Embed Size (px)
Citation preview
Pediatric Dermatology VoL 12 No. i 21-23
Erythrokeratoderma Variabilis: Case Reportand Review of the Literature
Ronald C. Knipe, M.D.,* Franklin P. Flowers, M.D.,t Franklin R. Johnson, Jr.4Franklin L. DeBusk, M.D.,§ and Francisco A. Ramos-Caro, M.D."
*Department of Dermatology, University of Texas Medical Branch, Galveston, Texas; fDepartment ofDermatology and Cutaneous Surgery, University of Florida, Gainesville, Florida; tLouisiana State
University School of Medicine, New Orleans, Louisiana; and §Department of Pediatrics, University ofFlorida and ^^Gainesville Veterans Administration Medical Center, Gainesville, Florida
Abstract: A 5-month-old boy with erythrokeratoderma variabitis is pre-sented. The parents noted that the asymptomatic erythematous plaqueschanged over the course of hours to days. Topicai therapy with retinoicacid proved ineffective. A brief review of the literature is presented.
Erythrokeratoderma variabiiis (EKV) is a raregenodermatosis first described by Mendes da Costain 1925 (1). This disease is characterized by circum-scribed erythematous and hyperkeratotic lesions in-herited in an autosomal-dominant pattern withmarked variability of expression. Close genetic link-age has been found between EKV and the Rh locuson the short arm of chromosome I (2). In general, thelesions first develop some months after birth until thethird year, but in approximately 30% of cases the le-sions are present at birth (3). Lesions occasionally ap-pear later in chUdhood or in adolescence.
CASE REPORT
A 5-month-old boy had erythematous scaly lesionsfirst noted six hours after birth. The parents statedthat the lesions changed shape and distribution overthe course of hours and were exacerbated by coldweather and emotional stress. He was otherwisehealthy and his skin condition did not appear to besymptomatic. A detailed family history revealed noother members with a similar condition.
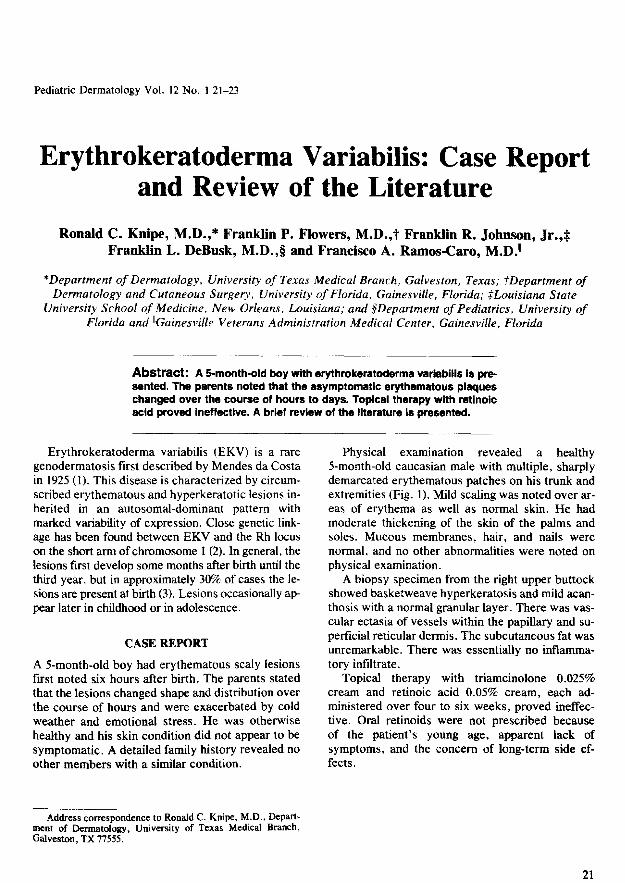
Physical examination revealed a healthy5-month-old Caucasian male with multiple, sharplydemarcated erythematous patches on his trunk andextremities (Fig. 1). Mild scaling was noted over ar-eas of erythema as well as normal skin. He hadmoderate thickening of the skin of the palms andsoles. Mucous membranes, hair, and nails werenormal, and no other abnormalities were noted onphysical examination.
A biopsy specimen from the right upper buttockshowed basketweave hyperkeratosis and mild acan-thosis with a normal granular layer. There was vas-cular ectasia of vessels within the papillary and su-perficial reticular dermis. The subcutaneous fat wasunremarkable. There was essentially no inflamma-tory infiltrate.
Topical therapy with triamcinolone 0.025%cream and retinoic acid 0.05% cream, each ad-ministered over four to six weeks, proved ineffec-tive. Oral retinoids were not prescribed becauseof the patient's young age, apparent lack ofsymptoms, and the concern of long-term side ef-fects.
Address correspondence to Ronald C. Knipe, M.D., Depart-ment of Dermatology, University of Texas Medical Branch,Galveston, TX 77555.
21
22 Pediatrie Dermatology Vol. 12 No. ! March 1995
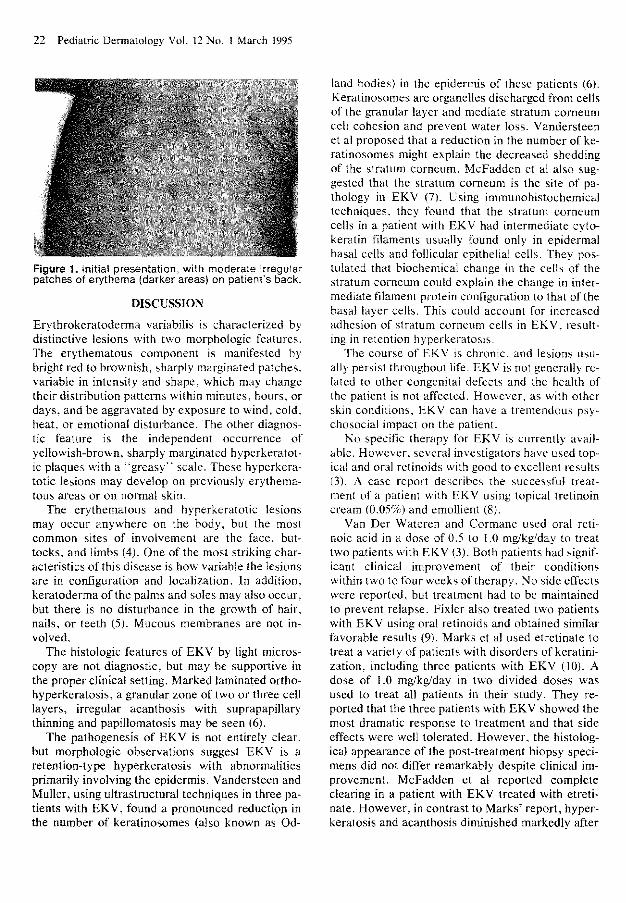
Figure 1. Initial presentation, with moderate irregularpatches of erythema (darker areas) on patient's back.
DISCUSSION
Erythrokeratoderma variabilis is characterized bydistinctive lesions with two morphologic features.The erythematous component is manifested bybright red to brownish, sharply marginated patches,variable in intensity and shape, which may changetheir distribution patterns within mitiutes, hours, ordays, and be aggravated by exposure to wind, cold,heat, or emotional disturbance. The other diagnos-tic feature is the independent occurrence ofyellowish-brown, sharply marginated hyperkeratot-ic plaques with a "greasy" scale. These hyperkera-totic lesions may develop on previously erythema-tous areas or on normal skin.
The erythematous and hyperkeratotic lesionsmay occur anywhere on the body, but the mostcommon sites of involvement are the face, but-tocks, and limbs (4). One ofthe most striking char-acteristics of this disease is how variable the lesionsare in configtjration and localization. In addition,keratoderma ofthe palms and soles may also occur,but there is no disturbance in the growth of hair,nails, or teeth (5). Mucous membranes are not in-volved.
The histologic features of EKV by light micros-copy are not diagnostic, but may be supportive inthe proper clinical setting. Marked laminated ortho-hyperkeratosis, a granular zone of two or three celllayers, irregular acanthosis with suprapapillarythinning and papillomatosis may be seen (6).
The pathogenesis of EKV is not entirely clear,but morphologic observations suggest EKV is aretention-type hyperkeratosis with abnormalitiesprimarily involving the epidermis. Vandersteen andMuller, using ultrastructural techniques in three pa-tients with EKV, found a pronounced reduction inthe number of keratinosomes (also known as Od-
iand bodies) in the epidermis of these patients (6).Keratinosomes are organelles discharged from cellsof the granular layer and mediate stratum corneumcell cohesion and prevent water loss. Vandersteenet al proposed that a reduction in the number of ke-ratinosomes might explain the decreased sheddingof the stratum corneum. McFadden et al also sug-gested that the stratum corneum is the site of pa-thology in EKV (7). Usitig immunohistochemicaltechniques, they found that the stratum corneumcells in a patient with EKV had intermediate cyto-keratin filaments usually found only in epidermalbasal cells and foUicular epithelial cells. They pos-tulated that biochemical change in the cells of thestratum corneum could explain the change in inter-mediate filament protein configuration to that ofthebasal layer cells. This could account for iticreasedadhesion of stratum corneum cells in EKV, result-ing in retention hyperkeratosis.
The course of EKV is chronic, and lesions usu-ally persist throughout life. EKV is not generally re-lated to other congenital defects and the health ofthe patient is not affected. However, as with otherskin conditions, EKV can have a tremendous psy-chosocial impact on the patient.
No specific therapy for EKV is currently avail-able. However, several investigators have used top-ical and oral retinoids with good to excellent results(3). A case report describes the successful treat-ment of a patient with EKV using topical tretinoincream (0.05%) and emollient (8).
Van Der Wateren and Cormane used oral reti-noic acid in a dose of 0.5 to 1.0 mg/kg/day to treattwo patients with EKV (3). Both patients had signif-icant clinical improvement of their conditionswithin two to four weeks of therapy. No side effectswere reported, but treatment had to be maintainedto prevent relapse. Fixler also treated two patientswith EKV using oral retinoids and obtained similarfavorable results (9). Marks et al used etretinate totreat a variety of patients with disorders of keratini-zation, including three patients with EKV (10). Adose of 1.0 mg/kg/day in two divided doses wasused to treat all patients in their study. They re-ported that the three patients with EKV showed themost dramatic response to treatment and that sideeffects were well tolerated. However, the histolog-ical appearance of the post-treatment biopsy speci-mens did not differ remarkably despite clinical im-provement. McFadden et al reported completeclearing in a patient with EKV treated with etreti-nate. However, in contrast to Marks' report, hyper-keratosis and acanthosis diminished markedly after
Knipe et al: Erythrokeratoderma Variabilis 23
treatment (7). Van der Kerhof el al successfullytreated an EKV patient with 25 to 35 mg/day of Ac-ilretin. However, they too saw rapid relapse aftertherapy ended (11).
It should be noted that, as with other keratoder-mas, not all cases of EKV respond to oral retinoids.One should carefully consider the risks of long-termoral retinoid use in EKV. a mostly asymptomatic,but admittedly emotionally troubling condition.
In conclusion, EKV is a rare, autosomal domi-nant hyperkeratotic genodermatosis. The pathogen-esis of this disorder is not well established and itscourse is chronic. Although topical retinoids havebeen successfully used to treat EKV, our patientdid not improve with this approach. EKV respondswell to oral refinoids, but relapse is the rule whentherapy is discontinued.
REFERENCES
1. Mendes Da Costa S. Erytliro-et-keratodermia Vari-abilis in a mother and a daughter, Acta Derm Ve-nereo! (Stockh) I925;6:255-261,
2, Van der Schroeff 30, Nijenhuis LE. Khan PiM, el al.Genetic linkage between erythrokeratodermia vari-abilis and Rh locus. Hum Genet 1984:68:165-168.
3, Van der Wateren AR, Cormane RH: Oral retinoicacid as therapy for erythrokeratoderraa variabilis. BrJ Dermatoi !977;97:83-85,
4, Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM,Austen KF, eds. Dermatology in General Medicine.New York: McGraw-Hill, 1987:510.
5, Schellander FG, Fritsch PO, Variable erythrokerato-derma. Arch Dermatol 1969; 100:744-748.
6, Vandersteen PR, Muller SA, Erythrokeratodermiavariabilis: an enzyme histochemical and ultrastruc-tural study. Arch Dermatoi 1971;103:362-370.
7, McFadden N, Oppedal BR, Ree K, Brandtzaeg P,Erythrokeratodermia variabilis: immunohistochemi-cal and ultrastructural studies of the epidermis. ActaDerm Venereol (Stockh) 1987:67:284-288,
8, Luy JT, Jacobs .-̂ H, Nickoioff BJ, A child with ery-thematous and hyperkeratotic patches. Archives ofDermatology 1988:124(8):1271-1272, 1274,
9, Fixler ZC, Treatment of erythrokeratodermia vari-abilis with oral synthetic retinoids. Cutis 1980:25:300-301,304,
10. Marks R, Finlay .-̂ Y, Holt P, Severe disorders of ke-ratinization: effects of treatment with tegison (etreti-nate), Br J Dermalol 1981 ;104:667-673,
11, Van der Kerkhof PCM, Steijlem PM, Van Dooren-Greebe RJ, Happle R, Acitretin in the treatment oferythrokeratodermia variabilis, Dermatologica 1990;18'l:330,






























