Embed Size (px)
Citation preview

Early Stage, Favorable Hodgkin
Lymphoma

How Would You Manage This Patient?
• 28 year old female, asymptomatic except for an enlarged left neck node (2 cm)
• There was no change with a course of antibiotics, an FNA was unhelpful, and excisional biopsy showed classical Hodgkin lymphoma, nodular sclerosingsubtype
• CBC and chemistry screen were normal, ESR was 15, and a PET scan showed only one residual hyper-metabolic node (SUV 7) in the left neck

How Would You Manage This Patient?1. ABVD x 2 cycles + 20 Gy radiotherapy2. ABVD x 2 cycles PET if negative ABVD x 1 cycle3. ABVD x 2 cycles PET if negative ABVD x 1 cycle
+ 30 Gy radiotherapy4. ABVD x 4 cycles PET if negative no more
treatment5. ABVD x 4 cycles + 30 Gy radiotherapy6. AVD x 6 cycles

What Is Early Stage Hodgkin Lymphoma?
• Ann Arbor stage 1 and 2, +/- E lesions
• Some would exclude very large masses

What Is Favorable, Early Stage Hodgkin Lymphoma?
Mass Individual HistologicGroup Size Sites ESR Types OtherGSHG No large <3 nodal <30 - -
mediastinal mass areas; no extranodal sites
NCI Canada/ No mass <4 nodal sites, <50 Nodular sclerosis Age <40>10 cm, no no intra-abdominal and lymphocytelarge mediastinal disease predominantmass
EORTC - - - - Complicatedscoring system
NCI Milan No large nodal or - - - No B symptomsmediastinal mass
Dana Farber No large nodal or - - - -mediastinal mass

Issues In Treating Patients With Favorable, Early Stage Hodgkin Lymphoma
• Cure rate generally >90%• In some series more deaths from treatment toxicity
than from lymphoma• Recent emphasis has been on reducing/eliminating
radiotherapy (thought to be the major contributor to late toxicity)
• Interim PET to direct therapy intensity/duration currently popular

7Armitage JO. N Engl J Med. 2010;363(7):653-662.

Omitting Radiotherapy In Early PET Negative Stage1/2 Hodgkin Lymphoma (EORTC/LYSA/FIL)• Standard arm - ABVD x 2 PET ABVD x 1 and 30
Gy radiotherapy
• Experimental arm - ABVD x 2:If PET negative ABVD x 2If PET positive BEACOPP x2 + 30 Gy radiotherapy
André MPE, et al. J Clin Oncol. 2017;35(16):1786-1794.

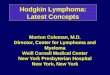
Omitting Radiotherapy In Early PET Negative Stage1/2 Hodgkin Lymphoma (EORTC/LYSA/FIL)
• Considering only early PET negative patients (i.e., ABVD x 3 + radiotherapy vs ABVD x4)
• Group Events p valueStandard 1 .017Experimental 9
André MPE, et al. J Clin Oncol. 2017;35(16):1786-1794.

Omitting Radiotherapy In Early PET Negative Stage1/2 Hodgkin Lymphoma (EORTC/LYSA/FIL)
André MPE, et al. J Clin Oncol. 2017;35(16):1786-1794.

Omitting Radiotherapy In Early PET Negative Stage1/2 Hodgkin Lymphoma (EORTC/LYSA/FIL)
André MPE, et al. J Clin Oncol. 2017;35(16):1786-1794.

Omitting Radiotherapy In Early PET Positive Stage1/2 Hodgkin Lymphoma (EORTC/LYSA/FIL)
André MPE, et al. J Clin Oncol. 2017;35(16):1786-1794.

Conclusions:1. There was a higher relapse rate without
radiotherapy.2. Early stage, favorable patients should all have
radiotherapy.3. Patients with a positive interim PET benefit from
BEACOPP
Omitting Radiotherapy In Stage1/2 Hodgkin Lymphoma (EORTC/LYSA/FIL)
André MPE, et al. J Clin Oncol. 2017;35(16):1786-1794.

Reduced Treatment Intensity In Patients With Favorable Early Stage Hodgkin Lymphoma (GHSG)
Treatment regimens (all combined modality):Regimen ABVD (cycles) Radiotherapy (Gy)
1 4 302 4 203 2 304 2 20
Engert A, et al. N Engl J Med. 2010;363(7):640-652.

Reduced Treatment Intensity In Patients With Early Stage Hodgkin Lymphoma (GHSG)Treatment outcome:Regimen 8-year PFS 8-year OS
1 88% 94%2 90% 95%3 85% 94%4 87% 95%
Engert A, et al. N Engl J Med. 2010;363(7):640-652.

• Since there was no difference in outcome, ABVD x 2 and 20 Gy should be the standard approach to patients with early stage, favorable Hodgkin’s lymphoma.
Reduced Treatment Intensity In Patients With Favorable Early Stage Hodgkin Lymphoma (GHSG)
Engert A, et al. N Engl J Med. 2010;363(7):640-652.

Omitting Dacarbazine, Bleomycin, or Both From ABVD In Early Stage Favorable Hodgkin Lymphoma (GHSG)
Treatment regimens:Regimen Chemotherapy Radiotherapy (Gy)
1 ABVD x 2 302 ABV x 2 303 AVD x 2 304 AV x 2 30
Behringer K, et al. Lancet. 2015;385(9976):1418-1427.

Omitting Dacarbazine, Bleomycin, or Both From ABVD In Early Stage Favorable Hodgkin Lymphoma (GHSG)Treatment outcome: Hazard ratioRegimen CR Rate 5-Year FFTF Compared to ABVD
1 97% 93% --2 96% 81% 2.063 98% 89% 1.504 89% 77% 2.57
Behringer K, et al. Lancet. 2015;385(9976):1418-1427.

Conclusion:• ABV and AV have significantly worse
outcome• Non-inferiority was not shown for AVD
Omitting Dacarbazine, Bleomycin, or Both From ABVD In Early Stage Favorable Hodgkin Lymphoma (GHSG)
Behringer K, et al. Lancet. 2015;385(9976):1418-1427.

PET Directed Therapy For Early Stage Hodgkin Lymphoma (RAPID Study, UK)
• Not all patients favorable by GHSG and EORTC criteria (~67%)
• Patients up to 75 years of age were included• A complete remission by PET was Deauville 2 (<
mediastinum) rather than the more commonly used but less stringent Deauville 3 (< liver)
• Non-inferiority was originally a 3 year PFS within 10% of the radiotherapy arm, but was later changed to 7%

• ABVD x 3 PET• If PET negative randomized to 30 Gy radiotherapy
versus no further therapy• If PET positive ABVD x 1 and 30 Gy radiotherapy
NEJM 2015; 372: 1598
PET Directed Therapy For Early Stage Hodgkin Lymphoma (RAPID Study, UK)

Treatment Outcome:Event Radiotherapy Observation Positive PETPFS 92% 89% 88%
Progression 4% 10% 7%Died WithoutProgression 2% 1% 2%
PET Directed Therapy For Early Stage Hodgkin Lymphoma (RAPID Study, UK)
Radford J, et al. N Engl J Med. 372(17):1598-1607.

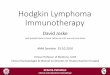
Kaplan–Meier Plots of Progression-free Survival (PET negative patients)
Radford J, et al. N Engl J Med. 372(17):1598-1607.

PET Directed Therapy For Early Stage Hodgkin Lymphoma (RAPID Study, UK)
Radford J, et al. N Engl J Med. 372(17):1598-1607.

PET Directed Therapy For Early Stage Hodgkin Lymphoma (RAPID Study, UK)
Conclusions:1. No difference in OS and marginal difference in
PFS with ABVD alone.2. It is reasonable to treat an early stage patient with
a brief course of ABVD if they have a negative interim PET (i.e., Deauville 2) and want to avoid the long term toxicity of radiotherapy
Radford J, et al. N Engl J Med. 372(17):1598-1607.

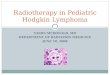
Declining Use Of Combined Modality Therapy In Early Stage Hodgkin Lymphoma In the USASource Time Frequency
National CancerDatabase 2003-2011 54% 45%
National CancerDatabase 2000-2012 53% 37%
Olszewski AJ, et al. J Clin Oncol. 2015;33(6):625-633. Goyal G, et al. Clin Lymphoma Myeloma Leuk. 2016;16(1):12-17.

How Would You Manage This Patient?1. ABVD x 2 cycles + 20 Gy radiotherapy2. ABVD x 2 cycles PET if negative ABVD x 1 cycle3. ABVD x 2 cycles PET if negative ABVD x 1 cycle
+ 30 Gy radiotherapy4. ABVD x 4 cycles PET if negative no more
treatment5. ABVD x 4 cycles + 30 Gy radiotherapy6. AVD x 6 cycles

Conclusions:
1. Eliminating radiotherapy yields a slightly higher relapse rate, but no clear survival difference.
2. However, follow-up in most studies is relatively short and eventual deaths from treatment toxicity and relapsed Hodgkin lymphoma may be underestimated.
3. New therapies (e.g. PD-1 blockers and brentuximab vedotin) might change things.
4. Today a reasonable physician could recommend, or not, a regimen containing radiotherapy – but the final decision should depend on the patient’s preference.