity [2], which is often not addressed with monotherapeuticpproaches. While efforts have been made to combine therapies tovercome resistance, rising drug costs, significant levels of toxicity,nd a lack of overall success have stymied efforts to effectively treatancer with multi-drug combinations [3].
Thus, the first aim of the Halifax Project was to produce a seriesf reviews, including this review on cancer metabolism, to broadlyssess current knowledge on the biology of cancer. The overall goalf the Halifax Project is to identify biological targets and prospec-ive lead compounds that could potentially be used to reach eachrioritized area, and synergistically target multiple hallmarks ofancer. By building this rationale into the approach a priori, theroblem of heterogeneity might be overcome. In theory, multiple
ow toxicity approaches could be experimentally combined, whichhen might lead to synergism within a given hallmark, such as can-er metabolism. Future studies will build upon these findings andest these hypotheses, as well as integrate these concepts into thepproaches recommended in other hallmark areas in this specialssue.
In this review, we first discuss the relationships betweenetabolism and cancer. We focus on major alterations in nutrientetabolism, as well as the emerging links between metabolism and
pigenetics. Next, we discuss potential therapeutic strategies thatould be used to manipulate metabolism in cancer cells or to manip-late host metabolism thereby influencing cancer metabolism.inally, we describe tradeoffs that should be considered wheneveraging these approaches. Together, this information will be theasis of significant future research to fully realize the potential ofargeting metabolism in cancer.
. Classic metabolic derangements
The first realization that metabolism is altered in cancer canrace its roots to the work of Otto Warburg. During the 1920s,
arburg found that unlike most normal tissues, cancer tissues fer-ented glucose to lactate at high rates regardless of the presence
f oxygen [4,5]. This was in contrast to the results that Pasteur hadbtained previously studying fermentation in yeast, whereby O2as found to inhibit fermentation [6,7]. To study the metabolism of
ancer in vivo, Warburg used Jensen sarcoma cells to form tumorsithin the abdomens of rats. By comparing arterial glucose and
actate concentrations to venous glucose and lactate concentra-ions, Warburg was able to infer the glucose uptake and lactatexcretion by the tumor. Whereas normal tissues took up 218% ofrterial glucose, tumors consumed 4770%. Lactate was not signif-
cantly changed in blood after perfusion of normal tissues, but by
arburgs calculations, tumors converted 66% of their consumedlucose into lactate. Thus, Warburg surmised that tumors take up Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
much more glucose than normal tissues and convert a much largerpercentage of it to lactate [4].
Warburgs work on respiration and fermentation in cancer cellsultimately led him to propose that the respiration of all cancercells is damaged [8]. In fact, he reasoned that known carcinogens,such as arsenic and hydrogen sulfide, likely worked by inhibitingrespiration. He suggested that the primary oncogenic insult wasan inability of cells to oxidize glucose carbons, and that X-rayswere carcinogenic mainly due to their effect on mitochondria [8],which by this time had been shown to be the respiratory center ofcells.
The exact molecular mechanisms leading to altered metabolismin cancer and the Warburg effect remain a major unsolved question;for a review, see [9]. Subsequent studies have shown that whilechanges in mitochondrial respiration are sometimes seen in cancercells, these alterations are not likely the driving lesion for mostcancer cells. For example, Warburgs follow-up work suggestedthat oxidative respiration was important in malignant tumors, andreported that placing rats in 5% O2 for 40 h resulted in the death ofmost cancer cells, suggesting that oxygen was needed for viabilityof those cancer cells [4]. Similarly, the work of his contemporariesshowed that oxygen consumption is intact in many cancers, therebydecoupling the Warburg effect from defective oxygen consump-tion [10,11]. However, oxygen consumption cannot be a directmeasurement of intact respiration, because mitochondrial cou-pling/uncoupling influences the efficiency of oxygen consumed toATP produced. Nevertheless, many cancer cells display increasedglucose uptake and elevated lactate production, irrespective ofoxygen availability also called aerobic glycolysis or the War-burg effect [12], and this observation remains a hallmark of alteredmetabolism in cancer cells.
3. Emerging metabolic derangements
While the mechanisms leading to the Warburg effect areunder intense investigation, the general consensus of the fieldis that dysregulated metabolism and altered mitochondrialstructurefunction [13] is consistently found in several cancercell types. These changes may occur before, as a result of, or incombination with, the genetic changes driving cancer, includingoncogene expression or tumor suppressor loss; for recent compre-hensive reviews on these concepts, see [14,15]. For example, onewell-studied link between oncogenesis and glucose metabolism isthe phosphoinositide 3-kinase (PI3K) signaling pathway. Activat-ing mutations in PI3K or overexpression of the AKT oncogenes,which lie downstream of PI3K, can induce high rates of aerobic gly-colysis in non-transformed cells. This occurs in part by increasingexpression and localization of the high-affinity glucose transporter,GLUT1, on the plasma membrane [16,17]. In addition, activa-tion of the PI3K pathway can accelerate flux through glycolysisby increasing the activity of hexokinase-2, phosphfructokinase-1 (PFK1), or phosphofructokinase-2 (PFK-2) [1820]. The tumorsuppressor p53, which has a well described role in DNA dam-
age sensing, cell cycle control, and control of apoptosis, is alsoable to oppose the Warburg effect by stimulating respiration andreducing glycolytic flux [2123]. Thus, loss of p53 in cancer cells
http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/http://creativecommons.org/licenses/by-nc-nd/4.0/
M.D. Hirschey et al. / Seminars in Canc
Table 1Prioritized pathways to target cancer metabolism.
Target Known pathways Predicted manipulation
Hexokinase 2 (HK2) Glucose metabolism Reduce glucose uptakeand metabolism
6-Phosphofructo-2-Kinase/Fructose-2,6-Biphosphatase 3(PFKFB3)
Glucose metabolism Reduce glycolysis
Pyruvate kinase isoformM2 (PKM2)
Glucose metabolism Activate pyruvateoxidation
Glutaminolysis Amino acidmetabolism
Inhibit glutamineanaplerosis
Reductive carboxylation Amino acidmetabolism
Inhibit reductivecarboxylation
O-GlcNAcylation Epigenetics UnknownMethylation/one-carbon
metabolismEpigenetics Unknown
Acetylation/sirtuindeacylases (SIRTs)
Epigenetics Unknown
Oncometabolites Epigenetics Inhibit oncometaboliteformation andsignaling
Lactate Glucose metabolism Inhibit use of lactate asa fuel
ic
saat(Aeptotiwap
cmgscsabbtplt
otaetmc
s another event that can impact glucose metabolism in cancerells.
Given the inextricable relationship between oncogenes, tumoruppressors, and the regulation of glycolysis, metabolic alter-tions including the Warburg effect could provide a selectivedvantage to rapidly proliferating cells [24]. Although fermen-ation produces almost 20 times less adenosine 5-triphosphateATP) per glucose molecule than oxidative glucose metabolism,TP is never limiting in dividing cells [24,25]. Instead, prolif-rating cells require macromolecular precursors and reducingower in the form of reduced nicotinamide adenine dinucleo-ide phosphate (NADPH) to synthesize new biomass. Therefore,ne possible advantage of the Warburg effect is that high fluxhrough glycolysis allows for more efficient use of glycolyticntermediates for NADPH production and biosynthetic path-
ays including lipid synthesis, nucleotide synthesis, and aminocid synthesis, which would be permissive for rapid cellularroliferation.
Although glucose metabolism is important for proliferatingells, other nutrient sources contribute as well. TCA cycle inter-ediates are required for biosynthetic processes, including the
eneration of citrate for lipid synthesis and aspartate for nucleotideynthesis. When these intermediates are removed from the TCAycle, they must be replenished in a process known as anaplero-is. Glutamine has been shown to be a key contributor tonaplerotic flux in many cancer cells [26,27]. Glutamine car-on entry into the TCA cycle supports both ATP generation andiosynthesis, and a wide variety of cancer cell types are sensi-ive to glutamine withdrawal [28,29]. Catabolism of extracellularrotein can also contribute carbon to the TCA cycle [30], and
ipids are scavenged to support proliferation of some cancer cellypes [31].
Collectively, metabolic shifts that enable the generationf biosynthetic precursors are a key feature in cancer ini-iation, development, and/or growth. Below, we discuss howlterations in key metabolic pathways contribute to biomass gen-
ration (Table 1). We discuss some prioritized targets withinhese pathways, their therapeutic potential, and strategies to
anipulate metabolism for the prevention or treatment ofancer.er Biology 35 (2015) S129S150 S131
4. Glucose metabolism
4.1. Hexokinase 2 (HK2)
Regulation of glycolysis is exerted by the three importantkinases that catalyze discrete phosphorylation reactions (Fig. 1).Hexokinases are a family of enzymes that catalyze the first phos-phorylation of glucose to glucose-6-phosphate. Early work on ahighly malignant AS-30D hepatoma cell line showed that oneisozyme of hexokinase was uniquely bound to the outer mitochon-drial membrane [32,33], which was later identified as Hexokinase2 (HK2) [34].
In a series of experiments in this system, removal of malig-nant tumor mitochondria containing bound hexokinase from thecytoplasm by centrifugation markedly decreased the rate of glycol-ysis. Then, when tumor mitochondria containing bound hexokinasewere added back to the tumor cytosol, the original glycolyticcapacity of the cytoplasm was restored. Finally, when solubilizedhexokinase alone was added to the liver cytosol, it markedlyenhanced the glycolytic rate [34]. Therefore, HK2 could be amajor contributor to high glycolysis and lactate production evenin the presence of oxygen. One mechanism by which HK2 bindsto mitochondria is via the outer membrane protein known as thevoltage-dependent anion channel VDAC [35]. This binding interac-tion facilitates the immortalization of cancer cells [36,37].
To identify compounds that could selectively inhibit the twomain energy-producing pathways (glycolysis and mitochondrialoxidative phosphorylation), a limited screen was performed in can-cer cells. The small molecule 3-bromopyruvate (3BP) was identifiedas an inhibitor of glycolysis and also as an inhibitor of mitochon-drial energy production, which could be explained by inhibitingHK2 [38]. Follow-up work showed that 3BP has potent anticanceractivity and has the capacity to eradicate cancers in differentanimal models [39]. Furthermore, 3BP was recently tested in asingle human case study and showed promising results [40,41].Future work will be directed at the role of other HK isoforms incancer, as well as the specificity of 3BP toward HK2. However,these early studies are one proof-of-principle that targeting energymetabolism of cancer cells can be an effective therapeutic approach.
4.2. 6-Phosphofructo-2-kinase/fructose-2,6-biphosphatase 3(PFKFB3)
Another gluco-regulatory kinase is phosphofructokinase (PFK),which catalyzes the phosphorylation of fructose-6-phosphate tofructose-1,6-bisphosphate (Fig. 1). PFK is regulated by severalmetabolites, including inhibition by high concentrations of ATPand activation by fructose 2,6-bisphosphate. Early studies indi-cated that phosphofructokinase activity correlated with the growthrate of Morris hepatomas transplanted in rats and also correlatedwith lactate production by slices of those tissues [42]. Those obser-vations suggested that inhibition of phosphofructokinase activityrepresented a logical target for inhibition of malignant tumorgrowth. With the discovery that fructose 2,6-bisphosphate is anactivator of phosphofructokinase 1 [43], the enzyme activity cat-alyzing the formation of fructose 2,6-bisphosphate became analternative target for the inhibition of glycolysis and cancer growth.Steady state levels of fructose 2,6-bisphosphate are regulated bybifunctional enzymes that have both phosphofructo-2-kinase andfructose-2,6-bisphosphatase (PFKFBs). Of these enzymes, PFKFB3has the highest phosphofructo-2-kinase activity [44]. Interestingly,PFKFB3 expression, but not other PFKFBs, is markedly elevated in
multiple aggressive primary cancers, including colon, breast, ovar-ian and thyroid carcinomas [45].
The role of PFKFB3 in the regulation of glucose metabolism incancer cells has been reviewed previously [46]. An early indication
S132 M.D. Hirschey et al. / Seminars in Cancer Biology 35 (2015) S129S150
F hemes
tmrtfgsitl
ig. 1. Schematic of glycolysis. Enzymes altered in cancer are shown in bold. Color scingle bonds, thin; double bonds, bold.
hat PFKFB3 might be a regulatory enzyme was the identification ofultiple copies of the AUUUA instability motif in its 3 untranslated
egion [44]. Expression of the PFKFB3 gene is induced by hypoxiahrough hypoxia-inducible factor-1 [47]. Low pH, a commoneature in malignant tumors, is another factor that results in upre-ulation of PFKFB3. This may be mediated through the metabolic
tress sensor AMP-activated protein kinase (AMPK) resulting in anncrease in serine phosphorylation [48]. In breast cancer cells, syn-hetic progestins activate PFKFB3 isoenzyme phosphorylation and aong-term sustained action due to increased PFKFB3 protein levels.: carbon, gray; oxygen, blue; phosphate, yellow; adenosine, A; NAD+/NADH, orange;
An immediate early response occurs through the ERK/RSK pathwayleading to phosphorylation on S461 followed by activation of tran-scription via cis-acting sequences on the PFKFB3 promoter [49]. Inmyeloproliferative neoplasms, PFKFB3 expression was upregulatedvia active JAK2 and STAT5 [50], suggesting that specific inhibitorsof PFKFB3 might inhibit JAK2/STAT5-dependent malignancies.Levels of PFKFB3 are regulated by ubiquitinylation during thecell cycle. PFKFB3 accumulates in mid to late G1 and breakdownin S phase occurs specifically via a distinct S273 residue withinthe conserved recognition site for SCF-beta-TrCP [51]. The activity
Canc
omhclaciwhiti
o[oCgRmbcavPpc3i
4
geArePepPi[Iaiatg
lpcfNedtctfrrg
M.D. Hirschey et al. / Seminars in
f PFKFB3 is short lasting, coinciding with a peak in glycolysis inid to late G1 in contrast to glutamine metabolism, which remains
igh throughout S phase [52]. Glycolysis is characteristically asso-iated with cytosolic fractions of cells but PFKFB3 has a nuclearocalization signal. Furthermore, nuclear localization of PFKFB3 wasssociated with increased proliferation by increased expression ofyclin-dependent kinases and decreased expression of the cell cyclenhibitor p27 [53]. This brings to mind the more recent observation
ith the pyruvate kinase isoenzyme PKM2 (described below) thatas been shown to have potential transcription regulatory action
n addition to its role in glycolysis [54]. Therefore, a dual func-ion may be associated with some regulatory enzymes involvedn glycolysis.
Molecular modeling studies were the basis for the identificationf the first published report of a small molecule inhibitor of PFKFB355]. This molecule, 3-(3-pyridinyl)-1-(4-pyridnyl)-2-propen-1-ne known as 3PO became commercially available throughalbiochem, EMD Millipore in 2013. 3PO was shown to suppresslucose uptake and glycolytic flux and was selectively cytostatic toas-transformed human bronchial epithelial cells relative to nor-al cells. Growth of human erythroleukemia cells was inhibited
y 3PO [50]. Treatment of tumor-bearing mice reduced the intra-ellular concentration of fructose 2,6-bisphosphate, glucose uptakend tumor growth. The observation that 3PO suppresses T-cell acti-ation indicates a potential use for small molecule inhibitors ofFKFB3 in the treatment of autoimmune conditions but might beroblematic in combination treatments with immunosuppressiveancer chemotherapeutic agents [56]. A more potent derivative ofPO designated PFK15 has been identified and a phase I clinical trial
s planned [57].
.3. Pyruvate kinase isoform M2 (PKM2)
Pyruvate kinase (PK) catalyzes the final rate-limiting step inlycolysis (Fig. 1), transferring a phosphate group from phospho-nolpyruvate (PEP) to ADP and thereby generating pyruvate andTP [58]. Humans have four PK enzymes: PKR is restricted to eryth-ocytes; PKL is found predominantly in liver and kidney; PKM1 isxpressed in differentiated somatic cells (e.g. muscle and brain) andKM2 is found in fetal tissues and proliferating cells. In cancer cells,xpression of PKM2 is up-regulated such that it becomes the mostredominant PK isoform [59]. Accumulating evidence suggests thatKM2 expression is elevated in cancer cells, as its enzymatic activ-ty can be regulated by various metabolic and signaling inputs24,60,61]. PKM2 influences the fate of glucose carbons (Fig. 1).n general, PKM2 activity is low in proliferating cells, which cre-tes a bottleneck at the terminal step in glycolysis, which resultsn elevated concentrations of upstream glycolytic metabolites. As
consequence, such intermediates are available for the biosyn-hetic reactions that branch off of glycolysis, thereby increasing theeneration of cellular building blocks needed for proliferation [24].
Current models describing the function of PKM2 in cellu-ar proliferation focus mainly on mechanisms that regulate itsyruvate-generating activity as a cytoplasmic component of gly-olysis [61,62]. However, recent studies have provided evidenceor activities of PKM2 that extend beyond this canonical role.amely, several nuclear activities for PKM2, and mechanisms thatnable the shuttling of PKM2 into the nucleus, have now beenescribed [54,6370]. Nuclear activity promotes tumor growthhrough the direct transcriptional activation of genes involved inancer metabolism, including PKM2 itself and the RNA splicing fac-ors that repress PKM1 [54,65,68]. In this way, PKM2 acts in a feed
orward loop to promote both its nuclear activities and its metabolicole in cancer metabolism. Ongoing studies seek to examine theelative contributions of these two functions in oncogensis androwth.er Biology 35 (2015) S129S150 S133
The central principle presented above asserts that inhibiting PKactivity facilitates proliferation. This can be achieved through theexpression of the less active and regulatable PK enzyme, PKM2.Alternatively, PKM2 might be upregulated to eliminate PKM1expression; PKM1 is a constitutively active enzyme, which reducesthe generation of carbon for anabolic reactions and facilitates thegeneration of ATP in the mitochondria. Recent support for this lineof thinking comes from the observation that PKM2 is not requiredfor tumor maintenance, where short hairpin (sh)RNA-mediateddepletion does not affect tumor growth [71]. Furthermore, geneticexperiments, in which the PKM2-specific exon was deleted in amouse model of breast cancer using Cre-lox technology, demon-strated that the absence of PKM2 increased oncogenesis andnegatively affected survival. Strikingly, these tumors showed notissue-specific PK expression. They did, however, still produce lac-tate from glucose, suggesting that alternative and non-canonicalmethods of pyruvate generation were functioning [72]. Collec-tively, these experiments demonstrate that PKM2 is not requiredfor oncogenesis or growth, and support for the concept that cancercells have a growth advantage by removing PKM1.
Despite potential mechanistic differences between these twomodels on the role of PK in cellular proliferation, they converge ona common point: constitutive PK activity is detrimental for prolif-eration. Consistent with this concept, the first study to examinethe activity of PK directly in an isogenic context demonstratedthat cancer cell lines engineered to express PKM1 produce lesslactate, consume more oxygen and are less tumorigenic in nudemouse xenografts than those expressing PKM2 [73]. Importantly,these results demonstrated that less PK activity provided a selectivegrowth advantage for cancer cells in vivo.
From a therapeutic standpoint, activation of PK may serve asa promising strategy to slow cancer growth. Indeed, numerousresearch teams in the public and private sectors have recentlydeveloped drug-like small molecule activators of PKM2 that makeit behave more like PKM1 [7479]. Studies using such compoundshave shown that activation of PKM2 results in decreased accumu-lation of biosynthetic carbon building blocks and reduced cancergrowth [74]. Interestingly, all compounds described thus far sharea high degree of structural similarity and bind at the same interfacein the PKM2 multimer. The small molecule activator binding pocketis distinct from the fructose bisphosphate (FBP) binding pocket,where PKM2 activators overcome negative regulation by phospho-tyrosine peptides. Together, these two activities enable compoundsto overcome mechanisms that negatively regulate PKM2.
Several of the compounds described above have been inves-tigated in animal models [74,75]. In one study, a compoundcalled TEPP-46 activated PKM2 and impaired tumor seeding andgrowth. Subsequent metabolic analyses support the hypothesisthat impaired anabolic metabolism is responsible for the growthinhibition. Future studies are now aimed at exploring the use ofthese agents in combination with cytotoxic chemotherapies thatgenerate oxidative stress. Support for this concept comes from theobservation that activating PKM2 impairs the metabolic controlof redox specifically the generation of reducing equivalents inthe form of NADPH and GSH [80] which sensitizes cancer cellsto further oxidative stress. Finally, PKM2 activators may prove tobe doubly effective, as multimer formation prevents the nucleartranslocation of PKM2 and thus its activity as a protein kinase andactivator of gene expression [67].
5. Amino acid metabolismIn addition to the well-established role for altered glucosemetabolism in cancer, recent research highlights the involve-ment of amino acid metabolism in cancer, especially glutamine.
S Canc
Iat[Tscccg
t(spntrAap
5
t[bGTbnggidcec
agfvidtaahelc
uscmgogaoogt
134 M.D. Hirschey et al. / Seminars in
n proliferating cells, the tricarboxylic acid (TCA) cycle functionss a source of precursors for macromolecular synthesis in additiono generating reducing equivalents for oxidative phosphorylation81]. Citrate, for example, is both the canonical entry point of theCA cycle and a precursor for the acetyl-CoA used in fatty acid/sterolynthesis and acetylation reactions. Normally, the withdrawal ofitrate to supply these other pathways is matched by an influx ofarbon into the cycle to yield oxaloacetate, refilling the pools of TCAycle intermediates and maintaining function of the cycle duringrowth [26].
In culture, many cancer cells meet their anaplerotic demandhrough the oxidative metabolism of glutamine to oxaloacetateFig. 2) [26]. Glutamine is an advantageous anaplerotic precur-or because its conversion to -ketoglutarate (-KG) has theotential to disperse nitrogen to hexosamines, nucleotides, andon-essential amino acids, all of which are required for growth. Fur-hermore, oxidative metabolism of -KG to oxaloacetate produceseducing equivalents that can be used to generate energy [82].lternative anaplerotic pathways, such as pyruvate carboxylation,lso produce oxaloacetate but do not satisfy these other demands,ositioning glutamine as a key player in mitochondrial metabolism.
.1. Glutaminolysis
Glutamine is a non-essential amino acid with an amine func-ional group and is the most abundant amino acid in circulation83]. Glutamine supplies nitrogen for nucleobase synthesis and car-on for the TCA cycle, lipid synthesis and nucleotide synthesis [84].lutamine is involved in both anabolic and catabolic processes.he catabolism of glutamine is called glutaminolysis, which cane converted into glutamate, aspartate, CO2, pyruvate, lactate, ala-ine and citrate. The first step of glutaminolysis is the conversion oflutamine to glutamate and ammonia via glutaminase (GLS). Afterlutamine is converted into glutamate, the glutamate is oxidizednto -KG. This most often occurs through the enzyme glutamateehydrogenase (GLDH), concomitant with the generation of mito-hondrial NADH or NADPH and ammonia [85]. This is the firstnergy-yielding step in glutaminolysis and is the link to the TCAycle (Fig. 2).
While glutaminolysis is a normal process for many cells, suchs lymphocytes and adipocytes, many cancer cells have elevatedlutamine flux. In cell culture, human glioma and HeLa cells wereound to be completely dependent upon glutamine for their sur-ival. The cells died in the absence of glutamine, despite beingn glucose-rich media, which is now known as the completeependence on glutamine for cell survival (a.k.a. glutamine addic-ion) [28,86]. Interestingly, not all cancer cells exhibit glutamineddiction. While the complete molecular mechanism of glutamineddiction is not known, several oncogenic mutations or alterationsave been found to explain glutamine-dependence in cancers. Forxample, Myc is able to increase glutamine metabolism by upregu-ating GLS expression, which leads to glutamate entry into the TCAycle as -KG [87].
The ability to use exogenous glutamine is enhanced by thepregulation of glutamine transporters [88]. For example, onetudy found the increase in glutaminolysis was so profound thatancer cells accumulated more glutamine than was necessary toeet the energy and anabolic requirements of the cell; excess
lutamine-derived carbon was secreted from the cells in the formf lactate or, to a lesser extent, alanine [28]. Further evidence sug-ests that overexpression of Myc is enough to induce glutamineddiction, due to the fact that this mutation causes the metabolism
f the mitochondria to be altered in such a manner as to relyn glutamine despite available glucose [28]. Interestingly, theselutamine-addicted cells were found to be keenly sensitive to elec-ron transport chain inhibitors. This observation could indicate thater Biology 35 (2015) S129S150
either the potential energy in glutamine is being used in the pro-duction of ATP [89] or that mitochondrial glutamate uptake by theglutamate/aspartate mitochondrial transporter requires a proton-motive force.
In human pancreatic ductal adenocarcinoma (PDAC), theoncogene KRAS contributed to glutamine dependency by usingglutamine-derived aspartate to produce oxaloacetate via aspar-tate transaminase (GOT1) in the cytoplasm. Oxaloacetate was inturn converted into malate and then pyruvate to maintain a highNADPH/NADP+ ratio for redox homeostasis. Therefore, disruptingthese reactions, and ultimately glutamine metabolism, led to sup-pression of PDAC growth in vitro and in vivo [90].
In a recent study, the use of nuclear magnetic resonance(NMR) spectroscopy and mass spectrometry (MS), as well as sta-ble isotope-resolved metabolomics, allowed the fate of 13C and 15Nfrom labeled glutamine in B lymphoma cells to be traced under aer-obic and hypoxic glucose-deprived conditions [91]. In this study,glutamine is the fuel that drives the TCA cycle, which is com-pletely independent of the glucose supply. This reprogramming ofthe TCA cycle is particularly advantageous to cancer cells underglucose-deprived and/or hypoxic conditions. Where glucose is pref-erentially converted to lactate under hypoxic conditions, glutaminemetabolism serves to sustain ATP production and redox homeosta-sis in order to support cancer cell growth and survival. This impliesthat even hypoxic cancer cells can oxidize glutamine through theTCA cycle, and in the absence of glucose, glutamine metabolismalone can sustain the TCA cycle and thereby meet the anapleuroticand energetic demands of the proliferating cancer cells.
Supporting this idea, Myc-transformed cells were found to relyon a means of -KG synthesis other than that involving GLDH.Aspartate and alanine transaminases reversibly convert glutamateinto -KG, along with oxaloacetate to aspartate or pyruvate toalanine, respectively (Fig. 2). These reactions occur despite the pres-ence of GLDH in the mitochondria of cancer cells, which catalyzesthe direct conversion of glutamate to -KG [92]. This is espe-cially important considering it was found that Myc-transformedbreast cancer cells undergo apoptosis when aspartate transami-nase is inhibited. This implies that this cancer is heavily reliant upontransaminase reactions to produce -KG [93,94].
Due to the central nature of glutaminolysis in many cancers, itis becoming an increasingly prominent target in cancer therapy.One of the early strategies to suppress glutamine metabolism wasto reduce the amount of available glutamine by using glutamineanalogs. Compounds such as 6-diazo-5-oxo-l-norleucine (DON)and acivicin showed cytotoxic effects against several malignanttumors types, including leukemia and colorectal cancers; howeverthese analogs are no longer clinically available due to patient tox-icity [95].
More recent strategies have focused on targeting the enzymesof glutamine metabolism. For example, GLS is a potential targetfor the inhibition of glutaminolysis in cancer cells. The kidney iso-form, GLS1, is found in many malignant tumors [96] while the liverisoform, GLS2, is less often expressed in cancers. The compound bis-2-(5-phenylacetimido-1,2,4,thiadiazol-2-yl)ethyl sulfide (BPTES)has been shown to inhibit growth of a variety of cancers in mousemodels and in cell culture, including B lymphoma, which allosteri-cally inhibits GLS1 by altering the conformation of the enzyme [97].The effect is enhanced under hypoxic conditions, often inducingcancer cell death [91].
GLDH is another potential target of glutaminolysis, which whenknocked-down by siRNA resulted in a marked decrease in the pro-liferation of glioblastoma cells that were glutamine dependent [98].
Green tea polyphenols, hexachlorophene, GW5074, and bithionolmay inhibit GLDH function. These inhibitors work by restrictingenzyme movement, either by forming rings around the enzymeor wedging between the enzymes subunits. Currently, green tea
M.D. Hirschey et al. / Seminars in Cancer Biology 35 (2015) S129S150 S135
F are shs e, A; b
papp
tigtipctairta
5
siv
ig. 2. Schematic of the TCA cycle and glutaminolysis. Enzymes altered in cancer cheme: carbon, gray; oxygen, blue; phosphate, yellow; nitrogen, brown; adenosinlue; single bonds, thin; double bonds, bold.
olyphenols have been shown to inhibit lung, colon, and prostatedenocarcinoma growth in xenograft models [99]. These com-ounds also had significant effects on glioblastoma, colon, lung androstate adenocarcinoma cell proliferation [100].
Another strategy to inhibit glutaminolysis is to target alanineransaminase through l-cycloserine [101] or aspartate transam-nase through amino oxyacetate [93] which nearly halted therowth of breast cancer xenografts in mice. Similarly, aspartateransaminase knockdown in pancreatic cancer is also dramat-cally growth inhibitory in vitro and in vivo and leads to arofound disruption of redox homeostasis [90]. In both of theseases, little to no toxicity was observed with transaminase inhibi-ion in non-neoplastic cells. These studies suggest that aspartateminotransferase is a promising cancer target. Finally, given thatnhibition of aspartate transaminase also leads to a disruption ofedox homeostasis, such inhibition may synergize with therapieshat increase reactive oxygen species (ROS), such as chemotherapynd radiation [102].
.2. Reductive carboxylationNot all cancer cells have the ability to perform glutaminoly-is. Hypoxia limits the oxidative capacity of the TCA cycle, andn particular suppresses production of acetyl-CoA from glucoseia pyruvate dehydrogenase (PDH) [103,104]. Furthermore, someown in bold. Reductive direction of the TCA cycle shown with blue arrows. Colorcoenzyme A, light gray; NAD+/NADH, orange; NADP+/NADPH, brown; FAD/FADH2,
cancer cells contain severe mutations in TCA cycle enzymes (suc-cinate dehydrogenase, fumarate hydratase) or in components ofthe electron transport chain that prevent efficient production ofoxaloacetate from glutamine [105]. Yet, both hypoxic cells andcells with defective mitochondria require glutamine for growth[106108]. To address this paradox, metabolic labeling experi-ments were performed using 13C, and revealed that these cellsmetabolize glutamine through an unusual pathway characterizedby reversal of isocitrate dehydrogenase (IDH) enzyme activity(Fig. 2, blue arrows) [106,107,109,110]. IDH typically acts as anoxidative decarboxylase, converting isocitrate to -KG and CO2in the presence of an electron acceptor. Indeed, IDH3, the mito-chondrial NAD+-dependent IDH isoform, functions exclusively inthis manner. However, the two other mammalian IDH isoforms,IDH1 and IDH2, use NADP+/NADPH as cofactors, and can acteither as oxidative decarboxylases or reductive carboxylases. Inthe latter reaction, -KG is carboxylated to produce isocitrate, con-verting NADPH to NADP+. Isocitrate is readily converted to citrate,which can then be cleaved to produce acetyl-CoA. Under condi-tions of reductive carboxylation, glutamine becomes the majorsource of acetyl-CoA for fatty acid synthesis, greatly decreasing
the need to produce acetyl-CoA from glucose. Furthermore, cit-rate cleavage yields oxaloacetate, which is converted to other4-carbon intermediates, meaning that essentially the entire cellu-lar pool of TCA cycle intermediates can be derived from reductive
S Canc
cd
mtcscmm(dieHmrcastcaddotg
ttdrNincg[ttt[asfir
aipcctr
nmrfoptcIe
136 M.D. Hirschey et al. / Seminars in
arboxylation, in reverse order to their conventional route of pro-uction (Fig. 2).
Reductive carboxylation had previously been observed as ainor source of isocitrate and citrate in a number of non-
ransformed mammalian tissues [111114]. Its importance inancer cell biology is related to its ability to serve as the majorource of citrate and acetyl-CoA when cellular circumstancesonspire to inactivate pathways that normally produce theseetabolites, including hypoxia and genetic reprogramming ofitochondrial metabolism. For example, the Von HippelLindau
VHL) tumor suppressor normally functions in the oxygen-ependent degradation of the alpha subunits of the hypoxia
nducible factor (HIF) transcriptional activators. Thus, in cellsxpressing VHL, oxygen facilitates the degradation of HIF1 andIF2 so that HIF target genes are not expressed. In contrast, inalignant tumor cells lacking VHL, HIF target genes are expressed
egardless of oxygen availability. These genes, which include glu-ose transporters and glycolytic enzymes, are part of the metabolicdaptation to hypoxia. Importantly, hypoxia stimulates the expres-ion of PDH kinase-1 (PDK1), which phosphorylates and inactivateshe PDH complex, impairing its ability to provide acetyl-CoA anditrate from glucose [103,104]. Cancer cells lacking VHL produce
substantial fraction of citrate and fatty acids using glutamine-ependent reductive carboxylation in culture, and a small butetectable fraction of citrate in vivo [115]. Heterologous expressionf wild-type Vhl, or silencing of PDK-1, partially reverts metabolismo a phenotype in which citrate and fatty acids are produced fromlucose/PDH [115].
Regulation of reductive carboxylation is an area of active inves-igation. Importantly, the pathway is stimulated by mutations inhe electron transport chain that impair recycling of mitochon-rial NADH to NAD+, but importantly NADPH is the cofactor foreductive carboxylation. This suggested a model in which a lowAD+/NADH ratio in mitochondria provides a source of reduc-
ng equivalents which are transmitted to NADPH by nicotinamideucleotide transhydrogenase (NNT) [107]. NNT is an inner mito-hondrial membrane protein that uses the electrochemical protonradient to transfer reducing equivalents from NADH to NADPH116]. Silencing NNT expression in SkMel5 melanoma cells reducedhe contribution of glutamine carbon to TCA cycle intermediateshrough both oxidative and reductive metabolism, and decreasedhe rate of growth of SkMel5-derived subcutaneous xenografts117]. In VHL-deficient 786-O renal carcinoma cells, which produce
large fraction of citrate via reductive carboxylation, NNT silencingignificantly suppressed reductive glutamine metabolism. Thesendings suggested that NADPH produced by NNT is required foreductive carboxylation in VHL-deficient cells.
Reductive carboxylation is also regulated by changes in thebundance of TCA cycle metabolites. Citrate levels tend to be lown cells with active reductive carboxylation, and maneuvers to sup-ress formation of citrate from glucose enhance the fraction ofitrate derived from reductive carboxylation [106,107,109,115]. Inontrast, supplying cells with exogenous acetate or citrate increaseshe ratio of citrate/-KG while reducing the overall contribution ofeductive carboxylation to TCA cycle metabolism [115].
Compartmentalization of the reductive carboxylation reaction isot well understood. IDH1 is cytosolic while IDH2 is localized to theitochondria, and data suggest that each isoform can participate in
eductive carboxylation. IDH2 was found to be the crucial isoformor reductive carboxylation in hypoxic glioma cells [109], whereasther cell lines required IDH1 under hypoxia [106]. Genetic sup-ression of pyruvate dehydrogenase in lung cancer cells is sufficient
o induce a net flux of reductive carboxylation, and under theseircumstances the flux is completely dependent on IDH1 [118].n cells with mutations in the electron transport chain, silencingither isoform reduced activity of the pathway, and silencing bother Biology 35 (2015) S129S150
together had a maximal effect [107]. The involvement of NNT as asource of NADPH argues for mitochondrial localization of the reduc-tive carboxylation reaction, at least in those cells that require NNTexpression to maintain citrate levels. However, cytosolic sources ofNADPH, including the oxidative branch of the pentose phosphatepathway, may play a more prominent role in cells where IDH1 cat-alyzes reductive carboxylation. Presumably, the choice of isoform isalso related to localization of an available source of the substrate -KG, meaning that compartmentalization of glutamine metabolismcould add another dimension to regulation of this pathway.
6. Lipid metabolism
Cancers may use a wide variety of substrates and substratesources to meet their catabolic and anabolic needs, includinginternally and externally derived fatty acids (FAs). Indeed, FAsare essential for cellular proliferation. In particular, FAs are usedas cellular building blocks for lipid membrane synthesis, forenergy storage and production, as well as for cellular signaling.Thus, limiting abundance of FAs could be a therapeutic strategyagainst cancer. Limiting cellular FAs could be achieved by: blockingsynthesis (lipogenesis), increasing breakdown (oxidation), reduc-ing availability from storage (lipolysis), or by increasing FA fluxtoward storage (re-esterification); these distinct strategies havebeen considered as chemotherapeutic strategies recently [119].As with other metabolic shifts in cancer, characterizing the stateof lipid metabolism in unique cancer types and cells lines is animportant first step. Indeed, successful chemotherapeutic strate-gies will require understanding the specific abnormalities in lipidmetabolism for a given cancer type. Targeting lipid metabolism incancer is an emerging idea that warrants further investigation.
7. Epigenetics and oncometabolites
In addition to alterations in metabolism, metabolic repro-gramming mediated by specific oncogenes and tumor suppressorscan impact dynamic regulation of chromatin via post-translationalmodifications. Indeed, increasing evidence indicates that alteredmetabolism can also lead to changes in nutrient-sensitive post-translational modifications. These chemical modifications, suchas O-GlcNAcylation, methylation, and acetylation, can impact theactivities of metabolic enzymes, signaling components, trans-criptional regulators, and chromatin-associated proteins such ashistones [120124]. Furthermore, oncometabolites, such as 2-hydroxyglutarate (2-HG), can have profound consequences onthe regulation of chromatin organization, gene expression, andgenome integrity. Improved understanding of the links betweenmetabolism and epigenetics is expected to have important thera-peutic implications, and intense efforts are currently geared towardtargeting both altered metabolism and epigenetics [125,126].
7.1. O-GlcNAcylation
The hexosamine biosynthetic pathway (HBP), a branchof metabolism that diverges from glycolysis at fructose-6-phosphate, generates uridine diphosphate N-acetylglucosamine(UDP-GlcNAc), a key donor substrate for glycosylation reac-tions, including the O-GlcNAc modification, which is mediated byO-GlcNAc transferase (OGT) [122,127,128]. O-GlcNAcylation is gen-erally elevated in cancer cells and has been linked to malignanttumor growth through direct modification of phosphofructoki-
nase (PFK1) and indirect regulation of FoxM1 [129131]. All fourhistones (H2A, H2B, H3, and H4) are modified by O-GlcNAc,which is dynamically regulated in response to nutrient availabil-ity [132134]. O-GlcNAcylation of histone H3 on Ser10 is cell cycle
Canc
r[uttTlWtf[it
7
icDlusmtmSarktnbidwaoteeltttchlttcon
7
a(Hmirstf
M.D. Hirschey et al. / Seminars in
egulated and suppresses mitosis-specific H3 phosphorylation135], whereas H2B Ser112 O-GlcNAcylation facilitates monoubiq-itylation of Lys120 of histone H2B, a mark associated with activeranscription, indicating a role for O-GlcNAc in gene regulationhrough chromatin modification [134]. OGT can also associate withenEleven-translocation (TET) family 5-methylcytosine hydroxy-ases and participate in TET-mediated gene regulation [136139].
hether cancer cells exhibit altered histone O-GlcNAcylation pat-erns due to metabolic alterations is not yet clear. Notably, TET2unction is frequently disrupted in hematopoietic malignancies140142], and future studies will determine whether changesn histone O-GlcNAcylation participate in cancer development inhese cases.
.2. Methylation
Alterations in histone and DNA methylation are widely observedn cancer. Many cancer types display global DNA hypomethylationompared with normal tissue, while genes regulating cell-cycle andNA damage response are frequently found to be hypermethy-
ated, and thus silenced [143]. Histone and DNA methyltransferasestilize the methyl donor S-adenosyl methionine (SAM), which isynthesized from methionine and ATP. Hence, SAM availability forethylation reactions may be sensitive to levels of methionine
aken up from the environment or synthesized through one-carbonetabolism pathways, discussed in more detail below. In yeast,
AM can serve as a sensor of amino acid availability, inhibitingutophagy and promoting growth [144]. While transformed cellsequire growth medium supplemented with methionine [145],nowledge of how cancer cells use methionine to regulate his-one and DNA methylation is still limited. Notably, the enzymeicotinamide N-methyltransferase (NNMT), which depletes SAMy catalyzing the transfer of SAMs methyl group to nicotinamide,
s frequently overexpressed in human cancers. A recent studyemonstrated that NNMT levels impact methylation in cancer cells,ith NNMT overexpression associated with reduced levels of SAM
nd histone methylation [146]. Interestingly, metabolic regulationf SAM production has also been implicated in modulating his-one methylation levels and maintaining pluripotency in mousembryonic stem cells [147]. In addition to overall cellular lev-ls of SAM, localized pools of SAM may provide an additionalayer of metabolic control. The enzyme methionine adenosyl-ransferase (MATII), which produces SAM, has been localizedo gene promoters and implicated in gene regulation, indicatinghat enzymatic production of metabolites can be targeted to spe-ific loci and coupled to transcriptional regulation [148]. DNA andistone methylation levels are also controlled by rates of demethy-
ation. Metabolic control of demethylation is discussed below inhe Oncometabolites sub-section. Given the substantial evidencehat DNA and histone methylation abnormalities contribute toancer initiation and growth, further investigation into the rolef metabolism in determining methylation changes in cancer iseeded.
.3. Acetylation
Lysine acetylation levels are determined by the combinedctions of lysine acetyltransferases (KATs) and deacetylasesHDACs), both of which may be influenced by metabolic state.istone proteins are acetylated at multiple lysines, and theseodifications are involved in chromatin-dependent processes,
ncluding gene transcription, DNA replication, and DNA damage
epair. In mammalian cells, nuclear-cytosolic acetyl-CoA, the donorubstrate for acetylation reactions, is generated either throughhe cleavage of citrate by ATP-citrate lyase (ACLY) or directlyrom acetate by acetyl-CoA synthetases [122]. Histone acetylationer Biology 35 (2015) S129S150 S137
can be regulated by the availability of glucose or acetyl CoA[149152], and in mammalian cells glucose-dependent regula-tion of histone acetylation occurs in an ACLY-dependent manner[149]. Reciprocally, nuclear-cytoplasmic lysine deacetylation canbe mediated by SIRT1, a member of the NAD+-dependent sir-tuin family of lysine deacetylases [class III histone deacetylases(HDACs)] [153,154]. NAD+ levels rise under nutrient-restrictedconditions, in part mediated by AMP-activated protein kinase(AMPK) [155,156]. In addition, the ketone body -hydroxybutyrate(OHB) was recently demonstrated to function as an endoge-nous inhibitor of class I HDACs under ketogenic conditions andinfluence the state of histone acetylation and gene transcription[157].
Metabolic control of histone acetylation is likely to impact can-cer growth, although this has not yet been directly shown. In yeast,acetyl-CoA acts as a growth signal, promoting histone acetylationat and expression of growth-related genes [151]. Levels of ACLYare frequently elevated in cancer [158], although the impact ofthis on overall histone acetylation is not yet known. Global his-tone acetylation levels are highly heterogeneous among cancers,and several studies have shown correlations with cancer recurrenceand patient survival [159163]. Both KAT and HDAC inhibitors haveshown promise in cancer therapy [125], although mechanisms ofaction remain poorly understood.
7.4. Sirtuin deacylases (SIRTs)
The sirtuins (SIRT1-7) are a class of conserved NAD+-dependentdeacylases that control cellular metabolic processes and protectthe cell against metabolic and genotoxic stresses. Not surprisingly,altered regulation of the sirtuins is associated with many dis-eases such as diabetes, neurodegenerative diseases, obesity, andcancer [164]. Rapidly proliferating cancer cells require shifts inmetabolism that promote anabolic metabolism; as such, the sir-tuins play important roles in controlling cancer development andprogression by maintaining normal cellular metabolism. Of the 7mammalian sirtuins, SIRT1, SIRT3, SIRT4, and SIRT6 have been asso-ciated with various types of cancer. SIRT1, SIRT3, and SIRT6 arestrong deacetylases, while the enzymatic activity of SIRT4 is lessclear but it has been shown to be a weak ADP-ribosyltransferase andpossibly a weak deacetylase [165]. SIRT1 and SIRT6 serve to mainlydeacetylate histones and transcription factors in the nucleus, whileSIRT3 and SIRT4 are mitochondrial, where they act on metabolicproteins [166].
SIRT1 shares the most homology to Sir2 (Saccharomyces cere-visiae), the first sirtuin identified, and has been shown to increaselifespan and protect against age-related diseases. The main targetsof SIRT1 are the transcription factor peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC1), the FOXOfamily of transcription factors, and the tumor suppressor p53 [167].Studies have found that SIRT1 expression is elevated in certain can-cers and repressed in others, making the role of SIRT1 in cancerdifficult to define [168]. It seems as though the main confusionunderlying the role of SIRT1 in cancer is the complexity behindthe SIRT1-mediated inhibitory deacetylation of p53. SIRT1 expres-sion is also positively regulated by p53 in an apparent negativefeedback loop where loss of p53 reduces SIRT1 expression, lead-ing to an increase in p53 activity [169]. SIRT1 has been describedas a tumor suppressor that promotes the DNA damage response,and SIRT1+/ p53+/ mice develop cancer in a variety of tissues,particularly sarcomas. Furthermore, SIRT1 overexpressing mice aremore metabolically efficient, resistant to diabetes, and no cancer
phenotype has been reported in these mice [170]. SIRT1 expres-sion is reduced in various human cancers, particularly breast cancerand hepatocellular carcinoma [171]. Activation of SIRT1 has alreadyproven beneficial in BRCA1-associated breast cancers as treatment
S Canc
wiacD
tSsot[ct2sill1taa
apoMimrlic
aobpfclsaf
tcitmplsseMmB(actsio
138 M.D. Hirschey et al. / Seminars in
ith resveratrol activated SIRT1 and inhibited cell proliferationn vitro and tumor growth in vivo [172]. It seems as thoughctivation of SIRT1 may have therapeutic potential in certain can-ers in order to normalize cellular metabolism and improve theNA damage response.
SIRT3 is the main mitochondrial deacetylase and as such it con-rols the activities of many metabolic enzymes in the mitochondria.IRT3 deacetylates a long list of mitochondrial proteins acting ateveral nodes of mitochondrial metabolism, including fatty acidxidation, glutamine metabolism, and mitochondrial ROS produc-ion. When SIRT3 is lost or ablated, metabolic derangements occur173], which may be the source for the link between SIRT3 andancer. The first described link between SIRT3 and cancer reportedhat SIRT3KO mice spontaneously develop mammary tumors after
years [174]. Furthermore, this study identified SIRT3 as a tumoruppressor by showing that SIRT3 KO MEFs could be transformedn vitro by the addition of a single oncogene, Myc or Ras [174]. Aater study attributed the elevated level of cellular ROS seen withoss of SIRT3 to the stabilization of HIF-1 and activation of HIF- glycolytic target genes, leading to altered cellular metabolismoward glycolysis [175]. It is possible that SIRT3 deficiency leads to
cancer permissive state by coordinating a shift in metabolism to Warburg phenotype.
Cancer cells also rely heavily on the metabolism of glutamine as nitrogen source for protein and nucleotide synthesis necessary forroliferation [28]. SIRT4 was previously found to inhibit the activityf glutamate dehydrogenase (GDH) activity by ADP-ribosylation.ore recently, one study showed that genotoxic stress causes an
nduction of SIRT4 expression leading to a repression of glutamineetabolism [176]. SIRT4 KO MEFs had higher glutamine uptake in
esponse to UV damage and increased glutamine-dependent pro-iferation compared to wild type cells. Finally, SIRT4KO mice hadncreased incidence of various types of cancer, particularly lungancer compared to wild type mice [176].
Finally, SIRT6 controls cancer metabolism and SIRT6 ablationctivates aerobic glycolysis and leads to oncogenesis, in the absencef oncogene activation [177]. This study showed that when aero-ic glycolysis was inhibited by inhibition of PDK1, an inhibitor ofyruvate dehydrogenase (PDH), the SIRT6 deficient cells failed toorm tumors, showing a reliance on glycolytic metabolism of glu-ose. Further, SIRT6 expression is also low in pancreatic, colon, andiver cancers in humans [177,178]. Overall, it seems as though SIRT6uppresses cancer growth by regulating aerobic glycolysis and that
mutator phenotype is not required for SIRT6-dependent tumorormation.
Collectively, these studies show that the loss of an individual sir-uin can promote oncogenesis by creating a state that is favorable toancer cell formation or survival, such as increasing DNA damage,nhibiting DNA repair mechanisms, or altering cellular metabolismoward a Warburg-like phenotype. Modulating sirtuin expression
ay be a way to alter substrate use by cancer cells and slow orrevent their growth. Many of the sirtuins are known to be regu-
ated by nutrient status, therefore it may be beneficial to modulateirtuin expression by diet and/or exercise. SIRT1 and SIRT3 expres-ion are induced with calorie restriction and fasting, and SIRT3xpression is reduced with high fat diet (HFD) feeding [179,180].odulating sirtuin expression through diet, and possibly exercise,ay be useful in combination with conventional cancer therapy.
y combining chemotherapy with calorie restriction or exercisedescribed below), sirtuin expression may be elevated leading to
more normalized cellular metabolism and better control of theancer, possibly increasing the efficacy of the drug therapy. Along
hese lines, efforts aimed at identifying calorie restriction mimetics,imilar in action to resveratrol, have the overall goal of increas-ng the expression or activity of the sirtuins. However, resveratrol,ther CR mimetics, and dietary manipulations are not selective forer Biology 35 (2015) S129S150
a particular sirtuin and may have undesired or off-target affects,and most importantly may not activate the sirtuins robustly. Moreinvestigation into the sirtuins in cancer is clearly needed, and bet-ter ways to selectively target individual sirtuins will be key movingforward.
7.5. One-carbon metabolism
The folate cycle in combination with the methionine cycle arecollectively referred to as the one-carbon metabolism, since car-bon units are circulated through multiple enzymatic reactions.The one-carbon cycle forms a critical component of the cellu-lar metabolic network, which is linked to nearly all of the majorbiosynthetic pathways. The main sources that put carbon units intothis cycle are serine and glycine biosynthetic pathways. Impor-tantly, the fate of the carbons (i.e. outputs) of the one-carboncycle consist of a variety of critical metabolic pathways; for exam-ple, some outputs include nucleotide metabolism [181], proteintranslation [182], lipid metabolism [183], methylation metabolism[121,123,184186], protein sulfhydration, and glutathione produc-tion. Therefore, the activity of the one-carbon cycle is importantin regulating the biosynthesis of the building blocks of a cell aswell as its epigenetic status. Furthermore, the redox state of thecell is regulated by this cycle at two levels: through the folatecycle by the function of tetrahydrofolate (THF), and also throughthe glutathione production via the transulfuration pathway thatmediates the levels of ROS in cells. Both of these mechanisms serveto regulate the balance of NADPH/NADP+ levels in the cell [24].Recently, a variety of cancers were shown to divert carbons fromglycolytic metabolism into the one-carbon cycle, providing a linkfrom the Warburg effect to the activity of one-carbon metabolism[187,188].
For example, phosphoglycerate dehydrogenase (PHGDH) ishyperactivated in a subset of cancers, resulting in over-productionof serine in these cancers [189,190]. Furthermore, the gene encod-ing PHGDH was shown to have undergone significant copy numbergain in some cancers and cancer cell lines, and these cell lineswere dependent on the PHGDH amplification for rapid proliferation[191].
A second instance where one-carbon metabolism has showncorrelations with cell transformation is the metabolism andgeneration of glycine. A metabolomics study on cancer celllines reported a strong association between glycine uptake andcatabolism with cancer cell proliferation [192]. Also another studyfound that ectopic expression of glycine dehydrogenase (GLDC,decarboxylating), phosphoserine aminotransferase (PSAT), andserine hydroxymethyltransferase (SHMT), all enzymes importantin glycine uptake and catabolism, could induce cell growth in NIH3T3 cells, thus conferring to these cells properties indicative of thehallmarks of cancer [193].
Additional levels at which the one-carbon cycle and its out-put pathways have been linked to cancer include nucleotidemetabolism, epigenetic modifications, polyamine metabolism, andthe regulation of the oxidative state of the cell. Multiple genesinvolved in nucleotide metabolism cause transformation by reduc-ing the genomic integrity [194]. Also, through the transfer of methylgroups to proteins, DNA, and RNA, S-adenosyl methionine regulatesprotein activity as well as epigenetic marks on DNA and proteins incells which are all broadly implicated in cancer.
Targeting one-carbon metabolism using folate antagonists haslong been used as a major class of cancer therapeutic agents[195]. Historically, aminopterin was the first one of such drugs,
and methotrexate and pemetrexed are still being used as commonchemotherapeutic agents in a variety of cancers acting to inhibitdi- and tetrahydrofolate reductase activities, thereby disrupting theone-carbon cycle. In addition to this class of compounds, another
Canc
mb5
botomao
dP(gtbpssat
7
mlctIithmmwt[
edidcswtep[mwpOaim(I
Issi
M.D. Hirschey et al. / Seminars in
ajor group of chemotherapeutic agents linked to the one car-on cycle are inhibitors of nucleotide metabolism. These include-fluorouracil (5-FU) and gemcitabine [196].
Furthermore, several novel anti-cancer drugs that are currentlyeing tested in clinical trials also target specific components of thene carbon cycle. These agents mostly target the epigenetic state ofhe cancer cells through inhibiting SAM or DNA methyltransferasesr polyamine synthesis [197]. Difluromethylornithine (DFMO),ethylglyoxal bis(guanylhydrazone) (MGBG), and an inhibitor of S-
denosylmethionine decarboxylase called SAM486A are examplesf such agents.
One carbon metabolism consists of enzymes that are in principleruggable [198]. Therefore, several promising drug targets includeHGDH, PSAT, PSPH, GCAT, GLDC, and glycine N-methyltransferaseGNMT). A recent study has shown that reduction in serine andlycine intake in diet can significantly reduce cancer cell prolifera-ion in mice, suggesting that one carbon metabolism can potentiallye targeted through dietary adjustments [199]. Finally, due to therevalence of anti-metabolite chemotherapeutic agents that areomehow involved with the one carbon cycle, expression levels ofome of the components of this pathway could potentially be useds biomarkers for drug selection and outcome prediction in severalypes of cancers [200,201].
.6. Oncometabolites
Isocitrate dehydrogenases (IDH1 and IDH2) are frequentlyutated in several cancer types, including glioma, acute myeloid
eukemia, and chondrosarcoma [202204], resulting in signifi-ant changes to the epigenetic landscape in cancers harboringhese mutations [120,141,205,206]. The products of wild typeDH1 and IDH2 enzymes, NADPH and -KG, play broad functionsn regulating cellular metabolism. The mutant IDH proteins loseheir wild type function and instead convert -KG into (R)-2-ydroxyglutarate [(R)-2HG], a structural analog of -KG [207]. IDHutant cancer cells can accumulate millimolar levels of this nor-ally undetectable metabolite [207,208]. Recently, mouse modelsith altered IDH2 activity have shown the capacity of IDH muta-
ions to facilitate malignant tumor development and maintenance209,210].
(R)-2HG is thought to act by competitively inhibiting certainnzymes that require -KG as a cofactor, including Jumonji-Comain histone demethylases (JHDMs) and TET proteins, which are
mplicated in DNA demethylation [211,212]. IDH mutant tumorsisplay a hypermethylation signature, associated with a block inellular differentiation [120,141,211]. A similar hypermethylationignature is associated with IDH mutations and TET2 mutations,hich occur in a mutually exclusive manner in AML, indicating that
hese mutations likely target the same pathway [141]. Moreover,ither treatment with (R)-2HG or silencing of TET2 was sufficient toromote growth factor-independent growth of TF-1 leukemia cells213]. However, the epigenetic alterations mediated by (R)-2HG
ay not fully explain its cancer promoting effects, since (S)-2HG,hich is not produced by mutant IDH but serves as an even moreotent inhibitor of TET2 than (R)-2HG, fails to transform TF-1 cells.ne possible explanation is that (R)-2HG, but not (S)-2HG, can act asn agonist for EGLN prolyl hydroxylases, which promote hypoxia-nducible factor (HIF) degradation; hence regulation of HIF proteins
ay also be a part of the malignant tumor-promoting activity ofR)-2HG [213,214]. Indeed, EGLN1 silencing impaired the ability ofDH1 R132H to transform TF-1 cells.
2HG has emerged as a useful diagnostic marker for patients with
DH mutant tumors. Patients with IDH mutant AML exhibit elevatederum 2HG levels, and those with the highest levels of 2HG hadhorter overall survival [215]. Moreover, 2HG can be detected non-nvasively by magnetic resonance spectroscopy in patients wither Biology 35 (2015) S129S150 S139
IDH mutant glioma [216]. Substantial interest has also arisen intherapeutic targeting of mutant IDH enzymes, as a cancer-specificmetabolic alteration. Inhibitors to mutant IDH1 and IDH2 wererecently reported. For example, an IDH2/R140Q inhibitor promotedthe differentiation of leukemia cells containing that mutation [217].An IDH1/R132H inhibitor likewise promoted differentiation andreduced histone methylation in glioma cells. Growth of gliomaxenografts was also impaired. Notably, the tumor growth inhibitoryeffects of the drug were observed at lower doses than were requiredto stimulate histone demethylation and differentiation, furthersuggesting that additional mechanisms may contribute to mutantIDH-mediated malignant tumor growth [218].
In addition to (R)-2HG, succinate and fumarate also have thepotential to act as oncometabolites. In specific cancer types, loss-of-function fumarate hydratase (FH) and succinate dehydrogenase(SDH) mutations are observed, resulting in build-up of fumarateand succinate, respectively. Similar to 2HG, fumarate and succinatecan competitively inhibit -KG-dependent dioxygenases. As such,succinate has been known for several years to promote HIF1 stabi-lization via inhibition of prolyl hydroxylases [219]. More recently, ithas been identified that succinate and fumarate also inhibit histonedemethylases and TET proteins [220]. Both SDH mutant gastroin-testinal stromal tumors and paraganglioma were shown to exhibita hypermethylation phenotype [221,222].
7.7. Lactate
Lactate is made from pyruvate by the enzyme lactate dehydro-genase (LDH) during normal cellular metabolism (Fig. 1). Cancercells produce high levels of lactate, as described above. Morerecently, a new role for lactate has been described wherein somecancer cells use lactate to enable proliferation. For example, ina cancer microenvironment, excess lactate is secreted and con-tributes to an extracellular environment that promotes cancerprogression [223]. Thus, lactate, which was previously considereda waste product of cancer cells, has now been identified as a keymetabolite that plays a direct role in promoting cellular growth.The concept of the role of lactate as a signal or as a fuel in cancer isoften called the reverse Warburg effect [224].
Lactate levels are governed by a number of factors, including dif-ferential expression of LDH isoforms, the lactate monocarboxylatetransporter (MCT) levels, and oxidative capacity of tissues. LDH isthe primary enzyme catalyzing lactate turnover, which intercon-verts pyruvate and lactate, with concomitant interconversion ofNADH and NAD+, respectively. LDH is involved in the metabolismof both glucose and glutamine carbon, as well as in determiningmalignant tumor pH and the activity of the TCA cycle [225]. LDH isclassified into five different subtypes (LDH15), which structurallyconform into homo- or hetero-tetramers of M protein subunitsencoded by LDH isoform A (LDHA) and H protein subunits encodedby LDH isoform B (LDHB) genes. These subtypes vary based of tissuedistribution. For example, in normal tissue, LDH1 has high expres-sion in the brain, heart, and kidney; LDH5 is found in glycolytictissues, such as liver or skeletal muscle [226].
Recently, LDHA was shown to be required for the maintenanceand progression of many cancers [227230], but the mechanismsby which LDHA facilitates cancer progression remain poorly under-stood [231]. Given the correlation between LDHA levels and canceroutcomes, LDHA has attracted attention as a cancer target. Reduc-ing LDHA levels (by shRNA) in cells leads to decreased proliferationand suppressed oncogenicity [227]. Furthermore, inhibition ofLDHA pharmacologically or by siRNA reduces ATP levels and results
in cellular death [228]. A follow-up study examining the com-bination treatment of the LDHA inhibitor FX11 and the NAD+
synthesis inhibitor FK866 resulted in lymphoma regression in axenograft model [228]. Another study found that LDHA plays a role
S Canc
irLrlr
ttdLiiwrt
mwstfltohaao
cowdt
8
ttaetsec
astatfetc
tbctmme
140 M.D. Hirschey et al. / Seminars in
n chemoresistance in breast cancer [232]. Specifically, paclitaxel-esistant breast cancer cells have high expression and activity ofDHA compared to paclitaxel-sensitive cells. Importantly, down-egulation of LDHA restores chemosensitivity, indicating thatactate dehydrogenase, and more broadly lactate levels, play a keyole in cancer drug resistance.
In addition to LDH, MCTs have gained interest as therapeuticargets for their ability to import and export lactate. This family ofransporters moves lactate and a proton down a concentration gra-ient, which determines the directionality of transport. Similar toDH, different MCT isoforms are expressed in tissue types accord-ng to their oxidative capacity [233,234]. For example, MCT1 is highn oxidative cell types like muscle sarcolemma [235], and increases
ith training. MCT4, on the other hand, is found in cells with highates of glycolysis, such as fast-twitch muscle cells. Consistent withhis idea, its expression is increased during hypoxia.
MCTs have also garnered interest as regulators of lactateetabolism. Indeed, inhibition of MCT1, either pharmacologicallyith -cyano-4-hydroxycinnamate (CHC), or by RNA interference,
hifted metabolism from lactate consumption to glucose consump-ion in normoxic cells. Interestingly, this also revealed a metabolicexibility of cancer cells. Some studies have tested MCT1 inhibi-ion in vivo. In one mouse model of lung cancer and in a xenograftf human colorectal adenocarcinoma, CHC administration reducedypoxia, induced tumor necrosis, and slowed overall growth. Innother study, CHC was able to induce anti-tumoral and anti-ngiogenic activity in gliomas, as well as to potentiate the effectf the alkylating agent temozolomide [236].
To conclude this section on emerging metabolic derangementsontributing to cancer cell growth, we end with lactate Warburgsriginal observation. Collectively, these studies support a modelhere metabolites, like lactate, which facilitate malignant tumorevelopment and/or survival, have the potential to be targetedherapeutically.
. Therapeutic strategies
Metabolism is a recent addition to the hallmarks of cancer, andhe nature of these changes and their significance for the etiology ofhe disease are areas of intense investigation. As in other reviews ofHallmarks of Cancer in this special issue, both molecular targetsnd small molecules were evaluated as lead candidates to influ-nce different aspects of cancer metabolism. Each of the priorityargets was outlined in the preceding sections and together areummarized in Table 1. These areas were chosen for their known ormerging mechanisms to contribute to dysregulated metabolism inancer.
A team of researchers consisting of specialists in each hallmarkrea performed an extensive literature search to determine if anytudies had been performed addressing the effect of each moleculararget (Table 1) on other hallmarks. The Target Validation Teamlso looked for any possible reports of effects by the identifiedherapeutic approaches on other hallmarks. Given the interest inuture research that will focus on combinatorial approaches, thisffort was primarily aimed at highlighting any evidence of con-rary effects in other hallmark areas. However, any potential foromplementarity or synergy were also considered as well.
Remarkably, many targets described above as having poten-ial to manipulate different aspects of cancer metabolism have noteen directly tested in the context of other hallmarks. Furthermore,ompounds directed at each molecular target need to be tested for
heir influence on other hallmarks, independent of their effects on
etabolism; this is the current major gap in knowledge. We pri-arily attribute this to the recent resurgence in metabolic studies,
specially in the context of cancer. Indeed, less is known about ifer Biology 35 (2015) S129S150
and how to effectively target cancer metabolism as a therapy than isknown about targeting other hallmarks of cancer. Thus, our analysisat this time shows that prioritized targets and lead compounds thatmight affect these targets need further investigation. With moreresearch, a broad-spectrum approach to target metabolism and tosynergize with other hallmarks of cancer could be achieved.
In the interim, based on current knowledge, we considerfrom a drug development perspective the unique environment ofmitochondria, which needs to be considered to target mitochon-drial function, and ultimately manipulate metabolism. Because ofthe challenges associated with targeting mitochondria, we alsotake a step back from the cellular and biochemical mechanismsof metabolism and discuss how alterations in host metabolismcould more broadly manipulate cancer metabolism in an effica-cious way. Together, considering cancer (direct) and host (indirect)metabolism could uncover novel therapeutic strategies or informa-tion that could be leveraged to target metabolism.
8.1. Strategies to target mitochondria in cancer
Traditionally, mitochondria were not thought of as a Drug-gable Target due to significant challenges unique to mitochondria,including selective delivery to this organelle, specific mitochondrialuptake within a targeted organ, and how to enhance the selectivedelivery to mitochondria within cancer cells; however, recent workis changing this view [237,238]. In part, this is due to the grow-ing realization that mitochondrial function contributes to multiplecellular functions, beyond energy metabolism, and these aspectscould be targeted. The development of strategies to target differentaspects of mitochondrial biology has led to the emergence of a newfield called mitochondrial pharmacology [237,238].
In mitochondrial pharmacology, development of drugs designedto affect mitochondria require the following considerations. Fore-most, mitochondria originate from the coordination of twogenomes, with 37 genes in the mitochondrial DNA and approx-imately 1500 proteins being imported into the mitochondriafollowing their transcription and translation from nuclear genes[239]. The expression of the two genomes is coordinated by anumber of nuclear transcription factors [240]. Targeting nuclear-versus mitochondrial-derived proteins could be important. Fur-thermore, the mitochondria themselves continually join andseparate through fission/fusion processes that are linked tothe turnover and degradation of damaged, defective or surplusmitochondria [241]. Thus, one way for drugs to alter mitochon-drial function is through interaction with the cellular machinerythat controls overall mitochondrial biogenesis. For example, drugssuch as 5-aminoimidazole-4-carboxamide ribonucleotide (AICAR)that interact with the AMP-activated protein kinase (AMPK) [242]may lead to upregulation of global mitochondrial biogenesis. Fur-thermore, agonists for PGC1, a transcriptional co-activator thatregulates gene expression of nuclear encoded mitochondrial pro-teins may do the same [243]. Such strategies may globally altermitochondrial nutrient oxidation or function in therapeuticallyuseful ways in cancer.
More direct strategies have been demonstrated by using drugsthat act on particular targets within mitochondria. For example,dichloroacetate has been explored as an anticancer agent by block-ing the activity of the inhibitory kinase that inactivates pyruvatedehydrogenase, thereby enhancing mitochondrial pyruvate oxida-tion [244]. Generally, in these examples, a drug acts on an aspect ofmetabolism that is mitochondrial and the selectivity comes fromthe interaction of the drug with its target, which happens to be in
the mitochondrion. However, emerging methods are available totarget compounds to mitochondria [237], and these may have anumber of advantages. In particular, the concentration of a com-pound within mitochondria greatly enhances the potency of the
Canc
tlmi
mdoiitoaois
tmmmRgseslfe
8a
ublswmwowioot
8
tspdstsvbiattio
M.D. Hirschey et al. / Seminars in
herapy, meaning far less of a compound might be required. Theocalization of the compound within the mitochondria also mini-
izes metabolism and toxicity associated with reactions elsewheren the body.
An important attribute in designing targeted therapies foritochondria is the distinct mitochondrial compartments, with
ramatically different properties. Most of energy metabolismccurs in the matrix and on the mitochondrial inner membrane. Thentermembrane space has limited metabolic activity, although it ismportant in protein import; this compartment contains many ofhe proteins that are released into the cytoplasm during activationf apoptotic pathways. The mitochondrial outer membrane is also
key component in the regulation of apoptosis. Furthermore, manyf the complexes involved in the propagation and stabilization ofnflammatory pathways are assembled on the cytoplasmic-facingurface of the mitochondrial outer membrane [245].
Overall, the role of mitochondria in cancer is becoming bet-er understood, suggesting that therapies targeted to the organelle
ay be useful [246,247]. Drugs could be designed to affectitochondrial function directly by binding to targets withinitochondria, or indirectly by altering mitochondrial biogenesis.
ecent developments have also led to robust strategies to tar-et bioactive compounds to mitochondria. These approaches mayelectively modify mitochondrial metabolism in cancer cells to gen-rate therapeutically beneficial outcomes, such as enhancing theelective killing or inhibiting growth of cancer cells. While manyimitations and uncertainties with these approaches remain, modi-ying mitochondrial function could become a therapeutically usefulxtension of current cancer treatments.
.2. Strategies to target metabolic interactions between cancernd host
As an alternative strategy, cancer metabolism might be manip-lated specifically through host metabolism. This rationale isased on the concept that pharmacological mimetics of weight
oss, calorie restriction, and/or targeting the associated hormonalystems and intracellular signaling pathways are emerging path-ays for novel cancer therapeutics. Indeed, one of the possibleechanisms underlying known efficacy of fasting, CR, exercise, oreight loss on cancer could be multi-faceted, synergistic effects
f these treatments. Thus, manipulating metabolism in theseays could be a successful therapeutic strategy. Further study-
ng physiological approaches that influence a broad-spectrumf targets and/or hallmarks could inform more effective designf pharmacological approaches aimed at a broad-spectrum ofargets.
.3. Calorie restriction, fasting, and cancer
Calorie restriction (CR), usually referring to a 2040% reduc-ion in the daily intake of calories without malnutrition has beenhown to extend lifespan and healthspan in multiple species, inart by delaying or preventing the occurrence of many age-relatedisorders including cancer [248250]. CR has been also demon-trated to reduce the frequency of spontaneous and inducibleumors in mice and primates [251256]. However, CR inducesignificant weight loss, which has limited its efficacy and has pre-ented its wide-spread clinical use. In some studies, CR delayedut did not stop tumor growth progression, and some tumors
ncluding those carrying a mutation in oncogenes such as PI3Knd phosphatase and tensin homolog (PTEN) have been shown
o be resistant to CR [257]. In addition, CR would be predictedo be incompatible with the treatment of most cancer patientsncluding those malnourished or at risk for severe weight loss,r affected by immunosuppression or cachexia [258]. In fact,er Biology 35 (2015) S129S150 S141
long-term CR can impair immune functions and delay woundhealing repair [259,260]. Thus, while CR might not be compat-ible with cancer therapy in humans, several lessons could belearned from the molecular pathways activated by CR and/or CRmimetics.
More recently, periodic fasting has emerged as a viable strategyto protect normal cells from toxicity associated with chemother-apy, while sensitizing cancer cells to treatment. Remarkably, fastingprotects normal cells from oxidants, common chemotherapeuticagents, and radiotherapy in several in vitro and in vivo models[261263]. Specifically, glucose and serum starvation in vitro anda 4872 h food deprivation (short-term starvation or STS) in miceactivated several stressresponse pathways that conferred resis-tance to oxidative stress induced by chemotherapy. The latter effectwas termed differential stress resistance (DSR) [264], and is basedon the concept that normal cells can adapt to stressors but not can-cer cells [265]. The mechanisms responsible of starvation-inducedDSR in mammals include reduced circulating insulin-like growthfactor 1 (IGF-1) levels and possible down-regulation of growthpathways [264]. In addition, in normal mammalian cells, starva-tion has been demonstrated to induce AMPK which stabilized p53and p21 thereby resulting in cell proliferation arrest [262].
In model organisms, including bacteria and yeast, the switchfrom nutrient rich media to water or buffer extends longevityand also increases resistance to a variety of toxins, including ROS[261,266,267]. In yeast cells, the molecular mechanisms respon-sible for fasting-mediated protection involve the reduced activityof components of the glucose-response Ras/cAMP/PKA pathwayand of the amino acids response Tor/S6K pathway [266,268,269].Similarly, fasting increases resistance to oxidative stress and pro-longs life-span in model organisms, such as worms and flies, bydown-regulating analogous nutrient-sensing pathways such as(PI3K/AKT/TOR) [270,271].
Cancer cells are characterized by the presence of oncogenicmutations in the same growth signaling pathways including IGF1receptor, PI3K, PTEN, Ras, and PKA that prevent the activation ofprotective systems in response to starvation (DSR) [1]. In additionto the absence of a stress resistant response to starvation, the setof mutations and chromosomal rearrangements prevent malignantcells from being able to adapt to a wide variety of conditions butparticularly to those that involve broad and extreme changes suchas starvation. Thus, differential stress sensitization (DSS) takesadvantage of the fact that most mutations reduce the ability ofcells to withstand changing environments. In one study, 4860 hof fasting retarded malignant tumor growth, similar to chemother-apy, and acted in synergy with chemotherapeutic drugs in killinga wide variety of cancer cells [264]. In mouse models for breastcancer, neuroblastoma, mesothelioma, and lung carcinoma, thecombination of fasting and chemotherapy promoted 2060% can-cer free survival, whereas neither one of them alone resulted in anycancer free survival [262,264]. Investigation of the molecular mech-anisms underlying the STS-mediated biological effects indicate thatbreast cancer cells attempt to compensate for the nutrient defi-

















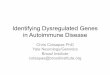






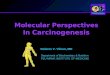



![Oncogenesis Virica Y Microbiana J(1)[1]](https://img.pdfslide.net/doc/110x75/5563f160d8b42ae33c8b4a49/oncogenesis-virica-y-microbiana-j11.jpg)
