Embed Size (px)
Citation preview

Psychopharmacology (1998) 139 : 261�268 © Springer-Verlag 1998
ORIGINAL INVESTIGATION
A.C. Parrott · J. Lasky
Ecstasy (MDMA) effects upon mood and cognition :before, during and after a Saturday night dance
Received: 3 November 1997/Final version: 27 February 1998
Abstract Three groups of young people (aged 19�30years) were compared: 15 regular ecstasy users whohad taken MDMA (3,4-methylenedioxymethampheta-mine) on ten or more occasions; 15 novice ecstasy userswho had taken MDMA on fewer than ten previousoccasions; and 15 controls who had never takenMDMA. Each subject completed a cognitive test andmood scale battery four times: an initial drug-free base-line, at a Saturday night dance/club (on-drug), then 2days later, and 7 days later. On the Saturday night, reg-ular ecstasy users took an average of 1.80 MDMAtablets, novice users took 1.45 MDMA tablets, whilecontrols mostly drank alcohol. The consumption ofcannabis and cocaine at the club was similar acrossgroups. All three groups reported positive moods at thedance club (on-drug), although there were borderlinetrends (P < 0.10) for less sadness /depression in theMDMA subgroups. However 2 days afterwards, theecstasy users felt signiÞcantly more depressed, abnor-mal, unsociable, unpleasant, and less good tempered,than the controls. Cognitive performance on both tasks(verbal recall, visual scanning) was signiÞcantlyreduced on-MDMA. Memory recall was alsosigniÞcantly impaired in drug-free MDMA users, withregular ecstasy users displaying the worst memoryscores at every test session. This agrees with previousÞndings of memory impairments in drug-free ecstasyusers. Animal data have shown that MDMA can gen-erate long-term serotonergic neurodegereration in var-ious brain areas, including the hippocampus. Thecognitive deÞcits in drug-free recreational ecstasy users,suggest that MDMA may also be neurotoxic inhumans.
Key words MDMA · 3,4 ethylenedioxymethampheta-mine · Ecstasy · Serotonin · Memory · Cognition ·Mood · Neurotoxicity
Introduction
The synthetic amphetamine derivative MDMA (3,4-methylenedioxymethamphetamine), or �ecstasy�, Þrstbecame popular in the mid-1980s at acid house partiesand raves. Today, it is readily available as an illicit drugat many clubs and recreational venues. It has been esti-mated that half-a-million ecstasy tablets are taken eachweekend in the UK (Saunders 1995), with 13% ofBritish university students reporting they had used it(Webb et al. 1996). It is also widely consumed in otherwesternised countries (Peroutka et al. 1988; Solowij et al. 1992; Cuomo et al. 1994; Saunders 1995; Lentonet al. 1997). Because of its illegal status, it is not pos-sible to study its e¤ects upon human behaviour usingthe traditional double-blind placebo-controlledmethodology [Downing (1986) was undertaken beforeMDMA was scheduled in the USA]. Most informa-tion on the psychobiological e¤ects of MDMA there-fore comes from the following sources. Firstly, studiesof recreational drug users, who are asked to describetheir experiences on MDMA (Peroutka et al. 1988;Solowij et al. 1992; Curran and Travill 1997; Davisonand Parrott 1997; Parrott and Stuart 1997). Secondly,medical case studies, following drug-induced hyper-thermia, hyponatraemia convulsions, and psychiatricor neurological disorders (Dowling et al. 1987; Schmidt1987; Henry et al. 1992; Lee 1994; Maxwell et al. 1994;Series et al. 1994; Squier et al. 1995; McCann et al.1996; Spatt et al. 1997). Thirdly animal data, whereMDMA is administered under controlled conditionsin the laboratory; these studies have provided extensiveinformation on the neurochemical and neurotoxice¤ects of MDMA in rats and monkeys (Ricaurte et al.
A.C. Parrott (*) · J. LaskyDepartment of Psychology, University of East London,London E15 4LZ, UKe-mail : [email protected], Fax: +44-181-849-3697

1988, 1992; Steele et al. 1994; Green et al. 1995;Frederick and Paule 1997).
Recreational durg users typically describe a range ofpositive moods on-MDMA: elation, energeticness,agreeableness, and closeness to others (Peroutka et al.1988; Liester et al. 1992; Solowij et al. 1992; Davisonand Parrott 1997; Parrott 1995, 1997; Parrott andStuart 1997). However, negative moods generallydevelop during the period of neurochemical depletionafterwards, when feelings of lethargy, irritability, anddepression predominate. This cycle of positive moodson-drug, and negative moods afterwards, wasconÞrmed in a prospective study by Curran and Travill(1997). Twelve recreational ecstasy users were com-pared with 12 alcohol drinkers (controls), at a Saturdaynight dance/club, then 1 and 4 days later. The ANOVAgroup by time interaction was signiÞcant for mostmood scales, with MDMA users reporting compara-tively better moods on the Saturday night, and worsemoods in the days afterwards (Table 2 in Curran andTravill 1997). Unfortunately, the data from each periodwere not separately analysed; thus it is unclear whethermoods were signiÞcantly better while on MDMA, orsigniÞcantly worse afterwards.
Several studies have found that drug-free recreationalecstasy users display signiÞcant memory impairments,whereas their performance on other cognitive tests isgenerally normal (Krystal et al. 1992; Spatt et al. 1997;Morgan 1998; Parrott 1998; Parrott et al. 1998).Animal studies have shown that MDMA can lead toserotonergic (5-HT) neurodegeneration, in the hip-pocampus and other brain areas (Ricaurte et al. 1988,1992; Steele et al. 1994; Green et al. 1995). This sug-gests that the memory decrements in humans mayreßect serotonergic neurodegeneration (Parrott andStuart 1997; Parrott et al. 1998; Spatt et al. 1997; Szaboet al. 1997; Morgan 1998). The current study wasdesigned to provide further data on the cognitive skillsand mood states of recreational ecstasy users. The Þrstaim was to assess the acute e¤ects of MDMA self-administration upon mood and cognition. Previously,this has only been reported by Curran and Travil(1997), but they did not have a pre-drug baseline. Thesecond aim was to monitor the time course of themood/cognitive changes, during the neurochemicalrecovery period afterwards. Finally, the study investi-gated whether drug-free ecstasy users would againdemonstrate a cognitive proÞle of selective memoryimpairments.
Materials and methods
Subjects
Forty-Þve unpaid subjects were obtained using the �snowball� tech-nique, developed for illicit drug research (Solowij et al. 1992; Parrottand Stuart 1997). Word of the study was spread amongst friends
and acquaintances who regularly visited a large nightclub in theEpping Forest area of north-east London. Three subgroups weretested: 15 regular ecstasy users who stated that they had takenMDMA (3,4-methylenedioxymethamphetamine) on ten or moreprevious occasions; 15 novice ecstasy users who had taken MDMAon one to nine previous occasions; and 15 controls who stated thatthey had never taken MDMA. The ages of each group were simi-lar (21.4, 22.8, 21.3 years, respectively; overall range 19�30 years);as was their gender distribution (8 /7, 8 /7 and 10/5 : females /malesper group, respectively). Drug use at the dance/club was recordedon a self-rating questionnaire, where each user noted the drugs theyhad taken that night. The regular ecstasy users took slightly moreMDMA than the novice users (1.80 compared to 1.45 MDMAtablets), while none of the control group took any MDMA. Threeother illicit drugs were taken: cannabis, cocaine, and amphetamine.Cannabis was smoked by: three non-user controls, one noviceMDMA user, and two regular MDMA users. Cocaine was takenby: two controls, two novice MDMA users, and four regularMDMA users. One novice MDMA user took amphetamine.Alcohol was taken by ten controls, Þve novice MDMA users, andsix regular MDMA users. The number of alcoholic drinks con-sumed by each drinker was somewhat higher in the controls : 5.0drinks per control group drinker, 2.7 drinks per novice MDMAgroup drinker, 3.7 drinks per regular MDMA group drinker.
Assessment measures
These comprised auditory word recall, visual search, and a moodscale battery. Auditory recall involved lists of 16 words, presentedat one word every 2 s, over headphones from a portable taperecorder. The subject listened to the word list, waited 30 s, and wheninstructed by the experimenter, wrote down all the words they couldremember in any order. Each word list was matched for frequencyof everyday occurrence and overall word length. Two word listswere given at each test session. Eight word lists were varied acrosssessions. This �supraspan� word recall task has been shown to besensitive to the amnesic e¤ects of scopolamine (Parrott 1986).
The visual search task was presented on a hand-held minicom-puter (Apple Newton Messagepad; Tiplady 1996). A target letter�L� was embedded in an array of distractor letters in di¤erent ori-entations. The subject was required to press the target letter witha light pen as rapidly as possible. In the easy discrimination con-dition, the distractor letters were all �X�s. In the hard discrimina-tion condition, the distractor letters were �T�s. Four sizes of matrixarray were presented: 2 × 2, 3 × 3, 4 × 4, and 5 × 5. Only the 2 × 2and 4 × 4 data were analysed/presented here, since we were onlyinterested in visual scanning at two levels of di¦culty. This taskhas been shown to be sensitive to the disruptive e¤ects of alcohol(Newman et al. 1996; Tiplady 1996).
Visual analogue mood scales were presented on the NewtonMessagepad (Newman et al. 1996; Tiplady 1996). For each unipo-lar mood state, one end of the linear scale was marked �Do notfeel at all� (0), while the other end was marked �Feel completely�(100). The subject indicated their current mood state by markingthe line with a light pen (initial responses could be amended). Sixteenmood states were covered; they are listed in Table 2.
Procedures and ethics
The baseline data were collected either at the subject�s home, or thehome of the experimenter. Each subject arranged a time for thisinitial baseline test when they were drug free, had not taken MDMAfor at least 1 week, or any other illicit drug for over 24 h. The base-line session preceded when the subjects stated they were going club-bing, and when the MDMA users were planning to take ecstasy.The second test session was undertaken at the dance club venue.This was noisy and crowded, but a comparatively quiet area was
262
arranged for testing. Each subject arranged to meet the experimenter2�8 h after they had taken their MDMA tablets, or equivalent timesfor control subjects.
Unfortunately, not every subject was seen as planned, and eightof the 30 MDMA subjects (four from each group), were tested 8�16hours after taking their MDMA. The third and fourth test sessionswere undertaken 2 days and 7 days later, at venues similar to theÞrst session.
The aims and objectives of the study were fully described to eachindividual beforehand. It was emphasised that neither the experi-menters nor the University condoned the taking of illicit drugs suchas MDMA. Thus the study should not be seen as providing approvalor encouragement for the use of ecstasy or other illegal drugs, par-ticularly since they could have serious side e¤ects. It was stated thattaking part in the study was voluntary, that they could withdrawat any time without giving a reason, that the data would be treatedas strictly conÞdential, and that subject names would not bedivulged outside the study. Those who agreed to take part wererequired to sign an informed consent form. The study was approvedby the University Ethics Committee.
Results
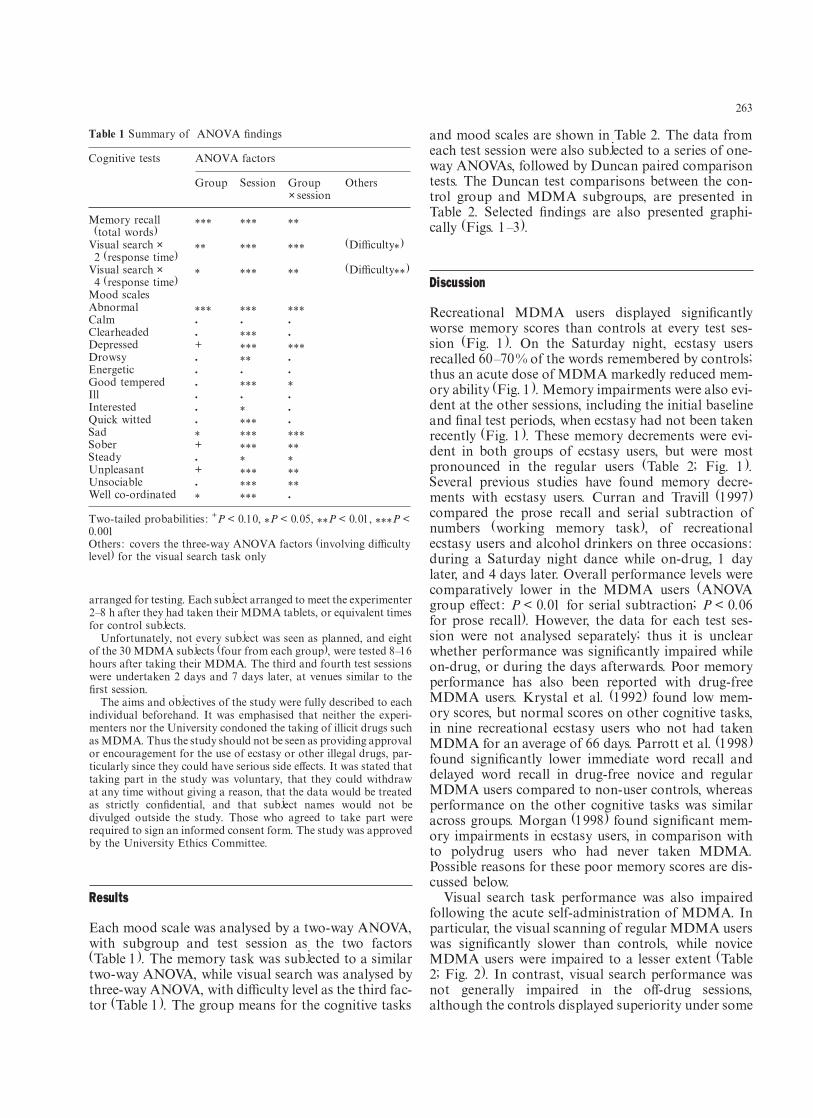
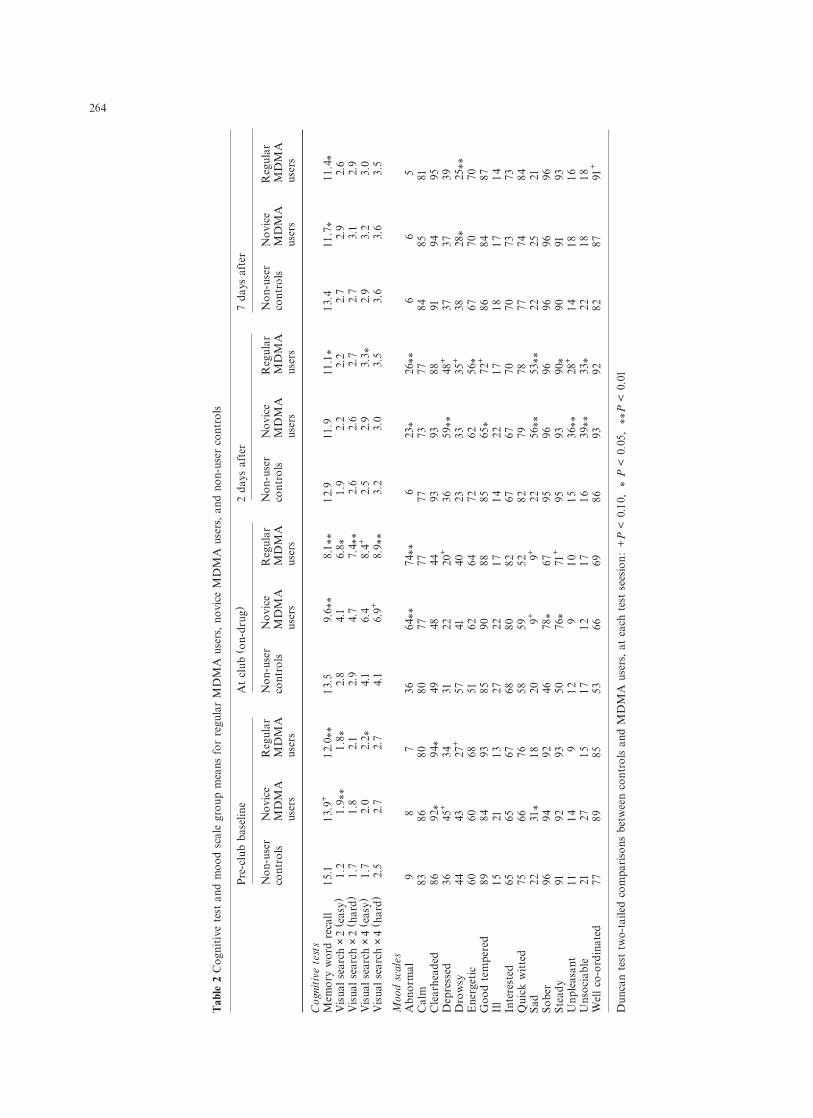
Each mood scale was analysed by a two-way ANOVA,with subgroup and test session as the two factors (Table 1). The memory task was subjected to a similartwo-way ANOVA, while visual search was analysed bythree-way ANOVA, with di¦culty level as the third fac-tor (Table 1). The group means for the cognitive tasks
and mood scales are shown in Table 2. The data fromeach test session were also subjected to a series of one-way ANOVAs, followed by Duncan paired comparisontests. The Duncan test comparisons between the con-trol group and MDMA subgroups, are presented inTable 2. Selected Þndings are also presented graphi-cally (Figs. 1�3).
Discussion
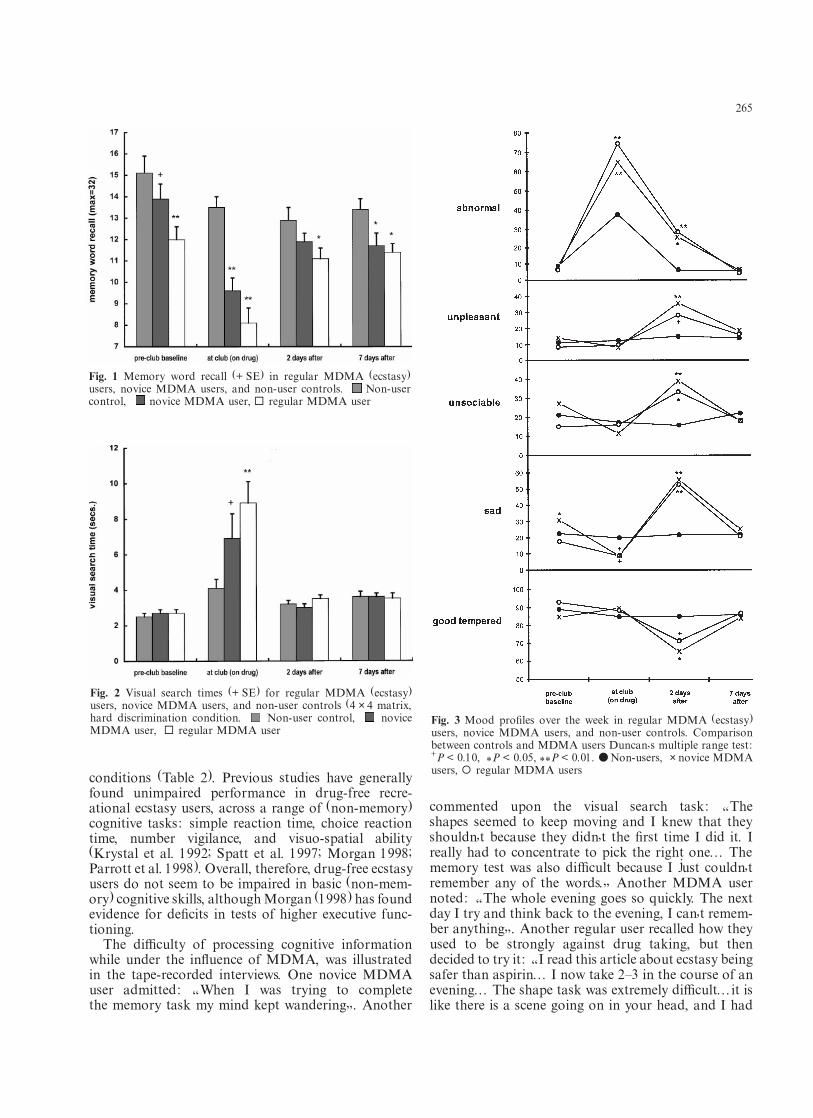
Recreational MDMA users displayed signiÞcantlyworse memory scores than controls at every test ses-sion (Fig. 1). On the Saturday night, ecstasy usersrecalled 60�70% of the words remembered by controls;thus an acute dose of MDMA markedly reduced mem-ory ability (Fig. 1). Memory impairments were also evi-dent at the other sessions, including the initial baselineand Þnal test periods, when ecstasy had not been takenrecently (Fig. 1). These memory decrements were evi-dent in both groups of ecstasy users, but were mostpronounced in the regular users (Table 2; Fig. 1).Several previous studies have found memory decre-ments with ecstasy users. Curran and Travill (1997)compared the prose recall and serial subtraction ofnumbers (working memory task), of recreationalecstasy users and alcohol drinkers on three occasions:during a Saturday night dance while on-drug, 1 daylater, and 4 days later. Overall performance levels werecomparatively lower in the MDMA users (ANOVAgroup e¤ect : P < 0.01 for serial subtraction; P < 0.06for prose recall). However, the data for each test ses-sion were not analysed separately; thus it is unclearwhether performance was signiÞcantly impaired whileon-drug, or during the days afterwards. Poor memoryperformance has also been reported with drug-freeMDMA users. Krystal et al. (1992) found low mem-ory scores, but normal scores on other cognitive tasks,in nine recreational ecstasy users who not had takenMDMA for an average of 66 days. Parrott et al. (1998)found signiÞcantly lower immediate word recall anddelayed word recall in drug-free novice and regularMDMA users compared to non-user controls, whereasperformance on the other cognitive tasks was similaracross groups. Morgan (1998) found signiÞcant mem-ory impairments in ecstasy users, in comparison withto polydrug users who had never taken MDMA.Possible reasons for these poor memory scores are dis-cussed below.
Visual search task performance was also impairedfollowing the acute self-administration of MDMA. Inparticular, the visual scanning of regular MDMA userswas signiÞcantly slower than controls, while noviceMDMA users were impaired to a lesser extent (Table2; Fig. 2). In contrast, visual search performance wasnot generally impaired in the o¤-drug sessions,although the controls displayed superiority under some
263
Table 1 Summary of ANOVA Þndings
Cognitive tests ANOVA factors
Group Session Group Others× session
Memory recall *** *** **(total words)
Visual search × ** *** *** (Di¦culty*)2 (response time)
Visual search × * *** ** (Di¦culty**)4 (response time)
Mood scalesAbnormal *** *** ***Calm � � �
Clearheaded � *** �
Depressed + *** ***Drowsy � ** �
Energetic � � �
Good tempered � *** *Ill � � �
Interested � * �
Quick witted � *** �
Sad * *** ***Sober + *** **Steady � * *Unpleasant + *** **Unsociable � *** **Well co-ordinated * *** �
Two-tailed probabilities : +P < 0.10, *P < 0.05, **P < 0.01, ***P <0.001Others : covers the three-way ANOVA factors (involving di¦cultylevel) for the visual search task only
264
Tab
le 2
Cog
niti
ve t
est
and
moo
d sc
ale
grou
p m
eans
for
reg
ular
MD
MA
use
rs,
novi
ce M
DM
A u
sers
, an
d no
n-us
er c
ontr
ols
Pre
-clu
b ba
selin
eA
t cl
ub (
on-d
rug)
2 da
ys a
fter
7 da
ys a
fter
Non
-use
rN
ovic
eR
egul
arN
on-u
ser
Nov
ice
Reg
ular
Non
-use
rN
ovic
eR
egul
arN
on-u
ser
Nov
ice
Reg
ular
cont
rols
MD
MA
MD
MA
cont
rols
MD
MA
MD
MA
cont
rols
MD
MA
MD
MA
cont
rols
MD
MA
MD
MA
user
sus
ers
user
sus
ers
user
sus
ers
user
sus
ers
Cog
niti
ve t
ests
Mem
ory
wor
d re
call
15.1
13.9
+12
.0**
13.5
9.6*
*8.
1**
12.9
11.9
11.1
*13
.411
.7*
11.4
*V
isua
l se
arch
×2
(eas
y)1.
21.
9**
1.8*
2.8
4.1
6.8*
1.9
2.2
2.2
2.7
2.9
2.6
Vis
ual
sear
ch×
2 (h
ard)
1.7
1.8
2.1
2.9
4.7
7.4*
*2.
62.
62.
72.
73.
12.
9V
isua
l se
arch
×4
(eas
y)1.
72.
02.
2*4.
16.
48.
4+2.
52.
93.
3*2.
93.
23.
0V
isua
l se
arch
×4
(har
d)
2
.52.
72.
74.
16.
9+8.
9**
3.2
3.0
3.5
3.6
3.6
3.5
Moo
d sc
ales
Abn
orm
al
98
736
64**
74**
6
23*
26**
66
5C
alm
8386
8080
7777
7773
7784
8581
Cle
arhe
aded
8692
*94
*49
4844
9393
8891
9495
Dep
ress
ed36
45+
3431
2220
+36
59**
48+
3737
39D
row
sy
4443
27+
5741
4023
3335
+38
28*
25**
Ene
rget
ic60
6068
5162
6472
6256
*67
7070
Goo
d te
mpe
red
8984
9385
9088
8565
*72
+86
8487
Ill
1521
1327
2217
1422
1718
1714
Inte
rest
ed
6565
6768
80
8267
6770
7073
73Q
uick
wit
ted
7566
7658
5952
8279
7877
7484
Sad
2231
*18
209+
9+22
56**
53**
2225
21So
ber
9694
9246
78*
6795
9696
9696
96St
eady
9192
9350
76*
71+
9593
90*
9091
93U
nple
asan
t11
149
129
1015
36**
28+
1418
16U
nsoc
iabl
e21
27
1517
1217
1639
**33
*22
1818
Wel
l co
-ord
inat
ed77
8985
5366
6986
9392
8287
91+
Dun
can
test
tw
o-ta
iled
com
pari
sons
bet
wee
n co
ntro
ls a
nd M
DM
A u
sers
, at
eac
h te
st s
eesi
on:
+P
< 0
.10,
*
P <
0.0
5,
**P
< 0
.01
conditions (Table 2). Previous studies have generallyfound unimpaired performance in drug-free recre-ational ecstasy users, across a range of (non-memory)cognitive tasks : simple reaction time, choice reactiontime, number vigilance, and visuo-spatial ability(Krystal et al. 1992; Spatt et al. 1997; Morgan 1998;Parrott et al. 1998). Overall, therefore, drug-free ecstasyusers do not seem to be impaired in basic (non-mem-ory) cognitive skills, although Morgan (1998) has foundevidence for deÞcits in tests of higher executive func-tioning.
The di¦culty of processing cognitive informationwhile under the inßuence of MDMA, was illustratedin the tape-recorded interviews. One novice MDMAuser admitted: �When I was trying to completethe memory task my mind kept wandering�. Another
commented upon the visual search task: �The shapes seemed to keep moving and I knew that theyshouldn�t because they didn�t the Þrst time I did it. Ireally had to concentrate to pick the right one� Thememory test was also di¦cult because I just couldn�tremember any of the words.� Another MDMA usernoted: �The whole evening goes so quickly. The nextday I try and think back to the evening, I can�t remem-ber anything�. Another regular user recalled how theyused to be strongly against drug taking, but thendecided to try it : �I read this article about ecstasy beingsafer than aspirin� I now take 2�3 in the course of anevening� The shape task was extremely di¦cult�it islike there is a scene going on in your head, and I had
265
Fig. 1 Memory word recall (+ SE) in regular MDMA (ecstasy)users, novice MDMA users, and non-user controls. Non-usercontrol, novice MDMA user, ¨ regular MDMA user
Fig. 2 Visual search times (+ SE) for regular MDMA (ecstasy)users, novice MDMA users, and non-user controls (4 × 4 matrix,hard discrimination condition. Non-user control, noviceMDMA user, ¨ regular MDMA user
Fig. 3 Mood proÞles over the week in regular MDMA (ecstasy)users, novice MDMA users, and non-user controls. Comparisonbetween controls and MDMA users Duncan�s multiple range test :+P < 0.10, *P < 0.05, **P < 0.01. ● Non-users, × novice MDMAusers, ¡ regular MDMA users

to keep reminding myself to stop watching and keepon with your experiment�there was the same problemwith the memory test�. Yet another regular MDMAuser admitted Þnding the memory task di¦cult, butcommented: �I have got a bad memory anyway�.
There are several possible explanations for the poormemories of drug-free ecstasy users. It may be due tochance, but this is unlikely given the number of stud-ies where memory deÞcits have now been shown(Krystal et al. 1992; Spatt et al. 1997; Morgan 1998;Parrott et al. 1998). Alternatively, it may reßect subjectself-selection, with only people having poor memoriesdeciding to take MDMA. However, this post-hocexplanation lacks a clear rationale, particularly giventhe near-normal scores of ecstasy users on other cog-nitive tasks (i.e. they are not cognitively impaired). Athird possibility is that the memory problems arecaused by other illicit drugs, particularly cannabis.Although this explanation is initially plausible, theempirical evidence is against it. Every subject in thestudy of Curran and Travill (1997) was a cannabis user,yet the controls still displayed better cognitive perfor-mance than the ecstasy users. The three groups in thecurrent study took similar amounts of other illicit drugsat the club, yet their memory scores were quite di¤erent(Table 1). Morgan (1998) attempted to match theirMDMA users and polydrug user controls, on the pastuse of other illicit drugs, but still found relative mem-ory impairments in the MDMA group. Thus the mem-ory deÞcits in ecstasy users do not seem to be anartefact of other drug use, although this issue remainscurrently unresolved [the long-term cognitive e¤ects ofall illicit psychoactive drugs (e.g. cannabis, LSD,cocaine) need to be properly studied, but this is di¦cultbecause of their illegal status]. The Þnal explanation isthat the memory deÞcits (Fig. 1) are directly caused byMDMA.
Laboratory studies with rats and monkeys haveshown that MDMA produces serotonergic neurode-generation; this has been demonstrated in various brainareas including the hippocampus, which is importantfor memory functioning (Ricaurte et al. 1988, 1992;Steele et al. 1994; Green et al. 1995). Serotonergic neu-rotoxicity following MDMA administration has beenshown in numerous studies; moreover, the neural dam-age seems to be long-lasting: �In nonhuman primatesMDMA-induced serotonin neurotoxicity is prolongedand possibly permanent�. The dose of MDMA thatdamages serotonin neurones in monkeys is close to thattypically taken by recreational users, and smaller thanthat taken by some MDMA abusers in the setting ofraves� (McCann et al. 1996, p. 112). There is also clin-ical evidence for brain damage in humans. Spatt et al.(1997) described a recreational MDMA user who pre-sented with anterograde amnesia and marked impair-ments in episodic memory, but normal performance onother neuropsychological tests. An MRI brain scanrevealed bilateral lesions in the serotonin-rich globus
pallidus, similar to that reported in an earlierMDMA/polydrug fatality (Squier et al. 1995). PETscans of recreational ecstasy users have also demon-strated reduced levels of 5-HT transporter binding, invarious brain regions (Szabo et al. 1997). There is there-fore consistent evidence that these memory deÞcits mayreßect serotonergic neurodegeneration, directly causedby MDMA self-administration (Fig. 1). This raises thequestion: how much ecstasy needs to be taken beforecognitive deÞcits develop? Our regular users were com-paratively more impaired than the novice users, pro-viding some support for the (arbitrary) split betweenthose who have taken ecstasy on less than, or morethan, ten occasions. However, the relationship betweencognitive performance and MDMA consumption(both frequency and intensity), need to be investigatedmore fully.
Turning to the mood state data, all three groupsreported surprisingly similar moods on the Saturdaynight. Thus each subgroup reported high ratings forfeeling �good tempered� at the nightclub (Fig. 3).Ecstasy users did report a borderline trend for lowersadness and less depression than controls (P < 0.10;Fig. 3), together with greater abnormality (Table 2). Incontrast, the controls were signiÞcantly less sober andless steady, probably because of their alcohol con-sumption (Table 2). In retrospective surveys, ecstasyusers typically describe feelings of euphoria, elation,and greater acceptance of others (Peroutka et al. 1988;Liester et al. 1992; Solowij et al. 1992; Davison andParrott 1997; Parrott 1995; Parrott and Stuart 1997),probably due to an acute boost of serotonin activity(Steele et al. 1994; Green et al. 1995). The absence ofsuperior moods in our ecstasy users was therefore unex-pected (Table 2; Fig. 3). Various factors may, however,have contributed to this. Firstly, previous studies havegenerally not included non-user controls (exceptCurran and Travill 1997), and most dancers /clubberswould be expected to experience good feelings on theirSaturday night out. Secondly, our controls had takena range of other psychoactive drugs which may havecontributed to their positive moods (Table 2; Fig. 3).Future studies should include a drug-free group,although the majority of clubbers do seem to take psy-choactive drugs [Lenton et al. (1997) found that only8% of clubbers had not consumed any psychoactivesubstance]. A related problem was ceiling/ßoor e¤ects.Thus ��good tempered�� ratings were already high in thecontrol group, making it di¦cult to generate signiÞcantmood superiority in the other groups.
Two days afterwards, the ecstasy users reported arange of deleterious moods: depression, sadness, unso-ciability, unpleasantliness, and abnormality (Table 2;Fig. 3). Negative moods tend to develop during theperiod of serotonin depletion which follows an ecstasytrip. Thus lethargy, depression, moodiness, and irri-tability, are often reported in the days post-MDMA(Peroutka et al. 1988; Solowij et al. 1992; Davison and
266

Parrott 1997). In their prospective study, Curran andTravill (1997) found a range of positive moods in activeecstasy users, but mid-week blues afterwards. It is there-fore clear that MDMA can lead to marked moodswings. Feelings of depression, sadness, calmness, pleas-antliness and sociability, ßuctuated markedly over theweek in our ecstasy users, whereas these moods werefairly stable over time in the controls (Fig. 3). Curranand Travill (1997) found that some of their ecstasy usersdeveloped clinically borderline levels of midweekdepression. This was conÞrmed in the interviews here,where depression was recognised as an occupationalhazard of regular ecstasy use: ��My other friends thatdo a lot more drugs than me are sometimes reallymoody, and some cry quite often for no reason��... ��IdeÞnitely do get depressed sometimes��... ��I had theoccasional mid-week depression, and occasionallyfound myself crying for no real reason��.
Although this study was not designed to monitor themedical or physiological e¤ects of MDMA, several ofthe interviews conÞrmed its dangerous side-e¤ects (e.g.hyperthermia, hyponatraemia, convulsions, catatonicstupor, vomiting, motor tics: Dowling et al. 1987;Schmidt 1987; Henry et al. 1992; Maxwell et al. 1993;Lee 1994; McCann et al. 1996). One regular MDMAuser admitted to vomiting after each period of drugtaking; another to paranoid feelings; a third to repet-itive tingles and spontaneous arm movements: ��Halfthe time I do even realise I am moving my arm, untilmy friend tells me stop...may be there is some perma-nent damage or something��. Two severe medical emer-gencies were also described: ��My boyfriend had a reallybad time...he was getting more and more worked upand really sweating badly. His face looked mad and hiseyes were practically poping out of his head. In the endthey had to take him to hospital...He wasn�t right fordays afterwards and now won�t touch pills. I still dothem occasionally, but never more than two��. Anotherregular user recalled: ��On holiday... I took two at onceand after about 45 minutes I couldn�t move a singlemuscle and basically just collapsed on the dance ßoor.My mates took me back to the hotel, and I was sickall night long, and kept having really bad hallucina-tions. My mates were more scared than me because thenext day I couldn�t remember a lot at all. I felt terri-ble for a couple of days, but after that I was Þne. Ithasn�t put me o¤ taking them��.
In summary, the current study was the Þrst to inves-tigate the acute e¤ects MDMA self-administrationupon mood and cognitive performance, in comparisonwith pre-drug baseline. As expected, the recreationalecstasy users reported very good feelings on-MDMA;however, the other clubbers/dancers also reported goodmoods, even though they had not taken any ecstasy.The good moods of all the Saturday night clubbers,illustrate the importance of context and expectacy forgenerating positive feelings. It might be argued that ourquestionnaire was insensitive to the unique mood ele-
vating properties of ecstasy; thus questions on ��ela-tion�� or ��empathy�� might have generated signiÞcantgroup di¤erences. However, the current mood scaleswere certainly sensitive to the negative feelings whichdeveloped in the days afterwards, during serotonergicdepletion. Thus our MDMA users reported consider-able mood swings during the week they had usedecstasy (Fig. 3). The cognitive test Þndings indicatedthat the acute self-administration of MDMA markedlyimpaired information processing ability (Figs. 1, 2), andemphasised the dangers of undertaking skilled activi-ties like car driving under its inßuence (Schifano 1995).However, the most worrying Þnding was the poor mem-ory scores of the drug-free ecstasy users, particularlythose who had taken MDMA on more than ten occa-sions (Fig. 1). When combined with the animal dataon serotonergic neurotoxicity (Ricaurte et al. 1992;Green et al. 1995; Frederick and Paule 1997), they sug-gest that serotonergic nerve damage may also be occur-ring in humans (Spatt et al. 1997; Szabo et al. 1997).This is obviously very worrying, given the widespreaduse of MDMA.
Acknowledgements The authors would like to thank Dr. BrianTiplady (Astra Pharmaceuticals), for the loan of his AppleMessagepad cognitive test system, also John Turner for valuablecomments and suggestions.
References
Cuomo MJ, Dyment PG, Gammino VM (1994) Increasing use ofEcstasy (MDMA) and other hallucinogens on a college cam-pus. J Am Coll Health 42:271�274
Curran HV, Travill RA (1997) Mood and cognitive e¤ects of 3,4-methylenedioxymethamphetamine (MDMA, ��ecstasy��) : week-end ��high�� followed by mid-week ��low��. Addiction 92:821�831
Davison D, Parrott AC (1997) Ecstasy (MDMA) in recreationalusers : self-reported psychological and physiological e¤ects.Hum Psychopharmacol 12:221�226
Dowling GP, McDonough ET, Bost RO (1987) ��Eve�� and��Ecstasy�� � a report of Þve deaths associated with the use ofMDEA and MDMA. JAMA 257:1615�1617
Downing J (1986) The psychological and physiological e¤ects ofMDMA on normal volunteers. J Psychoact Drugs 18:335�340
Frederick DL, Paule MG (1997) E¤ects of MDMA on complexbrain function in laboratory animals. Neurosci Biobehav Rev21:67�78
Green AR, Cross AJ, Goodwin GM (1995) Review of the pharmacology and clinical pharmacology of 3,4-methylene-dioxymethamphetamine (MDMA or ��ecstasy��). Psycho-pharmacology 119:247�260
Henry JA, Je¤reys KJ, Dawling S (1992) Toxicity and deaths from3,4-methylenedioxymethamphetamine (��ecstasy��). Lancet 340:384�387
Krystal JH, Price LH, Opsahl C, Ricaurte GA, Heninger GR (1992)Chronic 3,4-methylenedioxymethamphetamine (MDMA) use :e¤ects on mood and neuropsychological function? Am J DrAlcohol Abuse 18:331�341
Lee JWY (1994) Catatonic stupor after ��ecstasy��. BMJ 310:372�374
Lenton S, Boys A, Norcross K (1997) Raves, drugs and experience:drug use by a sample of people who attend raves in WesternAustralia. Addiction 92:1327�1337
267

Liester MB, Grob CS, Bravo GL, Walsh RN (1992) Phenomenologyand sequelae of 3,4-methylenedioxymethamphetamine use. JNerv Ment Dis 180:345�352
Maxwell DL, Polkey MI, Henry JA (1994) Hyponatraemia andcatatonic stupor after taking ��ecstasy��. BMJ 307: 1399
McCann UD, Slate SO, Ricaurte GA (1996) Adverse reactions with3,4-methylenedioxymethamphetamine (MDMA; Ecstasy).Drug Safety 15:107�115
Morgan M (1998) Lasting psychological sequelae of recreationaluse of MDMA (��ecstasy��): controlled studies in humans. JPsychopharmacol 12:101�102
Newman D, Speake DJ, Armstrong PJ, Tiplady B (1996) E¤ects ofethanol on control of attention. Hum Psychopharmacol12:235�241
Parrott AC (1986) The e¤ects of transdermal scopolamine and fourdoses of oral scopolamine (0.15, 0.3, 0.6, 1.2 mg) upon psy-chological performance. Psychopharmacology 89:347�354
Parrott AC (1995) Psychoactive drugs of use and abuse : wobble,rave, inhale, or crave? J Psychopharmacol 9 :390�391
Parrott AC (1997) MDMA, mood and memory: the agnosia of theecstasy. Br Psycho Soc Proc 5 :49
Parrott AC (1998) The psychobiology of MDMA or ��ecstasy�� :symposium report. J Psychopharmacol 12:97�102
Parrott AC, Stuart M (1997) Ecstasy (MDMA), amphetamine andLSD: comparative mood proÞles in recreational polydrug users.Hum Psychopharmacol 12:501�504
Parrott AC, Lees A, Garnham NJ, Jones M, Wesnes K (1998)Cognitive performance in recreational users of MDMA or��ecstasy��: evidence for memory deÞcits. J Psychopharmacol12:79�83
Peroutka SJ, Newman H, Harris H (1988) Subjective e¤ects of 3,4-methylenedioxymethamphetamine in recreational users.Neuropsychopharmacology 1 :273�277
Ricaurte GA, Forno LS, Wilson MA, DeLanney LE, Irwin I,Molliver ME, Langston JW (1988) 3,4-ethylenedioxymetham-phetamine selectively damages central serotonergic neurons innonhuman primates. JAMA 260:51�55
Ricaurte GA, Martello AL, Katz JL, Martello MB (1992) Lastinge¤ects of 3,4-methylenedioxymethamphetamine (MDMA) oncentral serotonergic neurons in nonhuman primates: neuro-chemical observations. J Pharmacol Exp Ther 261:616�622
Saunders N (1995) Ecstasy and the dance culture. Neal�s YardDesktop Publishing, London
Schifano F (1995) Dangerous driving and MDMA (ecstasy) abuse.J Serotonin Res 1 :53�57
Schmidt CJ (1987) Neurotoxicity of the psychedelic amphetamine:MDMA. J Pharmacol Exp Ther 240:1�7
Series H, Boeles S, Dorkins E, Peveler R (1994) Psychiatric com-plications of ��Ecstasy�� use. J Psychopharmacol 8 :60�61
Solowij N, Hall W, Lee N (1992) Recreational MDMA use inSydney: a proÞle of ecstasy users and their experience with thedrug. Br J Addict 87:1161�1172
Spatt J, Glawar B, Mamoli B (1997) A pure amnesic syndrome afterMDMA ��ecstasy�� ingestion (letter). J Neurol NeurosurgPsychiatry 62:418�419
Squier MV, Jalloh S, Hilton-Jones D, Series H (1996) Death afterecstasy ingestion: neuropathological Þndings (letter). J NeurolNeurosurg Psychiatry 58:756�764
Steele TD, McCann UD, Ricaurte GA (1994) 3,4-Methylenedioxymethamphetamine (MDMA, ��ecstasy��): phar-macology and toxicology in animals and humans. Addiction89:539�551
Szabo Z, Sche¤el U, McCann U, Dannals RF, Ravert HT, MathewsWB, Musachio JL, Ricaurte GA (1997) Reductions of 5-HTtransporters in MDMA users observed using PET with[C�11](+)McN5652. Soc Neurosci Abstr 123:23
Triplady B (1996) Use of a personal digital assistant to administera visual search task. J Psychopharmacol 10:A27
Webb E, Ashton CH, Kelly P, Kamali F (1996) Alcohol and druguse in UK university students. Lancet 348:922�925
268