Embed Size (px)
Citation preview
Educating Nursing Home
Nurses on Efficient Use of the
Emergency Department
N U R S E E D U C A T O R
Authors: Sandra Mercer, RN, CEN, and Sherry Robinson, PhD,
RNCS, Springfield, IllSection Editor: Laura T. Gantt, RN, PhD, CEN, CAN, BC
Sandra Mercer is Clinical Nurse III, Emergency Department, MemorialMedical Center, Springfield, Ill.
Sherry Robinson is Gerontological Clinical Nurse Specialist, SIU Schoolof Medicine, Department of Medicine, Springfield, Ill.
For correspondence, write: Sherry Robinson, PhD, RNCS, SIU Schoolof Medicine, Department of Medicine, PO Box 19636, Springfield, IL62794-9636; E-mail: [email protected].
J Emerg Nurs 2008;34:74-6.
Available online 3 December 2007.
0099-1767/$34.00
Copyright n 2008 by the Emergency Nurses Association.
doi: 10.1016/j.jen.2007.05.002
74
emorial Medical Center in Springfield, Illi-
M nois, is a ‘‘Nurses Improving Care to Health
Systems Elders’’ (NICHE) Hospital. One of
the goals of the NICHE Committee is to improve care
to elders across all services. The emergency nurse, who
is a member of the NICHE Committee, queried other
emergency nurses to identify the most pressing issues they
faced in caring for elders. Repeatedly, the response was
related to patients who were admitted from nursing homes.
Nurses believed elders residing in nursing homes experi-
enced excessive lengths of stay in the emergency department.
In addition to dealing with the elder’s urgent need, the
longer length of stay necessitated careful attention to basic
care issues of toileting, nutrition, pressure ulcer preven-
tion, comfort, and rest. The nurses did not believe they
had enough resources to deliver all the care needed. The
nurses believed that some long stays were related to finding
return transportation to the nursing home.
The gerontological clinical nurse specialist (GCNS),
who served the hospital, also made regular rounds at local
nursing homes. She was hearing similar complaints from
nurses at the other end of the spectrum. Nursing home
nurses could not understand why their patients had such
long waits in the emergency department.
Examining the Problem
To examine the issue further, the emergency nurse and
the GCNS examined records of 50 patients who arrived
from nursing homes. The study was granted exemption
by the Springfield Committee for Research Involving
Human Subjects. The average length of stay was 5 hours
and 50 minutes, with the longest stay being 17 hours and
JOURNAL OF EMERGENCY NURSING 34:1 February 2008

N U R S E E D U C A T O R / M e r c e r a n d R o b i n s o n
19 minutes. Twenty of the patients arrived in the emer-
gency department between 4 PM and 10 PM. In our com-
munity, medivans do not operate after 5 PM. Only
ambulance service is available, but a person must meet
certain criteria for the ambulance transport to be covered
by Medicare. Five elders who were ready to return to the
nursing home in the evening could not return because the
discharge criteria did not meet Medicare standards for an
ambulance transfer. They had to spend the night in the
emergency department and return to the nursing home via
medivan the next morning.
An additional problem was identified with the record
review. Of the 50 records examined, 26 of the elders came
through the emergency department because the physician
had ordered blood transfusions, replacement of a G-tube, a
radiograph, or placement of a peripherally inserted central
catheter (PICC) line. All of these procedures are provided
by infusion services, special procedures, radiology, or inter-
ventional radiology. At our hospital, these services are
staffed from 8:00 AM to 4:30 PM. Consequently, the elders
who came through the emergency department had to wait
until hours of operation or until they could be worked into
the special department’s schedule.
Developing the Educational Program
Questioning of nursing home nurses by the GCNS
revealed that many nurses were unaware of the Medicare
regulations for ambulance transfer. Additionally, they
explained that it often was late in the afternoon when
they received calls from physicians’ offices giving the orders
for the various procedures. They thought they were acting
appropriately by sending patients through the emergency
department for blood transfusions, radiographs, G-tube
placements, and PICC line placement.
To remedy the situation, the emergency nurse devel-
oped an education program for nursing home nurses.
All of the special services departments were contacted to
determine the most common procedures utilized by elders
from nursing homes. A short in-service session and a
laminated card with telephone numbers for (1) infusions
services, where blood transfusions could be arranged, (2)
special procedures, where scopes could be arranged, and
(3) radiology, where feeding tubes and PICC lines could be
February 2008 34:1
scheduled (Figure 1), were developed. All of these services
could be arranged without sending patients through the
emergency department. An appointment could be made and
elders would not experience excessive waits. At the top of
the card, the emergency charge nurse’s number was listed,
where nursing home nurses could call with any questions.
Additionally, a list of transportation services was in-
cluded. The emergency nurse was able to locate one ambu-
lance service that would transport persons with nonemergent
problems for a private fee.
The emergency nurse then visited 8 nursing homes in
Springfield, accompanied by a representative of one of
the ambulance services. During a brief in-service session,
the emergency nurse explained that if the condition of the
elder would not be compromised by waiting until morn-
ing, the services would be much more efficient. Elders
would not have to experience the long waits. The elder also
would be much less stressed and experience less discomfort.
The representative of the ambulance service explained the
criteria for returning patients to the nursing home via am-
bulance. Nursing home staff members were encouraged to
ask the physician if the patient could be transported the
next morning after an appointment was set with the special
services. Copies of the card were left with the directors of
nursing to distribute to the nursing units.
To reinforce the use of the cards, the GCNS carried
additional cards. As she made rounds at the nursing homes,
she checked with each nurses’ station to see if they had
received the card. If not, one was displayed in an
appropriate place.
The Outcomes
The emergency nurse was well received by the nursing
homes. The nurses appreciated that the emergency depart-
ment was reaching out to them and had prepared some-
thing for them to facilitate care for their elders. The
emergency nurse approached them with respect and in a
positive manner with no intent to criticize them, but with a
mutual goal of providing better care for their elders.
To our knowledge, within the past month there have
been no admissions through the emergency department
when appointments should have been made in the special
JOURNAL OF EMERGENCY NURSING 75
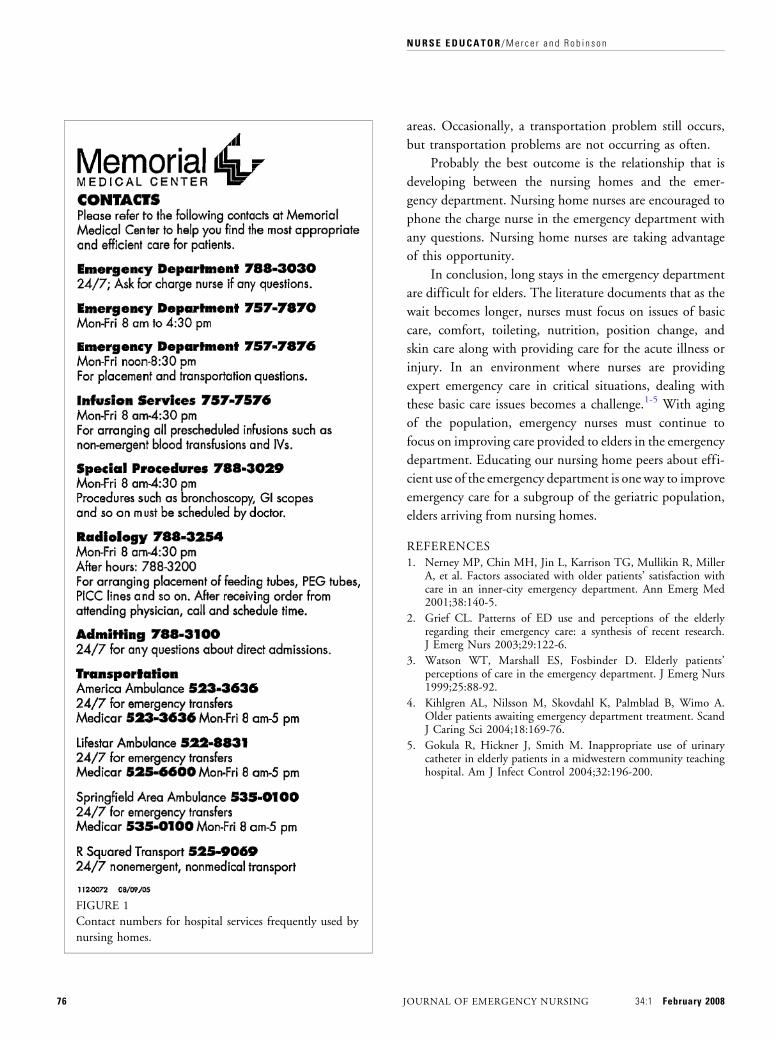
FIGURE 1
Contact numbers for hospital services frequently used by
nursing homes.
N U R S E E D U C A T O R / M e r c e r a n d R o b i n s o n
76 J
areas. Occasionally, a transportation problem still occurs,
but transportation problems are not occurring as often.
Probably the best outcome is the relationship that is
developing between the nursing homes and the emer-
gency department. Nursing home nurses are encouraged to
phone the charge nurse in the emergency department with
any questions. Nursing home nurses are taking advantage
of this opportunity.
In conclusion, long stays in the emergency department
are difficult for elders. The literature documents that as the
wait becomes longer, nurses must focus on issues of basic
care, comfort, toileting, nutrition, position change, and
skin care along with providing care for the acute illness or
injury. In an environment where nurses are providing
expert emergency care in critical situations, dealing with
these basic care issues becomes a challenge.1-5 With aging
of the population, emergency nurses must continue to
focus on improving care provided to elders in the emergency
department. Educating our nursing home peers about effi-
cient use of the emergency department is one way to improve
emergency care for a subgroup of the geriatric population,
elders arriving from nursing homes.
REFERENCES
1. Nerney MP, Chin MH, Jin L, Karrison TG, Mullikin R, MillerA, et al. Factors associated with older patients’ satisfaction withcare in an inner-city emergency department. Ann Emerg Med2001;38:140-5.
2. Grief CL. Patterns of ED use and perceptions of the elderlyregarding their emergency care: a synthesis of recent research.J Emerg Nurs 2003;29:122-6.
3. Watson WT, Marshall ES, Fosbinder D. Elderly patients’perceptions of care in the emergency department. J Emerg Nurs1999;25:88-92.
4. Kihlgren AL, Nilsson M, Skovdahl K, Palmblad B, Wimo A.Older patients awaiting emergency department treatment. ScandJ Caring Sci 2004;18:169-76.
5. Gokula R, Hickner J, Smith M. Inappropriate use of urinarycatheter in elderly patients in a midwestern community teachinghospital. Am J Infect Control 2004;32:196-200.
OURNAL OF EMERGENCY NURSING 34:1 February 2008





























