-
EPIDURAL ASSESSMENTRebecca M Humphreys, BSN, RNUnit Based
Educator, 5 EastSt. Lukes Health System, Boise
-
WHAT IS EPIDURAL ANALGESIA?The administration of
opioids/anesthetics via a catheter in the epidural space for pain
management. The epidural catheter is inserted by an
anesthesiologist or primary physician.
-
TERMINOLOGYIntraspinal- into the spine, either epidural or
intrathecalEpidural - the potential space above the dura mater
Intrathecal- the subarachnoid space. The cerebrospinal fluid
surrounds the spinal cord here. Spinal - same as
intrathecalSubarachnoid = spinal = intrathecal
-
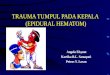
EPIDURAL INSERTION
-
EPIDURAL CATHETER PLACEMENT
-
ASSESSMENTMaintain IV access for a minimum of 4 hours following
last epidural dose or discontinuation of the epidural catheter.
Keep Naloxone (Narcan) 0.4mg available until 4 hours following last
dose.
-
ASSESSMENTAssess and document the following
parameters:Respiratory status: rate, depth and oxygen saturation
upon initiation, then every 30 minutes x 2, then every 1 hour x12
hours, and then every 2 hours x12 hours, then every 4 hours. Assess
in 4 hours and as needed after epidural discontinuation. If a bolus
is administered then assess every 30 minutes X 2 then return to
previous assessment times. Use a continuous pulse oximeter monitor
for patients on a continuous infusion unless provider constantly at
bedside. May place patient on continuous pulse oximeter per nursing
judgment.
-
ASSESSMENTSedation scale upon initiation, then every 30 minutes
x 2, then every 1 hour x 12 hours, then every 2 hours x 12 hours,
then every 4 hours until epidural discontinued. If a bolus is
administered then assess every 30 minutes X 2 then return to
previous assessment times. Pain scale, heart rate and BP upon
initiation, then every 30 minutes x 2, then every 4 hours on
non-obstetrical patients.
Motor and sensory function every 4 hours and prior to first
ambulation and 4 hours after catheter discontinued. Two (2) persons
will assist patient out of bed the first time and thereafter until
full motor function has returned. Use caution when transferring
/moving patient to assure catheter does not become dislodged.
-
ASSESSMENTEpidural assessment for hematoma every 4 hours until
12 hours after the catheter has been removed. Assess for:severe
back painleg weakness or numbnessincontinence of stool and/or
urineCatheter insertion site for displacement, leakage, kinking,
redness, fluid or bleeding every 4 hours and prior to bolus
administration Bladder distention, frequency, and urgency. Evaluate
ability to void within 4 to 6 hours of discontinuation of epidural
catheter. Nausea and vomiting especially related to movement.
Document at least every 4 hours until epidural discontinued.
Itching. Document at least every 4 hours until epidural
discontinued.
Why?
-
CAUTIONS!Do not give anticoagulants (other than low dose
heparin) until 2 hours after the epidral catheter has been
discontinued.No other CNS depressants are to be given without the
written order of the anesthesiologist, this includes medications
like muscle relaxants.
- WHEN TO CALL:Notify anesthesiologist or physician managing
epidural if:Respiratory rate
-
REMOVALRemoval of Epidural Catheter:Epidural catheters are
discontinued on the order from a physician. Check with physician
managing the epidural if patient has received anticoagulant.Have
patient roll head and shoulders caudally (knee to chest or fetal
position). This helps to expose back, slightly separate vertebrae,
and ease catheter removal. Wash hands.Don Gloves.Grasp catheter
close to skin and remove slowly, pulling steadily.Observe for
presence of metal or blue plastic tip. If not present, notify
anesthesiologist or physician managing the catheter.Cover insertion
site with a band-aid.Document procedure and assessment of insertion
site.
-
PRACTICE CHANGECONTINUOUS EPIDURAL
picture of me giving medT-CONNECTOR WILL BE PLACED ON THE END OF
YELLOW EPIDURAL TUBING INTO HUB OF EPIDURAL CATHTO GIVE BOLUS WITH
CONTINUOUS:SCRUB T-CONNECTOR PORT FOR 2 MINUTES WITH BETADINEDO NOT
USE ALCOHOLDAB WITH 2X2 IF WETUSING 25G 5/8 NEEDLE ON SYRINGE
MEDICATION, INSERT NEEDLE INTO PORTSLOWLY INJECTREMOVE ACTIVE
SAFETY NEEDLEDISCARD IN SHARPS QUESTIONS? CONTACT:KIM KRUTZ
[email protected] HANSEN - [email protected], 1-1505
6/2010
-
BOLUS DOSINGBOLUS DOSING (Not for the pregnant/laboring
patient)Administer a bolus dose for breakthrough pain while
receiving continuous infusions using the T-connector. Use
preservative-free medication and preservative free normal
salinePreservative-free vials are to be discarded after a single
useDraw up opioid dose:Add the preservative free normal saline, if
necessary Assess insertion site for:Excessive drainageCatheter
integritySigns and symptoms infection, redness, pain, or
swelling.Cleanse T-connector injection cap:Scrub with
povidone-iodine prep-pad. NEVER USE ALCOHOL WITH EPIDURAL
CATHETERS. Allow to dry for 2 minutes.Wipe with sterile 2x2 after
2-minute dry time has elapsed.Attach empty syringe and check for
placement of line by gently aspirating for blood or CSF.Insert an
empty 3-ml syringe with 25-gauge, 5/8-inch needle through the dry,
prepped injection cap and aspirate. Little (< 0.5ml) or no fluid
should return from the epidural space.If no fluid aspirated, remove
the needle and syringe from the epidural catheter cap.If bloody
fluid or clear fluid > 0.5 ml aspirated, STOP. Do not re-inject
the aspirate. Withdraw the needle and notify the anesthesiologist,
CRNA or physician managing the catheter.Attach syringe with
medication and administer slowly. You should feel some resistance
as you inject; however, if you are unable to inject the medication,
call the physician. Resume infusion.Document medication given.
-
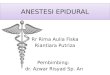
WHAT IF YOU SEE THIS?
-
CASE STUDY: MRS. GREEN - 12 HOURS POST HIP REPLACEMENT Its 2 AM,
Mrs. Green had Morphine 2 mg epidural at 1 AM. She appears to be
sleeping.Her respiratory rate is 10/min.She does not wake up when
you call her name.
-
WHAT WOULD YOU DO?StimulateTurn off continuous infusionCheck O2
saturationCall RTStart oxygenGive Narcan 0.4 IVP
-
CASE STUDY MR. JONES65 year old man with colon resection.Bolus
of Morphine given by anesthesia 5 MG.Continuous epidural with
Morphine at 0.5 mg/hr8 hours post op- Rates pain as 8
What would you assess?What do you think Mr. Jones needs to have
his pain relieved?Do you need to call the doctor?
-
MR. JONESAssess pain Assess AbdomenVital signsMedicate for
breakthrough pain (fentanyl) sterile techniqueConsider increasing
continuous morphineCall MD if order is needed or pain may be caused
by a complication.Nonpharmacologic pain measures
-
QUESTIONS?
?
**Terminology can be confusing. Epidural space is actually
subcutaneous tissue above the dura mater.Spinal cord surrounded by
cerebral spinal fluid (The intrathecal or subarachnoid space)3
layers of meninges protect the cord and CSF (pia mater, arachnoid
mater, dura mater)Epidural (above the dura)*The patient is placed
on their side with the chin tucked and the knees pulled up to help
round the back and thus open a wider space between the vertebrae
for easier access.This is the same position the patient is placed
in for catheter removal and for spinal tap (LP) for CSF specimen
collection to rule out meningitis.*Visual of epidural catheter
placement.*These are hives. That would indicate an allergic
reaction.What should you assess?(ABC, VS, Extent of hives)What
actions would you take?Stop drug, treat, hives with antihistamine,
epinephrine if ABC impaired, IV access, O2)*Ask groupwhat should
you do?Stimulate.Try to wake up-is she sleeping or is she
sedated?O2sat?
**