Embed Size (px)
Citation preview

ECMO in Evolution: The Impact of Changing Patient Demographics and Alternative Therapies on ECMO
By Jay M. Wilson, Lynne K. Bower, John E. Thompson, Dario O. Fauza, and James C. Fackler Boston, Massachuset ts
• The incidence of neonatal extracorporeal membrane oxygenation (ECMO} is decreasing nationally. This decrease is presumed to be a result of the emergence of alternative technologies such as high-frequency oscillatory ventilation (HFOV), nitric oxide (NO), and surfactant therapy as well as Others. The purposes of the present report were to determine just how rapidly the demographics of ECMO are changing and to determine the impact of competing technologies on ECMO use. The authors reviewed their entire ECMO experi- ence of 455 cases (370 neonatal, 38 pediatric, and 47 cardiac). The neonatal cases also were separated into diagnostic groups: MAS (meconium aspiration syndrome), PPHN (persis- tent pulmonary hypertension of the newborn), RDS (respira- tory distress syndrome), and sepsis. To al low statistical comparison, the patients were divided into four chronologi- cal groups, of equal 3-year duration, spanning the 12 years that ECMO has been available. The results of the analysis demonstrated four principle findings. (1) The total number of patients receiving ECMO per year was declining (P = .0001). This decline was attr ibutable to a reduction in the total number of neonatal patients, wi th the exception of cases of congenital diaphragmatic hernia. (2) The complexity of each ECMO run was increasing, as evidenced by substantial increases in mean ECMO duration per patient and an increase in the incidence of patient complications on ECMO (P = .0001). (3) There has been a significant decrease in the overall survival rate for patients treated wi th ECMO (P = .0001). (4) The ECMO population mix has shifted away from straightfor- ward neonatal cases and toward the more complex pediatric and cardiac cases. This demographic shift has occurred as a result of improvements in pre-ECMO management of neona- tal patients, and is primarily responsible for the findings noted above. However, there also has been a worsening of condition severity within each diagnostic group, which also is partly responsible for the changes noted. If these trends continue, pediatric, cardiac, and CDH patients wi l l likely account for the majority of ECMO patients. Consequently, existing ECMO centers must be prepared to adapt to the changing demographics by evolving programs that support pediatric, cardiac, and adult patients, in addition to neonates. Furthermore, the complexity associated wi th transporting these unstable older patients and the likelihood that the number of active ECMO centers wi l l decline may require remaining ECMO centers to develop long-distance ECMO transport capabilities. Copyright © 1996 by W.B. Saunders Company
From the Departments of Surgery, Anesthesia, and Respiratory Care, Children's Hospital, Boston, )VIA.
Presented at the 1995 Annual Meeting of the Section On Surgery of the American Academy of Pediatrics, San Francisco, California, October 13-15, 1995.
Address reprint requests to Jay M Wilson, MD, Children's Hospital, 300 Longwood Ave, Fegan 4, Boston, MA 02115.
Copyright © 1996 by W.B. Saunders Company 0022-3468/96/3108-0026503. 00/0
INDEX WORDS: Extracorporeal membrane oxygenation, con- genital diaphragmatic hernia, meconium aspiration syn- drome, high-frequency oscillating ventilation, nitric oxide.
I N 1982, Bartlett et al first reported that extracorpo- real membrane oxygenation (ECMO) could im-
prove the survival rate for neonates with profound persistent pulmonary hypertension of the newborn (PPHN). 1 The number of neonatal patients treated with ECMO rapidly proliferated until 1992, when the number of ECMO centers in the United States exceeded 100 and the number of neonates treated exceeded 1,400 per year. 2 The application of ECMO to nonneonatal patients with pulmonary or cardiac failure was less successful and, consequently, growth in these areas lagged behind that of neonatal ECMO. 3 However, since 1990 the use of ECMO in these patients has increased markedly throughout the United States.
Beginning in 1990, alternate modalities such as high-frequency oscillatory ventilation (HFOV), 4,5 sur- factant administration, 6,7 and (later) the investiga- tional use of nitric oxide ( N O ) 8,9 became available, Subsequently, experience with these modalities rap- idly increased and it appears that ECMO use in neonatal patients has begun to decline}
At our institution, neonatal ECMO was introduced in 1984, and subsequently pediatric pulmonary and cardiac capabilities were added. In 1991 and 1992, trials of HFOV and NO for treatment of neonatal pulmonary failure were begun. With encouraging initial experience, the utilization of both HFOV and NO has increased in neonates and the use of ECMO has decreased.
The purposes of the present study are to detail the changes that have occurred in our ECMO program during the past decade and to evaluate the recent impact of alternate therapies on ECMO use, ECMO duration, incidence of complications, and outcome by analyzing our 12-year experience with 455 patients treated with ECMO.
MATERIALS AND METHODS
ECMO was first introduced to our institution in 1984. Initially it was used exclusively for the treatment of infants with congenital diaphragmatic hernia (CDH). In 1985, a prospective randomized trial of ECMO versus conventional ventilation (CMV) was begun in patients with PPHN and meconium aspiration syndrome, l° At the conclusion of that trial in 1988, which demonstrated the
1116 Journal of Pediatric Surgery, Vo131, No 8 (August), 1996: pp 1116-1123

ECMO IN EVOLUTION 1117
superiority of ECMO over CMV, ECMO was offered broadly to all infants with PPHN in whom CMV had failed.
Until 1991, failure of CMV was defined as oxygenation index (OI = mean airway pressure x FIO2/Po2) of greater than 0.4, which previously had been demonstrated to predict high mortal- ity. 11 Beginning in 1991, HFOV became available, and by 1992 most infants with MAS, PPHN, and sepsis routinely received a trial of HFOV before referral for ECMO. Because no specific criteria were available to indicate failure of HFOV, less specific criteria (best characterized as failure to respond and presumption of a high likelihood of mortality) were used. Also beginning in 1992, NO became available and a prospective randomized trial to evaluate its performance was begun in August 1992. In 1994, the NO trial was modified to allow the use of both HFOV and NO in some patients.
For infants with CDH, ECMO was offered only postoperatively between 1984 and 1987. Between 1987 and 1991, ECMO was offered preoperatively for these patients, but the repair was performed after decannulation from ECMO. After 1991, the diaphragmatic hernia repair was performed while the patients received ECMO.
For the pediatric and cardiac patients, less specific criteria for ECMO institution were used throughout the study period. This was best characterized as failure to respond and presumption of a high likelihood of mortality. Some patients also were treated with NO or HFOV. 12
Until 1990, ECMO exclusion criteria among the neonatal popu- lation included gestational age of less than 34 weeks, birth weight of less than 2 kg, intracranial hemorrhage of greater than grade 1, uncontrollable coagulopathy, or presence of another fatal condi- tion. After 1990, with the introduction of aggressive exchange transfusions/plasmapheresis on ECMO for patients with coagulop- athy, this contraindication was dropped. After 1991, with the introduction of aminocaproic acid (AMICAR; Lederle Parenter- als, Carolina, Puerto Rico) the weight, gestational age, and intracranial hemorrhage criteria were dropped, and patients previ- ously excluded by those criteria were considered on a case-by-case basisfl 3
For purposes of statistical analysis, the 12-year period was broken into four equal groups of 3 years each: group 1 (1984-1986), all appropriate CDH patients and MAS/PPHN patients only as part of a randomized prospective trial; group 2 (1987-1989), unrestricted access of all appropriate CDH and MAS/PPHN cases, noncoagulopathic sepsis patients, pediatric pulmonary patients, and cardiac patients; group 3 (1990-1992), unrestricted access for all CDH, MAS/PPHN, sepsis (including coagulopathic), pediatric, and cardiac patients, with aminocaproic acid (AMICAR) and exchange transfusions employed routinely; group 4 (1992-1995), unrestricted access to all patient groups noted in group 3. However, patients with MAS/PPHN usually received a trial of HFOV and/or NO before referral for ECMO. The groups were compared with respect to ECMO volume, population demographics, ECMO duration, incidence of major complications, and outcome. The major patient complications included cardiopulmonary resuscita- tion immediately before or during ECMO, seizures, major hemor- rhage requiring operation or massive transfusion, development or extension of intracranial hemorrhage, cerebral infarct, dialysis, or brain death. Less severe complications (eg, hypertension, elevated bilirubin or creatinine level) were not evaluated. The major circuit complications evaluated included any malfunction in electronic equipment that required replacement or resulted in interruption of flow, replacement of any portion of the circuit for bleeding, rupture, thrombosis, or air. Less severe complications (eg, chatter or small amounts of air easily evacuated from circuit) were not analyzed. Survival was defined as discharge home.
Statistical analysis was performed using contingency table analy-
sis, regression analysis, or analysis of variance (ANOVA). The significance of pairwise comparisons within each group was deter- mined by post-hoc testing with the Scheffe F test. P values of less than .05 were considered significant.
RESULTS
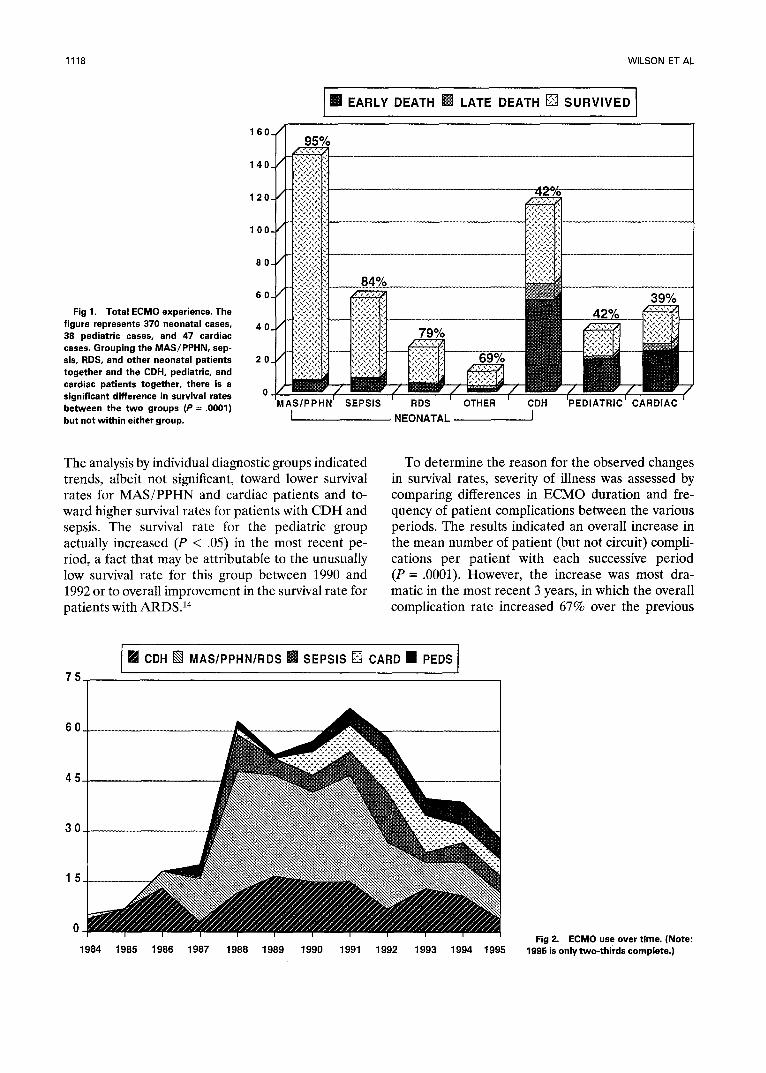
Be tw e e n F e b r u a r y 1984 and Augus t 1995, E C M O was p e r f o r m e d 455 t imes in 447 pa t ien ts . Eight pa t ien t s were p l a c e d on E C M O twice (5 C D H , 1 M A S , 1 sepsis, 1 card iac) , five of w h o m survived. T h e r e were 370 neona t a l cases, 38 ped i a t r i c cases, and 47 ca rd iac cases. Excluding the C D H cases, the survival ra te for the n e o n a t a l g roup was 89%. In contras t , the overal l survival ra te for the C D H , p e d i a t r i c , a n d c a r d i a c g r o u p s was a b o u t 41% (P = .0001) (Fig 1). The m e a n du ra t i on of E C M O var ied b e t w e e n the d iagnos t ic groups, bu t was signifi- cant ly longer only for the ped ia t r i c g roup (P = .0001). Similarly, the inc idence of ma jo r pa t i e n t and circui t compl ica t ions va r i ed widely b e t w e e n the groups; bu t again the inc idence was significantly g r e a t e r only for the ped ia t r i c g roup (P = .0001). However , when the inc idence of pa t i en t and ci rcui t compl ica t ions was ad jus ted for the m e a n E C M O d u r a t i o n of each group, t he re was no significant d i f ference b e t w e e n any of the groups with r ega rd to c i rcui t compl ica t ions , and pa t i en t compl ica t ions p e r hour on E C M O were s igni f icant ly h ighe r on ly for t he c a r d i a c g roup (P < .05).
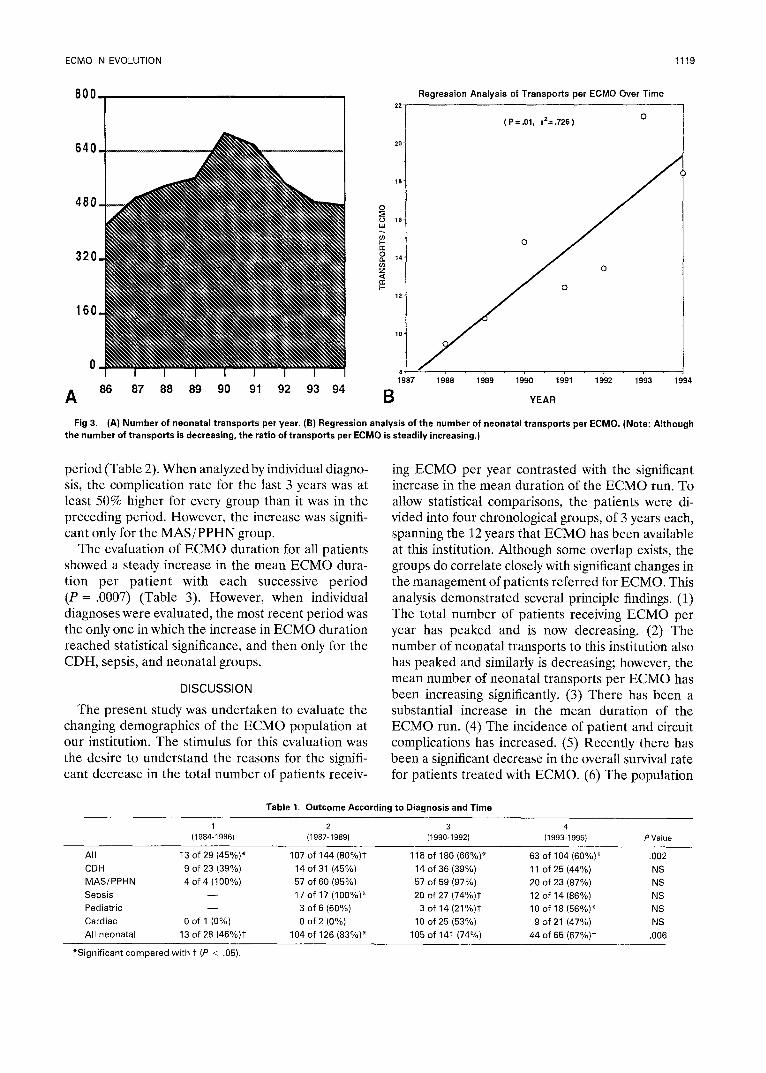
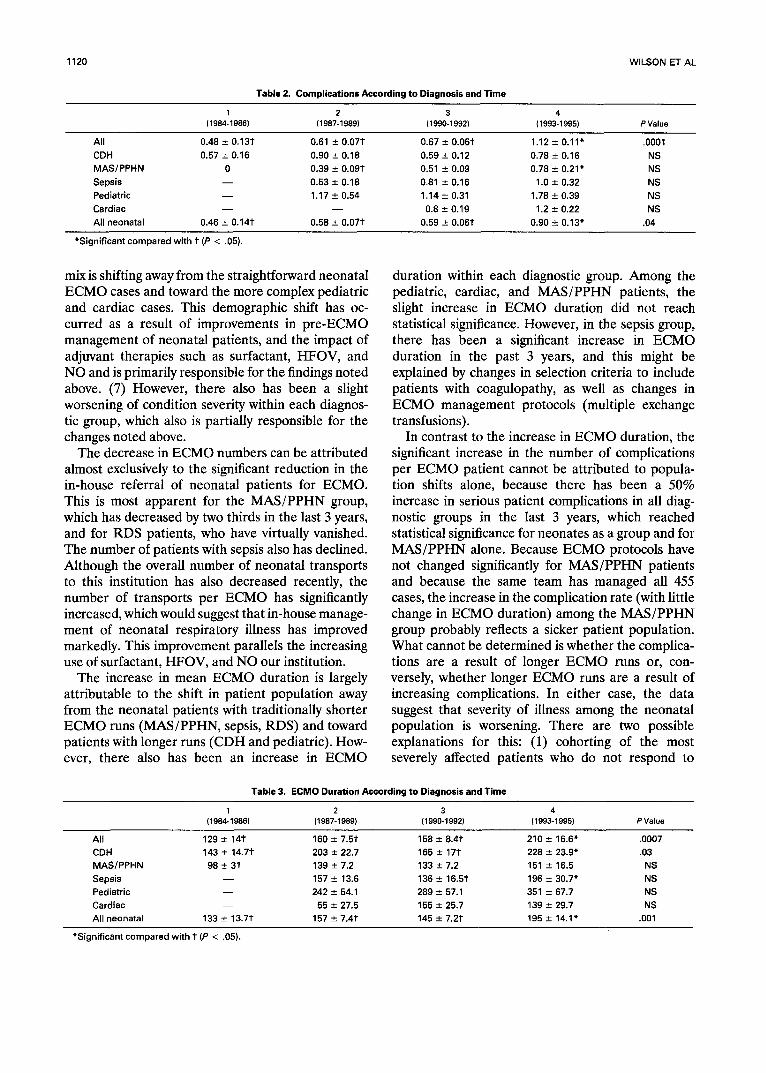
T h e analysis of E C M O use over t ime showed tha t the to ta l n u m b e r of E C M O cases p e r yea r p e a k e d in 1991 and s teadi ly d e c r e a s e d since (Fig 2). T h e num- be r of n e o n a t a l t r anspor t s to this ins t i tu t ion had a s imi lar pa t te rn , and has b e e n dec reas ing recen t ly (Fig 3). However , regress ion analysis of the m e a n n u m b e r of n e o n a t a l t r anspo r t s u n d e r t a k e n for each E C M O p e r f o r m e d ind ica t ed a significant inc rease in t r anspor t s pe r E C M O beg inn ing in 1988 (P = .01; R 2 = .726).
To al low sta t is t ical compar i sons , the to ta l E C M O exper i ence was d iv ided into four 3-year pe r i ods (each compr i s ing a 3-year p e r i o d ) r e p r e se n t i ng s e p a r a t e cl inical e ras of E C M O use, as desc r ibed above. This analysis d e m o n s t r a t e d an increase in the to ta l num- be r of E C M O cases over the first t h r e e -ye a r per iod , fo l lowed by a decl ine . This change was a t t r i bu tab le to a d r ama t i c dec rease in the n u m b e r neona t a l pa t i en t s with the except ion of C D H cases (Fig 2). Because the n u m b e r of C D H , ped ia t r ic , and ca rd iac pa t i en t s has no t d e c r e a s e d significantly, they accoun ted for a l a rger pe r c e n t a ge of the to ta l popu l a t i on in the last 3 years . C o n c o m i t a n t wi th the r ecen t dec l ine in E C M O vo lume was a significant dec rea se in the overal l survival ra te , f rom 80% in the second p e r i o d to 66% in the th i rd 60% in the four th (P = .002) (Tab le 1).
1118 WILSON ET AL
Fig 1. Total ECMO experience. The figure represents 370 neonatal cases, 38 pediatric cases, and 47 cardiac cases. Grouping the MAS/PPHN, sep- sis, RDS, and other neonatal patients together and the CDH, pediatric, and cardiac patients together, there is a significant difference in survival rates between the two groups (P = .0001) but not within either group.
1 6 0 .
1 4 0 .
1 2 0 .
1 0 0 .
8 0 -
6 0 -
4 0
20
0
I NN EARLY DEATH [] LATE DEATH [] SURVIVED ] 95%
-ii!iii!iii l J NEONATAL J
39%
The analysis by individual diagnostic groups indicated trends, albeit not significant, toward lower survival rates for MAS/PPHN and cardiac patients and to- ward higher survival rates for patients with CDH and sepsis. The survival rate for the pediatric group actually increased (P < .05) in the most recent pe- riod, a fact that may be attributable to the unusually low survival rate for this group between 1990 and 1992 or to overall improvement in the survival rate for patients with ARDS.14
To determine the reason for the observed changes in survival rates, severity of illness was assessed by comparing differences in ECMO duration and fre- quency of patient complications between the various periods. The results indicated an overall increase in the mean number of patient (but not circuit) compli- cations per patient with each successive period (P = .0001). However, the increase was most dra- matic in the most recent 3 years, in which the overall complication rate increased 67% over the previous
75 I PJ CDH [] MAS/PPHN/RDS • SEPSIS [] CARD • PEDS I
60
45
30
15
0 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995
Fig 2. ECMO use over time. (Note: 1996 is only two-thirds complete.)
Regression Analysis of Transports per ECMO Over Time
3 2 0 .
1 6 0 .
0
A
I I I i I I I 86 87 88 89 90 91 92 93 94
800
6 4 0 .
4 8 0 .
18
16
14
12
10
(P =.01, r2=.726) O
(
ECMO IN EVOLUTION 1119
8 ' , . . . . , .
87 1988 1989 1990 1991 1992 1993 1994
B YEAR
Fig 3. (A) Number of neonatal transports per year. (B) Regression analysis of the number of neonatal transports per ECMO. (Note: Although the number of transports is decreasing, the ratio of transports per ECMO is steadily increasing.)
period (Table 2). When analyzed by individual diagno- sis, the complication rate for the last 3 years was at least 50% higher for every group than it was in the preceding period. However, the increase was signifi- cant only for the MAS/PPHN group.
The evaluation of ECMO duration for all patients showed a steady increase in the mean ECMO dura- tion per patient with each successive period (P = .0007) (Table 3). However, when individual diagnoses were evaluated, the most recent period was the only one in which the increase in ECMO duration reached statistical significance, and then only for the CDH, sepsis, and neonatal groups.
DISCUSSION
The present study was undertaken to evaluate the changing demographics of the ECMO population at our institution. The stimulus for this evaluation was the desire to understand the reasons for the signifi- cant decrease in the total number of patients receiv-
ing ECMO per year contrasted with the significant increase in the mean duration of the ECMO run. To allow statistical comparisons, the patients were di- vided into four chronological groups, of 3 years each, spanning the 12 years that ECMO has been available at this institution. Although some overlap exists, the groups do correlate closely with significant changes in the management of patients referred for ECMO. This analysis demonstrated several principle findings. (1) The total number of patients receiving ECMO per year has peaked and is now decreasing. (2) The number of neonatal transports to this institution also has peaked and similarly is decreasing; however, the mean number of neonatal transports per ECMO has been increasing significantly. (3) There has been a substantial increase in the mean duration of the ECMO run. (4) The incidence of patient and circuit complications has increased. (5) Recently there has been a significant decrease in the overall survival rate for patients treated with ECMO. (6) The population
Table 1. Outcome According to Diagnosis and Time
1 2 3 4 (1984-1986) (1987-1989) (1990-1992) (1993-1995) P Value
All 13 of 29 (45%)* 107 of 144 (80%)1- 118 of 180 (66%)* 63 of 104 (60%)* .002
CDH 9 of 23 (39%) 14 of 31 (45%) 14 of 36 (39%) 11 of 25 (44%) NS MAS/PPHN 4 of 4 (100%) 57 of 60 (95%) 57 of 59 (97%) 20 of 23 (87%) NS
Sepsis - - 17 of 17 (100%)* 20 of 27 (74%)1- 12 of 14 (86%) NS Pediatric - - 3 of 6 (50%) 3 of 14 (21%)1" 10 of 18 (56%)* NS
Cardiac 0 of 1 (0%) 0 of 2 (0%) 10 of 25 (53%) 9 of 21 (47%) NS All neonatal 13 of 28 (46%)1. 104 of 126 (83%)* 105 of 141 (74%) 44 of 65 (67%)1" .006
*Significant compared with 1" (P < .05).
1120 WILSON ET AL
Table 2. Complications According to Diagnosis and Time
1 2 3 4 (1984-1986) (1987-1989) { 1990-1992) (1993-1995) P Value
All
CDH
MAS/PPHN
Sepsis Pediatric Cardiac All neonatal
0.48 _+ 0.13t 0.61 _+ 0.07t 0.67 _+ 0.06t 1.12 -+ 0.11" .0001
0.57 _+ 0.16 0.90 -+ 0.18 0.59 -+ 0.12 0.78 ± 0.16 NS
0 0.39 ± 0.09t 0.51 _+ 0.09 0.78 +_ 0.21" NS
- - 0.53 _+ 0.18 0.81 _+ 0.16 1.0 _+ 0.32 NS
- - 1.17 +_ 0.54 1.14 ± 0.31 1.78 _+ 0.39 NS
- - - - 0.8 -+ 0.19 1.2 _+ 0.22 NS
0.46 _+ 0.14t 0.58 -+ 0.07t 0.59 --- 0.06"¢ 0.90 +_ 0.13" .04
*Signi f icant compared wi th t (P < .05).
mix is shifting away from the straightforward neonatal ECMO cases and toward the more complex pediatric and cardiac cases. This demographic shift has oc- curred as a result of improvements in pre-ECMO management of neonatal patients, and the impact of adjuvant therapies such as surfactant, HFOV, and NO and is primarily responsible for the findings noted above. (7) However, there also has been a slight worsening of condition severity within each diagnos- tic group, which also is partially responsible for the changes noted above.
The decrease in ECMO numbers can be attributed almost exclusively to the significant reduction in the in-house referral of neonatal patients for ECMO. This is most apparent for the MAS/PPHN group, which has decreased by two thirds in the last 3 years, and for RDS patients, who have virtually vanished. The number of patients with sepsis also has declined. Although the overall number of neonatal transports to this institution has also decreased recently, the number of transports per ECMO has significantly increased, which would suggest that in-house manage- ment of neonatal respiratory illness has improved markedly. This improvement parallels the increasing use of surfactant, HFOV, and NO our institution.
The increase in mean ECMO duration is largely attributable to the shift in patient population away from the neonatal patients with traditionally shorter ECMO runs (MAS/PPHN, sepsis, RDS) and toward patients with longer runs (CDH and pediatric). How- ever, there also has been an increase in ECMO
duration within each diagnostic group. Among the pediatric, cardiac, and MAS/PPHN patients, the slight increase in ECMO duration did not reach statistical significance. However, in the sepsis group, there has been a significant increase in ECMO duration in the past 3 years, and this might be explained by changes in selection criteria to include patients with coagulopathy, as well as changes in ECMO management protocols (multiple exchange transfusions).
In contrast to the increase in ECMO duration, the significant increase in the number of complications per ECMO patient cannot be attributed to popula- tion shifts alone, because there has been a 50% increase in serious patient complications in all diag- nostic groups in the last 3 years, which reached statistical significance for neonates as a group and for MAS/PPHN alone. Because ECMO protocols have not changed significantly for MAS/PPHN patients and because the same team has managed all 455 cases, the increase in the complication rate (with little change in ECMO duration) among the MAS/PPHN group probably reflects a sicker patient population. What cannot be determined is whether the complica- tions are a result of longer ECMO runs or, con- versely, whether longer ECMO runs are a result of increasing complications. In either case, the data suggest that severity of illness among the neonatal population is worsening. There are two possible explanations for this: (1) cohorting of the most severely affected patients who do not respond to
Table 3. ECMO Duration According to Diagnosis and Time
1 2 3 4 ( 1984-1986) ( 1987-1989) ( 1990-1992) ( 1993-1995) P Value
All 129 -+ 14t 160 _+ 7.5t 158 _+ 8.4t 210 _+ 16.6" .0007
CDH 143 ± 14.7t 203 -+ 22.7 165 _+ 17t 228 _+ 23.9* .03
MAS/PPHN 98 _ 31 139 ± 7.2 133 -+ 7.2 151 _+ 16.5 NS
Sepsis - - 157 _+ 13.6 136 _+ 16.5t 196 _+ 30.7* NS
Pediatric - - 242 ± 54.1 289 - 57.1 351 _+ 67.7 NS
Cardiac - - 55 -+ 27.5 155 _+ 25.7 139 _+ 29.7 NS
All neonatal 133 ± 13.7t 157 ± 7.4t 145 ± 7.2t 195 -+ 14.1" .001
*Signi f icant compared wi th t (P < .05).

ECMO IN EVOLUTION 1121
surfactant, HFOV, or NO, and (2) delayed referral of patients because of inadequate predictors of failure of these alternative therapies. It is likely that both play a role.
Finally, the most disturbing finding is the fact that the overall survival rate has decreased significantly in the past 3 years. Again, this decrease can be attributed primarily to a decrease in the number of patients who traditionally had a higher survival rate (MAS/PPHN/ sepsis/RDS) and a relative increase in the number of patients with a historically lower survival rate (CDH, pediatric, cardiac). However, analysis of the diagnos- tic subgroups indicates that changing patient demo- graphics is only part of the story. Between 1987 and 1989, the survival rate for patients with sepsis was 100%. However, in that era the patients with coagu- lopathy were excluded. In 1990, this exclusion was dropped, permitting sicker patients to receive ECMO, and the survival rate decreased (to 74%). However, since 1992, the survival rate has increased (to 86%), probably as a consequence of the use of aggressive exchange transfusion in the patients with coagulopa- thy until the normalization of coagulation factors, followed by AMICAR administration. Among the cardiac patients, recently there has been a slight reduction in the survival rate, which again probably reflects a worsening patient population, as evidenced by the increasing percentage of direct conversions from cardiopulmonary bypass in the operating room to ECMO. The recent decrease in the survival rate among MAS/PPHN patients (from 97% to 87%), although not Statistically significant; also probably reflects a sicker cohort of patients in whom alterna- tive therapies have failed. An additional "hidden mortality" is occurring in the neonatal population, ie, the proliferation of HFOV availability in our commu- nity has led to an increase in the incidence of requests for transport "on ECMO" for infants who have failed HFOV and who are not able to be supported by conventional mechanical ventilation. This has re- sulted in at least six deaths in the past 3 years.
The changes noted above are not unique tO our institution. Recently, Haase et al reported the ECMO experience of Denver Children's Hospital; they noted a dramatic decrease in the number of neonatal referrals for ECMO, from 23 in 1990 to only two in
1993.15 Because the number of neonatal referrals to their institution had not changed significantly, the decrease in ECMO referrals was attributed to the introduction of HFOV and NO. They also noted a significant increase in the mean ECMO duration and in the length of hospitalization for ECMO patients. Data from the Extracorporeal Life Support Organiza- tion have shown a significant decrease in the total number of neonatal ECMO cases. 2 Furthermore, data reported to the Registry by the top 10 ECMO centers by volume show a significant decrease in the number of neonatal patients receiving ECMO at those institutions, as well as an increase in both the mean ECMO duration and in ECMO complications. 2 There was a significant increase in the average age of ECMO patients (from 40 to approximately 60 hours), which suggests a possible delay in ECMO referral. Thus, it appears that a national trend is developing in which the use Of ECMO in neonates is decreasing, apparently in direct response to increasing utilization of alternative therapies such as suffactant, HFOV, and NO, as well as general improvements in perinatal care. Although these techniques are unquestionably successful in avoiding ECMO, long-term studies are needed to assess the associated morbidity. Further- more, the national trend toward less neonatal ECMO appears to be associated with a trend toward sicker ECMO patients who require longer ECMO runs, have more complications, and have a higher mortality rate.
In the near future, pediatric, cardiac, and CDH patients likely will account for the majority of ECMO patients. Because the survival rates for these groups are not significantly improving with experience, bet- ter patient selection criteria are clearly required. Existing ECMO centers must be prepared to adapt to the changing demographics by evolving programs that support pediatric, cardiac, and adult patients in addition to neonates. Furthermore, the increasing incidence of neonatal deaths resulting from patients stranded on HFOV in centers without ECMO capa- bilities, as well as the complexity associated with transporting unstable older patients and the likeli- hood that the number of active ECMO centers will decline, will require continued development of long- distance ECMO transport capabilities.
REFERENCES
1. Bartlett RH, Andrews AF, Toomasian JM, et al: Extracorpo- real membrane oxygenation for newborn respiratory failure: 45 cases. Surgery 92:425-433, 1982
2. ECMO Data Registry. Ann Arbor, MI, University of Michi- gan, 1995
3. O'Rourke PP, Stolar CJH, Zwishenberger JB, et al: Extracor-
poreal membrane oxygenation: Support for overwhelming pulmo- nary failure in the pediatric population. Experience from the Extracorporeal Life Support Organization. J Pediatr Surg 28:523- 529, 1993
4. Carter JM, Gerstmann DR, Clark RH, et al: High frequency oscillatory ventilation and extracorporeal membrane oxygenation
1122 WILSON ET AL
for the treatment Of acute neonatal respiratory failure. Pediatrics 85:159-164, 1990
5. Clark RH, Y0der BA, Sell MS: Prospective randomized comparison Of high-frequency oscillation and conventional ventila- tion in candidates for extracorporeal membrane oxygenation. J Pediatr 124:447-454, 1994
6. Auten RL, Notter RH, Kendig JW, et al: Surfactant treat- ment of full-term newborns with respiratory failure. Pediatrics 87:101-107, 1991
7. Lotze A, Knight GR, Martin GR, et al: Improved pulmonary outcome after exogenous surfactant therapy for respiratory failure in term infants requiring extracOrporeal membrane oxygenation. J Pediatr 122:261-268, 1993
8. Roberts JD, Polaner DM, Lang P; et al: Inhaled nitric oxide in persistent pulmonary hypertension of the newborn. Lancet 340:818-819, 1992
9, Kir~sella JP, Neish SR, Shaffer E, et al: Low dose inhaiational nitric oxide in persistent pulmonary hypertension of the newborn. Lancet 340:819-820, 1992
10. O'Rourke PP, Crone R, Vacanti J, et al: Extracorporeal
membrane oxygenation and conventional medical therapy in neo- nates with persistent pulmonary hypertension of the newborn: A prospective randomized study. Pediatrics 84:957-963, 1989
11. Ortega M, Ramos A, Atkinson J, et al: Oxygenation index can predict outcome in neonates who are candidates for extracor- poreal membrane oxygenation. Pediatr Res 22:462A, 1987 (abstr)
12. Arnold JH, Truog RD, Thompson JE, et al: High-frequency oscillatory ventilation in pediatric respiratory failure. Crit Care Med 21:272, 1993
13. Wilson JM, Bower LK, Fackler JC, et al: Aminocaproic acid decreases the incidence of intracranial hemorrhage and other hemorrhagic complications of ECMO. J Pediatr Surg 28:536-541, 1993
14. Milberg JA, Davis DR, Steinberg KP, et al: Improved survival of patients with acute respiratory distress syndrome (ARDS): 1983-1993. JAMA 273:306, 1995
15. Haase GM, Kennaugh JM, Clarke DR: Adaptation of an ECMO team in the era of successful alternative therapies for neonatal pulmonary failure. J Pediatr Surg 30:674-678, 1995
Discuss ion
K.P. Lally (Houston, TX): Obviously we are all seeing that the neonatal numbers are failing. The implication is that newer therapies such as high- frequency ventilation are a major reason. The percep- tion is that it is a failure to refer patients for ECMO. And somehow implied, but maybe not actually stated, is that we are harming patients by using ECMO.
Do you have any data or at least some feel for the non-ECMO-t rea ted patients? BEcause our HFO- treated patients seem to do well. I mean, if they don't have to go to ECMO, they do seem to do well. So it doesn't appear that we are actually hurting these patients by not putting them on ECMO. However, we are seeing that the HFO failures fail in a hurry. Reese Clark published an article that says if conventional ventilation fails and you move to high frequency, you don't cross over well from high frequency back to conventional ventilation. I would like to know if that is your experience. Are you finding that the oscilla- tion patients, when they do need ECMO, need it quickly?
The corollary to that is that if there are non-ECMO centers that are doing high-frequency oscillation, when those patients fail HFO they may be in serious trouble in terms of getting to an ECMO center.
A.G. Coran (Ann Arbor, MI): That was a beautiful presentation.
I would like tO emphasize the point that Kevin just made. And that is the issue of a number of neonatal centers and community hospitals around the country that have access to high-frequency ventilation but not to ECMO. They treat these babies there, and then
when they crash, you are faced with how to resusci- tate them.
At our institution we have available a transport system that goes out and puts them on ECMO. Now, that is very, very expensive. I wonder whether you know what the incidence of placing patients on ECMO in the periphery has been in all the ECMO centers around the country.
B.W. Warner (Cincinnati, OH): I think this is a nice report. With all these new modalities, what has been your experience with nitric oxide before going on ECMO. We have seen a large number of children now meeting criteria for a longer period of time than we would normally accept to allow these other newer modalities to be tried. DO you think that is why some of these patients are perhaps sicker when they are placed on ECMO and might account for your in- creased morbidity or lower survival now?
P.C. Guzzetta (Dallas, TX): Again, Jay, a beautiful report. I think part of the frustration for those of us who treat a fair number of pediatric and cardiac patients is that some of the enthusiasm and the excitement about ECMO has been significantly damp- ened because the survival rate is worse. Can you elucidate a bit on a way we can pick the patients who are not going to be helped with this modality. You have a 40% mortality rate in your late group. Is there some way we c a n deny those patients who aren' t going to be helped and maybe get the enthusiasm back?
J.M. Wilson (response): With regard to the pediatric and cardiac patients and the poor survival, the prob- lem is that we don't have predictors. A very well

ECMO IN EVOLUTION 1123
organized attempt at a randomized prospective trial with five institutions to look at predictors of failure with pediatric ECMO has just fallen on its nose because of lack of patient recruitment. So I am doubtful that there is ever going to be a reasonable prospective randomized trial in the pediatric and cardiac patients. Consequently, ! think we are all going to end up doing the same thing, using "failure to respond," which means different things to different people.
With regard to nitric oxide, a lot of cardiac patients with postoperative pulmonary hypertension have re- sponded very well, but our experience with CDH patients has been abysmal. We have not saved a single diaphragmatic hernia case with nitric oxide.
With regard to Kevin's question about delayed institution of ECMO despite failure of alternate therapies, that is a big problem. At our institution in the past year and a half, there have been at least six deaths in the surrounding community of patients who have been stranded on high-frequency ventilation with no ability to transport to us.
Consequently, we also began considering the con-
cept of mobile ECMO in order to salvage these patients. The problem, as Dr Coran pointed out, is that it is very expensive and it only continues to encourage people in the community to keep patients. My concern is, if we open a mobile ECMO program designed to transport a half dozen people a year, then we are going to end up transporting all the patients.
My personal bias is that new therapies shouldn't be evaluated in the surrounding community without ECMO backup on site.
Regarding the question of whether we are hurting patients by trying these alternate therapies, I think the answer is yes and no. There is no question at our institution that we are salvaging about 60% to 70% of the patients with the alternate therapies, and so to say that this is no good obviously is wrong. On the other hand, it is becoming increasingly necessary for us to cannulate patients while we are doing CPR in straight- forward meconium aspiration cases.
What our data show is that these patients are being pumped longer and they are having more complica- tions. I think that's attributable, at least in part, to the pre-ECMO treatment that they get.








![TCS - ECMO - [Bow]€¦ · The Paris International Congress on ECMO will therefore become the TCS-ECMO ... Ethics: end of life and ECMO FRIDAY 1 ... TCS for the right ventricle M](https://img.pdfslide.net/doc/110x75/5aef5ebd7f8b9a8b4c8c350f/tcs-ecmo-bow-the-paris-international-congress-on-ecmo-will-therefore-become.jpg)




















