-
8/7/2019 ECG Interpretation Jocelyn
1/46
-
8/7/2019 ECG Interpretation Jocelyn
2/46
What is ECG ?
The electrocardiogram (ECG or EKG) is a noninvasive test that
is
used to reflect underlying heart conditions by measuring
theelectrical activity of the heart. By positioning leads
(electricalsensing devices) on the body in standardized locations,
informationabout many heart conditions can be learned by looking
for
characteristic patterns on the ECG.
-
8/7/2019 ECG Interpretation Jocelyn
3/46
General information
Purpose ofECG- To detect heart problems orblockages in the
coronary arteries.
- To draw a graph ofthe electrical impulses moving through the
heart
- Torecord heart rate and regularityofheart beats
- To diagnose a possible heart attack orotherheart disorders
Discomfort / painHow longWho does itWhere its done
-No pain-5 minutes-Technician
-Nurse
-Doctor
- Doctor office orclinic
- At hospitalbedside
Average costRisk/complicationSpecial equipmentResult reading
when
$$$$$-None-ECG machine
-Electrodes
-Alcohol or gel
-Immediately
-
8/7/2019 ECG Interpretation Jocelyn
4/46
Electrodes placementElectrode placement forprecordialleads
(for12-lead ECG option)
V1 4th intercostal space, right ofsternum
V2 4th intercostal space, left ofsternum
V3 Midwaybetween V2 and V4
V4 5th intercostal space, in the midclavicularline
V5 Same level as V4, at anterioraxillaryline (between V4 and
V6)
V6 In 5th intercostal space, in the midaxillaryline
Red Right arm
Black Right leg
yellow left arm
Green left leg
-
8/7/2019 ECG Interpretation Jocelyn
5/46
-
8/7/2019 ECG Interpretation Jocelyn
6/46
Chambers of the heartA Atria
The left and right atria are separated by theinteratrial
septum.
Right atrium: receives deoxygenatedsystemic blood from the SVC,
IVC, andthe coronary arteries
Left atrium: receives oxygenated bloodreturning from the lungs
via the 4pulmonary veins.
B- Ventricles
Are at higher pressure for pumping bloodinto the pulmonary and
the systemiccirculation
Right ventricle: receives blood from theright atrium and
contracts to eject bloodinto the pulmonary circulation via
thepulmonary artery.
Left ventricle: receives blood from theleft atrium and contracts
to eject blood
into the systemic circulation via the aorta
-
8/7/2019 ECG Interpretation Jocelyn
7/46
Impulse Conduction & the ECG
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers
-
8/7/2019 ECG Interpretation Jocelyn
8/46
Pacemaker of the heart
What is a naturalpacemaker?
The heart's "natural" pacemaker is called the sinoatrial (SA)
node orsinus node. It's a small mass of specialized cells in the
top of theheart's right atrium (upper chamber). It makes the
electricalimpulses that cause your heart to beat.
A chamber of the heart contracts when an electrical impulse
movesacross it. For the heart to beat properly, the signal must
traveldown a specific path to reach the ventricles, the heart's
lower(pumping) chambers.
The natural pacemaker may be defective, causing the heartbeat
tobe too fast, too slow or irregular. The heart's electrical
pathwaysalso may be blocked.
-
8/7/2019 ECG Interpretation Jocelyn
9/46
Pacemaker of the heart
SA Node : Dominant pacemaker
Rate : 60 100 Beats / minute
< 60 bradycardia > 100 tachycardia
AV Node : Back up pacemaker
Rate : 40 - 60 Beats / minute
> 60 accelerated junctional rhythm
> 100 junctional tachycardia
Ventricularcells : Back up pacemaker
Rate :
-
8/7/2019 ECG Interpretation Jocelyn
10/46
The PQRST
P wave - Atrialdepolarization
T wave - Ventricularrepolarization
QRS -Ventriculardepolarization
-
8/7/2019 ECG Interpretation Jocelyn
11/46
How to read an ECG ?
The ECG paper
Horizontally:One small box - 0.04 secOne large box - 0.20
sec
Vertically:One large box - 0.5 mV
-
8/7/2019 ECG Interpretation Jocelyn
12/46
When you are holding an ECG stripin your hand get a quick
look,
and while looking at it
answer these questions.
The 5 steps to interpret an ECG
-
8/7/2019 ECG Interpretation Jocelyn
13/46
1- Rate = Rapid ? or Slow ?
1 big box = 3oo beats / min ( duration 0.2sec )
2 big boxes = 150 beats / min ( duration 0.4sec )
3 big boxes = 100 beats / min ( duration 0.6 sec )
4 big boxes = 75 beats / min ( duration 0.8 sec )
5 big boxes = 60 beats / min ( duration is 1.0 sec )
6 big boxes = 50 beats / min
How to determine the rate
-
8/7/2019 ECG Interpretation Jocelyn
14/46
2 - Rhythm = Regular? or Irregular?
If it is regular if the number of large boxes between QRS
complexes isthe same all over the strip. If not, then the rhythm
may be irregular
Regular rhythm Irregular rhythm
-
8/7/2019 ECG Interpretation Jocelyn
15/46
3 - P wave
Look at the rhythm and ask yourself:
- Are Pwaves present?
- Do P waves have a normal shape - usually upright and rounded
on the rhythmstrip?
- Are all the P waves similar in size and shape?- Do all the P
waves point in the same direction?
P wave absent Inverted P wave
-
8/7/2019 ECG Interpretation Jocelyn
16/46
4 - QRS complexLook at the QRS and ask yourself
- Are all the complexes the same size and shape?
- What is the duration of the QRS complex? (Normal duration is
no more than 0.10-0.12 seconds (3 smallboxes); if greater, it
indicates a Bundle Branch Block(BBB) or originating from the
ventricles)
- Are all the QRS complexes the same distance from the T waves
that follow them?
- Do all the QRS complexes point in the same direction?
- Are any QRS complexes present that appear different from the
other QRS
complexes on the strip? If so, measure and describe each one
individually.
-
8/7/2019 ECG Interpretation Jocelyn
17/46
5 - PR intervalLook at the P to R interval and ask yourself
- What is the duration of the PR interval? (Normal 0.12 to 0.20
seconds)- Is the PR interval constant?
Note: if PR >0.20 sec Atrio-Ventricular Block
if PR < 0.12 sec Presence of an accessory pathway (Wolf
Parkinson white Syndrome)
The P to R interval represents the time it takes an impulse to
travel from the atria
through the AV node, bundle of His, and bundle branches to the
Purkinje's fiber.Location :The P to R interval extends from the
beginning of the P wave to thebeginning of the QRS complex.Duration
:0.12 to 0.20 seconds .The P to R interval is important in order to
determine if there's a heart block orconduction system disease.
-
8/7/2019 ECG Interpretation Jocelyn
18/46
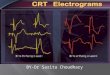
WolfParkinson White Syndrome
Delta wave
&
PR < 0.12 sec
Accessorypathwaybetween the left Atria & the left
Ventricle(Bundle ofKent)
-
8/7/2019 ECG Interpretation Jocelyn
19/46
BLOCKS
AV block-A
degree AV blockst1-1
to themarriedP present all the time & isfollowing QRS only
the PR interval is >0.20sec or 1 large Box
-
8/7/2019 ECG Interpretation Jocelyn
20/46
degree AV blocknd2-2
1degree Mobitznd
2-I
The PR interval is progressively widened until a P isdropped ( P
without a QRS )
:2degree Mobitznd2-II
The PR interval is constant (may be normal orwidened) until
suddenly a P is dropped (P without aQRS) and it is more dangerous
than the Mobitz 1
-
8/7/2019 ECG Interpretation Jocelyn
21/46
degree AV block orrd3-3
Complete Heart Block
There is a complete dissociation between the Atria &
theVentricles, there is no relation between the Ps & the
QRSs
The Atria have their own rate (faster) & the Ventricles
have
their own rate (slower)
-
8/7/2019 ECG Interpretation Jocelyn
22/46
(BBB)Bundle Branch Blocks-B
These are blocks within the ventricular bundlesmainly consist of
Left & Right Bundle BranchBlocks.
-
8/7/2019 ECG Interpretation Jocelyn
23/46
The Key to recognizing a Bundle Blockis to find an R-R wave
.
:The criteria consist of
QRS > 0.12 sec
&
Presence of2 R waves (R-R)
-
8/7/2019 ECG Interpretation Jocelyn
24/46
Right Bundle Branch Block (RBBB)-1
In the RBBB the Right Ventricular firing islate.
The QRS complex will be a QRRS complex
In V1-V2
R=Left Ventricular Depolarization
R=Delayed Right Ventricular Depolarization(Lead V1)
-
8/7/2019 ECG Interpretation Jocelyn
25/46
Left Bundle Branch Block LBBB-2
In the LBBB the Left Ventricular firing isdelayed
The QRS complex will be a QRRS complex
In V5-V6
R= Right Ventricular Depolarization
R=Delayed Left Ventricular Depolarization(Lead V5)
-
8/7/2019 ECG Interpretation Jocelyn
26/46
ST Elevation
One way todiagnose anacute MI is tolook for:Elevation ofthe
ST segment.
-
8/7/2019 ECG Interpretation Jocelyn
27/46
ST Elevation (cont)
Elevation of the STsegment (greaterthan 1 small box)in 2 leads
isconsistent with amyocardial
infarction.
-
8/7/2019 ECG Interpretation Jocelyn
28/46
-
8/7/2019 ECG Interpretation Jocelyn
29/46
-
8/7/2019 ECG Interpretation Jocelyn
30/46
Do you think this person is having a myocardial
infarction. If so, where?
-
8/7/2019 ECG Interpretation Jocelyn
31/46
Interpretation
Yes, this person is having an acute anteriorwall myocardial
infarction.
-
8/7/2019 ECG Interpretation Jocelyn
32/46
Other MI Locations
Now that you know where to look for ananterior wall myocardial
infarction letslook at how you would determine if the MIinvolves
the lateral wall or the inferior wallof the heart.
-
8/7/2019 ECG Interpretation Jocelyn
33/46
Other MI Locations
First, take alook at thispicture oftheheart.
Anterior
portion of the
heart
Lateral portion
of the heart
Inferior portion
of the heart
-
8/7/2019 ECG Interpretation Jocelyn
34/46
Other MI Locations
LimbLeads: I, II & III Augmented Leads
AVR, AVL & AVF
PrecordialLeads
V1 V6
-
8/7/2019 ECG Interpretation Jocelyn
35/46
Anterior MI
Remember the anterior portion of the heartis best viewed using
leads V1- V4.
LimbLeads Augmented Leads PrecordialLeads
-
8/7/2019 ECG Interpretation Jocelyn
36/46
Lateral MI
So what leads doyou
lateralthink the
ofthe heartportion
is best viewed?
LimbLeads Augmented Leads PrecordialLeads
Leads I, aVL, and V5- V6
-
8/7/2019 ECG Interpretation Jocelyn
37/46
Inferior MI
Now how aboutinferiorthe
oftheportion
heart?
Leads II, III and aVF
-
8/7/2019 ECG Interpretation Jocelyn
38/46
Putting it all Together
Now, where do you think this person ishaving a myocardial
infarction?
-
8/7/2019 ECG Interpretation Jocelyn
39/46
Inferior Wall MI
. Note the ST elevationinferiorMIThis is anin leads II, III and
aVF.
-
8/7/2019 ECG Interpretation Jocelyn
40/46
How about now?
-
8/7/2019 ECG Interpretation Jocelyn
41/46
Anterolateral MI
wallanteriorthebothThis persons MI involves)!aVL, and,
I6V-5Vwall (lateral) and the4V-2V(
-
8/7/2019 ECG Interpretation Jocelyn
42/46
My Questions
Please interpret the following rhythms
-
8/7/2019 ECG Interpretation Jocelyn
43/46
-
8/7/2019 ECG Interpretation Jocelyn
44/46
-
8/7/2019 ECG Interpretation Jocelyn
45/46
-
8/7/2019 ECG Interpretation Jocelyn
46/46