Embed Size (px)
Citation preview

Emergency Department Throughput,Crowding, and Financial Outcomesfor HospitalsDaniel A. Handel, MD, MPH, Joshua A. Hilton, MD, Michael J. Ward, MD, MBA, Elaine Rabin, MD,Frank L. Zwemer, Jr, MD, MBA and Jesse M. Pines, MD, MBA, MSCE
AbstractEmergency department (ED) crowding has been identified as a major public health problem in theUnited States by the Institute of Medicine. ED crowding not only is associated with poorer patientoutcomes, but it also contributes to lost demand for ED services when patients leave without being seenand hospitals must go on ambulance diversion. However, somewhat paradoxically, ED crowding mayfinancially benefit hospitals. This is because ED crowding allows hospitals to maximize occupancy withwell-insured, elective patients while patients wait in the ED. In this article, the authors propose a moreholistic model of hospital flow and revenue that contradicts this notion and offer suggestions forimprovements in ED and hospital management that may not only reduce crowding and improve quality,but also increase hospital revenues. Also proposed is that increased efficiency and quality in U.S. hospi-tals will require changes in systematic microeconomic and macroeconomic incentives that drive thedelivery of health services in the United States. Finally, the authors address several questions to proposemutually beneficial solutions to ED crowding that include the realignment of hospital incentives, chang-ing culture to promote flow, and several ED-based strategies to improve ED efficiency.
ACADEMIC EMERGENCY MEDICINE 2010; 17:840–847 ª 2010 by the Society for Academic EmergencyMedicine
Keywords: crowding, financial management, hospitals, outcome and process assessment (healthcare)
E mergency department (ED) crowding is a prob-lem that affects the majority of U.S. hospitals.1
However, in most hospitals, ED crowding is nota constant phenomenon, but a cyclic one. At certaintimes of the day and week, there are insufficient spaceand human resources to care for new ED patients.2 In a2009 study of Pennsylvania EDs, 83% of medical direc-tors agreed that ED crowding was a problem in theirhospitals, but most reported that their EDs werecrowded less than 25% of the time and that fewer than25% of patients who were admitted were delayed formore than 4 hours.3 ED crowding has also been associ-ated with compromised patient care and safety. Crowd-ing is associated with delays in antibiotic therapy inpneumonia,4 delays in care for acute myocardial infarc-tion5 and many urgent and emergent conditions,6–9
higher rates of complications for patients admitted withchest pain,10 and increased mortality in the criticallyill.11,12 Two Australian studies demonstrated increasedmortality at hospital day 7 (hazard ratio 1.3)11 and hospi-tal day 10 (relative risk 1.34).12 Therefore, the mortality
ISSN 1069-6563 ª 2010 by the Society for Academic Emergency Medicine840 PII ISSN 1069-6563583 doi: 10.1111/j.1553-2712.2010.00814.x
From the Center for Policy and Research in Emergency Medi-cine, Department of Emergency Medicine, Oregon Health &Science University (DAH), Portland, OR; the Department ofEmergency Medicine, University of Pennsylvania (JAH), Phila-delphia, PA; the Department of Emergency Medicine, Univer-sity of Cincinnati (MJW), Cincinnati, OH; the Department ofEmergency Medicine, Mount Sinai School of Medicine (ER),New York, NY; the Emergency Medicine Section, McGuireVAMC, and the Department of Emergency Medicine, VirginiaCommonwealth University (FLZ), Richmond, VA; and theDepartment of Emergency Medicine, George Washington Uni-versity School of Medicine, and the Department of Health Pol-icy, George Washington School of Public Health (JMP),Washington, DC.Received November 25, 2009; revision received February 11,2010; accepted February 23, 2010.Presented at the Society for Academic Emergency Medicineannual meeting, New Orleans, LA, May 2009.Supervising Editor: David M. Cline, MD.Address for correspondence and reprints: Daniel A. Handel,MD, MPH; e-mail: [email protected].

risks of the crowding may not be directly felt by theemergency physician, but more by their inpatient col-leagues. While these data have not been replicated inother countries, the delays in care demonstrated bycrowding suggest that the same mortality risks exist else-where.
ED crowding is caused by an inability to move patientsefficiently through the process of care to another setting,whether it is home, to an inpatient floor, or anotherhospital. Inefficiencies within the ED that cause delays incare are one cause for crowding. Some EDs are notproperly staffed or sized to accommodate significantsurges in the typical patient volumes. However, the mostcited cause of crowding is the boarding of admittedpatients in the ED when there is insufficient inpatientbed capacity for ED admissions.13–19 As a result, EDboarders occupy ED beds, consume ED resources,and reduce the capacity for new patients. The greatestvolume of boarding occurs when ED admissions andnon-ED admissions compete for the same inpatientbed resources (typically early in the Monday-Fridayworkweek).20–22 But high hospital occupancy itself is notthe only cause for boarding. Other operational issuescause prolonged boarding times, such as the lack of flexi-bility between service areas (e.g., open hospital beds areavailable but not on the appropriate floor or reservedfor elective patients), inefficiency in care transfer (e.g.,delays in physician or nursing report), a desire byinpatient services for patients to remain in the ED foradditional services (e.g., consultation, laboratory testing,or radiography), and other nonclinical administrativeinefficiencies (e.g., delays in room turnover). To addressthis, organizations like the Institution for HealthcareImprovement (http://www.ihi.org/ihi) have proposedsolutions and diagnostic strategies to improve hospitalflow in addition to improvement in ED processes.23
It has been proposed that ED crowding and the hospi-tal practice of boarding benefit the hospital financiallydue to the imbalance between revenues from EDpatients and non-ED patients. Support for this proposalcomes from the 2006 Institute of Medicine report on hos-pital-based emergency care: ‘‘No major change in healthcare can take place without strong financial incentives,and today hospitals have almost no incentives to addressthe myriad problems associated with inefficient patientflow or ED crowding. Indeed ... hospitals have a number
of financial incentives to continue the practices that leadto these problems,’’24 and studies have addressed theeconomic incentives and disincentives for boarding, EDcrowding, and ambulance diversion.
The purpose of this paper is to summarize and syn-thesize the current literature on ED crowding andfinancial outcomes for hospitals and to present severalsolutions to both reduce ED crowding and improve thefinancial health of hospitals. This work is prepared onbehalf of the Society for Academic Emergency Medi-cine ED Crowding Interest Group.
A CONCEPTUAL MODEL FOR HOSPITALADMISSIONS AND LOST DEMAND
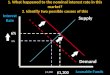
Patients are admitted to hospitals in three ways:through the ED, as direct admissions (which includesdirectly from clinics and scheduled procedures), or bytransfer from other health care facilities. The latter twocan be described together as non-ED admissions(Figure 1). In general, ED admissions generate a rela-tively stable demand for inpatient beds. Trended overtime, the number of daily inpatient admissions from theED is predictable. However, demand by service typecan vary, especially in large hospitals with morecomplex services (e.g., there may be variability inthe numbers of oncology admissions from the ED). Bycomparison, non-ED admissions demonstrate widerdifferences in the daily inpatient bed demands, inclu-ding intensive care unit beds.25 Elective admissionstypically mirror the Monday–Friday workweek withhigh numbers of admissions occurring during the weekand relatively few on weekends.
Long waits (either for ED admissions or non-EDadmissions) occur when there is insufficient bed capac-ity to meet demands. In operations-management terms,the concept of more demand than supply is known ascapacity-constraint. When the ED and hospital is atover- or near-capacity, long waits lead to ED patientsleaving without being seen (LWBS) or leaving beforecompleting treatment (LBCT). Additionally, some hospi-tals use ED wait times as criteria for ambulance diver-sion when patients being transported by ambulance aredirected to other hospitals. LWBS, LBCT, and ambu-lance diversion together can be described as lost EDdemand (Figure 1). A 2005 study estimated that the
Figure 1. Conceptual model of hospital demand with several sources of admissions.
ACAD EMERG MED • August 2010, Vol. 17, No. 8 • www.aemj.org 841

annual lost ED demand due to LWBS and ambulancediversion in one suburban teaching hospital exceeded$3 million.26 Similarly, long waits for non-ED admis-sions may also result in either lost demand (if a patientchooses another hospital or forgoes service use) ordeferred demand (if a patient chooses to wait until his/her case can be scheduled at a later date).
HOSPITAL OCCUPANCY AND REVENUES
Capacity constraint has become the norm in U.S. hospi-tals. This has been caused by the combination of hospitalclosures coupled with rising demand for services.27,28
From 1995 to 2005, annual ED visits in the U.S. increasedby 20% (from 96.5 to 115.3 million), and the ED utili-zation rate increased by 7% (from 36.9 to 39.6 ED visitsper 100 persons). Despite this increase in ED visits, thenumber of hospital EDs decreased by 381, the numberof U.S. hospitals decreased by 535, and the number ofhospital beds decreased by 134,000 during the samedecade.29
The imbalance between the hospital bed supply anddemand among surviving hospitals may be economi-cally advantageous for several reasons.30 Because hos-pitals operate with mostly fixed costs, the strategy thatmaximizes revenue is to maintain a full hospital.Assuming a favorable payer mix, an empty, staffed hos-pital bed is a missed revenue opportunity, much in thesame way that an empty airline seat or an unused hotelroom is lost revenue. However, if the hospital has apublic model with a greater uninsured population, thenthe converse is true in that filled beds may be a finan-cial liability. The strategy in the airline and hotel indus-try is to overbook because the industry calculates thatthe cost of an empty seat or room exceeds the cost ofthe service recovery from a displaced passenger orguest. Therefore, the fundamental economic principlein all these industries (including hospitals) is that main-taining high occupancy levels through surplus demandensures the greatest use of fixed resources and facili-ties.24 A 2009 study found a positive associationbetween ambulance diversion and hospital revenues.31
Periods of higher levels of ambulance diversion (a sur-rogate for full capacity) were associated with higherrevenues for the hospital, even at centers where EDadmissions were seen as more profitable than non-EDadmissions.31 Paradoxically, when hospital occupancyrates are greater than 85%, it has been shown that thewaiting time increases exponentially, which ultimatelyleads to lost demand as patients leave or are directedelsewhere.32 The business question then becomeswhich demand (ED or non-ED) is more expendable tomaintain a high occupancy level?
THE PROFITABILITY OF ED AND NON-EDINPATIENT ADMISSIONS
Studies have investigated whether ED inpatient admis-sions are more profitable than non-ED inpatient admis-sions.33,34 A 2009 study reported that ED admissionsresult in higher contribution margins (revenues minusdirect costs) than non-ED admissions in a single hospi-tal.33 However, a study in 2008 found that admissions
for Medicare beneficiaries admitted through the EDwere very unprofitable, while non-ED admissions werebarely profitable.34 Whether ED admissions are moreprofitable than non-ED admissions likely depends onlocal economics with regard to case mix, payer mix,and other externalities. For overall revenue, case mix isa critical matter because procedural care garners highpayments, and ED patients are less likely to have proce-dures than elective patients. In hospitals with high-volume elective procedures, non-ED admissions may beviewed as more profitable. Insurance prescreening ofelective admissions ensures better reimbursement thanfor unanticipated and frequently underinsured EDadmissions. In addition, local payment issues may alsoinfluence this calculation. There is one study that dem-onstrated higher profitability for ED patients in Massa-chusetts, which at the time of publication had a largeuncompensated care pool of funds available for EDpatients that may have been partly responsible for thefindings.33,35 Another example is in Pennsylvania,where workman’s compensation insurance pays hospi-tals 100% of the charges for severely injured traumapatients. This may make trauma diversion from EDcrowding result in largely negative swings in revenues.
However, there are several fundamental problemswith a one-to-one comparison of the profitability forED versus non-ED admissions. The first assumption,likely false, is that a non-ED admission will competewith and displace an ED admission on a one-for-onebasis. It is based on the premise that ED boarding iscaused only by the lack of bed availability, which is notthe case in many hospitals. Hospital operational ineffi-ciencies related to team assignment, differing opinionson when ED care has finished, and administrativedelays may also contribute to boarding. A second prob-lem with comparing ED to non-ED admission profitabil-ity is that there are cyclical supply and demand factors.Hospital occupancy varies considerably on a daily,weekly, and monthly basis, so that an ED admission isfrequently not competing with a non-ED admission.Even under the assumption that ED boarding is depen-dent only upon hospital occupancy, ED admissions dur-ing low occupancy times fill available capacity andallow hospitals to maintain high occupancy. Displacingand delaying non-ED admissions during high occu-pancy may be an effective strategy at specific times.The third issue in calculating the profitability for indi-vidual admissions is the matter of idiosyncrasies of hos-pital cost accounting, which can vary based on localaccounting practice.
THE ED AS A GATEWAY TO THE HOSPITAL
Over time, the ED has served as an increasing sourceof hospital admissions, going from 33% in 1993 toalmost 44% in 2006. In 2006, 49% of all admissions forpatients 18 and older were from the ED. During thisyear, 36% of admissions of 18- to 44-year-olds camefrom the ED, followed by 53% of 45- to 64-year-olds,55% of 65- to 84-year-olds, and 67% of the 85 and olderage group.36 Therefore, an alternative approach is totake a more holistic view of ED and hospital crowding.Rather than studying boarding in isolation, if the
842 Handel et al. • ED CROWDING AND FINANCES

ultimate goal is to maximize revenue, then any lostdemand (whether it is from an ED or non-ED source) isultimately undesirable. The immediate missed opportu-nities to capture revenue from ED admissions may becompounded if patients diverted to other institutionsultimately do not return to the diverting hospital forcare in the future. In addition, voluntary inpatient phy-sicians may decide to admit patients elsewhere ifadmissions through the ED prove cumbersome. Underthis more holistic view, ED boarding may not be justthe result of disordered incentives that entice hospitalsto overload the ED. Rather, systematic inefficienciesand incentives within hospitals lead to boarding, EDcrowding, and the negative outcomes that result. Thus,boarding may negatively affect a hospital’s bottom linethrough lost revenue as patients (both ED and non-ED)elect to go elsewhere or are directed elsewhereby ambulance diversion. By taking this alternativeapproach, we can start to consider what issues withinhospitals cause boarding and how understanding thereal causes can inform decisions to reduce boarding,increase ED efficiency, and maximize hospital revenue.
DISORDERED INCENTIVES AND HOSPITALCULTURES THAT PROMOTE NONFLOW
Hospitals are highly complex organizations with multi-ple stakeholders where often operational decision-makers are clinicians acting on their own authority orwithin a structured or semistructured set of complexhospital policies. Clinical work is by its nature highstress and unpredictable because it involves makingcomplex, often subjective decisions with incompleteinformation. Therefore, despite best intentions to struc-ture efficient operations, many minute-to-minutethroughput decisions are made at the bedside. And out-side of the ED, many clinicians often do not have per-sonal incentives to maintain high flow across thehospital.
While some clinicians have incentives based on pro-ductivity, many clinicians and other health care profes-sionals are compensated largely through fixed salaries.When paid a fixed salary, the financial incentive is tominimize new work because each additional work unitresults ultimately in a lower per unit pay. However, fewclinicians have direct incentives to increase their ownpersonal incremental utilization at the point of care andconsider flow through the entire system in bedsidedecision-making. This manifests as administrative ineffi-ciency, resulting in ED admission delays independent ofoverall hospital capacity. In many hospitals, the samelogic carries over to throughput for hospital admis-sions, critical procedures, testing, and hospital dis-charge. The overall effect of this disincentive is reducedflow through the entire system, and the behaviors thatensue, such as bed-blocking and delay tactics. ED andhospital crowding from disordered incentives results inlower revenue as demand is lost through the ED as thewhole process of care can be slowed by a culture ofinefficiency.
Another structural incentive that results in poorthroughput is the organization of hospitals into unitsthat sometimes only consider their own flow. Nonflow
in the ED caused by ED boarding may be viewed as anED problem, as opposed to a hospitalwide problem.However, nonflow in the ED may be caused at thatmoment by a backup in radiology, which is rarelyknown in real time to the radiologists who are inter-preting ED studies. A similar phenomenon may occurwith the laboratory or a floor charge nurse who maynot consider their personal decisions based on the flowthroughout the organization. Similarly, the ED may notrealize there are long waiting times for non-ED admis-sions or that elective cases may need to be canceled ifED flow does not improve. Finally, these rigid bound-aries between service lines can lead to an adversarial‘‘us v. them’’ culture that can lead each individual ser-vice to act in its own best interest and result in lowerflow and quality of care for patients in other locations.
SOLUTIONS FOR FIXING ED CROWDING,ALIGNING INCENTIVES, AND MAXIMIZINGREVENUE
Because hospitals are mostly fixed-cost organizations,when it comes to balancing the expected profits fromED versus non-ED patients, four questions emerge thatsuggest several potential solutions. Overall hospital rev-enues are the relevant outcome because from the per-spective of the entire hospital, allocating costs to oneparticular admission type becomes less meaningfulwhen considering the hospital as a whole.
Question 1: Should Hospitals Seeking to MaximizeRevenue Close Their EDs?In many settings, this is not a consideration due to reg-ulatory standards and requirements for hospitals tohave an ED. The answer is probably not. As mentionedbefore, this is also dependent on the payer mix seen inthe ED. With a high uninsured population at a publichospital, closing the ED would have a significant posi-tive effect on the financial bottom line, but may contra-dict the service mission of the institution. In contrast, aprivate hospital with a favorable ED payer mix may findthe ED as a profitable contributor to hospital opera-tions. Some capacity-constrained hospitals may be the-oretically viable without an ED, and certain institutions,such as subspecialty hospitals, choose not to have anED. But the financial, reputational, and operationalimpact of closing an ED in a general purpose hospitalmay not serve the institution’s best interests overall,regardless of perceived economic benefit. Even if netED revenues are not positive, longer-term financialbenefits from the loyalty of patients, voluntary physi-cians, and the community at large due to services avail-able in the ED may be great. Also, because of thecyclical nature of non-ED admissions and the relativeconstancy of ED admissions, ED admissions permitcapacity-constrained hospitals to maintain higher occu-pancy levels as the ED admission fills the gaps left bynon-ED admissions. Some nonconstrained hospitalsdepend on ED admissions to fill their capacity, andmany others find that ED admissions are more profit-able than their alternative admissions.33 In fact, Califor-nia hospitals with nontrauma EDs realize a loss on eachoutpatient ED visit, but a gain on each ED patient who
ACAD EMERG MED • August 2010, Vol. 17, No. 8 • www.aemj.org 843

is admitted as an inpatient. When the outpatient andinpatient effects are combined, hospitals with EDsderive an economic benefit from maintaining their EDs,and hospitals will even expand ED capacity if theexpanded capacity leads to an increase in hospitaladmissions.37
Question 2: For Hospitals That Choose to MaintainED Services, Which Bed Utilization and Prioritiza-tion Schemes Lead to the Highest HospitalRevenues?The current model in many hospitals is to scheduleelective admissions to hospital capacity (i.e., overbooklike the airline industry), allow unscheduled ED admis-sions to fill the gaps in specific service locations thathave beds, and permit overflow as ED boarding. In acapacity-constrained hospital, this minimizes lostdemand or deferred demand for elective cases whileED boarding results in lost ED demand and diversion.It allows the ED to be the buffer for hospital overflowbecause of the priority placed on non-ED patients.Aside from the clear association between this manage-ment practice and worse health outcomes,4,5,7,9,10 hospi-tals with high LWBS, LBCT, and ambulance diversionrates have considerable lost revenue from the ineffi-ciency of this bed prioritization scheme.26 This schemealso tends to have an inherent inefficiency: some peri-ods of increased boarding (and the resulting lost reve-nues) occur when inpatient beds are empty, reserved incase surgical patients need them and only released laterif they do not.
There are several alternative options for bed assign-ment and prioritization schemes that may reducecrowding and increase revenue. Two of these areadvanced bed allocation for ED admissions and increas-ing service-location flexibility. Because of the relativelystable demand for ED admissions, but the variabledemand by admission type, advanced bed allocationwould require an increase in the flexibility of inpatientfloors or intensive care units to handle variable types ofED admissions, operationally known as pooling. Then,allowing flexibility between service locations mayreduce the boarding associated with a lack of occu-pancy on a particular unit and allow hospitals to main-tain high occupancy in all staffed locations andultimately capture more ED demand. A second relatedconcept is to allow not only flexible capacity by servicelocation, but also flexible capacity of overall bed vol-ume. Because of the variable nature of the demand forinpatient beds, the ability to open and close inpatientbeds, such as through the use of a transition unit oralterative service locations (e.g., inpatient floor hallwaybeds) may reduce boarding and result in higher rates ofcapturing lost ED demand.38 The main barrier to imple-mentation of this scheme would likely be the neededflexibility in staffing.
Question 3: For Hospitals That Choose to MaintainED Services, Which Hospital Operations Manage-ment Interventions Lead to Reduced Variabilityand Improved Institutional Flow?In the ED, there have been several strategies proposedto increase ED operational efficiency. These include
immediate rooming of patients, bedside registration,advanced triage protocols, use of physicians ⁄ practitio-ners at triage, a dedicated ‘‘fast-track’’ service line,tracking systems and whiteboards, observation units,wireless communication devices, kiosk self check-in, EDdashboards, and personal health record technology(‘‘smart cards’’).39 While the revenue implications ofthese strategies are not known, implementing front-endoperational strategies that permit higher throughputwith the same physical space can reduce lost EDdemand due to inefficient ED operations and mayincrease overall revenue. Downstream from the ED inthe hospital, similar operational initiatives may beimplemented to streamline the admission process andreduce administrative barriers to bed placement.A 2007 paper in the operations literature demonstratedthat transferring admitted patients between hospitalfloors might be an effective strategy to alleviate board-ing and increase the utilization of existing hospitalcapacity.40 Implementing systems to improve communi-cation among departments (e.g., ED and radiology)might improve communication issues where individualdepartments are unaware of their roles in patient flowthrough the hospital.
Another effective strategy has been the concept ofreducing the variability in elective admissions, which inthe setting of elective surgery is termed surgical sche-dule smoothing or operating room (OR) schedulesmoothing. Surgical smoothing has been shown toreduce ED crowding and increase OR utilization ratesand likely will increase overall hospital revenues.40,41
However, the barrier to smoothing of elective admis-sions has been one of political power within hospitals.Because surgical services have great power due to theability of surgical specialties to generate demand, theimplementation of surgical schedule smoothing hasfailed in several hospitals. Individual surgical serviceshave balked at requests to alter OR scheduling becausethere is little incentive to improve ED and overall hospi-tal operations. However, in several centers wheresmoothing has been implemented, surgical serviceshave enjoyed reductions in surgery cancellations andmore predictable OR hours.42 As more such evidenceaccumulates, surgical services might become moreagreeable to smoothing OR schedules. However, hospi-tals will recognize a need to smooth the OR scheduleonly if they perceive the loss of revenue from EDcrowding to be greater than the potential loss of reve-nue from disgruntled surgical specialists who are freeto affiliate elsewhere. Where to begin in terms of oper-ational improvement depends on what are consideredthe greatest constraints for a particular institution,which only can be determined after review of all opera-tional processes. Using the theory of constraints logic,43
once it is determined what is the greatest bottleneck toefficient patient flow, this area should be addressedfirst.
In hospitals where incentives are not aligned to over-come the organizational culture or where there is nototherwise enough motivation to change the practice ofED boarding, external payment or policy regulationmay be necessary for efficient ED care. This is ofparticular significance to those hospitals that maintain
844 Handel et al. • ED CROWDING AND FINANCES

nonprofit status and receive tax subsidies from thelocal, state, and federal governments. These hospitalsare required to demonstrate community benefit. Themost visible role of an ED is the treatment of seriouslyill and injured patients.44 If an ED is crowded, boardingpatients, or diverting ambulances to other hospitals, itis not effectively serving the community. This may betaken into account when considering ‘‘community ben-efit standards.’’ Although most nonprofit hospital sys-tems do provide community benefits that are at leastequal to their tax subsidies, there is little standardiza-tion in the hospital industry with regard to quantifica-tion and reporting of those benefits. This has led to alack of credibility and ability to clearly demonstrate thebenefit provided.45,46 The threat of losing even a localtax subsidy may be enough to drive change in the larg-est health systems.
Question 4: How Can Hospitals Change Incentivesto Promote Flow and Reduce Lost Demand andRevenue From Inefficiency?Moving from problems to solutions will require betteraligning incentives across the hospital for improved flowthrough the entire system. Instead of the current state ofpermitting loss of ED demand in favor of non-ED admis-sions, efforts should be focused on improving through-put at all levels. Removing the bottlenecks and reducinginefficient processes will likely lead to improved patientcare, higher staff satisfaction, and a safer health caresystem. It may also improve the financial position ofhospitals. To do this, there need to be clinician-levelincentives to provide high-quality, efficient care not justfor patients located in one department (such as the ED),but to consider the flow of patients throughout the entirecontinuum of care. These incentives can be applied toboth ED and non-ED clinicians. To maintain both highflow and high quality, this will require all clinicians beingrewarded for the success of not only their individualunits, but the organization as a whole.
One of the most challenging aspects of affectingchange within an institution is changing the establishedculture and set of values. Instead of seeing each unit orinpatient versus the ED as distinct entities, the interop-erability of the patients throughout the institution needsto be appreciated by all involved in patient care. Insteadof looking at each area as an independent entity, like asilo, each unit should see itself as one step of many forthe patient in the continuum of care. A patient-centeredmodel needs to be the emphasis of the delivery of care,not location.
As reimbursement trends continue to squeeze profitmargins, hospitals will need to find ways to use theirexisting capacity more effectively. This will mean oper-ating at higher occupancy on a consistent basis, withthe focus of managers to reduce delays and capture alldemand (ED and non-ED) while delivering the highestquality care. Transition units, full-capacity protocols,and admission lounges serve as operational models tohelp alleviate crowding and long waiting times.
With alignment of incentives for reimbursement, hos-pitals should find it equally attractive to provide care inboth emergent and scheduled settings. But as long asreimbursement favors prescreened scheduled care,
emergency care may continue to have a secondary rolein the priorities of patient flow within hospitals. How-ever, with the aging of the population, it is likely thatthe ED will play an increasing role in U.S. health care,both with increasing comorbidities contributing topostprocedural complications and with more emergentdisease presentations. As the health care reform debatecontinues, this must be taken into consideration toassure that our patients have access to the care theyneed and deserve.
ED crowding is clearly a widespread situation thatnegatively affects ED patient care. From the perspectiveof hospitals, there are clear benefits and costs associ-ated with delays in ED throughput and resultant EDcrowding. The profitability of ED inpatient admissionsand the financial benefits of improved ED throughputneed to be carefully evaluated at the level of each insti-tution. We propose a holistic and integrated approachfor hospitals that incorporates financial solutions thatboth benefit hospitals and improve ED efficiency andcare.
References
1. Derlet R, Richards J, Kravitz R. Frequent over-crowding in U.S. emergency departments. AcadEmerg Med. 2001; 8:151–5.
2. Han JH, Zhou C, France DJ, et al. The effect ofemergency department expansion on emergencydepartment overcrowding. Acad Emerg Med. 2007;14:338–43.
3. Pines J, Isserman J. The association between EDcrowding and delays in time to OR in acute appen-dicitis [abstract]. Acad Emerg Med. 2009; 16:S207–8.
4. Fee C, Weber EJ, Maak CA, Bacchetti P. Effect ofemergency department crowding on time to antibi-otics in patients admitted with community-acquiredpneumonia. Ann Emerg Med. 2007; 50:501–5.
5. Schull MJ, Vermeulen M, Slaughter G, Morrison L,Daly P. Emergency department crowding andthrombolysis delays in acute myocardial infarction.Ann Emerg Med. 2004; 44:577–85.
6. Pines JM, Hollander JE. Emergency departmentcrowding is associated with poor care for patientswith severe pain. Ann Emerg Med. 2008; 51:1–5.
7. Mills AM, Shofer FS, Chen EH, Hollander JE, PinesJM. The association between emergency depart-ment crowding and analgesia administration inacute abdominal pain patients. Acad Emerg Med.2009; 16:603–8.
8. Hwang U, Richardson L, Livote E, Harris B, Spen-cer N, Sean Morrison R. Emergency departmentcrowding and decreased quality of pain care. AcadEmerg Med. 2008; 15:1248–55.
9. Bernstein SL, Aronsky D, Duseja R, et al. The effectof emergency department crowding on clinicallyoriented outcomes. Acad Emerg Med. 2009; 16:1–10.
10. Pines JM, Pollack CV Jr, Diercks DB, Chang AM,Shofer FS, Hollander JE. The association betweenemergency department crowding and adverse car-diovascular outcomes in patients with chest pain.Acad Emerg Med. 2009; 16:617–25.
ACAD EMERG MED • August 2010, Vol. 17, No. 8 • www.aemj.org 845

11. Sprivulis PC, Da Silva JA, Jacobs IG, Frazer AR,Jelinek GA. The association between hospital over-crowding and mortality among patients admittedvia Western Australian emergency departments.Med J Aust. 2006; 184:208–12.
12. Richardson DB. Increase in patient mortality at 10days associated with emergency department over-crowding. Med J Aust. 2006; 184:213–6.
13. Gallagher EJ, Lynn SG. The etiology of medicalgridlock: causes of emergency department over-crowding in New York City. J Emerg Med. 1990;8:785–90.
14. Andrulis DP, Kellermann A, Hintz EA, HackmanBB, Weslowski VB. Emergency departments andcrowding in United States teaching hospitals. AnnEmerg Med. 1991; 20:980–6.
15. Espinosa G, Miro O, Sanchez M, Coll-Vinent B,Milla J. Effects of external and internal factors onemergency department overcrowding. Ann EmergMed. 2002; 39:693–5.
16. Forster AJ, Stiell I, Wells G, Lee AJ, van WalravenC. The effect of hospital occupancy on emergencydepartment length of stay and patient disposition.Acad Emerg Med. 2003; 10:127–33.
17. Rathlev NK, Chessare J, Olshaker J, et al. Time ser-ies analysis of variables associated with daily meanemergency department length of stay. Ann EmergMed. 2007; 49:265–71.
18. Olshaker JS, Rathlev NK. Emergency departmentovercrowding and ambulance diversion: the impactand potential solutions of extended boarding ofadmitted patients in the emergency department.J Emerg Med. 2006; 30:351–6.
19. Boston University Program for the Management ofVariability in Health Care Delivery. Root CauseAnalysis of Emergency Department Crowding andAmbulance Diversion in Massachusetts, EmergencyRoom Diversion Study: Analysis and Findings. Bos-ton, MA: Boston University, October 2002, p 29.
20. Richardson DB. The access-block effect: relation-ship between delay to reaching an inpatient bedand inpatient length of stay. Med J Aust. 2002;177:492–5.
21. Fatovich DM, Nagree Y, Sprivulis P. Access blockcauses emergency department overcrowding andambulance diversion in Perth, Western Australia.Emerg Med J. 2005; 22:351–4.
22. Bernstein SL, Asplin BR. Emergency departmentcrowding: old problem, new solutions. Emerg MedClin North Am. 2006; 24:821–37.
23. Hospital Flow Diagnostic: Institute for HealthcareImprovement, 2010. Available at: http://www.ihi.org/IHI/Topics/Flow/PatientFlow/. Accessed May 23,2010.
24. Institute of Medicine. Hospital-based EmergencyCare: At the Breaking Point. Washington, DC:National Academies Press, 2006.
25. McManus ML, Long MC, Cooper A, et al. Variabil-ity in surgical caseload and access to intensive careservices. Anesthesiology. 2003; 98:1491–6.
26. Falvo T, Grove L, Stachura R, et al. The opportunityloss of boarding admitted patients in the emergencydepartment. Acad Emerg Med. 2007; 14:332–7.
27. Bazzoli GJ, Brewster LR, Liu G, Kuo S. Does U.S.hospital capacity need to be expanded? Health Aff(Millwood). 2003; 22:40–54.
28. Bazzoli GJ, Brewster LR, May JH, Kuo S. The tran-sition from excess capacity to strained capacity inU.S. hospitals. Milbank Q. 2006; 84:273–304.
29. Nawar EW, Niska RW, Xu J. National HospitalAmbulatory Medical Care Survey: 2005 emergencydepartment summary. Adv Data. 2007; (386):1–32.
30. The Lewin Group Inc. Emergency DepartmentOverload: A Growing Crisis; The Results of the AHASurvey of Emergency Department and HospitalCapacity. Available at: http://www.aha.org/aha/content/2002/pdf/EdoCrisisSlides.pdf. Accessed May 23,2010.
31. Handel DA, McConnell KJ. The financial impact ofambulance diversion on inpatient hospital revenuesand profits. Acad Emerg Med. 2009; 16:29–33.
32. Cachon G, Terwiesch C. Matching Supply WithDemand: An Introduction to Operations Manage-ment. Boston, MA: McGraw-Hill ⁄ Irwin, 2009.
33. Henneman PL, Lemanski M, Smithline HA, Toma-szewski A, Mayforth JA. Emergency departmentadmissions are more profitable than non-emer-gency department admissions. Ann Emerg Med.2009; 53:249–55.
34. McHugh M, Regenstein M, Siegel B. The profitabil-ity of Medicare admissions based on source ofadmission. Acad Emerg Med. 2008; 15:900–7.
35. Pines JM, Heckman JD. Emergency departmentboarding and profit maximization for high-capacityhospitals: challenging conventional wisdom. AnnEmerg Med. 2009; 53:256–8.
36. AHRQ, HCUPnet Provides Trend Information forthe 15 Year Period: 1993–2007. HCUPnet, 2010.Available at: http://hcupnet.ahrq.gov/. AccessedMay 23, 2010.
37. Melnick GA, Nawathe AC, Bamezai A, Green L.Emergency department capacity and access in Cali-fornia, 1990–2001: an economic analysis. Health Aff(Millwood). 2004; Web(4):W136–42.
38. Viccellio A, Santora C, Singer AJ, Thode HC Jr,Henry MC. The association between transfer ofemergency department boarders to inpatient hall-ways and mortality: a 4-year experience. AnnEmerg Med. 2009; 54:487–91.
39. Wiler JL, Gentle C, Halfpenny JM, et al. Optimizingemergency department front-end operations. AnnEmerg Med. 2009; 55:142–60.
40. Litvak E, Long MC, Cooper AB, McManus ML.Emergency department diversion: causes and solu-tions. Acad Emerg Med. 2001; 8:1108–10.
41. Litvak E. Optimizing Patient Flow by Managing itsVariability, From Front Office to Front Line:Essential Issues for Health Care Leaders. Oak-brook Terrace, IL: Joint Commission Resources,Inc., 2005.
42. Litvak E. Improving Patient Flow and Throughputin California Hospitals Operating Room Services.Boston, MA: Boston University, 2007.
43. Goldratt EM, Cox J. The Goal: A Process of Ongo-ing Improvement. Great Barrington, MA: NorthRiver Press, 2004.
846 Handel et al. • ED CROWDING AND FINANCES

44. Kellermann AL. Too sick to wait. JAMA. 1991;266:1123–5.
45. Schlesinger M, Gray BH. How nonprofits matter inAmerican medicine, and what to do about it. HealthAff (Millwood). 2006; 25:W287–303.
46. The Chartis Group. Community Benefit Contribu-tions and Reporting, 2009. Available at: http://www.chartisgroup.com/files/pdfs/chartis_group_white_paper_community_benefit.pdf. Accessed May 23,2010.
Call for Papers 2011 Academic Emergency Medicine Consensus Conference
Interventions to Assure Quality in the Crowded Emergency Department The 2011 Academic Emergency Medicine Consensus Conference “Interventions to Assure Quality in the Crowded Emergency Department” will be held on June 1, 2011, immediately preceding the SAEM Annual Meeting in Boston, Massachusetts. Original papers on the conference topic, if accepted, will be published together with the conference proceedings in the December 2011 issue of Academic Emergency Medicine.
The Institute of Medicine’s (IOM) Committee on the Future of Emergency Care characterized hospital-based emergency care in the US as “at the breaking point.” Many emergency departments (EDs) face frequent and prolonged periods of crowding because of mismatches between capacity and demand for services. Several studies have found that ED crowding delays the timeliness of emergency care. Studies have also demonstrated the negative effect of crowding on the other dimensions of quality including safety, effectiveness, efficiency, equity, and patient-centeredness.
System-wide constraints and/or inefficiencies in the ED and the hospital, including the lack of bed availability, cause ED crowding. Therefore, system-wide solutions are needed at the ED, hospital, community, and national levels. Some EDs and hospitals have experimented with different strategies (e.g. staffing, communication, information technology, etc) to safeguard the quality of emergency care during capacity-constrained periods. The main focus of the conference will be to develop a research agenda to study interventions aimed at improving ED and hospital flow. However, attention will also be paid to public policy or health care reform changes that may influence crowding and the quality of emergency care.
The specific goals of the consensus conference are: 1. To develop a research agenda that identifies promising interventions that safeguard one or more of the six IOM
domains of quality of care during crowded periods in the ED; 2. To review interventions that have been implemented to reduce crowding and summarize the evidence of their impact on the
delivery of emergency care; 3. To identify methodological challenges associated with the implementation and evaluation of interventions designed to
safeguard the quality of emergency care during crowded periods; and 4. To identify policy strategies as well as strategies used by other industries to optimize system performance and determine their
applicability to solving quality of care problems associated with crowding in the ED.
Interventional research aimed at assuring quality of care during crowded periods may address any of the above objectives. Examples of research topics that would qualify include:
• Studies that seek hospital-wide solutions to crowding in the ED; • Policy solutions (e.g. four hour rule in the United Kingdom or pay-for performance in Ontario, Canada); • Information technology interventions that may be used to warn ED providers or administrators that conditions in the ED have
reached an unsafe threshold; • Interventions that enhance ED throughput (efficiency and timeliness); and • Interventions that inform patients about delays in care and evaluate their impact on patient satisfaction (patient-centered care).
Original contributions describing relevant research or concepts in this topic will be considered for publication in the December 2011 special topics issue of AEM if received by Monday, March 28, 2011. All submissions will undergo peer review, and publication cannot be guaranteed. For queries, please contact Melissa McCarthy, ScD ([email protected]) or Jesse Pines, MD ([email protected]), Consensus Conference Co-Chairs. Information and updates will also be posted in the SAEM newsletter and the AEM and SAEM websites.
ACAD EMERG MED • August 2010, Vol. 17, No. 8 • www.aemj.org 847