Embed Size (px)
Citation preview

Appraisal and reappraisal of cardiac therapy Edited by Arthur C. DeGraff and Julian Frieden
Electrophysiology and pharmacology of cardiac arrhythmias. VII. Cardiac effects of quinidine
and procaine amide. 6.
Brian F. Hoffman, M.D. Michael R. Rosen, M.D.* Andrew L. Wit, Ph.D.* New York, N. Y.
Effects on electrical activity of cardiac cells
Quinidine and procaine amide have quite simi- lar effects on the transmembrane potentials and electrical activity of cells from all parts of the mammalian heart. Most of these effects are exerted directly by the drugs but some are due to drug-induced modification of responses to auto- nomic mediators. For the most part drug effects have been described for normal cardiac cells and only recently has systematic investigation of drug actions on depressed or diseased fibers been initiated. The information resulting from these latter studies will be essential for a correct under- standing of relationships between drug effects and antiarrhythmic activity. Because of their greater suitability for study by intracellular microelectrodes, cardiac Purkinje fibers have been used for the majority of investigations.
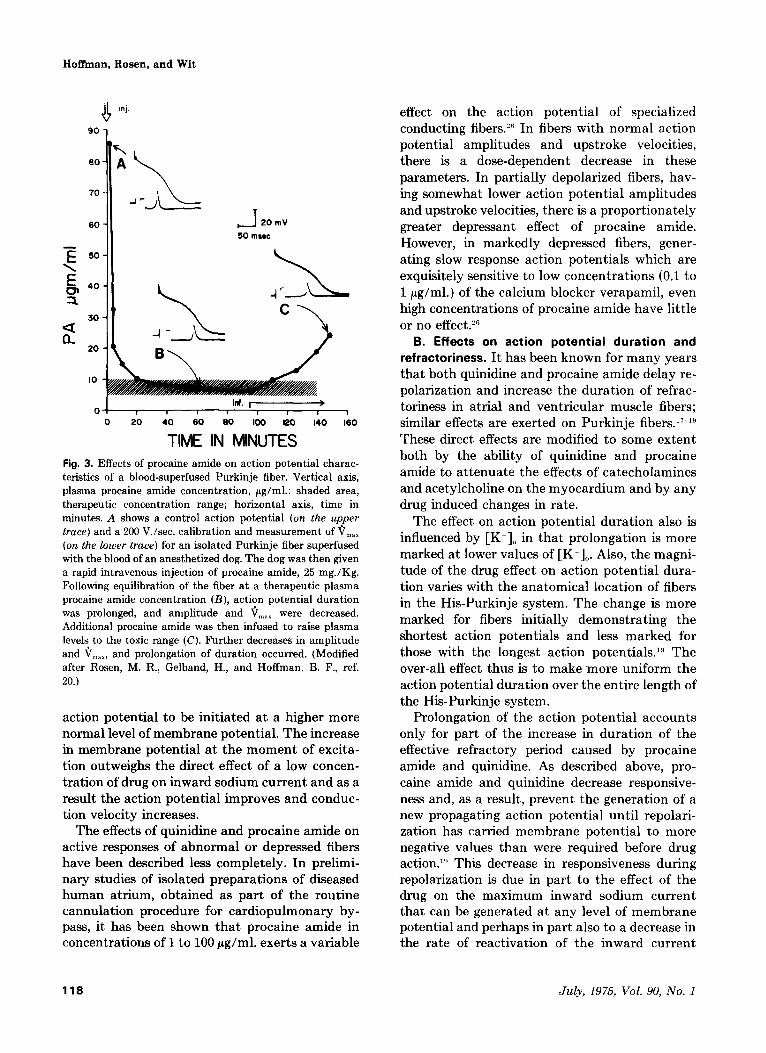
A. Effects on threshold and action potential upstroke. Quinidine and procaine amide, like other drugs exerting a local anesthetic action depress the responsiveness of cardiac cells.“.‘* Both drugs, in a dose dependent manner, decrease the maximum rate of depolarization and the amplitude of the action potential upstroke recorded from atria1 and ventricular muscle fiber and Purkinje fibers (Fig. 3). This effect is seen at
From the Department of Pharmacology, Columbia University College of Physicians and Surgeons, New York, N. Y.
Certain of the studies referred to in this paper were supported by United States Public Health Service grants HL-12738 and HL-08508.
Received for publication Feb. 24, 1975.
Reprint requests to: Michael R. Rosen, M.D., Department of Pharma- cology, Columbia University, College of Physicians and Surgeons, 630 W. 168 St., New York, N. Y. 10032.
*Drs. Rosen and Wit are Senior Investigators of the New York Heart Association.
July, 1975, Vol. 90, No. 1,pp. 117-122
concentrations which do not decrease the resting potential or maximum diastolic potential, i.e., 30 pg/ml. in Tyrode solution or 5 to 10 pg/ml. in blood.19.2” The decrease in responsiveness thus appears to result from a direct effect on the mechanism controlling the voltage and time- dependent increase in a sodium conductance.‘i.2* Most investigators have found that, for a given concentration of drug, the decrease in responsive- ness is increased by elevating extracellular potas- sium concentration ([K+],) and diminished by lowering [K+]0.22,23
Conduction velocity and excitability are modi- fied by those effects of quinidine and procaine amide on the mechanism responsible for gener- ating the active response. Because there is less of an increase in the inward, depolarizing current for any degree of depolarization, the threshold poten- tial is shifted to less negative values.” As a result, more stimulus current is needed to initiate an active response from the normal level of resting potential. Because of the effects on active response and threshold potential, conduction velocity usually is decreased progressively as drug concentration rises. There is one exception to this statement. If conduction is measured in Purkinje fibers which demonstrate marked Phase 4 depo- larization, low concentrations of either quinidine or procaine amide may increase the speed of impulse propagation.‘“.2” This occurs for the following reason. In the presence of marked phase 4 depolarization, the action potential upstroke is initiated at quite a low level of membrane poten- tial. Consequently, upstroke velocity and ampli- tude are low and the impulse propagates slowly. Low concentrations of drug will markedly decrease the slope of phase 4 and permit the
American Heart Journal 117
Hotian, Rosen, and Wit
o! id. ,M
1 1 0 I I 1 1 I 0 20 40 60 60 100 120 140 160
TIME IN MINUTES Fig. 3. Effects of procaine amide on action potential charac- teristics of a blood-superfused Purkinje fiber. Vertical axis, plasma procaine amide concentration, pg/ml.: shaded area, therapeutic concentration range; horizontal axis, time in minutes. A shows a control action potential (on the upper trace) and a 200 V./set. calibration and measurement of V,,, (on the lower trace) for an isolated Purkinje fiber super-fused with the blood of an anesthetized dog. The dog was then given a rapid intravenous injection of procaine amide, 25 mg./Kg. Following equilibration of the fiber at a therapeutic plasma procaine amide concentration (B), action potential duration was prolonged, and amplitude and 6,,, were decreased. Additional procaine amide was then infused to raise plasma levels to the toxic range (C). Further decreases in amplitude
and Q,,,,, and prolongation of duration occurred. (Modified after Rosen, M. R., Gelband, H., and Hoffman, B. F., ref. 20.)
action potential to be initiated at a higher more normal level of membrane potential. The increase in membrane potential at the moment of excita- tion outweighs the direct effect of a low concen- tration of drug on inward sodium current and as a result the action potential improves and conduc- tion velocity increases.
The effects of quinidine and procaine amide on active responses of abnormal or depressed fibers have been described less completely. In prelimi- nary studies of isolated preparations of diseased human atrium, obtained as part of the routine cannulation procedure for cardiopulmonary by- pass, it has been shown that procaine amide in concentrations of 1 to 100 pg/ml. exerts a variable
118
+J 20mV
50mwc
effect on the action potential of specialized conducting fibers.‘” In fibers with normal action potential amplitudes and upstroke velocities, there is a dose-dependent decrease in these parameters. In partially depolarized fibers, hav- ing somewhat lower action potential amplitudes and upstroke velocities, there is a proportionately greater depressant effect of procaine amide. However, in markedly depressed fibers, gener- ating slow response action potentials which are exquisitely sensitive to low concentrations (0.1 to 1 pg/ml.) of the calcium blocker verapamil, even high concentrations of procaine amide have little or no effect.‘”
B. Effects on action potential duration and refractoriness. It has been known for many years that both quinidine and procaine amide delay re- polarization and increase the duration of refrac- toriness in atria1 and ventricular muscle fibers; similar effects are exerted on Purkinje fibers.17-lY These direct effects are modified to some extent both by the ability of quinidine and procaine amide to attenuate the effects of catecholamines and acetylcholine on the myocardium and by any drug induced changes in rate.
The effect on action potential duration also is influenced by [K+], in that prolongation is more marked at lower values of [K+],. Also, the magni- tude of the drug effect on action potential dura- tion varies with the anatomical location of fibers in the His-Purkinje system. The change is more marked for fibers initially demonstrating the shortest action potentials and less marked for those with the longest action potentials.‘” The over-all effect thus is to make more uniform the action potential duration over the entire length of the His-Purkinje system.
Prolongation of the action potential accounts only for part of the increase in duration of the effective refractory period caused by procaine amide and quinidine. As described above, pro- caine amide and quinidine decrease responsive- ness and, as a result, prevent the generation of a new propagating action potential until repolari- zation has carried membrane potential to more negative values than were required before drug action.“’ This decrease in responsiveness during repolarization is due in part to the effect of the drug on the maximum inward sodium current that can be generated at any level of membrane potential and perhaps in part also to a decrease in the rate of reactivation of the inward current
July, 1975, Vol. 90, No. 1
Electrophysiology and pharmacology of cardiac c~rrhythmias
mechanism during repolarization. The increase in action potential duration is more prominent at low rates and is counteracted in large measure by the actions of catecholamines and sympathomi- metic agents.
C. Effects on resting potential, maximum dias- tolic potential, and automaticity. Both quinidine and procaine amide decrease the slope of the Phase 4 depolarization which is associated with normal automaticity. This effect is demonstrated most clearly for cardiac Purkinje fibers but, in sufficient concentration, each drug will decrease Phase 4 depolarization in atria1 specialized fibers and in cells of the sinoatrial node. At low concen- trations of drug the decrease in rate of automatic firing results primarily from the effect on the slope of phase 4 depolarization; at higher concen- trations, the shift in threshold potential towards zero contributes to the slowing because threshold potential has been moved farther from maximum diastolic potential.” Quite high concentrations of quinidine and procaine amide will decrease the resting potential and maximum diastolic poten- tial of normal fibers; this effect is noted at lower drug concentrations if the fibers are diseased or depressed.
Although the usual effect of these antiarrhyth- mic drugs is to decrease the slope of phase 4 depolarization and the rate of automatic firing, in high concentrations quinidine, and to a lesser extent procaine amide, will increase the slope of phase 4 depolarization and spontaneous rate. This effect is demonstrated only when there has been some drug-induced decrease in maximum diastolic potential.
There is increasing evidence that in partially depolarized cardiac fibers the action potential results from an abnormal mechanism-an inward current carried in large part by calcium rather than sodium and through “slow,” rather than through the normal “fast” channels.“” In such fibers phase 4 depolarization may be present and may result in automatic firing. The effects of quinidine and procaine amide on the type of phase 4 depolarization recorded from partially depolarized fibers have not yet been described completely. Nevertheless, some information is available concerning human atria1 tissues. In these studies, markedly depolarized fibers with spontaneous rhythm were less responsive to procaine amide than they were to the calcium blocker verapamil.“’
American Heart Journal
Ionic mechanisms for actions on cardiac trans- membrane potentials. It seems most likely that the major actions@of procaine amide and quin- idine on the electrical activity of cardiac cells are the result of drug-induced changes in the conduc- tance of the cell membrane to several species of ions. The best information on this subject is derived from studies on the effects of procaine and other local anesthetics on the excitable membrane of squid giant axons”‘,‘“‘; unfortunate- ly, many of the studies on cardiac fibers which are needed to provide direct evidence for compara- bility between nerve and heart still are lacking. In general it seems clear that local anesthetics like procaine and procaine amide penetrate the cell membrane in the uncharged form and then, as a charged particle, interact with a site on the inner surface of the membrane which exerts control over the fast sodium channel. As a result, the sodium conductance of the membrane increases less, and sometimes less rapidly, when the membrane is depolarized. This depression of the voltage- and time-dependent increase in sodium conductance results in a decrease in the rate of change of membrane potential during phase 0 (a decrease in V,,,) and a decrease in the magnitude of the action potential overshoot. It also shifts the threshold potential towards zero. All of these actions combine to decrease excitability and conduction velocity. They also account, at least in part, for the decreased responsiveness of partially depolarized fibers. It is possible that procaine amide and quinidine also may decrease the rate at which the fast sodium channel is reactivated during repolarization, but appro- priate studies on heart fibers are lacking.
Repolarization of nerve fibers is delayed by procaine as a result of an effect on potassium conductance similar to that described for sodium conductance.““,‘” Unfortunately, repolarization of cardiac fibers is much more complex than is the case for nerve. It may be that prolongation of the cardiac action potential by procaine amide and quinidine also results in part from a drug-induced change in one or more of the membrane channels that permit efflux of potassium; appropriate studies using voltage-clamp and other techniques are needed to clarify the matter.
Phase 4 depolarization of normally automatic cardiac cells in the specialized atria1 fiber tracts and His-Purkinje system seems to result from a voltage and time-dependent decrease in potas-
119
Hoiban, Rosen, and Wit
sium conductance. There is evidence that, when procaine amide diminishes the slope of phase 4 depolarization, there is no clear change in potas- sium conductance at the level of maximum dias- tolic potential.31 The mechanism by which procaine amide and quinidine act on automaticity of cardiac fibers thus remains unexplained. A decrease in the slope of phase 4 depolarization can result from an increase in outward current, presumably carried by potassium, or a decrease in inward current, which might be carried by either sodium or perhaps calcium. Each of these cur- rents, and the associated conductance, might be influenced by the two antiarrhythmic drugs.
Effects on the heart and circulation
Quinidine and procaine amide exert many similar effects on the cardiovascular system. For the most part these effects are dose related. As mentioned above, when administered intra- venously, quinidine strongly depresses the con- tractile function of the heart and causes a decrease in systemic vascular resistance. This is brought about primarily by blockade of alpha adrenergic receptors. These actions have marked- ly limited its administration by this route. Procaine amide exerts similar, but weaker effects on the heart and circulation although vasodila- tion probably is due mainly to ganglionic block- ade. During repeated intravenous injection of procaine amide in doses of 100 mg., at intervals of 5 minutes, blood pressure usually begins to show meaningful changes after a total dose of 600 to 800 mg.13 As might be expected in patients whose heart or circulation is compromised, decreases in output and blood pressure may occur at lower doses. Since both quinidine and procaine amide decrease the contractility of the heart, high blood levels may be associated with an increase in left ventricular end-diastolic pressure. The direct negative inotropic effect of quinidine contributes strongly to the cardiovascular depression and collapse which often result from intravenous administration of this drug. Although both procaine amide and quinidine have been reported to attenuate the effects of the vagus on the mammalian heart, evidence of this action in humans is not uniformly convincing.
As might be expected from their effects on the electrical activity of single cardiac cells, quinidine and procaine amide cause dose-dependent changes in the electrocardiogram which are
clearly evident at therapeutic plasma levels.13.ZZ Both drugs also can cause abnormalities of cardiac rhythm and conduction. Procaine amide, at plasma levels between 5 to 10 pg/ml., has little predictable effect on sinus rate or sinus rhythm. However, the P-R interval is slightly prolonged and this change is comparable in patients with normal and with slowed atrioventricular trans- mission. QRS duration also increases as a func- tion of plasma level and may be prolonged by 5 to 10 msec. at a plasma level of 10 pg/ml. Thera- peutic levels of procaine amide usually do not prolong the QRS beyond the normal range. Q-T intervals corrected for heart rate are increased by procaine amide as a result of effects on ventric- ular action potential duration and conduction.
Quinidine is likely to increase sinus rate because of the reflex sympathetic response to its hypotensive effect. Like procaine amide, quin- idine increases the P-R interval, QRS duration, and Q-T interval. During chronic oral administra- tion it has been shown that the prolongation in QRS is dependent on plasma level at values > 2 fig/ml. and can be clearly demonstrated within the entire therapeutic range.32 The increase in Q- T duration caused by quinidine is more marked than that caused by procaine amide and is easily detected at therapeutic levels. When the Q-T interval is prolonged before drug treatment and there are early premature ventricular depolariza- tions, or when the coupling of the VPDs is unusually short in the presence of a normal Q-T interval, administration of quinidine may be asso- ciated with increased risk because of the pro- duction of the R-on-T phenomenon.33 The magni- tude of the effect of quinidine on QRS duration does not seem to be dependent on the initial value. These findings for humans agree well with data reported for studies on conscious dogs.3’
High plasma levels of either procaine amide or quinidine can cause high grade atrioventricular block, asystole, ECG patterns resembling bundle branch block, other conduction abnormalities and ventricular arrhythmias including premature depolarizations, tachycardia, and fibrillation. Ex- cessive prolongation of the QRS complex ( > 35 per cent) usually indicates that more serious toxic effects are imminent.
Studies on humans using catheter ele,ctrodesZ5 have confirmed most of the actions demonstrated for procaine amide in experiments on laboratory animals. At therapeutic plasma levels the effec-
120 July, 1975, Vol. 90, No. 1
Electrophysiology and pharmacology of cardiac ar~hythmins
tive refractory period of the human atrium is significantly prolonged as is the ERP of the His- Purkinje system. Conduction in the His-Purkinje system, measured as the H-V interval, is slowed by 10 to 30 per cent as is conduction through the atrioventricular node. Probably because of its vagolytic effect, in these studies procaine amide shortened the ERP of the atrioventricular node and slightly increased sinus rate.35
Mechanism for antiarrhythmic action
Since procaine amide and quinidine modify almost all aspects of cardiac electrical activity, the range of possible mechanisms for antiarrhyth- mic action is immense. Here it is possible only to mention a few of the more probable ones. Many studies have shown that the likelihood of initia- tion, as well as the likelihood of persistence of fibrillation depend in a critical manner on the number of cells in the population which are able to respond to a stimulus (the propagating impulse) at any particular instant. Since both procaine amide and quinidine increase the effec- tive refractory period of atria1 and ventricular fibers (by decreasing the ability of incompletely repolarized fibers to generate an active response and by delaying the completion of repolarization) both agents may be expected to exert antifibrilla- tory action. The finding that the atria1 rate in both fibrillation and flutter decreases as a func- tion of drug action suggests that quinidine and procaine amide do in fact slow the maximum rep- etition rate for any given cell until it no longer is possible for a circulating wave front of excitation to find a sufficient mass of excitable cells.
The mechanism by which these drugs abolish premature depolarizations depends on the cause of the premature excitation. If it results from firing of an automatic focus which employs the normal mechanisms, we probably can assume that drug effect results from a suppression of the slope of phase 4 depolarization, perhaps coupled with a shift in the level of the threshold potential towards zero. If the premature depolarizations result from reentry, it seems that abolition of the arrhythmia is due to a depressant effect of drug on the reentrant path such that an area of unidi- rectional block is converted into an area of bidi- rectional block.” The most compelling evidence in support of this hypothesis comes from recent studies showing that procaine amide consistently and progressively increases the coupling interval
American Heart Journal
of ventricular premature depolarizations before abolishing them.‘” Unpublished observations show that quinidine has a similar effect.
Antiarrhythmic action in the case of parox- ysmal tachyarrhythmias is difficult to describe for all cases. Nevertheless, several points seem clear. If the tachyarrhythmia results from reentry like that causing ventricular premature depolarizations, procaine amide and quinidine might be expected to act by a similar mechanism. Termination also might result from prolongation of the ERP in tissues just proximal to the site of reentry. It is interesting to note that, if these are the mechanisms of action, one would expect the rate to decrease prior to termination of arrhyth- mia. If a reentrant atria1 rhythm results from participation of the atrioventricular or sinus nodes, its persistence is critically dependent on an appropriate balance between conduction time in the node and refractoriness in the atrium. Termi- nation of arrhythmia could result either from depression of the reentering response in the node, from prolongation of effective refractoriness in the atrium, or from both.
Other antiarrhythmic actions clearly are possi- ble. For example, the ability of both drugs to decrease the slope of phase 4 depolarization in normally automatic cells can improve the respon- siveness of these cells and in this manner could convert an area of depressed conduction with unidirectional block to an area of successful forward conduction. Since the magnitude of the change in action potential duration caused by procaine amide or quinidine varies with the loca- tion of the fiber in the specialized conducting system, this action also may contribute to anti- arrhythmic action. To clarify these possibilities, new and careful clinical studies are needed.
Treatment of toxicity
The toxic effects of quinidine and procaine amide on the cardiovascular system usually will disappear fairly rapidly if drug administration is stopped. If treatment of drug toxicity is needed, two types of intervention are possible. Adminis- tration of sodium lactate by vein will diminish the toxic effects of both procaine amide and quinidine on the heart’s electrical activity by lowering the plasma potassium level. For both drugs the inten- sity of effect on electrical activity is increased with increasing K+ concentrations. In addition, by changing plasma pH, sodium lac%ate will
121
Hoffman, Rosen, and Wit
increase the binding of quinidine to albumin and thus decrease the free drug level acting on the heart. Administration of beta adrenergic amines also will diminish the undesirable changes in electrical activity caused by quinidine and procaine amide and at the same time will help to attenuate any negative inotropic effect exerted by either agent.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
Moe, G. K., and Abildskov, J. A.: Antiarrhythmic drugs, in The pharmacological basis of therapeutics, L. S. Goodman, and A. Gilman, eds. New York, 1970, Macmillan Publishing Co., Inc., pp. 709-727. Willius, F. A., and Keys, T. E.: A remarkably early reference to the use of cinchona in cardiac arrhythmia, Proc. Staff Meet. Mayo Clin. 17:294, 1942. Frey, W.: Weitere enfahrungen mit chinidin bei absoluter herzunregelmasaigkeit, Wein. Klin. Wochenschr. 55:849, 1918. Mautz, F. R.: The reduction of cardiac irritability by the epicardial and systemic administration of drugs as a protection in cardiac surgery, J. Thorac. Surg. 5:612, 1936. Hoffman, B. F., and Bigger, J. T., Jr.: Antiarrhythmic drugs, in Drill’s Pharmacology in Medicine, edited by DiPalma, J. R., New York, 1971, McGraw-Hill Book Company, Inc., p. 824. Bigger, J. T., Jr.: Arrhythmias and antiarrhythmic drugs, in Advances in Internal Medicine, vol. 18, Chicago, 1972, Year Book Medical Publishers, Inc., p. 251. Wallace, A. G., Sealy, W. D., Gallagher, J. J., Svenson, R. H., Strauss, H. C., and Kasell, J.: Surgical correction of anomalous left ventricular preexcitation, Wolff- Parkinson-White (Type A), Circulation 49:206, 1974. Durrer, D., Schoo, L., Schuilenburg, R. M., and Wellens, H. J. J.: Role of premature beats in the initiation and the termination of supraventricular tachycardia in the Wolff-Parkinson-White syndrome, Circulation 36:644, 1967. Wellens, H. J. J., and Durrer, D.: Effect of procaine amide, quinidine, and ajamaline in the Wolff-Parkinson- White syndrome, Circulation 50:114, 1974. Ferrer. M. I.: The sick sinus svndrome. Circulation 47:63i, 1973. Bigger, J. T., Jr., and Giardina, E. G. V.: The pharmacol- ogy and clinical use of lidocaine and procainamide, M. Coll. Va. Q. 9:65, 1973. Bloomfield, S. S., Romhilt, M. D., Chou, T. C., and Fowler, N. 0.: Quinidine for prophylaxis of arrhythmias in acute myocardial infarction, N. Engl. J. Med. 265:979, 1971. Giardina, E. G. V., Heisaenbuttel, R. H., and Bigger, J. T., Jr.: Intermittent intravenous procaine amide to treat ventricular arrhythmias, Ann. Intern. Med. 78:183, 1973. Dreyfuss, J., Bigger, J. T., Jr., Cohen, A. I., and Schreiber, E. C.: Metabolism of procaine amide in rhesus monkey and man, Clin. Pharmacol. Ther. 13:366, 1972. Giardina, E. G. V., Dreyfuss, J., Bigger, J. T., Jr., Shaw, J. M., and Schreiber, E. C.: The metabolism of procaine amide-*%! in man: Identification and characterization of metabolitea, Circulation tiO(Supp1. 111):227, 1974. Ladd, A. T.: Procainamide induced lupus erythematosus, N. Engl. J. Med. 267:1357, 1962.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
Weidmann, S.: Effects of calcium ions and local anesthe- tics on electrical properties of Purkinje fibers, J. Physiol. 129:568, 1955. Hoffman, B. F.: Action of quinidine and procaine amide on single fibers of dog ventricle and specialized conducting system, Anais Acad. Brasil. Cienc. 29:365, 1958. Rosen, M., Gelband, H., Merker, C., and Hoffman, B.: Effects of procaine amide on the electrophysiologic properties of the canine ventricular conducting system, J. Pharmacol. Exp. Ther. 185:438, 1973. Rosen, M., Gelband, H., and Hoffman, B.: Canine elec- trocardiographic and cardiac electrophysiologic changes induced by procainamide, Circulation 46:528, 1972. Singh, B. N., and Hauswirth, 0.: Comparative mecha- nisms of action of antiarrhythmic drugs, ANI. HEART J. 87:367, 1974. Bellet, S.: Clinical disorders of the heart beat, Philadel- phia, 1963, Lea & Febiger, p. 864. Watanabe, Y., Dreifus, L., and Likoff, W.: Electrophysio- logical antagonism and synergism of potassium and anti- arrhythmic agents, Am. J. Cardiol. 12:702, 1963. Singer, D. H., Strauss, H. C., and Hoffman, B. F.: Biphasic effects of procaine amide on cardiac conduction, Bull N. Y. Acad. Med. 43:1994, 1967. Singer, D. H., and Ten Eick, R. E.: Pharmacology of car- disc arrhythmias, Progr. Cardiovasc. Dis. 11:488, 1969. Hordof. A.. Edie. R.. Malm. J.. and Rosen. M.: Effects of procaine amide’ and verapamil on electrophysiologic properties of human atria1 tissues, Pediatric Research 9:267, 1975. Wit, A. L., Rosen, M. R., and Hoffman, B. F.: Electro- physiology and pharmacology of cardiac arrhythmias. II. Relationship of normal and abnormal electrical activity of cardiac fibers to the genesis of arrhythmias, AM. HEART J. 88:515,1974. Wit, A. L., Rosen, M. R., and Hoffman, B. F.: Electro- physiology and pharmacology of cardiac arrhythmias. II. Relationship of normal and abnormal electrical activity of cardiac fibers to the genesis of arrhythmias B. Re- entry, Section I, AM. HEART J. 88:664, 1974. Taylor, R. E.: Effect of procaine on electrical properties of squid axon membrane, Am. J. Physiol. 916:1071, 1959. Narahashi, T., Frazier, D. T., and Yamada, M.: The site of action and active form of local anesthetics. I. Theory and pH experiments with tertiary compounds, J. Phar- macol. Exp. Ther. 171:32, 1970. Weld, F. M., and Bigger, J. T., Jr.: Effect of procaine amide on membrane conductance of cardiac Purkinje fibers, Circulation (Abstr.) 46:11-39, 1972. Heissenbuttel, R. H., and Bigger, J. T., Jr.: The effect of oral quinidine on intraventricular conduction in man: Correlation of plasma quinidine with changes in QRS duration, AM. HEART J. 80:453, 1970. Pick, A.: Manifestations of a vulnerable phase in human heart, in Sudden cardiac death, ed. by B. Surawicz and E.D. Pellegrino, New York, 1964, Grune & Stratton, Inc. Wallace, A. G., Cline, R. E., Sealy, W. C., Young, W. G., Jr., and Troyer, W. G., Jr.: Electrophysiologic effects of quinidine, C&. Res. 2 1:960, 1966. Joseoh. M. E.. Caracta. A. R.. Ricciutti. M. A.. Lau. S. H.. and *Damato; A. N.: ’ Electrophysioldgic properties of procainamide in man, Am. J. Cardiol. 33:596, 1974. Giardina, E. G. V., and Bigger, J. T., Jr.: Procaine amide against re-entrant ventricular arrhythmias, Circulation 48:959, 1973.
122 July, 1975, Vol. 90, No. 1