Embed Size (px)
Citation preview

andrologia 16 (5): 397-405 (1984) Received January 4,1984
Institute of Semeiotica Medica, Cattedra di Patoiogia Medica 111, University of Padua and
Postgraduate School of Andrology, Cattedra di Clinica Medica I, University of Pisa/Italy
Effects of Naloxone on Gonadotropin Secretion in Klinefelter Syndrome
C. FORESTA, G.F. MENCHINI FABRIS, R. MIONI, N. SICOLO and C. SCANDELLARI
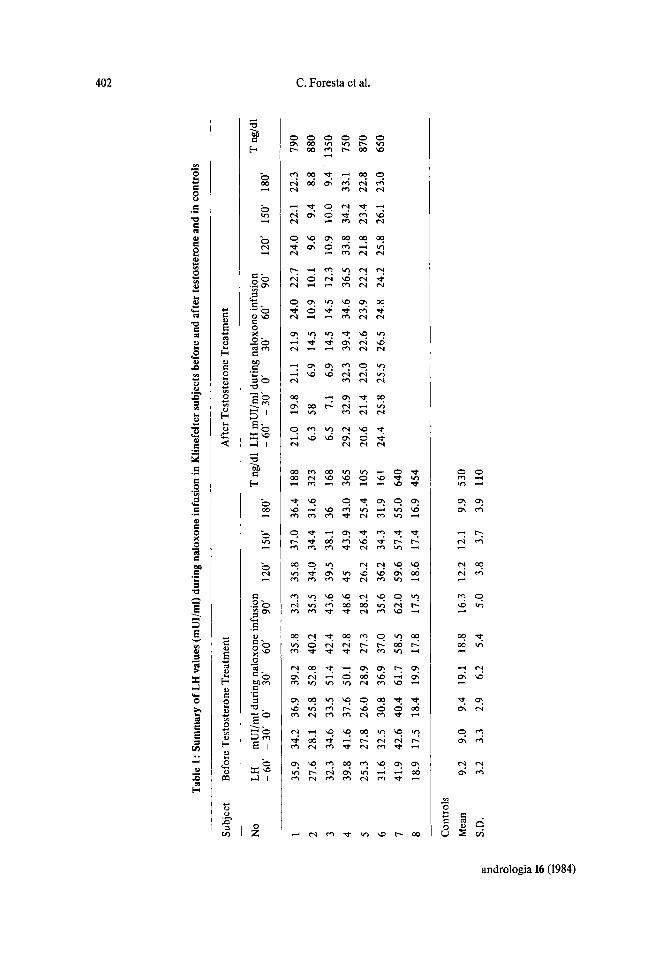
Summary: To study the opioid control on LH and FSH secretion in Klinefelter subjects (KS), the response of gonadotropin to an opioid antagonist, naloxone, was examined in 8 KS (age range 25-35 yrs) and in 8 age matched normal men. In 6 KS with low testos- terone plasma levels, naloxone infusion were also performed after treatment with testos- terone enanthate, 200 mg i.m. every 3 weeks for 4 months.
FSH did not show any important variation in KS and in normal men during naloxone infusion. In KS the percentage of naloxone induced LH increase was significantly lower than in controls and there was no correlation between testosterone plasma levels and LH increase after naloxone infusion. LH increases after naloxone infusion were not signifiant- ly different before and after testosterone treatment. The increases of naloxone induced LH plasma levels, before and after testosterone treatment, correlated well between them- selves (r = 0.93-p < 0.01). Plasma levels decreased in all patients after testosterone treat- ment, but only in two was there a return to normal range. There is a c l e w positive linear correlation between the percentage of LH decrease after testosterone treatment and LH increase after naloxone infusion (r = 0.81 ; p < 0.01).
After testosterone therapy FSH plasma levels fall by 63 k 15% in all patients and did not show any important variation after naloxone infusion.
In conclusion, our data are in agreement with the hypothesis that in Klinefelter’s syn- drome an alteration of opioid control on gonadotropin secretion may exist. This altera- tion does not appear to be due to androgen deficiency, but rather it may be caused by genetic abnormalities. In Klinefelter subjects the alterated opiatergic control on gonado- tropin secretion may cause the reduced LH feedback sensitivity to testosterone.
Wirkung von Naloxon auf die Gonadotropin-Sekretion beim Klinefelter Syndrom
Zusammenfassung: Urn die Opiat-Kontrolle der LH- und FSH-Sekretion bei Klinefel- ter-Patienten (KP) zu untersuchen, wurde die Wirkung von Naloxon, einem Opiat-Antago- nisten, auf die Gonadotropine bei 8 KP (Alter zwischen 25 und 35 Jahren) und 8 entspre- chenden gesunden Mannern untersucht.
Key words: Klinefelter syndrome, naloxone - gonadotropin, naloxone - naloxone, gonadotropin - testosterone, naloxone
andrologia 16 (1984)
398 C. Foresta et al.
Bei 6 KP mit herabgesetztem TestosteronPlasmaspiegel wurden Naloxon-Infusionen auch nach Behandlung mit Testosteron-Enanthat durchgef&rt, und zwar 200 mg i.m. al- le 3 Wochen uber 4 Monate.
FSH zeigte keine bedeutenden Unterschiede bei KP und bei gesunden Mannern. Bei KP war der Prozentsatz des Naloxon-induzierten LH-Anstieges signifiiant geringer als bei den Kontrollen; es gab keine Korrelation zwischen Testosteron-Plasmaspiegeln und LH- Anstieg nach Naloxon-Infusion. LH-Anstiege nach Naloxon-Infusionen unterschieden sich nicht signifkant vor und nach Testosteron-Behandlung. Der Anstieg der Naloxon-indu- zierten LH-Plasma-Konzentration korrelierte gut untereinander (r = 0,93; p < 0.01). Die Plasma-Konzentration sank bei allen Patienten nach Testosteron-Behandlung ; nur bei zwei Patienten erreichten sie wieder die normalen Werte. Es gibt eine klare positiv lineare Kor- relation zwischen der prozentualen LH-Verminderung nach Testosteron-Behandlung und dem LH-Anstieg nach Naloxon-Infusion (r = 0,81; p < 0,Ol).
Nach Testosteron-Behandlung sank die FSH-Plasma Konzentration um 63 * 15% bei allen Patienten und zeigte keine bedeutende Abweichung nach Naloxon-Infusion.
ZusammengefaPt stimmen die Daten mit der Hypothese uberein, daB bei dem Klinefel- ter Syndrom eine hderung der Opiat-Kontrolle der Gonadotropin-Sekretion bestehen konnte. Diese Xnderung scheint nicht durch einen Androgen-Mange1 verursacht zu sein, sondern eher durch genetische Abnormalitaten. Bei Khefelter Patienten scheint die ver- anderte Opiat-Kontrolle der Gonadotropin-Sekretion die verminderte LH-Ruckkopplungs- Empfmdlichkeit zu verursachen.
Introduction
Klinefelter’s syndrome is a form of primary hypogonadism associated with subtle ab- normalities in hypothalamic-pituitary regulation (Chelkh et al. - 1981; Dickerman et al. - 1981). In particular the function of the hypothalamic gonadal axis in this syndrome is not typical of hypergonadotropic hypogonadism. In fact in Klinefelter subjects even when testosterone plasma levels are normal, an inappropriately compensatory high LH plasma level exists (Paulsen et al. - 1968). Moreover, abnormalities in gonadotropin sup- pression with testosterone administration were demonstrated (Capell et al. - 1973; Forti et al. - 1978) and as well an absence of LH rise after clomiphene citrate administration was observed (Weinstein et al. - 1971).
of gonadotropin secretion in man (Stubbs et al. - 1978). Endogenous opioid peptides in- hibit LH secretion by interacting with specific opiate receptors at a suprahypophyseal level (Cicero et d. - 1980; Fraioli et al. - 1982) while naloxone, a specific opioid antago- nist, stimulates gonadotropin release (Grossman et al. - 1981).
The aim of this study was to investigate the opioid control of gonadotropin secretion in Klinefelter subjects.
Recent works report endogenous opioid peptides are involved in the control mechanism
Materials and Methods
47XXY) (age range 25-34 yrs) and 8 age-matched normal men. Informed consent was obtained from all subjects. None of the patients was taking gonadal steroid therapy. After an overnight fast, three 10 ml aliquots of venous blood were obtained at 30 minutes inter- vals from each patient. The mean of these three basal values at 08.00,08.30, and 09.00 hours represent the basal secretion and were defined as 100%. An intravenous bolus in-
The study was carried out on 8 subjects affected by Klinefelter syndrome (Karyotype
0 andrologia 16 (1984)
Naloxone 40 1
140 0
g 120 n s S i l o o -
;c' 8 0 -
0 Y 0 2
W M U
u Y 6 0 - I
5 4 0 -
2 0 -
c az W
W a
-
-
I P .z 0 . 0 0 1 7 . - . .
. t
- . - .
c aE W u
I 01
KLINEFELTEA 0 20 40 60 80 100 NORMAL
PERCENT LH INCREASE NALOXONE INDUCED
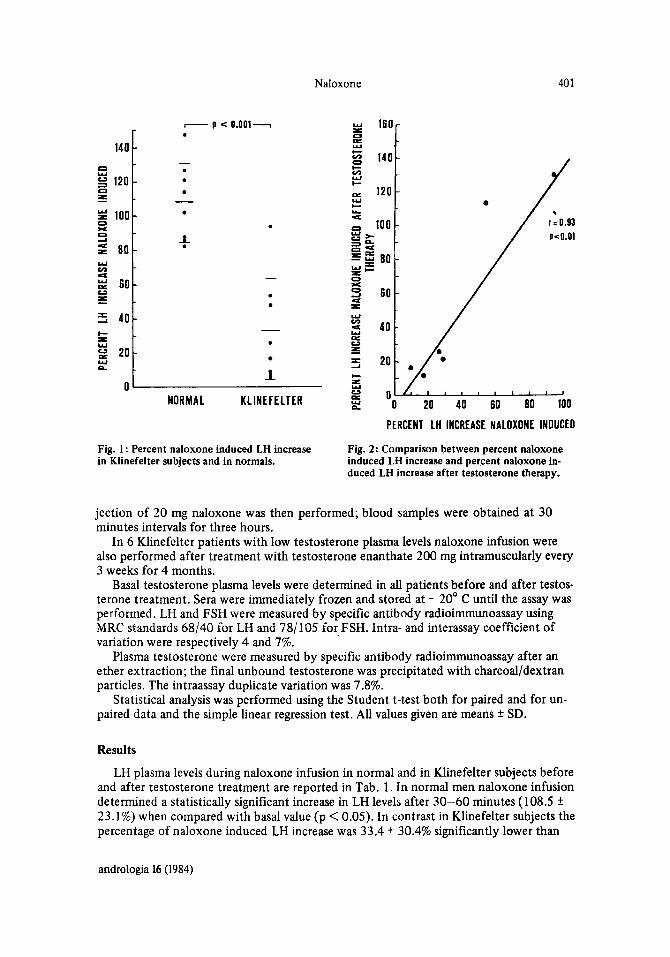
Fig. 1 : Percent naloxone induced LH increase in Klinefelter subjects and in normals.
Fig. 2: Comparison between percent naloxone induced LH increase and percent naloxone in- duced LH increase after testosterone therapy.
jection of 20 mg naloxone was then performed; blood samples were obtained at 30 minutes intervals for three hours.
In 6 Klinefelter patients with low testosterone plasma levels naloxone infusion were also performed after treatment with testosterone enanthate 200 mg intramuscularly every 3 weeks for 4 months.
Basal testosterone plasma levels were determined in all patients before and after testos- terone treatment. Sera were immediately frozen and stored at - 20' C until the assay was performed. LH and FSH were measured by specific antibody radioimmunoassay using MRC standards 68/40 for LH and 78/105 for FSH. fntra- and interassay coefficient of variation were respectively 4 and 7%.
Plasma testosterone were measured by specific antibody radioimmunoassay after an ether extraction; the final unbound testosterone was precipitated with charcoal/dextran particles. The intraassay duplicate variation was 7.8%.
Statistical analysis was performed using the Student t-test both for paired and for un- paired data and the simple linear regression test. All values given are means f SD.
Results
LH plasma levels during naloxone infusion in normal and in Klinefelter subjects before and after testosterone treatment are reported in Tab. 1. In normal men naloxone infusion determined a statistically significant increase in LH levels after 30-60 minutes (108.5 f 23.1%) when compared with basal value (p < 0.05). In contrast in Klinefelter subjects the percentage of naloxone induced LH increase-was 33.4 f 30.4% significantly lower than
andrologia 16 (1984)
P
0
I4
Tab
le 1
: Su
mm
ary
of L
H v
alue
s (m
UI/
ml)
duri
ng n
alox
one
infu
sion
in K
linef
elte
r sub
ject
s bef
ore
and
afte
r te
stos
tero
ne a
nd in
con
trol
s
Subj
ect
Bef
ore
Tes
tost
eron
e T
reat
men
t A
fter
Tes
tost
eron
e T
reat
men
t
No
LH
mU
I/m
l dur
ing
nalo
xone
infu
sion
T
ng/d
l LH
mU
I/m
l duf
ing
nalo
xone
ipfu
sion
T
ng/
dl
- 6
0’ -
30’
0’
30’
60’
90’
120’
15
0’
180’
-6
0’ -
30’
0 30
‘ 60
90
‘ 12
0’
150’
18
0‘
P 2
27.6
28
.1
25.8
52
.8
40.2
35
.5
34.0
34
.4
31.6
32
3 6.
3 58
6.
9 14
.5
10.9
10
.1
9.6
9.4
8.8
880
crl
r!
1 35
.9
34.2
36
.9
39.2
35
.8
32.3
35
.8
37.0
36
.4
188
21.0
19
.8
21.1
21
.9
24.0
22
.7
24.0
22
.1
22.3
79
0
$ 3
32.3
34
.6
33.5
51
.4
42.4
43
.6
39.5
38
.1
36
168
6.5
7.1
6.9
14.5
14
.5
12.3
10
.9
10.0
9.
4 13
50
4 39
.8
41.6
37
.6
50.1
42
.8
48.6
45
43
.9
43.0
36
5 29
.2
32.9
32
.3
39.4
34
.6
36.5
33
.8
34.2
33
.1
750
CD
*
5 25
.3
27.8
26
.0
28.9
27
.3
28.2
26
.2
26.4
25
.4
105
20.6
21
.4
22.0
22
.6
23.9
22
.2
21.8
23
.4
22.8
87
0 F-
6 31
.6
32.5
30
.8
36.9
37
.0
35.6
36
.2
34.3
31
.9
161
24.4
25
.8
25.5
26
.5
24.8
24
.2
25.8
26
.1
23.0
65
0 7
41.9
42
.6
40.4
61
.7
58.5
62
.0
59.6
57
.4
55.0
64
0 8
18.9
17
.5
18.4
19
.9
17.8
17
.5
18.6
17
.4
16.9
45
4
Con
trol
s M
ean
9.2
9.0
9.4
19.1
18
.8
16.3
12
.2
12.1
9.
9 53
0 Eu
S.D.
3.2
3.3
2.9
6.2
5.4
5.0
3.8
3.7
3.9
110
a 3

Naloxone 493
controls (p < 0.001). A clear increment of LH plasma levels in response to naloxone infu- sion was observed only in one patient; in two cases it was moderate and in the remaining patients slight (Fig. 1). There was no correlation between basal LH plasma levels and LH increase after naloxone infusion. FSH plasma levels did not show any important variation in normal and in Klinefelter subjects after naloxone infusion.
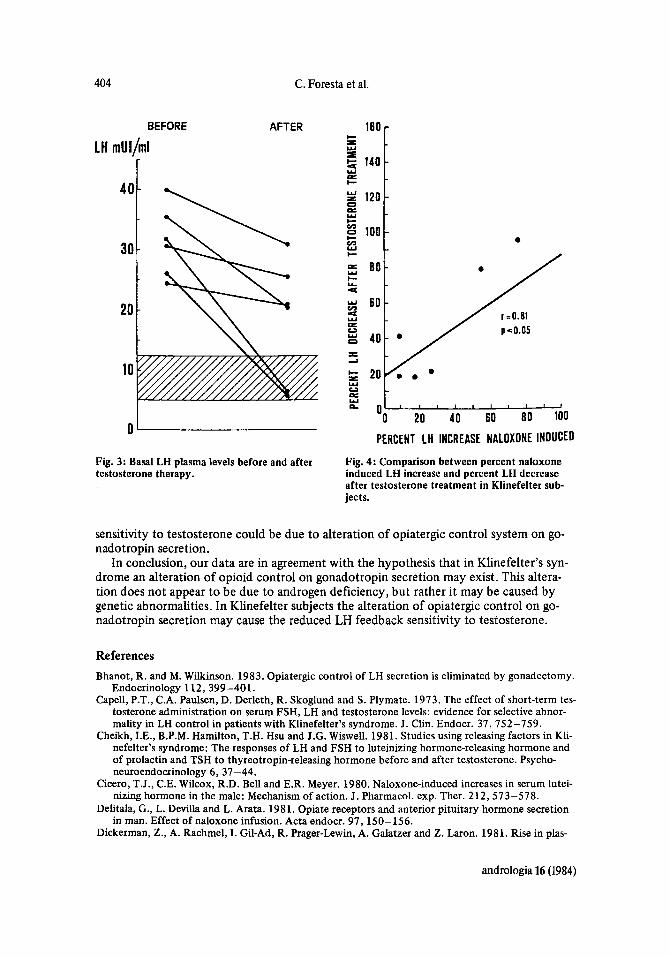
Testosterone plasma levels in Klinefelter subjects were 281 k 208 ng/100 ml, signifi- cantly lower (p < 0.01) than controls (530 k 120 ng/lOO ml) and only in two subjects they were in the normal range (Tab. 1). There was no correlation between testosterone plasma levels and LH increase after naloxone infusion. Intramuscular testosterone admin- istration for 4 months raised testosterone plasma levels in all patients. LH increases after naloxone infusion were not significantly different between before and after testosterone treatment. The increase of naloxone induced LH plasma levels, before and after testoste- rone treatment, correlated well between themselves (Fig. 2) (r = 0.93; p < 0.01). Plasma LH levels decreased in all patients after testosterone treatment, but only in two there was a return to normal range despite increased testosterone plasma levels in all patients (Fig. 3). There is a clearly positive linear correlation between the percentage of LH de- crease after testosterone treatment and LH increase after naloxone infusion (r = 0.8 1 ; p < 0.01) (Fig. 4). After testosterone therapy FSH plasma levels fell by 63 k 15% in all patients and did not show any important variation after naloxone infusion.
Discussion
The results of our experiments with naloxone suggest that in Klinefelter subjects an alteration of opioid control on gonadotropin secretion exists. The hypothalamic opiatergic system normally inhibits LH secretion by interacting with specific opiate receptors (Cice- ro et al. - 1980). Several studies suggested that endogenous opioid may be involved in the negative feedback by gonadal steroids on gonadotropin secretion both in animals (van Vugt et al. - 1981) and in man (Foresta e t al. - 1983). Moreover, recent works report that gonadal steroids regulate hypothalamic B-Endrophin and its release into the hypothalamic- hypophyseal portal blood (Wardlaw et al. - 1982). Opiate antagonist such as naloxone, acting to displace the agonist from the opiate receptors, can block agonist action (Delitala et al. - 1981).
In our Klinefelter subjects the LH response to naloxone infusion in 5 cases is almost absent, in 2 cases moderate and only in 1 case normal. Naloxone is unable to stimulate LH release when gonadal steroids are absent as after menopause (Lightman et al. - 1981) or in castrated men (Foresta and Scandellari - 1983) and animals (Bhanot and Wilkinson - 1983). In these cases gonadal replacement is able to largely restore the LH response to naloxone. In our patients the naloxone induced LH increase does not relate to testosterone plasma levels and testosterone replacement does not significantly improve the LH secre- tion after naloxone stimulation. Our data suggest however that in Klinefelter’s syndrome the alteration of opioid control on gonadotropin secretion is not due to the androgenic deficiency. This alteration could be due to the genetic abnormality.
ment for 4 months lowered the elevated basal LH and FSH plasma levels but normal values, especially LH levels, were not achieved in all patients despite normal plasma tes- tosterone levels. These results confirm that in Khefelter’s syndrome there are abnor- malities in testosterone LH feedback mechanisms. The suppressibility of LH plasma levels during testosterone treatment, in our patients, is related to the naloxone induced LH in- crease. These findings suggest that in Klinefelter’s syndrome the reduced LH feedback
In our study, in agreement with other authors (Smais et al. - 1979), testosterone treat-
andrologia 16 (1984)
404
I- = Y
140
2 120
g 100
W
I- a
0 = W
c vr
C. Foresta et al.
-
-
-
AFTER 160 r
LH
0 L
b
PERCENT L H INCREASE NALOXONE INDUCED
Fig. 3: Basal LH plasma levels before and after testosterone therapy.
Fig. 4: Comparison between percent naloxone induced LH increase and percent LH decrease. after testosterone treatment in Klinefelter sub- jects.
sensitivity to testosterone could be due to alteration of opiatergic control system on go- nadotropin secretion.
In conclusion, our data are in agreement with the hypothesis that in Klinefelter's syn- drome an alteration of opioid control on gonadotropin secretion may exist. This altera- tion does not appear to be due to androgen deficiency, but rather it may be caused by genetic abnormalities. In Klinefelter subjects the alteration of opiatergic control on go- nadotropin secretion may cause the reduced LH feedback sensitivity to testosterone.
References Bhanot, R. and M. Wilkinson. 1983. Opiatergic control of LH secretion is eliminated by gonadectomy.
Endocrinology 112, 399-401. Capell, P.T., C.A. Paulsen, D. Derleth, R. Skoglund and S. Plymate. 1973. The effect of short-term tes-
tosterone administration on serum FSH, LH and testosterone levels: evidence for selective abnor- mality in LH control in patients with Klinefelter's syndrome. J. Clin. Endocr. 37, 752-759.
Cheikh, I.E., B.P.M. Hamilton, T.H. Hsu and J.G. Wiswell. 1981. Studies using releasing factors in Kli- nefelter's syndrome: The responses of LH and FSH to luteinizing hormone-releasing hormone and of prolactin and TSH to thyreotropin-releasing hormone before and after testosterone. Psycho- neuroendocrinology 6, 37-44.
Cicero, T.J., C.E. Wilcox, R.D. Bell and E.R. Meyer. 1980. Naloxone-induced increases in serum lutei- nizing hormone in the male: Mechanism of action. J. Pharmacol. exp. Ther. 212,573-578.
Delitala, G., L. Devilla and L. Arata. 1981. Opiate receptors and anterior pituitary hormone secretion in man. Effect of naloxone infusion. Acta endocr. 97,150-156.
Dickerman, Z., A. Rachmel, I. Gil-Ad, R. Prager-Lewin, A. Galatzer and Z. Laron. 1981. Rise in plas-
andrologia 16 (1984)

Naloxone 405
ma growth hormone in response to exogenous LRH in Klinefelter’s syndrome. Clin Endocr. 15, 403-410.
Foresta, C., G. Scanelli, A. Fabbri, L. Gnessi, C. Moretti and F. Fraioli. 1983. Naloxone fails to in- crease LH levels in clomiphene treatment males. Hormon. metab. Res. (in press).
Foresta, C. and C. Scandellari. 1983. Opioid system and gonadotropin secretion: role of gonadal ste- roids. J. Endocrinol. Invest. 6 (Suppl. 1),8.
Forti, G., A. Borghi, G. Giusti, M. Pazzagli, P. Giannotti, M. Maunelli, S. Fusi and M. Serio. 1978. Kli- nefelter’s syndrome: effects of short-term testosterone administration on hypothalamic pituitary axis function. J. Endocr. 1,239-244.
Fraioli, F., A.E. Panerai, C. Santoro, A. Fabbri, F. Santoro and A. Isidori. 1982. Control of gonado- tropin secretion in man;role of opioid peptides. Horm. metab. Res. 14, 313-317.
Grossman, A., P.J.A. Moult, R.C. Gailard, G. Delitala, W.D. Toff, L.H. Ress and G.M. Besser. 1981. The opioid control of LH and FSH release: effects of a Met-Enkefalin analogue and naloxone. Clin. Endocr. 14,41-47.
opioid control of luteinizing hormone in different pathophysiological states. J. Clin. Endocr. 52, Lightman, S.L., H.S. Jacobs, A.K. Maguire, G. MacGarriek and S.L. Jeffcoata. 1981. Constancy of
1260-1263. Paulsen, C.A., D.L. Gordon, R.W. Carpenter, H.M. Gandy and W.D. Drucker. 1968. Klinefelter’s syn-
drome and its variants, a hormonal and chromosomal study. Recent Progr. Hormone Res. 24,321- 363.
Smals, A.G.H., P.W.C. Kloppenborg, G.F.E. Peters, W.H.L. Hoefnagels, R.M. Lequin and T.J. Benraad. 1979. Modulation of the gonadotropin response to constant luteinizing hormone releasing hormone infusion by acute and chronic testosterone administration in Klinefelter’s syndrome. J. Clin. Endocr. 48,148-152.
Stubbs, D.A., G. Delitala, A. Jones, W.J. Jeffcoate, C.R.W. Edwards, S.J. Ratter, G.M. Besser, S.R. Bloom and K.G.M.M. Alberti. 1978. Hormonal and metabolic responses to an enkephalin analogue in normal man. Lancet ii, 1225-1227.
Van Vugt, D.A., P.W. Sylvester, C.F. Aylsworth and J. Meites. 1982. Counteraction of gonadal steroid inhibition of luteinizing hormone release by naloxone. Neuroendocrinology 34,274-278.
Wardlaw, S.L., W.B. Wehrenberg, M. Ferin, J.L. Antunes, A.G. Frantz. 1982. Effect of sexsteroid on betaendorphin in hypophyseal portal blood. J. Clin. Endocr. 55, 877-883.
Weinstein, R.L., S.L. Kaplan and M.M. Grumbach. 1971. Gonadal and pituitary insensitivity to HCG and clomiphene. Program Endocrine Society 53, rd meeting A-102 abstract.
Address: C. FORESTA, Istituto di Semeiotica Medica, Universith di Padova, Via Ospedale 105, 35100- Padova/I talia.
andrologia 16 (1984)