Embed Size (px)
Citation preview
HOW TO READ ELECTROCARDIOGRAPHY
Department of Cardiology and Vascular MedicineFaculty of Medicine University of Indonesia
National Cardiovascular Center Harapan Kita
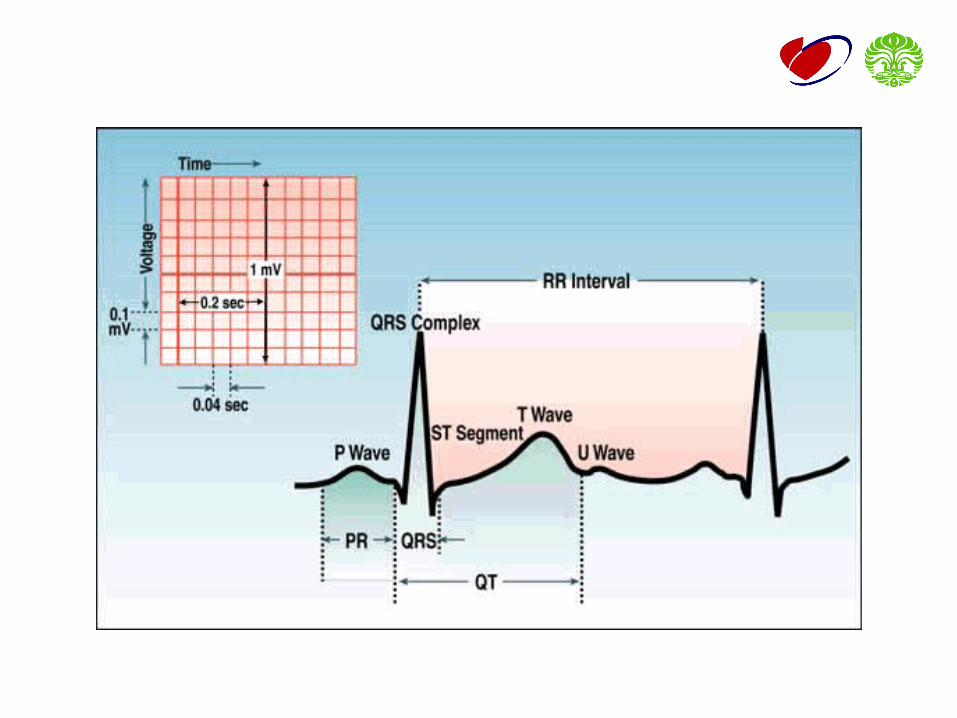
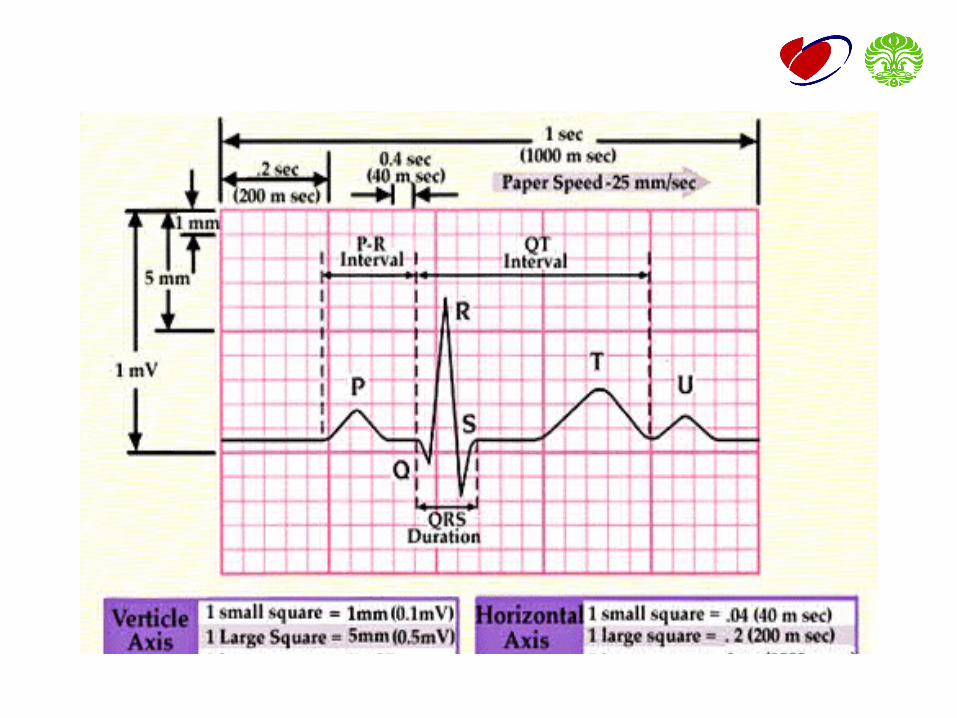
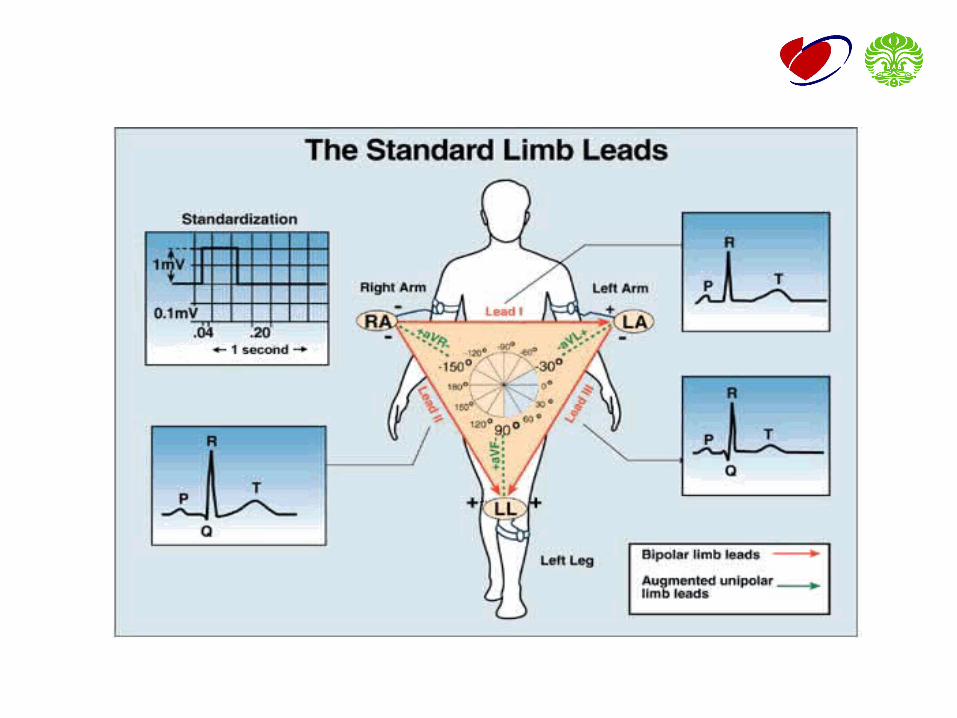
STANDARISASI EKG
• Kecepatan kertas standard EKG• 25 mm / s (10 – 25 – 50 mm / s
• Setiap kolom horizontal = 0.04 sec• Setiap kolom vertikal 10 mm = 1 mV
PEMASANGAN ELEKTRODE
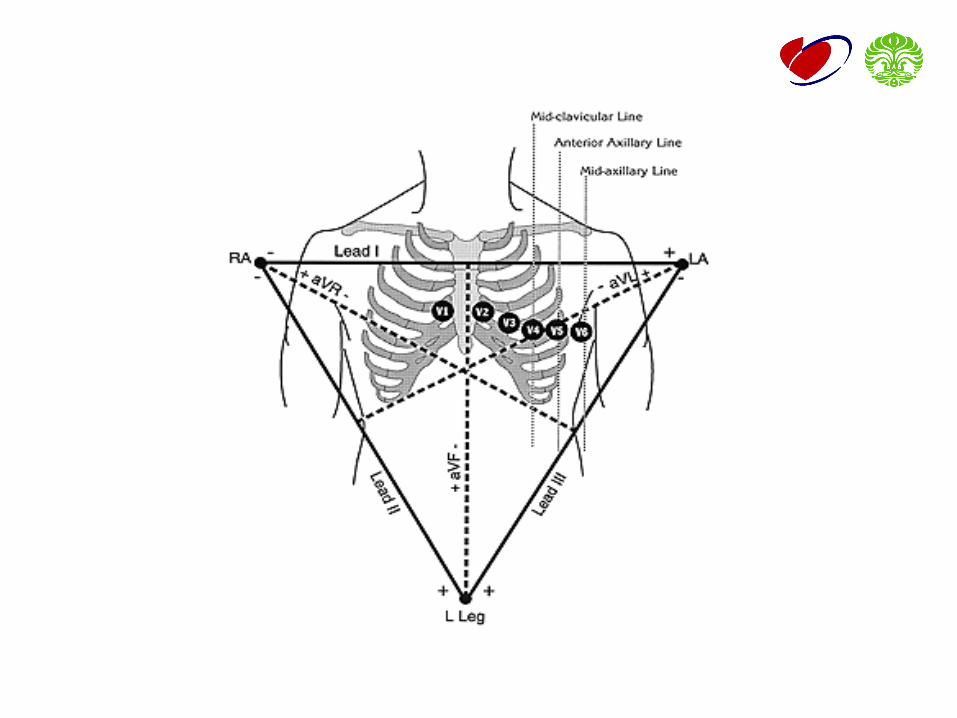
• PEMASANGAN ELEKTRODE EXTREMITAS• Lengan kanan dan lengan kiri• Kaki kanan dan kaki kiri
• PEMASANGAN ELEKTRODE DADA• V1 = Parasternal kanan di ICS-4• V2 = Parasternal kiri di ICS-4• V4 = MCL kiri di ICS-5• V3 = Median antara V2 dgn V4• V5 = Para Axillair Line kiri di ICS-5• V6 = Median Axillair kiri di ICS-5
SISTEM LEADS
• STANDARD LIMB LEADS • I, II, III
• AUGMENTED UNIPOLAR LIMB LEADS • aVR, aVL, aVF
• UNIPOLAR CHEST LEADS• V1, V2, V3, V4, V5, V6 • V3R, V4R, V5R, V6R• V7, V8, V9• V7R, V8R, V9R

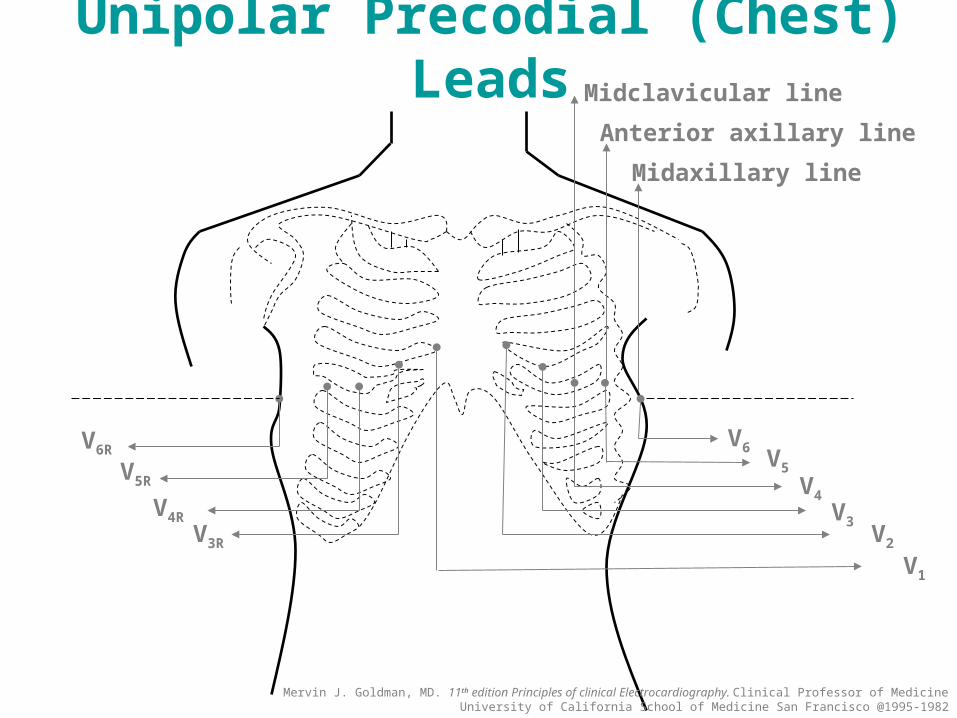
V6V5
V4 V3
V2
V1
V6R
V5R
V4R V3R
Midclavicular line
Anterior axillary line
Midaxillary line
Unipolar Precodial (Chest) Leads
Mervin J. Goldman, MD. 11th edition Principles of clinical Electrocardiography. Clinical Professor of Medicine University of California School of Medicine San Francisco @1995-1982
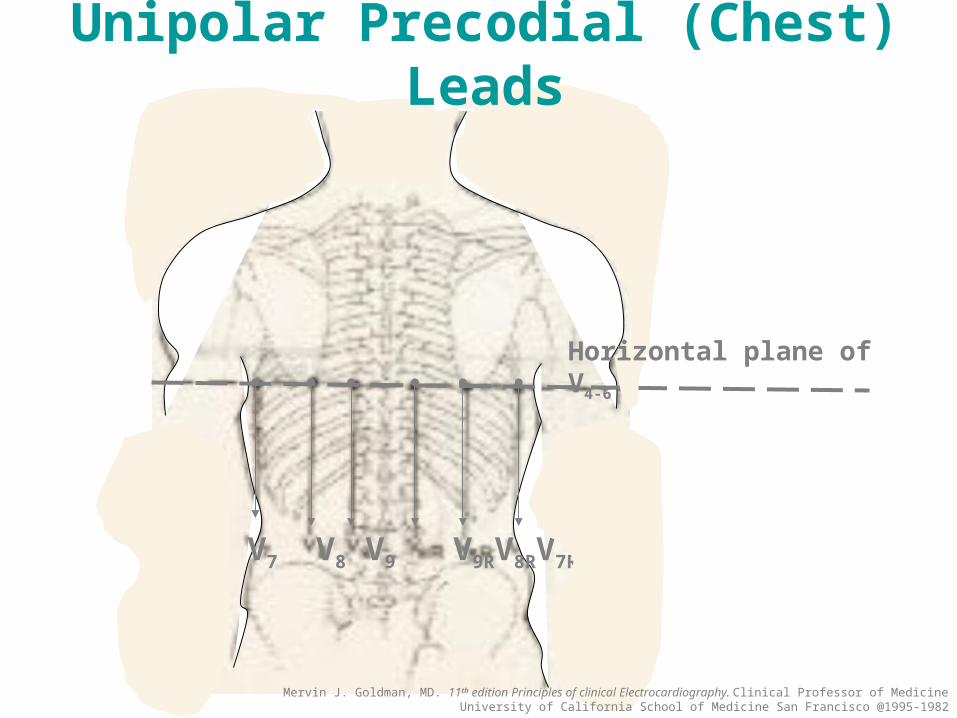
V7 V8 V9 V9RV8RV7R
Horizontal plane of V4-6
Unipolar Precodial (Chest) Leads
Mervin J. Goldman, MD. 11th edition Principles of clinical Electrocardiography. Clinical Professor of Medicine University of California School of Medicine San Francisco @1995-1982
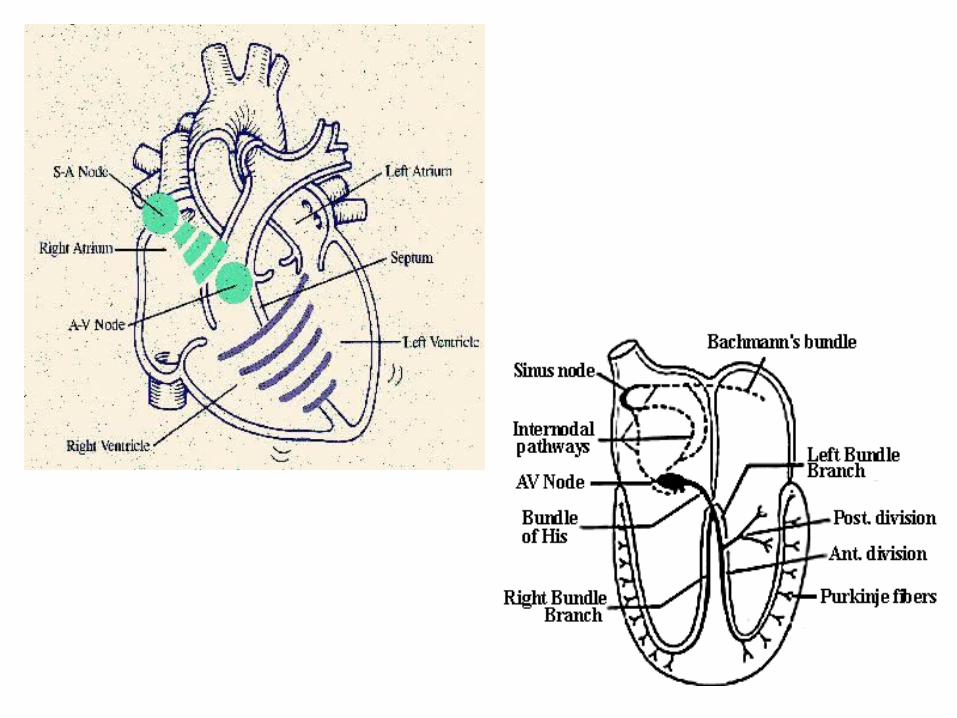
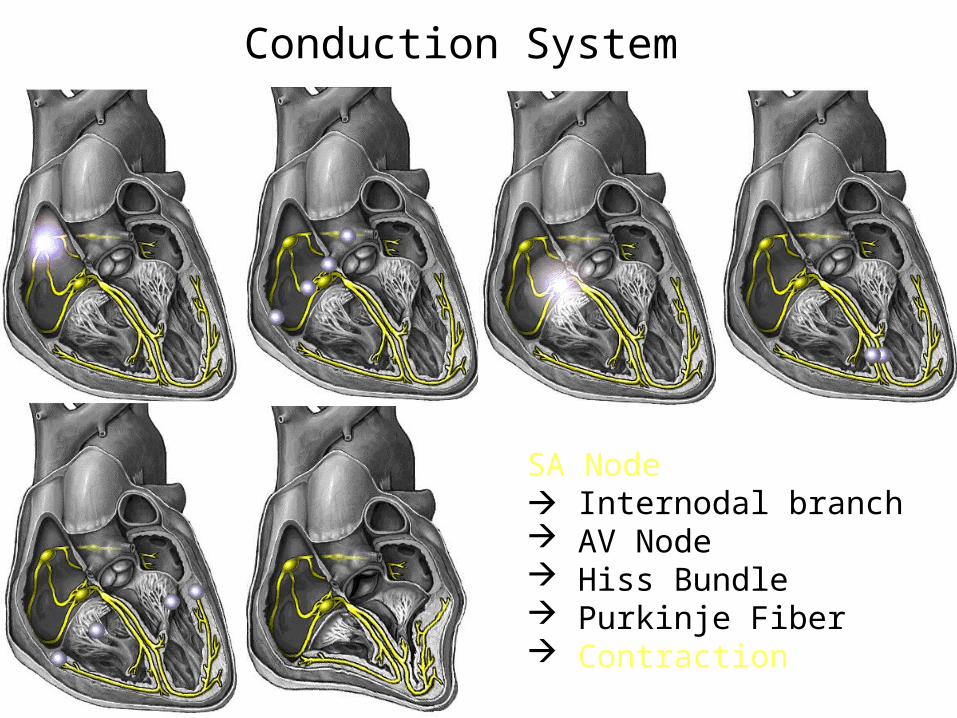
Conduction System
SA Node Internodal branch AV Node Hiss Bundle Purkinje Fiber Contraction
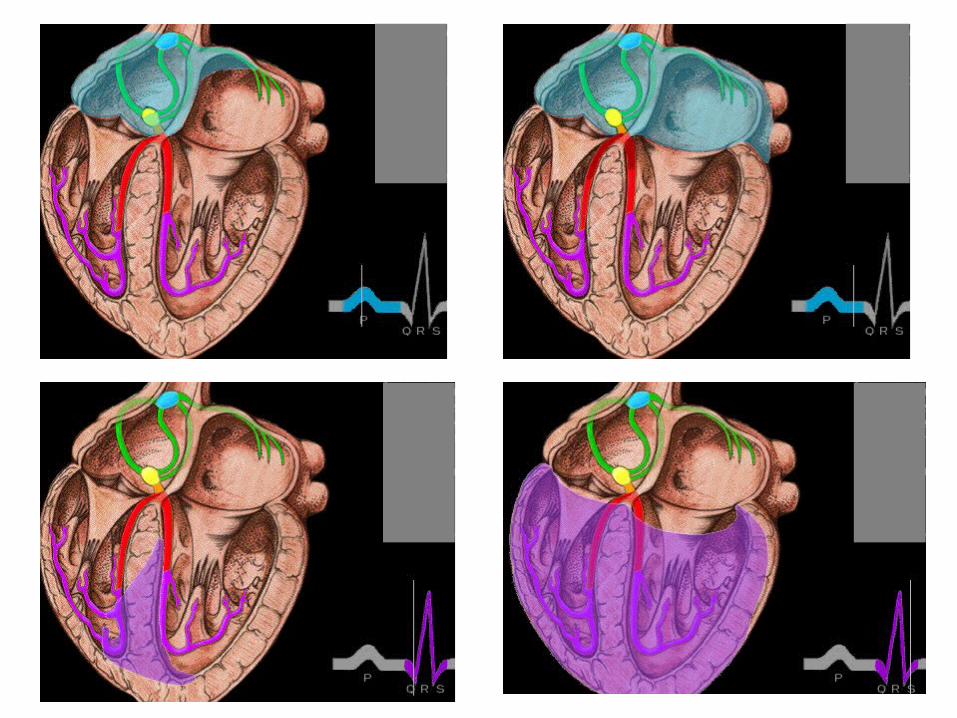
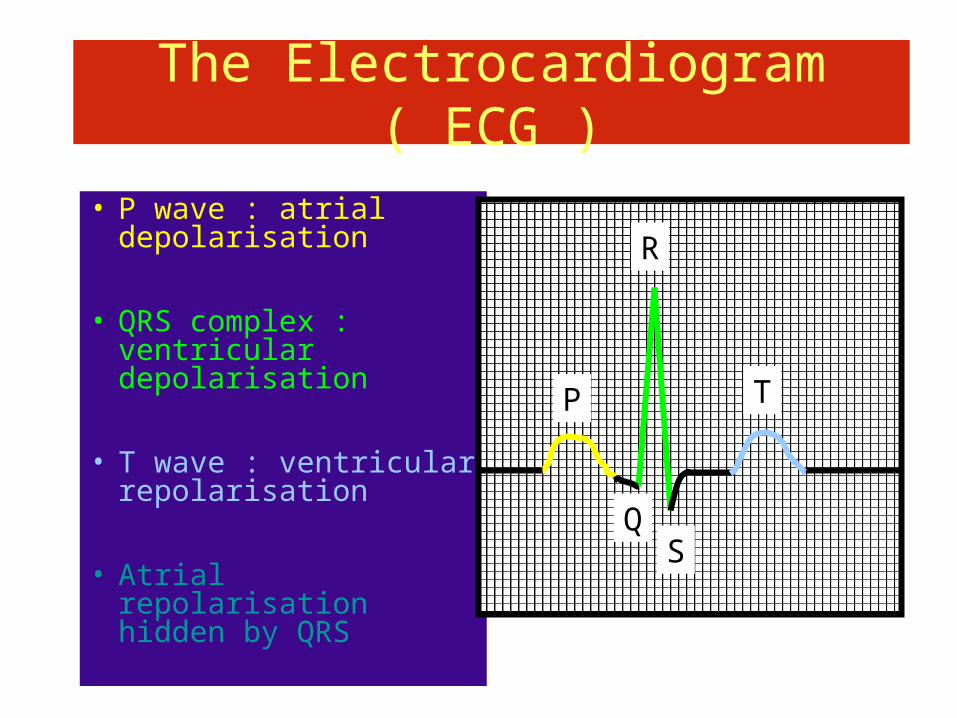
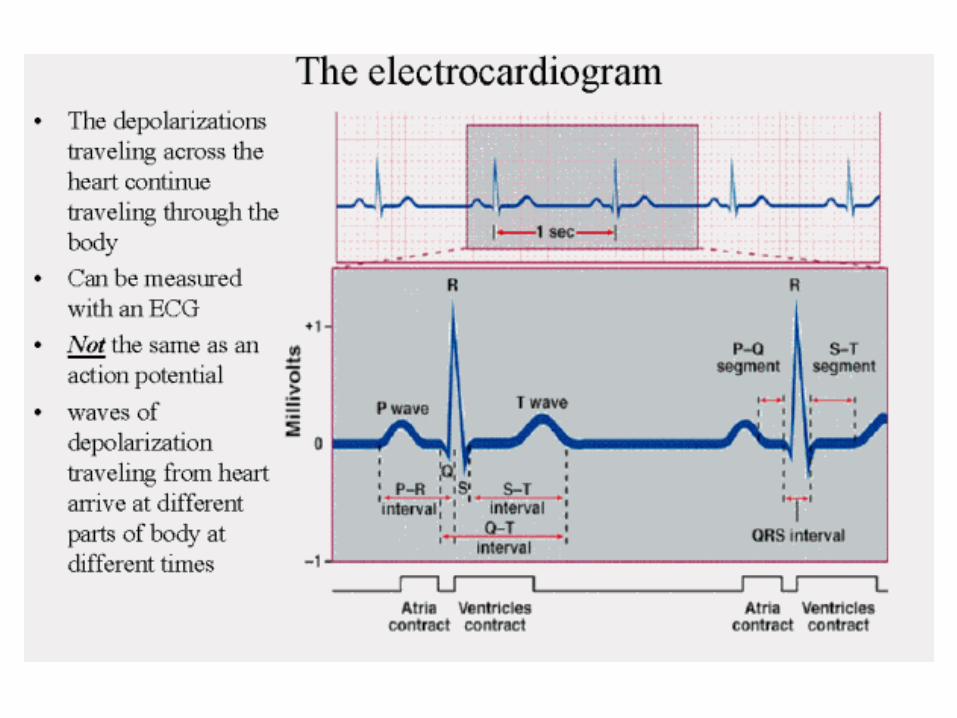
The Electrocardiogram ( ECG )
• P wave : atrial depolarisation
• QRS complex : ventricular depolarisation
• T wave : ventricular repolarisation
• Atrial repolarisation hidden by QRS
P
Q
R
S
T
ECG INTERPRETATION
1. RHYTM2. RATE3. AXIS 4. HIPERTROPHIC SIGNS5. MYOCARDIAL INFARCTION6. ARRHYTHMIA
1. RHYTHM
Normal cardiac rhythm : SINUS rhythm
Sinus rhythm characteristics :• Rate 60-100 bpm• Constant R – R interval• Negative P wave in aVR and positive di II• P wave is always followed by QRS complex
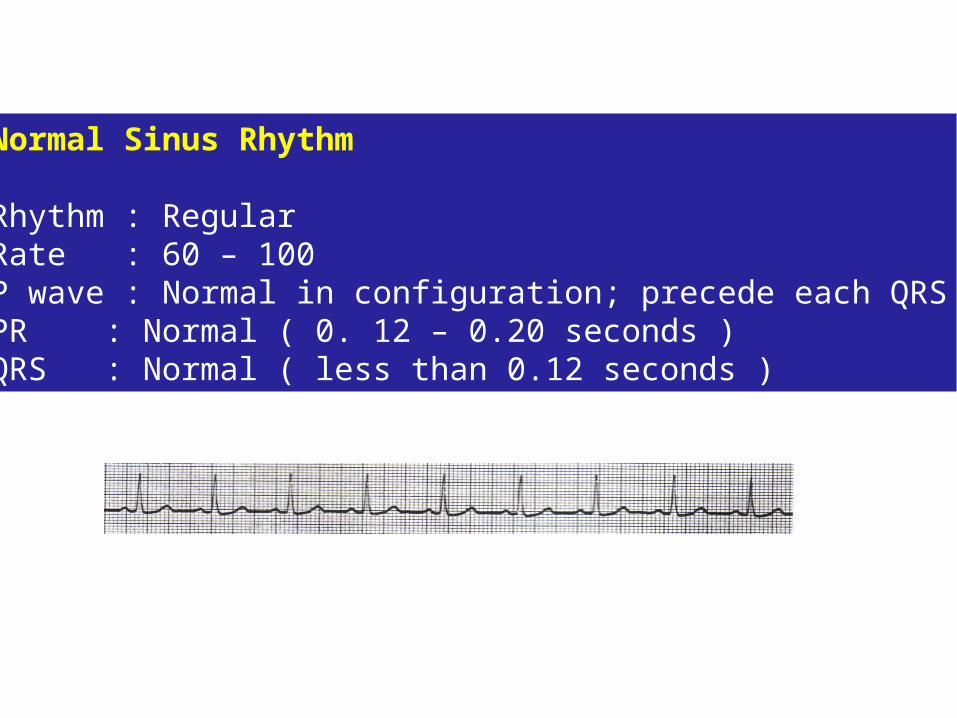
Normal Sinus Rhythm
Rhythm : RegularRate : 60 – 100P wave : Normal in configuration; precede each QRSPR : Normal ( 0. 12 – 0.20 seconds )QRS : Normal ( less than 0.12 seconds )
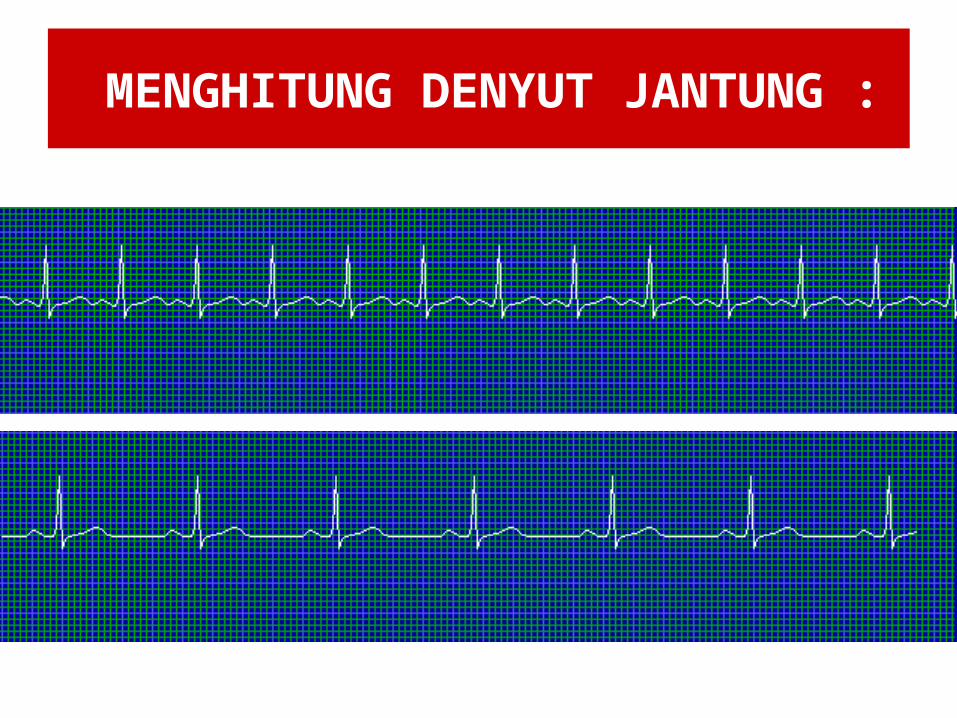
MENGHITUNG DENYUT JANTUNG :
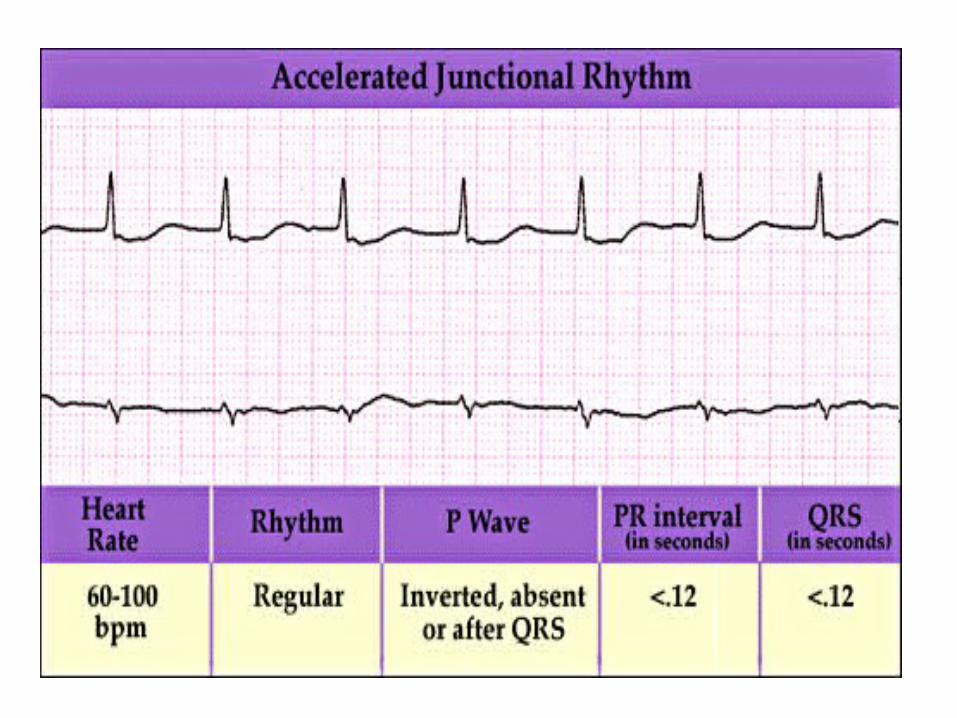
• JUNCTIONAL RHYTM
- Relatively slow regular rhytm with an
escape rate of 35 to 60 per minute
- Normal QRS complexes
- Ectopic P wave may precede or follow
the QRS complex
- PR interval < .12 second
- QRS duration < .12 second
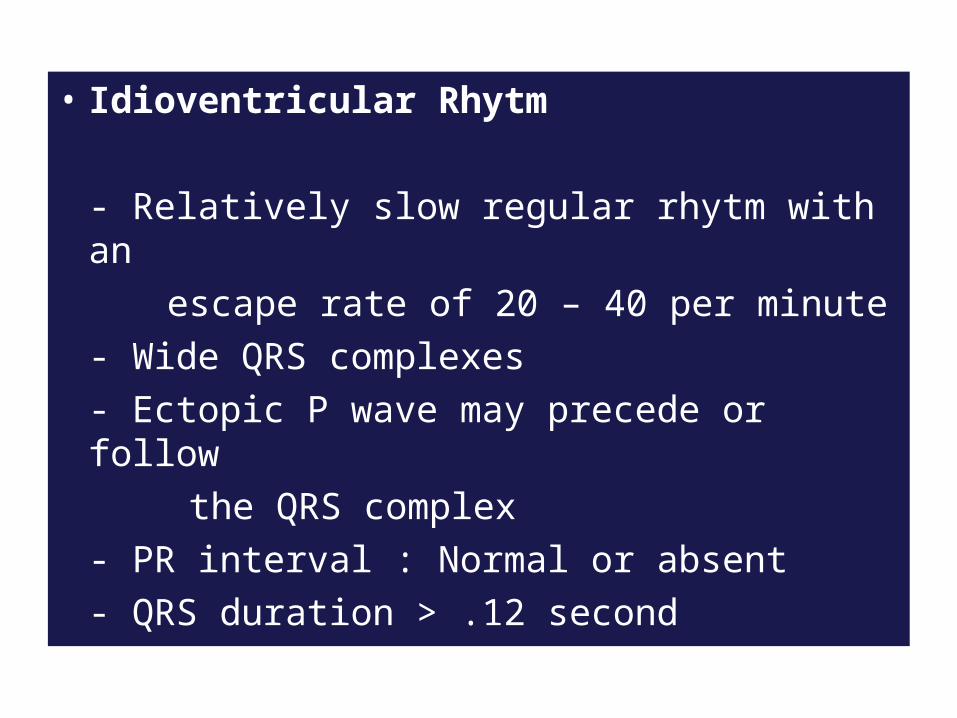
• Idioventricular Rhytm
- Relatively slow regular rhytm with an
escape rate of 20 – 40 per minute
- Wide QRS complexes
- Ectopic P wave may precede or follow
the QRS complex
- PR interval : Normal or absent
- QRS duration > .12 second
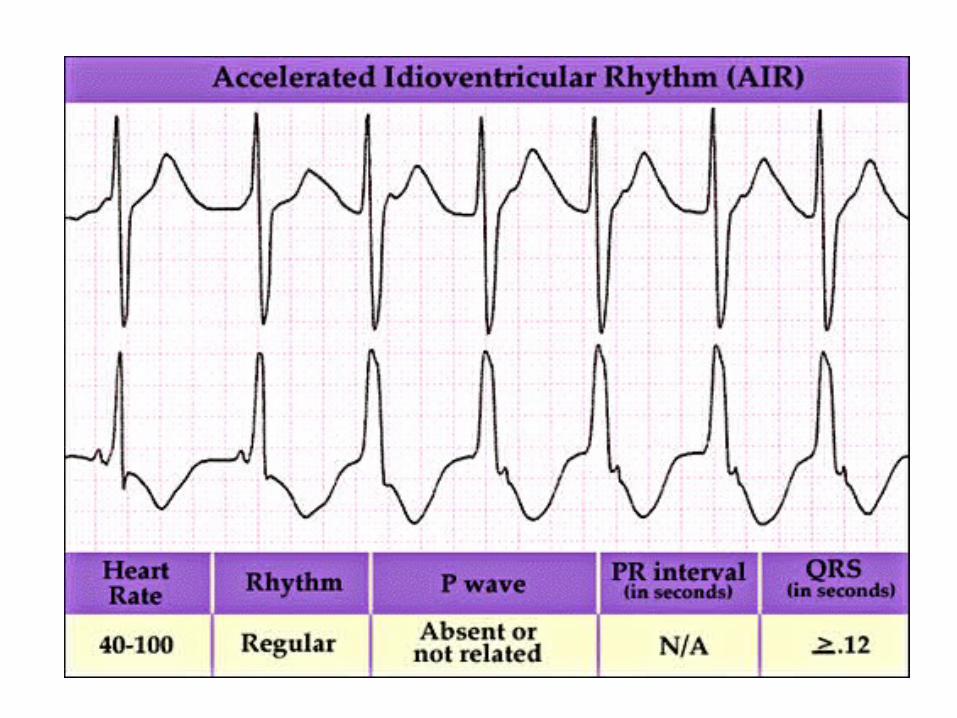
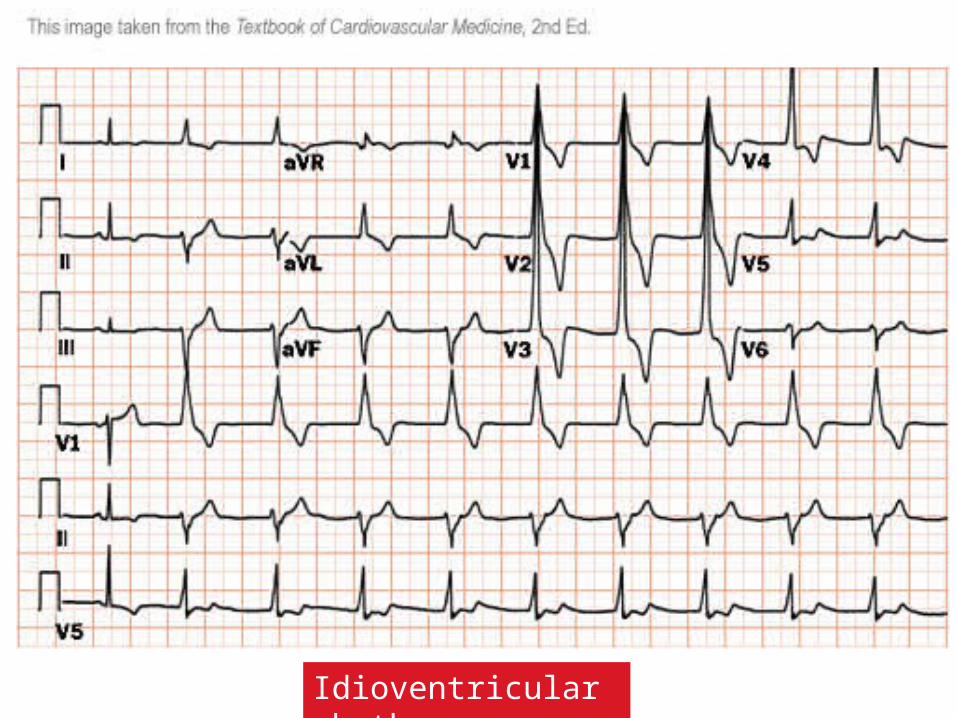
Idioventricular rhythm
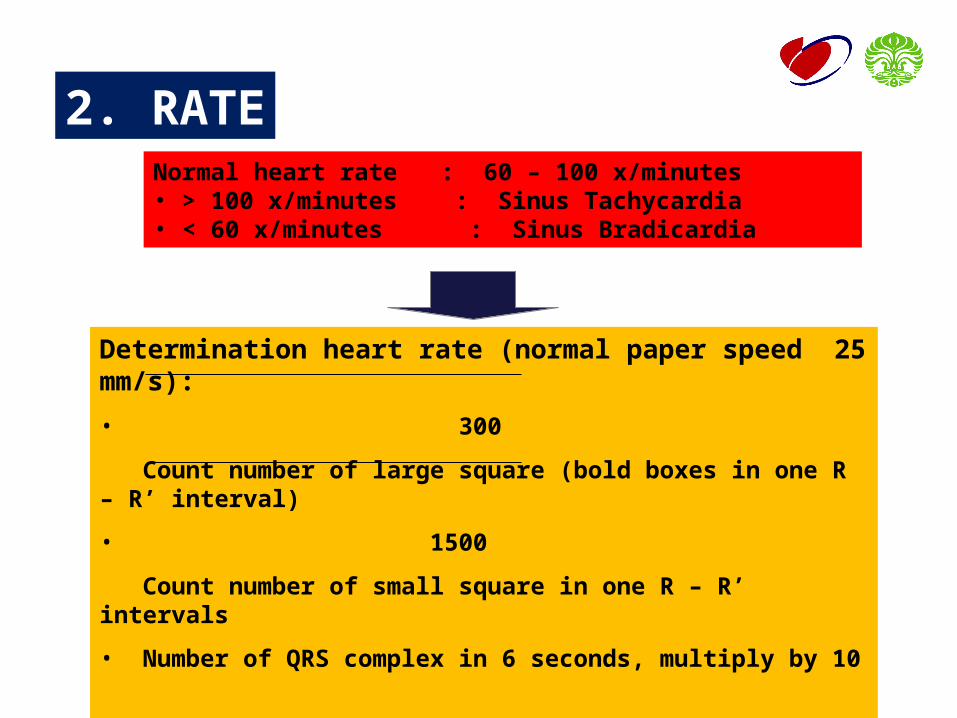
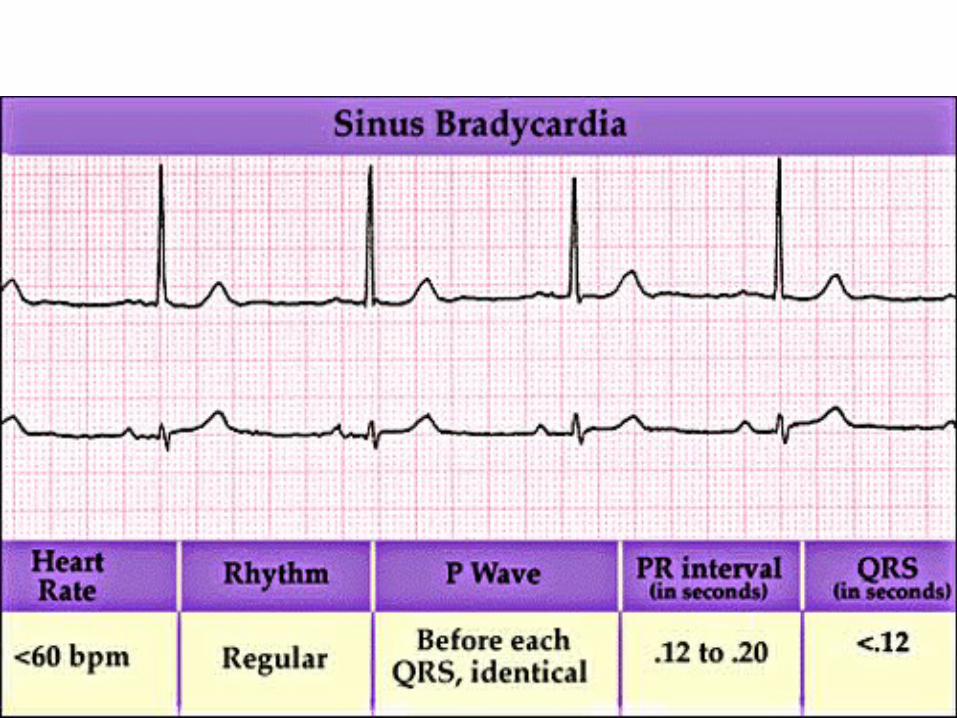
2. RATENormal heart rate : 60 – 100 x/minutes• > 100 x/minutes : Sinus Tachycardia• < 60 x/minutes : Sinus Bradicardia
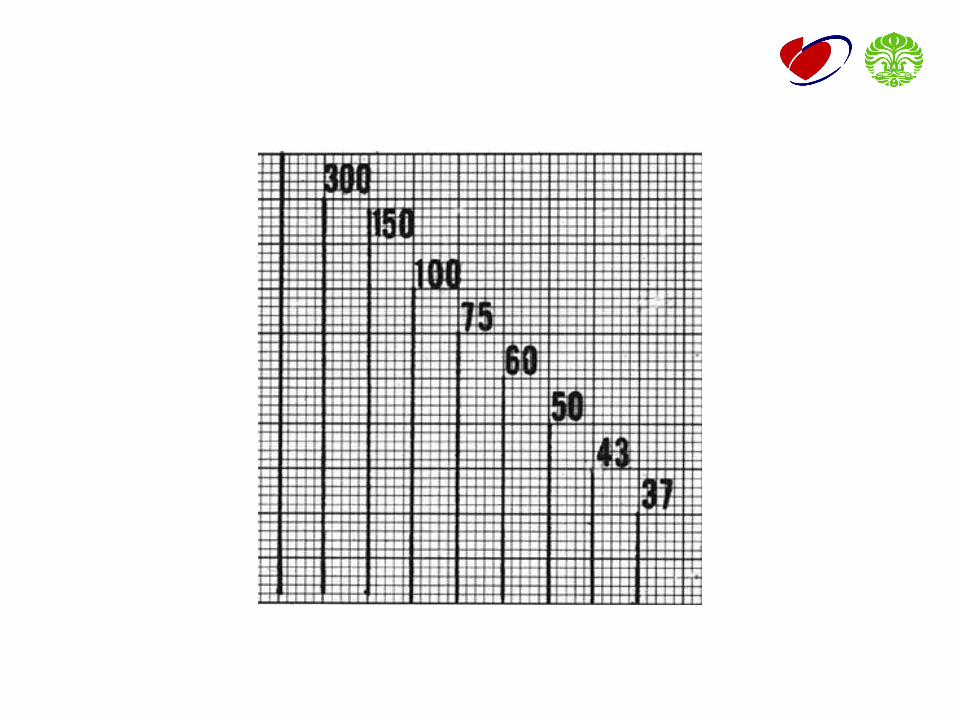
Determination heart rate (normal paper speed 25 mm/s):
• 300
Count number of large square (bold boxes in one R – R’ interval)
• 1500
Count number of small square in one R – R’ intervals
• Number of QRS complex in 6 seconds, multiply by 10
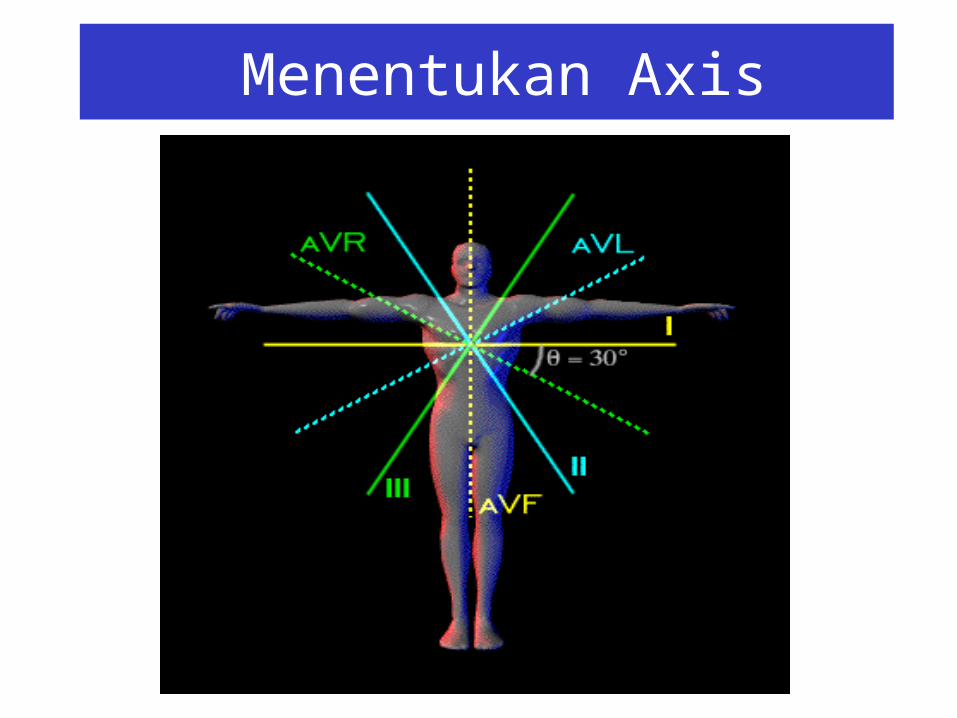
MENENTUKAN AXIS EKG
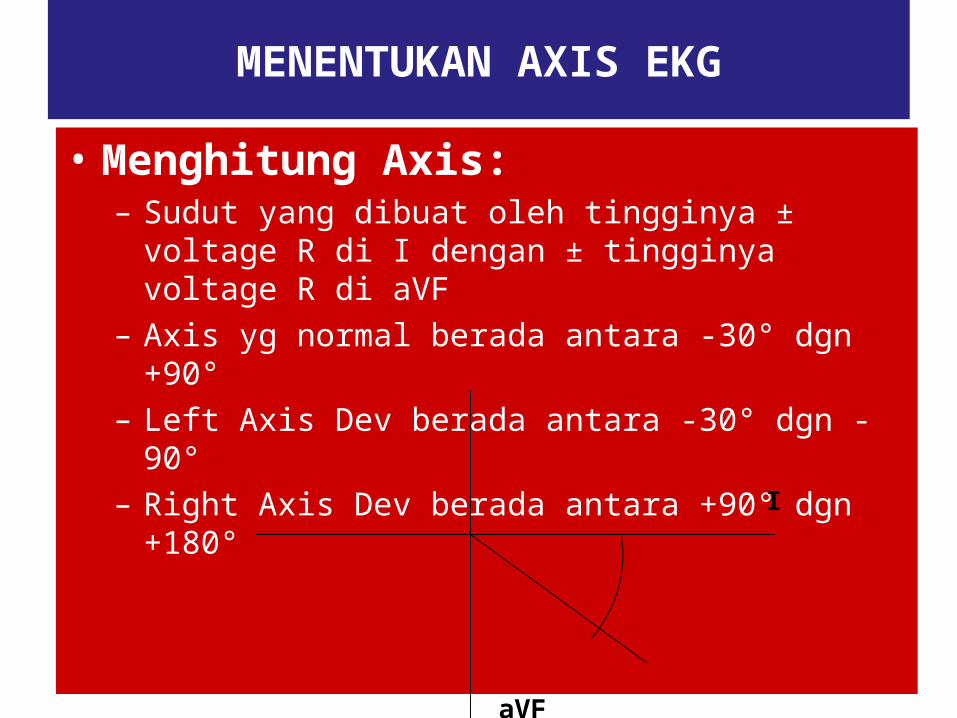
• Menghitung Axis:– Sudut yang dibuat oleh tingginya ± voltage R di I
dengan ± tingginya voltage R di aVF– Axis yg normal berada antara -30° dgn +90°– Left Axis Dev berada antara -30° dgn -90°– Right Axis Dev berada antara +90° dgn +180°
aVF
I
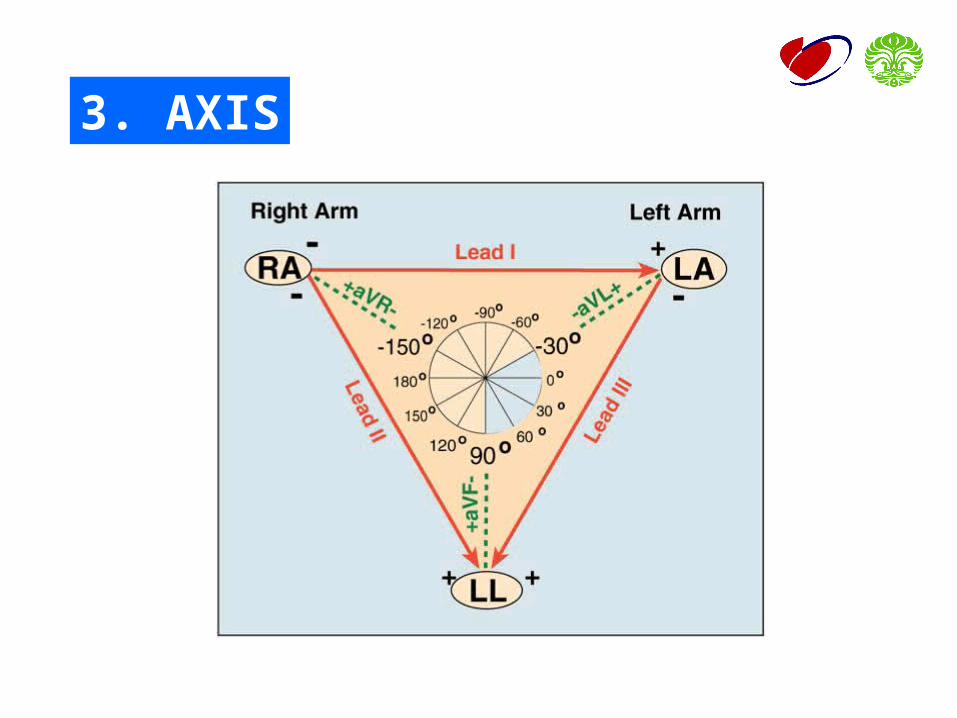
3. AXIS
Menentukan Axis
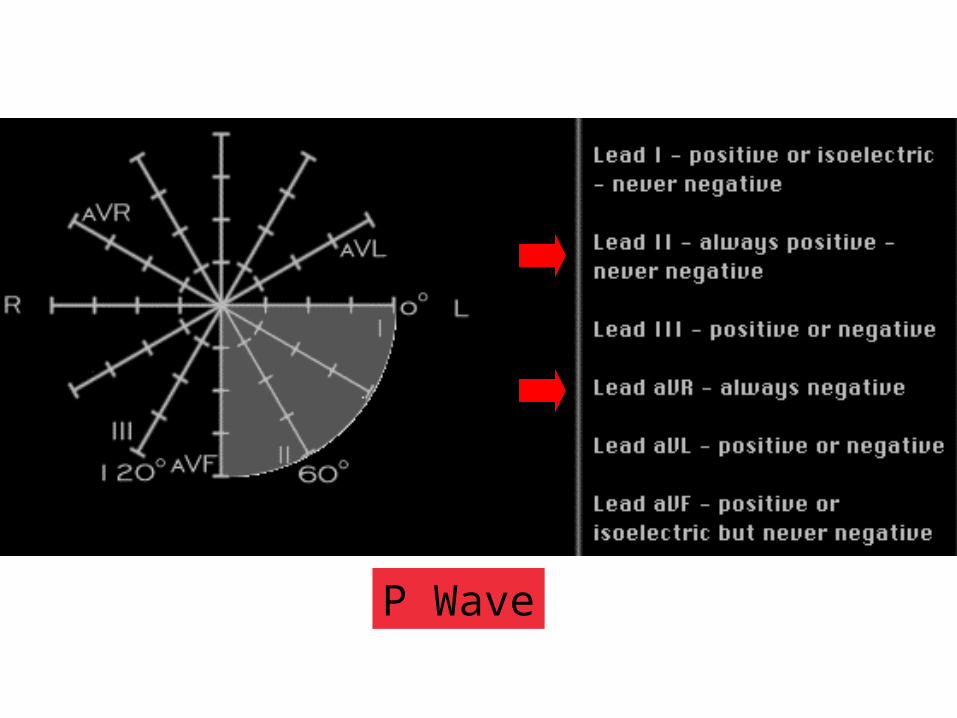
P Wave
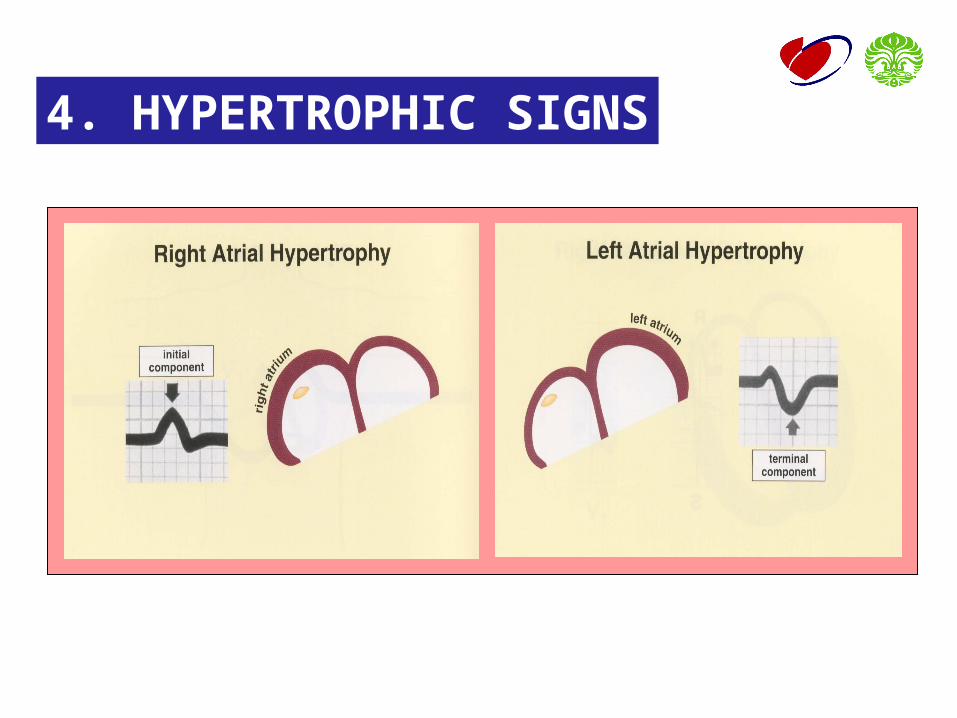
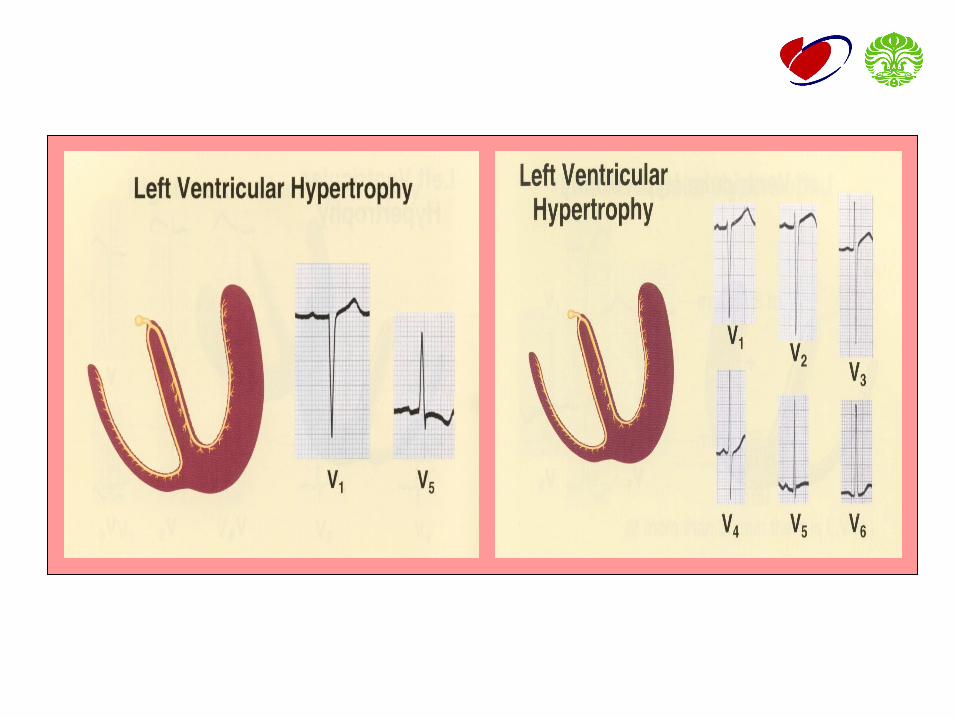
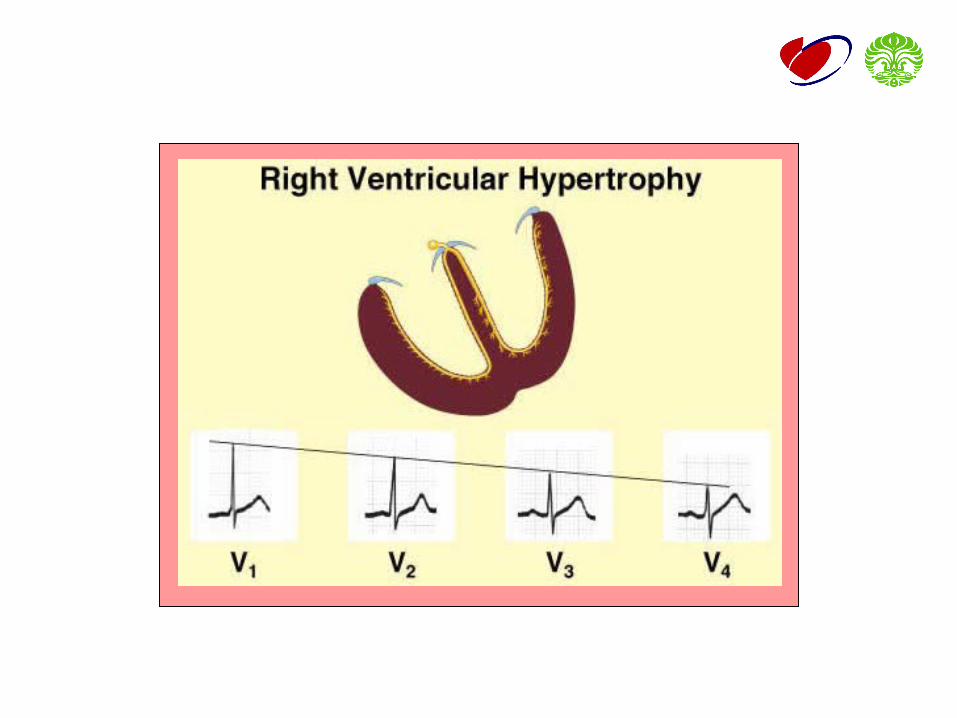
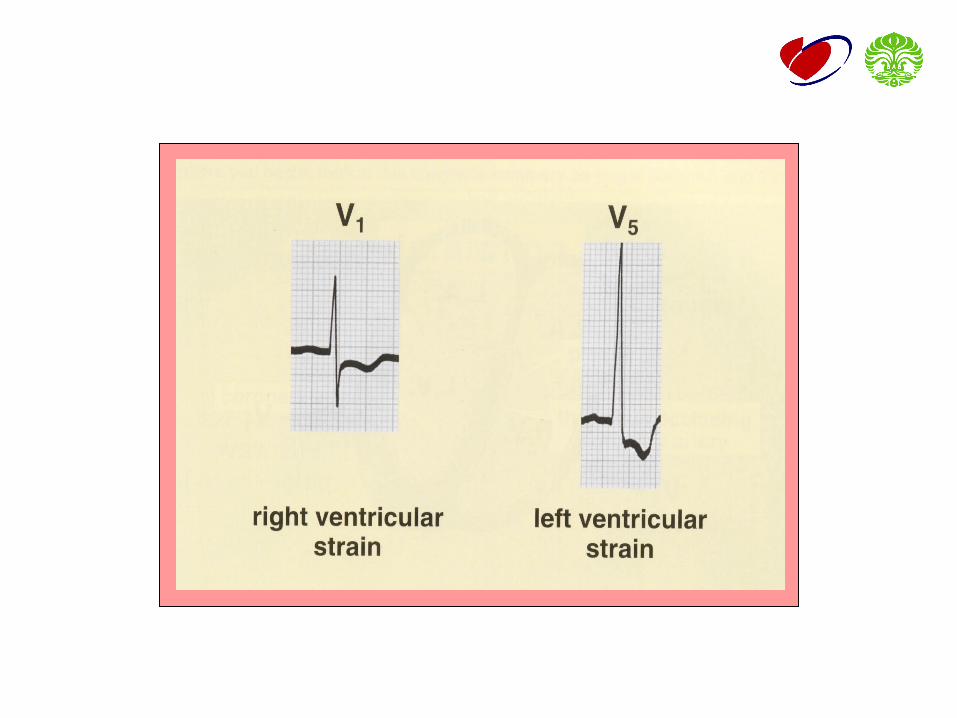
4. HYPERTROPHIC SIGNS
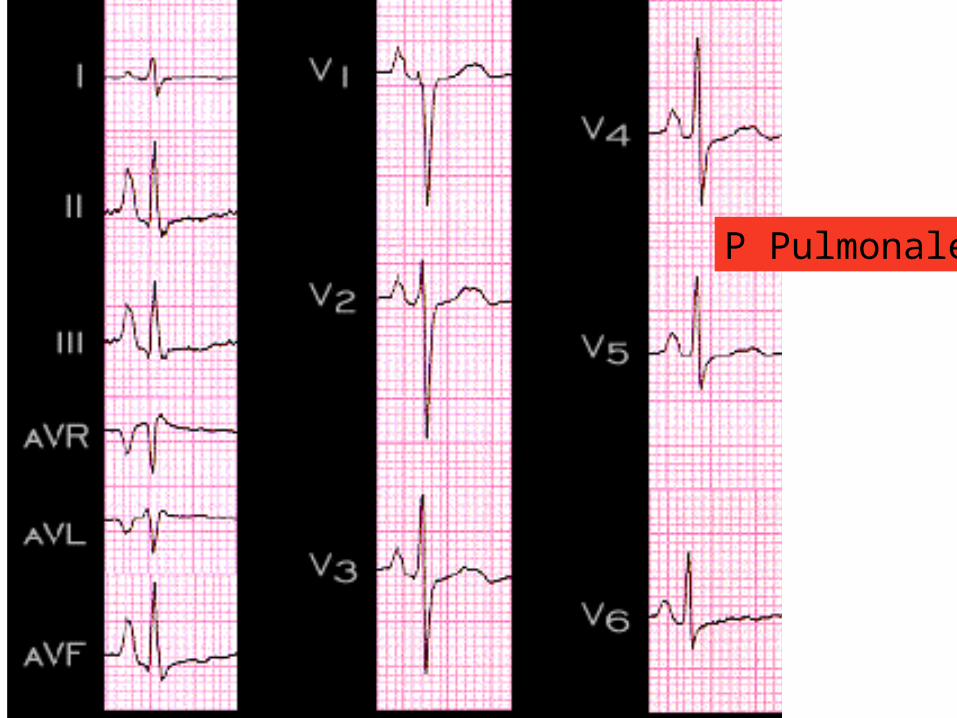
P Pulmonale
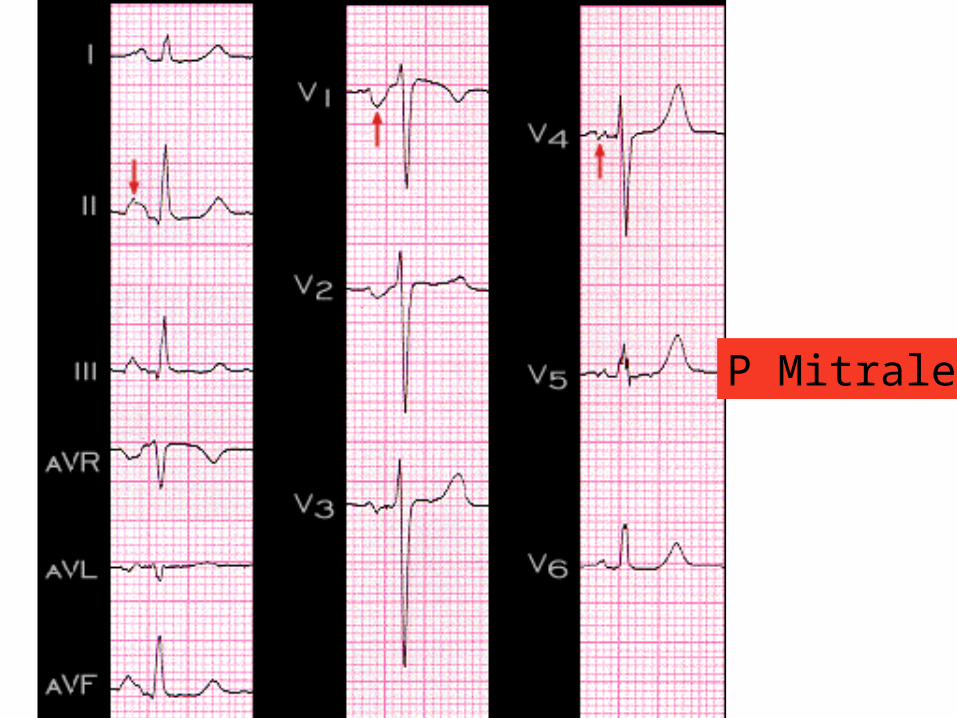
P Mitrale
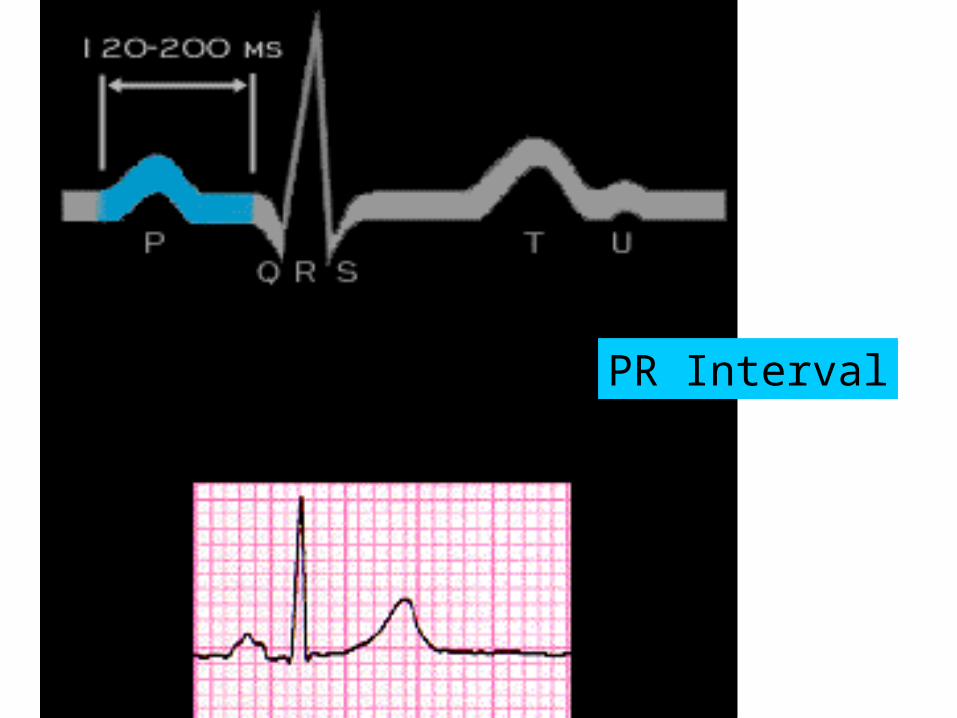
PR Interval
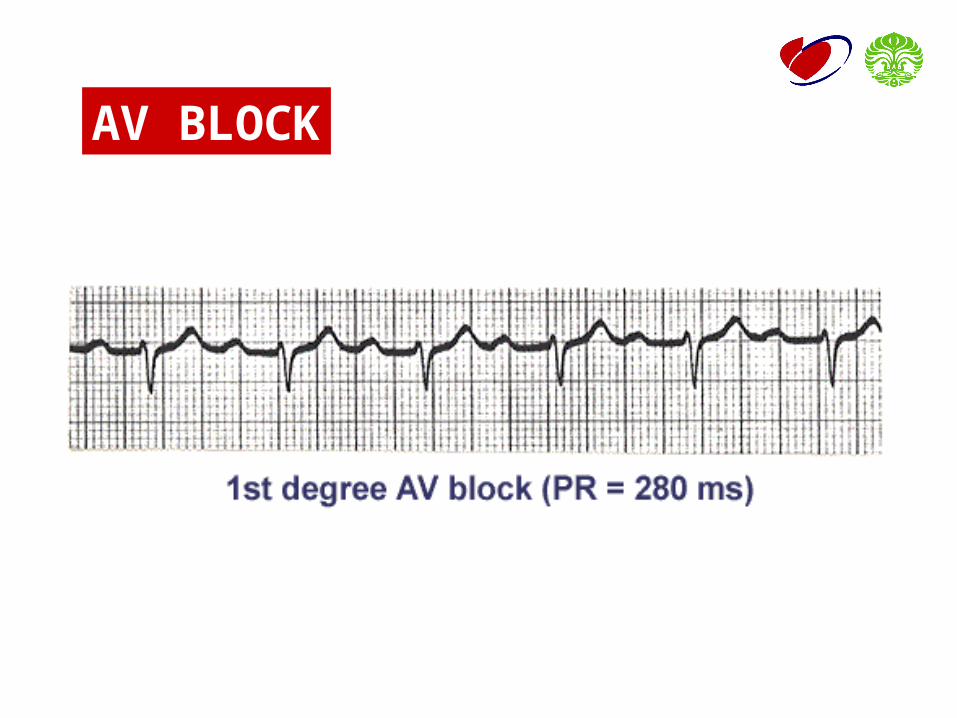
AV BLOCK
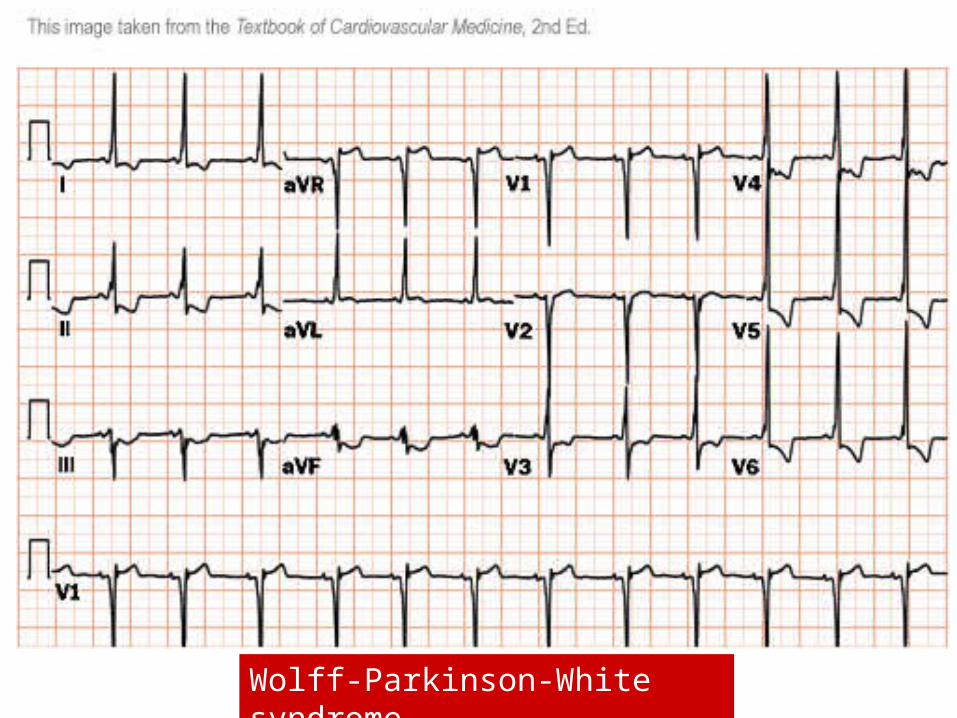
Wolff-Parkinson-White syndrome
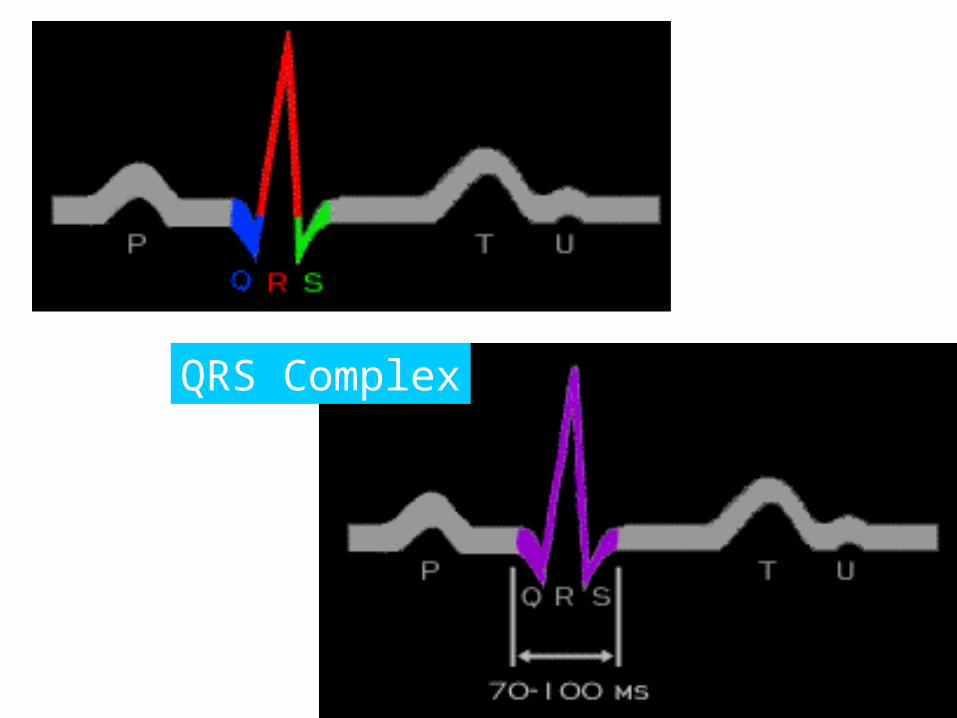
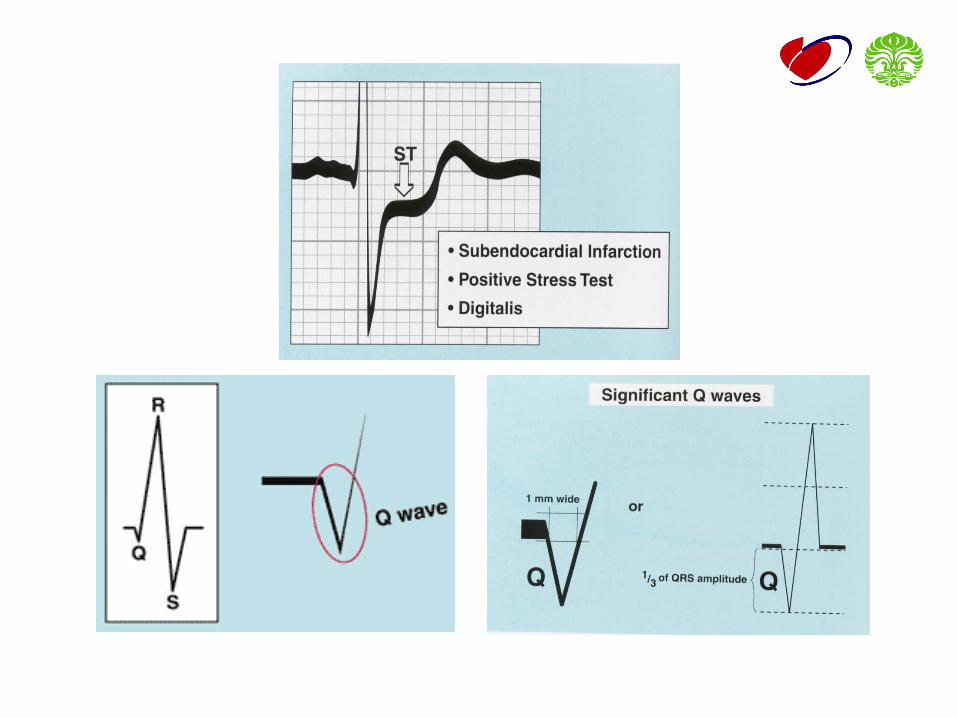
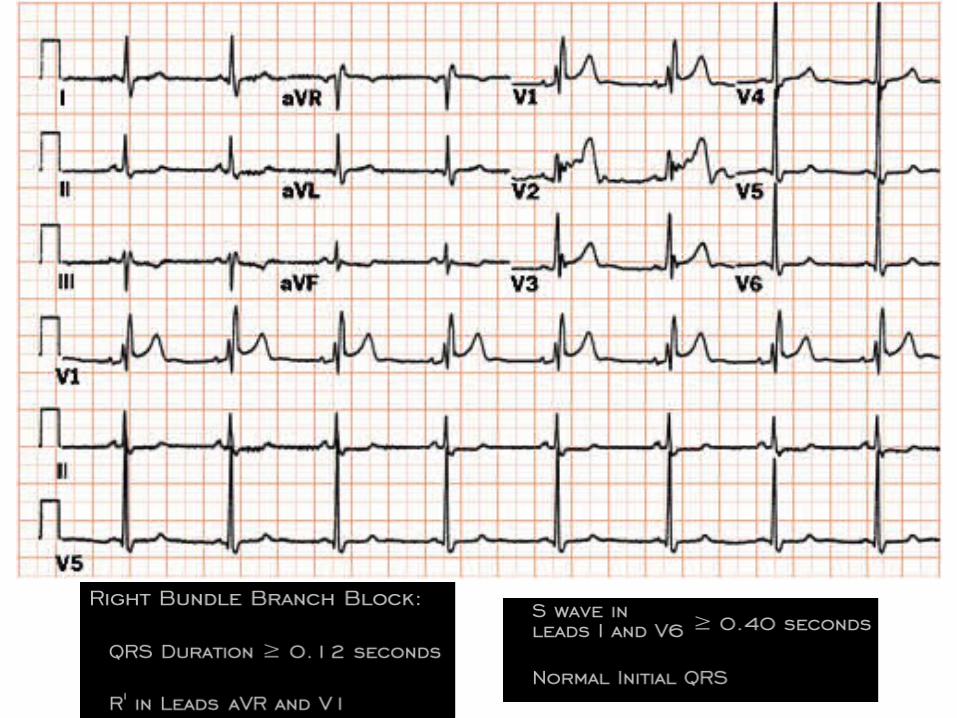
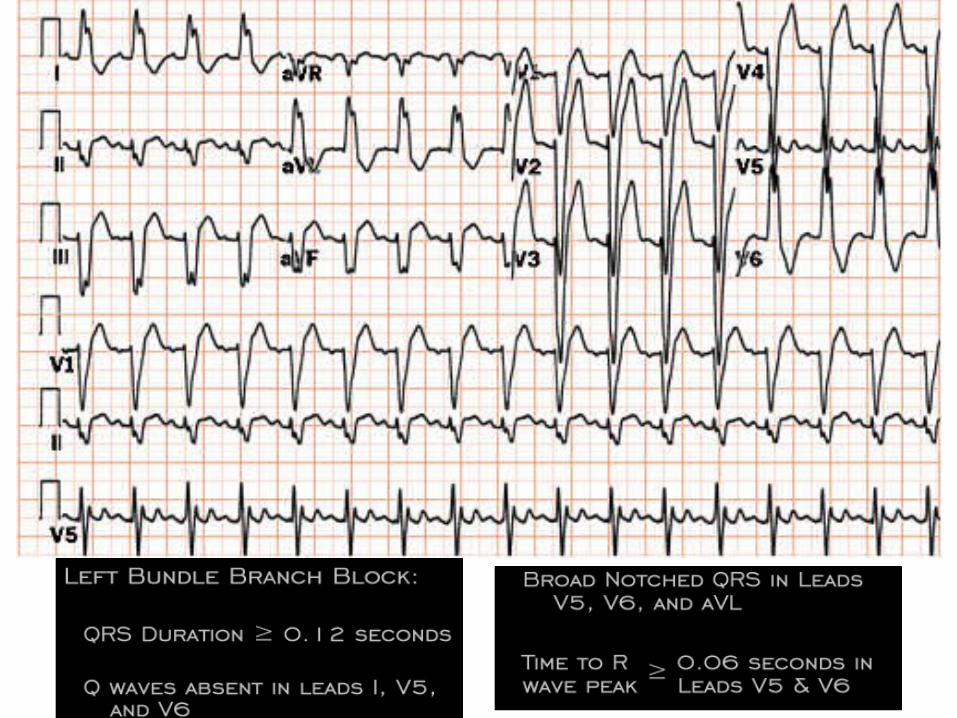
QRS Complex
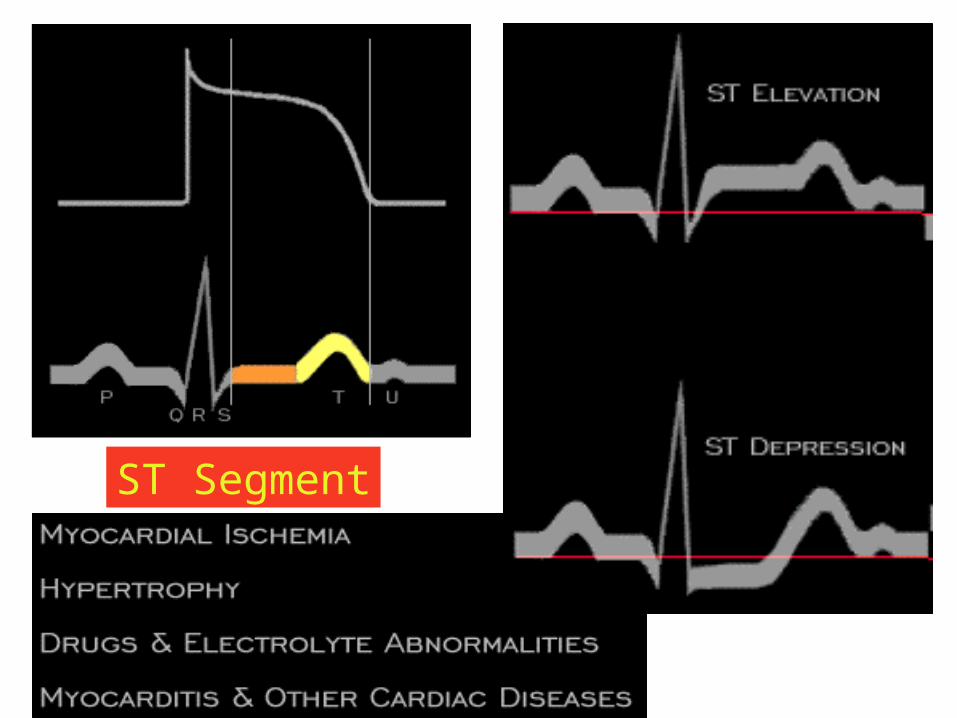
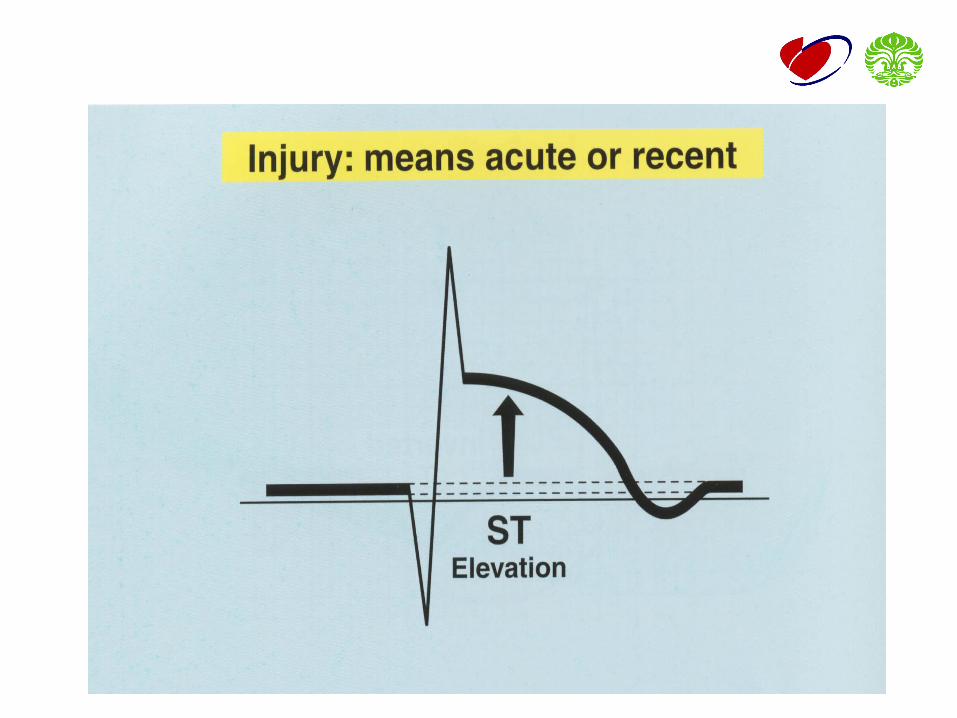
ST Segment
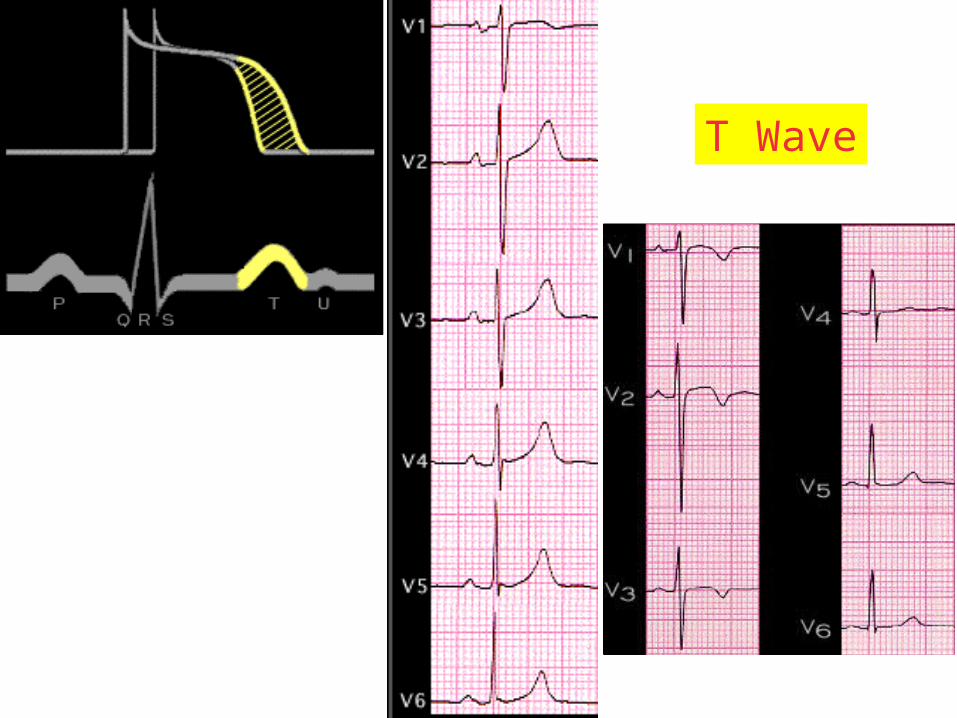
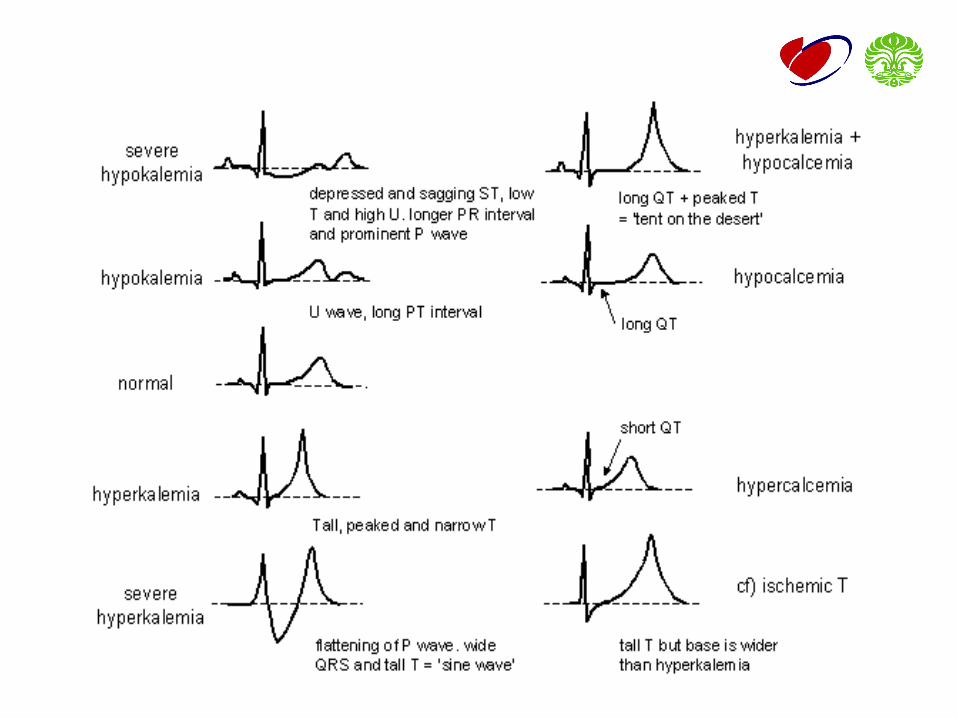
T Wave
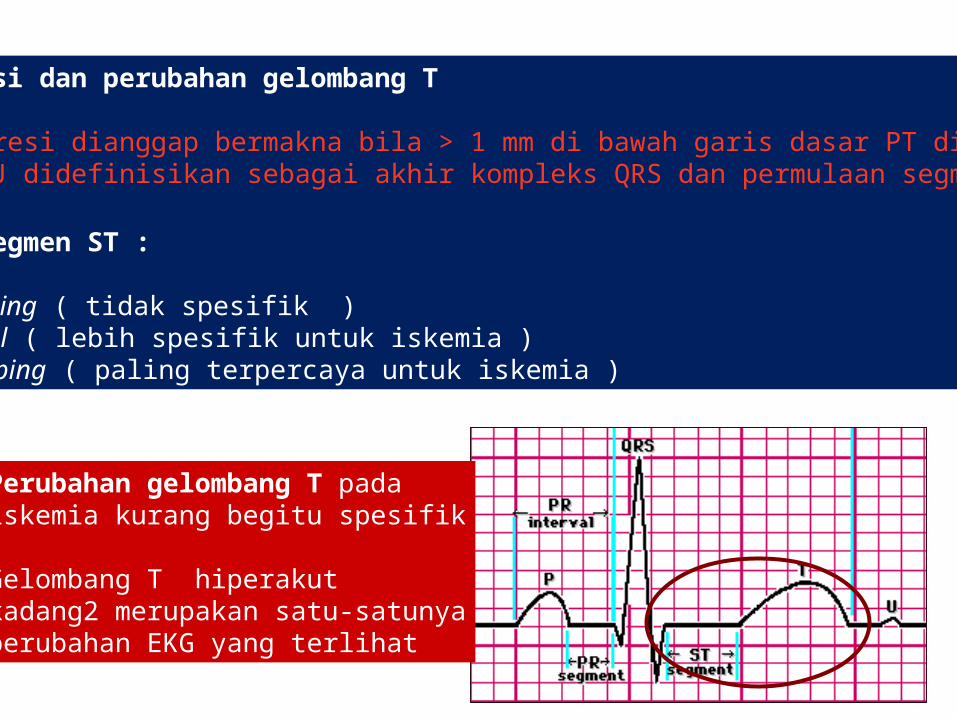
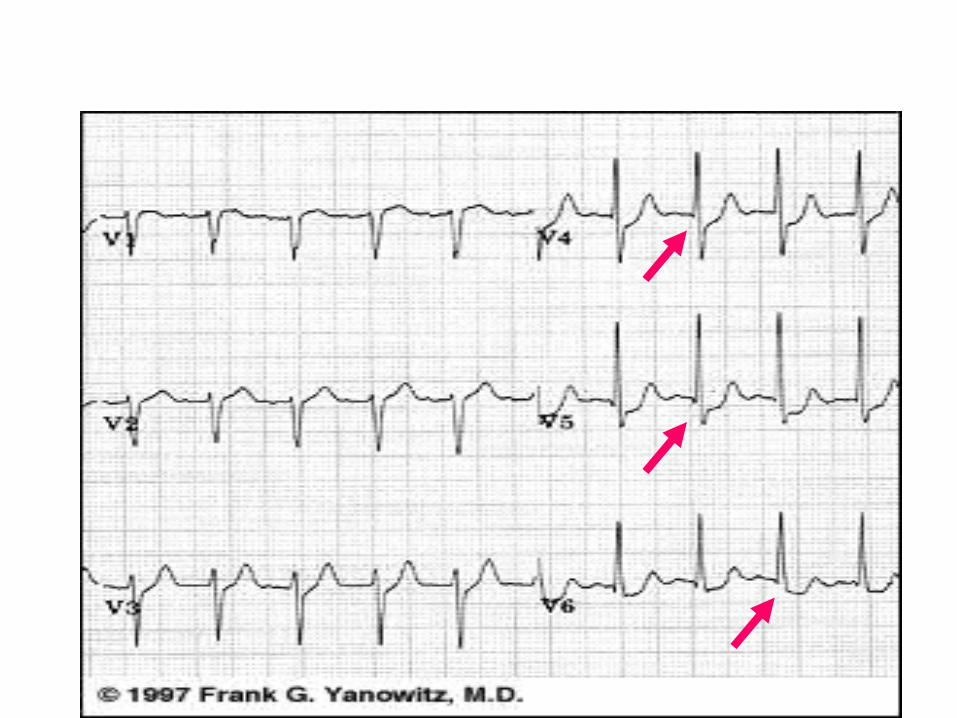
ST depresi dan perubahan gelombang T
ST depresi dianggap bermakna bila > 1 mm di bawah garis dasar PT di titik J• Titik J didefinisikan sebagai akhir kompleks QRS dan permulaan segmen ST
Bentuk segmen ST :
• up-sloping ( tidak spesifik )• horizontal ( lebih spesifik untuk iskemia )• down-sloping ( paling terpercaya untuk iskemia )
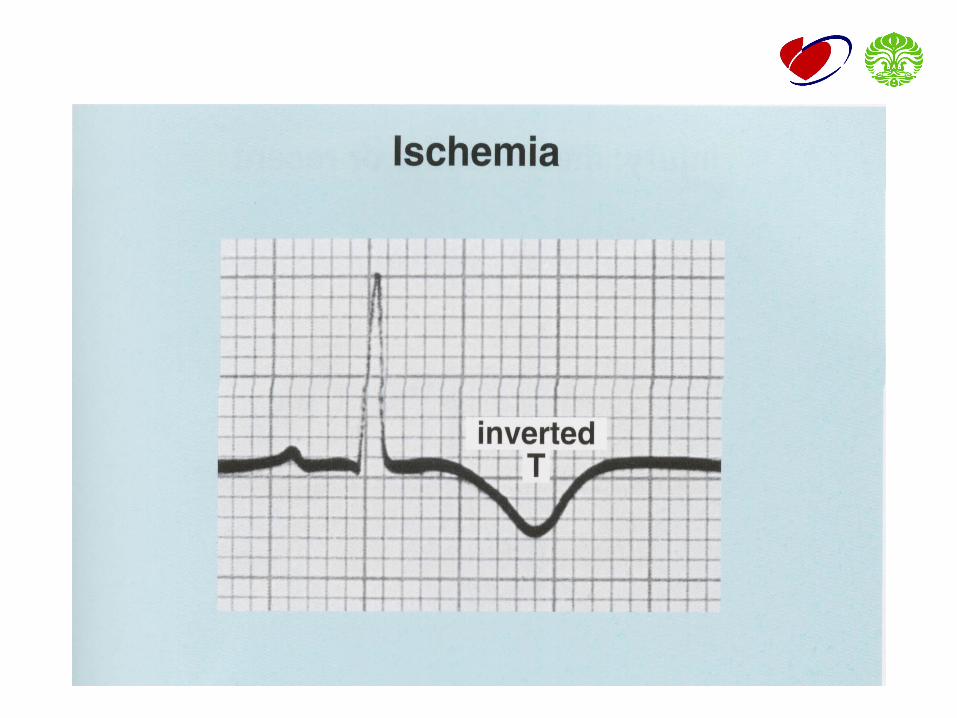
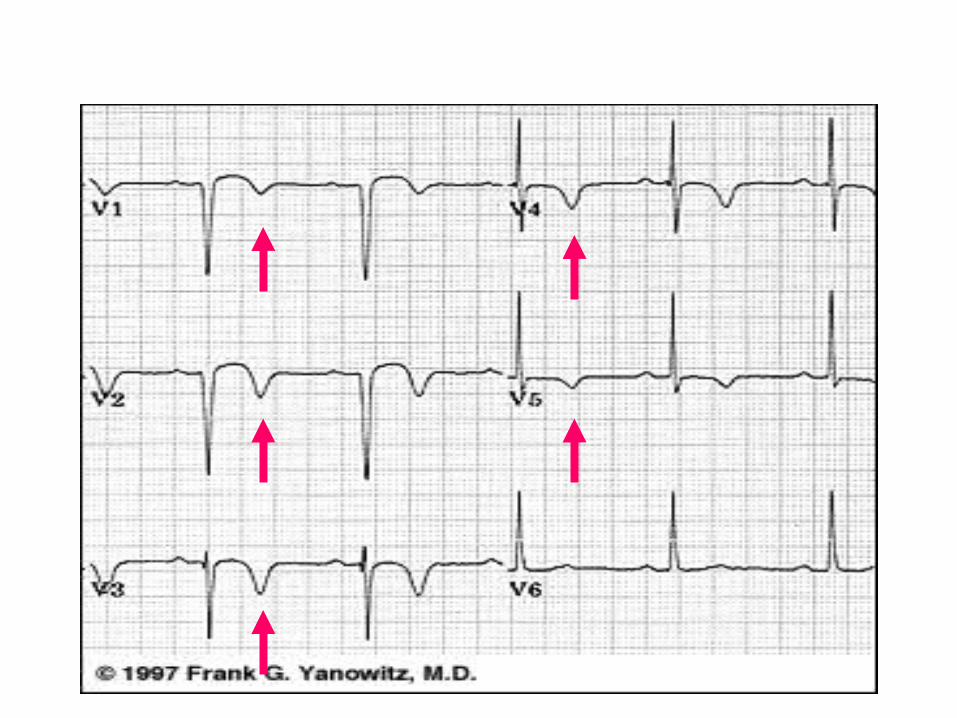
Perubahan gelombang T pada iskemia kurang begitu spesifik Gelombang T hiperakut kadang2 merupakan satu-satunyaperubahan EKG yang terlihat
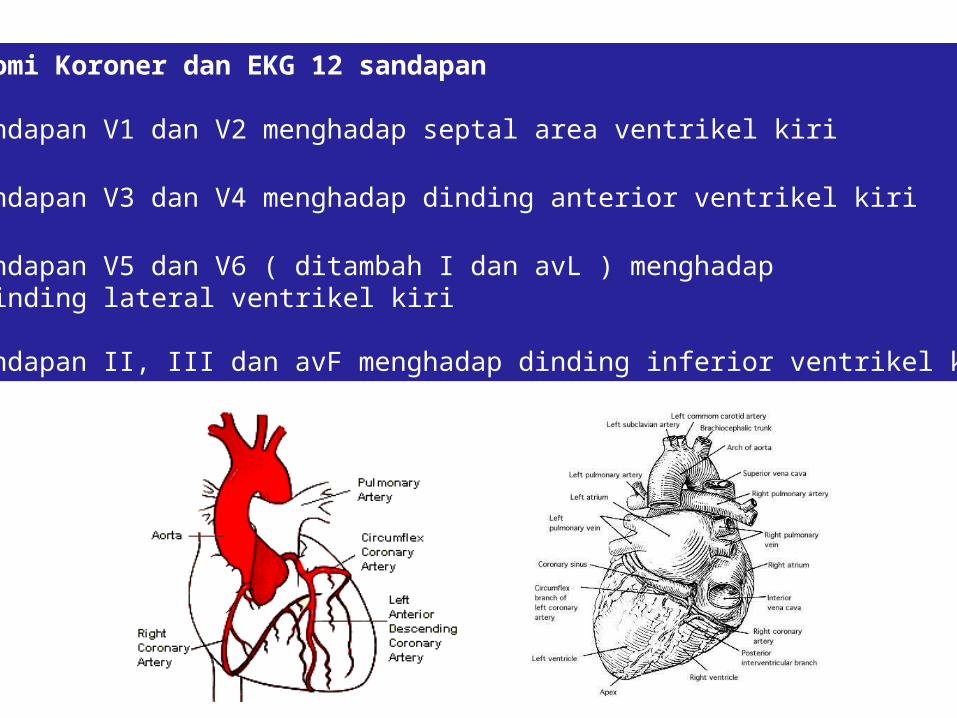
Anatomi Koroner dan EKG 12 sandapan
• Sandapan V1 dan V2 menghadap septal area ventrikel kiri
• Sandapan V3 dan V4 menghadap dinding anterior ventrikel kiri
• Sandapan V5 dan V6 ( ditambah I dan avL ) menghadap dinding lateral ventrikel kiri
• Sandapan II, III dan avF menghadap dinding inferior ventrikel kiri
5. MYOCARDIAL INFARCTION
• Ischemia
• Injury
• Necrosis
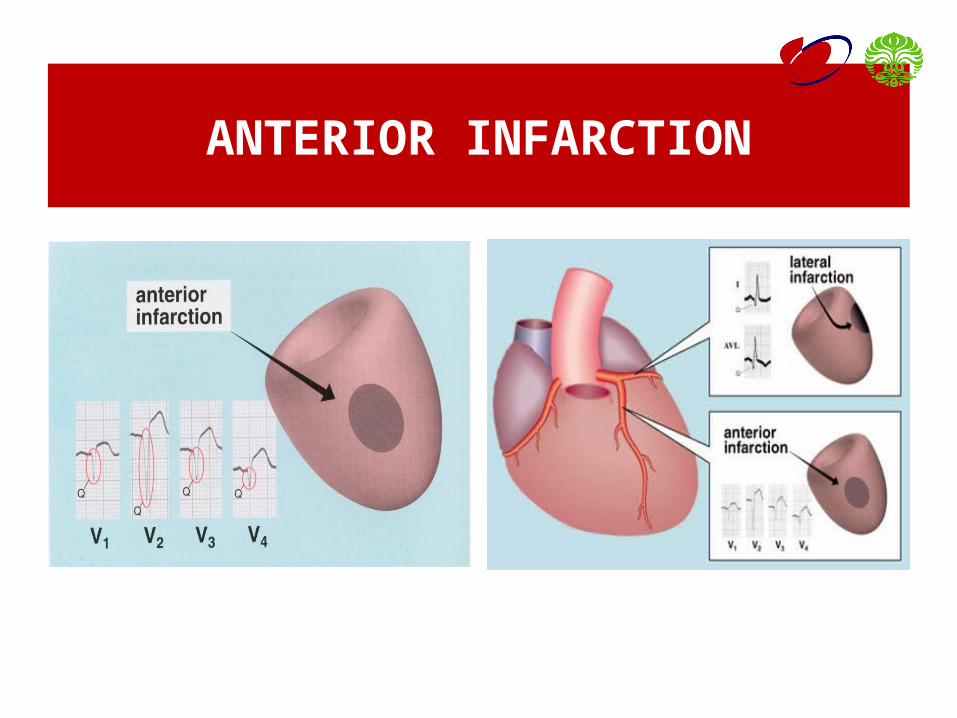
ANTERIOR INFARCTION
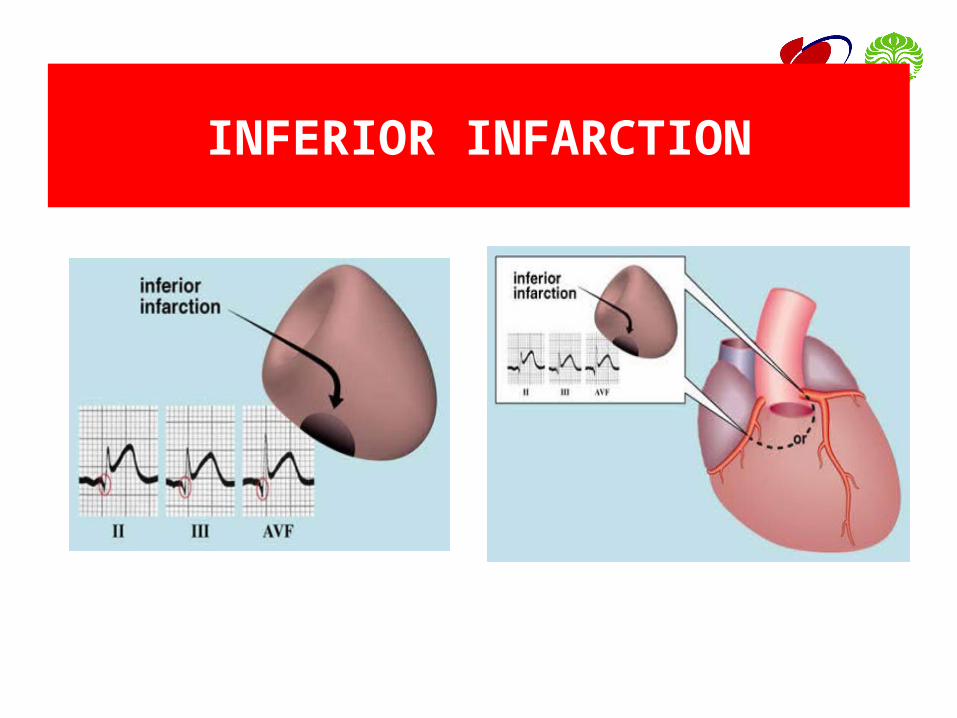
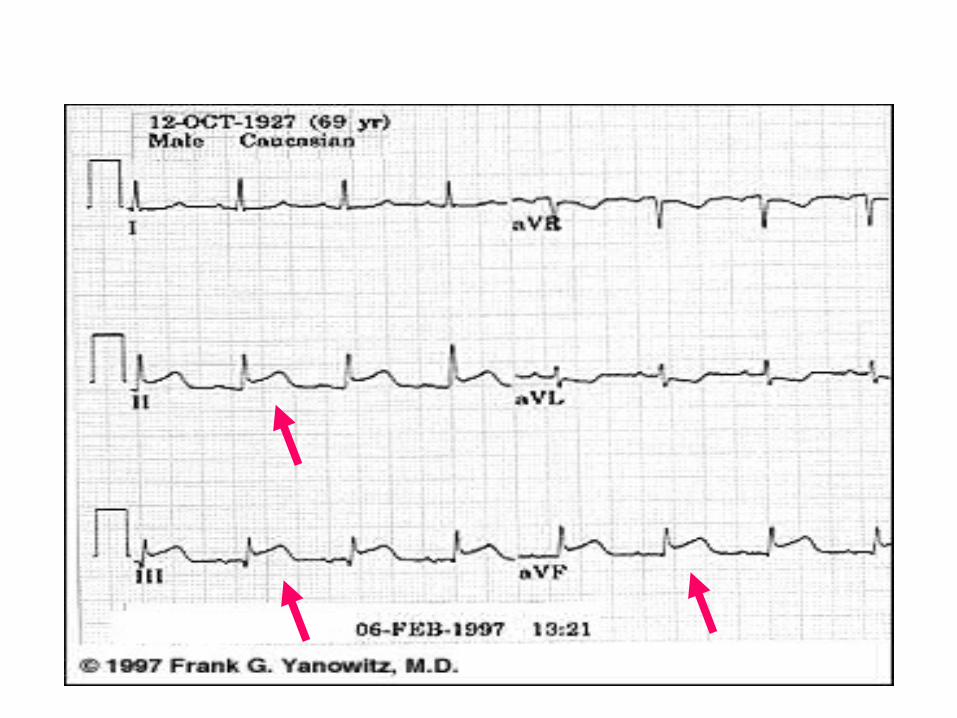
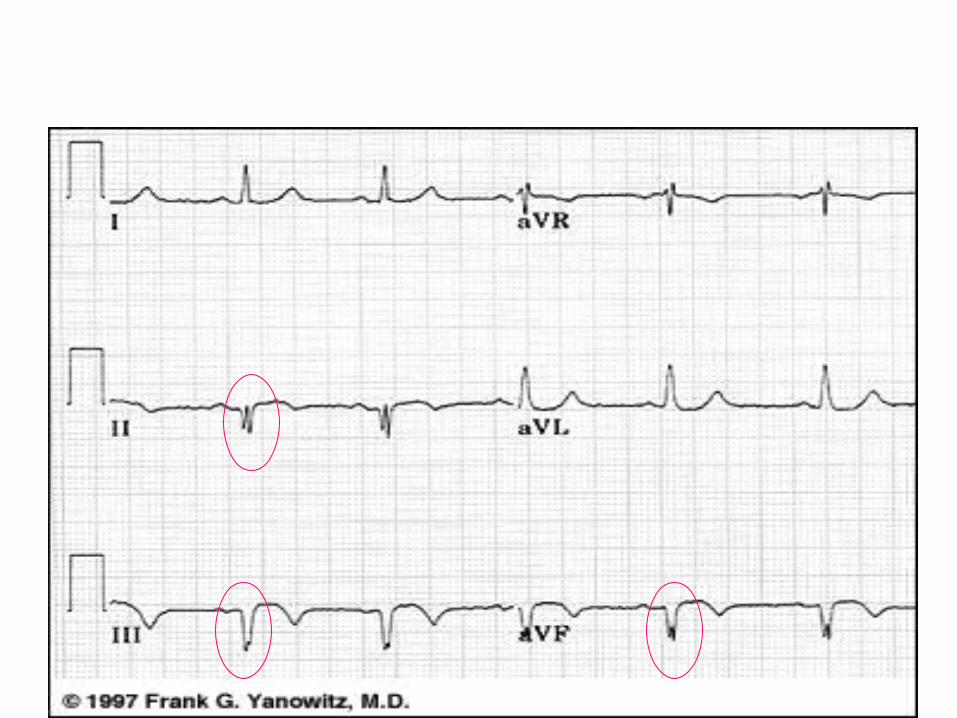
INFERIOR INFARCTION
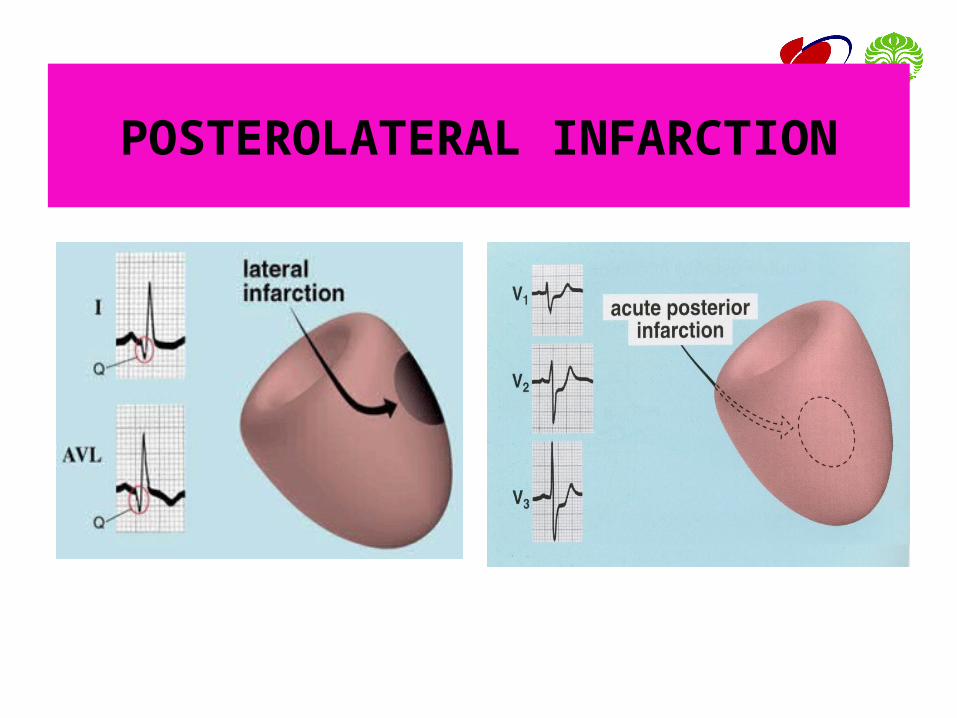
POSTEROLATERAL INFARCTION
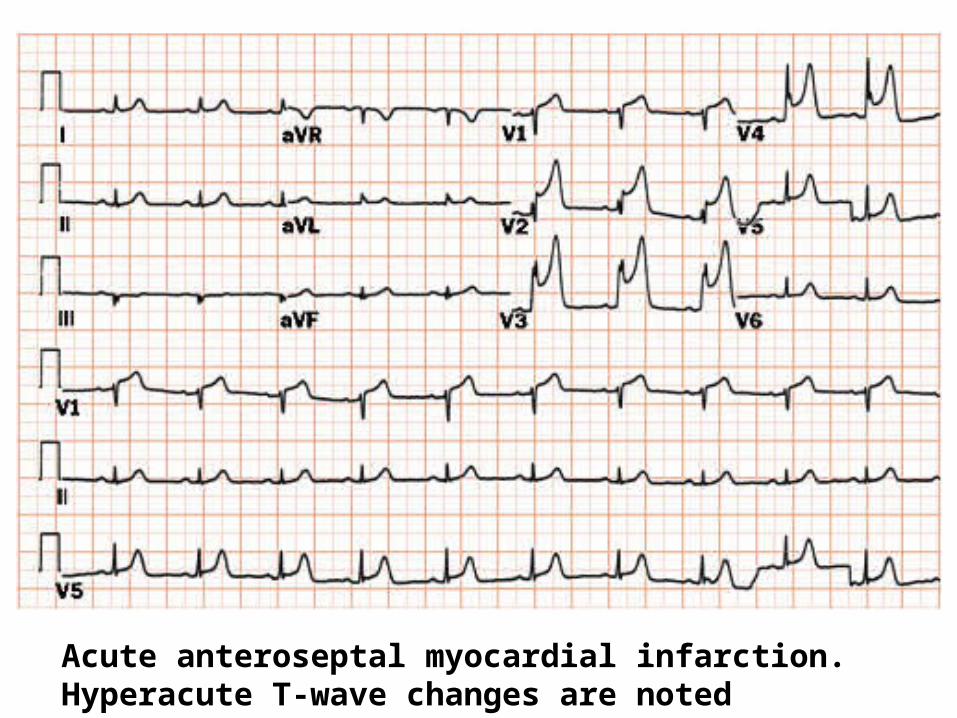
Acute anteroseptal myocardial infarction. Hyperacute T-wave changes are noted
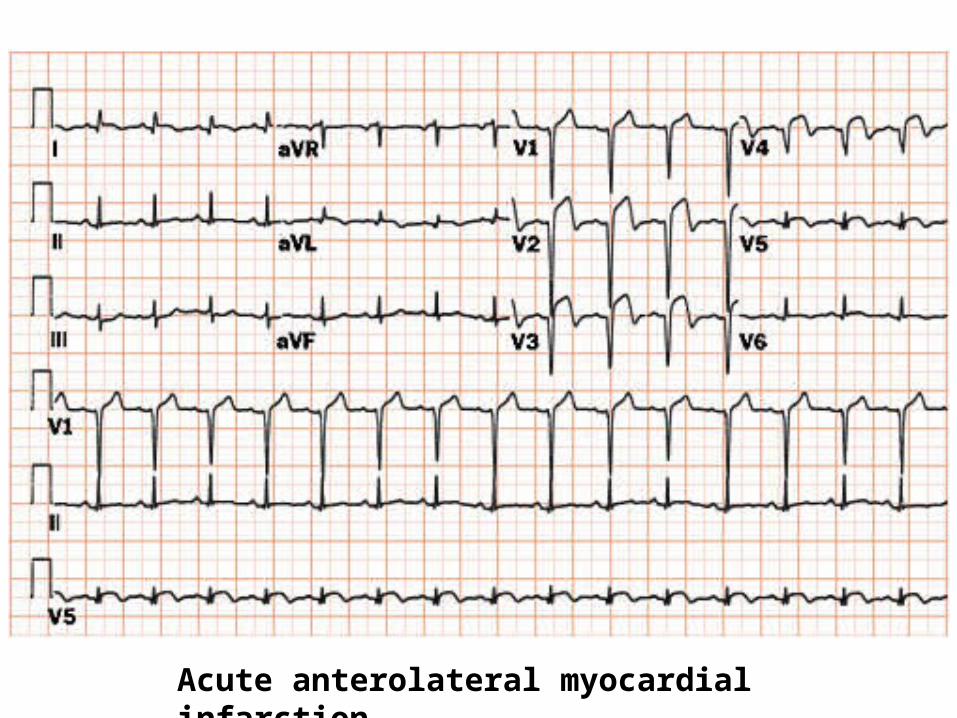
Acute anterolateral myocardial infarction
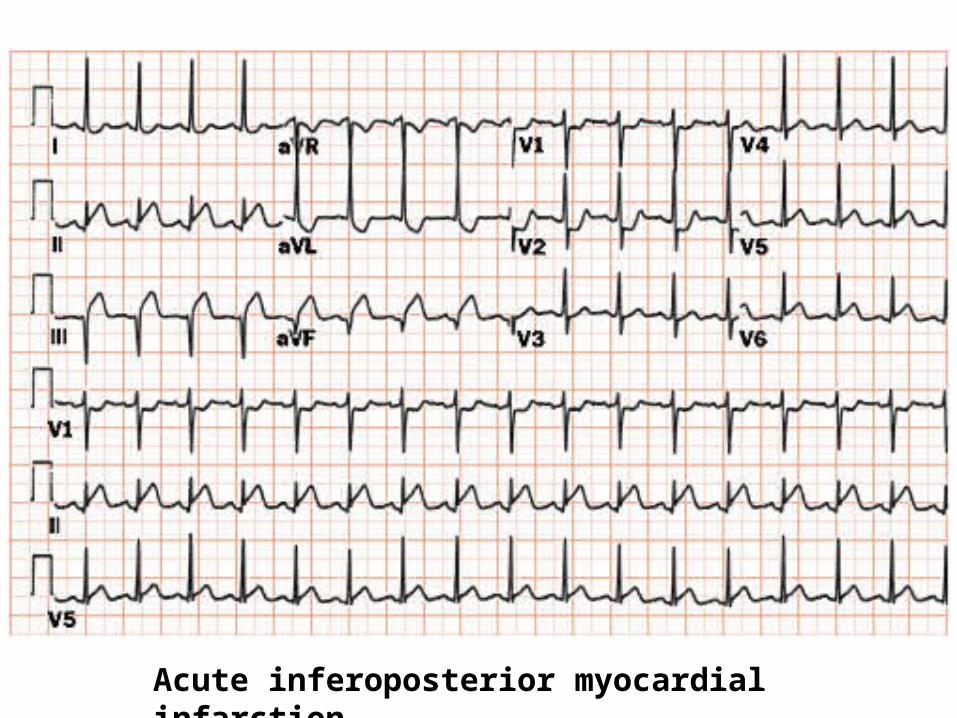
Acute inferoposterior myocardial infarction
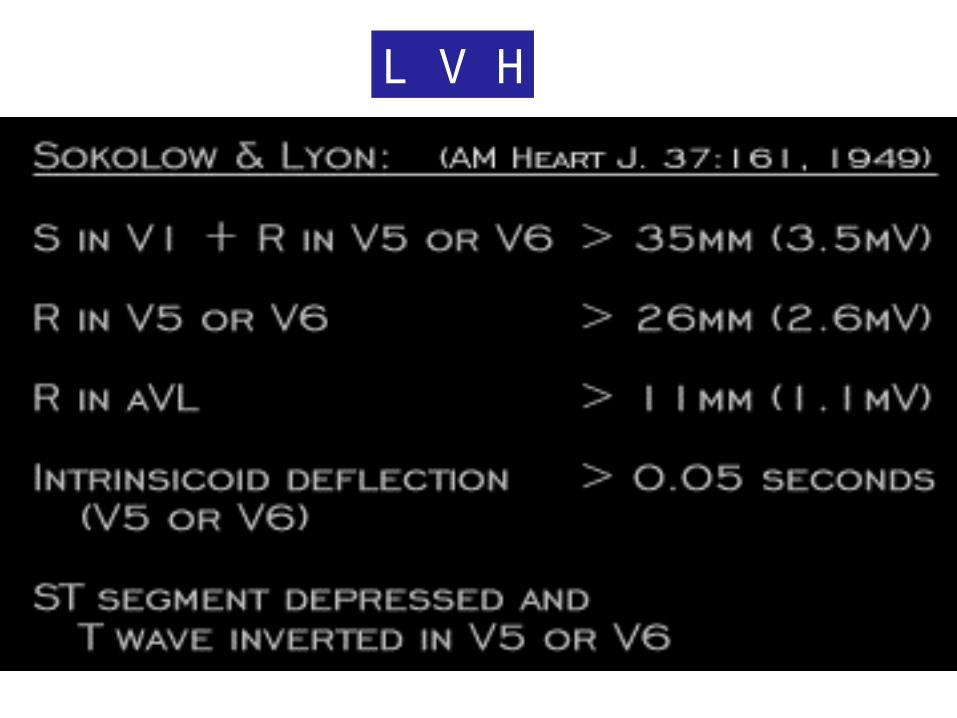
L V H
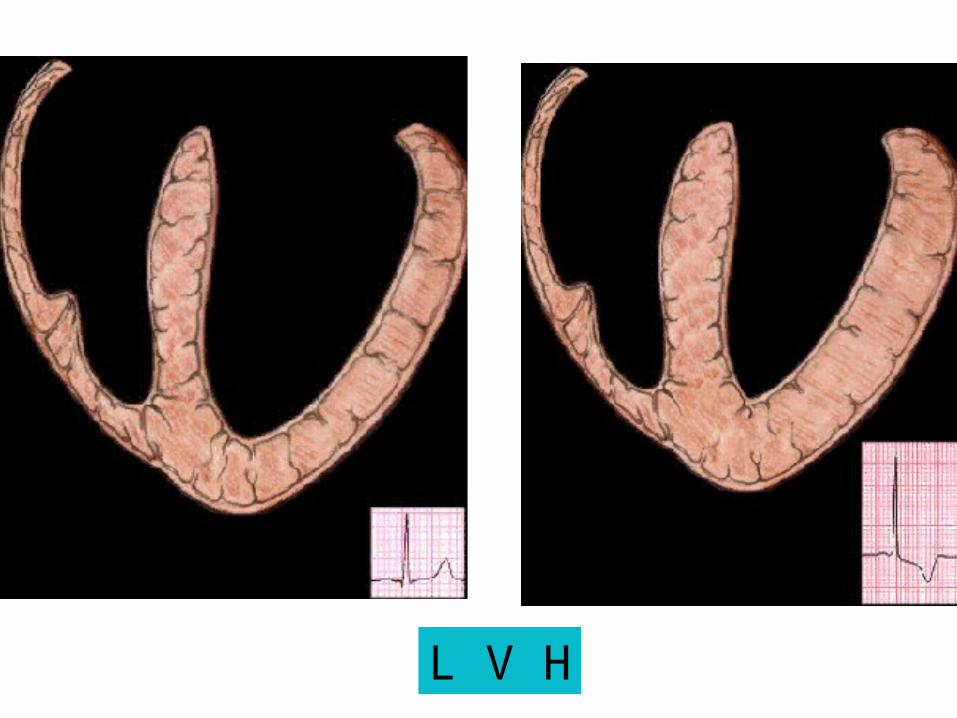
L V H
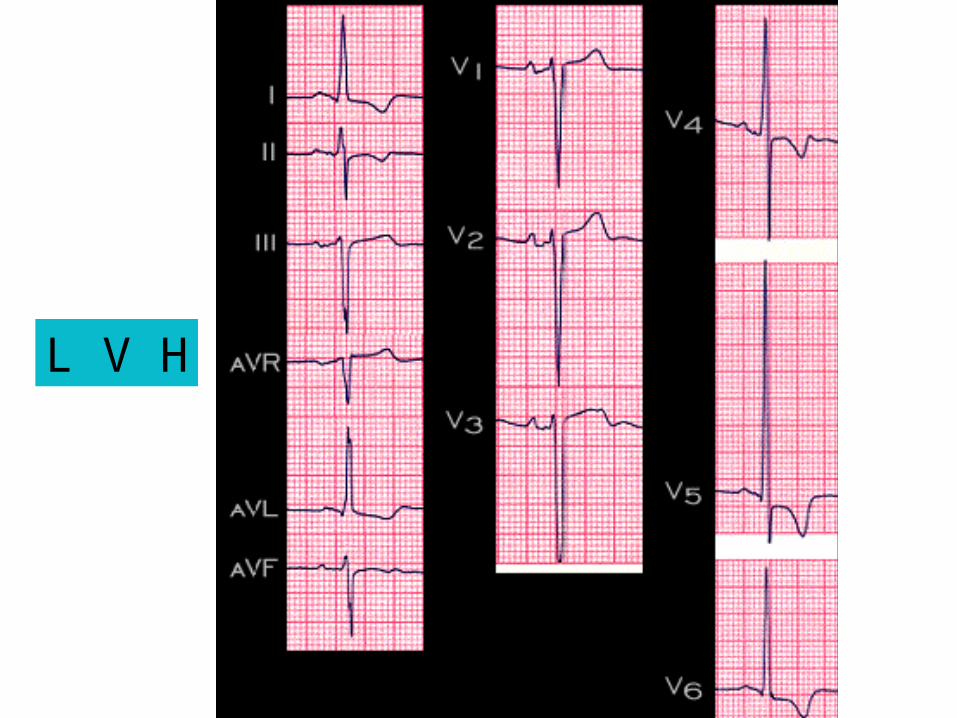
L V H
R V H
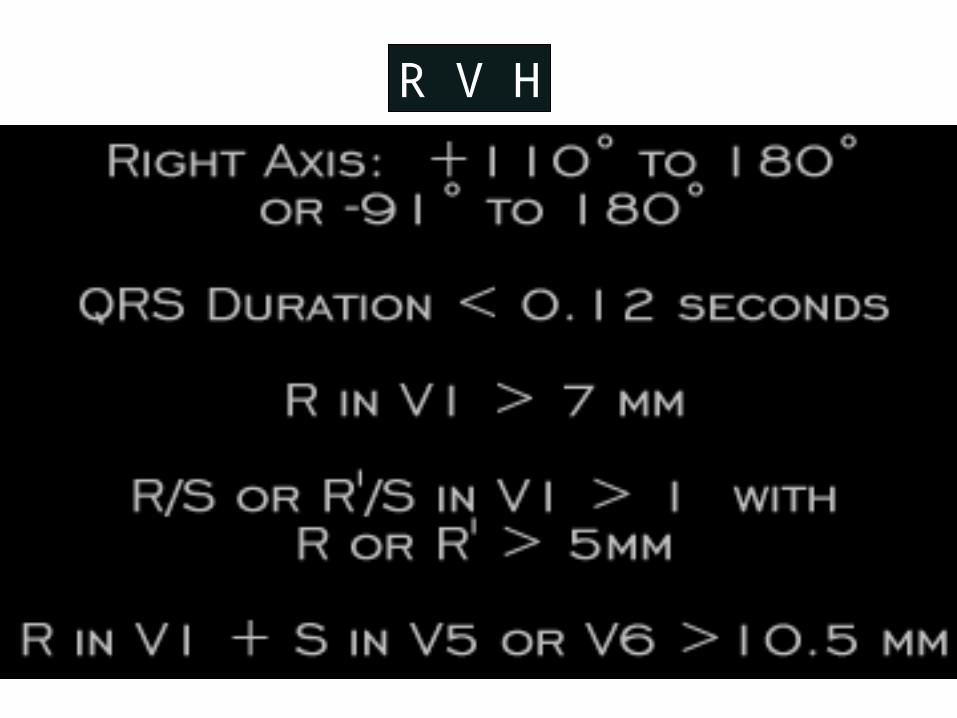
R V H
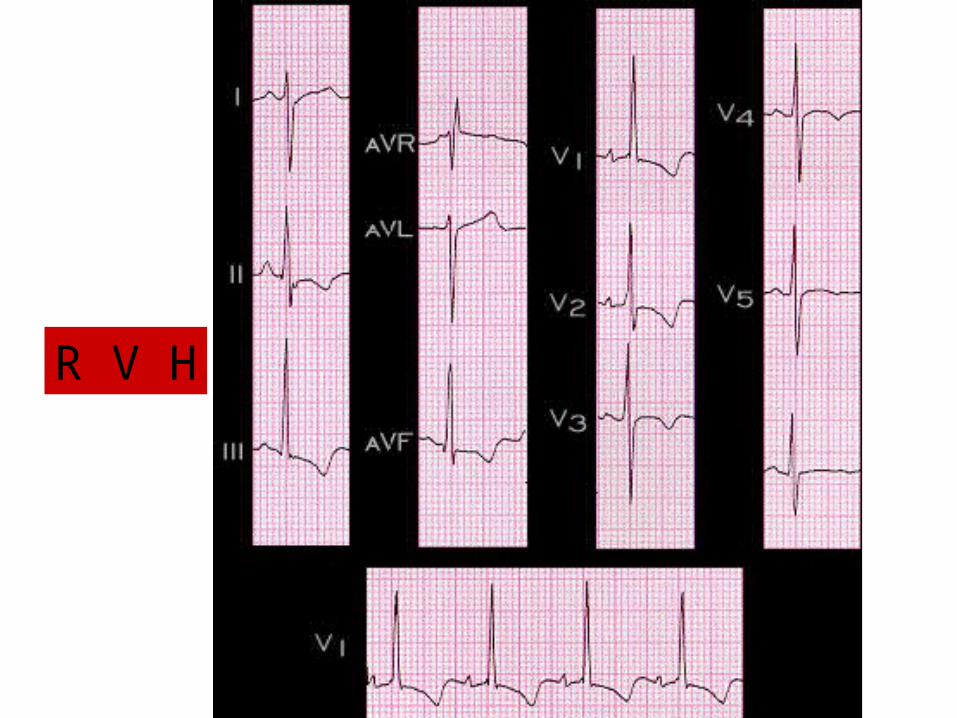
R V H

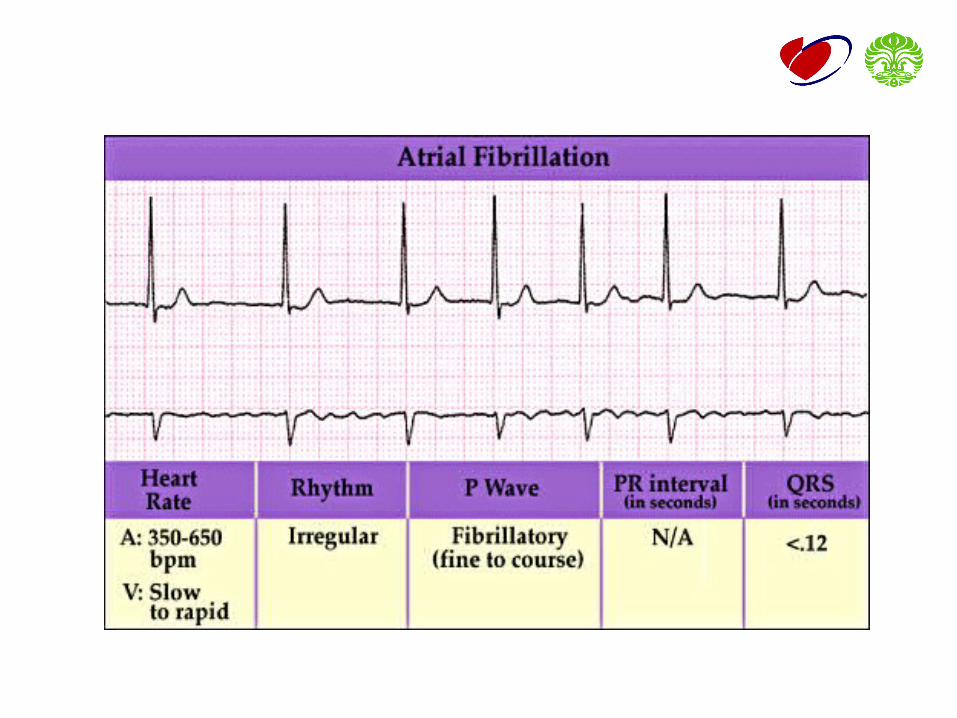
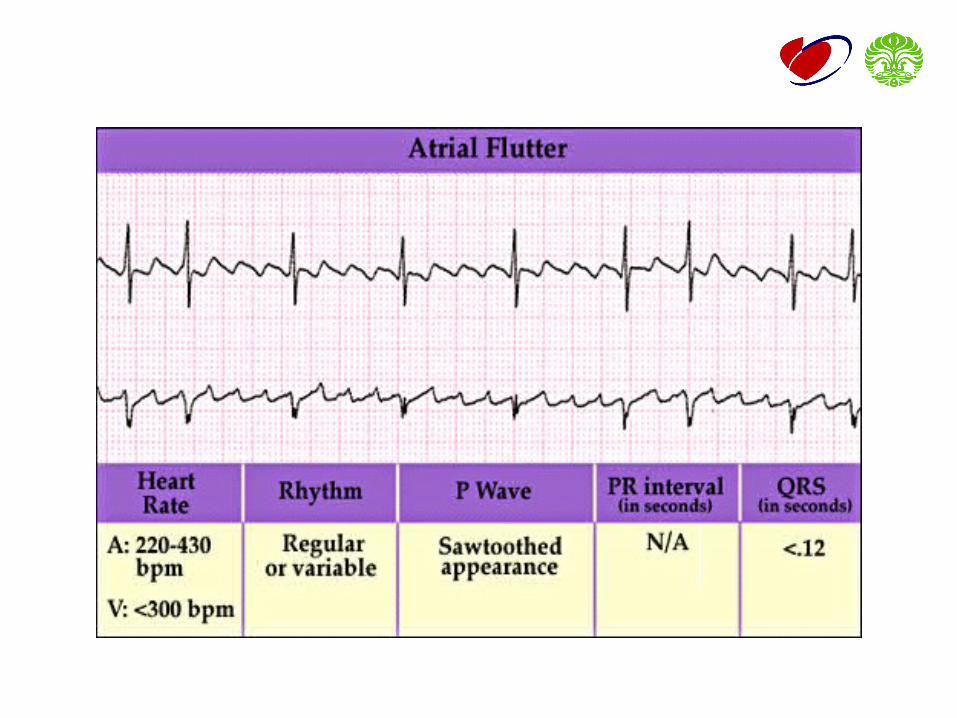
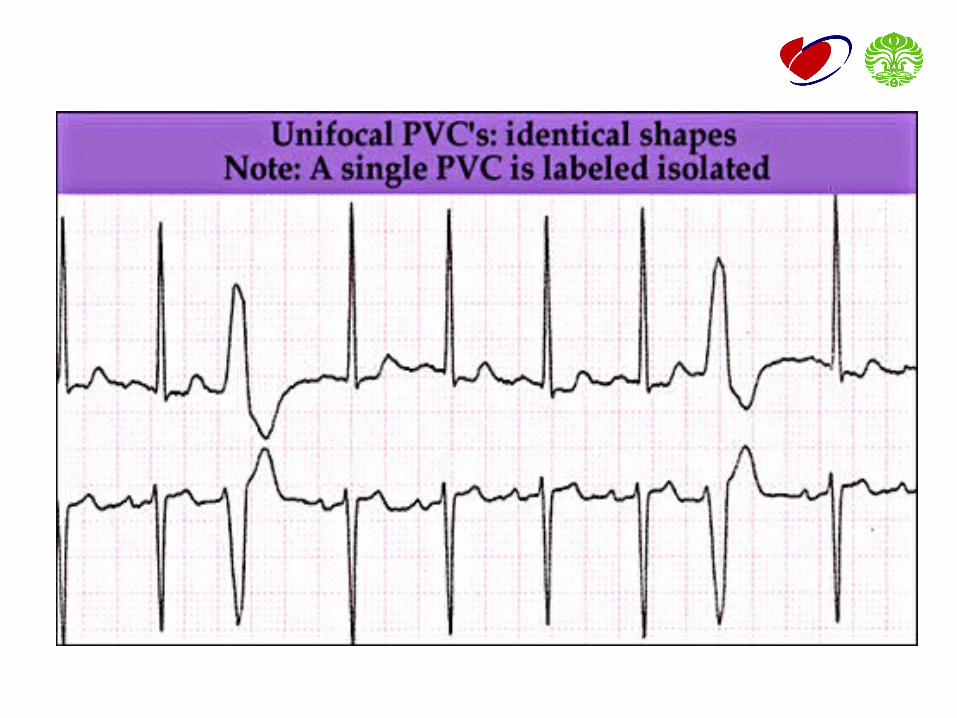
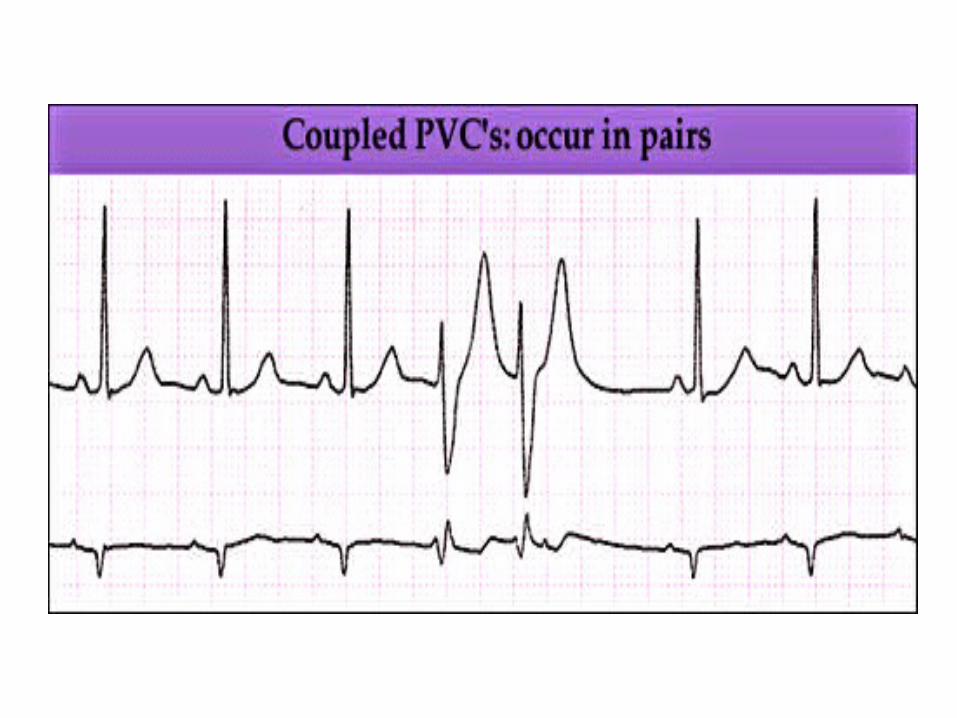
ARRHYTHMIA
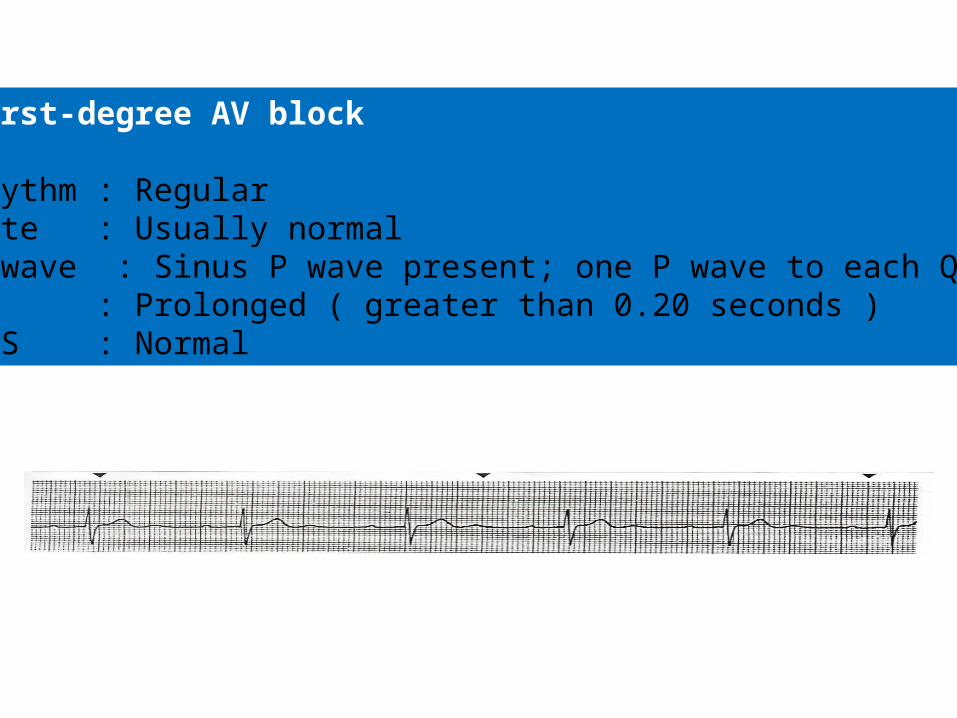
First-degree AV block
Rhythm : RegularRate : Usually normalP wave : Sinus P wave present; one P wave to each QRSPR : Prolonged ( greater than 0.20 seconds )QRS : Normal
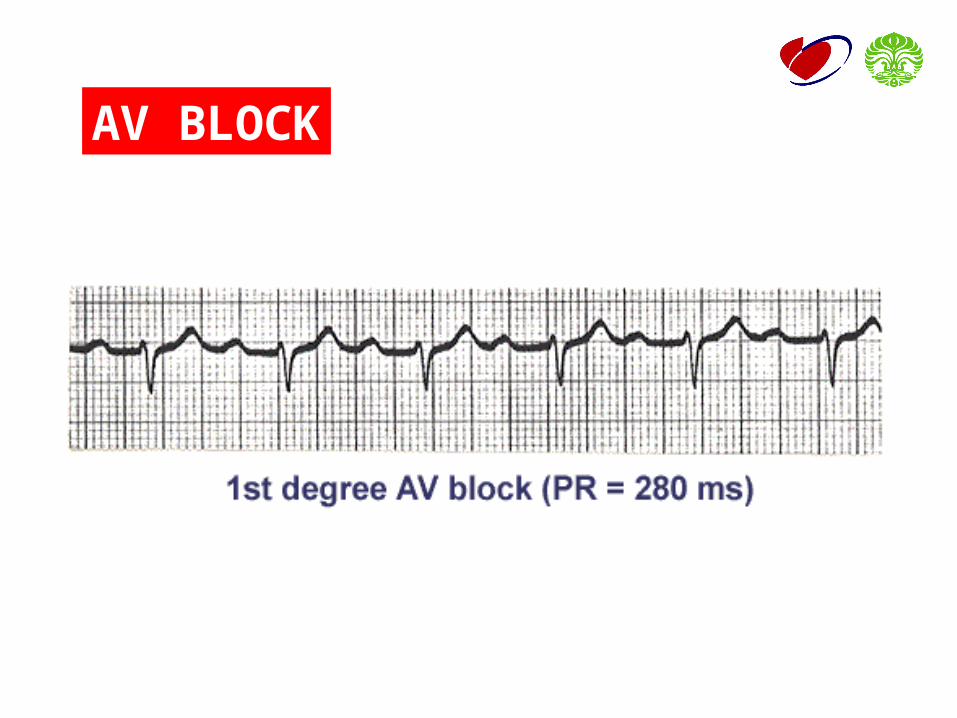
AV BLOCK
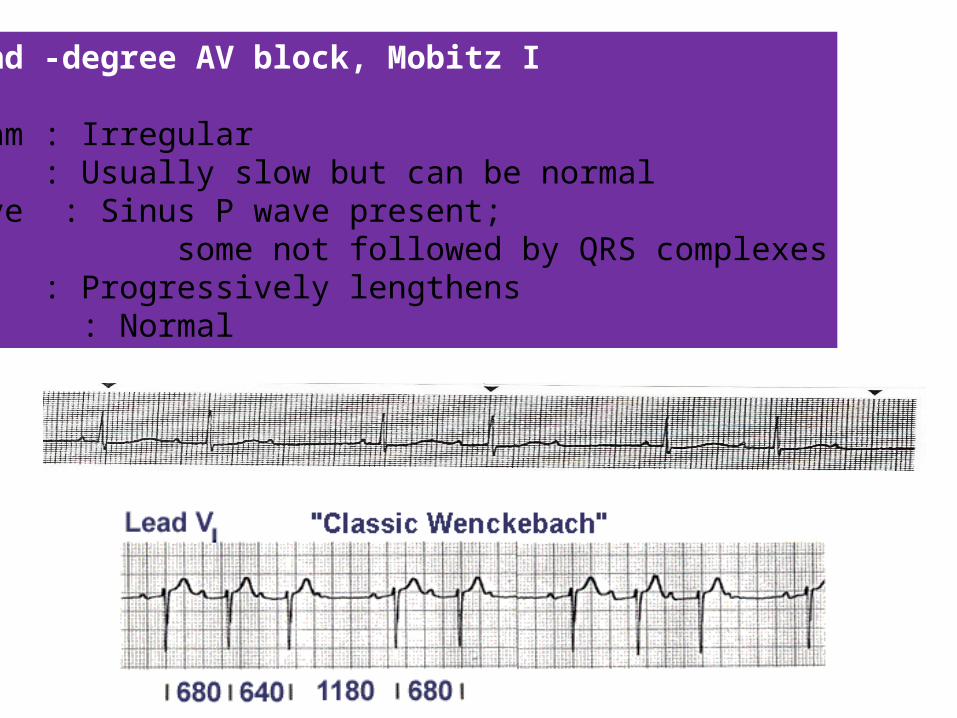
Second -degree AV block, Mobitz I
Rhythm : IrregularRate : Usually slow but can be normalP wave : Sinus P wave present; some not followed by QRS complexesPR : Progressively lengthensQRS : Normal
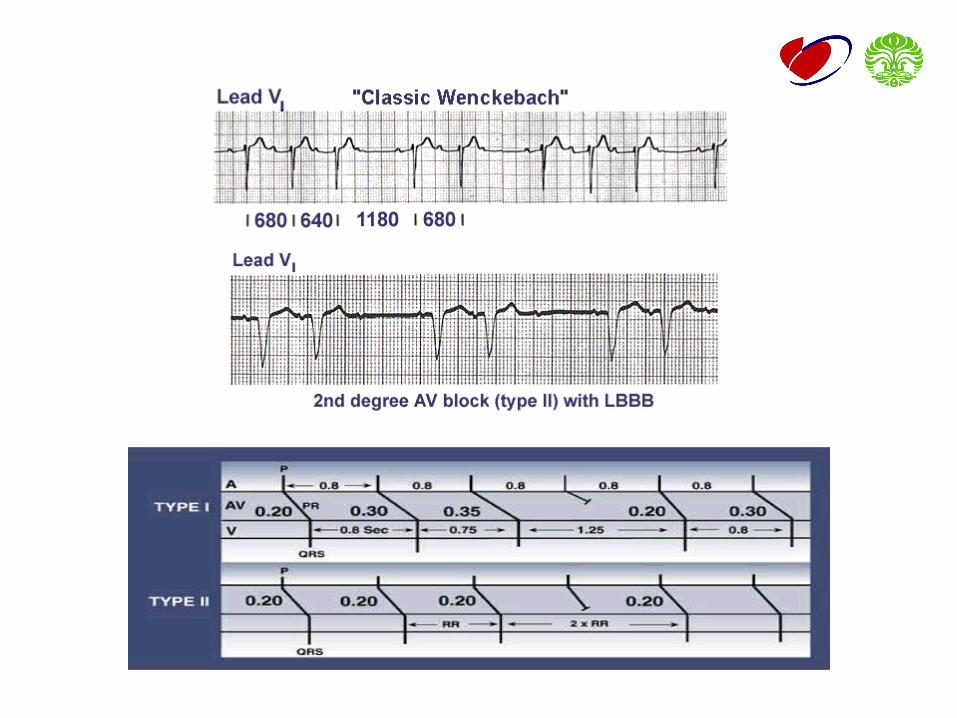
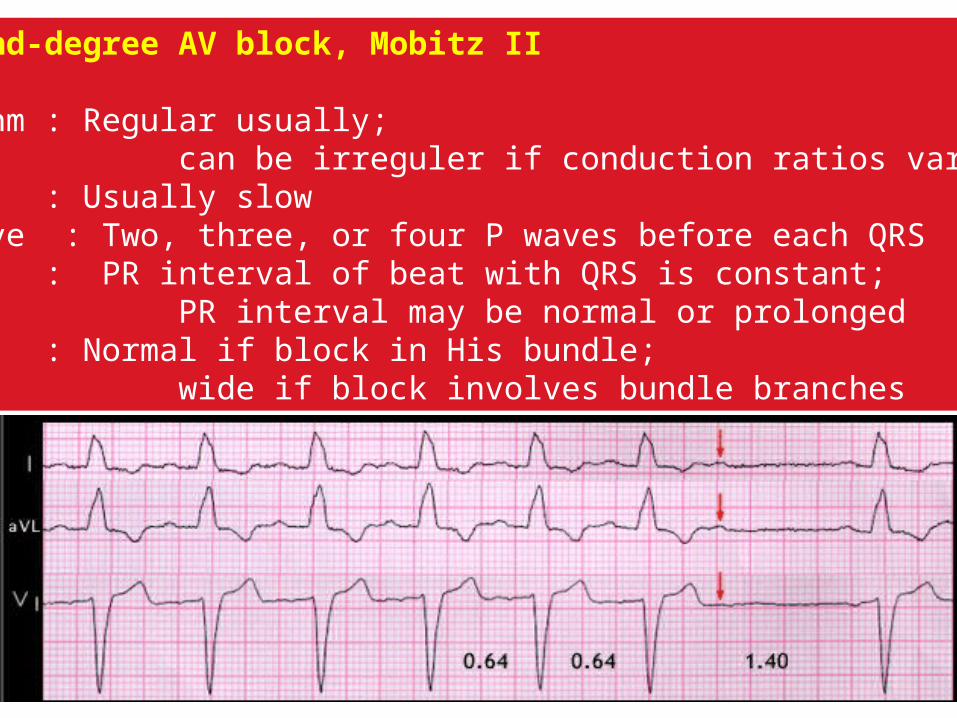
Second-degree AV block, Mobitz II
Rhythm : Regular usually; can be irreguler if conduction ratios varyRate : Usually slowP wave : Two, three, or four P waves before each QRSPR : PR interval of beat with QRS is constant; PR interval may be normal or prolongedQRS : Normal if block in His bundle; wide if block involves bundle branches
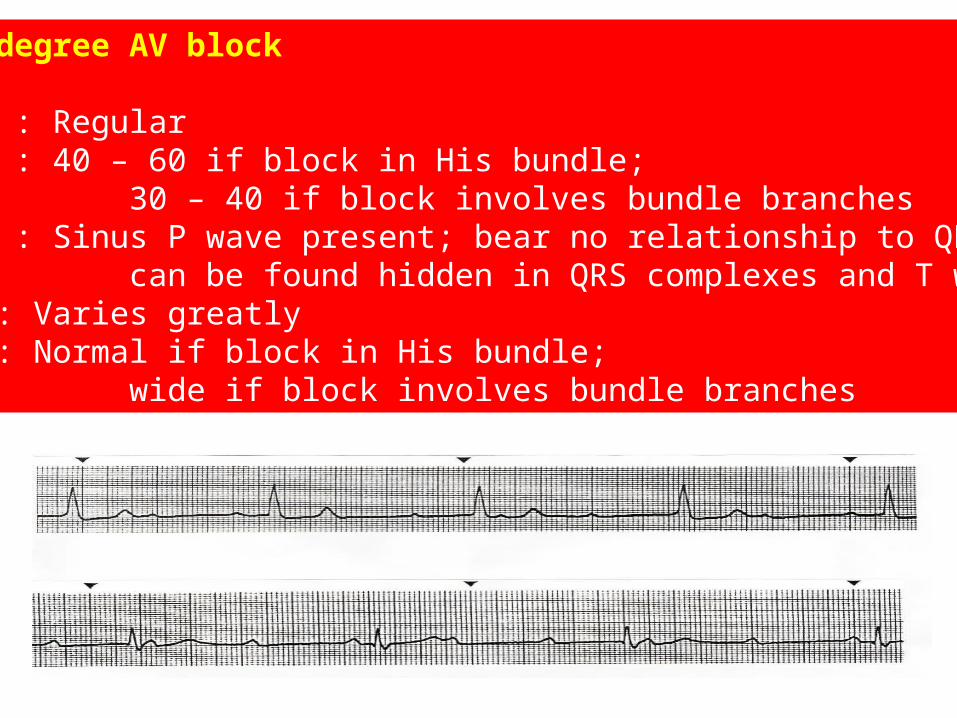
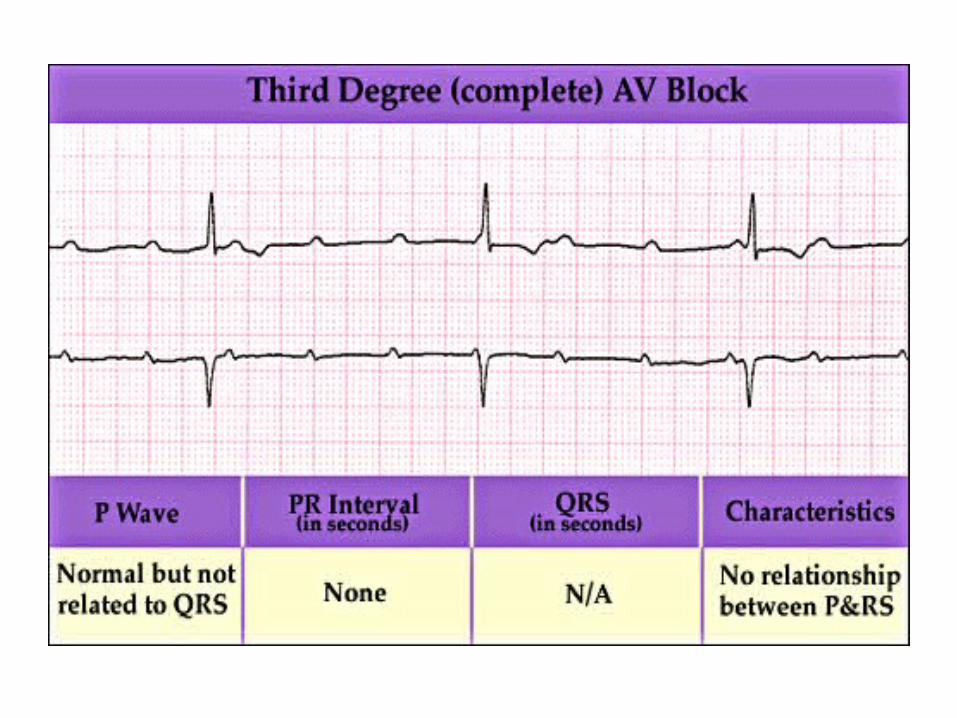
Third-degree AV block
Rhythm : RegularRate : 40 – 60 if block in His bundle; 30 – 40 if block involves bundle branchesP wave : Sinus P wave present; bear no relationship to QRS; can be found hidden in QRS complexes and T wavesPR : Varies greatlyQRS : Normal if block in His bundle; wide if block involves bundle branches
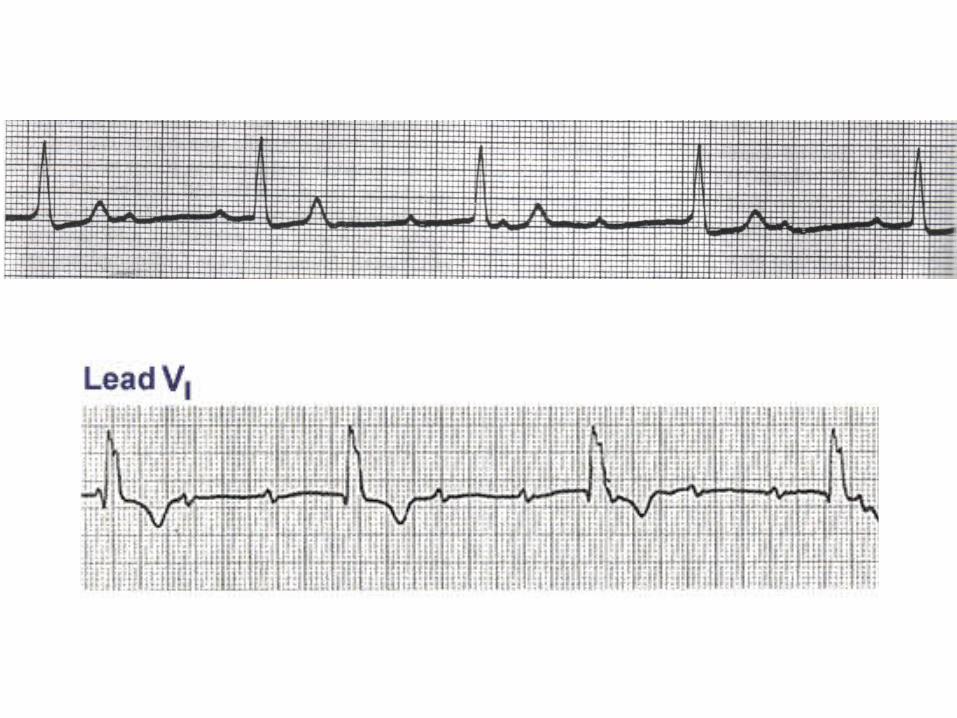
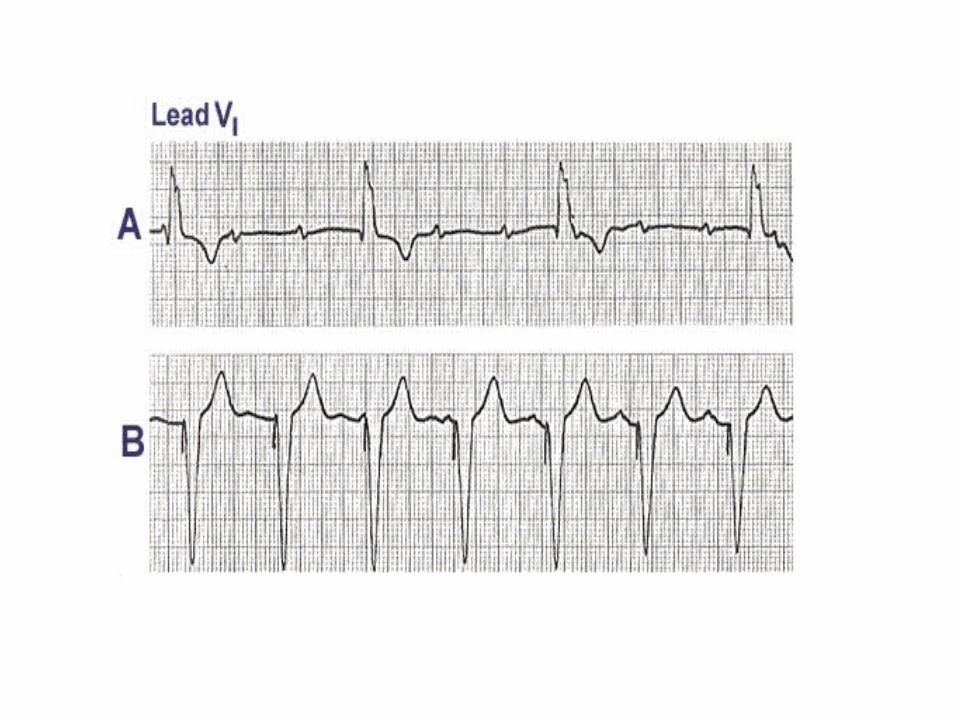
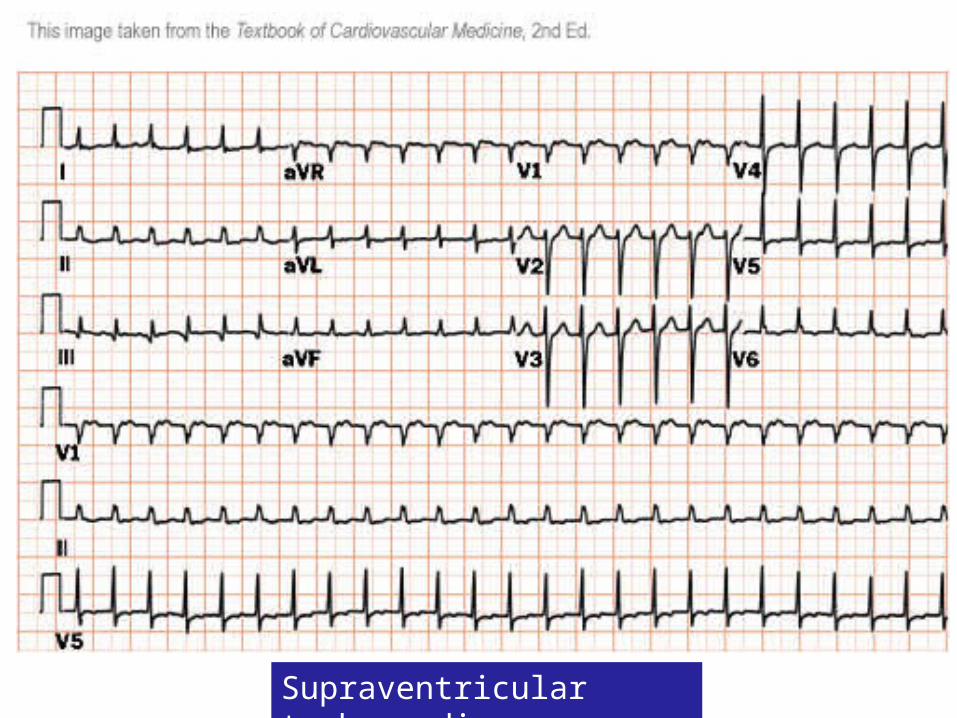
Supraventricular tachycardia
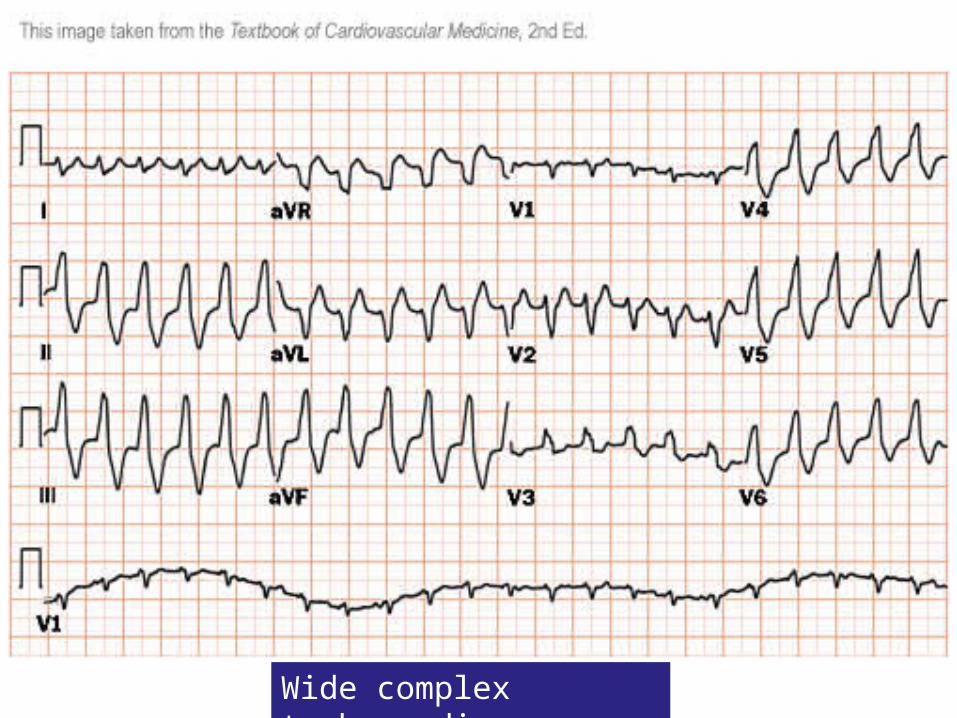
Wide complex tachycardia
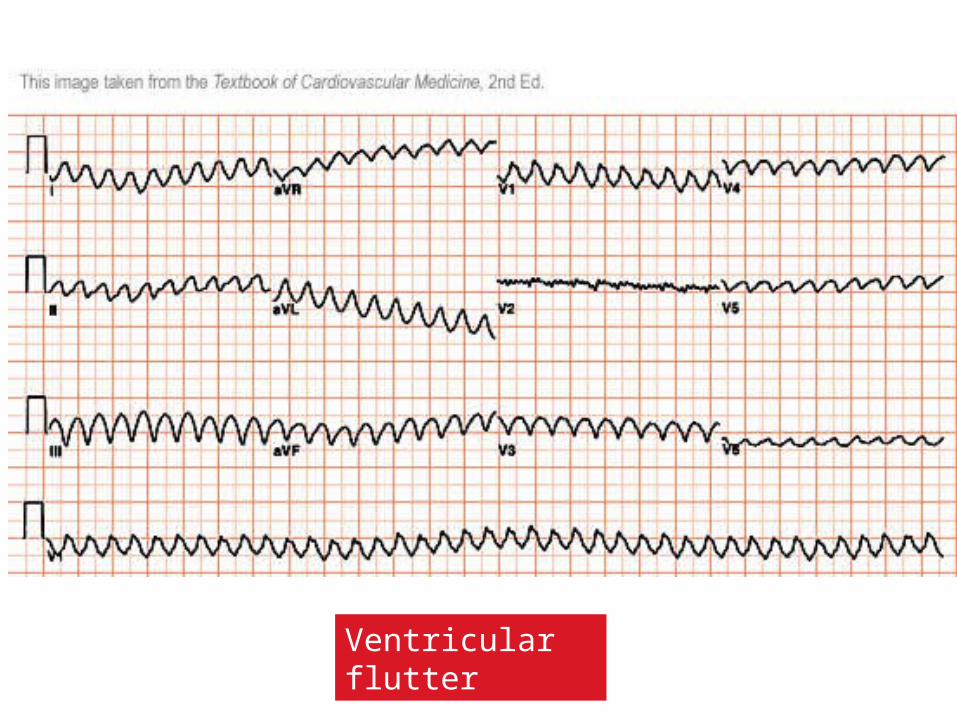
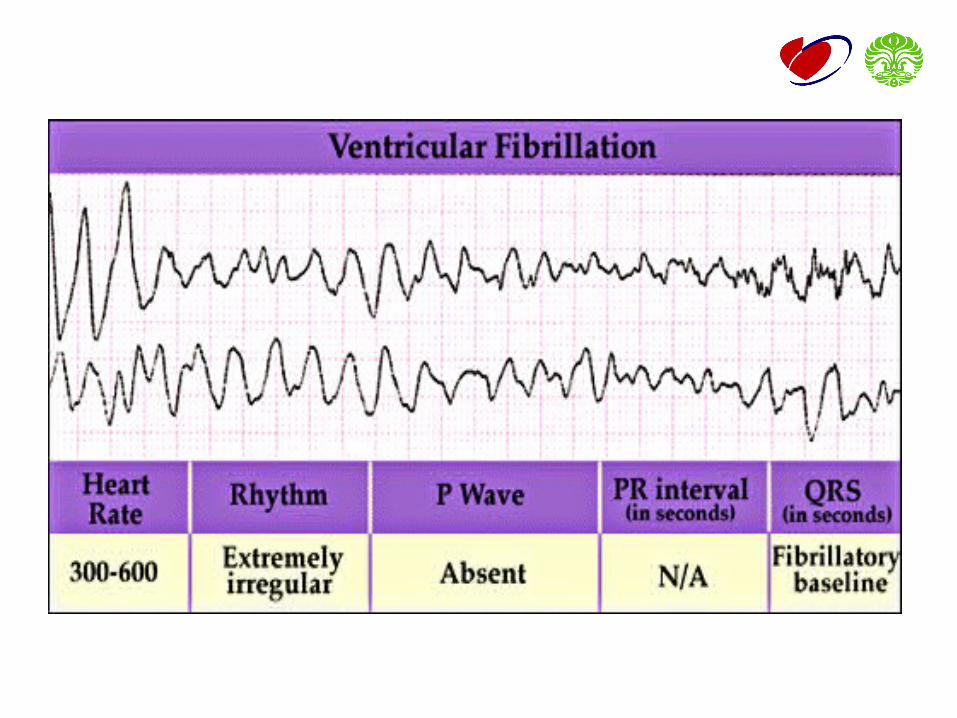
Ventricular flutter