Embed Size (px)
Citation preview
NEW CONCEPTS AND TECHNIQUES IN PEDIATRICANESTHESIA 0889–8537/02 $16.00 � .00
ETHICAL DILEMMAS FORPEDIATRIC SURGICAL PATIENTS
Arthur M. Boudreaux, MD, and Samuel J. Tilden, MD, JD
Anesthesiologists operate in an ethically complex environment.Consider the situation of the sedated patient who presents for surgerywithout a proper consent, the patient who refuses resuscitation in theoperating suite, the patient who refuses blood transfusion on religiousgrounds, and the difficult surgeon who brings the unprepared patientfor surgery. Almost every patient encounter is replete with subtle/latentethical overtones. Most of the time, there is little or no conflict, and theencounter proceeds without incident. On occasion, a dilemma may arisein which the patient, family, and physicians have well intentioned butdiverse opinions on the proper course of action.
For the pediatric anesthesiologist, the ethical environment is evenmore complex. Because of technological advances, doctors often pursuesurgical therapies on patients with extreme degrees of prematurity, ge-netic abnormality, and other severe illnesses unlikely to be amenable tosuch efforts. Most pediatric patients are not legally able to give informedconsents for planned operations, but many patients have the develop-mental abilities to participate in the decisions involving medical care.Parents have an obligation to help decide what is best for their children,19
but do they have the ultimate control over all decisions? Consider therecently publicized case of conjoined twins in Great Britain.26 In thiscase, the involved twins shared vital organs; surgical separation wouldresult in the death of one of the twins. The parents decided to foregothe operation. A British court ruled that it was in the best interest of the
From the Departments of Anesthesiology (AMB) and Pediatrics (SJT), University ofAlabama, Birmingham, Alabama
ANESTHESIOLOGY CLINICS OF NORTH AMERICA
VOLUME 20 • NUMBER 1 • MARCH 2002 227
228 BOUDREAUX & TILDEN
children to undergo surgery despite parental objection. The procedurewas performed and one twin, as expected, died. Suppose you wereasked to provide the anesthesia for that procedure! Though daily practicedoesn’t routinely include cases wrought with such controversy, physi-cians face their share of ethical conflict. It would be nice to consulta text entitled ‘‘Everything you need to know about ethics—all situationsincluded—the final word.’’ Unfortunately, such a reference does not exist.Nor would there be uniform agreement on its contents. Information ispresented in this article to help the anesthesiologist understand ethicaldecision-making involving pediatric surgical patients. The authors dis-cuss concepts and history of autonomy and informed parental consent,an algorithm useful in moral reflection, and a likely method the legalsystem would use to render decisions in the event a court becomesinvolved. With better understanding, logical solutions to ethical dilem-mas will result.
EXAMINING AUTONOMY IN MEDICAL DECISION-MAKING
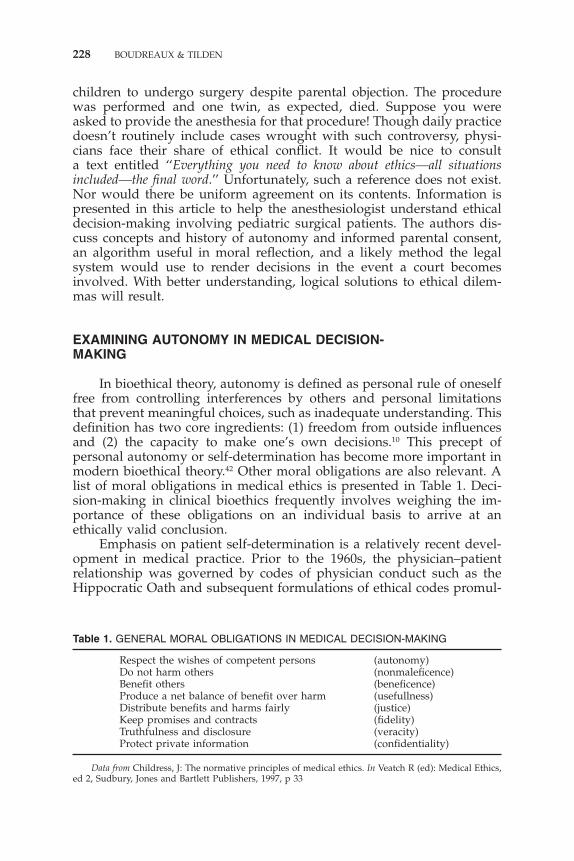
In bioethical theory, autonomy is defined as personal rule of oneselffree from controlling interferences by others and personal limitationsthat prevent meaningful choices, such as inadequate understanding. Thisdefinition has two core ingredients: (1) freedom from outside influencesand (2) the capacity to make one’s own decisions.10 This precept ofpersonal autonomy or self-determination has become more important inmodern bioethical theory.42 Other moral obligations are also relevant. Alist of moral obligations in medical ethics is presented in Table 1. Deci-sion-making in clinical bioethics frequently involves weighing the im-portance of these obligations on an individual basis to arrive at anethically valid conclusion.
Emphasis on patient self-determination is a relatively recent devel-opment in medical practice. Prior to the 1960s, the physician–patientrelationship was governed by codes of physician conduct such as theHippocratic Oath and subsequent formulations of ethical codes promul-
Table 1. GENERAL MORAL OBLIGATIONS IN MEDICAL DECISION-MAKING
Respect the wishes of competent persons (autonomy)Do not harm others (nonmaleficence)Benefit others (beneficence)Produce a net balance of benefit over harm (usefullness)Distribute benefits and harms fairly (justice)Keep promises and contracts (fidelity)Truthfulness and disclosure (veracity)Protect private information (confidentiality)
Data from Childress, J: The normative principles of medical ethics. In Veatch R (ed): Medical Ethics,ed 2, Sudbury, Jones and Bartlett Publishers, 1997, p 33

ETHICAL DILEMMAS FOR PEDIATRIC SURGICAL PATIENTS 229
gated by the American Medical Association.4 These codes consisted ofprescribed rules of behavior for the physician to follow when caring forpatients. They were based on the fundamental principle that a physicianshould act in the best interests of the patient. With this approach, manypatients, particularly those with serious medical conditions, were notapprised of their diagnoses if the physician or family feared that suchdisclosures would result in psychological harm. Treatment was pre-scribed on unilateral physician discretion. Moreover, it was not uncom-mon to include patients in human experimentation trials without in-forming them. Moral philosophers have labeled medical decision-making in this era as paternalistic.41 The concept of paternalism is aptlyillustrated by Rothman, quoting Oliver Wendell Holmes in an addressto new medical graduates:
Your patient has no more rights to all the truth you know than hehas to all the medicine in your saddlebags. . . He should get only
just so much as is good for him. . . It is a terrible thing to takeaway hope, every earthly hope, from a fellow creature.41
In the 1960s, the attitude toward medical decision-making began tochange. An important impetus was a publication in 1966 by Harvardanesthesiologist Henry Beecher, which exposed the questionable ethicalnature of a series of research studies published in reputable medicaljournals.11 Also, in 1968, initial reports of successful cardiac trans-plantations created considerable public interest on who should donateand receive transplanted organs. Furthermore, in 1969, the issue ofselective nontreatment of newborns received national attention. A childat Johns Hopkins University Hospital, with Down syndrome and duode-nal atresia, died after the parents refused surgical repair. All these eventsexposed actual or potential conflicts of interest between physicians andthe public they serve. Heightened scrutiny by governmental, legal, so-cial, and philosophical segments of society followed. Over the nextdecade, a shift in the physician–patient relationship occurred demandingfull disclosure of information and express consent to treatment.
From a legal standpoint, the concept of consent was a defense tothe international torts of battery and assault. Also, the courts had longhistories of adjudicating and preserving individual rights from govern-mental intrusion based on the constitutional protections afforded by theFourteenth Amendment, ‘‘Nor shall any state deprive any person of life,liberty, or property, without due process of law. . .’’.44 In a process muchlike bioethical decision-making, this required courts to balance the rela-tive interests of the individual and the state to determine which party’sinterests weighed more heavily. It, therefore, is not at all surprisingthat courts developed the doctrine of informed consent to protect thefundamental right of individuals to make choices when conflicts aroseregarding medical treatment involving the individual’s own body. Thisright of self-determination is categorized as a fundamental right by theU.S. Supreme Court.12 As a result, the advent of the principle of auton-
230 BOUDREAUX & TILDEN
omy in medical decision-making now fits in well with the legal conceptsembodied in a person’s freedom of choice.
Autonomy and Children
Any discussion of autonomy in the context of medical treatment ofchildren must address the inter-relationships among the physician, child,and parents. A child frequently lacks sufficient decision-making capacityto determine his or her own self interest. Generally, parents have thefundamental authority to raise and care for their children as they seefit.37 Historically, medical treatment for children proceeded under theprocess of informed parental consent with no requirement from the childto agree to treatment.
Because many pediatric patients have significant decision-makingcapacities, the process of informed parental consent has been criticizedas being inconsistent with the bioethical emphasis on autonomy. Re-cently, the American Academy of Pediatrics recommended another ap-proach to informed consent in children.3 The approach to informedconsent is composed of two elements: (1) assent of the child, and (2) aproxy consent by the parent, which is termed informed parental permission.Both elements together comprise informed consent. Assent of the patientmay be categorized as a developmentally appropriate transfer of infor-mation regarding treatment, with subsequent acceptance by the patient.The element of parental permission includes all aspects of informedconsent. Patient rejection of treatment is termed dissent. This new in-formed consent process is mandated by federal rules regulating humanexperimentation.14 Assent of the child as a research participant is re-quired unless a specified exception applies. The American Academy ofPediatrics recommends this process apply to medical treatment as well.3
ETHICAL PROBLEM SOLVING
Some prominent anesthesiologists suggest becoming leaders in ethi-cal decision-making involving patients.20 By nature of the specialty,anesthesiologists act to facilitate a surgical therapeutic plan. This plan isusually an agreement between the surgeon and the patient or family.Anesthesiologists often find themselves in conflict with the surgical planfor a variety of reasons. These conflicts, or dilemmas, may be of apractical or moral nature.9 Practical dilemmas involve conflicts betweenself-interests and moral principles or rules. Suppose a busy and de-manding surgeon must catch an airplane in 2 hours, for example. Onphysical examination of the patient, the anesthesiologist discovers aslight abnormality that warrants further laboratory testing. Should theanesthesiologist ignore the abnormality and proceed, or postpone, thecase and delay the surgeon? Self-interest issues might include avoiding
ETHICAL DILEMMAS FOR PEDIATRIC SURGICAL PATIENTS 231
delay, with its consequences of inconvenience, potential personal con-flict, loss of income, and emotional distress to the patient’s family.43 Themoral obligation might include the beneficent issue of determining riskand benefit and best preparing the patient for surgery. Because of dead-line pressure, anesthesiologists often face practical dilemmas in theirspecialties.17 A moral dilemma is a conflict between two or more moralprinciples or rules. Suppose a mature and healthy 16-year-old adolescentchild scheduled for an elective cosmetic plastic surgical procedure re-fuses the procedure on the morning of surgery. The parents and surgeonwant the anesthesiologist to proceed over the objection of the child, evenif pharmacological coercion is necessary. The child appears mature, hasdecision-making capacity, and understands the potential benefits, risks,and consequences of the procedure. A conflict exists involving the pa-tient’s right to self-determination and the desires of the parents andsurgeon to do what they believe is in the patient’s best interest. Withpractical dilemmas, the correct solution is most often obvious. Withmoral dilemmas, serious moral reflection is required to determine themost appropriate course of action.
A process of ethical decision-making might involve several steps.These include fundamental presuppositions, ethical theory, and a frame-work for analysis.35
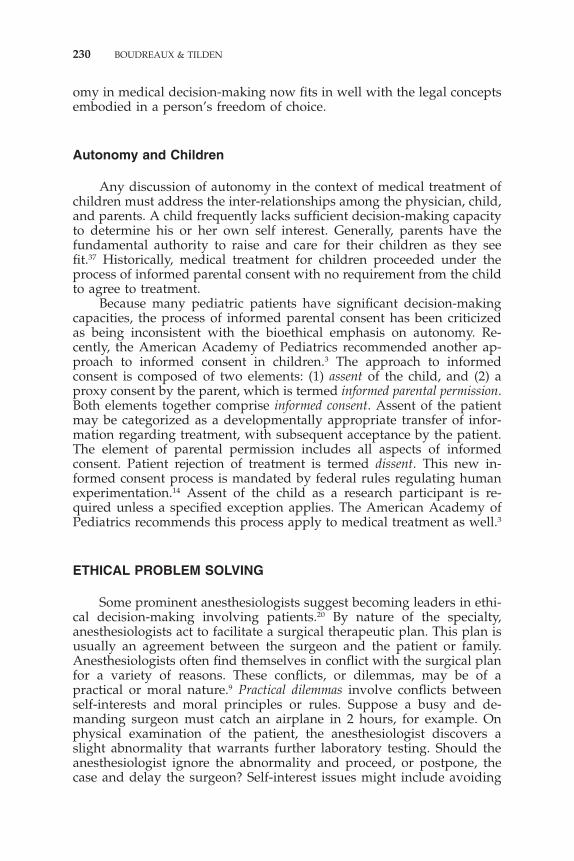
Individual personal presuppositions and biases create certainamounts of moral diversities. Because this is a multicultural society, weare assured differing views of morality.36 These views comprise the basefrom which we build a logical decision (Fig. 1). Well-intentioned andreasonable persons may disagree about the application of moral princi-ples, rules, and facts of a clinical situation.9 What is paramount to somemay be trivial to others. The influences of culture, religion, or even
Figure 1. Steps in ethical reflection. (Data from Pellegrino ED: Decisions to withdraw lifesustaining treatment: A moral algorithm. JAMA 283(8): 2000, pp 1065–67 and Pence GE:Classic Cases In Medical Ethics, ed 2. New York, McGraw-Hill, 1995, pp 4–5.)

232 BOUDREAUX & TILDEN
country of origin may influence decisions. In a recent survey of Europeanphysicians, for instance, country of origin was the most important factorin predicting physicians’ attitudes toward ethical issues in neonatal end-of-life care.40 It is easy to predict that physicians and their colleagues,patients, and the patients’ family members will occasionally reach differ-ent decisions. It is essential to understand that personal presuppositionshave major influences on decisions.
The second step is an appeal to ethical theory, principles, and rulesto justify decisions. Beauchamp and Childress9 promote a principle-based, common morality theory of bioethics that is widely taught inmedical education today. A moral dilemma is viewed in the context offour general ethical principles: beneficence, nonmaleficence, autonomy, andjustice. Beneficence is the obligation to ‘‘do good’’ for the patient. Itcomprises a group of norms for providing benefits and weighing risksand benefits. Nonmaleficence is the obligation to ‘‘do no harm.’’ Auton-omy deals with the right of patient self-determination. The concepts ofinformed consent, informed permission, assent, and surrogate decision-making fall into this category. Justice, the final principle, is an obligationto fairness, equitability, and entitlement in delivery of care. The overallgoal is a decision that satisfies all the aforementioned principles to thegreatest degree possible.
Conflict among the principles is common. It is often difficult todecide which principle takes precedence over the others in a particularcircumstance. For instance, a seemingly beneficial treatment may havegreat potential for harm or produce burdens not desired. A patient with‘‘do not resuscitate’’ orders, scheduled for surgery, is a prime exampleof potential conflict. The surgical procedure may have a significantpalliative benefit. If the need for resuscitation arises and that maneuveris carried out during the procedure, violation of the patient’s autonomymay occur. In addition, the burdens of long-term intensive care maybe set in motion. Medical societies such as the American Society ofAnesthesiologists publish guidelines to sort out these conflicts and makerecommendations for appropriate actions.5
Jonsen et al28 promote a case-based ethical reasoning model calledcasuistry.28 The model dissects the facts of a case, comparing them withprior cases that have been decided by consensus. This is similar to caselaw in the legal system. The method does not discount principles orethical rules but uses a specific practical methodology to analyze cases.
The last step is the use of a general framework for decision-making.Much like a routine evaluation in medical practice, with history, physicalexamination, assessment, and plan, Jonsen et al’s case-based reasoningdivides all cases into the following four general topics: medical indica-tions, patient preferences, quality of life, and contextual features.29 Thesetopics are present in all medical situations.
Medical indications examine information about history, physical ex-amination, laboratory results, diagnosis, prognosis, and goals of therapy.Risks, benefits, and possible burdens of treatment options are consid-ered.

ETHICAL DILEMMAS FOR PEDIATRIC SURGICAL PATIENTS 233
Patient preferences inspect issues of patient self-determination. Inpediatric practice, informed parental permission, assent or dissent of thepatient, and best-interest issues are reviewed.
Quality of life consider what effect the treatment plan will have onquality issues. Quality of life is complex and difficult to assess.30 Evalua-tions of quality of life ideally should include the perceptions of thepatient involved. This is difficult or impossible in many situations in-volving pediatric patients. The dynamic nature of quality of life assess-ments2 and the abilities of patients to adapt to their conditions are takeninto account.38
Contextual features survey other socioeconomic, family, and legalissues that may be present and compelling in the decision-making pro-cess. Family conflicts, financial burdens, and legal constraints are re-viewed.
Once all information is collected and examined, an informed andwell-reasoned decision may be agreed on. It is important to involve allrelevant parties in the decision-making process. Parents frequently feelleft out of the process, are often not informed when specialists disagreeon a course of action, and may not be told what will happen if theydisagree with the plan recommended by hospital staff.6
If we apply the aforementioned method to the 16-year-old patientscheduled for plastic surgery, the analysis might be as follows: (1) Thesurgery was indicated for correction of a congenital eyelid deformityand was totally elective, with no urgency. Risks were minimal from theprocedure and the anesthetic agent. Burdens of having or avoiding theprocedure were minimal. The parents believed it was in their daughter’sbest interest to proceed. (2) The patient did not want to undergo theprocedure and felt she was being compelled to have surgery she believedwas unnecessary. The patient was not bothered by the deformity andsaw no reason to proceed. Her mother scheduled her appointment withthe surgeon without the patient’s knowledge or any discussion. Thepatient dissented and felt she was being coerced. The father was indiffer-ent. (3) Quality of life issues are minimal. The mother believed herdaughter’s social life would be enhanced. The patient was perfectlycontent with her social life. (4) There was significant family disagree-ment. The surgeon wanted to proceed because he had scheduled theoperation and did not want to be inconvenienced. The local jurisdictionhad a ‘‘mature minors’’ doctrine in place. The anesthesiologist wascaught in the middle of the dispute. After discussion among all parties,it was agreed to postpone the procedure, allow the patient and parentstime for further reflection, and reschedule at a later time if the patientassented.
If a decision cannot be reached, help may be available through ahospital ethics committee.46 The Joint Commission on Accreditation ofHealthcare Organizations requires that each hospital develop a mecha-nism to solve ethical issues arising in clinical practice.27 Many hospitalshave appointed ethics committees to fulfill that requirement. An ethicsconsultant reviews the facts, interviews the involved parties, and gives
234 BOUDREAUX & TILDEN
an opinion using a method similar to that just described. This opinionmay be accepted or rejected by the parties involved. In the event of animpasse, a method of alternative dispute resolution may help resolvethe issue. Mediation is used successfully in some medical centers toresolve ethical disputes in an effort to avoid involvement of the courtsystem, where decisions are unpredictable. This method maintains ethi-cal decision-making within the control of the patient, family, and healthcare system.15
LEGAL CONTOURS IN MEDICAL DECISION-MAKING
Any ethical determination regarding medical treatment of a minorshould conform to lawful conduct. Fortunately, ethical disputes amongthe parties in the physician–patient relationship are uncommon. None-theless, when such disputes arise and cannot be resolved internally,individual ethical obligations may require the courts for resolution ofthe conflict, declaration of rights of the parties, and determination ofwhether an order to proceed with treatment should be issued. With thisin mind, an understanding of how courts analyze conflicts over treat-ment of minors may shed light on the relevance and limits of ethicaldecision-making. The doctrine of informed consent is usually the mecha-nism used by the courts to determine whether a minor should undergotreatment. Informed parental consent, generally, is both a necessaryand sufficient condition to proceed with treatment for minors.31 Severalexceptions originating in statutory and common laws may alter thegeneral rule and require balance among physician, child, parent, andstate interests for a proper determination.
Various competing interests come into play in the decision-makingprocess. The physician–patient relationship creates a responsibility ofthe physician to provide medical care to the child consonant with thatreasonably expected of the medical practitioner.18 Refusal of propermedical care by the parents may constitute child neglect and create astatutory duty on the physician to notify child protection services orrequest a court order authorizing treatment. Such a circumstance mightoccur in the case of an infant with life-threatening congenital heartdisease who requires cardiopulmonary bypass surgery and parents whorefuse to consent for blood transfusion for religious reasons, for instance.
The child’s and parental interests usually coincide and serve toprotect patient autonomy. Divergent interests between the child andparents may arise, however. The physician must be alert to the circum-stances in which this occurs. Parents are legally authorized to makeimportant decisions for their children based on the presumption thatthey know the interests and values of the child and act in the bestinterest of the child. Parental decision-making authority has limitationsas well. In many jurisdictions these include the ‘‘mature minor’’22 doc-trine and minor medical treatment acts,1 both of which recognize deci-sion-making input of adolescents who may have decision-making capac-ities. A court would certainly grant an order for a medically indicated

ETHICAL DILEMMAS FOR PEDIATRIC SURGICAL PATIENTS 235
blood transfusion over a parent’s objection if an adolescent minorwished to receive a blood transfusion, for instance.
The state has substantial authority to intervene on behalf of childrenin need of medical treatment. Various laws may waive the generalrequirement for parental consent in medical emergencies or conditionsin which a requirement for parental consent may discourage a minor’sinclination to seek medical care, such as chemical dependency, venerealdisease, or pregnancy.1 State child abuse and neglect statutes serve asmechanisms to outweigh parental refusal to consent to necessary medicalinterventions for their children. Even federal law mandates that statesfollow certain procedures under their child abuse and neglect statutesto safeguard treatment of disabled newborns.32 Failure to follow suchprocedures will serve to disqualify a state from federal funding of childabuse and neglect programs. Even without express statutory authority,the courts have a common law power known as parens patriae, whichrefers to the right and duty of the state to protect its children. Under thedoctrine of parens patriae, the courts may intervene in family matters tosafeguard a child’s health, educational development, and emotionalwell-being.39
JUDICIAL APPROACH
Most judicial decisions regarding medical treatment of children arebased on state law. As a result, the outcome of these judicial proceedingsmay vary from state to state, despite similar facts. The outcome iscertainly influenced by the expertise of respective counsel, weight ofprevious judicial authority, and the judge’s interpretation of the testi-mony and law. Furrow et al16 recently offered some generalizations onthe judicial approach to health care decision-making for children. First,courts are faced with two major legal presumptions that must be ad-dressed: (1) When treatment of a child averts death or significant risk ofserious harm, then treatment is warranted. And (2) the state should notintervene in the parent–child relationship without a compelling reasonto do so. These two presumptions appear similar to the bioethical princi-ples of beneficence and autonomy, respectively, and work in oppositedirections—on one hand, toward state intervention and on the other,toward parental–child autonomy. Second, when there is clear evidencerebutting both these presumptions, courts revert to balancing the respec-tive interests of parent, child, and state (including the medical profes-sion) to determine the welfare of the child. Most often, the test is whatis in the best interests of the child. Such an approach requires the courtsto analyze the following factors:
1. Seriousness of harm the child is suffering or the substantiallikelihood of serious harm (i.e., prognosis without treatment)
2. Previous medical evaluation and proposed medical treatmentand their effects on the child (i.e., invasiveness of therapy)

236 BOUDREAUX & TILDEN
3. The benefits and risks of the proposed therapy (i.e., prognosis,mortality and morbidity risks of treatment)
4. Expressed preferences of the child25, 33
Much of this analysis depends on accurate medical information. Prac-titioners seeking judicial orders to treat children over parental objectionsshould be prepared to provide the court with clinical data to assessthese factors. Following are some examples of court decisions regardingmedical treatment of children in the face of parental objections.
Case Example 1
A 16-year-old male patient who was a Jehovah’s Witness was injured in atrain accident. His upper limb was severely injured and his surgeons recom-mended a limb salvage procedure instead of simple amputation. The procedurewould definitely require a blood transfusion, which both the patient and hisfamily opposed on a religious basis. The county child protective service peti-tioned the family court for appointment of a temporary conservator to authorizemedical treatment, including surgery and blood transfusion. What was theresult? In O.G. v Baum,34 the Texas Court of Appeal upheld the appointment ofa conservator for the patient. Central to the court’s holding was that Texascommon law does not recognize the ‘‘mature minor’’ doctrine, which wouldhave allowed the minor to refuse the blood transfusion. It is likely that had thiscase been in Illinois, the court would have dismissed the case on the basis ofthe state’s ‘‘mature minor’’ doctrine.22
Case Example 2
A 15-month-old child with hydrocephalus was brought to medical attention.His parents had cared for him since birth, but because of religious beliefs theyhad not previously sought professional medical care. Child protective servicessought a petition in juvenile court granting them the authority to obtain medicalcare for the infant. What was the result? In the case of In Re: Jensen,24 the OregonCourt of Appeals granted an order for surgical intervention. Even though theinfant’s current condition was not life-threatening, the court recognized that thecondition posed a substantial likelihood of mental retardation and physicalhandicap in the future if left untreated. This decision is in contrast to thatinvolving Baby Jane Doe, a well-known New York case from 1983.45 Baby Jane Doewas born with spina bifida, hydrocephalus, and microcephaly. After receivingcontradictory expert medical advice, the parents chose not to intervene surgi-cally. The validity of this decision was upheld by the New York Court ofAppeals, and a subsequent action in federal court for violation of the federal‘‘Baby Jane Doe’’ regulations was dismissed as well. Baby Jane Doe differs fromJensen because, in Baby Jane Doe, the parents were choosing between two coursesof recommended medical care, whereas in Jensen the parents were refusing allmedical care.
Case Example 3
A 17-year-old male patient had severe scoliosis secondary to complicationsof poliomyelitis. He was unable to stand or ambulate and his physicians recom-mended a spinal fusion. The mother is a Jehovah’s Witness. She has agreed to
ETHICAL DILEMMAS FOR PEDIATRIC SURGICAL PATIENTS 237
the surgery but refuses to consent to a blood transfusion. A petition was broughtin juvenile court seeking an order for surgery and blood transfusion. Whatmight be the judicial outcome? In the Pennsylvania Supreme Court, In Re: Green23
considered similar facts and remanded the case for an evidentiary hearing ofthe minor’s preferences. Following the hearing, in which the boy rejected sur-gery, the court dismissed the petition and no surgery was performed. The courtin this instance focused on the risk of the surgery, the lack of immediate harmto the minor if surgery was not promptly performed, and the minor’s preference.The fact that the minor was nearly at the age of maturity certainly influencedthe court to not intervene. In this decision, the court decided that parent–childautonomy outweighed the risk:benefit ratio of surgery.
Case Example 4
Conjoined twins were born to Roman-Catholic parents. The infants werejoined at the pelvis, with Twin A having a normal heart and lungs and Twin Bhaving hypoplastic heart and lungs. By medical consensus, Twin B could notsurvive without the cross–circulation of Twin A. Twin B also had a severe brainmalformation. Physicians recommended surgical separation on the basis thatboth twins would not survive more than 1 year conjoined; and, if separated,Twin A would have the ability to lead a normal life. Twin B would almostcertainly not survive. The parents refused surgical intervention on the basis thatit was wrong to choose between the lives of two innocent children.
The facts of this scenario were recently faced by the British courtsIn Re: A (children).21 The High Court, affirmed by the Court of Appeals,granted an order for separation of the twins. Annas7 recently reviewedthe opinion of the British Court of Appeals in this case. Each judge inthe three-judge panel concurred with separation but no judge agreed asto why separation was justified. If the prognosis was correct—withoutseparation both twins would die within 1 year and with separation onetwin would live a normal lifespan—then the court’s decree that thetwins should be separated can be understood to maximize the potentiallives of both in the aggregate. The voluntary death of one innocent twincannot be clearly justified based on a best interest analysis of either twinalone. The best interest analysis for Twin A (survival if separationoccurs) leads to exactly the opposite conclusion for Twin B (death onseparation). But should the interest of the parents or the state controlhere? Though he personally agreed with the separation decision, Annasdisapproved of the decision of the court to override the parents’ wishes.But one must acknowledge that the parents’ decision-making capacityis, by nature, tainted by a conflict of interest. Of course the parentswanted both children to live, but if that was not an option, should bothbe allowed to die? Ultimately, the outcome may have turned on thecourt’s acceptance of the prognosis that both twins would die within ayear if not separated and on no other moral justification. In the past,courts in the United States have allowed separation of conjoined twinsin which one twin was certain to die. But, in those cases, immutableparental objection was not the main issue.8
238 BOUDREAUX & TILDEN
In difficult cases, courts analyze medical treatment of children bybalancing the interests of all parties—family autonomy versus necessarymedical treatment to promote the welfare of the child. This approach issomewhat analogous to bioethical decision-making using autonomy andbeneficence. As the examples given illustrate, similar situations/circum-stances allow for different results depending on the discretion of thecourt to accurately balance the interests. Though precedent in a jurisdic-tion is a helpful guide, the factual nature of each case precludes predic-tion of a result in any specific instance.
SUMMARY
Anesthesiologists are confronted with interesting and sometimesdifficult ethical situations in pediatric surgery. They are forced to dealwith everything from ‘‘do not resuscitate’’ issues, heroic last-chancesurgical efforts, religious and cultural conflicts, disputes among col-leagues, and situations that are, at worst, uncomfortable and, at best,miscarriages of duty. It is incumbent on anesthesiologists to learn howto logically and appropriately handle these issues. The pediatric surgicalpatient requires special consideration in bioethics. This article discussesthe principle of autonomy and its ascension in importance in bioethics.The concepts of informed parental permission, assent, and dissent arepresented. The authors provide a framework for ethical problem-solving,as well as a discussion of judicial decision-making. In addition, severalexamples of clinical–ethical situations and the processes used for resolu-tions are discussed. By using a well-reasoned ethical decision-makingprocess, any situation, from the simple conflict to the most seriousresuscitation and withdrawal of care issues, may be appropriately re-solved.
References
1. Alabama Code 22-8-4, 22-8-5, 22-8-6 (1997)2. Allison P, Locker D, Feine J: Quality of life: A dynamic construct. Soc Sci Med 45:
221–230, 19973. American Academy of Pediatrics Committee on Bioethics: Informed consent, parental
permission, and assent in pediatric practice. Pediatrics 95:314–317, 19954. American Medical Association, Council on Ethical and Judicial Affairs: Codes of
Medical Ethics: Current Opinions with Annotations. Chicago, American Medical Asso-ciation, 1998, pp xiv–xvi
5. American Society of Anesthesiologists: Ethical guidelines for the anesthesia care ofpatients with do not resuscitate orders or other directives that limit treatment: ASAStandards, Guidelines, and Statements. Park Ridge, IL, ASA, 1998, pp 13–14
6. Anderson B, Hall B: Parent’s perception of decision making for children. Journal ofLaw, Medicine, and Ethics 23:15–19, 1995
7. Annas GJ: Conjoined twins—the limits of law at the limit of life. N Engl J Med 344:1104–1108, 2001
ETHICAL DILEMMAS FOR PEDIATRIC SURGICAL PATIENTS 239
8. Annas GJ: Standard of Care: The Law of American Bioethics. New York, OxfordUniversity Press, 1993, pp 234–239
9. Beauchamp T, Childress J: Principles of Biomedical Ethics, ed 5. New York, OxfordUniversity Press, 2001
10. Beauchamp T, Childress J: Principles of Biomedical Ethics, ed 4. New York, OxfordUniversity Press, 1994, p 121
11. Beecher HK: Ethics and clinical research. N Engl J Med 74:1354–1360, 196612. Childress J: The normative principles of medical ethics. In Veatch R (ed): Medical
Ethics, ed 2. Sudbury, Jones and Bartlett Publishers, 1997, pp 33–3413. Cruzan v Director, Missouri Dept. of Health, 497 US 261, 110 SCt 2841, 111 LEd 2d
224 (1990)14. Department of Health and Human Services: Additional protections for children in-
volved as subjects in human research. 45 CFR 46. Sect 402 (b)–(c), 199115. Dubler NN, Marcus LJ: Mediating Bioethical Disputes. New York, United Hospital
Fund of New York, 199416. Furrows BR, Greaney TL, et al: Health Law, ed 2. St. Paul, MN, West Publishers, 2000,
p 86417. Gaba D, Howard S, Jump B: Production pressure in the work environment. California
anesthesiologists’ attitudes and experiences. Anesthesiology 81:488–500, 199418. Hall v Hilbum, 466 So 2d 835 (Miss 1985)19. Harrison C, Kenny N, et al: Involving children in medical decisions. In Singer P (ed):
Bioethics at the Bedside: A Clinician’s Guide. Ottawa, Canadian Medical Association,1999, pp 63–70
20. Hug CC Jr: Rovenstine lecture: Patient values, Hippocrates, science, and technology:What we (physicians) can do versus what we should do for the patient. Anesthesiology93:556–564, 2000
21. In re: A (children), 4 All ER 961 (2000)22. In re: E.G. 139 Ill. Dec. 810, p 815–816, 549 N.E. 2d 322, 327–28 (Ill. 1989)23. In re: Green, 448 Pa. 388, 292 A. 2d387 (Pa. 1972)24. In re: Jensen, 54 OR APP 1, 633 P.2d 1302 (1981)25. In re: Philip B, 156 Ca Rept 48, 92 Cal-App. 3d 796 (1979)26. Jenkins R: Siamese twin Jodie is bright and flourishing. The Sunday Times, London,
Times Newspapers, Dec. 16, 200027. Joint Commission on Accreditation of Healthcare Organizations: Comprehensive Ac-
creditation Manual for Hospitals. Oakbrook Terrace, IL, 200028. Jonsen AR, Siegler M, Winslade W: Clinical Ethics, ed 4. New York, McGraw-Hill
Health Professions Division, 199829. Jonsen AR: Case analysis in clinical ethics. J Clin Ethics 1:63–65, 199030. Leplege A, Hunt S: The problem of quality of life in medicine. JAMA 278:47–50, 199731. Mnookin RH, Weisburg D, et al: Child, Family and State: Problems and Materials on
Children and the Law, ed 4. New York, Aspen Publishers, 200032. National Child Protection Act of 1993, 42USC Sec 5118e (a) (1994 & Supp 1997)33. Newmark v Williams, 588 A 2d 11008 (Del 1991)34. O.G. v Baum, 790 SW 2d 839 (Tex App-Houston [1st Dist] 1990)35. Pellegrino ED: Decisions to withdraw life-sustaining treatment: A moral algorithm.
JAMA 283:1065–1067, 200036. Pence G: Classic Cases in Medical Ethics, ed 2. New York, McGraw-Hill, 1995, pp 3–537. Pierce v. Society of Sisters, 268 US 510 (1925)38. Postulart D, Adang E: Response shift and adaptation in chronically ill patients. Med
Decis Making 20:186–193, 200039. Prince v Massachusetts, 321 US 158, 64 SCt 438, 88 LEd 645 (1944)40. Rebagliato M, Cuttini M, et al: Neonatal end of life decision making: Physicians’
attitudes and relationship with self-reported practices in 10 European countries. JAMA284:2451–2459, 2000
41. Rothman D: Strangers at the Bedside: History of How Law and Bioethics TransformedMedical Decision-Making. Basic Books, 1991, pp 101–126
42. Schneider C: The Practice of Autonomy: Patients, Doctors, and Medical Decisions.New York, Oxford University Press, 1998, p 3

240 BOUDREAUX & TILDEN
43. Tait A, Voepel-Lewis T, et al: Cancellation of pediatric outpatient surgery: Economicand emotional implications for patients and their families. J Clin Anesth 9:213–219,1997
44. US Constitution, Amendment XIV, Sec 1. d2.45. US v Univ Hospital, 575 F Supp 607 (1983)46. Waisel D, Troug R: How an anesthesiologist can use an ethics consultation service.
Anesthesiology 87:1231–1238, 1997
Address reprint requests to
Arthur M. Boudreaux, MD619 19th Street South
Birmingham, AL 35249–6810
















![New1 Ethical Dilemmas[1]](https://img.pdfslide.net/doc/110x75/577cdffd1a28ab9e78b27109/new1-ethical-dilemmas1.jpg)









