Embed Size (px)
Citation preview

Giovambattista DesideriDivisione di Geriatria
Università degli Studi di L’Aquila
Effetto della riduzione immediata della pressione
arteriosa su mortalità e disabilità nel paziente con
stroke ischemico acuto: troppo è dannoso (secondo
lo studio CATIS....)
ü In Italia l’ictus è la terza causa di mortedopo le malattie cardiovascolari e le neoplasie, causando il 10%-12% di tutti i decessi per anno, e rappresenta la principale causa di invalidità.
ü Ogni anno si verificano in Italia (dati estrapolati dalla popolazione del 2001) circa 196.000 ictus, di cui l’80% sono nuovi episodi e il 20% recidive.
ü L’incidenza dell’ictus aumenta progressivamente con l’età raggiungendo il valore massimo negli ultra ottantacinquenni. Il 75% degli ictus si verifica in soggetti ultrasessantacinquenni.
ü Il tasso di prevalenza di ictus nella popolazione anziana (età 65-84 anni) italiana è del 6,5%, più alto negli uomini (7,4%) rispetto alle donne (5,9%).
AfterBefore
Acute phase
Hypertension and Brain: dangerous relationships…
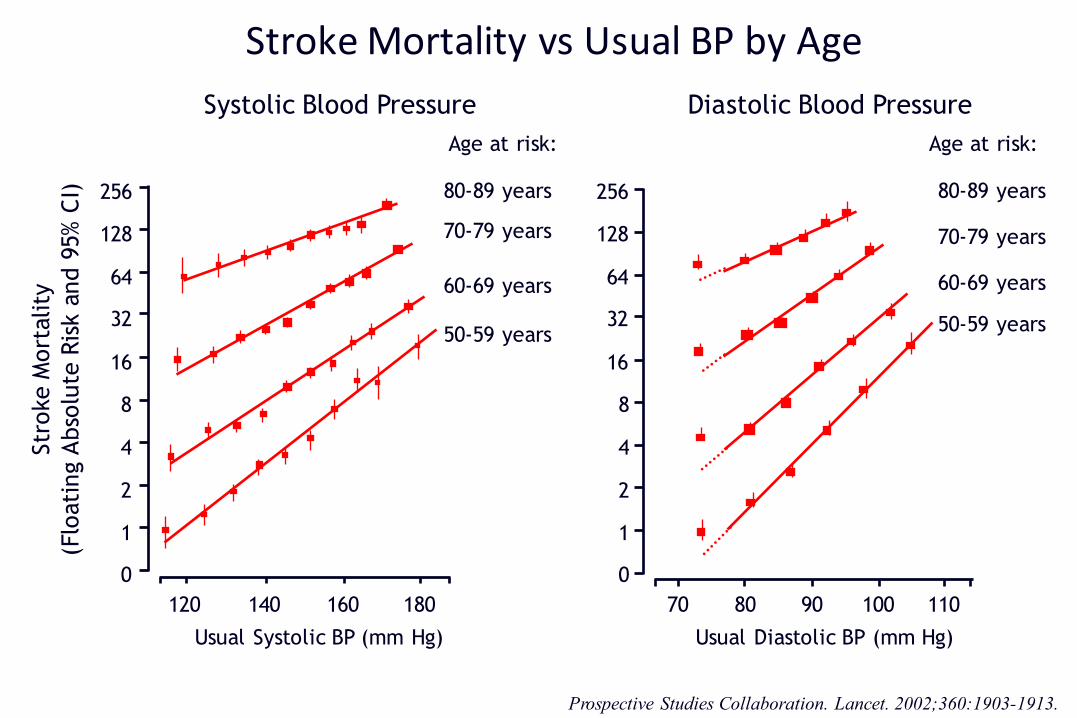
StrokeMortalityvsUsualBPbyAge
Prospective Studies Collaboration. Lancet. 2002;360:1903-1913.
Stro
ke M
ort
alit
y(F
loat
ing
Abso
lute
Ris
k an
d 9
5% C
I)
Usual Systolic BP (mm Hg)
50-59 years
60-69 years
70-79 years
80-89 years
Systolic Blood Pressure Diastolic Blood Pressure
Usual Diastolic BP (mm Hg)
50-59 years
60-69 years
70-79 years
80-89 years
Age at risk: Age at risk:
256
128
64
32
16
8
4
2
1
0
120 140 160 180
256
128
64
32
16
8
4
2
1
0
70 80 90 110100
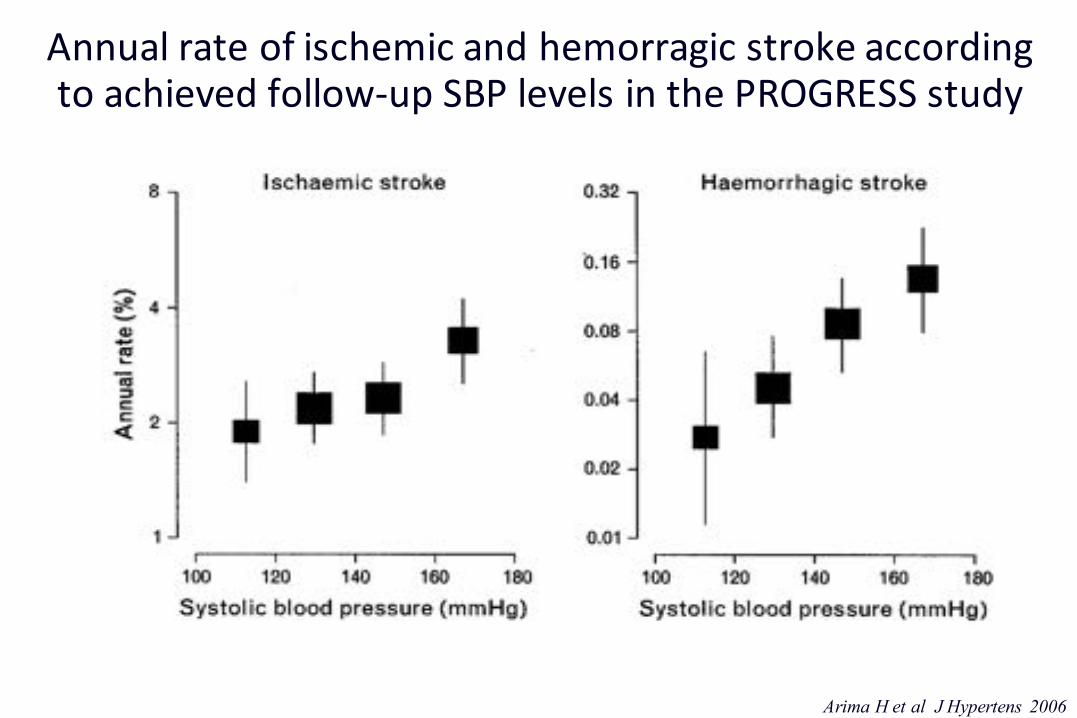
Annual rateofischemic andhemorragic stroke accordingtoachieved follow-upSBPlevels inthePROGRESSstudy
Arima H et al J Hypertens 2006
AfterBefore
Acute phase
Hypertension and Brain: dangerous relationships…
…The management of arterial hypertension in patients notundergoing reperfusion strategies remains challenging.
Data to guide recommendations for treatment are inconclusive or conflicting…
Jauch EC et al. Stroke. 2013;44:870-947
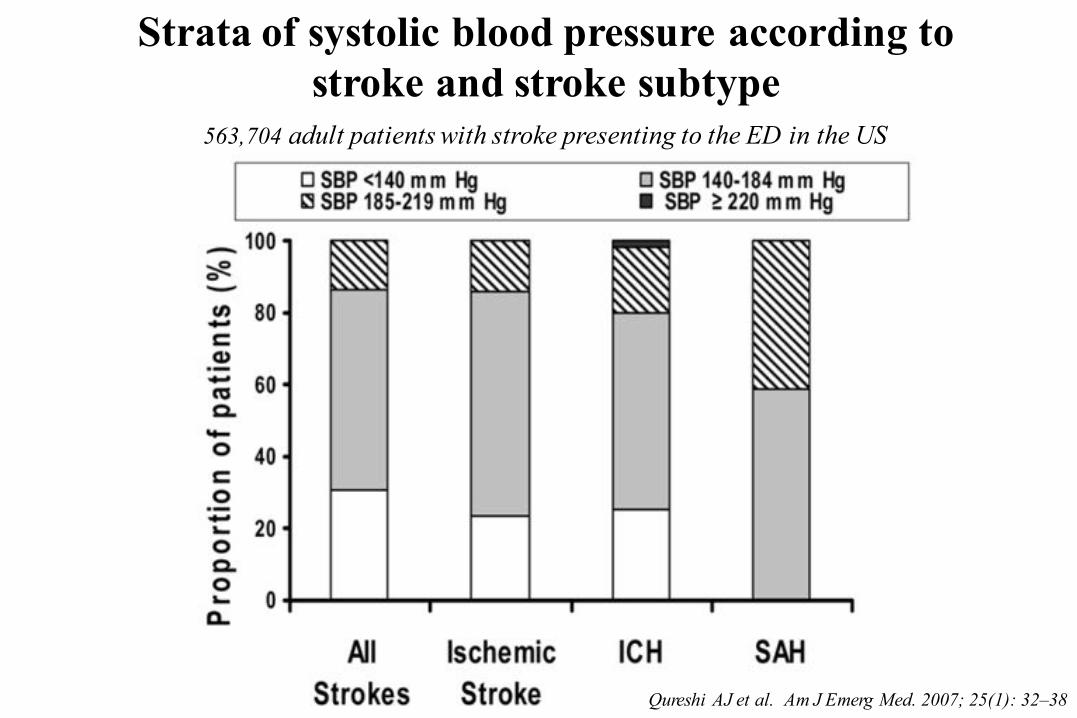
563,704 adult patients with stroke presenting to the ED in the US
Strata of systolic blood pressure according to stroke and stroke subtype
Qureshi AJ et al. Am J Emerg Med. 2007; 25(1): 32–38
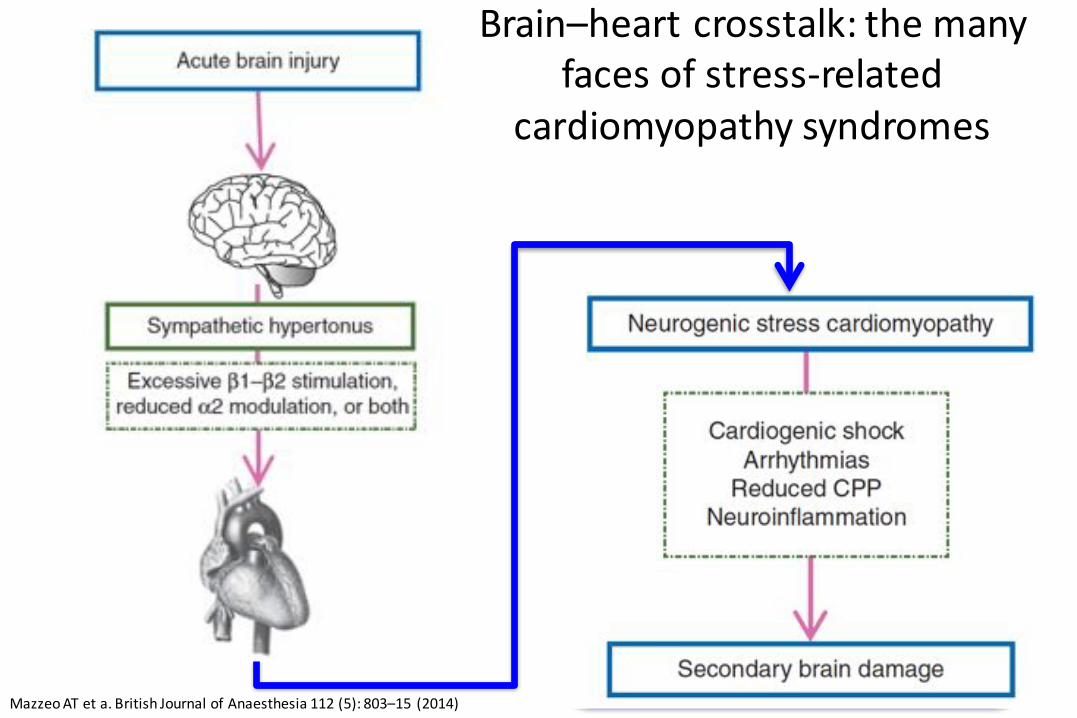
Brain–heart crosstalk:themanyfaces ofstress-related
cardiomyopathy syndromes
MazzeoATeta.BritishJournalofAnaesthesia112(5):803–15 (2014)
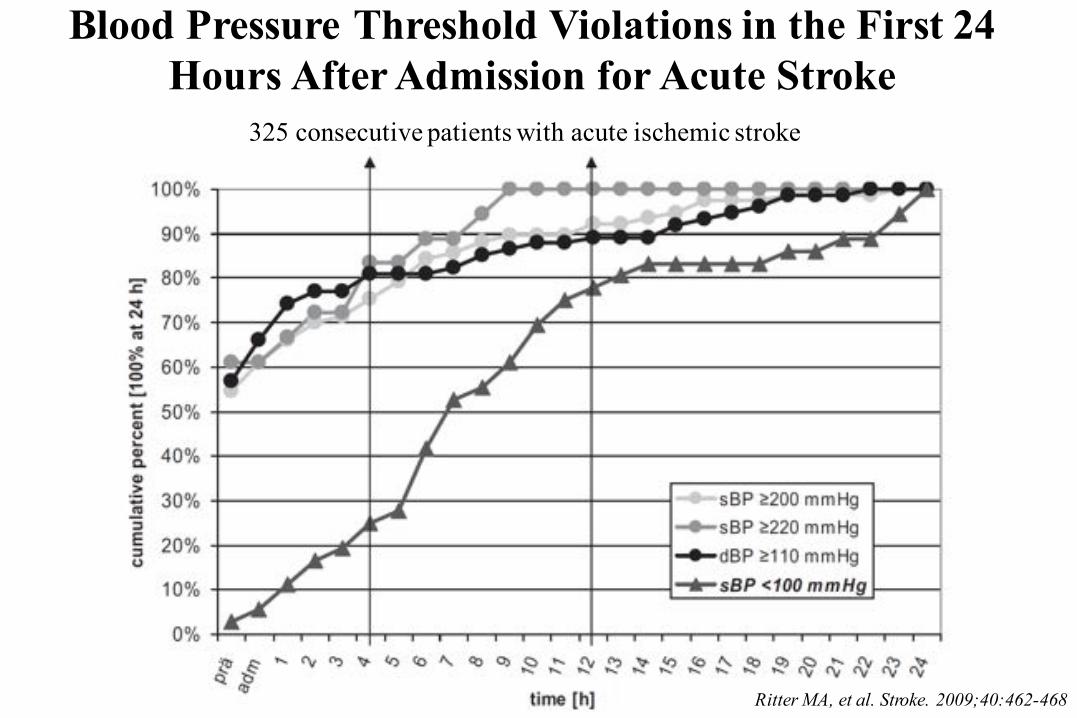
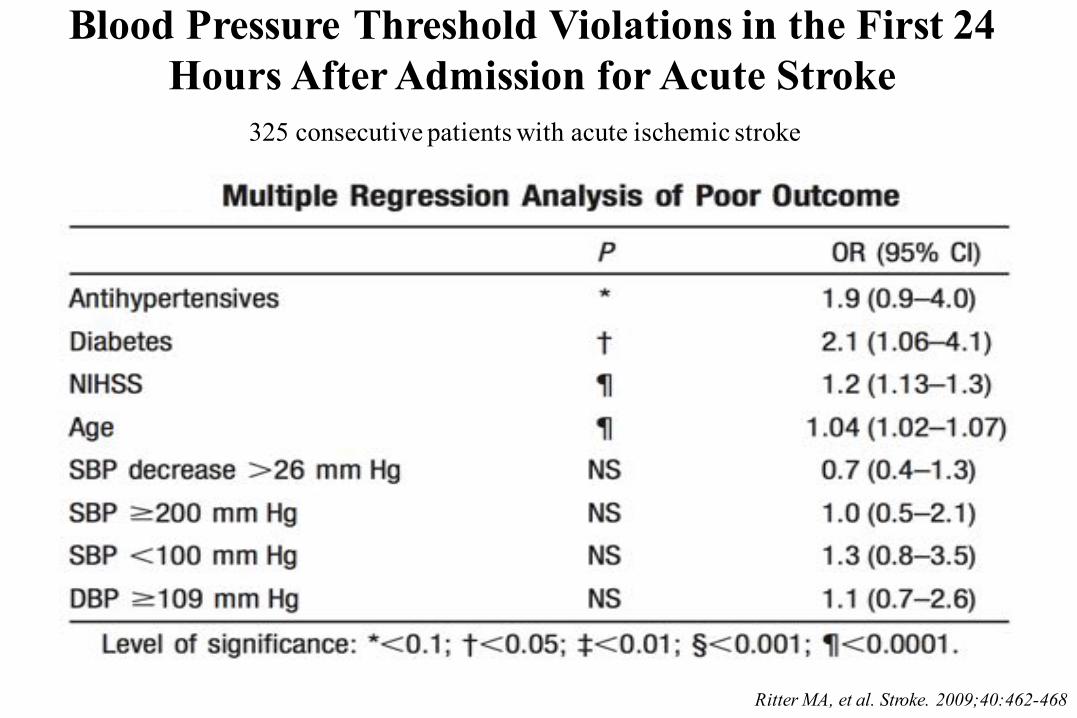
Blood Pressure Threshold Violations in the First 24 Hours After Admission for Acute Stroke
Ritter MA, et al. Stroke. 2009;40:462-468
325 consecutive patients with acute ischemic stroke
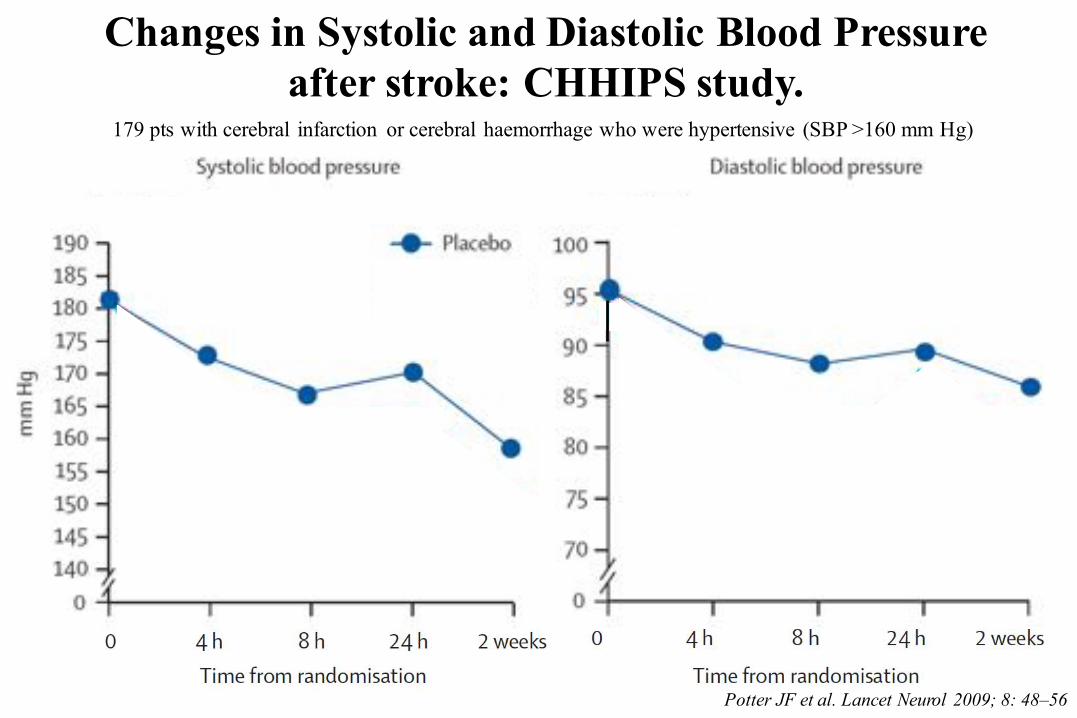
Changes in Systolic and Diastolic Blood Pressure after stroke: CHHIPS study.
Potter JF et al. Lancet Neurol 2009; 8: 48–56
179 pts with cerebral infarction or cerebral haemorrhage who were hypertensive (SBP >160 mm Hg)
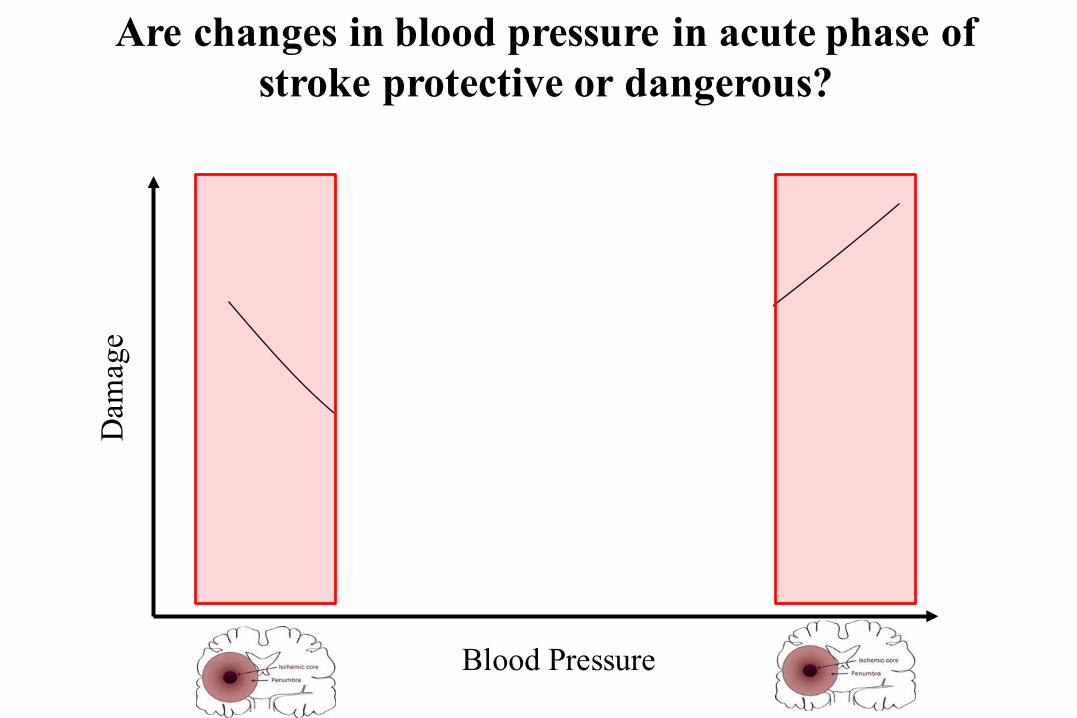
Are changes in blood pressure in acute phase of stroke protective or dangerous?
Blood Pressure
Dam
age
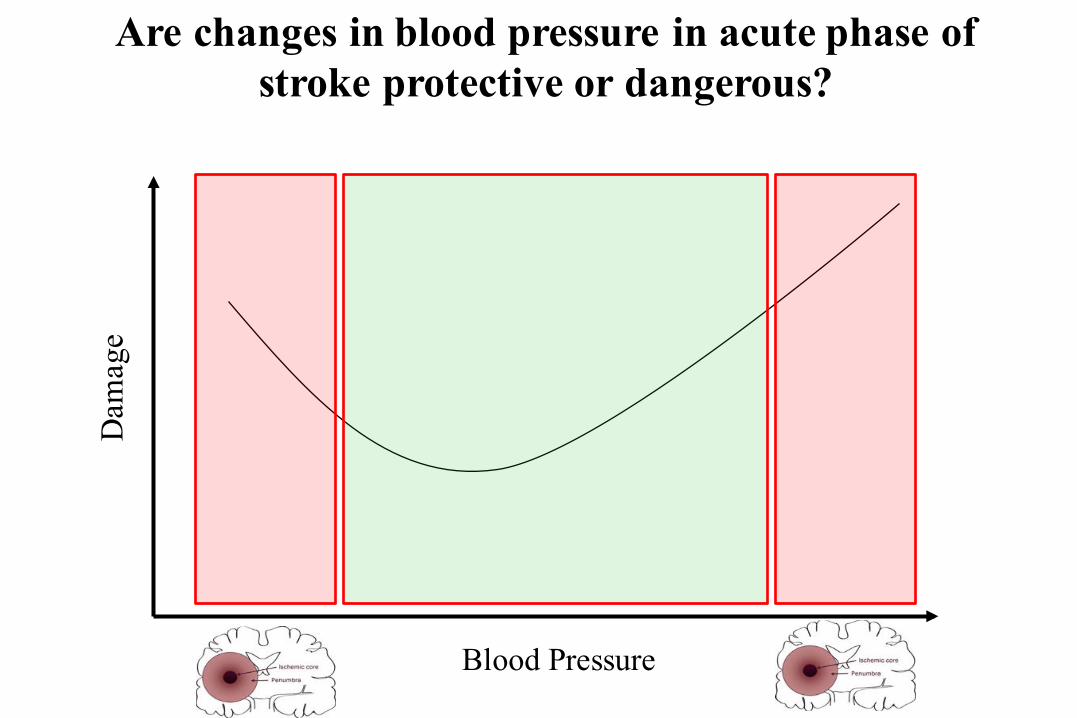
Are changes in blood pressure in acute phase of stroke protective or dangerous?
Blood Pressure
Dam
age
Are changes in blood pressure in acute phase of stroke protective or dangerous?
Blood Pressure
Dam
age
Are changes in blood pressure in acute phase of stroke protective or dangerous?
Blood Pressure
Dam
age
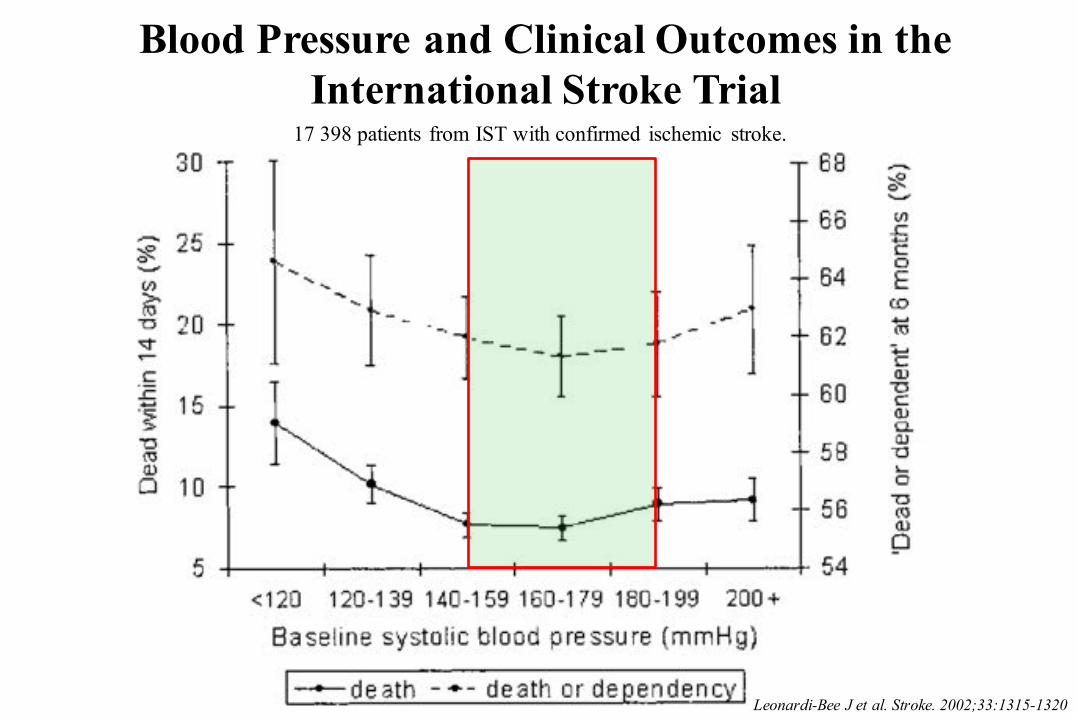
Blood Pressure and Clinical Outcomes in theInternational Stroke Trial
Leonardi-Bee J et al. Stroke. 2002;33:1315-1320
17 398 patients from IST with confirmed ischemic stroke.
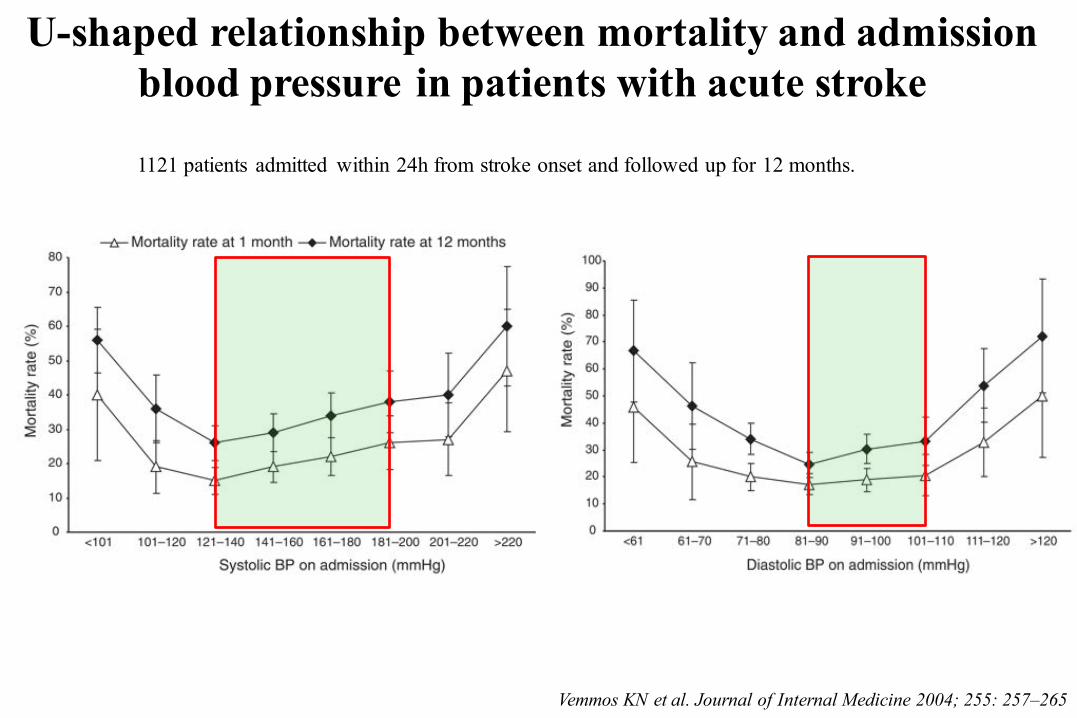
U-shaped relationship between mortality and admissionblood pressure in patients with acute stroke
Vemmos KN et al. Journal of Internal Medicine 2004; 255: 257–265
1121 patients admitted within 24h from stroke onset and followed up for 12 months.
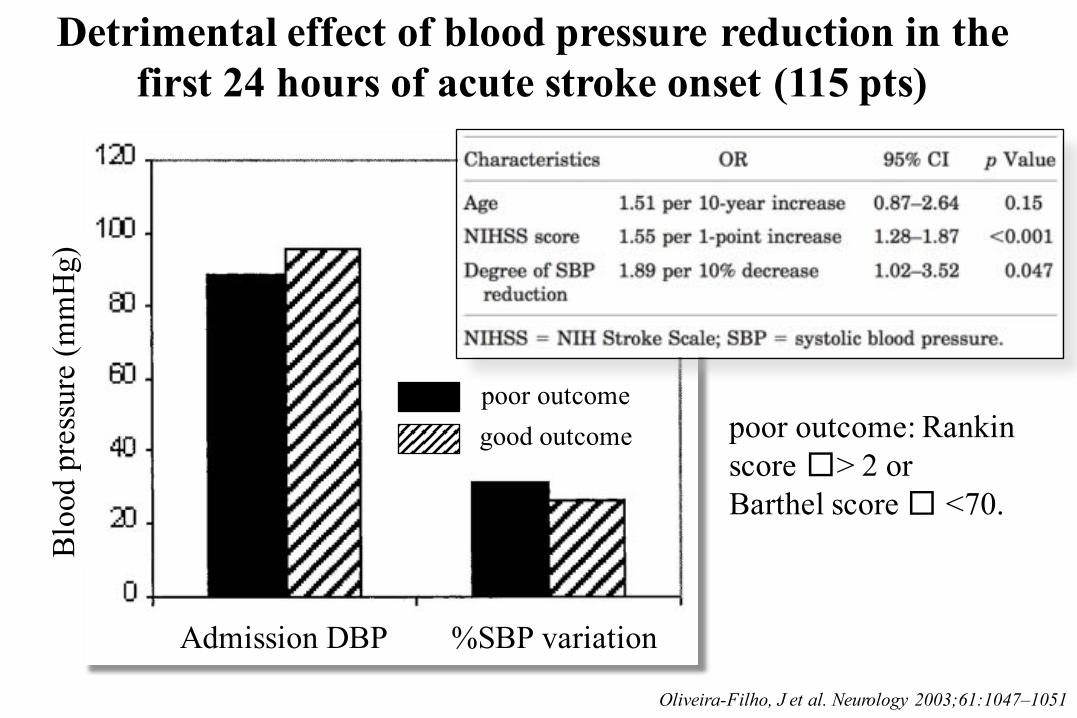
Detrimental effect of blood pressure reduction in the first 24 hours of acute stroke onset (115 pts)
Oliveira-Filho, J et al. Neurology 2003;61:1047–1051
Admission DBP %SBP variation
Blo
od p
ress
ure
(mm
Hg)
good outcomepoor outcome
poor outcome: Rankinscore �> 2 or Barthel score � <70.
Blood Pressure Threshold Violations in the First 24 Hours After Admission for Acute Stroke
Ritter MA, et al. Stroke. 2009;40:462-468
325 consecutive patients with acute ischemic stroke
I don’t know!
Are changes in blood pressure in acute phase of stroke protective or dangerous?
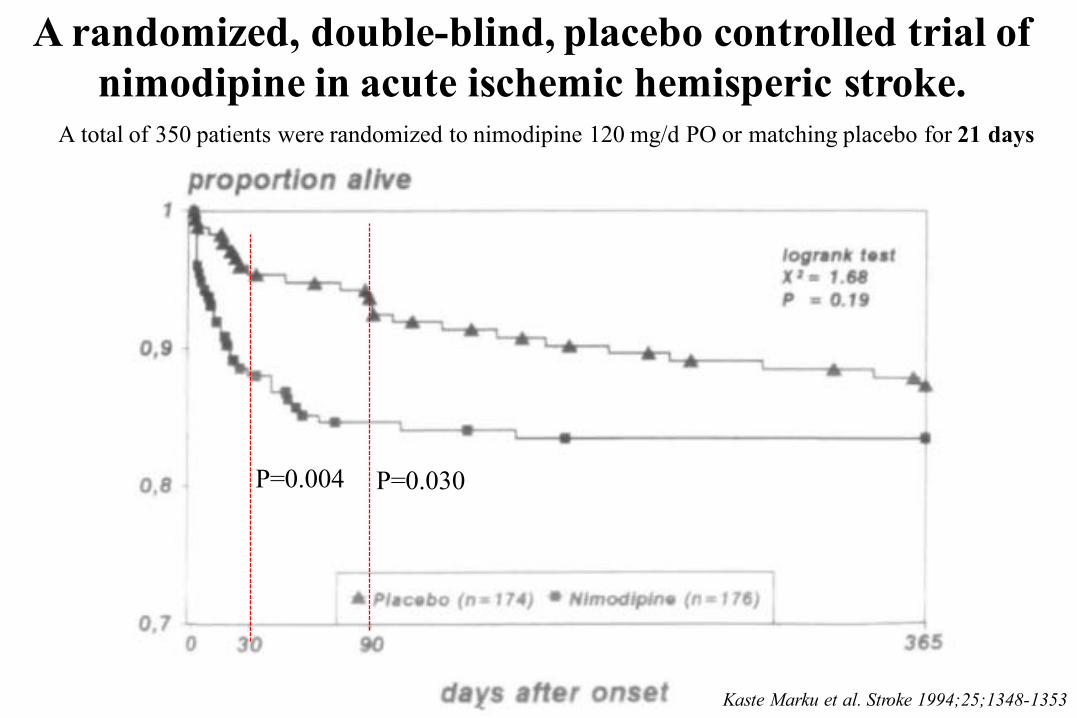
A randomized, double-blind, placebo controlled trial of nimodipine in acute ischemic hemisperic stroke.
Kaste Marku et al. Stroke 1994;25;1348-1353
P=0.004 P=0.030
A total of 350 patients were randomized to nimodipine 120 mg/d PO or matching placebo for 21 days
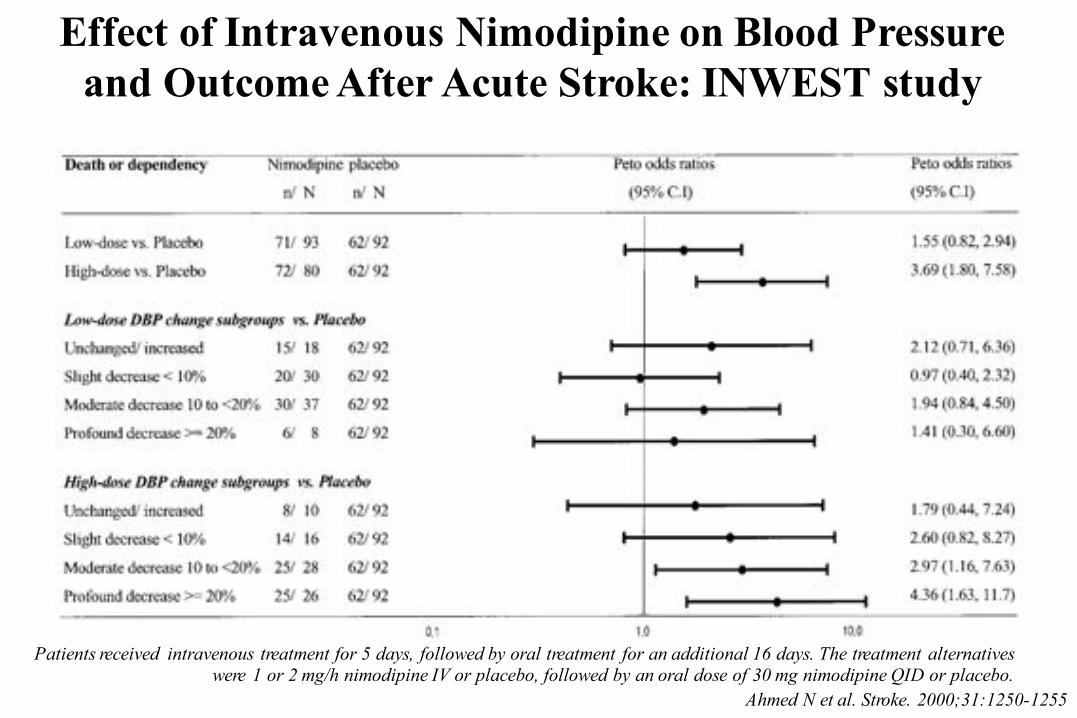
Effect of Intravenous Nimodipine on Blood Pressure and Outcome After Acute Stroke: INWEST study
Ahmed N et al. Stroke. 2000;31:1250-1255
Patients received intravenous treatment for 5 days, followed by oral treatment for an additional 16 days. The treatment alternativeswere 1 or 2 mg/h nimodipine IV or placebo, followed by an oral dose of 30 mg nimodipine QID or placebo.
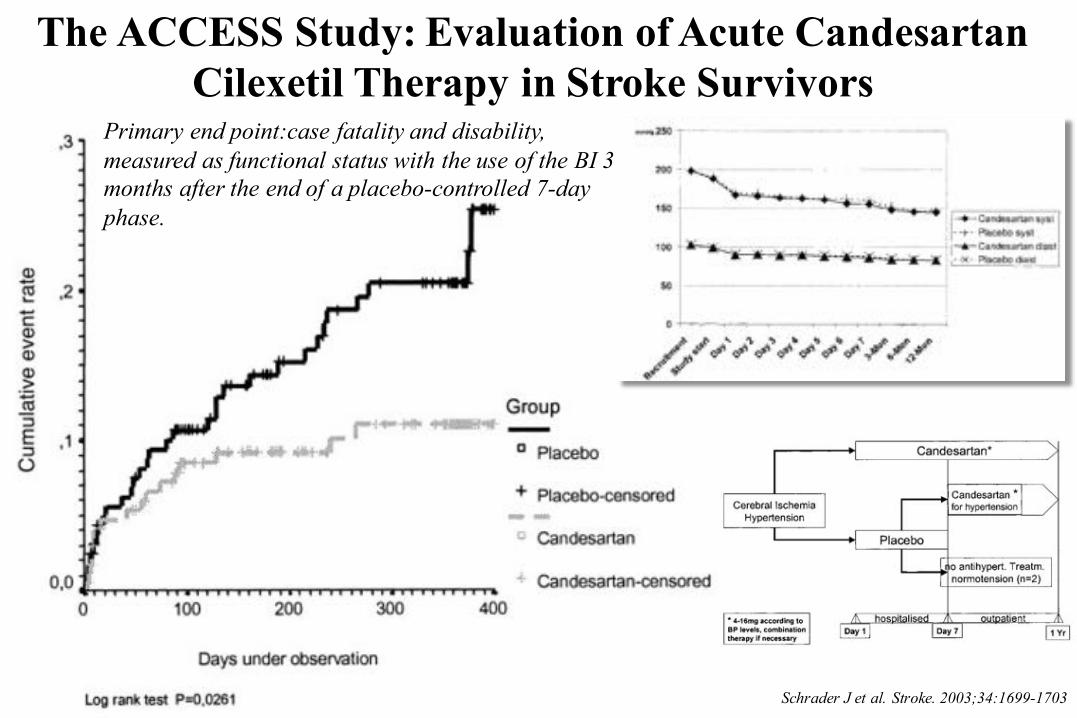
The ACCESS Study: Evaluation of Acute CandesartanCilexetil Therapy in Stroke Survivors
Schrader J et al. Stroke. 2003;34:1699-1703
Primary end point:case fatality and disability, measured as functional status with the use of the BI 3 months after the end of a placebo-controlled 7-day phase.
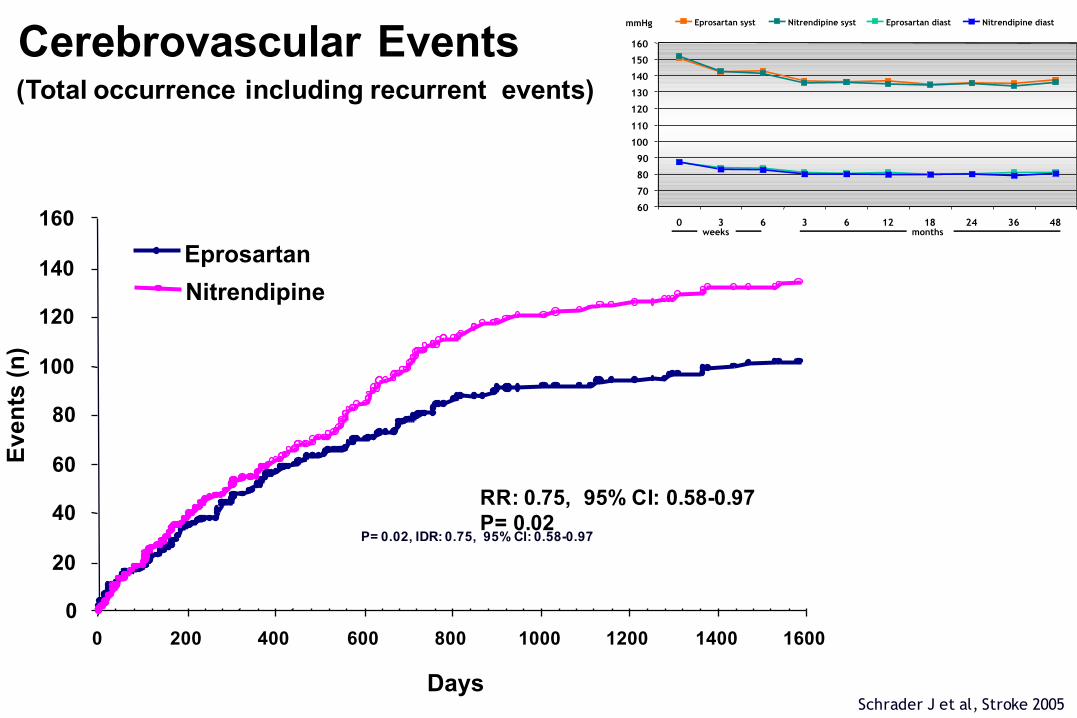
occurrence including recurrent vents
Schrader J et al, Stroke 2005
Cerebrovascular Events(Total occurrence including recurrent events)
P= 0.02, IDR: 0.75, 95% CI: 0.58-0.97
0
20
40
60
80
100
120
140
160
0 200 400 600 800 1000 1200 1400 1600
Days
Eve
nts
(n)
Eprosartan
Nitrendipine
RR: 0.75, 95% CI: 0.58-0.97P= 0.02
60 70 80 90
100 110 120 130 140 150 160
0 3 6 3 6 12 18 24 36 48
Eprosartan syst Nitrendipine syst Eprosartan diast Nitrendipine diast
months weeks
mmHg
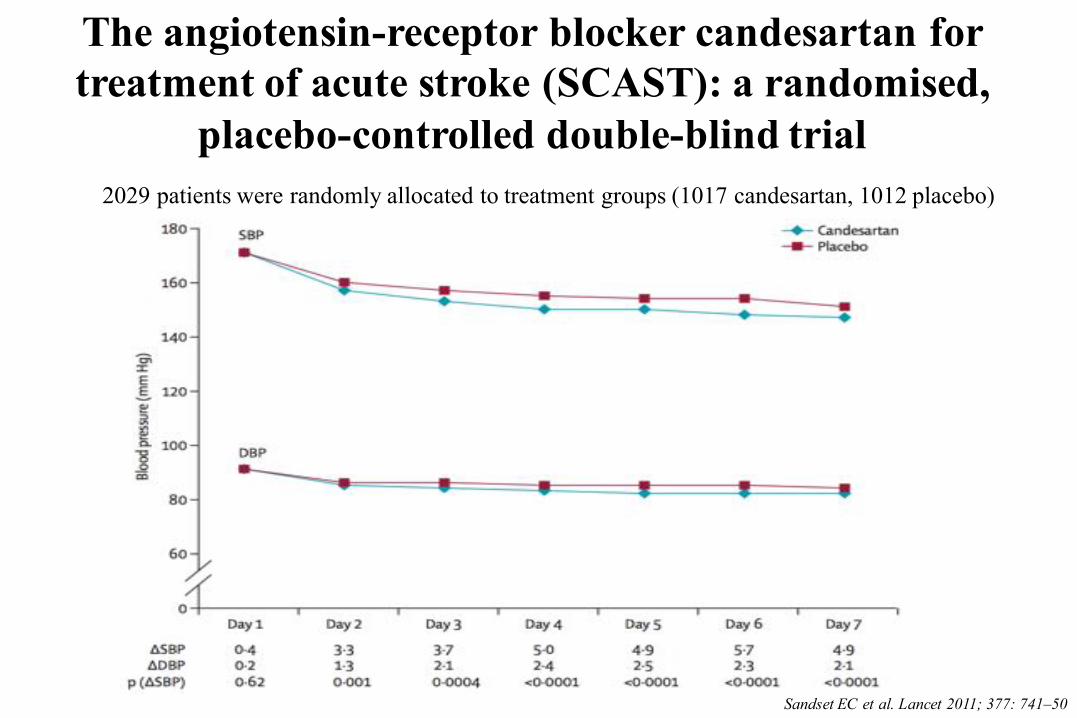
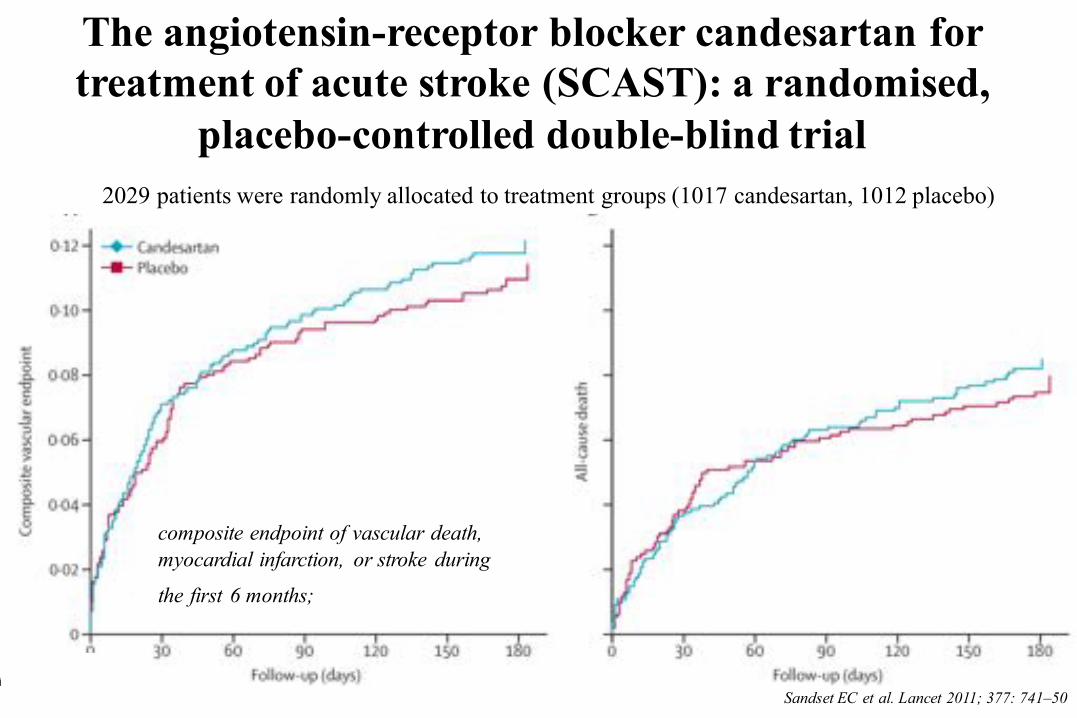
The angiotensin-receptor blocker candesartan for treatment of acute stroke (SCAST): a randomised,
placebo-controlled double-blind trial
Sandset EC et al. Lancet 2011; 377: 741–50
2029 patients were randomly allocated to treatment groups (1017 candesartan, 1012 placebo)
The angiotensin-receptor blocker candesartan for treatment of acute stroke (SCAST): a randomised,
placebo-controlled double-blind trial
Sandset EC et al. Lancet 2011; 377: 741–50
2029 patients were randomly allocated to treatment groups (1017 candesartan, 1012 placebo)
composite endpoint of vascular death, myocardial infarction, or stroke during
the first 6 months;
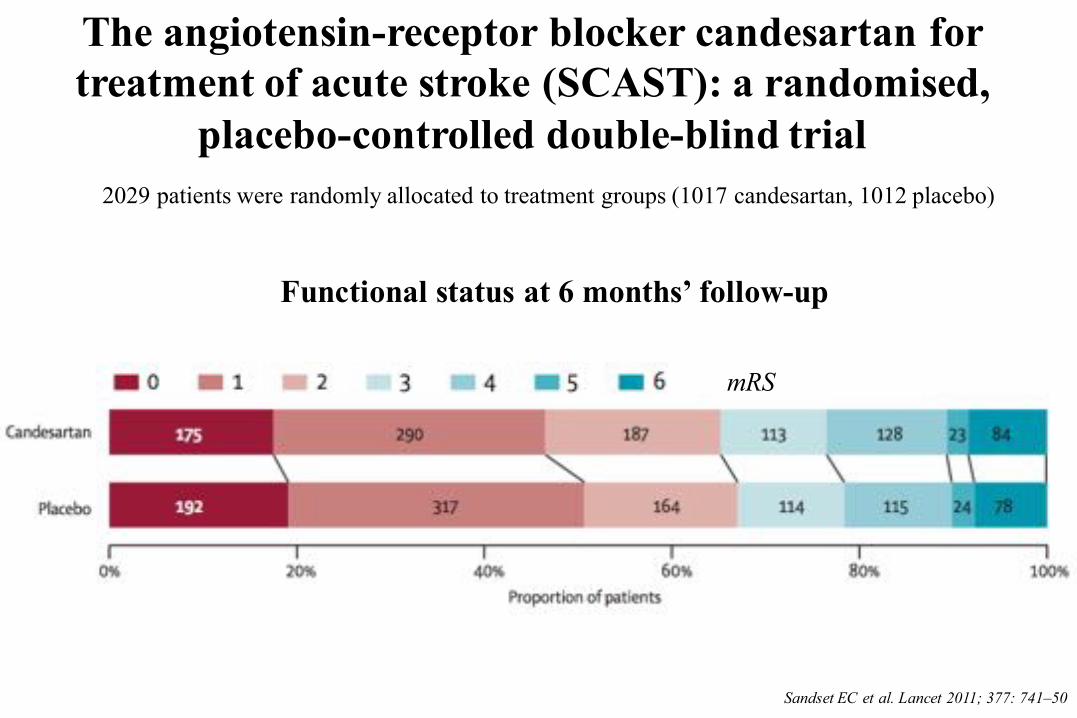
The angiotensin-receptor blocker candesartan for treatment of acute stroke (SCAST): a randomised,
placebo-controlled double-blind trial
Sandset EC et al. Lancet 2011; 377: 741–50
2029 patients were randomly allocated to treatment groups (1017 candesartan, 1012 placebo)
Functional status at 6 months’ follow-up
mRS
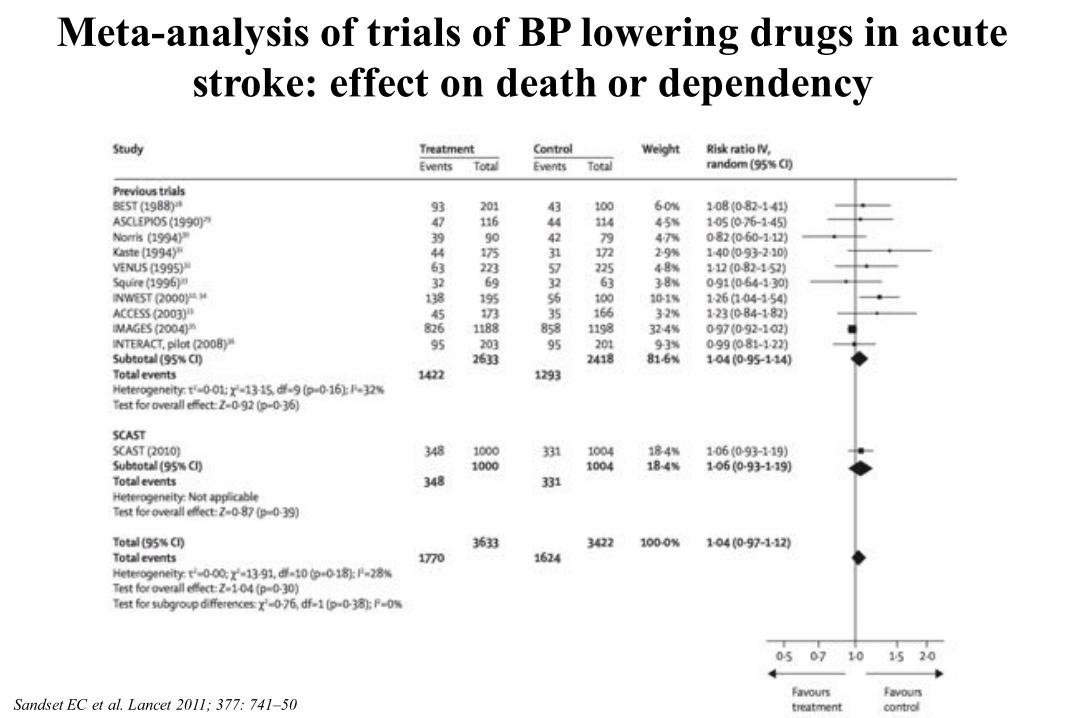
Meta-analysis of trials of BP lowering drugs in acute stroke: effect on death or dependency
Sandset EC et al. Lancet 2011; 377: 741–50
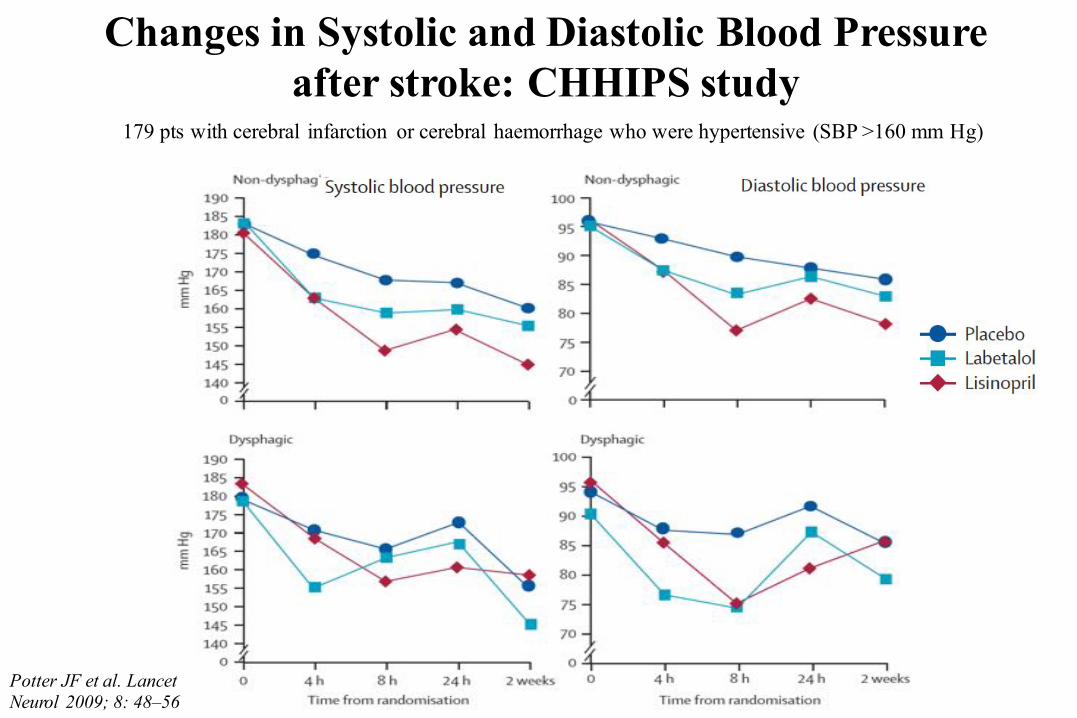
Changes in Systolic and Diastolic Blood Pressure after stroke: CHHIPS study
Potter JF et al. Lancet Neurol 2009; 8: 48–56
179 pts with cerebral infarction or cerebral haemorrhage who were hypertensive (SBP >160 mm Hg)
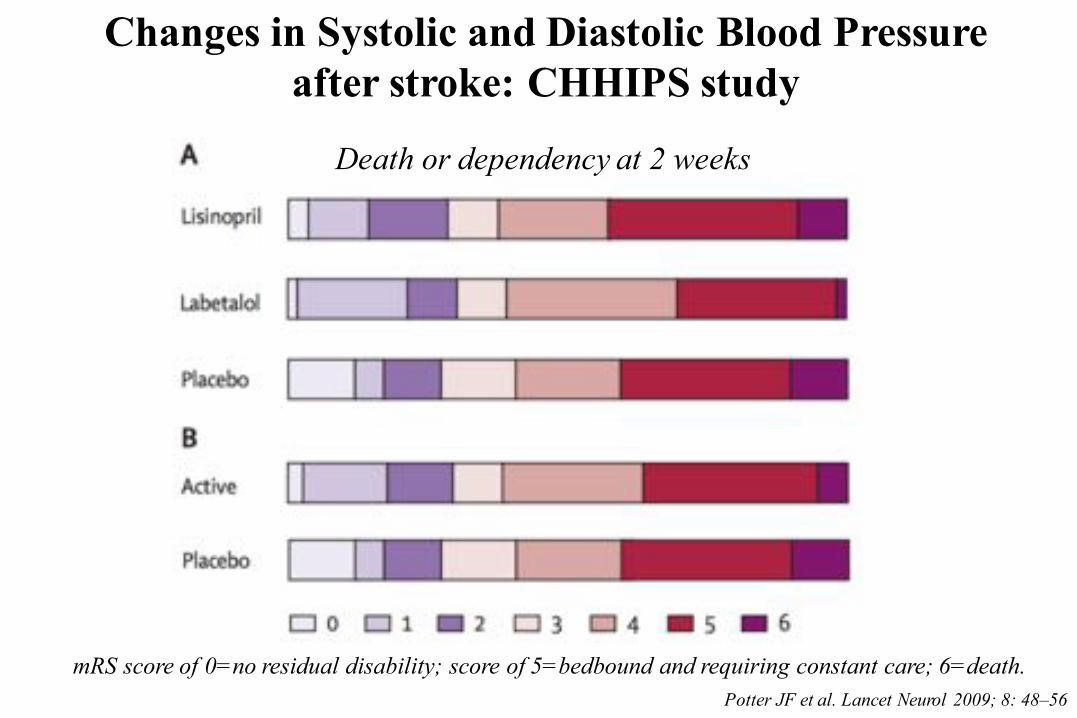
Changes in Systolic and Diastolic Blood Pressure after stroke: CHHIPS study
Potter JF et al. Lancet Neurol 2009; 8: 48–56
Death or dependency at 2 weeks
mRS score of 0=no residual disability; score of 5=bedbound and requiring constant care; 6=death.
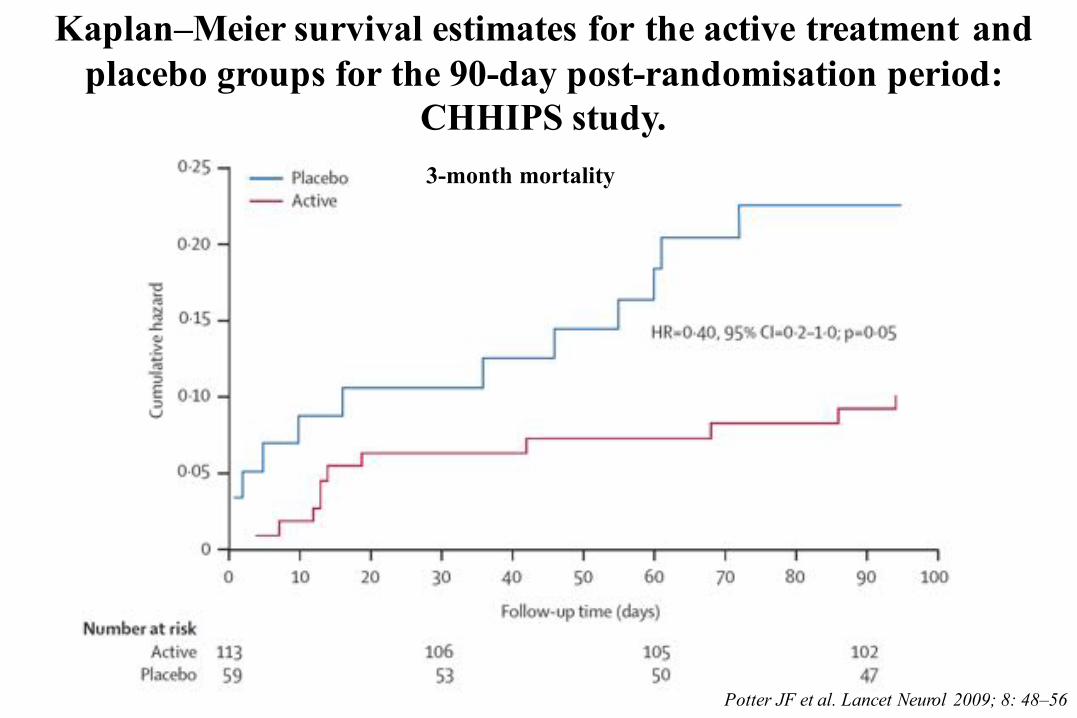
Kaplan–Meier survival estimates for the active treatment and placebo groups for the 90-day post-randomisation period:
CHHIPS study.
Potter JF et al. Lancet Neurol 2009; 8: 48–56
3-month mortality
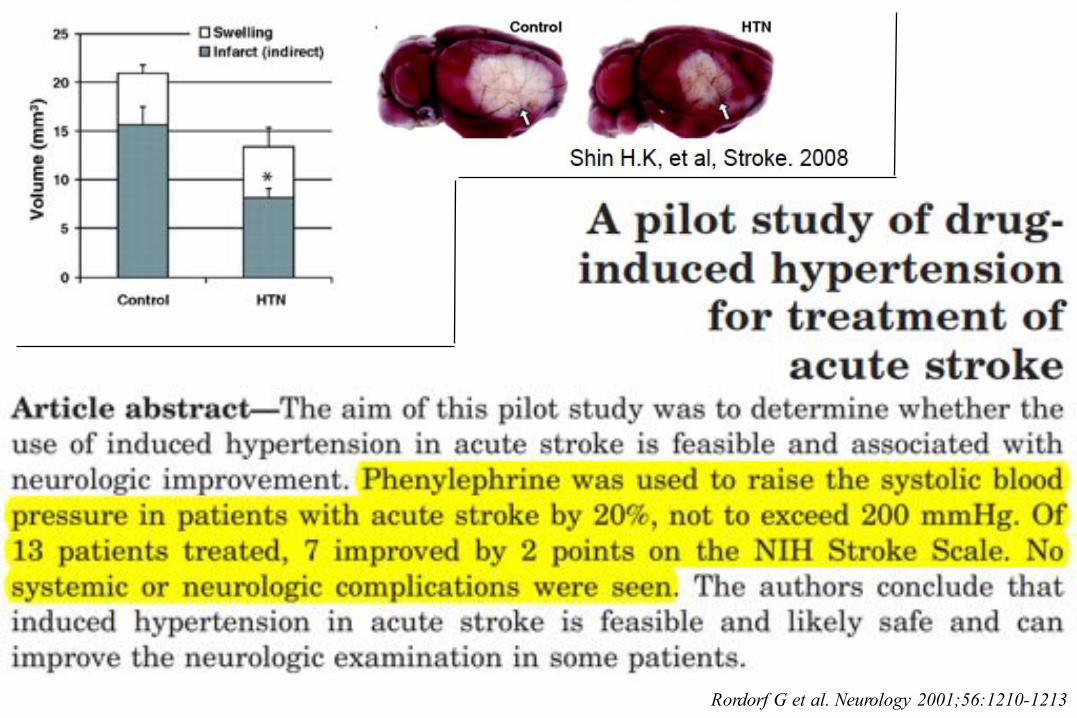
Rordorf G et al. Neurology 2001;56:1210-1213
…. It remains unclear what the risk-benefit ratio is for lowering or raising the blood pressure during acute ischemicstroke. Larger trials with well-defined criteria are needed.
Jauch EC et al. Stroke. 2013;44:870-947
In the meanwhile…?
….At this time, the previous recommendation not to lowerthe blood pressure during the initial 24 hours of acute ischemic stroke unless the blood pressure is >220/120 mm Hg or there is a concomitant specific medical conditionthat would benefit from blood pressure lowering remainsreasonable.
Jauch EC et al. Stroke. 2013;44:870-947
…. When BP management is indicated for a specific medicalcondition in the setting of concurrent acute cerebralischemia, an optimal approach has not been determined, and at present, BP targets are based on best clinical judgment. A reasonable estimate might be to initially lower the SBP by 15% and monitor for neurological deterioration relatedto the pressure lowering. Jauch EC et al. Stroke. 2013;44:870-947
Patients who have elevated blood pressure and are otherwiseeligible for treatment with intravenous rtPA should havetheir blood pressure carefully lowered so that their systolicblood pressure is <185 mm Hg and their diastolic bloodpressure is <110 mm Hg before fibrinolytic therapy isinitiated.
Jauch EC et al. Stroke. 2013;44:870-947
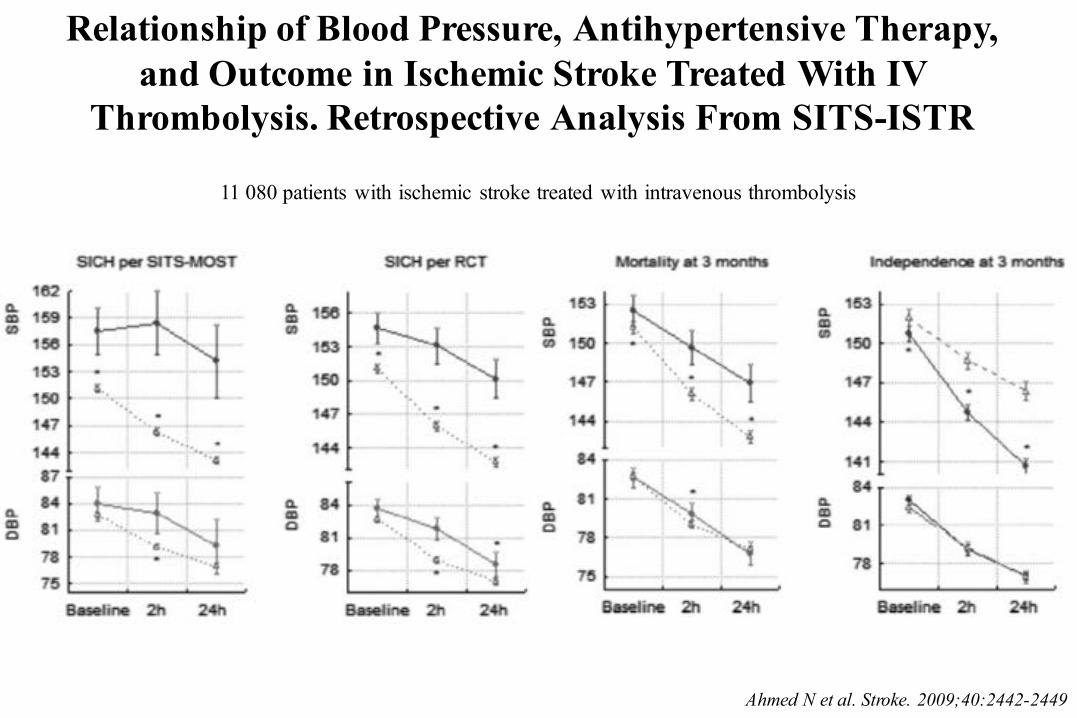
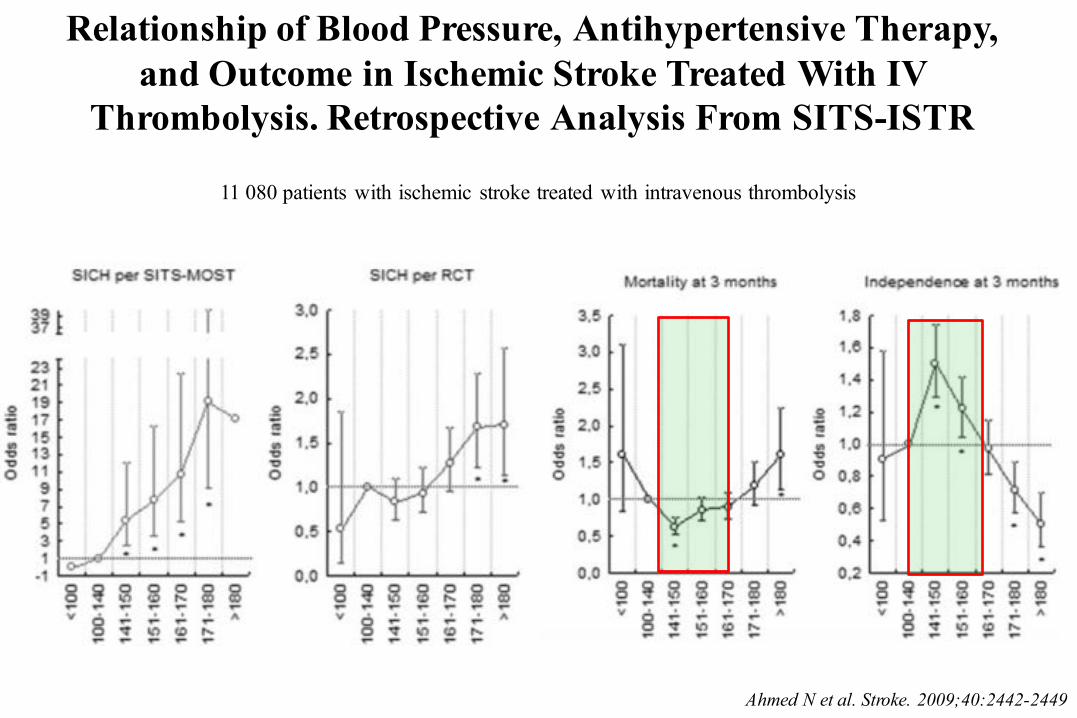
Relationship of Blood Pressure, Antihypertensive Therapy,and Outcome in Ischemic Stroke Treated With IV
Thrombolysis. Retrospective Analysis From SITS-ISTR
Ahmed N et al. Stroke. 2009;40:2442-2449
11 080 patients with ischemic stroke treated with intravenous thrombolysis
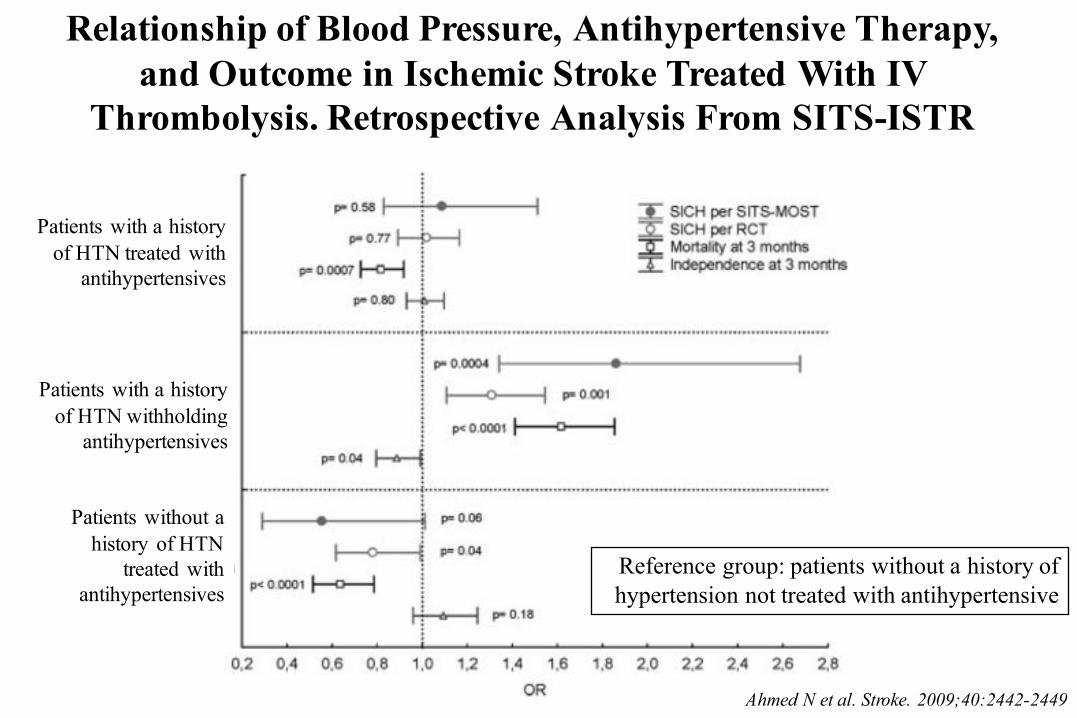
Relationship of Blood Pressure, Antihypertensive Therapy,and Outcome in Ischemic Stroke Treated With IV
Thrombolysis. Retrospective Analysis From SITS-ISTR
Ahmed N et al. Stroke. 2009;40:2442-2449
11 080 patients with ischemic stroke treated with intravenous thrombolysis
Relationship of Blood Pressure, Antihypertensive Therapy,and Outcome in Ischemic Stroke Treated With IV
Thrombolysis. Retrospective Analysis From SITS-ISTR
Ahmed N et al. Stroke. 2009;40:2442-2449
Patients with a historyof HTN treated with
antihypertensives
Patients with a historyof HTN withholding
antihypertensives
Patients without a history of HTN
treated withantihypertensives
Reference group: patients without a history of hypertension not treated with antihypertensive
If medications are given to lower blood pressure, the clinician should be sure that the blood pressure is stabilizedat the lower level before beginning treatment with intravenous rtPA and maintained below 180/105 mm Hg for at least the first 24 hours after intravenous rtPAtreatment.
Jauch EC et al. Stroke. 2013;44:870-947
Cimitero Acattolico, Roma
jamanetwork.com
Available at jama.com and mobile.jamanetwork.com
J He and coauthors for the CATIS Investigators
Effects of Immediate Blood Pressure Reduction on Death and Major Disability in Patients With Acute Ischemic Stroke: The CATIS Randomized Clinical Trial
Published online November 17, 2013
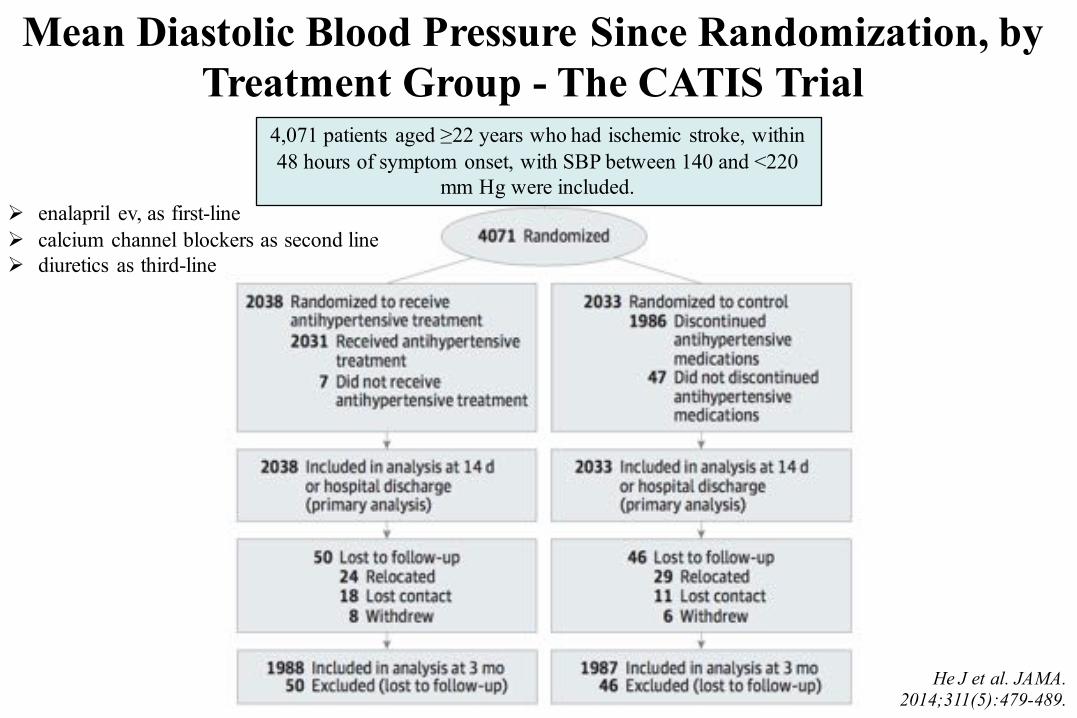
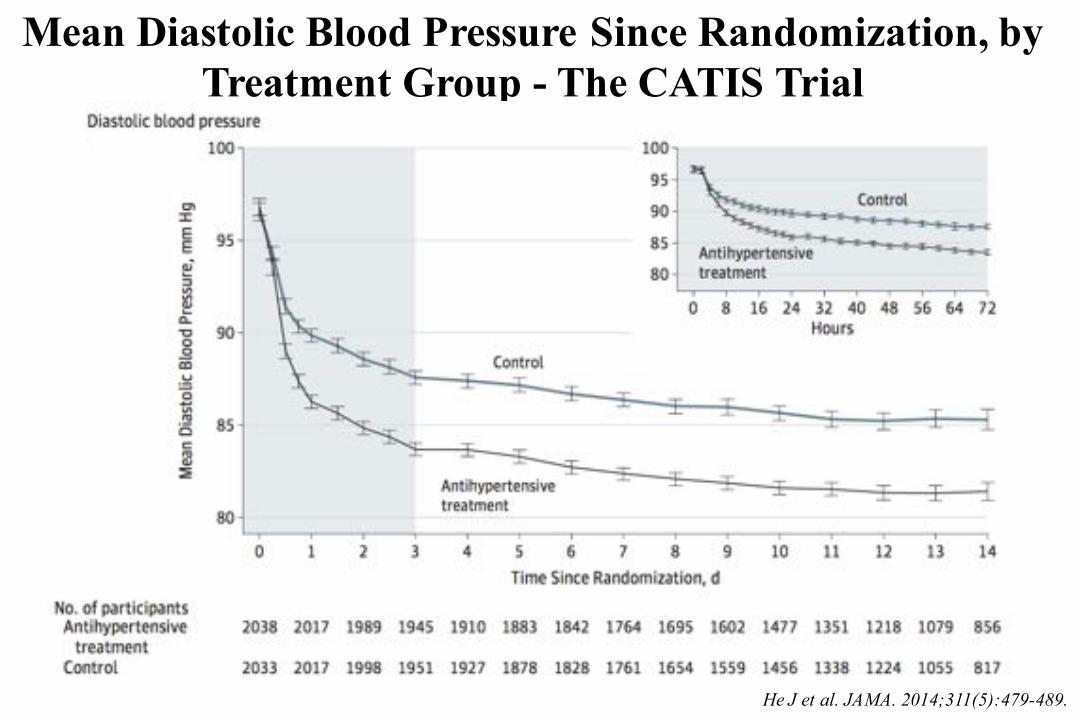
Mean Diastolic Blood Pressure Since Randomization, by Treatment Group - The CATIS Trial
He J et al. JAMA. 2014;311(5):479-489.
Ø enalapril ev, as first-lineØ calcium channel blockers as second lineØ diuretics as third-line
4,071 patients aged ≥22 years who had ischemic stroke, within48 hours of symptom onset, with SBP between 140 and <220
mm Hg were included.
Intervention
²Antihypertensive treatment ØLowering systolic BP by 10-25% within the first
24 hours after randomizationØAchieving a systolic BP <140 and diastolic BP
<90 mm Hg within 7 days, and maintaining this level of BP control during the remainder of a patient’s hospitalization
²Control ØDiscontinuing all home antihypertensive
medicationsHe J et al. JAMA. 2014;311(5):479-489.
He J et al. JAMA. 2014;311(5):479-489.
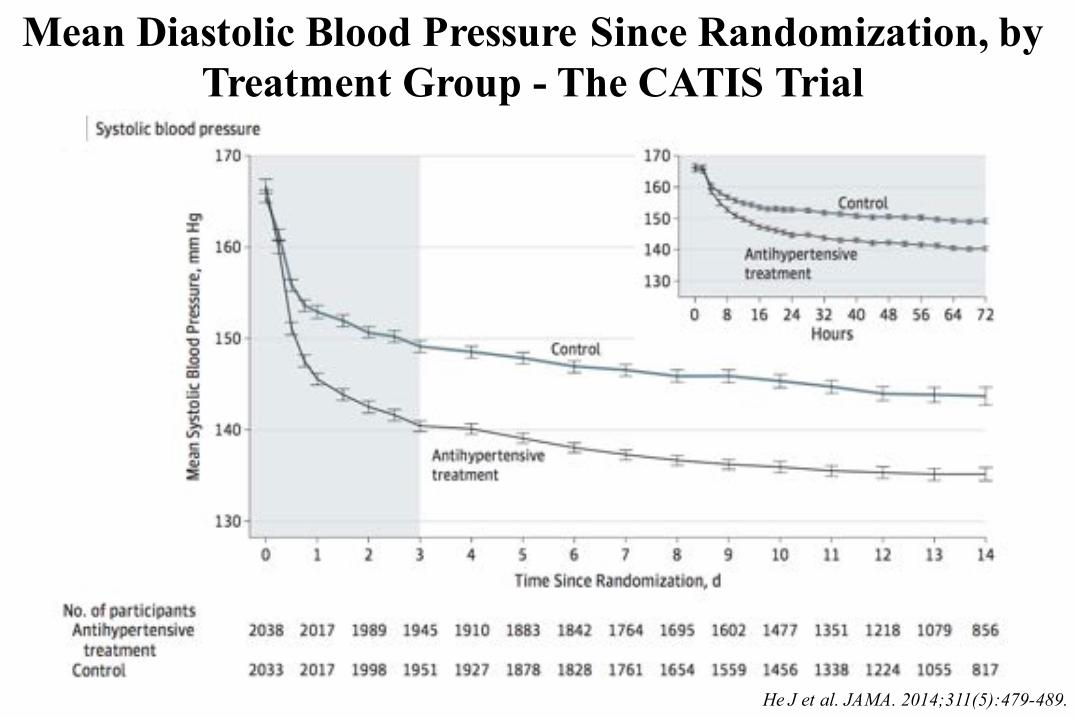
Mean Diastolic Blood Pressure Since Randomization, by Treatment Group - The CATIS Trial
Mean Diastolic Blood Pressure Since Randomization, by Treatment Group - The CATIS Trial
He J et al. JAMA. 2014;311(5):479-489.
He J et al. JAMA. 2014;311(5):479-489.
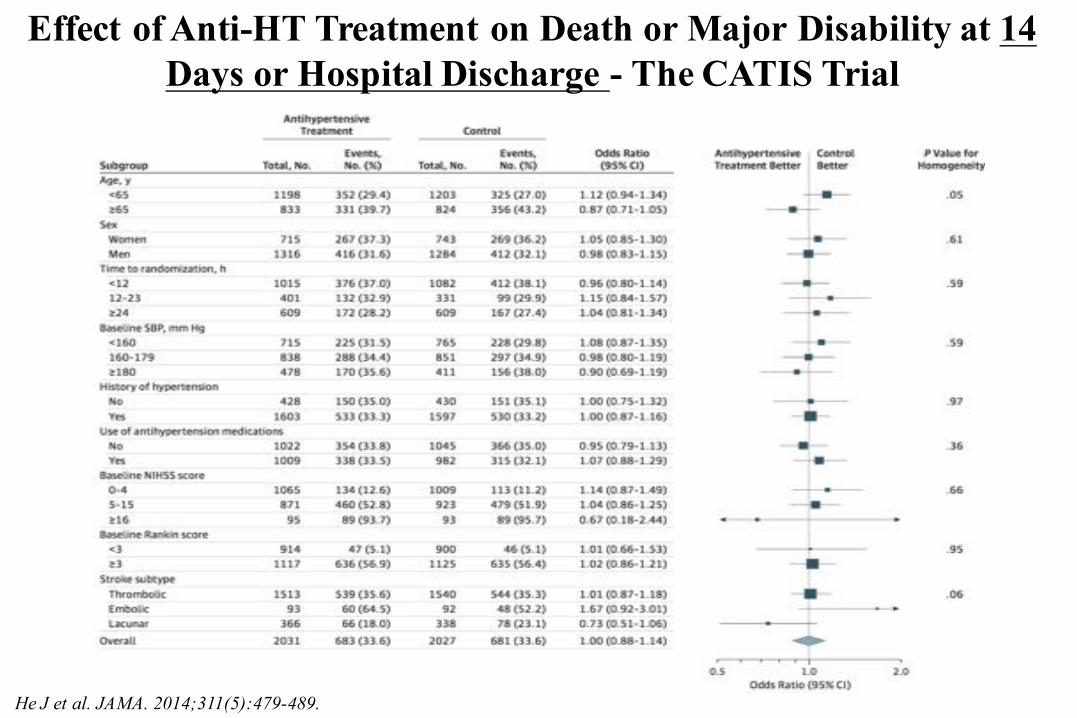
Effect of Anti-HT Treatment on Death or Major Disability at 14 Days or Hospital Discharge - The CATIS Trial
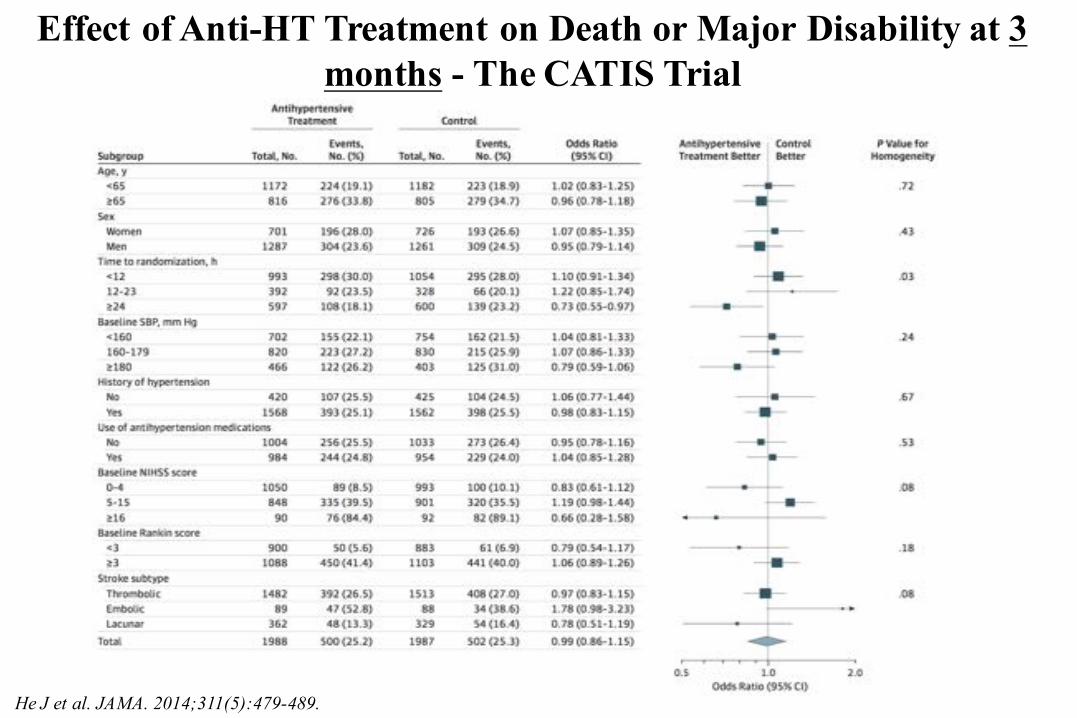
Effect of Anti-HT Treatment on Death or Major Disability at 3 months - The CATIS Trial
He J et al. JAMA. 2014;311(5):479-489.
Limitations
²Patients treated with intravenous thrombolytic therapy (i.e., intravenous rtPA) at baseline were excluded from this trial.
²Patients included in this trial had a lower median NIHSS of 4 (interquartile range 2-8) compared with 7 (2-10) in Chinese national registry data.
²This trial was conducted exclusively in Chinese patients.
He J et al. JAMA. 2014;311(5):479-489.
Conclusion
²Among patients with acute ischemic stroke, BP reduction with antihypertensive medications compared with the absence of antihypertensive medications did not reduce death and major disability at 14 days or hospital discharge.
²These findings suggest that unless a patient’s BP ≥220/120 mmHg, the decision to lower BP with antihypertensive treatment in patients with acute ischemic stroke should be based on individual clinical judgment.
He J et al. JAMA. 2014;311(5):479-489.
AfterBefore
Acute phase
Hypertension and Brain: dangerous relationships…
the day…after
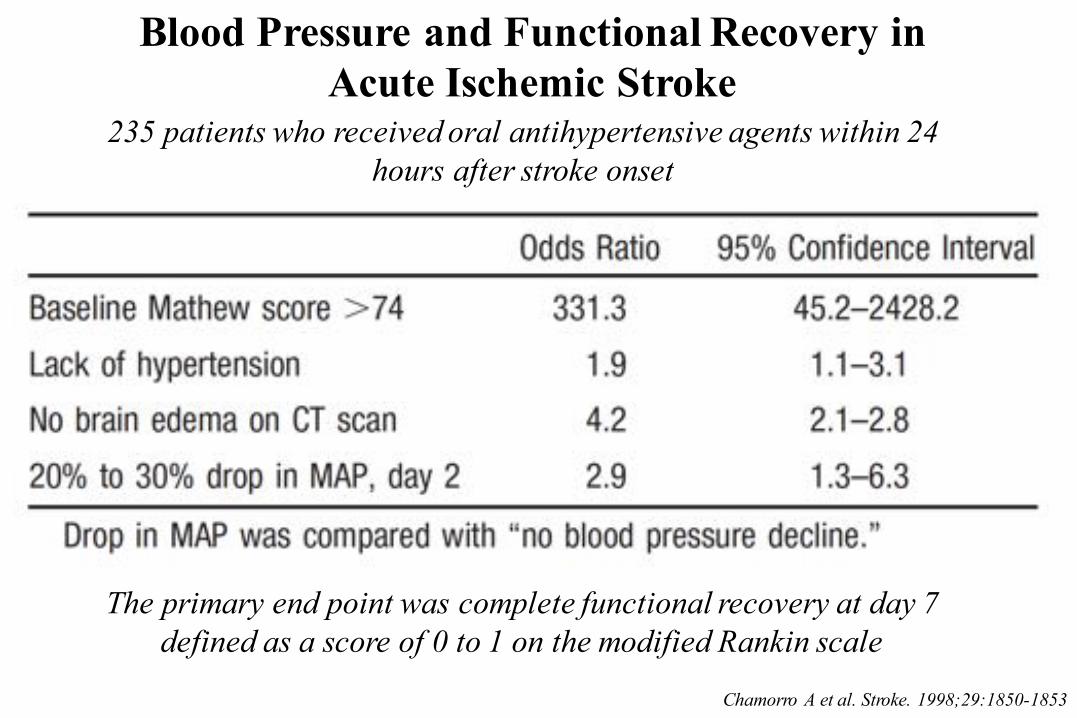
Blood Pressure and Functional Recovery inAcute Ischemic Stroke
Chamorro A et al. Stroke. 1998;29:1850-1853
235 patients who received oral antihypertensive agents within 24 hours after stroke onset
The primary end point was complete functional recovery at day 7 defined as a score of 0 to 1 on the modified Rankin scale
Ø Up to 50% of patients with acute stroke are taking antihypertensivedrugs on hospital admission. However, whether such treatment shouldbe continued during the immediate post-stroke period is unclear. Wetherefore aimed to assess the efficacy and safety of continuing or stopping pre-existing antihypertensive drugs in patients who hadrecently had a stroke.
Ø 763 patients were assigned to continue (n=379) or stop (n=384) pre-existing antihypertensive drugs.
Robinson Rg et al. Lancet Neurol 2010; 9: 767–75
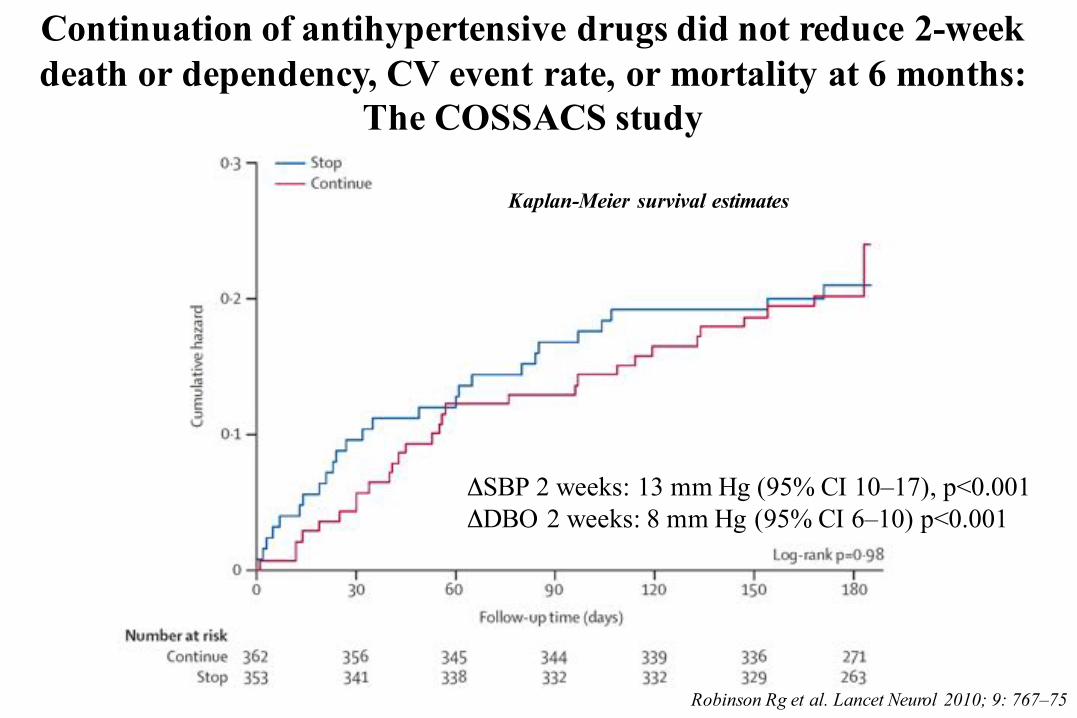
Continuation of antihypertensive drugs did not reduce 2-week death or dependency, CV event rate, or mortality at 6 months:
The COSSACS study
Robinson Rg et al. Lancet Neurol 2010; 9: 767–75
Kaplan-Meier survival estimates
ΔSBP 2 weeks: 13 mm Hg (95% CI 10–17), p<0.001 ΔDBO 2 weeks: 8 mm Hg (95% CI 6–10) p<0.001
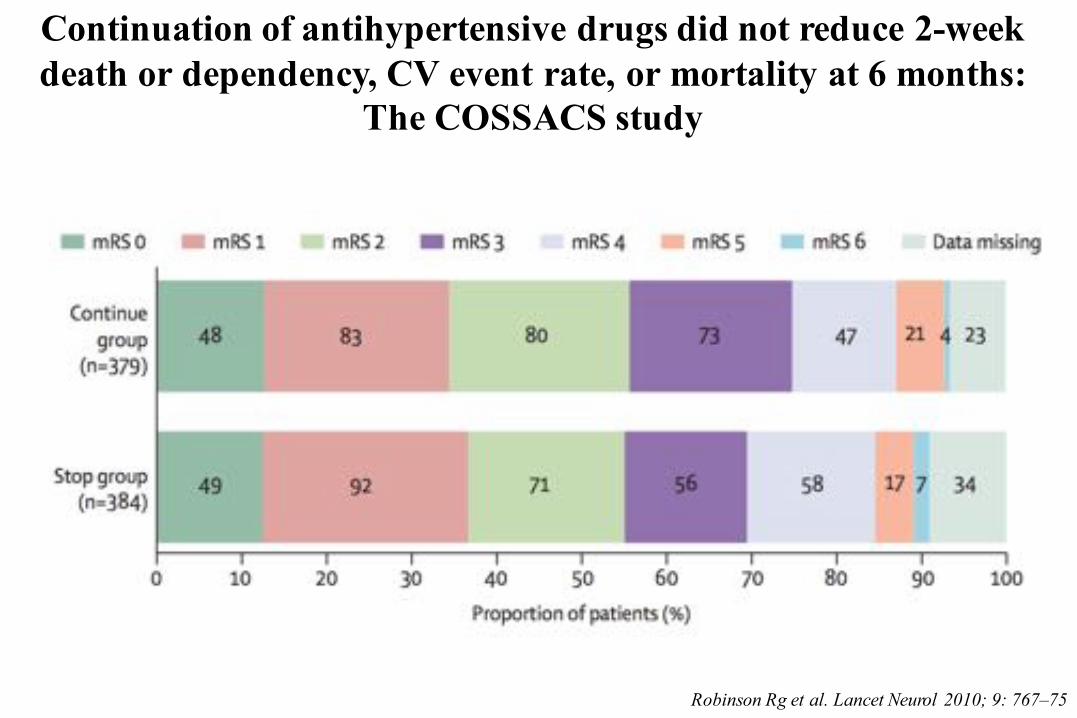
Continuation of antihypertensive drugs did not reduce 2-week death or dependency, CV event rate, or mortality at 6 months:
The COSSACS study
Robinson Rg et al. Lancet Neurol 2010; 9: 767–75
…. Evidence from one clinical trial indicates that initiationof antihypertensive therapy within 24 hours of stroke isrelatively safe. Restarting antihypertensive medications isreasonable after the first 24 hours for patients who havepreexisting hypertension and are neurologically stable unlessa specific contraindication to restarting treatment is known…
Jauch EC et al. Stroke. 2013;44:870-947
…. In exceptional cases with systemic hypotensionproducing neurological sequelae, a physician may prescribevasopressors to improve cerebral blood flow. If drug-induced hypertension is used, close neurological and cardiac monitoring is recommended…
Jauch EC et al. Stroke. 2013;44:870-947
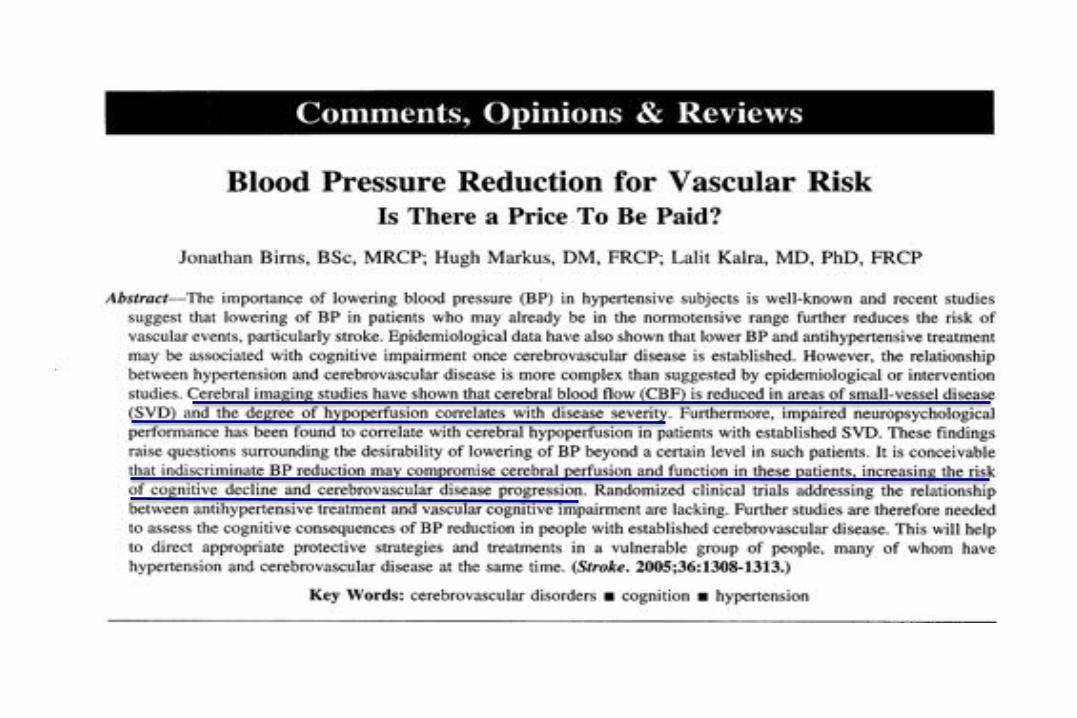
Normal cerebral autoregulation curve with its lower and upper limits of MAP, and a narrowed range with a steeper curve.
Bood
flow
0 50 100 150 200 Mean blood pressure (mmHg)
Normal
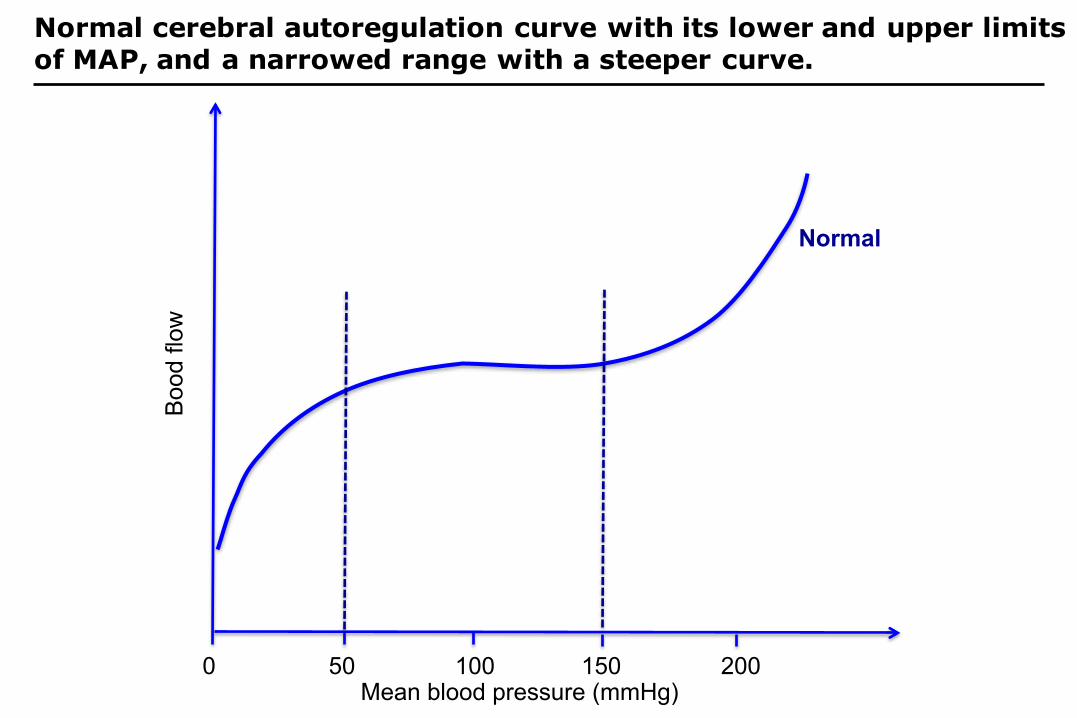
Normal cerebral autoregulation curve with its lower and upper limits of MAP, and a narrowed range with a steeper curve.
Bood
flow
0 50 100 150 200 Mean blood pressure (mmHg)
Normal
Narrowed: hypertension, hypotension, diabetes, vascular
disease, stroke, smoking
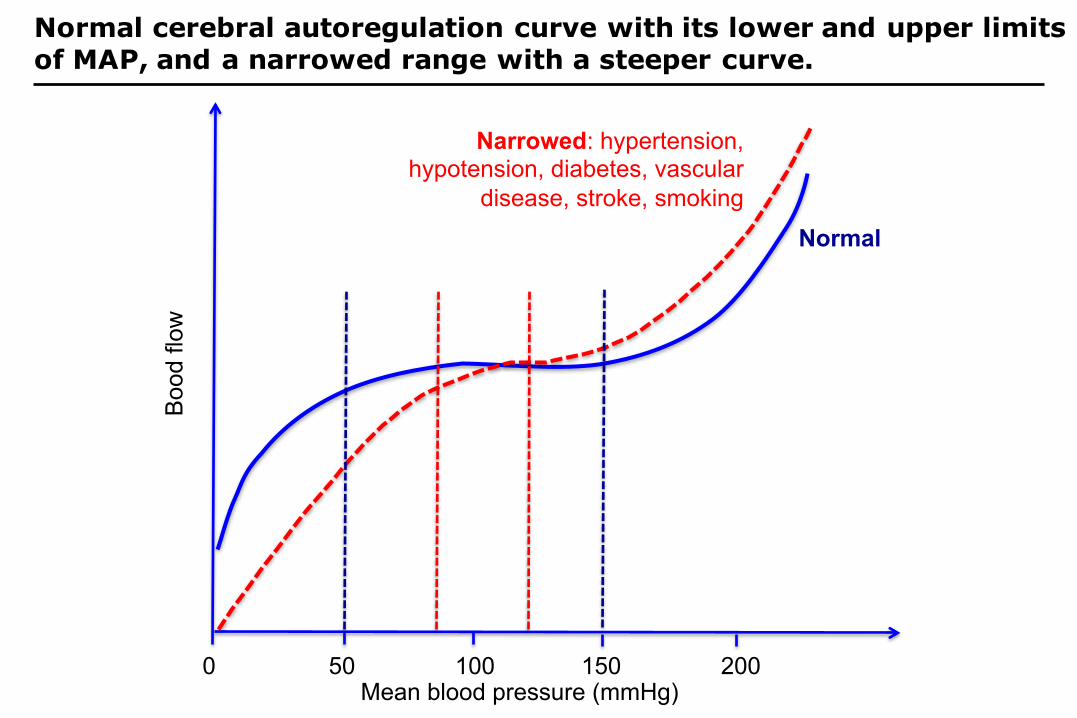
A Randomized Trial of Intensive versus Standard Blood-Pressure Control: The SPRINT Research Group
N Eng J Med 2015
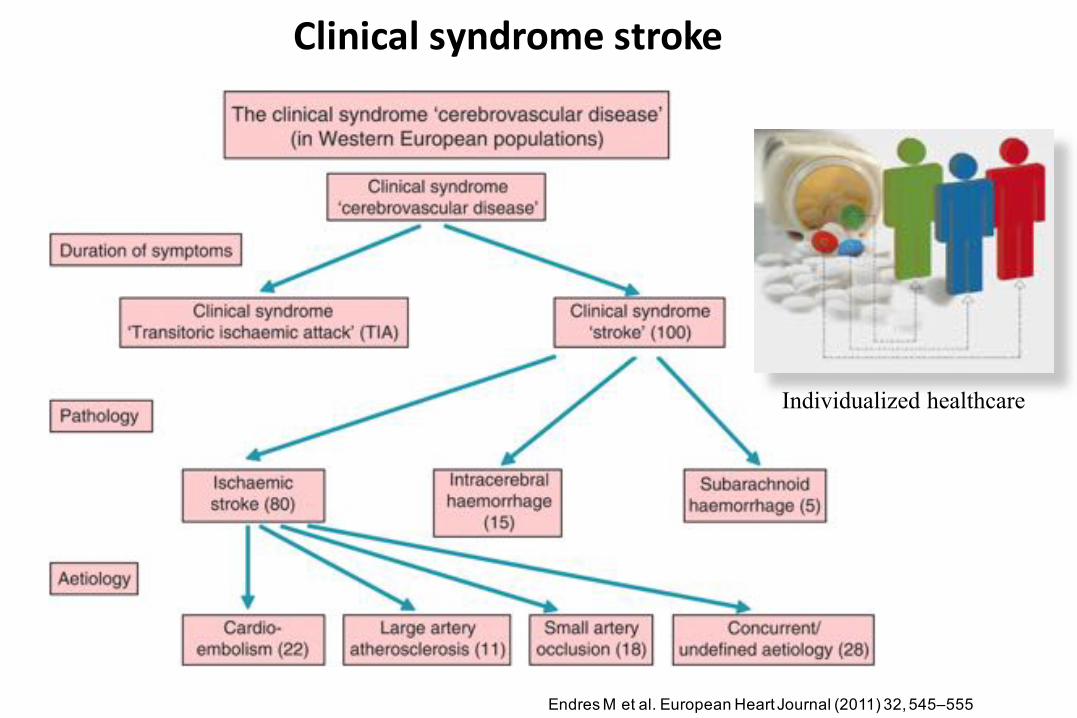
Clinical syndrome stroke
Endres M et al. European Heart Journal (2011) 32, 545–555
Individualized healthcare





























