Embed Size (px)
Citation preview
Research Forum Abstracts
Methods: Nineteen subjects performed up to 50 minutes of treadmill walkingwhile wearing TPC in a heated room and were followed for two hours aftertermination of exercise. Psychomotor vigilance (PV) and cognitive function wereassessed at baseline (PRE), immediately post-exercise (IPE), 60 minutes (E�60), and120 minutes (E�120) after exercise.
Results: Exercise duration was 48.1 (3.6) min. and subjects lost 1.1 (0.4) kg bodymass. Immediately post exercise, pulse rate was 167�19 bpm and core temperature(Tc) was 38.9 � 0.5°C and did not return to baseline until E�120. PV false startsincreased E�120 when compared to PRE (p�0.03), IPE (p�0.02) and E�30(p�0.001). Arithmetic ability as measured by serial addition was higher at all post-exercise time points when compared to PRE with increased errors at E�120 whencompared to other post-exercise time points. Other tests did not show consistentdecrements following exercise.
Conclusions: Fifty minutes of treadmill exercise in TPC resulted in significantphysiologic strain but neither enhanced nor impaired cognitive performance.Decreased attention was noted two hours following exercise when Tc returned tobaseline. Delayed impairment of cognitive function may jeopardize firefighters in thehours following an emergency incident.
EMF-5 Emergency Department Crowding:Community Determinants and PatientOutcomes
Sun, MD, MPP B/University of California, Los Angeles, Los Angeles, CA
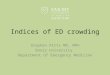
Background: Emergency department (ED) crowding has strained the acute caresystem to its breaking point. Two of the most visible symptoms of ED crowding,ambulance diversion and “left before being seen” visit rates, have dramaticallyincreased over time and are now routine in many centers. ED crowding causes delaysin evaluation and treatment, which in turn may contribute to adverse outcomes.Consequently, the American College of Emergency Physicians has identified EDcrowding as one of the top problems threatening the safety and quality of emergencycare. However, policymakers and health system leaders have failed to address EDcrowding as a top public health priority. The primary reason for inaction is thepaucity of data on community disparities in ED crowding and the impact of EDcrowding on patient outcomes.
Study Objectives: In order to assess patterns and outcomes of ED crowding, wepropose a retrospective cohort study of all 2007 ED visits in Los Angeles County. Thisanalysis will include 2.2 million discharges and 460,000 hospitalizations from 77 EDs.We will use daily ambulance diversion hours and “left before being seen” (LBBS) visitrates as measures of ED crowding. This study has the following specific aims:
1. Identify community level predictors of emergency department crowding.2. Assess the relationship between emergency department crowding and 7-day
bounce-back hospitalizations after emergency department discharge.3. Assess the relationship between emergency department crowding and inpatient
outcomes, including death, length of stay, and costs.
This exploratory study will provide important insights into the determinants andimpact of ED crowding. It will also lay the methodological foundations for futurestudies of multi-year, statewide data to understand this critical health policy issue.
334 Arm Circumference for a Rapid Estimate ofEmergency Patient Weight
Graber M, Rucker E, Chavez E, Thompson K, Ortiz M/Texas Tech Health ScienceCenter, El Paso, TX
Study Objectives: Emergency patients are often treated with weight-based fluids andmedications with only a guess as to their actual weight. The patients who are too ill for atriage-obtained weight are those most likely to receive weight-based, life-savingmedications such as heparin, low molecular weight heparins, thrombolytics, vasopressors,and anti-arrhythmics. There are no validated methods by which to estimate adult patientweight in the emergency department. Prior work has suggested that mid-armcircumference (MAC) may be a valid measurement from which to derive a weight inchildren. The need for a simple but accurate bedside weight estimate method for adultswould ensure that the correct doses of these medications are given instead of doses basedupon the wildly inaccurate guesses currently used. Therefore, the objective of this study isto develop a simple yet accurate method to estimate weight at the bedside.
Methods: This was an IRB-approved study conducted at a large, university-
affiliated hospital. Triaged patients had bilateral MAC measured. Age and measuredVolume , . : September
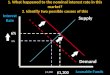
triage weight were also collected. Using regression analysis, a plot and formula for theconversion of MAC to weight has been derived.
Results: 408 patients have been evaluated. A formula converting MAC to weighthas been derived as follows: Weight Kg � (MACcm x 3.5) - 30.
Conclusions: We have developed a simple formula to convert arm circumferenceto weight. This will allow those patients too ill for triage weights to receive properdoses of weight-based medications. A patient’s weight in kg is estimated by (armcircumference in cm x 3.5) �30.
335 Physician Training Has No Effect on Bounce-BackRates In Pediatric Emergency Departments
Walsh B, Walsh K/Morristown Memorial Hospital, Morristown, NJ
Study Objectives: The physician staffing of pediatric emergency departments(PEDs) is controversial. One measure of quality may be return visits within 48 hours(“bounce-backs.”) We sought to determine if there was a difference in bounce-backrates between general emergency physicians (EM), pediatricians (P), and pediatricemergency medicine specialists (PEM).
Methods: Design: Retrospective cohort. Setting: Four designated pediatricemergency departments in NY and NJ. Protocol: From the database of 30,000randomly selected patients over a five-year period, the PED records of all patients lessthan 12 years of age who presented to the PED were reviewed. The attendingphysicians caring for the patients were categorized based on their training into thefollowing categories: EM, P, or PEM. Patients seen by physicians with other trainingwere excluded. Patients were considered to have “bounced back” if they returned tothe PED within 48 hours. Admission rates and bounce-back rates with 95%confidence intervals (CI) were calculated for each cohort.
Results: Of 30,000 patients placed in the PED database, 16,833 (56%) were �12 years old and seen by EM, P, or PEM. The average patient age and admission rateswere similar between cohorts. Of the 4,225 patients seen by EM, 4.6% (CI: 4.0-5.2)bounced back within 48 hours. Of the 5405 patients seen by P, 4.4% (CI: 3.8-4.9)bounced back. Of the 7203 patients seen by PEM, 4.4% (CI: 3.9-4.8) bounced back.There was no significant difference in bounce-back rates between the groups.
Conclusion: Based on bounce-back rates, there is no difference in the quality ofcare provided by physicians trained in EM, P, or PEM in designated pediatricemergency departments. This information may be useful for administrators indetermining how to staff their PEDs.
336 Emergency Severity Index Triage Reliability DuringVariable Patient Volumes
Franks NM, Houry D/Emory University School of Medicine, Atlanta, GA
Study Objective: Patient safety in crowded emergency departments (ED) requiresaccurate triage of medical urgency and streamlined throughput in the ED. Weassessed the reliability of nurse-assigned triage levels compared to physician reviewersacross varying shift times in a community ED using the Emergency Severity Index(ESI) five-level triage system. We hypothesize that a high correlation between nurseand physician ESI scores during high patient volumes will accurately assess patientsafety in an crowded ED.
Methods: This retrospective, convenience study reviewed patients evaluated in
the ED within a 2-month period. Patients from three different time shifts wereAnnals of Emergency Medicine S109