Embed Size (px)
Citation preview

Journal of the American Academy of DermatologyVolume 29, Number 5, Part 2
44. Leaker B, McGregor A, Griffiths M, et al. Insidious loss ofrenal function in patients with anticardiolipin antibodiesand absence of overt nephritis. Br J Rheumatol 1991;30:422-5.
45. Hazeltine M, Rauch J, Danoff D, et at. Antiphospholipidantibodies in systemic lupus erythematosus: evidence of as-
Amster et al.
sociation with positive Coombs' and hypocomplementemia.J RheumatoI1988;15:80-6.
46. Asherson R, Hughes GRV. Hypoadrenalism, Addisonsdisease and antiphospholipid antibodies. J Rheumatol1991;18:1-3.
Eruptive pseudoangiomatosis: A unique childhoodexanthem?Neil S. Prose, MD,a, b Whitney Tope, MD,c Sara E. Miller, PhD,d, e andHideko Kamino, MDa, e Durham, North Carolina, and Portland, Oregon
We describe three children with an acute onset and spontaneous resolution of angioma-likepapules during an apparent viral illness. A biopsy specimen from one patient revealed a uniquehistologic appearance that consisted of dilated dermal blood vessels with plump hobnailshaped endothelial cells. On the basis of the natural history and histopathologic features ofthis exanthem, we suggest the name eruptive pseudoangiomatosis. (J AM ACAD DERMATOL1993;29:857-9.)
In 1969, Cherry et aU described four childrenwith an acute echovirus infection who had "hemangioma-like" skin lesions. The lesions resolved spontaneously within several days. We have recently observed three children with an identical eruption.
CASE REPORTS
Case 1
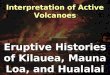
A 6-month-old white boy had two 4 mm bright-redpapules on the left cheek that developed in 24 hours(Fig. 1). The lesions blanched completely with pressureand rapidly refilled from the center on release. The onsetof the lesions coincided with the resolution of an upperrespiratory infection. The lesions resolved completely in3 days.
Case 2
A 61h-month-old white boy with an upper respiratoryinfection had bright red papules on the trunk and
From the Departments of Medicine (Dermatology),- Pediatrics,b Microbiology,d and Pathology," Duke University Medical Center, andthe Department of Dermatology," Oregon Health Sciences University.
Reprint requests: Neil S. Prose, MD, Box 3252, Duke University Medical Center, Durham, NC 27710.
Copyright © 1993 by the American Academy of Dermatology, Inc.0190-9622/93 $1.00 +.10 16/4/48323
extremities that developed during the course of 4 days.During the next 3 days several lesions resolved spontaneously and several new lesions developed. Examination revealed six I to 2 mm, bright-red angiomatous papules onthe hands, arms, and forehead (Fig. 2). The lesionsblanched completely with pressure. One week later all lesions had resolved.
Case 3
A 6-year-old white boy had fever, temporal headache,severe vomiting, and malaise for 2 days. Examination revealed enlarged and erythematous tonsils. In addition, hehad 10 blanchable angiomatous macules and papules onthe face, shoulder, arm, and back.
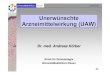
Skin biopsy specimens for light and electron microscopy were obtained from lesions on the arm. Histologicexamination revealed several dilated capillaries and smallblood vessels in the upper reticular dermis but mainly inthe papillary dermis (Fig. 3). The vessels were notincreased in number. The vessels were lined by plump endothelial cells, some of which had a hobnail appearance(Fig. 4). The nuclei were slightly enlarged and a few endothelial cells were in mitosis. There was a sparseperivascular lymphohistiocytic infiltrate. The epidermisshowed no pathologic changes.
Electron microscopy revealed swollen endothelial cellswith curly intermediate filaments that were 8 to 12 nm indiameter. These cytoplasmic filaments were believed toresult from increased activity within the endothelial cells
857

858 Prose et al.Journal of the American Academy of Dermatology
November 1993
Fig. 1. Case 1. Two blanchable angiomatous papules of I-day duration.Fig. 2. Case 2. Small blanchable angiomatous papules.Fig. 3. Case 3. Dilated blood vessels in papillary dermis and upper reticular dermis andsparse perivascular infiltrate.Fig. 4. Case 3. Higher magnification shows prominent endothelial cells lining the lumen ofa very dilated blood vessel. Some cells have a hobnail appearance.
and were not believed to be viral particles.2 No enterovirus particles were seen.
DISCUSSION
Acute hemangioma-like lesions were observed byCherry et aLl in four infants between the ages of 8and 11 months. They were described as 2 to 4 mmsparse erythematous papules surrounded by a 1 to 4mm halo ofblanching. Pressure on the center ofeachlesion resulted in complete blanching. Echovirus 25was isolated from two children, and echovirus 32 wasisolated from the other two children.
Cherryet a1. I performed no skin biopsies but recognized the unique vascular appearance of the skinlesions and suggested that viral localization in endothelial cells caused capillary dilation. They hypothesized that the lesions resulted from either a direct
effect of viral infection on endothelial cells or antigen-antibody complexes binding to endothelium.
The appearance of the skin lesions in our patientsis remarkably similar to the appearance of thelesions reported by Cherry et al. l The clinical picturesuggested a viral illness in all three children, but ourattempt to document this in one patient was unsuccessful.
The histologic appearance of dilated blood vesselswith plump endothelial cells and no evidence of vascular proliferation is unique. Because the lesionshave the clinical appearance of angiomas but showno histologic evidence of an increased number ofblood vessels, we propose the name eruptivepseudoangiomatosis.
The histologic differential diagnosis of eruptivepseudoangiomatosis includes telangiectases and spi-

Journal of the American Academy of DermatologyVolume 29, Number 5, Part 2
der angiomas. The lesions of eruptive pseudoangiomatosis can be differentiated from telangiectasesby the presence ofendothelial cells that protrude intothe vessel lumen. In spider angiomas there are centrally located dilated arterioles with thin branches,without prominence of the endothelial lining.
Clinically, eruptive pseudoangiomatosis must bedifferentiated from bacillary angiomatosis, bartonellosis, and pyogenic granuloma. In all three of thesedisorders the skin lesions are generally larger andlast considerably longer than the 7- to IO-day duration that we observed in our patients. Spontaneousresolution does not occur. The occurrence of multiple pyogenic granulomas is relatively rare.3
Histologically, eruptive pseudoangiomatosisshares with bacillary angiomatosis and bartonellosisthe presence of a prominent endothelial lining.4
However, eruptive pseudoangiomatosis shows noblood vessel proliferation, inflammatory infiltratewith neutrophils, or granular deposits that representclustered bacilli. Pyogenic granuloma is characterized by a dome-shaped proliferation of small blood
Prose et al.
vessels lined by oval endothelial cells. An epidermalcollarette and a variable degree of mixed inflammatory infiltrate may be present.
Although the data of Cherryet aLI implicated anenterovirus, the evidence linking the cutaneous lesions to a systemic viral infection in our patients wascircumstantiaL It appears most likely that eruptivepseudoangiomatosis is a viral exanthem. However, itmay be an unusual cutaneous reaction pattern toseveral different organisms.
REFERENCES1. Cherry JD, Bobinski JE, Horvath FL, et al. Acute heman
gioma-like lesions associated with ECHO viral infections.Pediatrics 1969;44:498-502.
2. Ghadially FN. Ultrastructural pathology of the cell. Stoneham, Mass.: Butterworth-Heinemann, 1975:424-8.
3. Dillman AM, Miller RC, Hansen RC. Multiple pyogenicgranulomata in childhood. Pediatr DermatoI1991;8:28-31.
4. LeBoit PE, Berger TG, Egbert BM, et al. Bacillary angiomatosis: the histopathology and differential diagnosis of apseudoneoplastic infection in patients with human immunodeficiency virus disease. Am J Surg Pathol 1989;13:90920.
Granuloma annulare perforans in herpes zosterscarsDieter Krahl, MD, Wolfgang Hartschuh, MD, and Wolfgang Tilgen, MDHeidelberg, Germany
Granuloma annulare perforans limited to a thoracic dermatome that was previously involvedby herpes zoster occurred in a 51-year-old woman who also had Lennert's lymphoma. Of thevarious local granulomatous infiltrates described after herpes zoster, granuloma annulareperforans is unique, although ordinary granuloma annulare has been described in a few patients. Ahigh incidence of specific and nonspecific reaction patterns in herpes zoster scars hasbeen described in patients with malignant lymphoma. In contrast to previous patients, all ofwhom had chronic lymphatic leukemia, our patient had Lennert's lymphoma. (J AM ACADDERMATOL 1993;29:859-62.)
Several variants ofgranuloma annulare (GA) canbe distinguished clinically and histopathologically,including the lichenoid, infiltrated, plaquelike, tu-
From the Universitals-Hautklinik, Ruprecht-Karls-University.Reprint requests: Dicter Krahl, MD, Universitats-Haulklinik, Vossslr.
2, D-6911S Heidelberg, Germany.Copyright ® 1993 by the American Academy of Dermatology, Inc.0190.9622/93 $1.00 +.10 16/4/48998
berous, subcutaneous, and perforating types withlimited, disseminated, or generalized distribution. 1
The chief histologic patterns are the palisadinggranuloma and the interstitial form. A rare epithelioid nodule type also occurs. Combinations of thesepatterns frequently occur within individual lesionsand in the same patient. Perforating granuloma annulare (PGA) shows transepidermal elimination ofdegenerated collagen from the center of palisadinggranuloma type lesions.
859