Embed Size (px)
Citation preview

1
PowerPoint Slides English Text Brazilian Portuguese Translation
Oncologic Emergencies: Part 1 VideoTranscript
Emergências Oncológicas: Primeira parte Roteiro para vídeo
Professional Oncology Education Oncologic Emergencies: Part 1 Time: 35:04
Educação Profissional em Oncologia
Emergências Oncológicas: Primeira parte Duração: 35:04
John Patlan, M.D. Associate Professor General Internal Medicine The University of Texas MD Anderson Cancer Center
John Patlan, M.D. Professor Associado Medicina Interna Geral MD Anderson Cancer Center – Universidade do Texas
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Oncologic Emergencies:Oncologic Emergencies:
Part IPart I
John Patlan, M.D.
Associate Professor
General Internal Medicine
Welcome! My name is John Patlan. I am a physician here at the University of Texas MD Anderson Cancer Center in the Department of General Internal Medicine, and I am going to talk to you today about oncologic emergencies. Our talk will be divided into two parts. This will be part 1, and please stay tuned for part 2. And we are going talk about the classic oncological cancer-related emergencies.
Bem-vindos! Eu sou John Patlan. Sou médico do Departamento de Medicina Interna Geral do MD Anderson Cancer Center, da Universidade do Texas e, hoje, falarei sobre emergências oncológicas. Nossa palestra consta de duas partes. Esta será a primeira parte. Fiquem alertas para a segunda parte. Falaremos sobre emergências oncológicas clássicas relacionadas ao câncer.

2
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
ObjectivesObjectivesObjectivesObjectives
• Be able to differentiate cancer-related and
non-cancer-related emergency problems
• Understand the common oncologic emergencies:
structural, infectious, hematologic and metabolic
problems
• Overview of the diagnosis and treatment of cancer-
related emergencies
Now, in our talk, I want to emphasize that all --- not all emergency problems are cancer-related. And I want you to be able to differentiate between cancer-related or oncologic emergencies and non-cancer-related emergency problems, which may also occur in cancer patients. But the focus of our talk will remain on oncologic or cancer-related emergencies, which are classically divided into structural problems, infectious problems, hematologic problems, and metabolic problems. And we will touch on each of those in turn, and I am going to give you an overview of how to diagnose and manage these problems in the emergency setting.
Nesta palestra, quero enfatizar que todos... que nem todos os problemas de emergência são relacionados ao câncer. E quero que vocês possam diferenciar as emergências oncológicas relacionadas ao câncer dos problemas emergenciais não relacionados ao câncer, que também podem acontecer em pacientes com câncer. Mas, o foco desta palestra continuará sendo emergências oncológicas ou relacionadas ao câncer, as quais são divididas tradicionalmente em problemas estruturais, infecciosos, hematológicos e metabólicos. E abordaremos cada uma ao seu tempo, além de dar um panorama geral de como diagnosticar e manejar esses problemas em situações de emergência.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Emergency Problems in Cancer PatientsEmergency Problems in Cancer PatientsEmergency Problems in Cancer PatientsEmergency Problems in Cancer Patients
• Don’t always assume that symptoms or
acute decompensation are due to the cancer
or its treatment
• Non-cancer-related problems
– Acute coronary syndromes, congestive heart failure,
arrhythmias (e.g. atrial fibrillation), COPD exacerbation,
GI bleeding
• Signs/symptoms may be blunted/masked
– Steroid use, neutropenia, advanced age
– Have a high pre-test probability of “badness”
Now, I do want to emphasize that you should not assume that the symptoms that the patient presents with, or whatever acute decompensation prompts their emergency room visit, is because of the cancer or its treatment. Cancer patients have all the same comorbid medical conditions that non-cancer patients do. So they present to the emergency center with chest pain, which may not be related to lung cancer. It could be an acute coronary syndrome. They may come in with shortness of breath, which is not because of pleural effusion, a malignant pleural effusion. It may be congestive heart failure. They come in with COPD exacerbations, cardiac arrhythmias, GI bleedings, all of the same non-cancer emergency problems that other patients present with. It is important to keep in mind. The other caveat that I want you to remember is that in cancer patients, the signs and symptoms of disease may be blunted or masked. The things that are you classically taught to look for
Agora, quero enfatizar que não devem presumir que os sintomas apresentados pelo paciente, ou qualquer descompensação aguda que motive seu comparecimento ao pronto-socorro, se devem ao câncer ou seu tratamento. Os pacientes com câncer apresentam todos os quadros clínicos comórbidos que os que não sofrem de câncer também apresentam. Então, eles comparecem ao pronto-socorro com dor no peito, que talvez não esteja relacionado a câncer pulmonar. Poderia ser uma síndrome coronariana aguda. Eles podem chegar com falta de ar, que não é causada por efusão pleural, uma efusão pleural maligna. Pode ser insuficiência cardíaca congestiva. Eles chegam com exacerbações da doença pulmonar obstrutiva crônica, arritmias cardíacas, hemorragias gastrintestinais, todos os mesmos problemas emergenciais de origem não canceroso que outros pacientes apresentam. É importante ter isto em mente. A outra advertência que gostaria que

3
to try to rule in or rule out some diagnosis may be difficult to find in cancer patients, and this happens for a lot of reasons. One – steroid use. A lot of the patients receive corticosteroids as part of their treatment, which blunts the inflammatory response, which mediates a lot of the signs and symptoms you are taught to look for. For instance, patients with an acute abdomen may come in and have very little of its classical guarding or rebound that you may be expecting. Neutropenia similarly blunts the inflammatory response, and so patients could have fairly significant infections yet have very little objective findings to suggest that. They may have pneumonias with minimal or absent infiltrate on chest x-ray, for example. Also, cancer happens more often in elderly patients. So, all patients with advanced age may present with more subtle signs and symptoms of disease. So, one thing I ask all practitioners to remember is that you should have a higher pre-test probability of badness, and by that I mean whatever the worst diagnosis that this that could be leading to this symptom or this presentation, have a higher pre-test probability for that. So, if you think some test is indicated to evaluate for that, you might go ahead and order the test, because it is harder to figure out in cancer patients without that.
lembrassem é que, em pacientes com câncer, os sinais e sintomas da doença podem aparecer enfraquecidos ou disfarçados. Talvez seja difícil encontrar nos pacientes com câncer o que lhes ensinaram a buscar, como regra geral, para tentar confirmar ou descartar um ou outro diagnóstico, e são várias as razões. Primeiro, o uso de esteroides. Muitos pacientes recebem corticosteroides como parte do tratamento, que enfraquecem a resposta inflamatória, que media muitos dos sinais e sintomas que nos ensinaram devíamos buscar. Por exemplo, os pacientes com abdome agudo podem chegar e apresentar muito pouco da resistência [abdominal] ou descompressão [brusca] que tipicamente esperaríamos. De maneira semelhante, a neutropenia enfraquece a resposta inflamatória e os pacientes poderiam ter infecções bastante significativas, todavia, apresentam poucos achados objetivos que pudessem sugerir isso. Por exemplo, podem apresentar pneumonias com infiltrados mínimos ou ausentes nas radiografias torácicas. Além disso, o câncer ocorre com mais frequência em pacientes idosos. Portanto, a manifestação dos sinais e sintomas de todos os pacientes de idade avançada pode ser mais sutil. Algo que peço aos médicos para lembrarem é que deve haver uma probabilidade mais alta no pré-teste para malignidade e, com isso, quero dizer qualquer que seja o diagnóstico, mesmo o pior, para este caso e que pudesse levar a este sintoma ou aquela manifestação, usem a maior probabilidade para o pré-teste. Se vocês acreditam que um determinado exame é indicado para avaliá-lo, vão em frente e prescrevam o teste, porque, em pacientes com câncer, o diagnóstico é mais difícil sem ele.

4
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Oncologic (CancerOncologic (CancerOncologic (CancerOncologic (Cancer----related) Emergenciesrelated) Emergenciesrelated) Emergenciesrelated) Emergencies
• Problems due to the underlying malignancy
or its treatment:
– Structural problems
– Metabolic problems
– Hematologic problems
– Infectious problems
Now, the remainder of our talk will be focused on the classic oncological cancer-related emergencies. As I mentioned, the --- this topic is classically divided into four sections: structural problems, metabolic problems, hematologic problems, and infectious problems. So, all of the rest of the talk at this point will be talking about emergency problems that are due to the cancer, the underlying cancer, or its treatment.
O restante da nossa palestra se concentrará nas emergências oncológicas clássicas relacionadas ao câncer. Como já havia mencionado, este assunto é dividido em quatro seções: problemas estruturais, metabólicos, hematológicos e infecciosos. Neste momento, o restante da apresentação versará sobre problemas de emergência decorrentes do câncer, o câncer subjacente ou seu tratamento.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Structural ProblemsStructural ProblemsStructural ProblemsStructural Problems
• Compression, obstruction, or invasion of
vital structures:
- Spinal cord compression
- Superior vena cava syndrome
- Brain metastases/cerebral edema
Now, structural problems are fairly easy to understand. A cancer mass lesion can compress or obstruct or invade some vital structure. The things that are typically included in the oncologic emergencies lecture are spinal cord compression, superior vena cava syndrome, and [I will] also talk about cerebral metastasis with associated edema, because that is a fairly common and urgent problem as well.
Os problemas estruturais são bastante fáceis de entender. A lesão da massa cancerosa pode comprimir ou obstruir ou invadir algumas estruturas vitais. O que normalmente são incluídas nas apresentações sobre emergências oncológicas são: a compressão da medula espinhal, a síndrome da veia cava superior e [também] falarei a respeito da metástase cerebral com edema associado, porque este também é um problema bastante comum e urgente.

5
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord Compression: EtiologySpinal Cord Compression: EtiologySpinal Cord Compression: EtiologySpinal Cord Compression: Etiology
• Metastatic tumor from any primary site, most
from tumors with tendency to metastasize to
spinal column
• Breast, lung, and prostate cancer most common
• Usually from tumor with spread to vertebral
body and direct extension into epidural space,
compression of thecal sac
• Radiologic definition: indentation of thecal sac
So, spinal cord compression is a fairly common problem. And this is usually occurs because patients have metastatic disease, which can really be from any primary site. But breast cancer, lung cancer because they are very common, prostate cancer because it is also common, and all of which tend to have bony metastasis, are the most common causes of this. And so what happens is that the patient develops a bony metastasis to --- usually to the vertebral body that extends directly into the epidural space and then compresses the spinal cord. If you see radiologically that you have epidural extension of tumor and indentation of the thecal sac, that is a radiologic definition of spinal cord compression whether or not the patient has associated clinical symptoms.
A compressão da medula espinhal é um problema bastante comum. E, geralmente, ocorre porque os pacientes apresentam doença metastática, que, na verdade, pode originar-se de qualquer sítio primário. Mas, por serem muito comuns, o câncer de mama e o de pulmão, bem como o de próstata que também é comum, e porque todos eles tendem a apresentar metástases ósseas, são as causas mais comuns disto. O que acontece é que o paciente apresenta metástase óssea... geralmente, do corpo vertebral, que se estende diretamente ao espaço epidural e, depois, comprime a medula espinhal. Se em uma radiografia puderem ver uma extensão epidural do tumor e indentação do saco dural, isso é a definição radiológica de compressão da medula espinhal de um paciente com ou sem sintomas clínicos associados.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord CompressionSpinal Cord CompressionSpinal Cord CompressionSpinal Cord Compression
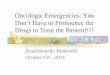
• MRI preferred imaging mode
• Arrows indicate metastatic
disease at T5 and T12
extending posteriorly into
spinal canal, compressing
the cord (C)
Now, this is going to require a radiologic study to diagnose this. The MRI is the preferred imaging mode. On this sample MRI, you can see that the arrows indicate two vertebral bodies, which are markedly different than the others. They are less dense. There is a compression fracture in the higher vertebral body. And you can see where the spinal cord is labeled C that there is some compression of the spinal cord by the tumor, which is indenting the thecal sac. So, that is radiologic spinal cord compression.
Mas, para poder ser diagnosticado, será necessário um estudo radiológico. A ressonância magnética é a modalidade preferencial de [estudo por] imagem. Nesta amostra de ressonância magnética, pode-se ver que as setas indicam dois corpos vertebrais, que são notadamente diferentes dos outros. São menos densos. Nota-se uma fratura por compressão no corpo vertebral superior. E pode-se ver que a medula espinhal está identificada com "C", indicando certa compressão da medula espinhal pelo tumor, que causa uma indentação do saco dural. Essa é a compressão da medula espinhal radiológica.

6
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord Compression: Symptoms and SignsSpinal Cord Compression: Symptoms and SignsSpinal Cord Compression: Symptoms and SignsSpinal Cord Compression: Symptoms and Signs
• Range of presentations
• Asymptomatic with radiologic findings
• Back pain at affected level without neurologic
compromise
- 70% thoracic
- 20% lumbosacral
- 10% cervical
- Pain worse with recumbency, valsalva
Now, clinically, there can be a whole range of presentations. It is hard to imagine, but some patients can be fairly asymptomatic, yet have that same kind of radiologic presentation that I just showed you. They may have a little bit of back pain, but it may not be striking, but an asymptomatic patient with that kind of MRI is uncommon, but possible. What is more common is that patients will present with back pain. Almost all of them will present with back pain. One clue that this is different than the typical garden-variety low back pain, which is one of the most common causes for any patient to seek medical attention, is that this is typically located in thoracic vertebral column. Some will be lumbosacral. Some will be cervical. Another clue this is a different kind of back pain is that this pain may be worse with recumbency or with valsalva, which is not typical for ordinary lumbosacral sprain.
Mas, do ponto de vista clínico, pode haver uma grande variação de manifestações sintomatológicas. É difícil imaginar, mas alguns pacientes podem ser bastante assintomáticos e, mesmo assim, apresentarem o mesmo tipo de características radiológicas que acabei de mostrar. Pode ser que sintam um pouco de dor nas costas, mas talvez não chame a atenção. Embora possível, um paciente assintomático com esse tipo de RM é raro [de acontecer]. O mais comum é que os pacientes apresentem lombalgia. Quase todos apresentaram lombalgia. Um indício de que é diferente de uma típica lombalgia comum, que é um dos principais motivos pelos quais o paciente busca atenção médica, é de ser localizada especificamente na região torácica da coluna vertebral. Algumas serão na região lombossacral; outras, na região cervical. Outro indício seria que a lombalgia pode piorar na posição reclinada ou com [manobra de] Valsalva, o que não é comum no entorse lombossacral comum.

7
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord Compression: Symptoms and SignsSpinal Cord Compression: Symptoms and SignsSpinal Cord Compression: Symptoms and SignsSpinal Cord Compression: Symptoms and Signs
• Motor weakness below level of compression
• Sensory deficits less common
- Sensory level may be 1-5 levels below level
of compression
• Bowel and bladder dysfunction - usually
urinary retention
Now, as things progress, they may develop neurologic compromise. So, they can find --- they can have motor weakness below the level of compression. An even more advanced sign of cord compression would be the development of sensory deficits. It is very difficult sometimes to localize a level of compression, and your objective sensory level may be several levels below where the cord is actually compressed. A very late sign would be bowel or bladder dysfunction. The thing that you would usually find will be urinary retention.
À medida que a doença progride, pode haver comprometimento neurológico dos pacientes. Eles podem encontrar.... podem apresentar debilidade motora abaixo do nível da compressão. E, inclusive, um sinal mais avançado da compressão da medula [espinhal] seria a ocorrência de déficit sensorial. Às vezes, é muito difícil localizar um nível de compressão e o nível sensorial objetivo talvez se localize vários níveis abaixo do ponto de compressão da medula espinhal. Um sinal bastante tardio seria a disfunção do intestino ou da bexiga. O que geralmente observamos é retenção urinária.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord Compression: Diagnosis Spinal Cord Compression: Diagnosis Spinal Cord Compression: Diagnosis Spinal Cord Compression: Diagnosis and Treatmentand Treatmentand Treatmentand Treatment
• Rapid radiologic diagnosis and initiation of treatment
is necessary to preserve neurologic function
- Initiate corticosteroids - EX: dexamethasone 10-20
mg IV then 4-6 mg Q6hrs
• MRI of affected spinal region
• CT myelogram is option if MRI contraindicated
Vecht CJ et al. Neurology 1989 39(9):1255
So, once you suspect this diagnosis, because of new or worsening back pain that is atypical or the patient is developing some neurologic compromise, it is urgent that you perform a radiologic study to establish the radiologic diagnosis. And, even when the diagnosis is suspected, even before the MRI is performed, it is reasonable to initiate corticosteroids to try to preserve neurologic function. Dexamethasone is the usual steroid that we choose. The optimal dose is really not defined. There has never really been any randomized control trial to give us the optimal dose. Standard dosing, however, usually is somewhere between a 10 to 20 mg bolus. Some people have used up to 100 mg or higher in patients with severe neurologic compromise and then some scheduled divided dose after that. You will need to get an urgent MRI as I mentioned. If patients can’t get an MRI because they have got a pacemaker or they have metal in their body or there is some other contraindication,
Depois de suspeitarmos deste diagnóstico, por causa de uma lombalgia nova ou pior que é atípica ou pelo paciente apresentar certo comprometimento neurológico, é urgente realizarmos um estudo radiológico para estabelecer o diagnóstico radiológico. E, mesmo quando houver suspeita do diagnóstico, mesmo antes de realizar uma RM, é razoável iniciar corticosteroides para tentar preservar a função neurológica. A dexametasona é o esteroide comum de escolha. Na realidade, a dose ideal não está definida. Nunca foi realizado um estudo randomizado com controle para se obter a dose ideal. No entanto, a dose padrão fica em torno de 10 mg a 20 mg administrada em bolus. Algumas pessoas administraram até 100 mg ou mais em pacientes com comprometimento neurológico grave e, depois, há quem tenha programado administrar a dose dividida. Vocês devem obter uma RM urgentemente, como já mencionei. Se os pacientes não puderem fazer uma

8
you can get a CT myelogram. RM porque usam marca-passo ou por terem algum metal no corpo ou por alguma contraindicação, peçam uma TC ou um mielograma.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord Compression: TreatmentSpinal Cord Compression: TreatmentSpinal Cord Compression: TreatmentSpinal Cord Compression: Treatment
• Radiation therapy for most
• Neurosurgical decompression
- If previously irradiated, or if spinal
stabilization is needed
- Decompression + RT superior
to RT alone
• Chemotherapy may be option for extremely
chemosensitive tumors
Now, once you have diagnosed this, once you have gotten your radiologic study, you see that there is indentation of the thecal sac, they will require some urgent treatment. Hopefully, you have already initiated corticosteroid therapy. Most patients will be treated with radiation treatment. A neurosurgeon should always be involved for consultation, and if the patient has been previously irradiated because of known vertebral metastasis, or if their spine is unstable, they will probably require neurosurgical intervention. You will see listed in various textbooks that chemotherapy is an option for very chemosensitive tumors such as germ cell tumors or lymphomas. In real life, most patients will receive steroids and radiation treatment up front.
Uma vez realizado o diagnóstico, uma vez obtido o estudo radiológico, observa-se que há uma indentação no saco dural [e] eles precisarão de tratamento urgente. É de esperar que vocês já tenham iniciado terapia com corticosteroides. A maioria dos pacientes receberão radioterapia. Deve haver sempre um neurocirurgião disponível para consultas e, se o paciente já recebeu a irradiação por ter apresentado metástase vertebral ou instabilidade na espinha dorsal, é provável que precise intervenção neurocirúrgica. Vocês verão em livros textos indicações de quimioterapia como opção para tumores muito quimiossensíveis, como tumores de células germinativas ou linfomas. Na vida real, a maioria dos pacientes recebe tratamentos com esteroides e irradiação já no início.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Spinal Cord Compression: PrognosisSpinal Cord Compression: PrognosisSpinal Cord Compression: PrognosisSpinal Cord Compression: Prognosis
• Prognosis depends on neurologic status at time of diagnosis
• If ambulatory, 80-100% chance of retaining ambulation
• If paretic, 1/3 may walk; only 6% if paraplegic
• Pain symptom often precedes onset of neurologic deficits by weeks
– Consider MRI in high-risk patients with new/worsening back pain
Helweg-Larsen S et al. Eur J Cancer 1994 30A(3):396
Now, the prognosis depends upon whatever the neurologic status is at the time of diagnosis and when treatment is initiated. If the patients are ambulatory, there is a very good chance that they will be able to walk out of the hospital if they walked into your emergency room. If they do have some weakness, some lower extremity weakness, however, only about a third of them will remain ambulatory after we finish their treatment. If they are completely paraplegic, the prognosis is not good, only 6% will regain locomotion. Now, as I have described it to you, I mentioned that there is a whole range of symptoms from very little symptoms with radiologic cord compression, to back pain, to the development of motor weakness, to the development of sensory deficits, and finally to bowel and bladder dysfunction. This process from pain to
O prognóstico depende da condição neurológica no momento do diagnóstico e quando for iniciado o tratamento. No caso de pacientes ambulatoriais, há uma boa chance de que possam sair caminhando do hospital se chegaram caminhando ao pronto-socorro. Porém, se apresentarem alguma fraqueza, debilidade dos membros inferiores, somente uma terça parte deles permanecerá na condição ambulatorial depois do término do tratamento. Se estiverem completamente paraplégicos, o prognóstico não será bom, somente 6% recuperarão a locomoção. Como já descrevi, há toda uma série de sintomas, de muito poucos sintomas com compressão radiológica da medula à lombalgia, à manifestação de fraqueza motora, à manifestação de déficits sensoriais e, finalmente, à disfunção do intestino e da bexiga. Este processo

9
neurologic compromise develops typically over a period of weeks. In one study, patients who are ultimately diagnosed with cord compression were asked to identify when did they develop new and worsening back pain and, on average, it was probably six to seven weeks when the back pain started. Now, that is good news and bad news. The bad news is patients were developing cord compression and it took six or seven weeks to be able to figure that out. The good news is that, in general, this is a kind of a subacute process, and so, you have time to work with. So, if you have a high-risk patient, say a patient with metastatic prostate cancer, known vertebral metastasis, or a patient with some other high risk cancer with known bony metastasis and they have some suspicious clinical sign or symptom, new or worsening back pain, even if they don’t yet have neurologic compromise, consider getting an MRI. It is not an emergency. You don’t have to do it immediately, but if you can get it within the next 24-48 hours as long as they are neurologically intact, that would be reasonable.
da dor até o comprometimento neurológico desenvolve-se ao longo de semanas. Em um estudo, solicitou-se a pacientes que haviam sido diagnosticados com compressão da medula que identificassem o momento do primeiro aparecimento da lombalgia ou o agravamento dela, caso já a apresentassem, e o início dessa dor, em média, foi de seis a sete semanas. Isto representa boas e más notícias. É uma má notícia porque os pacientes sofriam de compressão da medula e levou seis ou sete semanas para perceber o problema. A boa notícia é que, em geral, este é um tipo de processo subagudo e, por conseguinte, temos tempo para resolvê-lo. Então, no caso de um paciente de alto risco, suponhamos um paciente com câncer de próstata com metástase ou um paciente com outro câncer de alto risco com metástase óssea diagnosticada e que apresentasse algum sinal ou sintoma clínicos sugestivos, o aparecimento ou o agravamento de uma lombalgia, mesmo não apresentando comprometimento neurológico, considerem pedir uma RM. Não é uma emergência. Não há necessidade de fazê-la imediatamente, mas seria razoável se puderem fazê-la nas próximas 24 a 48 horas, sempre que a sua condição neurológica se mantenha intacta.

10
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Superior Vena Cava Syndrome: EtiologySuperior Vena Cava Syndrome: EtiologySuperior Vena Cava Syndrome: EtiologySuperior Vena Cava Syndrome: Etiology
• Obstruction of the venous drainage from the
head and upper extremities
• Invasion or external compression of the SVC
by tumor or lymph nodes, and/or by thrombosis
within the SVC
• Thoracic malignancy cause of 60-85% of
cases – others due to intravascular devices
• SVC obstruction as presenting symptom of
undiagnosed tumor in 60% of cases
Now, the next structural emergency we are going to talk about is superior vena cava syndrome. I will tell you superior vena cave syndrome, while it is always presented in the classic oncologic emergencies lecture, strictly speaking is not a real emergency. It is an urgent problem, but also a subacute problem that develops over a period of at least weeks. Now, this happens because you have, usually because you have some tumor that is causing obstruction of venous drainage from the head and upper extremities. Usually, there is a mass or lymphadenopathy in the mediastinum that causes external compression or sometimes invasion and thrombosis of the superior vena cava. And because this is a thoracic or mediastinal problem, thoracic malignancies, such as lung cancers or sometimes lymphomas, are the primary cause of this. Occasionally, we will also see it as a complication of the presence of a central venous catheter causing some intraluminal stenosis or thrombosis. Now, one problem that you will encounter is that vena cava obstruction, when patients present with this --- this is the presenting sign or symptom of their diagnosis in about 60% of the time. In other words, about 60% of patients with superior vena cava syndrome do not yet have a tissue diagnosis. This is the presenting feature of their disease, and this becomes a problem, as you will see in just a minute.
A próxima emergência estrutural sobre a qual falaremos será a síndrome da veia cava superior. Saibam que a síndrome da veia cava superior, embora seja sempre apresentada nas emergências oncológicas clássicas, a rigor, não é uma emergência verdadeira. É um problema urgente, mas também é um problema subagudo que se desenvolve ao longo de, pelo menos, algumas semanas. Isto acontece porque, geralmente, existe um tumor que obstrui a drenagem venosa da cabeça aos membros superiores. Geralmente, uma massa ou linfadenopatia no mediastino causa compressão externa ou, às vezes, invasão e trombose da veia cava superior. E porque este é um problema torácico ou do mediastino, as principais causas são as neoplasias malignas do tórax, como cânceres ou, às vezes, linfomas pulmonares. De vez em quando, o vemos, também, como uma complicação da presença de um cateter venoso central, causando estenose ou trombose intraluminal. Um problema com o qual vocês irão se deparar é a obstrução da veia cava. Quando os pacientes a apresentarem, esse seria o sinal ou sintoma apresentado no diagnóstico em cerca de 60% dos casos. Ou seja, cerca de 60% dos pacientes com síndrome da veia cava superior ainda não têm nenhum diagnóstico tecidual. Esse é o sintoma característico da doença e torna-se um problema, como poderão ver em um minuto.

11
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Superior Vena Cava Syndrome: Superior Vena Cava Syndrome: Superior Vena Cava Syndrome: Superior Vena Cava Syndrome: Symptoms and SignsSymptoms and SignsSymptoms and SignsSymptoms and Signs
• Dyspnea most common symptom
• May report facial swelling (worse with lying down),
cough, arm edema
• May see venous distension of neck and chest
wall, facial edema and/or plethora
• Rarely, obtundation or stridor
So, when they come in, they can have a variety of symptoms, they may complain of shortness of breath, more specifically, they may have some facial swelling, some cough, some edema of the upper extremities. Since this process develops over a subacute period of time or period of weeks, you develop collateral vessels over the anterior chest wall and the neck. They frequently have some edema or plethora of the face. Very rarely, if the patients are very, very advanced, they may be obtunded if they have complete obstruction of the cerebral venous drainage, or, if they have airway compromise, they can have stridor. But that is very rare and you will likely never see that in clinical practice.
Quando [os pacientes] chegam, podem apresentar diversos sintomas, queixar-se de falta de ar, mais especificamente, poderão apresentar um pouco de tosse e edema na face e nos membros superiores. Uma vez que este processo se desenvolve ao longo de um intervalo subagudo de semanas, ocorre a formação de veias colaterais na parede torácica anterior e no pescoço. Frequentemente, apresentam um pouco de edema ou pletora na face. Muito raramente, caso os pacientes estejam muito, muito avançados, podem apresentar obnubilação se a obstrução da drenagem venosa cerebral for completa ou, se houver comprometimento das vias respiratórias, podem apresentar estridor. Porém, isso é muito raro e, talvez nunca o vejam na prática clínica.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
SVC Syndrome: BeforeSVC Syndrome: BeforeSVC Syndrome: BeforeSVC Syndrome: Before
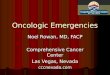
So, here is a picture of a man with superior vena cava syndrome. I will show you later an after picture after treatment. But I think in this picture you can appreciate that his face is kind of plethoric and ruddy, and when I show you the after picture, you will also appreciate how puffy, swollen, and edematous his face is.
Esta é uma foto de um homem com síndrome da veia cava superior. Depois, mostrarei uma foto tirada após o tratamento. Mas, acho que nesta foto, vocês podem perceber que o seu rosto aparece um pouco pletórico e corado, e quando mostrar a foto tirada posteriormente, poderão perceber o aspecto inchado e edematoso do rosto.

12
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Superior Vena Cava Syndrome: DiagnosisSuperior Vena Cava Syndrome: DiagnosisSuperior Vena Cava Syndrome: DiagnosisSuperior Vena Cava Syndrome: Diagnosis
• Chest CT with contrast can define level and extent
of venous obstruction, presence of SVC thrombosis,
and cause of obstruction
• MRI for patients with contrast allergy
So, when a patient comes in, they have got these kinds of signs or symptoms, you probably have already had a chest x-ray showing some kind of mediastinal mass. What you will need to get is a chest CT with contrast so that you can understand the level and extent of the venous obstruction and see whether there is any associated thrombosis of the superior vena cava. If patients have an iodinated contrast allergy, you get an MRI with gadolinium.
Quando o paciente chegar apresentando esses sinais e sintomas, talvez, vocês já tenham uma radiografia do tórax que mostre algum tipo de massa no mediastino. O que precisam fazer é uma TC do tórax com contraste para poder entender o nível e a extensão da obstrução venosa e ver se existe alguma trombose associada à veia cava superior. Se os pacientes tiverem alergia ao contraste com iodo, vocês poderão fazer uma RM com gadolínio.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Superior Vena Cava Syndrome: TreatmentSuperior Vena Cava Syndrome: TreatmentSuperior Vena Cava Syndrome: TreatmentSuperior Vena Cava Syndrome: Treatment
• Tissue diagnosis is necessary to choose optimal therapy
• Prebiopsy radiation can obscure histology
• Intraluminal stents can provide rapid relief of symptoms, does not preclude subsequent therapy
Now, the problem, as I mentioned to you, is that most of these patients do not yet have a tissue diagnosis. They may have a non-small cell lung cancer. They may have a lymphoma. Those will both be treated very differently, and optimal therapy really is going to depend upon the treatment of the underlying cancer. So, you are going to need to get a tissue diagnosis. Now, when they come in and they have got this clinical problem, what was frequently done in the past was to do urgent radiation treatment. The problem with that, is that if you get radiation before you have obtained a biopsy and establish a tissue diagnosis, that can obscure your histology and really limit your ability to treat the patient effectively in the future. So, if the patient requires rapid relief of their symptoms, they have got fairly significant vena cava obstruction, you can put in an intraluminal stent to open up the vena cava and provide some venous drainage and that will not preclude any subsequent therapy that you are able
O problema é que, como já havia dito, a maioria dos pacientes ainda não têm um diagnóstico tecidual. Pode ser que apresentem câncer de pulmão de células não pequenas. Podem ser portadores de linfoma. Aqueles que apresentarem ambas as doenças serão tratados de maneira muito diferente, e a terapia ótima dependerá do tratamento do câncer subjacente Por isso, precisarão obter um diagnóstico tecidual. Anteriormente, quando os pacientes chegavam com esse problema clínico, o que se fazia muito era o tratamento radioterápico de urgência. O problema disso é que, ao realizar a irradiação antes de obter a biópsia e de estabelecer o diagnóstico tecidual, os resultados da histologia não são claros e limitam nossa capacidade de oferecer um tratamento eficaz ao paciente. Por conseguinte, se o paciente precisar de alívio imediato dos sintomas, [por] apresentar uma obstrução bastante significativa da veia cava, poderemos colocar uma endoprótese intraluminal

13
to do. para abrir a veia cava e drenar um pouco a circulação, mas isso não impede que possamos realizar outra terapia subsequentemente.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
SVC Stenting by Interventional RadiologySVC Stenting by Interventional RadiologySVC Stenting by Interventional RadiologySVC Stenting by Interventional Radiology
This is a picture of a stent being placed by an interventional radiologist. On the left-hand picture, you can see a catheter being threaded from below and a blush of contrast is being injected to outline the superior vena cava and the venous circulation. On the right-hand side, you see the stent that has been deployed.
Esta é uma foto de uma endoprótese colocada por um radiologista intervencionista. Na foto à esquerda, podem ver um cateter sendo trançado por baixo e um contraste sendo injetado para demarcar a veia cava superior e a circulação venosa. À direita, podem ver a endoprótese já implantada.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
SVC Syndrome: AfterSVC Syndrome: AfterSVC Syndrome: AfterSVC Syndrome: After
And here is the after picture of that same patient. So, you see on the right-hand picture, his face is much less red. He is much less puffy, and although he is not smiling in that picture, I am sure he is very, very happy that you have helped him and made him feel much better by relieving his obstruction.
E aqui está a foto posterior do mesmo paciente. Podem ver na foto à direita que seu rosto está muito menos vermelho. Não está tão inchado e, embora não esteja sorrindo nessa foto, tenho certeza de que está muito, muito feliz de que o tenham ajudado a sentir-se muito melhor ao aliviar a obstrução.

14
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Superior Vena Cava Syndrome: TreatmentSuperior Vena Cava Syndrome: TreatmentSuperior Vena Cava Syndrome: TreatmentSuperior Vena Cava Syndrome: Treatment
• Lymphoma, germ cell tumors, small cell lung
cancer usually responsive to chemotherapy +/-
radiation therapy
• Non-small cell lung cancer - poor prognosis -
treatment aimed at palliation of symptoms
(endovascular stent or RT)
• Questionable efficacy of RT to re-establish SVC
patency
So, as I mentioned, because this is a thoracic problem, it is caused by thoracic tumors, lymphomas, germ cell tumors, small cell lung cancers. Those are usually very chemosensitive. And so chemotherapy with or without radiation is going to be the mainstay of treatment. Unfortunately, the majority of patients will probably have a non-small cell lung cancer. It is a poor prognostic sign when patients present with non-small cell lung cancer and superior vena cava syndrome. So, really you are going to be aimed at treating --- palliating their symptoms. Now, there have been questions raised recently about how effective radiation treatment really is at re-establishing SVC patency, but even when it does not re-establish full patency, it does provide significant relief of symptoms, so it is still frequently done.
Como já tinha dito, por tratar-se de um problema torácico, é causado por tumores torácicos, linfomas, tumores de células germinativas e cânceres de pulmão de pequenas células. Geralmente, são muito quimiossensíveis. Por isso, a quimioterapia com ou sem irradiação será o pilar do tratamento. Infelizmente, é provável que a maioria dos pacientes seja portadora de câncer de pulmão de células não pequenas. É um sinal de prognóstico ruim quando os pacientes apresentam câncer de pulmão de células não pequenas e síndrome da veia cava superior. Nesse caso vocês devem se concentrar em tratar... em aliviar os sintomas. Ultimamente, tem-se questionado a eficácia da radioterapia no restabelecimento da permeabilidade da veia cava superior, mas mesmo quando sua permeabilidade não é restabelecida completamente, oferece alívio significativo dos sintomas e, por isso, é frequentemente realizada.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Superior Vena Cava Syndrome: PrognosisSuperior Vena Cava Syndrome: PrognosisSuperior Vena Cava Syndrome: PrognosisSuperior Vena Cava Syndrome: Prognosis
• Unless tracheal obstruction, not immediately
life-threatening
• Mortality related to underlying malignancy
The prognosis is really related to the underlying malignancy. If it is a good prognosis cancer, such as a curable lymphoma or a germ cell tumor, then the prognosis may be very good. If it is an advanced but incurable disease, like a metastatic or locally advanced non-small cell lung cancer, prognosis is not so good. One of the take-home messages that I want you to leave with though, is that, although it is always discussed in the oncologic emergencies lecture, this is not really an emergency problem. It is usually not immediately life-threatening unless there is tracheal obstruction or severe cerebral edema with mental status changes. But as I mentioned, that is very rare, so again a subacute problem, you have time to do your job.
O prognóstico está relacionado ao câncer subjacente. Se o câncer tiver um bom prognóstico, como um linfoma curável ou um tumor de células germinativas, então, o prognóstico poderá ser muito bom. Se for uma doença em estado avançado, mas incurável, como o câncer de pulmão de células não pequenas com metástase ou avançado, o prognóstico não será tão bom. Uma das lições que gostaria que levassem para casa é que, embora sempre se discuta nas palestras sobre emergências oncológicas, este não é um problema de emergência. Geralmente, não põe em risco a vida do paciente de forma imediata, a menos que haja obstrução da traqueia ou grave edema cerebral com alterações da condição mental. Mas, como já mencionei, isso é muito raro; então, repito, é um problema subagudo e temos tempo de fazer nosso

15
trabalho.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Cerebral Metastases/EdemaCerebral Metastases/EdemaCerebral Metastases/EdemaCerebral Metastases/Edema
• Patients may present with headache, focal
neurologic symptoms, seizures, or sometimes
idiopathic nausea/vomiting
• Tumors produce vasogenic edema
• Diagnosis: imaging by CT or MRI
• Initiate corticosteroids to decrease edema
The next structural problem we are going to talk about is cerebral metastasis, unfortunately, a very common problem and sometimes not easy to diagnose. Patients can present with a whole range of symptoms: headaches, sometimes focal neurologic symptoms, sometimes intermittent or transient neurologic symptoms. Patients may have a suspected transient ischemic attack when really it is a tumor that is causing this problem. They may have seizures, occasionally sometimes just idiopathic nausea and vomiting, which is likely related to cerebral edema. So, if patient --- if a patient with a cancer comes in and they have got nausea or vomiting and there is no good reason for it, they are several weeks out from chemotherapy, they are not hypercalcemic, consider cerebral metastasis is a cause. Now, a lot of this --- in general, the symptoms that are produced by the tumors are in large part mediated by the vasogenic edema of the tumor, so relief of that edema is going to help you with symptom management. When you have a patient and you suspect that this may be the problem, you are going to need to get an imaging study. If you don’t have much time to work, you can get a CT scan. A more definitive study would be an MRI. And it will be important to initiate corticosteroids to reduce edema to try to get control of their symptoms.
O próximo problema estrutural do qual falaremos é a metástase cerebral. Infelizmente, um problema muito comum e, às vezes, não muito fácil de diagnosticar. Os pacientes podem apresentar vários sintomas: cefaleias, às vezes, sintomas neurológicos focais, outras vezes, sintomas neurológicos intermitentes ou transientes. Os pacientes podem apresentar ataques isquêmicos transientes sugestivos quando a causa do problema for realmente um tumor. Podem apresentar convulsões e, de vez em quando, apenas náuseas e vômitos idiopáticos, provavelmente relacionados ao edema cerebral. Se um paciente com câncer chegar com náuseas e vômitos e não houver uma boa razão para isso, se já fizer várias semanas que não recebem quimioterapia e não estiverem hipercalcêmicos, então, considerem a causa como sendo metástase cerebral. Muito disto.... em geral, os sintomas produzidos pelos tumores são mediados, em grande parte, pelo edema vasogênico do tumor. Então, o alívio do edema facilitará o manejo dos sintomas. Quando suspeitarmos que esse possa ser o problema do paciente, devemos pedir um estudo por imagem. Se não houver muito tempo, podemos pedir uma TC. Um estudo mais definitivo seria uma RM. E será importante iniciar terapia com corticosteroides para reduzir o edema e tentar controlar os sintomas.

16
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
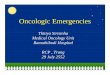
• MRI T1 unenhanced image
(upper left) showing edema
• Contrast-enhanced images
(other 3) showing enhancing
lesions (w/ arrows)
• Distinguish from other
CNS lesions?
Cerebral Metastases/EdemaCerebral Metastases/EdemaCerebral Metastases/EdemaCerebral Metastases/Edema
So, this is an MRI showing a patient with multifocal brain metastasis. On the upper left-hand view, this is --- that is non-contrast enhanced lesions, and I think even the non-radiologists among us can appreciate there is some asymmetry between the two sides. There is some hypodensity on one side that is not seen on the other. And on the other three images, which are enhanced with gadolinium contrast, you see the arrows pointing to the multifocal enhancing lesions. So this is unfortunately a --- unfortunately a patient with multifocal brain metastasis.
Esta é uma RM de um paciente com metástase multifocal do cérebro. Na parte superior esquerda, há... são lesões com realce sem contraste e acredito que, mesmo aqueles entre nós que não somos radiologistas, podemos perceber uma certa assimetria entre os dois lados. Há certa hipodensidade em um lado que está ausente no outro. E, nas outras três imagens, com realce por contraste com gadolínio, podem ver as setas que indicam as lesões multifocais com realce. Infelizmente, este é um paciente com metástase multifocal do cérebro.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
• Corticosteroids reduce edema/improve symptoms
within hours
• Dexamethasone preferred due to lack of
mineralocorticoid activity, lower side effect profile
• 10 mg bolus, followed by 16 mg divided BID-QID
Vecht CJ et al. Neurology 1994 44(4):675
Cerebral Metastases/EdemaCerebral Metastases/EdemaCerebral Metastases/EdemaCerebral Metastases/Edema
Now, what you are going to do is, in the immediate emergency phase, you are going to start them on corticosteroids to try to reduce the edema, improve their symptoms. They can work very dramatically and very quickly. Just within a few hours patients can feel much, much better. We generally use dexamethasone because of its lack of mineralocorticoid activity. If patients have cerebral edema and some increased intracranial pressure, you would not want to give them a steroid that could potentially further raise their blood pressure, intracranial pressure. And again, as in spinal cord compression, the optimal dosing is not really defined, but, in general, a 10 to 20 mg dose as a bolus followed by a divided dose over a period of time.
O que devemos fazer é, na fase de emergência imediata, iniciar o paciente com corticosteroides para procurar reduzir o edema e melhorar os sintomas. [Os corticosteroides] podem agir muito rápida e intensamente. Apenas em poucas horas, os pacientes já se sentem muito, muito melhor. Geralmente, utilizamos dexametasona por não apresentar atividade mineralocorticoide. No caso de os pacientes apresentarem edema e aumento da pressão intracraniana, não seria recomendável administrar esteroides, pois poderiam aumentar ainda mais a pressão arterial e a pressão intracraniana. E, novamente, como no caso da compressão da medula espinhal, a dose ideal ainda não foi definida, mas, em geral, é uma dose de 10 mg a 20 mg administrada em bolus, seguida de uma dose dividida durante um certo tempo.

17
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Corticosteroids for Cerebral EdemaCorticosteroids for Cerebral EdemaCorticosteroids for Cerebral EdemaCorticosteroids for Cerebral Edema
• Prevent complications of corticosteroid therapy
(GI prophylaxis, manage hyperglycemia)
• Be aware of side effects (mental status changes,
myopathy, risk of infection, e.g. PCP)
• Subsequent dosing lowest possible dose to control
edema, minimize side effects
• If significantly increased ICP, need other measures
(mannitol, BP control, fluid restriction)
Now, because your patient with cerebral metastasis is going to remain on corticosteroids for some period of time, it is going to be important for you to try to remember to try to prevent the complications of corticosteroid therapy. Prevent ulcer formation with some acid suppression. You are going to be aware and look for hyperglycemia should it occur and it occurs very commonly. And you should be aware that corticosteroids can have less commonly recognized side effects, mental status changes. Sometimes patients just feel sort of wired and excited. Sometimes they can be frankly psychotic. Over a long period of time, they can develop some steroid myopathy. Unfortunately, the only treatment for that is withdrawal of steroids, and, if patients are maintained on steroids for a longer period of time, they have an increased risk of opportunistic infections such as pneumocystis carinii, so they may require some prophylaxis for that. So, because of these problems, we will try to minimize --- or lower the dose as we can to try to control their edema, yet minimize these side effects. And, if in the emergency setting, patients have very significantly increased intracranial pressure, they are developing some focal neurologic findings, their mental status is declining, you are going to need more urgent measures to control their intracranial pressures such as mannitol, fluid restrictions, and neurosurgical consultation.
Desde que o paciente com metástase cerebral permanecerá com corticosteroides por algum tempo, é importante não nos esquecermos de evitar as complicações decorrentes da terapia com corticosteroides. Evitar a formação de úlceras com supressores de ácido. Devemos estar alertas e observar a ocorrência de hiperglicemia, que é muito comum. E devemos estar cientes de que os corticosteroides podem apresentar efeitos colaterais e alterações menos reconhecíveis no estado mental. Às vezes, os pacientes ficam um pouco ansiosos e empolgados. E, francamente, outras vezes, se mostram psicóticos. Durante um longo período, podem apresentar miopatias por esteroides. Infelizmente, o único tratamento para isso é a retirada dos esteroides e, se os pacientes os receberem por muito tempo, correrão maior risco de adquirir infecções oportunistas, como por Pneumocystis carinii, para a qual precisarão tratamento profilático. Por causa desses problemas, procuraremos minimizar.... ou reduzir a dose enquanto procuramos controlar o edema e minimizar os efeitos secundários ao mesmo tempo. E, em situações de emergência, ocorre um aumento muito significativo da pressão intracraniana nos pacientes. Manifestam alguns achados neurológicos focais, seu estado mental declina, [e] vocês terão de usar medidas mais urgentes para controlar a pressão intracraniana, como [o uso de] manitol, restrição de líquidos e consulta com o neurocirurgião.

18
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Cerebral Metastases: PrognosisCerebral Metastases: PrognosisCerebral Metastases: PrognosisCerebral Metastases: Prognosis
• Depends on age, performance status, extent
of extracranial disease
• Favorable prognosis: survival 7.1 months
• Poor prognosis: survival 2.3 months
Gaspar LE et al. Int J Radiat Oncol Biol Phy 2000 47(4):1001
So, the prognosis is not good. This is a bad place to have your cancer, so it really depends upon the patient’s overall status, their age, their performance status, and how likely it is that their treating oncologist is going to be able to get control of their extracranial disease. And in general, patients are divided into favorable or poor prognosis. If they have favorable prognosis, based on those factors that I mentioned, survival is about seven, a little over seven months. Poor prognosis, they have more advanced age, poor performance status, very widespread systemic disease, then survival is only about two months.
Então, o prognóstico não é bom. Não é um bom local para ter câncer. Por isso, depende da condição geral do paciente, da sua idade, do seu estado funcional e da probabilidade de que o oncologista responsável possa vir a controlar a doença extracraniana. Em geral, os pacientes se classificam segundo apresentem prognóstico favorável ou desfavorável. No caso de apresentarem prognóstico favorável, com base nos fatores que mencionei, a sobrevida é cerca de sete, um pouco mais de sete meses. Prognóstico desfavorável: são pessoas de idade mais avançada, estado funcional comprometido, doença sistêmica muito disseminada, a sobrevida é de somente uns dois meses.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Metabolic ProblemsMetabolic ProblemsMetabolic ProblemsMetabolic Problems
• Hypercalcemia
• Hyperuricemia/tumor lysis syndrome
• Hyponatremia
- Paraneoplastic SIADH
• Hyperkalemia
- Spurious elevation if high WBC
- Renal insufficiency/tumor lysis
So, next we are going to talk about metabolic problems. We see a lot of metabolic problems, both in and out of the hospital in cancer patients. Common problems include hypercalcemia, hyperuricemia, or Tumor Lysis Syndrome, hyponatremia, which is probably the most common electrolyte disturbance of --- in any hospital, and hyperkalemia, which can happen for variety of reasons. We are really going to focus our discussion on hypercalcemia and Tumor Lysis Syndrome.
A seguir, falaremos sobre problemas metabólicos. Vemos muitos problemas metabólicos em pacientes com câncer, tanto dentro quanto fora do hospital. Dentre os problemas comuns estão a hipercalcemia, a hiperuricemia ou síndrome da lise tumoral, a hiponatremia, que talvez seja o distúrbio eletrolítico mais comum em qualquer hospital, e a hiperpotassemia, que pode ocorrer por diversas razões. O foco da nossa discussão será sobre hipercalcemia e síndrome da lise tumoral.

19
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
HypercalcemiaHypercalcemiaHypercalcemiaHypercalcemia: Etiology: Etiology: Etiology: Etiology
• Common in cancer pts 10-20% of cases
• May occur in solid tumors or leukemia,
lymphoma, myeloma
• Most common in myeloma, breast, lung CA
• Increased bone resorption, release of Ca++
– Paraneoplastic: release of PTH-related
protein (PTHrP)
– Osteolytic metastases
So, hypercalcemia is a very, very common problem. It occurs in up to 20% of all cancer patients and can occur across a whole range of tumor types: leukemia patients, lymphoma patients, a variety of solid tumor patients such as breast cancer, lung cancer patients. And it can happen for variety of reasons. Intuitively, it can happen because the patient may have osteolytic metastases and then release of calcium that has been locked up in the bones there. But more commonly it happens through paraneoplastic means, because the tumor can produce a parathyroid-related protein, which is sort of a false hormone, which then causes release of calcium from the bone into the circulation.
A hipercalcemia é um problema muito, muito comum. Pode ocorrer em até 20% de todos os pacientes com câncer e pode ocorrer em uma ampla variedade de tipos de tumor: pacientes com leucemia, com linfoma, com diversos tumores sólidos, como câncer de mama e de pulmão. E pode ocorrer por diversas razões. Intuitivamente, pode ocorrer porque o paciente pode apresentar metástase osteolítica e, depois, pela liberação do cálcio que estava depositado nos ossos. Mas, ocorre principalmente por meios paraneoplásicos porque o tumor pode produzir uma proteína relacionada à paratireoide, que atua como um falso hormônio, o qual, por sua vez, causa a liberação do cálcio dos ossos para a circulação.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Hypercalcemia: SymptomsHypercalcemia: SymptomsHypercalcemia: SymptomsHypercalcemia: Symptoms
• Generalized weakness, lethargy, fatigue
• Nausea/vomiting, constipation, anorexia
• Mental status changes, sedation,
cognitive dysfunction
• Polyuria/polydipsia, dehydration
• Hypertension, shortened QT interval
The symptoms early on are kind of nonspecific and more --- as the hypercalcemia progresses they become more pronounced. In general, patients complain of kind of generalized weakness, they are lethargic. They are fatigued and they may have some nausea, vomiting, constipation, and anorexia. This is all very nonspecific, and this is probably the typical symptom profile of any cancer patient that is getting active treatment. As things get more advanced and the serum calcium gets higher and higher, they may start to develop some mental status changes; may be very sedated, sleeping, you know, 12 to 18 hours a day, and may have some cognitive dysfunctions: difficulty concentrating, saying things that don’t make sense, maybe hallucinating. And because hypercalcemia impairs your ability to repair --- to reabsorb free water, patients develop polyuria and polydipsia and virtually all patients who have clinically significant hypercalcemia are significantly volume-depleted
No início, os sintomas não são muito específicos e mais... à medida que a hipercalcemia evolui, tornam-se mais pronunciados. Em geral, os pacientes se queixam de um tipo generalizado de fraqueza e ficam em estado letárgico. Sentem fadiga e podem ter um pouco de náusea, vômito, constipação e anorexia. Tudo isto não é muito específico e, talvez, seja o perfil sintomatológico típico dos pacientes com câncer que se encontram no período de tratamento ativo. À medida que a doença continua avançando e o cálcio sérico aumenta cada vez mais, os pacientes podem começar a apresentar alterações no estado mental; talvez, estejam bem sedados, dormindo, de 12 a 18 horas por dia e possam apresentar disfunções cognitivas: dificuldade de concentração, dizem coisas sem sentido, talvez tenham alucinações. E porque a hipercalcemia compromete a capacidade do reparo... de reabsorver água livre, os pacientes apresentam poliúria e polidipsia e, finalmente, todos

20
and dehydrated by the time they present to you. In various textbooks, you will also see hypertension as a manifestation of hypercalcemia and shortened QT interval and a predisposition to arrhythmias as a risk. Although, in clinical practice, this is virtually never seen.
os pacientes com níveis significativos de hipercalcemia se encontram significativamente hipovolêmicos e desidratados quando chegam para serem examinados. Além disso, em vários livros textos, observa-se a hipertensão como manifestação de hipercalcemia e menor intervalo QT, além de predisposição para arritmias como risco. Embora, na verdade, isso não aconteça na prática clínica.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Hypercalcemia: TreatmentHypercalcemia: TreatmentHypercalcemia: TreatmentHypercalcemia: Treatment
• Increase urinary calcium excretion
- Isotonic saline (lots of it)
- Loop diuretics?
- Replace other electrolyte loss (K+, Mg++)
- Will lower calcium quickly
Suki et al. N Engl J Med 1970 283(16):836
Now, what you should do when the patient comes in, you have identified them as having significant hypercalcemia for which they are symptomatic. If they have kidneys that work, you are going to need to increase their urinary calcium excretion. As I mentioned, virtually all of these patients are volume-depleted, so they are going to require a lot of volume replacement. So just give them lots and lots of isotonic saline. This will facilitate some calcium uresis. Now, traditionally, we have also used loop diuretics in conjunction with saline. This is one of the very few indications for concomitant administration of both saline and diuretics. There is actually very little evidence for that. There are really no randomized controlled trials. The use of this is based on some old studies from the 1960s. We still do it, but if you do do it, be sure to try to replace other electrolytes which may be depleted such as potassium or magnesium. Now, saline calciuresis will help you quickly and in the short term, but it is not a very potent treatment. So, it will bring down your calcium, but it will not bring you down close to normal just yet.
Mas, o que fazer quando o paciente chega e identificamos que tem hipercalcemia significativa para a qual é assintomático. Se tiver rins funcionais, teremos que aumentar a excreção do cálcio urinário. Como já mencionei, praticamente, todos estes pacientes apresentam hipovolemia e, por isso, precisarão de reposição de volume. Por conseguinte, administrem muito soro isotônico. Isso facilitará, em parte, a diurese do cálcio. Tradicionalmente, usamos diuréticos de alça com o soro fisiológico. Esta é uma das poucas indicações para a administração concomitante de soro fisiológico e diuréticos. Na realidade, há muito pouca evidência para essa prática. Não há estudos randomizados controlados. Seu uso fundamenta-se em alguns antigos estudos da década de 1960. Ainda a aplicamos, mas se forem usá-la, não se esqueçam de substituir outros eletrólitos que podem estar reduzidos, como o potássio e o magnésio. A calciurese salina servirá de ajuda rápida e solução de curto prazo, mas não é um tratamento muito potente. Permitirá a redução do cálcio, mas não será suficiente para retorná-lo aos valores normais.

21
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Hypercalcemia: TreatmentHypercalcemia: TreatmentHypercalcemia: TreatmentHypercalcemia: Treatment
• Inhibit bone resorption
• SQ Calcitonin Q6-12hrs
- Onset within 4-6 hours
- Duration 48 hours (development of tachyphylaxis)
• Bisphosphonates: IV zoledronic acid > pamidronate
- Quicker infusion over 15 min (vs 2-24 hours)
- Onset 24-72 hrs, duration 3-4 weeks
- Caution in renal insufficiency, all bisphosphonates associated with osteonecrosis of jaw with chronic usage (1-15%?)
You may require some other treatment, which is to --- which is really going to try to turn off the problem at its source. As I mentioned to you, the problem is usually paraneoplastic, because you have excessive bone reabsorption and release of calcium from the bone where most of it is stored. The most potent treatment you have available to you is at the bottom of the page here, which is bisphosphonate therapy. A variety of bisphosphonates are available. The one that is probably most commonly used these days is zoledronic acid or Zometa®. The reason it is popular is because it can be used --- it can be infused quickly over about 15 minutes or so as opposed to pamidronate, which is one of the older bisphosphonates, which required a much longer infusion up to 24 hours. The problem with all the bisphosphonates though is they have a slow onset of action. You are really not going to get any peak onset for several days, but they will last for a long time, in general for about 3 to 4 weeks. So, saline diuresis gives you a quick treatment, but not very potent. Bisphosphonates give you a potent treatment, but not very quick. What you can use, sort of in between, is calcitonin. This is delivered subcutaneously and has an onset of action of just a few hours. It will only last for maybe 24 to 48 hours. After that, you will develop --- the patients will develop tachyphylaxis and it will no longer work. And, in the patients with very severe hypercalcemia, you will probably require all three of these modes of therapy.
Teremos que lançar mão de outros tratamentos, com os que realmente se poderá resolver a origem do problema. Como já mencionei, normalmente, o problema é paraneoplásico porque há um excesso de reabsorção óssea e liberação de cálcio do osso onde se encontra armazenado em maior concentração. O tratamento disponível de maior potência está na parte inferior da página, que é a terapia com bifosfonato. Existem diversos bifosfonatos disponíveis. O que talvez seja o mais utilizado na atualidade é o ácido zoledrônico ou Zometa®. A razão da sua popularidade é porque pode ser utilizado rapidamente por infusão, em cerca de 15 minutos, ao contrário do pamidronato, que é um dos bifosfonatos mais antigos e que exige um tempo de infusão mais longo, de até 24 horas. Porém, o problema de todos os bifosfonatos é seu lento início de ação. Não conseguiremos nenhum pico inicial por vários dias, mas durará por longo tempo, em geral, por cerca de 3 a 4 semanas. A diurese salina propicia um tratamento rápido, mas não muito potente. Os bifosfonatos oferecem um tratamento potente, mas não muito rápido. O que podemos usar como tratamento intermediário seria a calcitonina. Ela é administrada por via subcutânea e apresenta um início de ação de poucas horas. Talvez dure apenas por 24 a 48 horas. Depois disso, vocês... os pacientes apresentarão taquifilaxia e não funcionará mais. Nos pacientes com hipercalcemia muito grave, talvez precisemos utilizar as três modalidades de terapia.

22
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Tumor Tumor Tumor Tumor LysisLysisLysisLysis Syndrome: DefinitionSyndrome: DefinitionSyndrome: DefinitionSyndrome: Definition
• Group of metabolic derangements that result from
high tumor burden/rapid cell turnover, release of
intracellular contents:
– Hyperkalemia
– Hyperphosphatemia
– Hypocalcemia (due to precipitation of CaPO4)
– Hyperuricemia (purine metabolite)
– Acute renal failure
Now, the next metabolic problem we are going to talk about is really only seen in cancer patients, and this is Tumor Lysis Syndrome. And by the name syndrome, obviously we are referring to a group of problems that tend to occur together. The basic underlying pathophysiology is that you have some bulky tumor with a high tumor burden and you have a rapid cell turnover and release of intracellular contents. So, you will have release of potassium, which is a primarily intracellular ion, release of phosphate, which is also primarily intracellular. And if patients have significant hyperphosphatemia that can then precipitate with calcium and so you have a secondary hypocalcemia. You have release of nucleic acids and purines, and that is metabolized to uric acid, so you develop hyperuricemia, and ultimately this can produce acute renal failure.
O próximo problema metabólico do qual falaremos será a síndrome da lise tumoral, que é observada somente em pacientes com câncer. Com o termo síndrome, obviamente, nos referimos a um grupo de problemas que tendem a ocorrer ao mesmo tempo. A fisiopatologia subjacente é um tumor volumoso com elevada carga tumoral, rápida renovação celular e liberação do conteúdo intracelular. Haverá liberação de potássio, que é, sobretudo, um íon intracelular, liberação de fosfato, que também é, principalmente, um [íon] intracelular. E, se os pacientes apresentarem hiperfosfatemia significativa a ponto de formar precipitados com o cálcio, se produzirá uma hipocalcemia secundária. Ocorre a liberação de ácidos nucleicos e purinas, que são metabolizadas a ácido úrico; com isso há formação de hiperuricemia, que, em última análise, produz a insuficiência renal aguda.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Tumor Tumor Tumor Tumor LysisLysisLysisLysis Syndrome: EtiologySyndrome: EtiologySyndrome: EtiologySyndrome: Etiology
• Most common with poorly differentiated lymphomas (Burkitt’s) and leukemias, ALL > AML
- Usually occurs after cytotoxic treatment
- May occur spontaneously
- Insoluble uric acid crystallizes in acidic urine, obstructs
renal tubules
• Has also been described in patients with myeloma, various solid tumors
So, as I mentioned, this is common in patients with high tumor burden. We typically see this in poorly differentiated lymphomas, like Burkitt’s and some leukemia patients with very high tumor burden, more commonly in acute lymphoblastic lymphoma, then acute myeloblastic lymphoma. Usually, this is something that occurs after treatment. This is usually a post-treatment problem. Rarely, but possibly, it can occur spontaneously. The classic would be a Burkitt’s patient. And what is happening is that you have this rapid cell turnover, release of intracellular contents, the purines get metabolized to uric acid, the uric acid is insoluble in acidic urine. And normal urine is acidic, so these uric acid crystals crystallize in the renal tubules and then start to obstruct the tubules and cause renal failure.
Como já mencionei, isso é comum em pacientes com elevada carga tumoral. Geralmente, observamos isso em linfomas muito pouco diferenciados, tipo Burkitt, e em alguns pacientes com leucemia e carga tumoral muito elevada, mais comumente no linfoma linfoblástico agudo e, depois, no linfoma mieloblástico agudo. Normalmente, isso ocorre após o tratamento. Normalmente, é um problema pós-tratamento. Mesmo raro, mas possível, pode ocorrer espontaneamente. O clássico seria o paciente com [linfoma de] Burkitt. No caso, temos uma rápida renovação celular, liberação do conteúdo intracelular, metabolização das purinas a ácido úrico e o ácido úrico é insolúvel na urina ácida. A urina normal é ácida, e os cristais do ácido úrico se cristalizam nos túbulos renais, que começam a ser obstruídos, causando insuficiência renal.

23
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
TLS: CairoTLS: CairoTLS: CairoTLS: Cairo----Bishop DefinitionBishop DefinitionBishop DefinitionBishop Definition
• Laboratory TLS: any 2 of the following…
– Uric acid > 8.0 mg/dL
– K > 6.0 mEq/L
– PO4 > 4.5 mg/dL
– Ca < 7 mg/dL
• Clinical TLS: Above, plus…
– Cr > 1.5 ULN, arrhythmia, seizure
Coiffier B et al. J Clin Oncol 2008 26(16):2767
Now, because all of these parameters, serum uric acid, potassium, phosphorous, calcium, they all exist on a continuum, we have criteria for diagnosing Tumor Lysis Syndrome. The criteria that I am showing you here is the Cairo-Bishop definition, which is the most commonly used definition for Tumor Lysis Syndrome. Patients are said to have Tumor Lysis, laboratory Tumor Lysis, if they satisfy any two of these criteria: the uric acid is above 8, potassium above 6, phosphorous greater than 4.5, or a calcium less than 7. Now, they are said to have clinical Tumor Lysis if they have any of those two plus the development of renal failure, and the usual criteria is creatinine is greater than 1.5 times the upper limit of normal, or because of hypocalcemia, they are developing arrhythmias or seizures.
Por causa de todos esses fatores — o ácido úrico, o potássio, o fósforo e o cálcio séricos, todos eles existem em uma série contínua —, dispomos de critérios para diagnosticar a síndrome da lise tumoral. Os critérios que estou mostrando aqui correspondem à definição de Cairo-Bishop, que é a definição mais utilizada para a síndrome da lise tumoral. Consideram-se pacientes com lise tumoral, lise tumoral laboratorial, os que satisfizerem dois dos seguintes critérios: níveis de ácido úrico acima de 8, potássio acima de 6, fósforo superior a 4,5 ou cálcio abaixo de 7. Diz-se que têm lise tumoral clínica se apresentarem dois desses critérios além de insuficiência renal. E o critério usual é o valor da creatinina ser 1,5 vezes maior do que o limite superior do valor normal, ou por causa da hipocalcemia, apresentam arritmias ou convulsões.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Tumor Tumor Tumor Tumor LysisLysisLysisLysis Syndrome: TreatmentSyndrome: TreatmentSyndrome: TreatmentSyndrome: Treatment
• After acute renal failure has occurred:
– Wash out obstructing uric acid crystals
– IV fluids and loop diuretics
– Use of recombinant uricase to catalyze insoluble uric acid to water-soluble allantoin
– Sodium bicarbonate not helpful at this stage to
alkalinize urine
– Hemodialysis if diuresis cannot be induced
• Best Treatment of TLS is Prevention
Now, the treatment of Tumor Lysis is difficult. If patients don’t present, don’t begin to receive treatment until after renal failure has occurred, then this is very difficult. You can try to hydrate them, give them some diuresis or some saline to try to wash out the obstructing uric acid crystals. This is another case where frequently we will give intravenous fluids and loop diuretics to try to facilitate washing out these crystals. You can also use a recombinant uricase, for instance rasburicase, to try to catalyze the destruction of the insoluble uric acid. And it will then form a water-soluble substance called allantoin. What is not helpful at this stage is administration of sodium bicarbonate. Recall that I mentioned to you that the uric acid crystals are insoluble in the normal acidic urine. What is intuitive is that, well, maybe if we alkalinize the urine by giving the patients sodium bicarbonate, that can
O tratamento da lise tumoral é difícil. Se os pacientes só começarem a receber tratamento após o aparecimento da insuficiência renal, então será muito difícil. Podemos tentar hidratá-los, administrar diuréticos ou soro fisiológico para desobstruir os cristais de ácido úrico. Este é outro caso em que, frequentemente, administramos líquidos via intravenosa e diuréticos de alça para tentar facilitar a eliminação dos cristais. Além disso, podemos utilizar uricase recombinante, por exemplo, a rasburicase, para tentar catalisar a destruição do ácido úrico insolúvel. Formará uma substância hidrossolúvel denominada alantoína. Neste ponto, o que não ajuda é administrar bicarbonato de sódio. Lembremos o que mencionei a respeito de os cristais de ácido úrico serem insolúveis na urina ácida normal. O que é intuitivo é que, talvez, se alcalinizássemos a urina fornecendo bicarbonato de

24
help present --- prevent the formation of these uric acid crystals and treat this problem. Unfortunately, once renal failure has also --- is already occurred, this is not helpful and just buys you more metabolic problems. So, I would not recommend it at this phase. If patients have very advanced disease and are not responding to the treatment that you have instituted so far, sometimes they will require hemodialysis. So really the best treatment of Tumor Lysis is prevention.
sódio aos pacientes, poderíamos evitar a formação dos cristais de ácido úrico e tratar o problema. Infelizmente, uma vez manifestada a insuficiência renal, não seria de ajuda alguma e só nos traria mais problemas metabólicos. Por isso, não o recomendo nesta fase. Se a doença estiver em estágio muito avançado e o paciente não responder ao tratamento prescrito, talvez precisem de hemodiálise. Portanto, o melhor tratamento para a lise tumoral é a prevenção.
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Tumor Tumor Tumor Tumor LysisLysisLysisLysis Syndrome: PreventionSyndrome: PreventionSyndrome: PreventionSyndrome: Prevention
• At-risk patients, before treatment
– Allopurinol for 2 days (xanthine oxidase inhibitor,
reduces production of uric acid)
– Consider recombinant uricase (rasburicase) for very
high risk pts
– Hydration +/- mannitol to maintain urine output >
2.5 L/day
– Urinary alkalinization to pH ≥ 7.0 with sodium bicarbonate controversial: no proven benefit vs
hydration alone
So, for high-risk patients like the ones that I have mentioned to you: leukemias, lymphomas, Burkitt’s patients; they generally get allopurinol before they begin treatment. This is a xanthine oxidase inhibitor. So, what will happen is that it will shunt the purines to a different pathway to reduce production of uric acid. Patients who are very high risk may be candidates for prophylactic administration of rasburicase, which is this recombinant uricase enzyme that I mentioned. They will also reduce the uric acid level. Patients who are coming in for treatment will --- who are considered to be high risk, will receive a lot of hydration, sometimes with mannitol to increase a very brisk urine output, at least 2 to 2.5 liters per day. The faster your urine flow is, the less likely it is that uric acid crystals will form. And, at this point, if you want to use bicarbonate to alkalinize the urine, this is the point when --- where it may be helpful to try to keep the urine pH above 7.0. To be honest with you though, there is no proven benefit for alkalinization versus hydration alone.
Então, os pacientes de alto risco, como os que já indiquei, aqueles com leucemias, linfomas, linfomas de Burkitt, geralmente, recebem alopurinol antes de começar o tratamento. Este é um inibidor da xantina oxidase. O que acontece é que o inibidor desvia as purinas para outra via metabólica e reduz a produção de ácido úrico. Os pacientes de risco muito alto podem ser candidatos para receberem profilaticamente a rasburicase, que é a enzima uricase recombinante da qual já falei. O nível do ácido úrico também é reduzido. Os pacientes que chegam para receber o tratamento e que são considerados de alto risco receberão um grande volume de líquidos para sua hidratação, às vezes, com manitol para aumentar a produção rápida de urina, pelo menos de 2 a 2,5 litros por dia. Quanto mais rápido o fluxo da urina, menor a probabilidade de formação de cristais de ácido úrico. Neste momento, se quisermos utilizar bicarbonato para alcalinizar a urina, este é o momento em que poderá ser oportuno para manter o pH da urina acima de 7,0. Sinceramente, não há prova alguma do benefício da alcalinização versus a utilização isolada da hidratação.

25
Oncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part IOncologic Emergencies: Part I
Oncologic (CancerOncologic (CancerOncologic (CancerOncologic (Cancer----related) Emergenciesrelated) Emergenciesrelated) Emergenciesrelated) Emergencies
• Problems due to the underlying malignancy or
its treatment:
– Structural problems
– Metabolic problems
– Hematologic problems
– Infectious problems
So, in summary, the oncologic emergencies include structural problems, which we have discussed, metabolic problems, which we have discussed. And, in Part 2 of this lecture, we will talk about hematologic problems and infectious problems. I thank you for your attention.
Resumindo, as emergências oncológicas incluem problemas estruturais, os quais discutimos, [e] problemas metabólicos, os quais discutimos. Na segunda parte desta palestra, falaremos sobre os problemas hematológicos e os infecciosos. Obrigado pela atenção.