Embed Size (px)
Citation preview

Electrophysiology of Oral Encainide
WARREN M. JACKMAN, MD DOUGLAS P. ZIPES, MD, FACC
GERALD V. NACCARELLI, MD
ROBERT L. RINKENBERGER, MD
JAMES J. HEGER, MD, FACC
ERIC N. PRYSTOWSKY, MD, FACC
Indianapolis, Indiana
From the Krannert Institute of Cardiology, the Department of Medicine, lndll University School of Medicine, and the Veterans Administration Medical Center, Indianapolis, Indiana. This work was supported in part by the Herman C. Krannert Fund, Indianapolis. Indiana; by Grants HL-06308, HL-07 182 and HL-18795 from the National Heart, Lung and Blood Institute, National Institutes of Health, Bethesda, Maryland; and by the American Heart Association, Indiana Affiliate, Inc., India- napolis, Indiana. Manuscript received July 6. 198 1; revised manuscript received October 26 .1981, accepted October 29, 1981.
Address for reprints: Eric N. Prystowsky. MD, Department of Medicine, lndlla University School of Medicine, Krannert Institute of Cardiology, 1100 West Michigan Street, Indianapolis, Indiana 46223.
The electrophysiologic effects of oral encainide were assessed in 15 patients. Electrophysiologic studies were performed before and after 3 or more days of oral encainide therapy, 100 to 300 mg/day (mean 242 f 66). Patients received no other cardioactive drugs during this time. Encainide significantly (p <0.005) lengthened the following: A-H interval (74.5 f 21.5 to 105.5 f 39.1 ms, mean f standard deviation), the shortest atrial pacing cycle length maintaining 1:l atrioventricular (A-V) nodal conduction (339.0 f 71.3 to 417.0 f 66.6 ms), H-V interval (47.5 f 7.6 to 67.1 f 12.9 ms), QRS interval (103.5 f 30.9 to 132.3 f 35.7 ms), right atrial (233.6 f 27.2 ms to 262.9 f 36.6 ms) and right ventricular (235.7 f 15.6 to 267.1 f 36.9 ms) effective refractory periods and Q-T interval (364.4 f 36.0 to 416.9 f 55.3 ms). The spontaneous sinus cycle length did not change significantly. in four patients who had accessory A-V muscle connections (two manifest, two concealed) encainide abolished anterograde conduction over the accessory pathway in two patients, and increased the retrograde effective refractory period and/or lengthened retrograde conduction time or blocked retrograde conduction in the ac- cessory pathway, or ail three variables, in all four patlents. There was no correlation between the plasma encainide concentration obtained at the time of study and the magnitude of change in any electrophysiologic variable.
lt is concluded that (1) encainide depresses conduction in the A-V node, His-Purkinje system and accessory pathway, and increases refractoriness of the atrium, ventricle and accessory pathway, and (2) differences be- tween these results and those of earlier studies using encainide in a single intravenous dose (which found no significant effects on A-V nodal con- duction or atrial and ventricular refractoriness) may be explained in part by the effects of an active metabolite of encainide.
Encainide HCl, a new benzanilide derivative (4-methoxy-2’-[2- (methyl-2-piperidyl) ethyl] benzanilide hydrochloride), is reported to be more potent than quinidine or procainamide in abolishing a variety of experimental atria1 and ventricular arrhythmias.‘-” In human beings, encainide administered either intravenously4,5 or orally5-7 effectively suppresses premature ventricular complexes, and preliminary data in selected patients who have ventricular tachycardia demonstrate that encainide can prevent recurrence of the arrhythmia.s-10
In both dogsl’ and human subjects,12 a single intravenous dose (0.6 to 0.9 mg/kg) of encainide substantially lengthens H-V and QRS inter- vals without affecting atrioventricular (A-V) nodal conduction or re- fractoriness of atrium, ventricle or atrioventricular node. The electro- physiologic effects of oral encainide administration are not known. The results of such studies would be of interest because recent data”T5r6J3 suggest that encainide may have active metabolites, whose effects might not be observed in electrophysiologic studies performed after a single intravenous dose. Thus, the purpose of this study was to determine the electrophysiologic effects of oral encainide in human beings.
1276 April 1, 1982 The American Journal of CARDIOLOGY Volume 49

ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL.
Methods
Electrophysiologic study: Fifteen patients who had a variety of arrhythmias (Table I) underwent electrophysiologic study before and during oral encainide therapy. Patients were studied in the postabsorptive, nonsedated state after dis- continuation of all cardioactive medications for a period ex- ceeding five times the elimination half-life of the respective medications. Three or four multipolar electrode catheters were inserted percutaneously and advanced to the heart under fluoroscopic guidance. The catheters were positioned in the high lateral right atrium, in the right ventricle, across the tricuspid valve in the region of the His bundle and, in six pa- tients, into the coronary sinus.
Intracardiac electrograms and standard electrocardio- graphic leads I, II, III and VI were displayed simultaneously on a multichannel oscilloscope and recorded at paper speeds of 100 and 150 mm/s. The intracardiac and surface electro- grams were recorded at frequencies of 30 to 500 and 0.1 to 20 hertz, respectively. Programmed electrical stimulation (1.8 ms rectangular stimuli at twice late diastolic threshold cur- rent) included: (1) incremental high right atria1 pacing, be- ginning at a cycle length just shorter than the spontaneous cycle length and shortening the pacing cycle length by 10 to 20 ms decrements until A-V nodal block occurred or until limited by patient symptoms; and (2) atria1 and ventricular refractory period determinations. In patients with an acces- sory A-V pathway the shortest pacing cycle length main- taining 1:l conduction over the accessory pathway and the effective refractory period of the accessory pathway were determined in the anterograde and retrograde directions.
Atria1 and ventricular refractory period determinations were performed by pacing the respective chamber at a con- stant cycle length for 30 seconds. Then, without interrupting the pacing cycle length, premature stimuli were introduced after every eighth paced complex beginning with a premature interval (SI-S~) too short to result in a response. Each pre- mature interval was tested twice, then lengthened by 5 to 10 ms increments until the atria1 or ventricular effective and functional refractory periods were determined. This technique allows an uninterrupted driving sequence, preventing varia- tion in cycle length which can influence refractoriness.14J5
The effective refractory period of the atrium and ventricle was defined as the longest S1-S2 interval at which Sa, on two consecutive attempts, failed to induce atria1 or ventricular depolarization, respectively. The anterograde and retrograde effective refractory periods of the accessory pathway were defined as the longest AI-AZ or VI-V~ interval, respectively, at which conduction did not occur over the accessory pathway. The functional refractory periods of the atrium and ventricle were the shortest obtainable atria1 (Al-AZ) and ventricular (VI-V,) responses. P-A, A-H, H-V, QRS and Q-Tc (Q-T/JR-R)16 intervals were measured during sinus rhythm. A-H and Q-T intervals were also measured during high right atria1 pacing at a cycle length of 600 ms to eliminate variation resulting from changes in sinus rate. The Q-T interval was measured from the earliest inscribed QRS complex to latest inscribed T wave in any of four surface electrocardiographic leads recorded simultaneously at 100 mm/s.
Encainide therapy: After completing the stimulation protocol, Patients 12,14 and 15 received a single intravenous dose of encainide (0.6, 0.7 and 0.9 mg/kg, respectively), ad- ministered over 15 minutes. Twenty minutes after completion of the infusion, the stimulation protocol was repeated.
After the control electrophysiologic study, all 15 patients were treated with oral encainide. The drug was administered at 4 or 6 hour intervals in doses totaling 100 to 300 mg/day
TABLE I
Patient Characteristics
Age W Patient & Sex
Cardiac Diagnosis* Arrhythmia
: 52M CAD 57M CAD ZT
3 4
:
:
1: 11 12 13 14 15
34M 59M 52M 27M 43M 48F 53F 61F 55F 17M 49M 52F 18M
E MVP MVP PED PED WPW WPW WPW WPW PED
VT VT VT VT VT VT VT VT RT RT
z5 AVNRT
l Cardiac diagnosis is based on angiographic data in all patients with ventricular tachycardia (Patients 1 to 10) except Patient 8 (echocar- diographic evidence of mitral valve prolapse).
AVNRT = atrioventricular nodal reentrant tachvcardia: CAD = cor- onary artery disease; CM = idiopathic dilated c&diom;opathy; F = female; M = male: MVP = mitral valve prolapse; PED = primary electrical disease (presence of arrhythmia and no detectable structural heart disease); RT = reciprocating tachycardia using the A-V node- His-Purkinje system for anterograde conduction and an accessory atrioventricular muscle connection for retrograde conduction; VT = recurrent ventricular tachycardia; WPW = Wolff-Parkinson-White syndrome.
(mean 242 f 66). After 3 to 10 days (mean 4.1 f 1.9) of en- cainide therapy a repeat electrophysiologic study was per- formed.
At the repeat (encainide) electrophysiologic study, the atria1 and ventricular catheters were placed under fluoroscopic guidance close to their respective positions during the control study. The QRS axis and morphologic characteristics in four electrocardiographic leads during ventricular pacing were similar for both studies. For each patient, refractory period determinations were performed at the same pacing cycle length during the control and encainide studies using stimuli of twice late diastolic threshold for all studies. Atria1 refractory period determinations were performed at pacing cycle lengths of 350 to 800 ms (median 500) and ventricular refractory pe- riod determinations at pacing cycle lengths of 400 to 600 ms (median 450).
Plasma encainide concentration: A sample of venous blood was obtained at the conclusion of the encainide elec- trophysiologic studies, which was 1.5 to 6 hours after the pa- tient’s preceding encainide dose. Plasma encainide concen- tration was determined by radioimmunoassay17 in four pa- tients and by high pressure liquid chromatography’i in seven patients, and was not obtained in four patients. Values de- termined by both techniques correlate very closely (r = 0.97).17 Because of the strongly alkaline extraction procedure, the radioimmunoassay is relatively selective for the parent com- pound. High pressure liquid chromatography provides indi- vidual quantitation of the parent compound and several demethylated metabolites including 0-demethyl encainide, N-demethyl encainide and N,O-bis-demethyl encainide. The radioimmunoassay and high pressure liquid chromatographic assay are sensitive to 0.2 and 10 ng/ml, respectively.17
Data analysis: Data are expressed as mean f 1 standard deviation. The t test for paired data was used to assess the significance of changes from control in electrophysiologic variables within patients. Linear regression analysis (and multiple linear regression analysis) was used to assess the
April 1, 1982 The American Journal of CARDIOLOGY Volume 49 1271

ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL.
TABLE II
Eleclrophysiologic Effects of Encainide
Control Encainide Percent n (ms) (ms) Change P
Electrocardiographic intervals P-R QRS - - Q-T, Q-T (CL 600)
13 164.6 f 22.5 13 103.5 f 30.9 13 413.6 f 34.4 9 364.4 f 30.0
214.2 f 36.2 132.3 f 35.7 464.4 f 40.6 416.9 f 55.3
30.1 <O.OOl 27.8 <O.OOl 12.3 <O.OOl 14.4 <0.005
S-A nodal auiomaticity SDont CL 14 832.5 f ia8 ala.9 f 130 3 1.6 NS
Atiial conduction and refractoriness P-A interval ERP FRP
A-V nodal conduction A-H interval (NSR) A-H interval (CL 600) Shortest CL-l : 1 AVN conduction
His-Purkinje system conduction H-V interval
:: 49.3 f 11.6 65.7 f 14.3
233.6 f 27.2 282.9 f 38.6 i 33.3 <O.OOl 21.0 <O.OOl
12 261.7 f 26.7 317.5 f 40.4 21.3 <O.OOl
14 64.6 f 16.2 64.6 f 21.5 31.0 <O.OOl 10 74.5 f 21.5 105.5 f 39.1 41.6 <O.OOl 10 339.0 f 71.3 417.0 f 88.6
i
23.0 <O.OOl
12 47.5 f 7.8 67.1 f 12.9 f 41.3 <O.OOl Ventricular refractoriness
ERP FRP
A-H interval (CL 600) = A-H interval measured
during atrial pacing at cycle length 600 ms; Q-T, cycle length (mean of 10 consecutive cycles).
length 600 ms; Shortest CL-l: 1 !VN conduction = shortest right interval (NSR) = A-H interval measured during normal sinus rhythm; A-V =
= not significant; O-T (CL 600) = Q-T interval measured S-A = sinoatrial; Spont CL = spontaneous sinus
relation between plasma encainide (or demethylated metab- olite, or both) concentration and the magnitude of change in electrophysiologic variables.
Results
Electrophysiologic Effects of Encainide
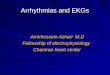
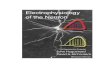
Atrium, ventricle and normal conduction system: The effects of oral encainide therapy on selected electrophysiologic variables are listed in Table II and displayed in Figures 1 to 3. Encainide significantly lengthened: atria1 and ventricular refractory periods (Fig. 1); the A-H interval, the shortest right atria1 pacing cycle length maintaining 1:l A-V nodal con-
360 -
340 -
320 -
z 300 -
f - 280 -
z a 260 -
rr : 240 -
220 -
200 - p<o.o01
I I 1
CONTROL ENCAINIDE
360 -
340 -
320 -
300 -
280 -
260 -
240 -
220 -
200 -
duction, and the H-V interval (Fig. 2); and QRS and Q-T in- tervals (Fig. 3). The combined prolongation of conduction time in the atrium (P-A interval), A-V node (A-H interval), and His-Purkinje system (H-V interval) resulted in 30.1 percent lengthening of the P-R interval (Fig. 3). No significant change was observed in sinus nodal automaticity.
Patients 12,14 and 15 received intravenous encainide (0.6, 0.7 and 0.9 mglkg, respectively) during their first electro- physiologic study after collection of control data. Atria1 and ventricular effective refractory periods did not change after intravenous encainide administration in any patient. In Pa- tients 14 and 15, atria1 and ventricular effective refractory periods lengthened 20 to 80 ms after oral encainide. In Patient
” = 14 p< 0.005
L I CONTROL ENCAINIDE
FIGURE 1. Effect of encainide on atrial effective refractory period (ERP) (lefl) and ventricular ef- fective refractory period (right). Lines connect values for each patient during control and en- cainide therapy. Horizontal lines in each column represent mean values.
1272 April 1, 1982 The American Journal of CARDIOLOGY Volume 49

180 -
160 -
tl
; 140 -
: 120 -
d
28 100 -
d; <-
2 80 -
: z 60 -
s
40 -
20 -
k - 4 - 9
” -10 p<o.o01
650
1 600 -
- 550-
:
8 500 -
: 450 -
i
: 400 -
$ F 350 -
% 2 300 -
250 -
ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL
110
100
1
90 -
80 -
70 -
: 2 60-
? z 50 - ( 8)
2 40 -
30 -
” =lO p<o.o01
20
1
n= 12 p<o.o01
I - I CONTROL ENCAINIDE CONTROL ENCAlNlDE CONTROL ENCAINIDE
FIGURE 2. Effect of encainide on atrioventricular (A-V) conduction. Left, A-H interval measured during high right atrial pacing at cycle length (CL) of 600 ms. Middle, shortest pacing cycle length (CL) maintaining 1:l A-V nodal (AVN) conduction (COND) during incremental right atrial pacing. Open circles indicate that incremental atrial pacing was terminated before the onset of A-V nodal Wenckebach block. Right, H-V interval during sinus rhythm.
12 the atria1 and ventricular effective refractory periods were unchanged from control periods after oral encainide admin- istration. The A-H interval (measured at the same right atria1 pacing cycle length) increased after intravenous encainide in Patients 14 and 15, but substantially less than during oral encainide therapy (Fig. 4), and was unchanged in Patient 12. In Patients 12 and 15,l:l A-V nodal conduction occurred to atria1 pacing cycle lengths of 320 ms or less and 300 ms or less, respectively, both before and after intravenous therapy.
300
280
260
240
220
200
180
160
140
120
FIGURE 3. Effect c
/ / - -4 / n= 13
p <O.OOl
I I
CONTROL ENCAINIDE
220 -
200 -
180 -
j 160-
< 2 140 -
if
z 120 -
z
u loo-
80 -
60 -
During oral encainide therapy, 1:l A-V nodal conduction was maintained only to a pacing cycle length of 350 ms in both patients. In Patient 14, anterograde conduction over the ac- cessory pathway prevented determination of the shortest atria1 pacing cycle length sustaining 1:l A-V nodal conduc- tion.
Atrioventricular nodal reentrant tachycardia demon- strating long anterograde conduction time (A,-H) and short retrograde conduction time (H-A,) was induced during the
/
/
/
-
* J ” = 13
p<o.o01
500 7
480 -
460 -
E 440 -
: d 420 -
$2 2;
400 -
a-
&z 380 -
if f 360 -
&
340 -
320 -
/
9 i n-9 p<o.oos
_L 1
I .
I 1 I
CONTROL ENCAINIDE CONTROL ENCAINIDE
ncainide on electrocardiographic intervals. Left, P-R interval during sinus rhythm. Mlddle, QRS interval during sinus rhythm. Rlght, Q-T interval during atrial pacing at a cycle length (CL) of 600 ms.
Aprtf 1,1362 The American Journal of CARDIOLOGY Volume 43 1273

ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL.
A. CONTROL
I-
ll -
B. IV ENCAINIDE C. ORAL ENCAINIDE
Illlllhlbll~lklkil~I Illll~lillklklkAk~khi h~~~~3l~~~hh~ll~hl~~l~lllhll 111111111111 Ill1 Ill1 III/ Ill IIII Ill llll Ill Ill1 lill Ill l/II II 1111111 III1 /III 11111111 l/lllll II/I III III1 III1 III III1 Ill Illl II III II III II I II III I II II III w III III III II Ill1 11111111 III Ill Ill1 II Ill1 III /III 11111111 III1 Ill 1111
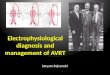
FIGURE 4. Patient 14. Effect of encainide on atrioventricular nodal and accessory pathway conduction during atria1 pacing at cycle length 500 ms. The top four tra&gS are standard electrocardiographic leads I, II, Ill and VI. The bottom two tracm are intracardiac electrograms recorded from catheters positioned in the high right atrium (HRA) and His bundle region (HBE). In panels A and B the broken line denotes onset of ventricular preexcitation (delta wave). A, during control study, ventricular depolarization begins before His bundle depolarization and the A-H interval is 105 ms. B, after a single intravenous (IV) dose of encainide (0.7 mg/kg), anterograde conduction over the accessory pathway is present and the interval from stimulus artifact to delta wave (165 ms) is unchanged from the control value. The A-H interval is 150 ms. C, during oral encainide therapy, ventricular PreeXCitatiOn is no longer present (absent delta wave, H-V interval of 90 ms, left bundle branch block) and the A-H interval increases to 365 mS. The combination of A-H and H-V prolongation causes the stimulus to QRS interval to exceed 510 ms and the ventricular complex occurs after the neti atrial pacing stimulus. A, Hand V represent the atrial, His bundle and ventricular depolarizations, respectively, of one conducted complex. The interval between the tall tlme lines is 50 ms and is the same for all figures.
control electrophysiologic study in Patient 15. Tachycardia of 380 ms or less. Single intravenous dose encainide (0.9 could not be induced during oral encainide therapy. Encainide mg/kg) failed to prevent the induction of tachycardia but lengthened the anterograde effective refractory period of the lengthened the tachycardia cycle length from 320 to 360 ms “slow” A-V nodal pathway from less than 270 to 320 ms, but because of an increase in the A,-H interval from 240 to 270 ms appeared to prevent supraventricular tachycardia by and an increase in the H-A, interval from 80 to 90 ms. This lengthening refractoriness in the retrograde limb of the patient has continued to receive encainide therapy and after tachycardia circuit. During encainide therapy premature atrial 7 months has not had a recurrence of tachycardia. stimuli did not result in atria1 echo beats even though Al-As Accessory pathways: Patients 11 to 14 had accessory A-V versus HI-Hs curves were still discontinuous and greater pathways (Tables I and III). In Patients 13 and 14, 1:l an- As-Hz prolongation occurred than that required for the in- terograde conduction over the accessory pathway (ventricular duction of tachycardia during the control study. During in- preexcitation) occurred at atria1 pacing cycle lengths of 300 cremental ventricular pacing, ventriculoatrial block occurred and 310 ms, respectively, during the control study. Oral en- in the A-V node at a cycle length of 540 ms after encainide cainide therapy resulted in loss of ventricular preexcitation administration, whereas during control study, 1:l ventricu- during sinus rhythm and at all atria1 pacing cycle lengths in loatrial conduction was maintained to a pacing cycle length both patients (Table III, Fig. 4).
TABLE Ill
Electrophyslologlc Effects of Encainlde on Accessory Atrloventrlcular Pathway
Anterograde AP Function (Atrial Pacing) Retrograde AP Function (Ventricular Pacing)
Shortest PCL- 1: 1 AP Shortest PCL-1:l AP Conduction (ms) ERP (ms) Conduction (ms) ERP (ms)
AP IV Oral IV Oral IV Oral IV Oral Patient Location Cont En En PCL Cont En En Cont En En PCL Cont En En
11 Left No preexcitation No preexcitation --- - 450 240 - - - - lateral
12 Left No preexcitation No preexcitation Q420 270 670 600 <265 <260 Block anterior
13 Left 300 --- Block 600 <250 --- Block 300 - - - Block 600 <250 - - - Block paraseptal
14 Left 310 350 Block 600 315 335 Block 320 340 570 600 360 380 515 lateral
AP = accessory pathway; Cont = control: ERP = effective refractory period, measured at the same pacing cycle length during control and after intravenous and oral encainide therapy; IV En = single intravenous dose of encalnfde; Oral En = oral encainide therapy; PCL = pacing cycle length; - = ventriculoatrial conduction time shorter over the normal conduction system than the accessory pathway; - - - = intravenous encainide not administered.
1274 April 1, 1982 The American Journal of CARDIOLDGY Volume 49

ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL.
PCS
DCS
HBE
IV ENCAINIDE
0. ORAL ENCAINIDE
RV
PCS
DCS
FIGURE 5. Patient 12. Effect of encainide on retrograde conduction over an accessory pathway during right ventricular pacing. A, after a single intravenous (IV) dose of encainide (0.6 mg/kg), 1:l retrograde accessory pathway conduction is maintained to a cycle length of 270 ms and 2: 1 ventriculoatrial block occurs at a cycle length of 260 ms. The refmgrade atrial activation sequence is identical to the sequence during recipro- cating tachycardia (Fig. 6). with earliest activation recorded in the distal coronary sinus electrogram. B, during oral encainide therapy, retrograde conduction is absent at a ventricular pacing cycle length of 650 ms. Sinus rhythm is undisturbed (third QRS complex is a conducted sinus impulse). Note the normal anterograde atrial activation sequence of proximal coronary sinus activation preceding distal coronary sinus activation. DCS = distal coronary sinus electrogram; PCS = proximal coronary sinus electrogram; RV = right ventricular electrogram.
Before oral encainide therapy, 1:l retrograde conduction overthe accessory pathway occurred to ventricular pacing cycle lengths of 320 ms or less in Patients 13 and 14 (Table III). In Patient 12 the shortest ventricular pacing cycle length sustaining 1:l retrograde conduction was not determined in the control state but was 270 ms after intravenous encainide.
During oral encainide therapy, retrograde conduction over the accessory pathway was abolished in Patient 13 and main- tained only to pacing cycle lengths of 670 and 570 ms in Pa- tients 12 and 14, respectively (Table III, Fig. 5). In Patient 11 ventriculoatrial (V-A) conduction time at all pacing cycle lengths was shorter over the normal conduction system (A-V node).
The retrograde effective refractory period of the accessory pathway lengthened with oral encainide by 155 ms in Patient 14 but could not be determined during encainide therapy in Patients 12 and 13 because of retrograde block over the ac- cessory pathway at the pacing cycle length tested, or in Patient 11 because at all premature coupling intervals V-A conduction occurred earliest over the A-V node (Table III). Single intra- venous dose encainide, administered to Patients 12 and 14, had minimal effect on accessory pathway conduction and refractoriness (Tables III and IV, Fig. 4 to 6).
In all four patients, programmed electrical stimulation of the control study induced sustained reciprocating tachycardia utilizing the normal A-V conduction system for anterograde conduction and an accessory pathway for retro- grade conduction. Oral encainide therapy prevented induction of tachycardia in Patients 12 and 13 because of retrograde block in the accessory pathway; and in Patient 11, only non- sustained episodes were induced which terminated with ret- rograde block in the accessory pathway (Table IV). In Patient 14 sustained tachycardia with a cycle length 205 ms longer than the control length was induced (Table IV, Fig. 7). Pa- tients 11 to 13 have continued to receive encainide therapy (100 to 240 mg/day) for 8 to 11 months without recurrence of tachycardia.
Ventriculoatrial conduction time during tachycardia lengthened after oral encainide by 125 and 200 ms in Patients 11 and 14, respectively (Table IV, Fig. 7). Part of the increase in V-A conduction time was due to intraventricular conduc- tion delay, because encainide resulted in left bundle branch block during tachycardia in both patients. The QRS interval increased with encainide by 70 ms in Patient 11 and by 55 ms in Patient 14. The “local” ventriculoatrial conduction time, in which the onset of both ventricular and atria1 activation was measured in the electrogram recorded closest to the accessory pathway (distal coronary sinus), increased with encainide from 80 to 150 ms in Patient 11 and from 150 to 260 ms in Patient 14, suggesting that prolongation of conduction time over the accessory pathway also occurred.
Plasma encainide concentration: The plasma encainide levels, drawn at the conclusion of the repeat electrophysiologic
TABLE IV
Effects of Encainide on Conduction Intervals During Reciprocating Tachycardla in WPW Syndrome
Patient
Tachycardia Cycle Length (ms) AI-H (ms) H-V (ms) V-A’ (ms)’
IV Oral IV Oral IV Oral IV Oral Cont En En Cont En En Cont En En Cont En En
:: 335 235 - 335 - - 365+ NI 1% 120 55 NI 55 40 60 250% 55 125 180 180 -
:: 290 410 - 430 - - 6% 110 135 --- 130 !A 35 40 --- 45 90 N”I 235 145 --- 255 435x f!
l V-A’ = intervals measured using the atrial depolarization on the His bundle electrogram. 7 Nonsustained tachycardia; duration of longest episode was 10 seconds. t Left bundle branch block during tachycardia. - - - Intravenous encainide not administered. Cont = control; IV en = intravenous encainide therapy; NI = reciprocating tachycardia was not inducible with programmed atrial or ventricular
stimulation; Oral en = oral encainide therapy; WPW = Wolff-Parkinson-White syndrome.
April 1, 1982 The American Journal of CARDIOLOGY Volume 49 1275

ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL.
A. CONTROL
“1
PCS
DCS
HBE
B. IV ENCAINIDE
“1
PCS
DCS
HBE
FIGURE 6. Patient 12. Effect of a single intravenous dose (0.6 mg/kg) of encainide on reciprocating tachycardia in the Wolff-Parkinson-White syndrome. A, before encainide the tachycardia cycle length is 335 ms with an A-H interval of 115 ms, an H-V interval of 40 ms and a V-A in- terval of 180 ms. The interval from onset of ventricular depolarization to the earliest retrograde atrial activation (distal coronary sinus elec- trogram) is 105 ms. B, after intravenous (IV) encainide, reciprocating tachycardia is reinitiated. The V-A interval during tachycardia is un- changed from control. The tachycardia cycle length increases only 20 ms because of A-H and H-V increases of 5 and 15 ms, respectively.
studies, varied widely from less than 15 to 674 ng/ml (mean 285 f 242). The largest values occurred in samples drawn 2 to 4 hours after the preceding dose of encainide. Plasma concentration of 0-demethyl encainide varied to a lesser ex- tent (mean 203 f 108 ng/ml), and there was no apparent relation to the time of the preceding encainide dose. No N- demethyl or N,O-bis-demethyl encainide was found in the seven patients in whom high pressure liquid chromatography was used.
The relation between plasma drug concentration and electrophysiologic effect was examined. No significant cor- relation was found between the percent change in atria1 or ventricular effective refractory periods, H-V interval, QRS interval or the shortest atria1 pacing cycle length maintaining 1:l A-V nodal conduction and the plasma concentration of encainide, the natural logarithm of the encainide concentra- tion, the plasma concentration of 0-demethyl encainide or combinations of encainide and metabolite concentrations.
Discussion
Oral encainide therapy substantially depressed conduction in the A-V node and His-Purkinje system and lengthened refractoriness of atrium, ventricle and accessory A-V muscle connections. In association with these changes, encainide suppressed supraventricular tachycardia utilizing an accessory A-V pathway in three of four patients and due to A-V nodal reentry in one patient. Although each patient served as his or
_ _ _
IIIIIIIIIIIIIIIIIIIIIIIIIII II/l IIll Ill1 III Ill1 Ill1 IIll II0 Ill1 Ill1 Ill1 Ill1 III1 III1 Ill1 /III II/l Ill1 Ill1 III II11 IllI III1 1111 IllI IIII
B. ORAL ENCAINIDE
. i
IIIIIIIIIIIIIIIIIIIIIIIIIII III1 IllI Ill1 IllI III1 III1 III1 Ill1 Ill1 1111 Ill1 Ill1 Ill1 Ill1 Ill1 Ill1 IIll IllI Ill1 l/II III/ Ill1 /III Ill1 Ill1 II/I
FIGURE 7. Patient 14. Oral encainide therapy greatly prolonged the cycle length of reciprocating tachycardia in the Wolff-Parkinson-White syndrome. A, before encainide, the tachycardia cycle length (CL) is 410 ms. B, oral encainide therapy lengthens ventriculoatrial conduction time (V-A’) 200 ms, and H-V interval 50 ms. Although the A-H interval shortens by 45 ms (presumably secondary to the slower tachycardia rate), the tachycardia cycle length during encainide therapy is 205 ms longer than that during the control period.
her own control, alteration of hemodynamic state or autonomic tone during encainide therapy could affect the measured electrophysiologic variables; However, the changes during encainide therapy were highly signifi- cant and consistent and most likely represent the effect of encainide.
Single intravenous dose versus chronic oral en- cainide therapy: The electrophysiologic effects that we noted with oral encainide therapy differ considerably from those found by us and others1iJ2 after single in- travenous dose encainide. Although H-V and QRS in- tervals increased to nearly the same extent as with oral therapy, a single intravenous dose (0.6 to 0.9 mg/kg) of encainide had no significant effect on atria1 refractori- ness, ventricular refractoriness or A-V nodal conduc- tion. In reported studies11J2 using intravenous en- cainide, maximal H-V and QRS prolongation occurred immediately after the 15 minute infusion, and the percent change in H-V and QRS intervals correlated well with peak plasma encainide concentration.l’ During oral therapy no significant relation was found between plasma encainide concentration obtained at the time of electrophysiologic study and the degree of change in atria1 or ventricular effective refractory pe-
1276 April 1, 1962 The American Journal of CARDIOLOGY Volume 49

God, shortest atria1 pacing cycle length sustaining 1:l A-V nodal conduction, H-V interval or QRS interval.
In concentrations comparable with the plasma con- centrations in this study, encainide greatly depressed the action potential upstroke velocity (V,,,) without lengthening the effective refractory period in atrial, ventricular and Purkinje cells.18l1g Encainide had no effect on slow response action potentiaIs.lg These results correlate well with the clinical electrophysiologic aspects of single intravenous dose encainide, but fail to explain the pronounced effect on atria1 and ventricular refrac- toriness and A-V nodal conduction seen after oral en- cainide administration. Changes in autonomic tone can modify A-V nodal conduction, but encainide exerted no effect on the sympathetic (alpha or beta) or parasym- pathetic nervous system in several in vitro and in vivo preparationGo and intravenous encainide does not significantly affect heart rate or blood pressure in ca- nine” or human4.12 subjects.
Our data can be explained by one or more metabo- lites of encainide that exert electrophysiologic effects different from those of the parent compound. Fur- thermore, one of the active metabolites could have slow channel blocking effects, accounting for the substantial effects on A-V nodal function caused by oral encainide therapy. Alternatively, the effects of oral encainide therapy might result from tissue accumulation of the parent compound. However, the rapid metabolism of encainide (half-life approximately 3 hour@) makes the latter explanation unlikely.
Role of metabolites in oral encainide’s electro- physiologic effects: Recent reported data support the hypothesis that one or more metabolites are responsible for much of the electrophysiologic effects of oral en- cainide therapy. In a study of 11 patients who had fre- quent premature ventricular complexes the investiga- tors” found an unusually wide range of minimal effective (antiarrhythmic) plasma encainide concentration in the 10 responding patients. One patient had no change in electrocardiographic intervals or frequency of prema- ture ventricular complexes after encainide therapy. That patient eliminated encainide much more slowly than did the other patients (half-life 13.6 hours) and was
ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL.
the only patient who had no detectable plasma O- demethyl encainide. The same laboratory subsequently demonstrated that doses of 0-demethyl encainide, one-tenth as large as encainide, lengthened the QRS interval and prevented aconit,ine-induced ventricular tachycardia in rats.” In another study5 involving pa- tients who had frequent premature ventricular com- plexes, the minimal effective plasma encainide con- centration was lower and duration of antiarrhythmic activity longer when encainide was administered orally than when administered intravenously. The investiga- tors also found a longer elimination half-life for several demethylated metabolites of encainide than for the parent compound.
The cellular electrophysiologic effects of two me- tabolites, MJ 14030, a 3 methoxy 4 hydroxy metabolite, and MJ 9444, the 0-demethyl metabolite, were studied in isolated canine cardiac Purkinje fibers.l:j Like en- cainide, both compounds depressed o,,,, propagation velocity and action potential duration and all failed to suppress slow channel-dependent action potentials induced in K+-depolarized catecholamine-treated fi- bers. No compound altered automaticity arising from low levels of resting potential induced by current in- jection using the single sucrose gap technique. There- fore, although these metabolites may have an important antiarrhythmic role, their cellular electrophysiologic effects do not explain the lengthening of atria1 and ventricular refractoriness or the depression of A-V nodal conduction that occurs after oral encainide adminis- tration.
In summary, oral encainide, or possibly one or more of its metabolites, causes substantial electrophysiologic effects in several types of cardiac tissue that are not affected by single dose intravenous encainide therapy.
Acknowledgment
We thank Elizabeth Darling, RN for her assist.ance during the electrophysiologic studies; Nancy Lineback and Bettie McCloud for their assistance in the preparation of the man- uscript; and Robert Mayol, PhD, Mead Johnson Pharma- ceutical Division, for performing the drug assays.
1.
2.
3.
4.
5.
6.
References
Byrne JE, Gomoll AW, !&Kinney GR. Antiarrhythmic properties of MJ 9067 in acute animal models. J Pharmacol Exp Ther 1977;200:147-54. Encainide: Investigator’s Brochure. Evansville, Indiana, Mead Johnson Pharmaceutical Division, 1979: p 3-9. Roden DM, Duff HJ, Wang T, Woosley RL. Contribution of a me- tabolite to the ECG and antiarrhythmic actions of encainide (abstr). Circulation 1980;62:Suppl lll:1ll-141. Kestelott H, Stroobandt l?. Clinical experience of encainide (MJ 9067): a new antiarrhythmic drug. Eur J Clin Pharmacol 1979; 16:323-6. Winkle RA, Peters F, Kates RE, Tucker C, Harrison DC. Clinical pharmacology and antiarrhythmic efficacy of encainide in patients with chronic ventricular arrhythmias. Circulation 1981;64:290- 6. Roden DM, Reele SB, Higgins SB, Mayo1 RF, Gammans RE, Oates JA, Woosley RL. Total suppression of ventricular arrhythmias by
10.
11.
encainide: pharmacokinetic and electrocardiographic character- istics. N Engl J Med 1980;302:877-82. Sami M, DeBusk R, Kraemer H, Houston N, Harrison D. Evaluation of antiarrhythmic efficacy of encainide and quinidine (abstr). Cir- culation 1979;6O:Suppl ll:ll-184. Heger JJ, Nattel S, Rinkenberger R, Zipes DP. Encainide therapy in patients with drug-resistant ventricular tachycardia (abstr). Cir- cuiation 1979;6O:Sippl ll:ll-185. Heaer JJ. Prvstowskv ‘EN. Jackman WM. Naccarelli GV. Zi~es DP:Repeiiti& ventri&lar iachycardia: clinical and electroph&i- ological characteristics (abstr). Circulation 1980;62:Suppl lll:lll- 321. Mason JW, Peters FA. Antiarrhythmic efficacy of encainide in patients with refractory recurrent ventricular tachycardia. Circu- lation 1981;63:670-5. Sami M, Mason JW, Oh G, Harrison DC. Canine electrophysiology of encainide, a new antiarrhythmic drug. Am J Cardiol 1979;43:
April 1, 1982 The American Journal of CARDIOLOGY Volume 49 1277

ELECTROPHYSIOLOGY OF ORAL ENCAINIDE-JACKMAN ET AL
1149-54. Heart 1920;7:353-70. 12. Sami M, Mason JW, Peters F, Harrison DC. Clinical eiectro-
physiologic effects of encainide, a newly developed ant&rhythmic agent. Am J Cardiol 1979;44:526-32.
13. Elharrar V, Zipes DP. Electrophysioiogic effects of encainide and two metabolites (abstr). Circulation 1981;64:Suppi IV:iV-272.
14. Janse MJ, van der Steen ABM, van Dam RTh, Durrer D. Refractory period of the dog’s ventricular myocardium following sudden changes in frequency. Circ Res 1969;24:251-62.
15. Han J, Moe GK. Cumulative effects of cycle length on refractory periods of cardiac tissues. Am J Physioi 1969;217:106-9.
16. Bazett HC. An analysis of the time-relations of electrocardiograms.
17. Mayoi RF, Gammans RE. Analysis of encainide in plasma by ra- dioimmunoassay and high pressure liquid chromatography. Ther- apeutic Drug Monitoring 1979;1:507-24.
18. Gibson JK, Somani P, Bassett AL. Eiectrophysiologic effects of encainide (MJ9067) on canine Purkinje fibres. Eur J Pharmacoi 197852:161-g.
19. Carmeiiet E. Eiectrophysiologicai effects of encainide on isolated cardiac muscle and Purkinje fibers and on the Langendorff-perfused guinea-pig heart. Eur J Pharmacoi 1980;61:247-62.
20. Encainide: investigator’s Brochure. in Ref 2: 20-21.
1278 April 1, 1982 The American Journal of CARDIOLOGY Volume 49