Embed Size (px)
Citation preview
CentralBringing Excellence in Open Access
Journal of Neurological Disorders & Stroke
Cite this article: He Z, Cui L, Ferguson SA, Paule MG (2016) Epidural Steroid Injection Therapy, Complications and Experimental Approaches Simulating Accidental Intra-Arterial Injection. J Neurol Disord Stroke 4(2): 1113. 1/5
*Corresponding authorZhen He, Department of Neurotoxicology, National Center for Toxicological Research, Food and Drug Administration, 3900 NCTR Road, Jefferson AR 72079, USA, Tel: 870-543-7053; Fax: 870-543-7745; Email:
Submitted: 01 January 2016
Accepted: 22 June 2016
Published: 13 July 2016
Copyright© 2016 He et al.
OPEN ACCESS
Keywords•Epidural steroid injection•Severe neurological complications•Ischemia•Intra - arterial injection
Review Article
Epidural Steroid Injection Therapy, Complications and Experimental Approaches Simulating Accidental Intra-Arterial InjectionZhen He1*, Li Cui2, Sherry A. Ferguson1, and Merle G. Paule1
1Department of Neurotoxicology, National Center for Toxicological Research, USA2Department of Microbiology and Immunology, University of Arkansas for Medical Sciences, USA
Abstract
Epidural steroid injections (ESIs) as minimally invasive procedures have been widely used for the relief of neck, arm, back, and leg pain potentially due to spinal stenosis, spondylolysis, or disc herniation. In rare instances, ESI therapy may cause clinical complications, some of which can be catastrophic. The surgical procedure itself including needle penetration, the potential use of contrast media, the injected medications (i.e., conventional steroids), or a combination of these in association with the original cause of the targeted pain which may include local inflammation, may account for such adverse complications. Nevertheless, there is increasing evidence indicating that ischemia and/or hemorrhage (stroke) in the brain and/or spinal cord, following accidental intra - arterial injection of the medication is a primary contributor to the severe neurologic events. Descriptions of experimental intra - arterial injections simulating the noted catastrophic outcomes associated with ESI therapy are very limited in the literature. Identifying and describing the cause of severe ESI complications will likely rely on the establishment of new experimental models simulating intra - vertebral artery or intra-radiculomedullary artery steroid injections.
INTRODUCTIONBack pain is one of the most common chronic adverse human
conditions. The life - time prevalence of chronic low back pain in young males is 13% [1], while the incidence in 50-70 - year - old men and women increases to 62~83% [2]. The conventional causes of back pain are spinal degeneration, including spinal stenosis and disc herniation [3] as well as spondylolysis. Exemplarily, disc herniation - induced back pain can be attributed mechanistically to direct pressure of the herniated disc on nerve roots, direct toxic damage of the nucleus pulposus to the nerve root [4] and/or vascular inflammation - associated infiltration elicited by the nucleus pulposus following disc rupture [5].
Epidural steroid injection (ESI) therapy for back pain was established as early as the 1950s [6,7]. In a subsequent double - blind controlled trial, the approach was judged to be a valuable treatment for the management of lumbar nerve root compression syndromes associated with degenerative disc disease and
the therapeutic effects of ESI were ascribed to its local anti - inflammatory capability [8]. A recent systematic review of the literature and comprehensive analysis of the published data indicates that ESI therapy is effective in relieving pain and delaying or sparing surgery [9]. Although the effects of ESI are temporary, the pain relief accompanying ESI may last for several days or even years [http://www.mayfieldclinic.com/PE-ESI.htm#.VSgRluFInhl].
Interestingly, the earliest experimental approach of the effects of ESI did not appear until the 1970s in which the potential side effects were addressed using the dog as the experimental subject [10]. In addition to the variety of corticosteroids that can be given via epidural injection, there are several alternative sites at which ESI can be employed including interlaminar, transforaminal, and caudal. Selection of the injection site to be used depends upon the type of pain to be treated and its anatomical location. The experience of the treating clinician likely also contributes to the selection of which approach is taken.
CentralBringing Excellence in Open Access
He et al. (2016)Email:
J Neurol Disord Stroke 4(2): 1113 (2016) 2/5
ESI procedures Interlaminar injections: This approach aims at delivery
of the selected steroids into the epidural space around the spinal nerve roots that are inflamed and painful. The needle placement here has been well described in a recent report [11]. The procedure includes confirmation of the injection location, inserting the needle between the spinosus processes of two vertebrae and traversing the ligamentum flavum until the epidural space is entered and then delivering the steroid(s). Theoretically, the injected therapeutic should be delivered to both sides of the inflamed nerve root at the same time.
Transforaminal injections: Transforaminal steroid injections have traditionally been performed using guided fluoroscopy employing injections of contrast media to confirm the targeted injection location. Guidance of needle placement under fluoroscopy with the use of a contrast media for ESI was first applied with the caudal injection approach [12]: needle placement is well described in a recent report [11]. After identifying the appropriate bony landmarks, the needle can be directed towards the superior, lateral, or anterior aspect of the neural formen after it has been inserted approximately halfway between the two adjacent transverse processes and thereafter advanced toward the lower edge of the transverse process, near its junction with the superior articular process. In practice, local anesthetics may be used and a contrast media injected to verify the epidural space prior to injection of the therapeutic steroid [13].
Caudal injections: Caudal injections are typically executed through the sacral hiatus, a small opening to the epidural space between the anatomical landmarks, the left and right sacral cornua. A landmark triangle can be visualized to localize the
sacral hiatus by marking the posterior superior iliac spines as the baseline of the triangle and then drawing two equilateral lines caudally to the triangle apex: the sacral hiatus lies under, or adjacent to, this apex [14]. The needle can be advanced cephalically through the sacral hiatus into the sacral spinal canal in as much as it remains below the S-2 segment [12]. A catheter may be placed through the needle and, as long as it remains within the epidural space, this can accommodate much more cephalic injections of the medications. In practice, a catheter can safely be placed until its tip reaches the L-5 vertebra [15].
Pitfalls and merits in selection of different ESI procedures: The epidural space extends from the foramen magnum to the sacral hiatus/notch. That space contains nerve roots with their associated vestments, blood vessels, adipose tissue, and loose areolar tissue. A midline septum (i.e., the plica mediana dorsalis) can completely separate the epidural space into right and left compartments [15]. Because the cal sac usually ends around sacral level 2 and the sacral hiatus is located far below that level (S-4 ~ S-5 level), caudal injections would seemingly have little chance of resulting in an intrathecal injection. Indeed, routine utilization of the caudal approach has resulted in few complications [14]. On the other hand, it has been reported that there is approximately a 30% incidence of misplaced epidural injections, even in experienced hands [16,17]. Proper placement of the injection needle into the epidural space appears far more successful when using the lumbar interlaminar approach than the caudal approach (93% vs. 64%, respectively) [18]. Guidance under fluoroscopy with or without the use of a contrast agent may be required to improve the success rate for caudal ESI [12]. As a consequence, exposure to X - rays and contrast media should be considered as risk factors for post - procedure complications. In addition, the caudal approach is more likely than the lumbar interlaminar approach to result in an intravenous injection (6-9% incidence) [16,19].
Utilizing the transforaminal ESI approach has two benefits: It provides diagnostic information and places the therapeutic at the nerve root that is the source of the pain. If the injection results in the loss or amelioration of pain, then the nerve targeted by the injection is likely to be the source of the pain. In other words, a patient who experiences immediate relief is an indication that the therapeutic efficacy has verified the pain source. Accordingly, this information is a key for guiding future treatment options, including surgical interventions, as ESI therapy is considered only a temporary measure for pain relief.
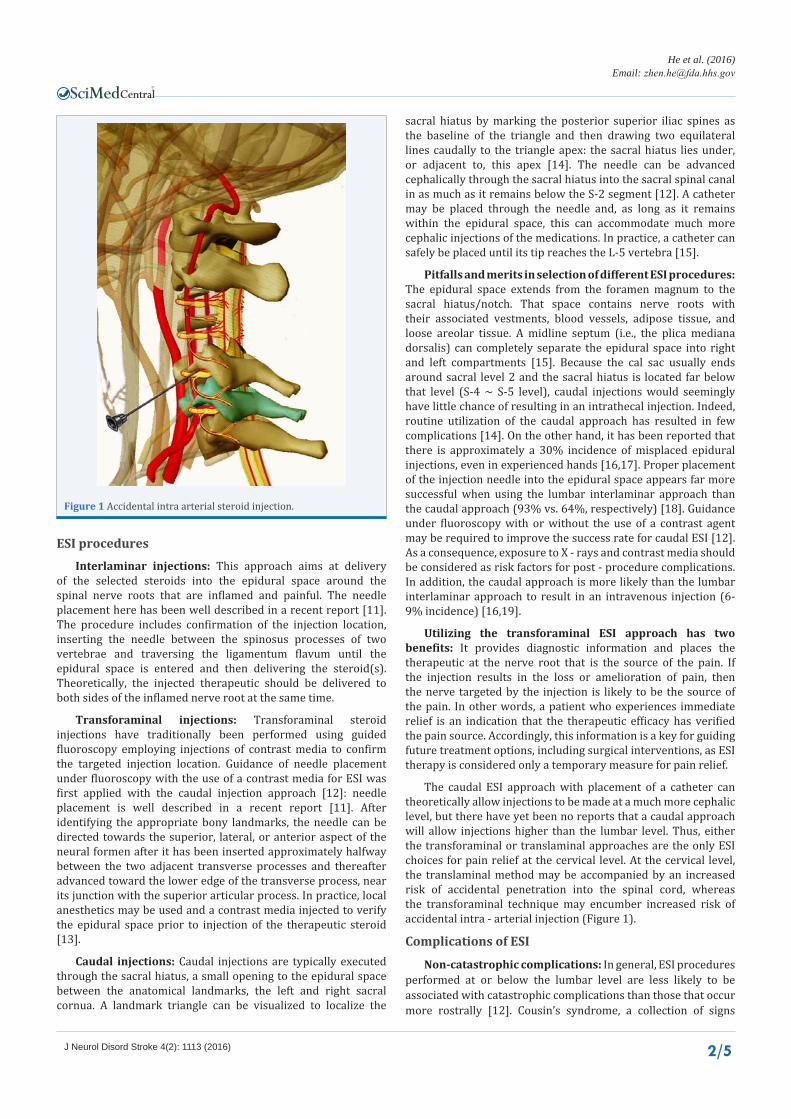
The caudal ESI approach with placement of a catheter can theoretically allow injections to be made at a much more cephalic level, but there have yet been no reports that a caudal approach will allow injections higher than the lumbar level. Thus, either the transforaminal or translaminal approaches are the only ESI choices for pain relief at the cervical level. At the cervical level, the translaminal method may be accompanied by an increased risk of accidental penetration into the spinal cord, whereas the transforaminal technique may encumber increased risk of accidental intra - arterial injection (Figure 1).
Complications of ESI
Non-catastrophic complications: In general, ESI procedures performed at or below the lumbar level are less likely to be associated with catastrophic complications than those that occur more rostrally [12]. Cousin’s syndrome, a collection of signs
Figure 1 Accidental intra arterial steroid injection.

CentralBringing Excellence in Open Access
He et al. (2016)Email:
J Neurol Disord Stroke 4(2): 1113 (2016) 3/5
and symptoms including but not limited to high blood pressure, weight gain (especially upper body), a round red face and thin arms and legs, can be associated with repeated steroid injections [20]. Epidural anesthetic applications, a procedure associated with ESI therapy, may cause transient, mild hypotension, whereas accidental intrathecal injections of anesthetics may cause profound hypotension [12]. Meningitis may occur due to accidental subarachnoid injections [21]. Tens of arachnoiditis cases that have occurred in conjunction with ESIs have been reported, yet there is insufficient clinical detail to make a reasonable assessment of the underlying cause in the majority of cases [22].
Severe or catastrophic complications: The FDA has issued a warning with respect to ESIs: “serious neurologic events, some resulting in death, have been reported with epidural injection of corticosteroids. Specific events reported include, but are not limited to, spinal cord infarction, paraplegia, quadriplegia, cortical blindness, and stroke. These serious neurologic events have been reported with and without use of fluoroscopy” [22]. Importantly, the reported serious neurologic events [23] appear to be primarily due to the accidental intra - arterial injection of corticosteroids during attempted ESIs [24,25] (Figure 1).
Efforts to improving ESI procedures
A “safe triangle” area in which to execute transforaminal ESIs has been described [26,27]. Its three sides include a side made up by the pedicle, a tangential side that corresponds to the exiting nerve root, and a side that is made by the lateral border of the vertebral body, implying a potential risk in an injection beyond the territory. The triangle delineates an area of safety for the nerve roots: injections within the triangle would avoid direct injury. The triangle, however, does not signify an area in which there is no risk of needle penetration into the spinal radicular artery or other vessel [28] (Figure 1).
The arteries of Adamkiewicz (the great anterior radiculomedullary artery or arteria radicularis anterior magna) are most often (97%) located in the superior half of the foramen [29] where the spinal nerve roots reside; however, they can be found at almost any location within the neural foramen [29]. A congested vascular region indicates where in the radiculomedullary arteries and/or the arteries of Adamkiewicz become invested within the superior and anterior aspect of the nerve root sleeve [30]. The “Dorsal technique” has been developed in which the tip of the spinal injection needle is placed dorsal to the dorsal root ganglion [28] and Zhu et al. [30] have described a modified posterior approach in which the tip of spinal needle is placed toward the posterior epidural space to avoid puncturing the spinal radicular artery and to minimize nerve root penetrations while delivering medication into the epidural space through the foramen. It is important to note that needle type has been considered a risk factor for the incidence of intravascular injection during transforaminal epidural injections [31]. The aforementioned efforts do not completely eliminate the risks of damaging the vertebral artery or its branches or of making intra - arterial injections. Anatomical anomalies of the human vertebral artery have been identified and categorized [32], and indicate that unexpected variations at the site of cervical transforaminal ESIs may account for unintended intra - arterial injections and the resulting severe neurological complications.
Pathogenic mechanisms underlying severe complications following ESI
Hypothetically, needle penetration, potential use of contrast medium, the injected medication (typically, conventional steroids), or their combined effects in association with the original cause of the treatment (trauma, pain), and associated local inflammation, may contribute to disastrous neurological events. The occurrence of brain or spinal cord stroke can typically be ascribed to two events: inadvertent penetration of an artery and/or the injected material acts as an embolus. Evidence supporting the embolic hypothesis includes: 1) some steroids, including methylprednisolone [33], the most commonly used drug for ESI, tend to form aggregates [34] which range in size from 20 to 100 microns with the potential to block supply arteries [35]; 2) clinical reports suggest that the particulate steroids such as methylprednisolone are those most often associated with the occurrence of ischemia [9,36]; 3) the clinical evidence indicates a relatively high incidence of intra - arterial needle placement during ESI [37,38] with the incidence of vascular penetration during fluoroscopically guided, contrast - enhanced, transforaminal lumbar ESI being between 8.1 ~ 21.3% [39], this clearly suggests the possibility that therapeutic steroids can be injected into arteries; and 4) accidental placements of injected steroids into the vertebral artery have been documented in clinical reports [9,35,36,40]. Nevertheless, other reasons for ischemia/stroke have been proffered including the presence of arterial intimal flaps, arterial dissections, and dislodgement of intravascular plaques causing emboli, arterial muscle spasms, and embolism of fresh thrombi following disruption of the intima [23].
Interestingly, the intra - arterial injection of steroids has been employed experimentally to assess their potential neurotoxicity [41]. The authors also examined whether different steroid formulations those with and without particulates behaved differently in causing CNS damage. Based on mg/kg body weight, half or less of the typical clinical dose of corticosteroid (i.e., DEPO - MEDROL), if administered intra - arterially was capable of causing multiple cerebral parenchymal hemorrhages, thought to be associated with extensive damage to the blood-brain barrier [41]. A case report has clearly linked ESI to hemorrhagic stroke [42]. Nevertheless, infarct or ischemic stroke rather than hemorrhagic stroke has been typically identified as a complication of ESI [40].
Discrepancies between clinical observations and experimental outcomes
The reasons why experimental outcomes often do not replicate what is seen in most clinical cases (i.e., hemorrhage vs. ischemia) remain unknown. Future studies should be designed to seek answers to the following questions. First, the previously reported experimental results require verification: as yet, no publications, other than the original report by [41] are available that demonstrate multiple, parenchymal hemorrhage following intra - arterial steroid injection. Second, the dose - dependency of the toxicity associated with selected steroids such as methylprednisolone should be determined over a wide range of doses, allowing for the detection of ischemic changes other than just hemorrhagic changes. Third, time course studies focusing on the parenchymal hemorrhagic injury following intra -arterial injections of steroids will help exclude hemorrhage or increased BBB permeability that may occur secondary to

CentralBringing Excellence in Open Access
He et al. (2016)Email:
J Neurol Disord Stroke 4(2): 1113 (2016) 4/5
other subtypes of stroke such as embolic. For example, time course data obtained from living animals using MRI or retinal microscopic imaging (e.g., using Phonix Micron IV) approaches would allow the determination of whether ischemia occurs before or after the occurrence of hemorrhage or increased BBB permeability. Fourth, it is known that aging plays a role in affecting the pathogenic cascade elicited by the intra - arterial injection of steroids: the most severe clinical sequelae following ESI likely occur in aged subjects [25]. Finally, “refining” the experimental models for studying the intra - arterial injection of steroids to better simulate actual clinical scenarios would allow for a better determination of whether or not damage related to needle insertion into an artery might largely be responsible for determining the subtypes of stroke that ensue: the original study on the intra - arterial injection of steroids employed a catheter placed into the right internal carotid artery via a cut through the right external carotid artery. Because the catheter was secured via ligation, the location of the vascular injury was separated from the general circulation and, thus, any systemic coagulating cascade elicited by the vascular damage would be limited. Furthermore, there are substantial differences between the carotid artery system and the vertebral - basilar artery system with respect to blood flow dynamics and regions supplied [the vertebral - basilar artery system supplies many critical brain structures that directly control vital functions such as circulation (heart rate, blood pressure) and respiration (rate and depth)]. In other words, models employing injections of steroid via ligated cannulae would focus on the cytotoxicity of steroids per se, whereas models employing injections of steroids via needle - syringe units would better address the combined effects of steroids and needle-caused trauma to the targeted artery.
Future experimental studiesIntracarotid artery injections are viable options for modeling
accidental intra - arterial injections that can occur in the clinic during ESI therapy. The procedure can be readily performed with laboratory animals due to well - established procedures dating back at least 4 decades [43]. This procedure also lends itself to effective control of catastrophic events, such as using vascular clips to stop unintended bleeding. Unfortunately, the carotid artery supplies the forebrain, an area largely irrelevant to the areas served by vessels likely to be affected by errant ESIs. Thus, intracarotid injections of steroids would not be expected to result in physiological responses precisely mimicking those expected to occur in the case of a poor ESI.
A logical step next is to establish an experimental model mimicking intra vertebral artery or intra - radiculomedullary artery injections. The laboratory rat is the most likely candidate considering factors such as cost, animal numbers, and experimental feasibility. To our knowledge, there is currently no published experimental protocol in which laboratory animals have been used to model intra vertebral artery injections. Nevertheless, rat global ischemia models employing either 4-vessel-occlusions [bilateral carotid and vertebral arteries [44-48]] or 8-vessel-occlusions [the aforementioned vessels plus the bilateral ala foramen and external carotid arteries (ECA), [45,49] involve procedures that access the bilateral vertebral arteries. In this case, an electrical coagulator is used to occlude the vertebral arteries. In the case of modeling intra vertebral artery injections, a needle would be inserted into the vessel rather than an electrical cauterizer. Accordingly, developing a model of intra vertebral
artery injection is eminently feasible with sufficient practice.
REFERENCES1. Shim JH, Lee KS, Yoon SY, Lee CH, Doh JW, Bae HG. Chronic low back
pain in young korean urban males: the life-time prevalence and its impact on health related quality of life. J Korean Neurosurg Soc. 2014; 56: 482-487.
2. Werber A, Zimmermann-Stenzel M, Moradi B, Neubauer E, Schiltenwolf M. Awareness of the German population of common available guidelines of how to cope with lower back pain. Pain Physician. 2014; 17: 217-226.
3. Leone A, Costantini AM, Guglielmi G, Tancioni V, Moschini M. Degenerative disease of the lumbosacral spine: disk herniation and stenosis. Rays. 2000; 25: 35-48.
4. Olmarker K, Byröd G, Cornefjord M, Nordborg C, Rydevik B. Effects of methylprednisolone on nucleus pulposus-induced nerve root injury. Spine (Phila Pa 1976). 1994; 19: 1803-1808.
5. Byröd G, Otani K, Brisby H, Rydevik B, Olmarker K. Methylprednisolone reduces the early vascular permeability increase in spinal nerve roots induced by epidural nucleus pulposus application. J Orthop Res. 2000; 18: 983-987.
6. Robecchi A, Capra R. [Hydrocortisone (compound F); first clinical experiments in the field of rheumatology]. Minerva Med. 1952; 43: 1259-1263.
7. Gerest F. [Treatment of sciatic neuralgia by epidural injections of hydrocortisone]. J Med Lyon. 1958; 39: 261-264.
8. Dilke TF, Burry HC, Grahame R. Extradural corticosteroid injection in management of lumbar nerve root compression. Br Med J. 1973; 2: 635-637.
9. Engel A, King W, MacVicar J. The effectiveness and risks of fluoroscopically guided cervical transforaminal injections of steroids: a systematic review with comprehensive analysis of the published data. Pain Med. 2014; 15: 386-402.
10. Dürr UM. [Tolerance studies on the epidural administration of dexamethasone in the dog]. Dtsch Tierarztl Wochenschr. 1974; 81: 352-353.
11. Rathmell JP, Benzon HT, Dreyfuss P, Huntoon M, Wallace M, Baker R, et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology. 2015; 122: 974-984.
12. E1-Khouri GY, Ehara S, Weinstein JN, Montgomery WJ, Kathol MH. Epidural steroid injection: a procedure ideally performed with fluoroscopic control. Radiology 1988; 168: 554-557.
13. Kraiwattanapong C, Wechmongkolgorn S, Chatriyanuyok B, Woratanarat P, Udomsubpayakul U, Chanplakorn P, et al. Outcomes of fluoroscopically guided lumbar transforaminal epidural steroid injections in degenerative lumbar spondylolisthesis patients. Asian Spine J. 2014; 8: 119-128.
14. Gordon J. Caudal extradural injection for the treatment of low back pain. Anaesthesia, 1980; 35: 515-516.
15. Roberson GH, Hatten HP, Hesselink JH. Epidurography: selective catheter technique and review of 53 cases. AJR 1979; 132: 787-793.
16. White AH, Derby R, Wynne G. Epidural injections in the diagnosis and treatment of low back pain. Spine 1980; 5: 78-86.
17. Stewart HD, Quinnell RC, Dann N. Epidurography in the management of sciatica. Br J Rheumatol 1987; 26: 424-429.
18. Price CM, Rogers PD, Prosser AS, Arden NK. Comparison of the caudal
CentralBringing Excellence in Open Access
He et al. (2016)Email:
J Neurol Disord Stroke 4(2): 1113 (2016) 5/5
and lumbar approaches to the epidural space. Ann Rheum Dis. 2000; 59: 879-882.
19. Renfrew DL, Moore TE, Kathol MH, El-Khoury GY, Lemke JH, Walker CW. Correct placement of epidural steroid injections: fluoroscopic guidance and contrast administration. Am J Neuroradiol 1991; 12: 1003-1007.
20. Stambough JL, Booth RE. Rothman RH. Transient hypercorticism after epidural steroid injection. J Bone Joint Surg Am. 1984; 66: 1115-1116.
21. Dougherty JH, Fraser RAR. Complications following intraspinal injection of steroids. J Neurosurg 1978; 48:1023-1025.
22. FDA Briefing Document: Epidural Steroid Injections (ESI) and the Risk of Serious Neurologic Adverse Reactions. Anesthetic and Analgesic Drug Products Advisory Committee Meeting November 24-25, 2014.
23. Manchikanti L, Hirsch JA. Neurological complications associated with epidural steroid injections. Curr Pain Headache Rep. 2015; 19: 482.
24. Baker R, Dreyfuss P, Mercer S, Bogduk N. Cervical transforaminal injection of corticosteroids into a radicular artery: a possible mechanism for spinal cord injury. Pain 2003; 103: 211-215.
25. ManchikantiL, Candido KD, Singh V, Gharibo CG, Boswell MV, Benyamin RM, et al. Epidural steroid warning controversy still dogging FDA. Pain Physician. 2014; 17: 451-474.
26. Bogduk N, Aprill C, Derby R. Epidural steroid injections. In: White AH, Schofferman J, editors. Spinal care diagnosis and treatment. St. Louis (MO): Mosby; 1995; 322-43.
27. Lutz GE, Vad VB, Wisneski RJ. Fluoroscopic transforaminal lumbar epidural steroids: an outcome study. Arch Phys Med Rehabil. 1998; 79: 1362-1366.
28. Zhu J, Falco FJ, Formoso F, Onyewu O, Irwin FL. Alternative approach for lumbar transforaminal epidural steroid injections. Pain Physician. 2011; 14: 331-341.
29. Murthy NS, Maus TP, Behrns CL. Intraforaminal location of the great anterior radiculomedullary artery (artery of Adamkiewicz): a retrospective review. Pain Med. 2010; 11: 1756-1764.
30. Glaser SE, Shah RV. Root cause analysis of paraplegia following transforaminal epidural steroid injections: the ‘unsafe’ triangle. Pain Physician. 2010; 13: 237-244.
31. Smuck M, Yu AJ, Tang CT, Zemper E. Influence of needle type on the incidence of intravascular injection during transforaminal epidural injections: a comparison of short-bevel and long-bevel needles. Spine J 2010; 10: 367-371.
32. Gitkind AI, Olson TR, Downie SA. Vertebral artery anatomical variations as they relate to cervical transforaminal epidural steroid injections. Pain Med. 2014; 15: 1109-1114.
33. Okubadejo GO, Talcott MR, Schmidt RE, Sharma A, Patel AA, Mackey RB, et al. Perils of intravascular methylprednisolone injection into the vertebral artery. An animal study. J Bone Joint Surg Am. 2008; 90: 1932-1938.
34. Benzon HT, Chew TL, McCarthy RJ, Benzon HA, Walega DR. Comparison of the particle sizes of different steroids and the effect of dilution: a review of the relative neurotoxicities of the steroids. Anesthesiology. 2007; 106: 331-338.
35. Tiso RL, Cutler T, Catania JA, Whalen K. Adverse central nervous system sequelae after selective transforaminal block: the role of corticosteroids. Spine J. 2004; 4: 468-474.
36. Rozin L, Rozin R, Koehler SA, Shakir A, Ladham S, Barmada M, et al. Death during transforaminal epidural steroid nerve root block (C7) due to perforation of the left vertebral artery. Am J Forensic Med Pathol. 2003; 24: 351-355.
37. Kimdo W, Han KR, Kim C, Chae YJ. Intravascular flow patterns in transforaminal epidural injections: a comparative study of the cervical and lumbar vertebral segments. Anesth Analg. 2009; 109: 233-239.
38. El Abd OH, Amadera JE, Pimentel DC, Pimentel TS. Intravascular flow detection during transforaminal epidural injections: a prospective assessment. Pain Physician. 2014; 17: 21-27.
39. Furman MB, O’Brien EM, Zgleszewski TM. Incidence of intravascular penetration in transforaminal lumbosacral epidural steroid injections. Spine 2000; 25: 2628-2632.
40. Scanlon GC, Moeller-Bertram T, Romanowsky SM, Wallace MS. Cervical transforaminal epidural steroid injections: more dangerous than we think? Spine. 2007; 32: 1249-1256.
41. Dawley JD, Moeller-Bertram T, Wallace MS, Patel PM. Intra-arterial injection in the rat brain: evaluation of steroids used for transforaminal epidurals. Spine. 2009; 34: 1638-1643.
42. Ziai WC, Ardelt AA, Llinas RH. Brain stem stroke following uncomplicated cervical epidural steroid injection. Arch Neurol. 2006; 63: 1643-1646.
43. Fujishima M, Omae T. Carotid back pressure following bilateral carotid occlusion in normotensive and spontaneously hypertensive rats. Experientia. 1976; 32:1021-1022.
44. He Z, He YJ, Day AL, Simpkins JW. Proestrus Levels of Estradiol during Transient Global Cerebral ischemia Improves Histological Outcome of the Hippocampal CA1 Region: Perfusion-Dependent and -Independent Mechanisms, J Neurol Sci. 2002; 193: 79-87.
45. He Z, Cui L, Meschia J, Dickson DW, Brott TG, Simpkins JW, et al. Hippocampal progenitor cells express nestin following cerebral ischemia in rats. NeuroReport. 2005; 16: 1541-1544.
46. He Z, Crook JE, Meschia JF, Brott TG, Dickson DW, Mickinney M. Aging Blunts Ischemic-Preconditioning-Induced Neuroprotection Following Transient Global Ischemia in Rats. Curr Neurovasc Res. 2005; 2: 365-374.
47. He Z, Meschia JF, Brott TG, Dickson DW, Mickinney M. Aging is Neuroprotective during Global Ischemia but Leads to Increased Caspase-3 and Apoptotic Activity in Hippocampal Neurons. Curr Neurovasc. Res 2006; 3: 181-186.
48. He Z, He B, Behrle B, Fejleh MP, Cui L, Paule MG, et al. Ischemia-induced increases in microvascular phosphodiesterase 4D expression in rat hippocampus associated with blood brain barrier permeability: Effect of age. ACS Chem. Neurosci. 2012; 3: 428-432.
49. He Z, Cui L, Wu SS, Li XY, Simpkins JW, Mckinney M, et al. Increased severity of acute cerebral ischemic injury correlates with enhanced stem cell induction as well as with predictive behavioral profiling. Curr Neurovasc Res. 2004; 1: 399-409.
He Z, Cui L, Ferguson SA, Paule MG (2016) Epidural Steroid Injection Therapy, Complications and Experimental Approaches Simulating Accidental Intra-Arterial Injection. J Neurol Disord Stroke 4(2): 1113.
Cite this article










![Epidural steroid injections: our experience and a review of the ......Infectious Epidural abscess, Discitis, Osteomyelitis [38-45] Intravascular injection Intravenous or Intraarterial](https://img.pdfslide.net/doc/110x75/60df39605510cf3a1862f983/epidural-steroid-injections-our-experience-and-a-review-of-the-infectious.jpg)


















