Embed Size (px)
Citation preview
728
Effect of Adenosine or Adenosine Triphosphate onAntidromic Tachycardia
HUAGUI G. LI, MD, PHD, CARLOS A . MORILLO, MD, MARCO ZARDINI, MD,
RANJAN K. THAKUR, MD, FACC, RAYMOND YEE, MD, FACC, GEORGE J . KLEIN, MD, FACC
London, Ontario, Canada
O4setives. This study was designed to determine the effect ofadenosine or adenosine triphosphate (ATP) on antidromic tachy-ardia.
aaeiigrouad. Adeaoslae and adenosine triphosphate are usefulfor dilreatial diagnosis of wide QRS tachyardia . It has beenbelieved that tachyardia termination caused by these agents isdue to the preferential depressive effect on the atrioveatricular(AV) mode, whereas their effect on accessory pathways is minimal .
Methods. We studied the effect of adenosine or ATP on thetermination pattern of antidromic tachyardla In 17 patients (10men, 7 wows; mean age (tSDI 32 t 11 years) with one or moreaccessory pathways . Adenosine (6 to 12 mg [a =101) or ATP (8 to20 ssg (n a 7)) was Injected rapidly through a central venous lineand followed by 10 ml of saline flush after Induction of sustainedantidromic tachyardia .
Rendts. Tahhyardla was terminated In <2 min in 14 patients(82%) after the injection and remained unchanged In 3 (18%) .
Both adenosine and adenosine triphosphate (ATP) have beenshown to be highly effective for termination of reentranttachycardia in which the atrioventricular (AV) node is anobligate part of the reentrant circuit (1-3) . The relevantelectrophysiologic effect is a brief but potent negative dromo-tropic action on the AV node, resulting in failure of conduc-tion . This feature has proved useful in the assessment of wideQRS tachycardia in which it is generally assumed that termi-nation of tachycardia signifies that the AV node is a part ofthe circuit and that ventricular tachycardia or accessory path-ways are generally not influenced by adenosine or ATP (4) .
Antidromic AV tachycardia has a reentrant circuit com-posed of an accessory pathway (anterograde limb) and the normalAV conduction system (retrograde limb) (5). The effect ofadenosine or ATP on antidromic tachycardia is unknown . We
From the Arrhythmia Service, Department of Medicine, University ofWestern Ontario, Ladon, Ontario, Canada . Dr. Li is a recipient of a ResearchFellowship from the Heart and Stroke Foundation of Canada, Ottawa, Ontario .Dr. Klein is a distinguished research professor of the Heart and StrokeFoundation of Ontario, Toronto, Ontario. This study was supported by the Heartand Stroke Foundation of Toronto, Toronto, Ontario .
Manuscript received September 20, 1993 ; revised manuscript receivedJamury 24, 1994, accepted March 31, 1994.Add= for glumandm: Dr. George J. Klein, University Hospital, 339
Windermere Road, London, Ontario N6A 5A5, Canada .
01994 by the American College of Cardiology
JACC Vol . 24, No. 3September 1994 :728-31
Tachycardia termination was due to conduction block in theaccessory pathway (anterograde limb) in seven patients (5070) andin the AV node (retrograde limb) in another seven . Adenosine orATP caused accessory pathway block in seven (88%) of the eightpatients lacking retrograde accessory pathway conduction and innone of the nine patients having retrograde accessory pathwayconduction (p < 0.01). All five patients with an atriofascicularaccessory pathway and unidirectional anterograde conductionhad tachyardia termination due to anterograde accessory path-way block after injection of adenosine or ATP.
Confusions. 1) Adenosine or ATP effectively terminates anti-dromic tachyardia ; 2) the termination is related to block in eitherthe accessory pathway or the AV node ; 3) accessory pathway blockoccurs in patients with a unidirectional, anterogradely conductingaccessory pathway, especially an atriofascicular accessory path-way.
(! Am Coll Cardiol 1994;24:728-31)
hypothesized that administration of either agent during anti-dromic AV tachycardia would cause tachycardia termination byblock in the retrograde limb of the reentrant circuit (AV node)and be useful in the clinical assessment of pre-excited tachycardia .
MethodsPatients. Seventeen patients with one or more accessory
pathways and antidromic tachycardia were studied from 1986to 1993 (10 men, 7 women; mean age [±SDI 32 ± 11 years,range 14 to 48), all referred for symptomatic tachycardia . WideQRS tachycardia was documented before the electrophysi-ologic study in 10 patients; in 7 it was induced only in theelectrophysiology laboratory .
Electrophysiologic study. Administration of all antiar-rhythmic drugs was stopped by a5 half-lives before the study .After oral and written consent was obtained, the patient wasstudied in the postabsorptive state in the electrophysiologylaboratory . Multipolar electrode catheters were percutane-ously inserted under local anesthesia and positioned in thecoronary sinus, high right atrium, His bundle region and rightventricular apex. Programmed stimulation was performed aspreviously described (6). Surface electrocardiographic (ECG)leads I, II, III, Vl and V6, as well as bipolar endocardialelectrograms from the coronary sinus, high right atrium, His
0735-1097/94157 .00
JAW MA. 24, No. 3September 1994 : 72 8 -31
PIRA
HOE
___J
IV-V
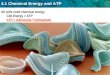
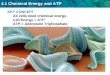
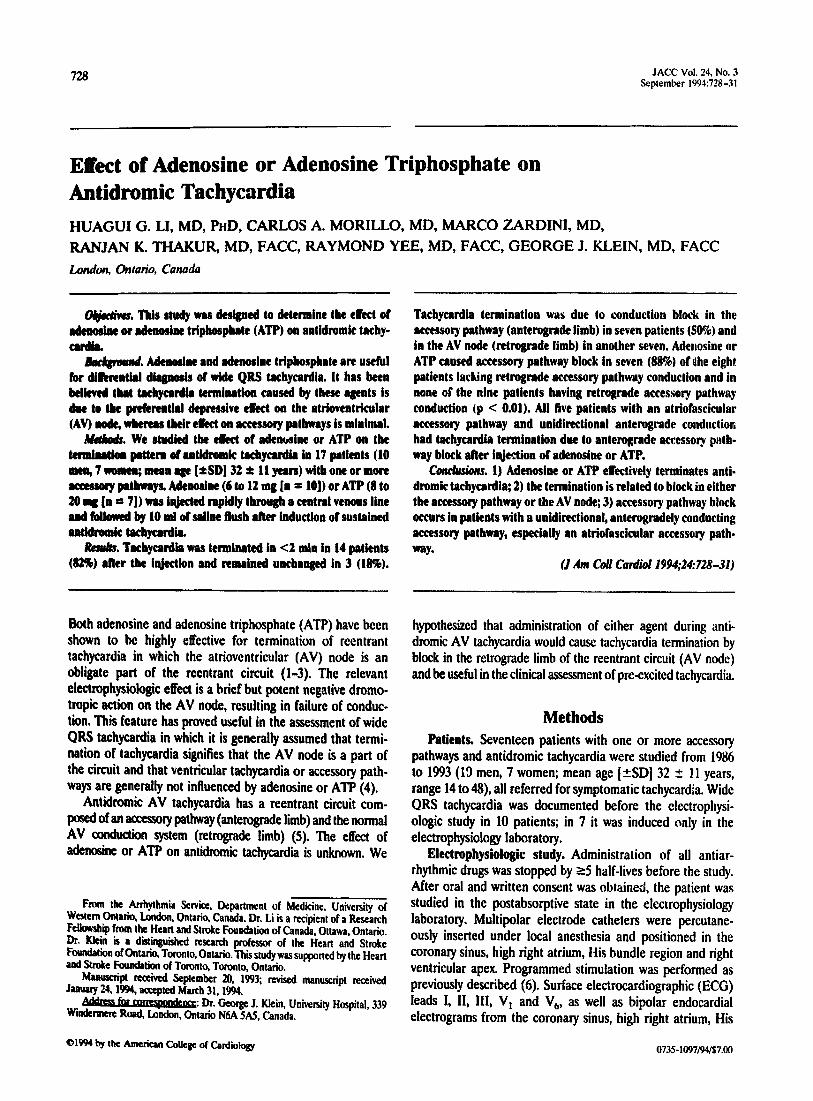
Figure 1. Termination of antidromic tachycardia resulted from antero-grade accessory conduction block after adenosine injection (6 mg) in apatient with an atriofascicular accessory pathway. Shown are surfaceelectrocardiographic leads 1, 11, V, and bipolar endocardiograms fromthe high right atrium (FIRA), His bundle region (HBE) and proximal(CS ) and distal (CS,,) coronary sinus . No apparent change in tachy-cardia cycle length was observed before termination . The QRS com-plex during sinus rhythm was normal, as typically observed withatriofuscicular pathways . H' indicates a retrograde His potential, whichis usually close to the QRS onset in atriofascicular pathways .
bundle region and right ventricular apex, were simultaneouslydisplayed on an oscilloscope, recorded on an ink recorder atthe speed of 100 mm/s and stored on the optical disk of an EPLab computer (Biomedical Instrument, Inc ., Toronto) .
Antidromic AV tachycardia was defined by demonstrationof anterograde conduction over an accessory AV pathway andretrograde conduction over the AV node (5) .
After the induction of sustained antidromic tachycardia(>5 min), 6 mg of adenosine (n = 10) or 8 mg of ATP (n = 7)was rapidly injected through the side port of a femoral sheathand followed by 10 ml of saline flush while the ECG wascontinuously monitored. If the tachycardia did not terminate in10 min, repeat injection at the same dose or twice the initialdose of adenosine or ATP was carried out . No further injectionwas given if doubling of the dose did not terminate tachycardia .
Follow-up. After the study, I I patients underwent success-ful surgical ablation of the accessory pathway, and 5 hadsuccessful catheter ablation using radiofrequency current ;1 patient whose tachycardia was well controlled with pro-pafenone did not undergo the ablation procedure . Repeatelectrophysiologic study was performed I week after thesurgical ablation and 30 min after the radiofrequency ablation .
Statistical analysis. Group values were expressed as meanvalue ± SD . A paired t test was performed for comparisonof values within the group and an unpaired t test for analysis ofmeans between different groups. A Fisher exact test wasperformed for analysis of incidence . A p value < 0.05 wasconsidered significant .
ResultsAccessory pathways. There were 21 accessory pathways in
the 17 patients (4 patients had a second accessory pathway) .There were I I left lateral, 8 right free wall and 2 right posteriorsepta] accessory pathways. Five patients had atriofascicular
LI ET AL. 729ADENOSINE OR ATP IN AN't 113ROMIC TACHYCARDIA
HRA- A*-T ---
f-11f---t
ACS,
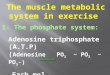
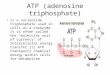
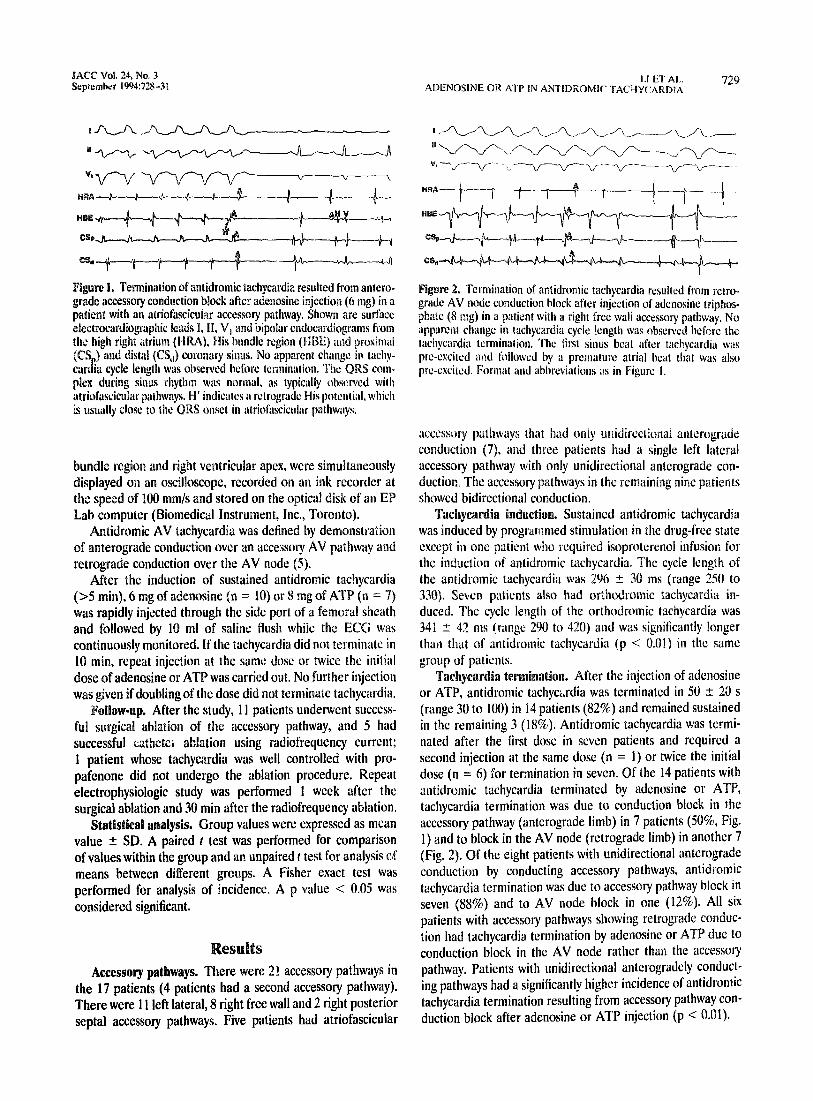
Figure 2 . Termination of antidromic tachycardia resulted from retro-grade AV node conduction block after injection of adenosine triphos-phate (8 mg) in a patient with a right free wall accessory pathway . Noapparent change in tachycardia cycle length was observed before thetachycardia termination . The first sinus beat after tachycardia waspre-excited and followed by a premature atrial beat that was alsopre-excited . Format and abbreviations as in Figure I .
accessory pathways that had only unidirectional anterogradeconduction (7), and three patients had a single left lateralaccessory pathway with only unidirectional anterograde con-duction. The accessory pathways in the remaining nine patientsshowed bidirectional conduction .
Tachycardia induction. Sustained antidromic tachycardiawas induced by programmed stimulation in the drug-free stateexcept in one patient who required isoproterenol infusion forthe induction of antidromic tachycardia. The cycle length ofthe antidromic tachycardia was 296 ± 30 ins (range 250 to330). Seven patients also had orthodromic tachycardia in-duced. The cycle length of the orthodromic tachycardia was341 ± 42 ms
( 'rage 290 to 420) and was significantly longer
than that of antidromic tachycardia (p < 0 .01) in the samegroup of patients .
Tachycardia termination. After the injection of adenosineor ATP, antidromic tachycardia was terminated in 50 ± 20 s(range 30 to 100) in 14 patients (82%) and remained sustainedin the remaining 3 (18%) . Antidromic tachycardia was termi-nated after the first dose in seven patients and required asecond injection at the same dose (n = 1) or twice the initialdose (n = 6) for termination in seven . Of the 14 patients withantidromic tachycardia terminated by adenosine or ATP,tachycardia termination was due to conduction block in theaccessory pathway (anterograde limb) in 7 patients (50%, Fig .1) and to block in the AV node (retrograde limb) in another 7(Fig . 2) . Of the eight patients with unidirectional anterogradeconduction by conducting accessory pathways, antidromictachycardia termination was due to accessory pathway block inseven (88%) and to AV node block in one (12%) . All sixpatients with accessory pathways showing retrograde conduc-tion had tachycardia termination by adenosine or ATP due toconduction block in the AV node rather than the accessorypathway. Patients with unidirectional anterogradely conduct-ing pathways had a significantly higher incidence of antidromictachycardia termination resulting from accessory pathway con-duction block after adenosine or ATP injection (p < 0 .01) .
730 LI ET ALADENOSINE OR ATP IN ANTIDROMIC TACHYCARDIA
Of the eight patients with right-sided accessory pathways,five patients (63%) had tachycardia termination in the acces-sory pathway. In contrast, only two (22%) of the nine patientswith left-sided accessory pathways had tachycardia terminationin the accessory pathway (p = NS) . All five patients withatriofascicular accessory pathways (7) showed decrementalconduction (progressive A-delta interval prolongation duringright atrial decremental pacing and extrastimulation) and hadtachycardia termination resulting from accessory pathway con-duction block . Decremental conduction was not observed inthe two patients with a single unidirectional anterogradelyconducting left lateral accessory pathway . There was no signif-icant difference in the anterograde effective refractory periodsof the AV node (264 ± 36 vs. 260 ± 30 ms, p = NS) and theaccessory pathway (285 ± 37 vs. 249 ± 36 ms, p = NS), andthe retrograde effective refractory period of the ventricu-loatrial conduction system (233 ± 45 vs . 265 ± 35 ms . p = NS)between the group with tachycardia termination in the acces-sory pathway and the group with tachycardia termination in theAV node (basic drive cycle length 600 ms) .
Additional accessory pathways. Of the four patients with asecond accessory pathway that was not involved in antidromictachycardia, two had concealed left lateral and two hadconcealed posteroseptal accessory pathways . The effect ofadenosine or ATP on these pathways could not be determinedbecause the study was performed only during antidromictachycardia .
Follow-up. In 16 of the 17 patients, all accessory pathwayswere successfully ablated by surgey (n = 11) or radio-frequency energy (n = 5) ; the remaining patient, whosetachycardia involved a single left lateral accessory pathway andwas well controlled with propafenone, did not undergo anablation procedure. After accessory pathway ablation, dual AVnode pathway physiology was observed in two patients butneither had induction of nonsustained or sustained AV nodereentrant tachycardia,
DiscussionPrevious studies. Adenosine and ATP are useful in the
diagnosis and treatment of reentrant tachycardia involving theAV node (1-4). The termination of a tachycardia involvingthe AV node is believed to be mainly due to a preferentialdepression of AV node conduction (2,4). In a previous studyfrom our laboratory (8), adenosine or ATP was found to haveminimal effects on the functional properties of AV accessorypathways in patients with orthodromic tachycardia . In patientswith antidromic tachycardia, the functional properties of theaccessory pathway and the AV node may be different fromthose in patients with only orthodromic tachycardia (9) . Others(10) have found shortening of the anterograde effective refrac-tory period of accessory pathways by adenosine .
Present study. Our present findings demonstrated thatantidromic tachycardia can be terminated by adenosine orATP in the majority of patients. Failure to terminate anti-dromic tachycardia in the minority of our patients might have
JACC Vol . 24, No. 3September 1994:'28-31
been due to insufficient dose . It is apparent in this study thatthe pattern of tachycardia termination depends on the prop-erties of the accessory pathway. In patients with unidirectional,anterogradely conducting accessory pathways, adenosine orATP terminated the antidromic tachycardia mainly by causingconduction block in the accessory pathway . In contrast, inpatients with bidirectional conducting accessory pathways,adenosine or ATP terminated the tachycardia mainly bycausing conduction block in the AV node. Our five patientswith right-sided atriofascicular accessory pathways all showeddecremental conduction in the accessory pathway and hadantidromic tachycardia termination by adenosine or ATP inthe accessory pathway. However, the absence of retrogradeconduction, rather than decremental conduction, may he amore significant determinant of the pattern of tachycardiatermination . This possibility is supported by our finding thattwo patients with left lateral accessory pathways demonstratingunidirectional anterograde conduction but no decrementalconduction also had antidromic tachycardia termination result-ing from accessory pathway conduction block .
Mechanism of induction of accessory pathway block byadenosine or ATP. It is not clear how adenosine and ATPinduce block in the accessory pathways . Both agents have beenshown to have multiple cardiovascular effects, including nega-tive chronotropic, dromotropic, vasodilator and antiadrenergicactions (11) . A preferential depressive effect of adenosine orATP on the AV node, which has predominantly calcium-dependent current in patients with orthodromic tachycardia,implies that adenosine or ATP may induce tachycardia termi-nation through the inhibitory effect on calcium current (11) .Atriofascicular accessory pathways and accessory pathwayswith unidirectionally anterograde conduction may have func-tional properties similar to those of the AV node (7) and thusrespond to adenosine or ATP.
Diagnosis of true antidromic tachycardia . This diagnosiswas confirmed by demonstration of obligatory anterogradeconduction over the accessory pathway and retrograde conduc-tion over he AV node . Pre-excited tachycardia involvingmultiple accessory pathways was excluded by the analysis ofactivation patterns. Atrioventricuiar node reentrant tachycar-dia with bystander anterograde accessory pathway conductionwas excluded by failure to demonstrate AV node reentranttachycardia before or after ablation of the accessory pathways .
implications. This study demonstrates that adenosine andATP are highly effective in terminating antidromic tachycardia .However, it also indicates that termination of a wide QRStachycardia may not necessarily be the result of AV nodeconduction block, even in reentrant tachycardia involving theAV node. This observation is also supported by recent reports(12-14) of termination of certain atrial and ventricular tachy-cardias after injection of adenosine or ATP . The present studyalso indicates that the termination pattern of a pre-excitedtachycardia by adenosine or ATP is not useful in differentiatingtrue antidromic AV tachycardia from AV node reentranttachycardia with bystander anterograde accessory pathway

JACC Vol . 24, No. 3September 1994 :728-31
conduction or AV reentry utilizing multiple accessory path-ways.
References
1 . 9elhassen B, Pelleg A, Shoshani D, Geva B, Laniado S . Electrophysiologiceffects of adenosine-5'-triphosphate on atrioventricular reentrant lachycar-dia. Circulation 1983;68:827-33 .
2 . DiMarco JP, Sellers TD, Berne RM, West A, Belardinelli L. Adenosine :electrophysiologic affects and therapeutic use for terminating paroxysmalsupraventricular tachycardia . Circulation 1983 ;68:1254-63 .
3, Berne RM. DiMarco JP, Belardinelli L. Dromotropic effects of adenosineand adenosine antagonists in the treatment of cardiac arrhythmias involvingthe atrioventricular node. Circulation 1984;69 :1195-7 .
4. Sharma AD, Klein GJ, Yee R . Intravenous adenosine triphosphate duringwide QRS complex tachycardia : safety, therapeutic efficacy, and diagnosticutility. Am J Med 199(1;88 :337-4.3 .
5 . Klein GJ . Pryonsky E Pritchett K Davis D, Gallagher L Atypical patternsof retrograde conduction over accessory airioventricular pathways in theWolli.Parkinson-White syndrome . Circulation 1979 ;60:1477-83 .
6 . Atie J, Brugada 11 , Brugada J, et al . Clinical and clecirophysiologic charac-teristics of patients with antidromic circus movement tachycardia in theWolfs-Parkinson-White syndrome . Am J (41W 1990;66 :108291 .
LI ET AL 731ADENOSINE OR ATP IN ANTIDROMIC TACHYCARDIA
7. Klein GJ, Yee R, Guiraudon GM . Accessory pathways with decrementalproperties. In : Josephson ME, Wellens HJJ, editors. Tachycardias: Mecha-nisms and Management . Mount Kisco, NY- Futura, 1993 :297-312.
8 . Rinne C, Sharma AD, Klein GJ, Yee R, Szabo T . Comparative effects ofadenosine triphosphate on accessory pathway and atrioventricular nodalconduction. Am Heart J 1988;115 :1042-7 .
9. Packer DL, Gallagher JJ, Prystowsky EN. Physiological substrate for anti-dromic reciprocating tachycardia . Prerequisite characteristics of the acces-sory pathways and atrioventricular conduction system . Circulation 1992;85 :574-88 .
10. Garrat CJ, Griffith J, O'Nunain S, Ward DE, Camm A] . Effects ofintravenous adenosine on antegrade refractoriness of accessory atrioventric-ular connections . Circulation 1991 ;84:1962-8 .
11 . Belardinelli L, Wu S-N, Visentin S . Adenosine regulation of cardiacelectrical activity . In : Zipes D, Jolifc J. editors. Cardiac Electrophysiology .From Cell to Bedside. Philadelphia : Saunders, 1990 :284-90.
12 . Perelman MS, Krikler DM. Termination of focal atrial tachycardia byadenosine triphosphate . Br Heart J 1987 ;528 :28-30.
13 . Wilber DJ, Baerman J, Olshansky B, Kall J, Kopp D. Adenosine-sensitiveventricular tachycardia. Clinical characteristics and response to catheterablation. Circulation 1993 ;87 :126-34.
14. Lerman BB, Belardinelli L, West GA, Berne RB, DiMarco JP . Adenosine-sensitive ventricular fachyeardia : evidence suggesting cyclic AMP-mediatedtriggered activity . Circulation 1986 ;74 :270-80.