Embed Size (px)
Citation preview

MOUNT SINAI JOURNAL OF MEDICINE 75:299–311, 2008 299
Evaluation and Treatment ofThyroid Nodules: A Clinical Guide
Juan C. Galofre, MD, PhD,1,2 Stylianos Lomvardias, MD,3 andTerry F. Davies, MD, FRCP1
1 Thyroid Research Unit, Mount Sinai School of Medicine, James J. Peters VA Medical Center, New York, NY2 Departamento de Endocrinologıa y Nutricion, Clınica Universitaria, University of Navarra, Pamplona, Spain
3 Department of Pathology, James J. Peters VA Medical Center, New York, NY
ABSTRACT
Thyroid nodules are inexplicably frequent and affectapproximately one-third of the adult population. Theappropriate clinical management is focused primarilyon excluding thyroid cancer and also on evaluat-ing thyroid dysfunction and mechanical obstruction.There remains no evidence that a benign thyroidnodule, once diagnosed appropriately, will progressto a malignant lesion. The initial evaluation shouldinclude a complete clinical review, a thyroid sono-gram by an experienced sonographer, a laboratoryassessment of thyroid function, and, where indicated,a cytological assessment of the nodule(s) by fineneedle aspiration under ultrasound guidance. Onlypatients with suppressed serum thyroid-stimulatinghormone levels, indicating hyperthyroidism, mayneed further evaluation by radioactive iodine uptakeand scanning. Optimal treatment depends on thepatient as well as the nodule characteristics. Theusual options remain a simple annual follow-up todetect changes in nodule size and thyroid func-tion and surgical removal. Levothyroxine therapyis now seldom indicated because of poor efficacyin nodule suppression and its inability to differenti-ate benign lesions from thyroid carcinoma. Clinicalguidelines have a very arbitrary recommendationof aspiration biopsy in all lesions greater than1 cm in size, but this proposal has no scientificbasis and should always be viewed in the clinicalcontext. Mt Sinai J Med 75:299–311, 2008. 2008Mount Sinai School of Medicine
Address Correspondence to:
Terry F. DaviesThyroid Research Unit
Mount Sinai Medical CenterEmail: [email protected]
Key Words: benign, diagnosis, malignant, manage-ment, multinodular, nodules, thyroid, treatment.
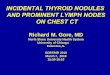
Thyroid nodules (TNs) are among the leading causesof referring patients to an endocrinologist. Indeed,by the time we reach 80 years of age, almost80% of us have 1 or more such nodules.1 Hence,the neck check has been introduced (Figure 1).2
Usually in clinical practice, when a patient noticesa lump in his neck, his principal concern is thepossibility of malignancy. However, the vast majorityof such lesions are benign, and the patient simplyrequires periodic follow-up after a careful study ofhis nodule’s characteristics. Many clinicians are usedto considering such nodules as hot or cold, but thistype of thinking no longer applies. First, all nodulestake up radioiodine, and rarely are they truly cold;second, the activity of a nodule or nodules is betterassessed by the patient’s serum thyroid-stimulatinghormone (TSH) level, which is exquisitely sensitiveto thyroid hormone output.
TNs may be single, multiple, cystic, or solidand may or may not be functional. Furthermore,they may be found in the presence of unrelatedthyroid dysfunction (eg, secondary to inflammation).Accordingly, both the thyroid functional statusand pathological evaluation need to be assessed.In addition, there is a wide spectrum of TNs,ranging from small incidentalomas to bothersome,symptomatic, large neck masses.
NOMENCLATURE
A wide variety of terms are used in discussions ofTNs. Benign and malignant are self-explanatory. Hotrefers to positive uptake of radioiodine on scanning,whereas cold is the old term suggesting a reduceduptake of radioiodine. Some people even use the
Published online in Wiley InterScience (www.interscience.wiley.com).DOI:10.1002/msj.20040
2008 Mount Sinai School of Medicine. † This article is a US government work and, as such, is in the public domain in theUnited States of America.
300 J. C. GALOFRE ETAL: EVALUATION AND TREATMENT OF THYROID NODULES
Fig 1. The thyroid neck check. All you need is aglass of water and a handheld mirror. Hold the mirror,focusing on your neck just between the Adam’s appleand the collarbone, where your thyroid is located. Whilefocusing on this area, tip your head back, take a drinkof water, and swallow. As you swallow, look at yourneck. Check for any bulges or enlargement in thisarea while you swallow. Do not confuse the Adam’sapple with the thyroid gland. Reprinted with permissionfrom http://www.thyroidawareness.com.2 Copyright 2008,American Association of Clinical Endocrinologists. [Colorfigure can be viewed in the online issue, which is availableat www.interscience.wiley.com.].
term warm for an in-between result. Cystic refers tothe accumulation of fluid seen on ultrasound (US),whereas complex refers to a lesion with both solidand cystic components. Multinodular goiter is usuallyused when there are more than 2 nodules, whereasthe term colloid goiter is now used by pathologistsonly to express the presence of colloid formation ina benign follicular lesion.
EPIDEMIOLOGY
The prevalence of TNs by physical examinationis around 5% to 10% of the population, butphysical examination of the thyroid gland hasproven to be remarkably inaccurate with the
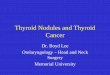
introduction of thyroid sonography. This has causedmost thyroidologists to perform their own thyroidsonographic examinations, and some of us believethat a real-time US examination is an essential partof all thyroid patient evaluations.3 Indeed, US candiscover TNs in 20% to 60% of the population,TNs being more frequent in women and theelderly4–6 (Figure 2). The old fashioned evaluationby radioiodine scanning showed that 5% to 10% ofpalpated TNs were hot, whereas approximately 85%were cold, but data from US series show a muchlower frequency of active nodules.1 Nevertheless, asignificant proportion of patients with multinodularthyroid disease have suppressed TSH levels andactive nodules. The active single nodule, however,remains relatively uncommon.
FREQUENCY OF MALIGNANCY
The risk of a TN being thyroid cancer is between1% and 10%.7 It was once thought to be betterto have more than 1 TN, but the prevalence ofcancer is similar between solitary and multinodulargoiters.8 Usually, cancers take up less radioiodinethan normal thyroid tissue and are called coldnodules on scintigraphy, but this does not meanthat cold nodule is synonymous with malignancybecause the vast majority of cold nodules are benign.Hence, routine thyroid scanning is a quite uselessand expensive evaluation.
Fig 2. Prevalence of palpable thyroid nodules detectedat autopsy or by ultrasonography (solid circles) or bypalpation (open squares) in subjects without radiationexposure or known thyroid disease. Reprinted withpermission from the New England Journal of Medicine.4
Copyright 1993, Massachusetts Medical Society.
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 301
ETIOLOGY AND NATURAL HISTORY
Many environmental and constitutional factors havebeen related to the increased risk of developing TNs9
(Table 1).The first step in the transformation of the
thyroid epithelial cell from the normal state to anabnormal state follows the generation of cellularhyperplasia. This may be induced by randomsomatic mutations or rearrangements in genes thatencode mitogen-activated protein kinase pathwayeffectors,10 the TSH receptor,11,12 or a G-protein,13
or this may follow a goitrogenic stimulus such asexcessive TSH stimulation (Figure 3). This inductionof growth exacerbates cellular mutagenesis with theformation of mutated cellular clones that generate thenodules.13–15 When the mutation results in an activeTSH receptor, the resulting nodule is autonomous,and the patient may develop hyperthyroidism and asuppressed TSH.
The evolution and natural history of TNs arevariable and unpredictable. Some TNs will continuegrowing, and some will grow to a great extentand cause tracheal obstruction, whereas others willdiminish with time, perhaps following infarctionand hemorrhage. Hence, solid nodules tend topersist, and cystic lesions sometimes spontaneouslydisappear. As more nodules develop, the chance ofan autonomous nodule being among them increases,and so a toxic multinodular goiter develops, mostcommonly in the elderly. Such TN activity may varyin time, and some autonomous lesions may evolve tocause changes in total thyroid function only afterexposure to iodine; this is seen commonly aftercomputed tomography (CT) scanning with iodine-containing contrast material. The iodine load allows
Table 1. Factors Related to Increased Risk ofThyroid Nodule Development.
Origin Event
Environmental Radiation exposureSmokingIodine deficiencyDrugsEmotional stressInfectionPregnancy
Constitutional Family historyFemale genderAge
NOTE: All these events have been related to theappearance of thyroid nodules. Nevertheless,the specific role of these factors is poorlyunderstood.
the production of thyroid hormones more efficientlythan before. Such development of autonomousnodules has been reported to occur in approximately5% of cases.16
CLINICAL MANAGEMENT
In the study of TNs, clinicians must always be awareof the possibility of thyroid cancer, and certainclinical, analytical, US, and cytological data raise thesuspicion of malignancy, but on their own, they maynot prove it. However, the presence of these riskfactors indicates a higher chance of malignancy.
Recent American and European guidelinesrecommend performing a complete evaluation onlyof those nodules that are larger than 1 cm.5,17
However, the rationale for this recommendationis bewildering.18,19 A malignant nodule starts itsevolution as a single malignant cell. In theory, someof these malignant cells may have evolved from apreviously benign abnormal cell within a TN, but themalignant transformation may also have started froma normal thyroid epithelial cell or from a thyroidstem cell.20,21 Therefore, the malignant TNs will havebeen smaller than 1 cm, and a small nodule doesnot guarantee benignity or low risk.22 In fact, somestudies have calculated that the risk of malignancy inTNs less than 1 cm in size is as much as 10%. Of evenmore concern is the finding that 70% of these patientswith small malignant nodules may have positive locallymph nodes.7
Office Evaluation
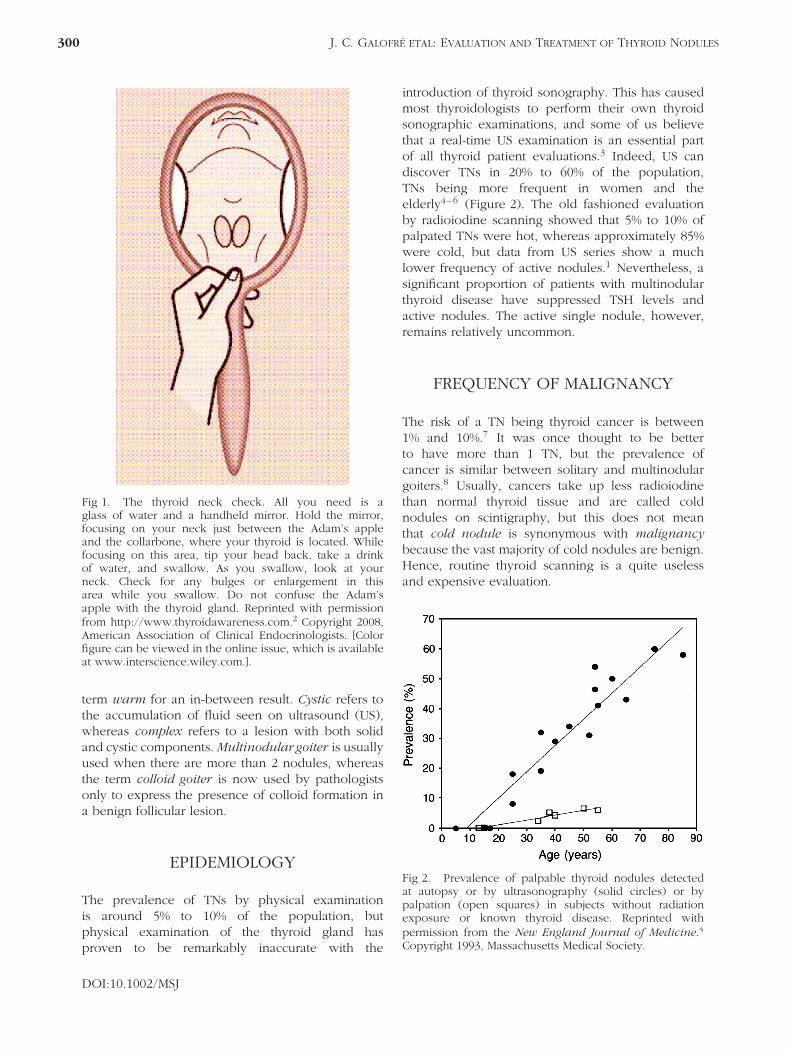
HistoryNormally functioning TNs are usually asymptomaticand are generally detected by routine neck exam-ination (Figure 4). At presentation, the patient maycomplain of the presence of a slowly growing lumpin the neck. TNs are rarely painful unless there hasbeen an acute hemorrhage. Occasionally, TNs pro-duce difficulty in swallowing that may indicate rapidgrowth, which is characteristic of malignancy. Moreoften, it is vague discomfort on swallowing. The exis-tence of a family history of benign TNs is common,and familial thyroid cancer is well described.23 Amoderate risk factor for malignancy is an age below20 years and greater than 45 years, and male genderis also a factor,5 whereas a highly suspicious indi-cator of malignancy includes a history of head andneck radiation.
DOI:10.1002/MSJ
302 J. C. GALOFRE ETAL: EVALUATION AND TREATMENT OF THYROID NODULES
Follicularcell
RET rearrangementBRAF mutation
Undifferentiatedcarcinoma
PapillaryCarcinoma
FollicularCarcinomaRas mutation?
FollicularAdenoma PPARG rearrangement
GNAS1mutationTSHR mutation
Hyper-functioningFollicular adenoma
MetastaticPapillary
Carcinoma
Cyclin D1 overexpressionp27 downregulation
TP53mutation
-
CTNNB1mutation
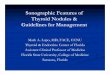
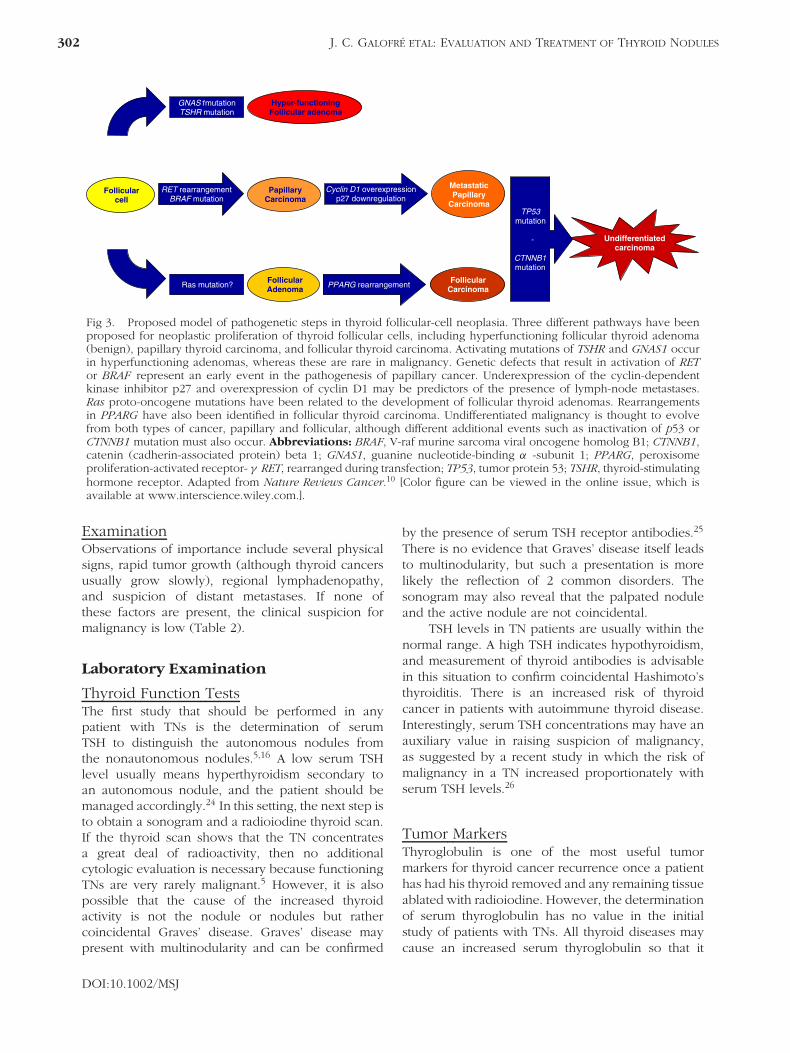
Fig 3. Proposed model of pathogenetic steps in thyroid follicular-cell neoplasia. Three different pathways have beenproposed for neoplastic proliferation of thyroid follicular cells, including hyperfunctioning follicular thyroid adenoma(benign), papillary thyroid carcinoma, and follicular thyroid carcinoma. Activating mutations of TSHR and GNAS1 occurin hyperfunctioning adenomas, whereas these are rare in malignancy. Genetic defects that result in activation of RETor BRAF represent an early event in the pathogenesis of papillary cancer. Underexpression of the cyclin-dependentkinase inhibitor p27 and overexpression of cyclin D1 may be predictors of the presence of lymph-node metastases.Ras proto-oncogene mutations have been related to the development of follicular thyroid adenomas. Rearrangementsin PPARG have also been identified in follicular thyroid carcinoma. Undifferentiated malignancy is thought to evolvefrom both types of cancer, papillary and follicular, although different additional events such as inactivation of p53 orCTNNB1 mutation must also occur. Abbreviations: BRAF, V-raf murine sarcoma viral oncogene homolog B1; CTNNB1,catenin (cadherin-associated protein) beta 1; GNAS1, guanine nucleotide-binding α -subunit 1; PPARG, peroxisomeproliferation-activated receptor- γ RET, rearranged during transfection; TP53, tumor protein 53; TSHR, thyroid-stimulatinghormone receptor. Adapted from Nature Reviews Cancer.10 [Color figure can be viewed in the online issue, which isavailable at www.interscience.wiley.com.].
ExaminationObservations of importance include several physicalsigns, rapid tumor growth (although thyroid cancersusually grow slowly), regional lymphadenopathy,and suspicion of distant metastases. If none ofthese factors are present, the clinical suspicion formalignancy is low (Table 2).
Laboratory Examination
Thyroid Function TestsThe first study that should be performed in anypatient with TNs is the determination of serumTSH to distinguish the autonomous nodules fromthe nonautonomous nodules.5,16 A low serum TSHlevel usually means hyperthyroidism secondary toan autonomous nodule, and the patient should bemanaged accordingly.24 In this setting, the next step isto obtain a sonogram and a radioiodine thyroid scan.If the thyroid scan shows that the TN concentratesa great deal of radioactivity, then no additionalcytologic evaluation is necessary because functioningTNs are very rarely malignant.5 However, it is alsopossible that the cause of the increased thyroidactivity is not the nodule or nodules but rathercoincidental Graves’ disease. Graves’ disease maypresent with multinodularity and can be confirmed
by the presence of serum TSH receptor antibodies.25
There is no evidence that Graves’ disease itself leadsto multinodularity, but such a presentation is morelikely the reflection of 2 common disorders. Thesonogram may also reveal that the palpated noduleand the active nodule are not coincidental.
TSH levels in TN patients are usually within thenormal range. A high TSH indicates hypothyroidism,and measurement of thyroid antibodies is advisablein this situation to confirm coincidental Hashimoto’sthyroiditis. There is an increased risk of thyroidcancer in patients with autoimmune thyroid disease.Interestingly, serum TSH concentrations may have anauxiliary value in raising suspicion of malignancy,as suggested by a recent study in which the risk ofmalignancy in a TN increased proportionately withserum TSH levels.26
Tumor MarkersThyroglobulin is one of the most useful tumormarkers for thyroid cancer recurrence once a patienthas had his thyroid removed and any remaining tissueablated with radioiodine. However, the determinationof serum thyroglobulin has no value in the initialstudy of patients with TNs. All thyroid diseases maycause an increased serum thyroglobulin so that it
DOI:10.1002/MSJ
MOUNT SINAI JOURNAL OF MEDICINE 303
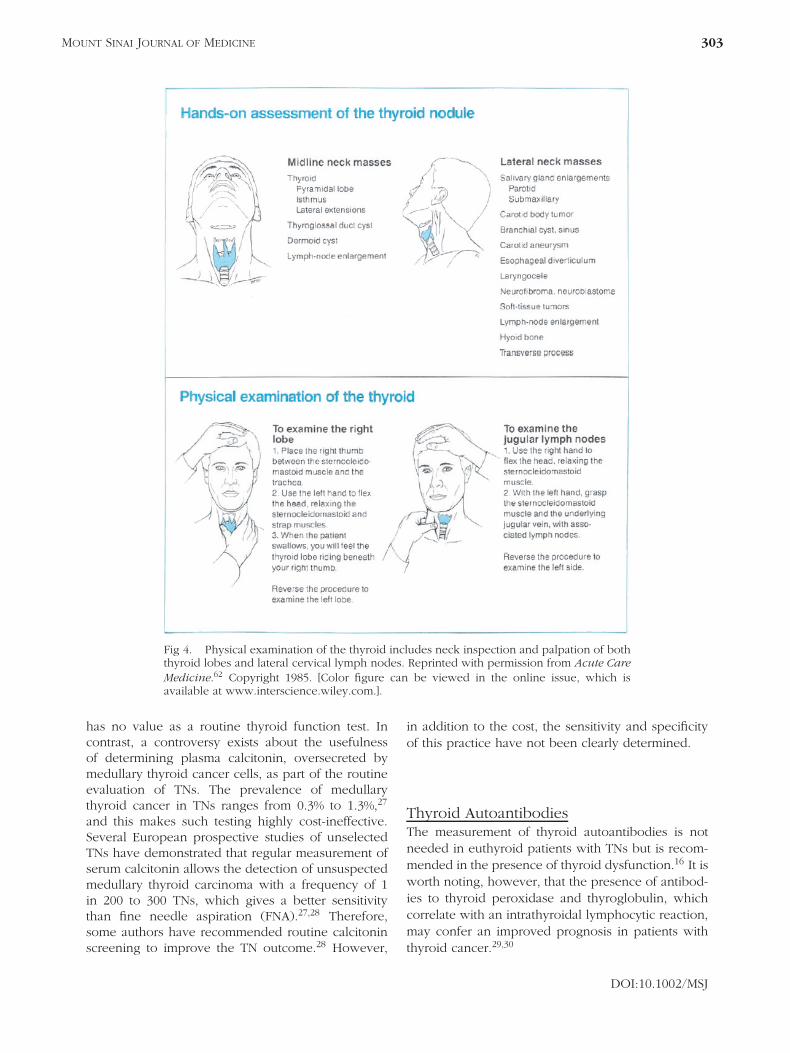
Fig 4. Physical examination of the thyroid includes neck inspection and palpation of boththyroid lobes and lateral cervical lymph nodes. Reprinted with permission from Acute CareMedicine.62 Copyright 1985. [Color figure can be viewed in the online issue, which isavailable at www.interscience.wiley.com.].
has no value as a routine thyroid function test. Incontrast, a controversy exists about the usefulnessof determining plasma calcitonin, oversecreted bymedullary thyroid cancer cells, as part of the routineevaluation of TNs. The prevalence of medullarythyroid cancer in TNs ranges from 0.3% to 1.3%,27
and this makes such testing highly cost-ineffective.Several European prospective studies of unselectedTNs have demonstrated that regular measurement ofserum calcitonin allows the detection of unsuspectedmedullary thyroid carcinoma with a frequency of 1in 200 to 300 TNs, which gives a better sensitivitythan fine needle aspiration (FNA).27,28 Therefore,some authors have recommended routine calcitoninscreening to improve the TN outcome.28 However,
in addition to the cost, the sensitivity and specificityof this practice have not been clearly determined.
Thyroid AutoantibodiesThe measurement of thyroid autoantibodies is notneeded in euthyroid patients with TNs but is recom-mended in the presence of thyroid dysfunction.16 It isworth noting, however, that the presence of antibod-ies to thyroid peroxidase and thyroglobulin, whichcorrelate with an intrathyroidal lymphocytic reaction,may confer an improved prognosis in patients withthyroid cancer.29,30
DOI:10.1002/MSJ

304 J. C. GALOFRE ETAL: EVALUATION AND TREATMENT OF THYROID NODULES
Table 2. Indicators of Possible Malignancy.
Clinical Indicators Physical Signs Sonographic Indicators
Past family history of thyroidcancer (especially inmedullary cancer)History of head and neckradiationRapid tumor growth
Hard consistencyFixation to surrounding structuresHoarseness (vocal cord palsy)Regional lymphadenopathyCompressive symptoms(dysphagia, dyspnea, or coughing)Large nodules (>4 cm)
Intranodular microcalcificationIntranodular hypervascularity(evaluated by Doppler)HypoechogenicityNodule with irregular bordersAbsence of peripheral haloPresence of regionallymphadenopathy
US Examination
Initial EvaluationThyroid US is the most accurate imaging techniquefor the detection of TNs, and this procedure ismandatory when a nodule is discovered at palpationor by any other method [eg, CT or magneticresonance (MRI)]. It is important to know thenodule size, the number of nodules (presence ofadditional nonpalpable nodules), and their locationand characteristics. In addition, US exploration isuseful for detection of suspicious lymph nodes,which is important in the assessment of malignancy.Furthermore, US has the advantage of being awell-tolerated innocuous technique with low costand no irradiation of the patient. The maindrawbacks of thyroid US are the dependence on theoperator’s experience and the difficulty in viewinglow retrosternal goiters, which may require CT/MRIevaluation.
Diagnostic AccuracyThe sonogram can help not only in the diagnosisof TNs but also in the evaluation of the nodules.However, US features of malignancy are not highlyreliable when applied to the individual patient andsimply add to the constellation of risk factors avail-able for the clinician to consider. US characteristicssuggestive of malignancy are summarized in Table 2.A combination of these findings may be highly pre-dictive for malignancy. Although such sonographiccharacteristics are superior to just nodule size foridentifying malignancy, a rapid increase in size isalso an important risk factor.31
Other Imaging Techniques
ScintigraphyThis has been the imaging technique of choiceto evaluate the functional activity of the thyroidgland and the TN in hyperthyroid states. Asalready mentioned, routine thyroid scintigraphy with
radioactive iodine (RAI) or technetium is not helpfulin the evaluation of euthyroid or hypothyroid patientswith TNs. Scintigraphy uses ionized radiation; hence,it is contraindicated in pregnancy and lactation.
CT/MRI ScanningThese techniques are particularly useful in theevaluation of retrosternal goiters. They cannotdistinguish benign TNs from malignant ones andare not as helpful as US in distinguishing benignlymph nodes from malignant ones. In TN patients, itis better to use MRI than CT because the high iodineload in the CT contrast medium can precipitate atoxic nodular goiter.32 This is not a problem withMRI contrast media.
Positron Emission TomographyPositron emission tomography evaluations are highlyinformative for thyroid functionality but have noadvantage over other scanning procedures in theroutine evaluation of TNs. A recent study showedthat fluorodeoxyglucose metabolic activity did notsignificantly differ between malignant and benignfollicular neoplasias.33
FNA
IndicationsThe general recommendation is that nodules greaterthan 1 cm in size should be biopsied. This of coursemakes no biological sense because even carcinomasstart small. However, as a practical approach, thismay be appropriate, but any fast growing lesion andany lesion with suspicious US characteristics shouldbe aspirated. Patients with suppressed TSH levelsshould have RAI scanning beforehand because thebiopsy of active nodules is not necessary.
TechniqueA #27 or #25 needle, mounted in a 10-mL syringe, ispassed through the lesion under US control. Negative
DOI:10.1002/MSJ
MOUNT SINAI JOURNAL OF MEDICINE 305
pressure is induced and released before withdrawalof the needle so that the aspirate will remain in theneedle hub. The aspirate is smeared on a glass slide,fixed, and stained for examination. Complications arerare. The patient may have at the very most somemild discomfort, swelling, and ecchymoses and mostcommonly has none of these.
Improving the Yield of FNAUS is an excellent aid for improving the accuracy ofFNA cytology. US guidance can reduce the rate ofinadequate smears from 15% to 3%.34 Since 2007, allFNA procedures should have been performed withUS guidance.5
CytologyFor determining whether a TN is malignant or benign,cytological diagnosis is, despite its limitations, stillthe most accurate and powerful preoperative studyand must be included in the initial evaluation of allTNs except the autonomous variety.5 Unfortunately,cytological reports are frequently confusing.35 Cyto-logical samples should be first divided into adequateand inadequate samples.36 The term nondiagnosticis ambiguous and should be avoided in cytologicalreports. Some authors consider adequate only thosespecimens that include 6 or more groups of 10 to 20well-preserved follicular cells on at least 2 slides.34
Inadequate samples often necessitate a repeat FNA.Data from Mount Sinai in a series of almost 500cytologic samples showed 43% of such samples tobe inadequate specimens. This high percentage isrelated to the large number of different referringphysicians (>50) who perform too few proceduresto develop good technique and confirms the impor-tance of a certain degree of skill and experienceneeded to yield useful data.37
Five Categories of Adequate Samples36
Benign This category includes adenomatous nod-ules, multinodular goiters, cysts, and thyroiditis(Figure 5). Nodules should be periodically observed,and if they are highly suspicious, FNA should berepeated. A recent study showed the result of repeatFNAs in 282 benign nodules.38 Thirty-five of the ini-tially benign nodules showed features suspicious ofmalignancy, and 7 (20%) of these suspicious nod-ules were proven to be malignant at surgery. Theauthors recommended a minimum of 3 benign FNAstudies for complete follow-up; much more than 3would certainly not seem practical. Indeed, if a clin-ician is so suspicious of malignancy that he pursues
A
C
B
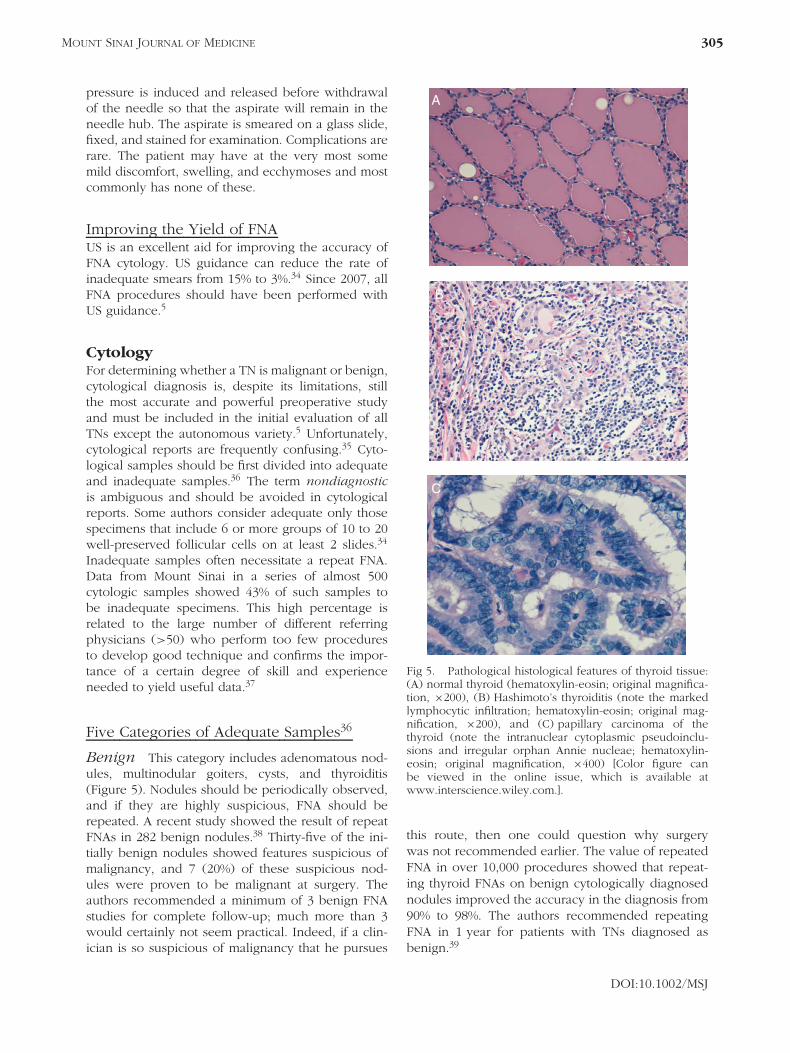
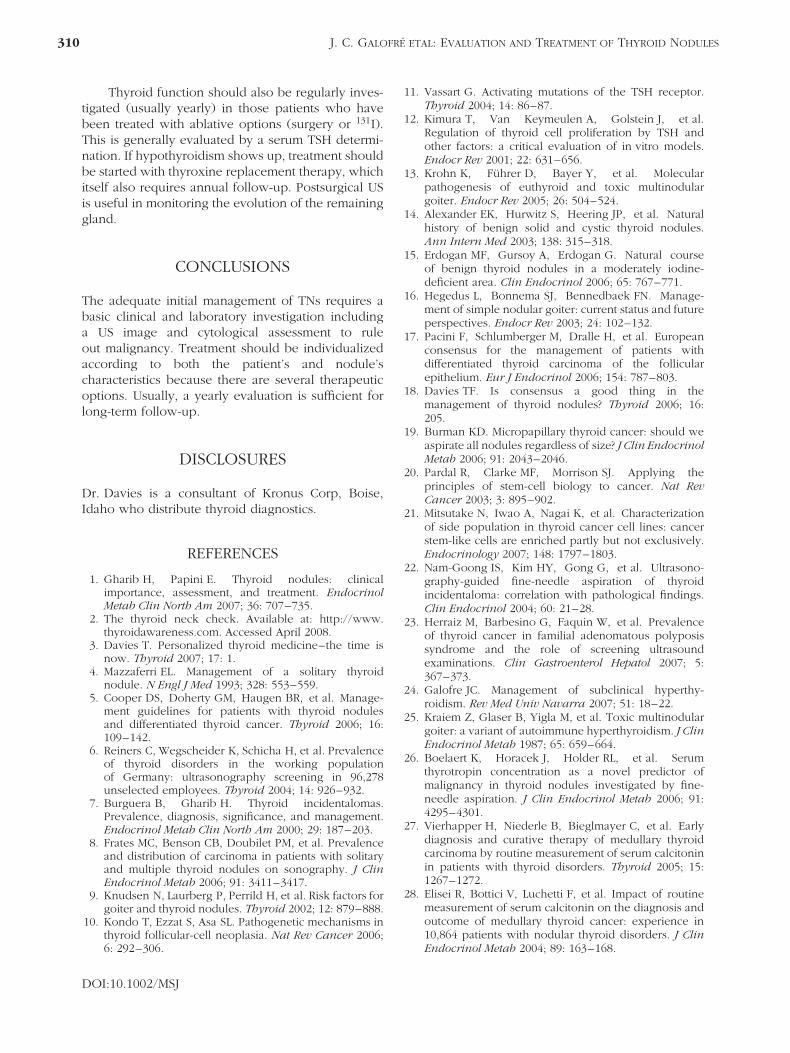
Fig 5. Pathological histological features of thyroid tissue:(A) normal thyroid (hematoxylin-eosin; original magnifica-tion, ×200), (B) Hashimoto’s thyroiditis (note the markedlymphocytic infiltration; hematoxylin-eosin; original mag-nification, ×200), and (C) papillary carcinoma of thethyroid (note the intranuclear cytoplasmic pseudoinclu-sions and irregular orphan Annie nucleae; hematoxylin-eosin; original magnification, ×400) [Color figure canbe viewed in the online issue, which is available atwww.interscience.wiley.com.].
this route, then one could question why surgerywas not recommended earlier. The value of repeatedFNA in over 10,000 procedures showed that repeat-ing thyroid FNAs on benign cytologically diagnosednodules improved the accuracy in the diagnosis from90% to 98%. The authors recommended repeatingFNA in 1 year for patients with TNs diagnosed asbenign.39
DOI:10.1002/MSJ

306 J. C. GALOFRE ETAL: EVALUATION AND TREATMENT OF THYROID NODULES
Malignant This category encompasses carcinoma(papillary, medullary, and anaplastic), lymphoma,and metastases from another primary cancer. Cytolog-ical features of papillary thyroid cancer are straight-forward, and generally the diagnosis is not an issue(Table 3 and Figure 5). The recommended procedurefor these lesions is, of course, surgical excision.
Follicular Neoplasm Approximately 15% of TNsfall under this category, which covers both benign(adenoma) and malignant (carcinoma) follicular neo-plasias. Around 20% of these cases are cancers.20
Cytology cannot usually distinguish between follic-ular adenoma and follicular carcinoma, as the cellsappear very similar. The pathological difference liesin the presence of vascular or capsular invasion, andthis feature can be evaluated only by histologicalexamination of the excised nodule. The recom-mended procedure for this category is uncertain. Theclinician must decide whether to follow the patientfor a possible increase in size or to recommend sur-gical excision. Such decisions are influenced by othersuggestive features of potential malignancy discussedearlier.
Inconclusive or Indeterminate There aresituations in which, despite the presence of adequatematerial, the cytological characteristics are notsufficient for diagnosis, as may occur in hyperplasticHurthle cell nodules, or in which features donot permit distinguishing between adenomatousnodules and follicular neoplasms. The recommendedprocedure is to repeat the FNA or to recommend
surgery if other clinical or sonographic suspiciousfeatures are present.
Suspicious for Carcinoma This category refersto cellular atypia, but the number and featuresof cells are insufficient for a definitive diagnosisof malignancy. It is recommended that surgery beadvised in this situation.
Multiple NodulesThe management of patients with multiple TNs doesnot differ from the management of patients withsolitary nodules. In the evaluation of multinodulargoiters, it is advisable to biopsy nodules showingsuspicious features on US as well as the largernodules. The prevalence of malignancy in nodulesfrom multinodular goiters is comparable to that insolitary nodules: 13% for both categories in 1 study.8
Cancer was multifocal in 46% of such cases withmultiple nodules, and 72% of cancers occurred in thelargest (dominant) nodule. It can be concluded thatin patients with 1 or more nodules, the likelihoodof thyroid cancer per patient is independent ofthe number of nodules, whereas the likelihood pernodule decreases as the number of nodules increases.For cancer exclusion in a thyroid with multiplenodules larger than 1 cm, up to 4 nodules shouldbe considered for FNA evaluation.8
Molecular Markers of MalignancyImmunohistochemical markers for abnormal proteinexpression (eg, glucose transporters and galectin)
Table 3. Cytological Categories of FNA Specimens with Suggested Management.
Category Diagnosis Suggested Management Frequency
Benign Adenomatous nodule with abundant colloidCyst, thyroiditis (chronic, acute, subacute, orfibrous), or multinodular goiter
Periodic observationincluding repeated FNA
70% (50%–90%)
Malignant Papillary, medullary, or anaplasticcarcinomasLymphoma or rarely metastases
Surgical intervention:almost always totalthyroidectomy
5% (1%–10%)
Follicular neoplasm Follicular adenoma or follicular carcinomaOxyphilic cell neoplasm
Surgical intervention:hemithyroidectomy or totalthyroidectomy
10% (5%–20%)
Inconclusive orindeterminate
Cellular adenomatous nodule versusfollicular neoplasmCellular follicular lesion favoring neoplasticnoduleHyperplastic oxyphilic (Hurthle) cellnodule
Consideration of repeatFNA or surgicalintervention:hemithyroidectomy or totalthyroidectomy
10% (5%–15%)
Suspicious forcarcinoma
Suspected papillary or medullary carcinomaCellular atypia with insufficient cellularity
Consideration of surgicalintervention
2% (0%–5%)
Inadequate Insufficient material for diagnosis Repetition of FNA 10% (5%–30%)∗
Abbreviation: FNA, fine needle aspiration.∗ This can be reduced by rebiopsy.
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 307
have been uniformly disappointing in comparisonwith direct cytology.40 However, with the identi-fication of V-raf murine sarcoma viral oncogenehomolog B1 (Braf) and rearranged during transfec-tion/papillary thyroid carcinoma (Ret-PTC) mutationsin up to 70% of papillary thyroid cancers,41 the era ofmolecular diagnostics is upon us. Preliminary stud-ies indicate that polymerase chain reaction analysisof FNA samples can contribute to the identificationof malignancy.42,43 However, to date, the sensitiv-ity of such testing does not match the cytologicalassessment but may contribute to the identification ofhigh-risk patients. In the near future, molecular mark-ers will likely succeed the cytological approach, butthey are not yet part of the routine TN evaluation.5
TREATMENT APPROACH
The treatment plan may depend on the patient’s ageand gender and the characteristics of the nodule(cytology, size, consistency, activity, and number).However, the diagnosis given by the cytologist is themost reliable indication for treatment. The clinicalcriteria should prevail only when cytological study isinconclusive.34 However, it is fair to say that thereremain significant differences between subspecialistsin treatment preferences and that this reflects the lackof evidence-based medicine in this area.44–48,50
Asymptomatic benign euthyroid TNs need onlya watchful follow-up with annual or biannual US andTSH testing. Nevertheless, on some occasions benignTNs do require therapeutic intervention, especiallywhen they grow large and low and when they causeobstructive symptoms.
Any type of malignancy (or when malignancycannot be ruled out) indicates the need for surgicalresection. The extent of surgery depends, in somecenters, on the type of tumor. Simple hemithyroidec-tomy may be recommended as the initial step fora follicular neoplasm or as the definitive treatmentfor a small, isolated papillary carcinoma if no otherrisk factors are present.5 All other thyroid malignan-cies deserve total thyroidectomy with complementarylocal node resection. If the histology of the follicularneoplasm confirms the presence of carcinoma, then atotal thyroidectomy should be completed.5 The char-acteristics of the commonest treatments for TNs aresummarized in Table 4.
Surgery
IndicationsThere are 4 major indications for thyroid surgery inpatients with TNs:
1. Suspected malignancy.2. Large goiters that generate local compressive
symptoms.3. Toxic nodules in young patients.4. Recurrent cysts after ineffective therapeutic aspira-
tions of the fluid because these lesions may havemalignant cells in up to 10% of cases.16
PrecautionsIn addition to the routine potential complicationsof thyroid surgery, including hypoparathyroidism(temporary or permanent) and damage to therecurrent laryngeal nerve (temporary or permanent),long-term compression of the trachea may lead toatrophy and tracheal collapse after surgery.
EfficacyRecurrence is common (15%–40%) in inadequatelyremoved multinodular goiters.51 A second interven-tion increases the chance of complications. Hence,we recommend a total thyroidectomy as the ini-tial procedure in patients with bilateral nodules.Presurgical thyroxine administration has been sug-gested to reduce the gland size and consequentlythe surgical risk, but there is no evidence to sup-port this approach. Also, postsurgical thyroxine isoften prescribed with the idea of suppressing anyfuture nodule formation. Although this is logical, theevidence for this maneuver is also absent.
AdvantagesIn addition to immediate relief of symptoms andconcerns, surgery provides a gland for pathologicalevaluation.
DisadvantagesThis is an expensive procedure that usually requiresat least overnight hospitalization. The associated mor-bidity and efficacy are heavily dependent on thesurgeon’s experience. The main complications arelesions of the recurrent nerve (1%) and in totalsurgery the problem of permanent hypoparathy-roidism (1%). The development of postsurgicalhypothyroidism is dependent on the amount andquality of the remaining tissue (only ∼1% withhemithyroidectomies).
Radioiodine 131I
IndicationsThe main indications for radioiodine ablation areas follows: (1) hyperfunctioning multinodular goiters
DOI:10.1002/MSJ

308 J. C. GALOFRE ETAL: EVALUATION AND TREATMENT OF THYROID NODULES
Table 4. Characteristics of the Commonest Treatments for a Thyroid Nodule.
Surgery Radioiodine Thyroxine
Mainindications
Suspected malignancyLarge goiterToxic nodulesRecurrent cyst
Hyperfunctioning nodule ormultinodular goiter(especially in the elderly)Graves’ disease
When no other treatmentoption is
possible in a euthyroid patient
Contraindications Surgical contraindications Pregnancy and lactation Low plasma TSH levelEfficacy Excellent [recurrences are
common with incompletethyroidectomy (15%–40%)]
50% goiter reduction after1 year
PoorSize reduction of 15%–40%butrecurrence if treatment isstopped
Advantages Immediate relief ofcompressive symptomsAvailability of definitivehistologic diagnosis
Medium-term relief ofsymptomsOutpatient procedure withlow costWell-toleratedRepeat treatment feasible
Low costPossible prevention of newnoduleformation
Disadvantages High cost: requiredhospitalizationSurgery-associated risks:vocal cord paralysis (1%)and hypoparathyroidism(1%)HypothyroidismRecurrences possible
Secondary effects:hypothyroidism (50%–90%),thyroiditis (1%–3%),transient enlargement, andGraves’ disease (1%–5%)Less effective in large goiters
Induction of osteopenia andatrial
fibrillationLifelong treatment
Otherconsiderations
Nodule malignancy must beruled out before treatment.Pretreatment with rhTSHmay improve the outcome.
Abbreviations: rhTSH, recombinant human thyroid-stimulating hormone; TSH, thyroid-stimulating hormone.
(for which it may be the treatment of choice);(2) hyperfunctioning single nodules; and (3) theneed to reduce the size of a normally functioningmultinodular goiter that is causing cosmetic orobstructive difficulties for the patient,51 especiallywhen surgery is contraindicated. Generally, RAI is apreferred therapeutic option for elderly patients.
PrecautionsBefore RAI administration, any possibility of malig-nancy should be ruled out. Pregnancy is of course acontraindication, but the fear of developing obstruc-tive problems after the administration of the radioio-dine is not justified by experience.52 Radiation-induced transient thyroiditis, with a tender gland andincreased thyroid hormone levels, may develop inthe week following treatment of a toxic multinodulargland, but this is more often seen after the treatmentof Graves’ disease.
DoseFor RAI, 100 to 200 µCi of I131 therapeutic activityper gram of thyroid tissue is often recommended.16,51
Generally, to ablate a gland, treatment with 20 to 30mCi achieves >90% success.51
EfficacyThe success of radioiodine treatment depends onmany factors other than the 24-hour radioiodineuptake. These include the administered dose and TNconsistency because cystic and fibrotic areas will bemore resistant to shrinkage. The decrease in nodulesize after the procedure is directly related to thedose and inversely related to the initial nodule size.In small (<100 g) multinodular goiters, the typicalreduction is about 50%, and the efficacy of thesecond dose is comparable to that of the first.53
The shrinkage normally starts in the first weeks,but the maximum result may not be achieved for 1to 2 years. Around 15% to 30% of patients requirea second dose unless maximum ablation is thegoal.
AdvantagesThis is a simple and cheap procedure that does notrequire hospitalization.
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 309
DisadvantagesIf the physician is aiming for euthyroidism, he will bedisappointed. The longer the patient is followed, thegreater the likelihood of hypothyroidism developing.Using size-related doses causes mild hypothyroidismin 10% to 40% of cases, whereas overt hypothy-roidism occurs in up to 50% of patients. Thyroidfailure develops mostly in the first 2 years aftertreatment. Hypothyroidism is particularly frequent inthose who have small goiters, anti–thyroid peroxi-dase antibodies, and/or a family history of thyroidautoimmunity.
Transient thyrotoxicosis, thyroid swelling, neckpain, and tenderness may be seen during the firstmonth after RAI in 10% of cases, but postradiationinflammation and swelling that would requiredecompressive surgery are not seen. Long-termstudies have shown that the associated risk ofnon–thyroid cancer development after RAI treatmentis small.54 However, around 1% to 5% of patientstreated with lower doses of RAI may developGraves’ disease,51 which is presumably precipitatedby the release of thyroid autoantigens and otherimmunogenic effects of radioiodine on thyroid-autoreactive lymphocytes. Graves’ disease withnodules is a known clinical entity of 2 commondisorders developing together, and RAI may causesubclinical Graves’ disease to worsen. This reactionis seen at 3 to 10 months after 131I administration andis more frequent in anti–thyroid peroxidase–positivesubjects.
Utility of Recombinant HumanThyroid-Stimulating Hormone (Thyrogen)Pretreatment with recombinant human thyroid-stimulating hormone offers the prospect that radioio-dine treatment of nontoxic nodular goiters can besimplified and improved, although more informa-tion about this strategy is needed.51 However, thisis particularly important in patients with multinodu-lar goiters and low RAI uptakes who would be besttreated with RAI. Some studies of nontoxic goitershave shown that pretreatment with 0.03 mg of recom-binant human thyroid-stimulating hormone increasesthe RAI uptake to such an extent that it allows anRAI dose reduction of 60% and improves thyroid sizereduction by 35% but with a 5-fold increase in therate of early hypothyroidism.53,55
Other Options
ThyroxineThe rationale for this strategy is to suppress the TSHstimulatory effect on the TN by providing an excess of
thyroxine in the circulation to suppress endogenousTSH levels. This strategy does not work well, andwhere it has been shown to work, any effect is lostafter withdrawal of thyroxine.56 Suppressing TSH inthis way causes atrophy of the normal thyroid, andthis may give the incorrect appearance of the nodulebecoming smaller. Given the associated risks of highthyroid hormone levels (eg, arrhythmias and bonethinning), routine thyroxine use is not recommendedbecause such side effects overcome the benefits.56,57
There are also data suggesting that thyroxine canreduce multinodular goiter size by 15% to 40% inapproximately 50% of subjects, but once again thisis likely to be mostly due to a reduction in thenormal thyroid tissue, and the same side effects areapparent.51,58
EthanolThe injection, under US control, of ethanol into a TNmay be a painful procedure. The size of the nodulesmay be reduced by 50% in 50% of patients, butusually this needs repeated sessions, sometimes upto 12.59 The danger of local fibrosis and scarring ofthe recurrent laryngeal nerve has reduced enthusiasmfor this procedure at the present time.
Laser TherapyUltrasonographically guided interstitial laser photoco-agulation has been used as a nonsurgical alternativein the treatment of benign, solitary, solid (both coldand hot) TNs in patients who cannot (or will not)undergo surgery.60,61 The technique has the advan-tage of not inducing hypothyroidism, but the efficacyis inferior to 131I in normalizing TSH in patientswith hot nodules. This procedure warrants furtherinvestigation.
The Follow-UpThe follow-up of benign euthyroid TNs dependson the clinical, US, and cytological characteristicsdescribed earlier. Usually, TNs require re-evaluationevery 6 to 18 months by clinical assessment (historyand physical examination), US, and TSH.52 Nodulesthat have been cytologically labeled as inadequate,inconclusive, or indeterminate may need more carefulmonitoring and repeat biopsies.
Substantial growth detected by US (defined as anenlargement of more than 20% or more than 2 mm)does not necessarily indicate malignancy becausebenign lesions also grow larger, but a repeat FNAshould be considered.5,34 The same recommendationis valid if new clinical or US features of malignancyappear.
DOI:10.1002/MSJ
310 J. C. GALOFRE ETAL: EVALUATION AND TREATMENT OF THYROID NODULES
Thyroid function should also be regularly inves-tigated (usually yearly) in those patients who havebeen treated with ablative options (surgery or 131I).This is generally evaluated by a serum TSH determi-nation. If hypothyroidism shows up, treatment shouldbe started with thyroxine replacement therapy, whichitself also requires annual follow-up. Postsurgical USis useful in monitoring the evolution of the remaininggland.
CONCLUSIONS
The adequate initial management of TNs requires abasic clinical and laboratory investigation includinga US image and cytological assessment to ruleout malignancy. Treatment should be individualizedaccording to both the patient’s and nodule’scharacteristics because there are several therapeuticoptions. Usually, a yearly evaluation is sufficient forlong-term follow-up.
DISCLOSURES
Dr. Davies is a consultant of Kronus Corp, Boise,Idaho who distribute thyroid diagnostics.
REFERENCES
1. Gharib H, Papini E. Thyroid nodules: clinicalimportance, assessment, and treatment. EndocrinolMetab Clin North Am 2007; 36: 707–735.
2. The thyroid neck check. Available at: http://www.thyroidawareness.com. Accessed April 2008.
3. Davies T. Personalized thyroid medicine–the time isnow. Thyroid 2007; 17: 1.
4. Mazzaferri EL. Management of a solitary thyroidnodule. N Engl J Med 1993; 328: 553–559.
5. Cooper DS, Doherty GM, Haugen BR, et al. Manage-ment guidelines for patients with thyroid nodulesand differentiated thyroid cancer. Thyroid 2006; 16:109–142.
6. Reiners C, Wegscheider K, Schicha H, et al. Prevalenceof thyroid disorders in the working populationof Germany: ultrasonography screening in 96,278unselected employees. Thyroid 2004; 14: 926–932.
7. Burguera B, Gharib H. Thyroid incidentalomas.Prevalence, diagnosis, significance, and management.Endocrinol Metab Clin North Am 2000; 29: 187–203.
8. Frates MC, Benson CB, Doubilet PM, et al. Prevalenceand distribution of carcinoma in patients with solitaryand multiple thyroid nodules on sonography. J ClinEndocrinol Metab 2006; 91: 3411–3417.
9. Knudsen N, Laurberg P, Perrild H, et al. Risk factors forgoiter and thyroid nodules. Thyroid 2002; 12: 879–888.
10. Kondo T, Ezzat S, Asa SL. Pathogenetic mechanisms inthyroid follicular-cell neoplasia. Nat Rev Cancer 2006;6: 292–306.
11. Vassart G. Activating mutations of the TSH receptor.Thyroid 2004; 14: 86–87.
12. Kimura T, Van Keymeulen A, Golstein J, et al.Regulation of thyroid cell proliferation by TSH andother factors: a critical evaluation of in vitro models.Endocr Rev 2001; 22: 631–656.
13. Krohn K, Fuhrer D, Bayer Y, et al. Molecularpathogenesis of euthyroid and toxic multinodulargoiter. Endocr Rev 2005; 26: 504–524.
14. Alexander EK, Hurwitz S, Heering JP, et al. Naturalhistory of benign solid and cystic thyroid nodules.Ann Intern Med 2003; 138: 315–318.
15. Erdogan MF, Gursoy A, Erdogan G. Natural courseof benign thyroid nodules in a moderately iodine-deficient area. Clin Endocrinol 2006; 65: 767–771.
16. Hegedus L, Bonnema SJ, Bennedbaek FN. Manage-ment of simple nodular goiter: current status and futureperspectives. Endocr Rev 2003; 24: 102–132.
17. Pacini F, Schlumberger M, Dralle H, et al. Europeanconsensus for the management of patients withdifferentiated thyroid carcinoma of the follicularepithelium. Eur J Endocrinol 2006; 154: 787–803.
18. Davies TF. Is consensus a good thing in themanagement of thyroid nodules? Thyroid 2006; 16:205.
19. Burman KD. Micropapillary thyroid cancer: should weaspirate all nodules regardless of size? J Clin EndocrinolMetab 2006; 91: 2043–2046.
20. Pardal R, Clarke MF, Morrison SJ. Applying theprinciples of stem-cell biology to cancer. Nat RevCancer 2003; 3: 895–902.
21. Mitsutake N, Iwao A, Nagai K, et al. Characterizationof side population in thyroid cancer cell lines: cancerstem-like cells are enriched partly but not exclusively.Endocrinology 2007; 148: 1797–1803.
22. Nam-Goong IS, Kim HY, Gong G, et al. Ultrasono-graphy-guided fine-needle aspiration of thyroidincidentaloma: correlation with pathological findings.Clin Endocrinol 2004; 60: 21–28.
23. Herraiz M, Barbesino G, Faquin W, et al. Prevalenceof thyroid cancer in familial adenomatous polyposissyndrome and the role of screening ultrasoundexaminations. Clin Gastroenterol Hepatol 2007; 5:367–373.
24. Galofre JC. Management of subclinical hyperthy-roidism. Rev Med Univ Navarra 2007; 51: 18–22.
25. Kraiem Z, Glaser B, Yigla M, et al. Toxic multinodulargoiter: a variant of autoimmune hyperthyroidism. J ClinEndocrinol Metab 1987; 65: 659–664.
26. Boelaert K, Horacek J, Holder RL, et al. Serumthyrotropin concentration as a novel predictor ofmalignancy in thyroid nodules investigated by fine-needle aspiration. J Clin Endocrinol Metab 2006; 91:4295–4301.
27. Vierhapper H, Niederle B, Bieglmayer C, et al. Earlydiagnosis and curative therapy of medullary thyroidcarcinoma by routine measurement of serum calcitoninin patients with thyroid disorders. Thyroid 2005; 15:1267–1272.
28. Elisei R, Bottici V, Luchetti F, et al. Impact of routinemeasurement of serum calcitonin on the diagnosis andoutcome of medullary thyroid cancer: experience in10,864 patients with nodular thyroid disorders. J ClinEndocrinol Metab 2004; 89: 163–168.
DOI:10.1002/MSJ
MOUNT SINAI JOURNAL OF MEDICINE 311
29. Baker JR Jr, Fosso CK. Immunological aspects ofcancers arising from thyroid follicular cells. EndocrRev 1993; 14: 729–746.
30. Matsubayashi S, Kawai K, Matsumoto Y, et al. Thecorrelation between papillary thyroid carcinoma andlymphocytic infiltration in the thyroid gland. J ClinEndocrinol Metab 1995; 80: 3421–3424.
31. Frates MC, Benson CB, Charboneau JW, et al.Management of thyroid nodules detected at US: Societyof Radiologists in Ultrasound consensus conferencestatement. Radiology 2005; 237: 794–800.
32. Rajatanavin R, Safran M, Stoller WA, et al. Five patientswith iodine-induced hyperthyroidism. Am J Med 1984;77: 378–834.
33. Kim JM, Ryu JS, Kim TY, et al. 18F-fluorodeoxyglucosepositron emission tomography does not predictmalignancy in thyroid nodules cytologically diagnosedas follicular neoplasm. J Clin Endocrinol Metab 2007;92: 1630–1634.
34. Castro MR, Gharib H. Continuing controversies in themanagement of thyroid nodules. Ann Intern Med 2005;142: 926–931.
35. Oertel YC. Unsatisfactory (vs. nondiagnostic) thyroidalaspirates: a semantic issue? Diagn Cytopathol 2006; 34:87–88.
36. Oertel YC. Cytopathology reports from fine needleaspirations of the thyroid gland: can they be improved?Thyroid 2007; 17: 33–35.
37. Kelman AS, Rathan A, Leibowitz J, et al. Thyroidcytology and the risk of malignancy in thyroidnodules: importance of nuclear atypia in indeterminatespecimens. Thyroid 2001; 11: 271–277.
38. Illouz F, Rodien P, Saint-Andre JP, et al. Usefulness ofrepeated fine-needle cytology in the follow-up of non-operated thyroid nodules. Eur J Endocrinol 2007; 156:303–308.
39. Oertel YC, Miyahara-Felipe L, Mendoza MG, Yu K.Value of repeated fine needle aspirations of the thyroid:an analysis of over ten thousand FNAs. Thyroid 2007;17: 1061–1066.
40. Haugen BR, Woodmansee WW, McDermott MT.Towards improving the utility of fine-needle aspirationbiopsy for the diagnosis of thyroid tumours. ClinEndocrinol 2002; 56: 281–290.
41. Xing M. BRAF mutation in thyroid cancer. Endocr RelatCancer 2005; 12: 245–262.
42. Foukakis T, Gusnanto A, Au AY, et al. A PCR-basedexpression signature of malignancy in follicular thyroidtumors. Endocr Relat Cancer 2007; 14: 381–391.
43. Delys L, Detours V, Franc B, et al. Gene expressionand the biological phenotype of papillary thyroidcarcinomas. Oncogene 2007; 26: 7894–7903.
44. Bonnema SJ, Bennedbaek FN, Wiersinga WM,Hegedus L. Management of the nontoxic multinodulargoitre: a European questionnaire study. ClinEndocrinol 2000; 53: 5–12.
45. Bennedbaek FN, Hegedus L. Management of thesolitary thyroid nodule: results of a North Americansurvey. J Clin Endocrinol Metab 2000; 85: 2493–2498.
46. Bennedbaek FN, Perrild H, Hegedus L. Diagnosis andtreatment of the solitary thyroid nodule. Resultsof a European survey. Clin Endocrinol 1999; 50:357–363.
47. Bhagat MC, Dhaliwal SS, Bonnema SJ, et al. Differ-ences between endocrine surgeons and endocrinol-ogists in the management of non-toxic multinodulargoitre. Br J Surg 2003; 90: 1103–1112.
48. Diehl LA, Garcia V, Bonnema SJ, et al. Managementof the nontoxic multinodular goiter in Latin America:comparison with North America and Europe, anelectronic survey. J Clin Endocrinol Metab 2005; 90:117–123.
50. Walsh JP, Ryan SA, Lisewski D, et al. Differencesbetween endocrinologists and endocrine surgeonsin management of the solitary thyroid nodule. ClinEndocrinol 2007; 66: 844–853.
51. Weetman AP. Radioiodine treatment for benign thyroiddiseases. Clin Endocrinol 2007; 66: 757–764.
52. Hegedus L. The thyroid nodule. N Engl J Med 2004;351: 1764–1771.
53. Albino CC, Mesa CO Jr, Olandoski M, et al.Recombinant human thyrotropin as adjuvant in thetreatment of multinodular goiters with radioiodine. JClin Endocrinol Metab 2005; 90: 2775–2780.
54. Read CH Jr, Tansey MJ, Menda Y. A 36-yearretrospective analysis of the efficacy and safety ofradioactive iodine in treating young Graves’ patients. JClin Endocrinol Metab 2004; 89: 4229–4233.
55. Nielsen VE, Bonnema SJ, Hegedus L. The effects ofrecombinant human thyrotropin, in normal subjectsand patients with goitre. Clin Endocrinol 2004; 61:655–663.
56. Sdano MT, Falciglia M, Welge JA, Steward DL. Efficacyof thyroid hormone suppression for benignthyroid nodules: meta-analysis of randomized trials.Otolaryngol Head Neck Surg 2005; 133: 391–396.
57. Koc M, Ersoz HO, Akpinar I, et al. Effect of low- andhigh-dose levothyroxine on thyroid nodule volume:a crossover placebo-controlled trial. Clin Endocrinol2002; 57: 621–628.
58. Mandel SJ, Brent GA, Larsen PR. Levothyroxinetherapy in patients with thyroid disease. Ann InternMed 1993; 119: 492–502.
59. Del Prete S, Caraglia M, Russo D, et al. Percutaneousethanol injection efficacy in the treatment of largesymptomatic thyroid cystic nodules: ten-year follow-upof a large series. Thyroid 2002; 12: 815–821.
60. Dossing H, Bennedbaek FN, Karstrup S, Hegedus L.Benign solitary solid cold thyroid nodules: US-guidedinterstitial laser photocoagulation-initial experience.Radiology 2002; 225: 53–57.
61. Dossing H, Bennedbaek FN, Bonnema SJ, et al.Randomized prospective study comparing a singleradioiodine dose and a single laser therapy sessionin autonomously functioning thyroid nodules. Eur JEndocrinol 2007; 157: 95–100.
62. Davies TF, Schwartz AE. Thyroid nodules: malignantor benign? Acute Care Med 1985; 36–45.
DOI:10.1002/MSJ