Embed Size (px)
Citation preview

T R A N S F U S I O N C O M P L I C A T I O N S
Evaluation of an automated microbiologic blood culture device for detection of bacteria in platelet components
SJ. Wagner and D. Robinette
~ ~
BACKGROUND: Automated culture methods have been used by several investigators to detect bacterial con- tamination of cellular blood components. We investi- gated several factors affecting detection by automated culture of bacteria in platelet concentrates (PCs). These factors included the initial contamination level in PCs, the PC sample volume, the PC sample time, and the white cell level in relation to bacteria levels in the PCs. STUDY DESIGN AND METHODS Staphy/mmus epidermidis or Escherichia coli was inoculated into freshly prepared PCs or white cell-reduced PCs to yield colony-forming unit (CFU) levels of 10, 1, or 0.1 per mL. At the time of inoculation (t = 0) and at t = 6, t = 24, and t = 48 hours, 0.5, 1 .O, and 2.0 mL samples of the con- taminated PCs were transferred into culture bottles. The presence of bacteria in the culture bottles was subse- quently monitored by an automated blood culturing in- strument. Bacteria levels in the PC at the time of first automated culture detection were determined by quanti- tative plating. RESULTS: E. mli was detected in 92 percent of experi- ments when 1 .O- or 2.0-mL samples were taken at t = 6 hours. At t = 24 hours, 1 00-percent detection was ob- served with all tested inoculation volumes; however, by that time, >1 O7 CFU per mL of bacteria were present in every PC. For S. epidermidis, 89 percent and 83 percent of contaminated PCs were detected with a t = 24 hour sampling time and 2.0- or 1 -0-mL sampling volume. Seven of 36 PCs with a 2.0-mL sampling volume and 10 of 36 PCs with a 1 .O-mL sampling volume contained >los CFU per mL of S. epidermidis at the time of first detection. CONCLUSION: Data from this preliminary evaluation suggest that sampling times of 24 hours or more would be necessary to provide confidence in detection of E. coli or S. epidermidis in PCs using this culture method.
he introduction of closed sterile plastic container systems for blood collection, processing, and storage greatly improved the sterility of trans- T fused components. Despite these measures,
transfusion-associated bacterial sepsis continues to be a concern in transfusion medicine. Septic deaths, although infrequent, have been a recurrent theme in the literature during the last 30 years.' Although there have been similar numbers of septic events following transfusion of red cells compared with platelet components,lB2 the frequency of sepsis from platelet transfusions is approximately 10-fold that of red cells because fewer platelet units are transfused. Investigators have explored several methods for bacterial detection in blood components, including: detection of bacterial growth by culture methods3n4; indirect measure- ment of bacterial metabolism by measurement of platelet pH5-8 and glucose levels516; indirect observation of bacterial metabolism by a change in the color of red cellss or the ces- sation of platelet swirlin@'; direct detection of bacteria by microscopic evaluation of blood smears stained with Gram's ~ t a i n ' ~ - ~ ~ or acridine orange fluorescence stain9J6J7; and direct detection of bacteria by the presence of genomic DNAlB or ribosomal RNA.81deallp a bacterial test should be simple to perform; rapid; affordable; adequately sensitive to prevent the great majority, if not all, of the episodes of transfusion-associated sepsis; and capable of detecting the numerous strains of implicated organisms. Despite many
ABBREVIATIONS: CFU = colony-forming unit(s); F4 = frequen- cy; PC(s) = platelet concentrate(s1; PRP = platelet-rich plasma; Td = time to detection.
From the Jerome H. Holland Laboratory for the Biomedical Sci- ences, American Red Cross Biomedical Services, Rockville, MD 20855.
and by a grant from Organon Teknika.
November 23,1997, and accepted December 12, 1997.
Supported by the American Red Cross Biomedical Services
Received for publication August 4, 1997; revision received
TRANSFUSION 1998;38:674-679.
674 TRANSFUSION Volume 38, July 1998

AUTOMATED MICROBIOLOGICAL CULTURE
attempts, no detection technique has been developed that meets all the requirements for a successful test.
Automated bacterial blood culturing systems satisfy many of the requirements of an ideal test. Culture tech- niques can detect a wide range of organsims at concentra- tions as low as one organism per culture bottle inoculum, and are relatively easy to use. However, detection of organ- isms by automated culture may require a 1- to 2-day incu- bation following bottle inoculation, which could reduce the availability of platelet components if units are quarantined until bacterial testing is completed. Therefore, this investi- gation focused on several factors affecting detection of bac- teria in platelet components by automated culture.
Bacterial levels implicated in transfusion-associated sepsis are poorly understood, and depend on both patient and strain factor^.'^ Nevertheless, a number of septic events have been observed after transfusion of components con- taining between lo6 and 108 colony-formingunits (CFU) per mL of bacteria20-22; one report cites a case of transfusion- associated bacteremia from a platelet unit containing lo5 CFU per mL.23
The experiments determined the level of bacteria present in deliberately inoculated platelet concentrate (PC) when an automated culture system first detected the pres- ence of bacteria. E. coli was selected to model a fast grow- ing organism and S. epidermidis was used to model a slow growing organism to reflect the diversity in species impli- cated in sepsis from platelet transfusions. The objective was to evaluate if culture conditions (time of sampling, sam- pling volume) could be identified that would permit sensi- tive detection of bacteria, and if detection occurred prior to levels reaching 105 to lo6 CFU per mL in the PC and white cell-reduced PC.
MATERIALS AND METHODS Blood collection, processing, and storage W o units ofABO-identical whole blood (450 f 50 mL) were collected into 63 mL of CPD in quad-pack container sys- tems (PL146 primary container and PL-732 platelet con- tainer, Baxter Healthcare, Deerfield, IL). W o units of plate- let-rich plasma (PRP) were prepared by centrifugation of whole blood at 1471 x g for 4 minutes. The resulting PRP units were subsequently pooled. One-half of the pool was passed through a white cell reduction filter (ATS PL, Pall Biomedical Inc, Fajardo, PR) into a PL-732 container. The other half of the pool was placed in a separate PL-732 con- tainer. PCs were prepared by centrifugation at 2995 x gfor 10 minutes at 20 to 24°C removal of all but approximately 50 mL of plasma, and resting of the undisturbed platelet pellets for approximately 1 hour before gentle resuspen- sion. PCs were stored for up to 5 days at 20 to 24°C with end- over-end agitation (Model PC400, Helmer Laboratories, Chicago, IL).
Bacterial species and culture conditlons S. epidermidis (#12228, American 'Ifrpe Culture Collection Rockville, MI)) was obtained commercially. A clinical iso- late of E. coli that is resistant to the bactericidal effects of plasma was provided by Joseph Campos, PhD (Children's National Medical Center, Washington, DC). Fresh overnight cultures of bacteria were prepared by inoculating single- colony isolates into trypticase soy broth (Becton Dickinson, Cockeysville, MD) and then incubating the broth at 30°C under aerobic conditions. Cultures were diluted in unbuf- fered sterile saline immediately before their inoculation into PCs.
We determined bacterial counts by 1 -in- 10 serial dilu- tion of fully mixed samples in unbuffered saline. Diluted samples were added to 3.0 mL of 0.8-percent molten agar (43"C), and onto trypticase soy agar plates. E. coli and S. epidermidis colonies were counted after incubation at 30°C for 16 to 24 or 40 to 48 hours, respectively. All colonies from all plates that contained up to 1000 colonies were enumer- ated.
The level of bacteria in the fresh overnight culture was estimated, and appropriate dilutions were calculated for the inoculation of 1.0 mL of the diluted suspension into the filtered and unfiltered PCs (approx. 50 mL each). Levels of bacteria in the inocula were determined by quantitative counts; initial bacterial levels in the PCs (calculated from inoculalevels) averaged (n=6) 8.2* 1.2,0.91*0.13,and0.14 f 0.07 CFU per mLforE. coliand 7.0 f 2.3,1.2 f 0.4, and 0.1 f 0.05 CFU per mL for S. epidermidis.
Experimental design In total, 72 PCs were used.The experiment employed a pool and split design. For each of the two studied bacteria, 36 PCs were pooled in pairs, split, and stored in PL-732 con- tainers. One of each of the 18 pairs was then white cell re- duced. Six pairs were inoculated within 1 hour of platelet preparation to achieve a final concentration of either 10,1, or 0.1 CFU per mL. We defined the time of inoculation as t = 0. At t = 0, t = 6, t = 24, and t = 48 hours, we withdrew 0.5- mL, 1.0-mL, and 2.0-mL samples from the contaminated PCs. The samples were inoculated into 40-mLvented adult aerobic culture bottles (BacTIAlert, Organon Teknika, Durham, NC) (10 and 1 CFU/mL PC inocula) or 20-mL BacTlAlert vented pediatric aerobic culture bottles (0.1 CFUlmL PC inocula). The pediatric culture bottles were used with the 0.1 CFU per mL inocula to improve the time to detection of S. epidermidis. Culture bottles were incu- bated with shaking at 34 to 35°C for up to 5 days. For each inoculated bottle, the time to first detection was captured by the automated culture system (BacT/Alert 240, Organon Teknika) .
The levels of bacteria in the contaminated PCs were also determined by quantitatively plating diluted and un- diluted samples of the contaminated PC at t = 0, t = 6, t =
Volume 38, July 1998 TRANSFUSION 675
WAGNER AND ROBINETTE
24, t = 48, t = 72, and t = 96 hours. For experiments per- formed with E. coli, we determined bacterial levels in the PC at an additional timepoint between t = 6 and t = 24 for improved quantitation of the organism's growth. For each experiment, a logarithmic growth curve was prepared and the level of bacteria in the PC was determined at the time of first detection by the BacTlAlert 240.
Statistical analysis Average times to first detection and average bacterial lev- els in the PC at the time of first detection were calculated as well as their respective standard deviations. Because of their different growth rates, results from experiments with E. coli and S. epidermidiswere analyzed separately. Results obtained with a specified bacterial inoculum level, sam- pling time, and volume were similar for PCs and white cell reduced PCs (overlapping average values with standard deviations). As a result, their respective data were pooled. Data results were expressed as the number of experiments, of a total of 12 experiments (6 PCs and 6 white cell-reduced PCs for one inoculation level, sampling time, and sampling volume), in which bacteria were detected. This frequency of detection was compared at each condition by Fisher's exact test (Instat, GraphPad Software, San Diego, CA) .Wo- tailed p values were considered significant with p<0.05.
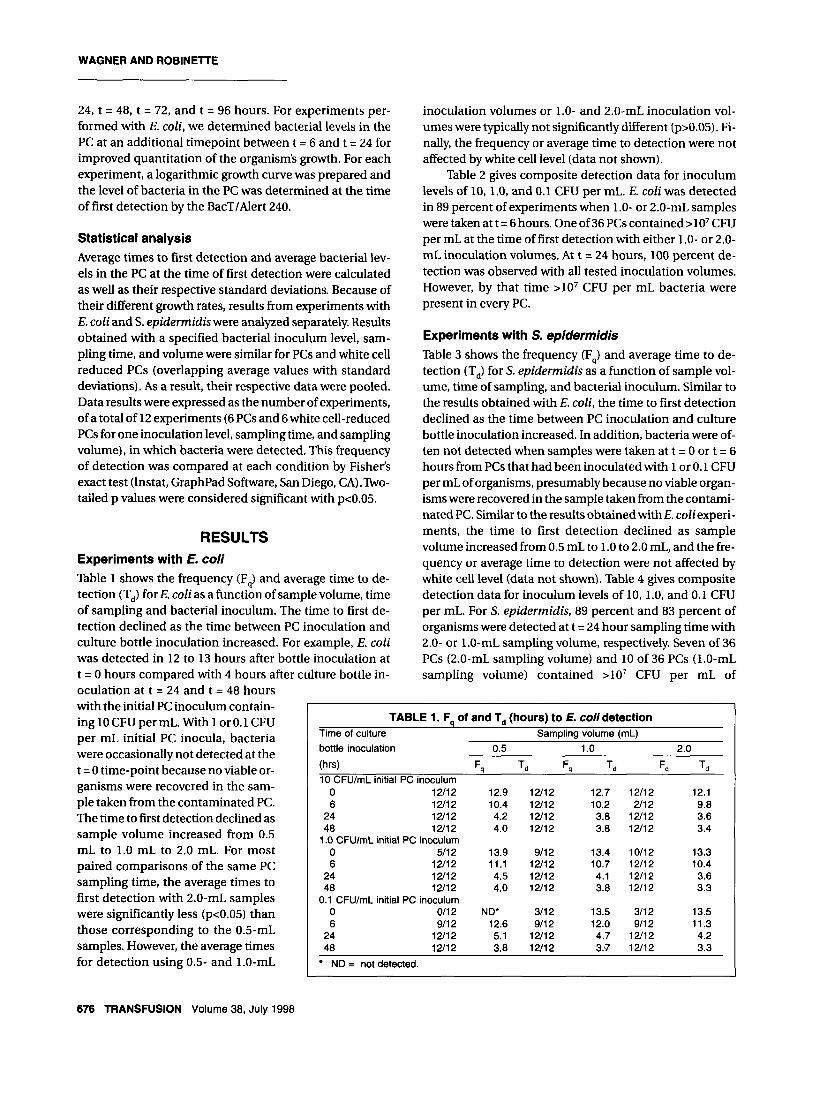
RESULTS Experiments with E. coli Table 1 shows the frequency (F,) and average time to de- tection (T,) for E. coli as a function of sample volume, time of sampling and bacterial inoculum. The time to first de- tection declined as the time between PC inoculation and culture bottle inoculation increased. For example, E. coli was detected in 12 to 13 hours after bottle inoculation at t = 0 hours compared with 4 hours after culture bottle in- oculation at t = 24 and t = 48 hours with the initial PC inoculum contain- ing 10 CFU per mL. With 1 or 0.1 CFU per mL initial PC inocula, bacteria were occasionally not detected at the t = 0 time-point because no viable or- ganisms were recovered in the sam- ple taken from the contaminated PC. The time to first detection declined as sample volume increased from 0.5 mL to 1.0 mL to 2.0 mL. For most paired comparisons of the same PC sampling time, the average times to first detection with 2.0-mL samples were significantly less (p<0.05) than those corresponding to the 0.5-mL samples. However, the average times for detection using 0.5- and 1.0-mL
inoculation volumes or 1.0- and 2.0-mL inoculation vol- umes were typically not significantly different (p>0.05). Fi- nally, the frequency or average time to detection were not affected by white cell level (data not shown).
Table 2 gives composite detection data for inoculum levels of 10, 1.0, and 0.1 CFU per mL. E. coli was detected in 89 percent of experiments when 1.0- or 2.0-mL samples were taken at t = 6 hours. One of 36 PCs contained >lo7 CFU per mL at the time of first detection with either 1.0- or 2.0- mL inoculation volumes. At t = 24 hours, 100 percent de- tection was observed with all tested inoculation volumes. However, by that time >lo7 CFU per mL bacteria were present in every PC.
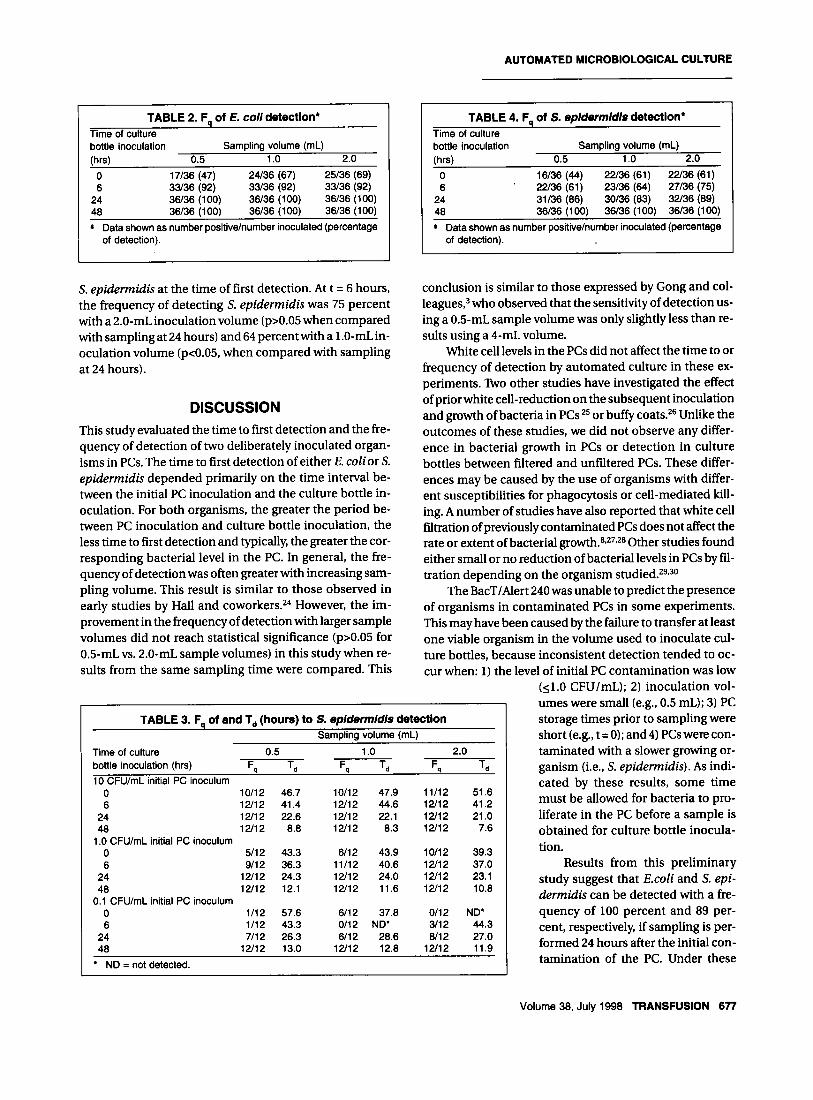
Experiments with S. epidermidis Table 3 shows the frequency (F,) and average time to de- tection (T,) for S. epidermidis as a function of sample vol- ume, time of sampling, and bacterial inoculum. Similar to the results obtained with E. coli, the time to first detection declined as the time between PC inoculation and culture bottle inoculation increased. In addition, bacteria were of- ten not detected when samples were taken at t = 0 or t = 6 hours from PCs that had been inoculated with 1 or 0.1 CFU per mL of organisms, presumably because no viable organ- isms were recovered in the sample taken from the contami- nated PC. Similar to the results obtainedwithE. coliexperi- ments, the time to first detection declined as sample volume increased from 0.5 mL to 1.0 to 2.0 mL, and the fre- quency or average time to detection were not affected by white cell level (data not shown). Table 4 gives composite detection data for inoculum levels of 10, 1.0, and 0.1 CFU per mL. For S. epidermidis, 89 percent and 83 percent of organisms were detected at t = 24 hour sampling time with 2.0- or 1.0-mL sampling volume, respectively. Seven of 36 PCs (2.0-mL sampling volume) and 10 of 36 PCs (1.0-mL sampling volume) contained >lo7 CFU per mL of
TABLE 1. F, of and T, (hours) to E. coli detection Time of culture bottle inoculation 0.5 1 .o 2.0
Sampling volume (mL)
(hr4 Fq T d F, Td Fq Td 10 CFUImL initial PC inoculum
0 1211 2 12.9 12/12 12.7 12/12 12.1 6 12/12 10.4 12/12 10.2 2/12 9.8
24 12/12 4.2 12/12 3.8 12/12 3.6 48 12/12 4.0 12/12 3.8 12/12 3.4
0 511 2 13.9 9/12 13.4 10112 13.3 6 12/12 11.1 12/12 10.7 12/12 10.4
24 1211 2 4.5 12/12 4.1 12/12 3.6 48 12/12 4.0 12/12 3.8 12/12 3.3
0 0112 ND' 311 2 13.5 3/12 13.5 6 911 2 12.6 9/12 12.0 9/12 11.3
24 12/12 5.1 12/12 4.7 12/12 4.2 48 12/12 3.8 12/12 3.7 12/12 3.3
1 .O CFU/mL initial PC inoculum
0.1 CFUImL initial PC inoculum
ND = not detected.
676 TRANSFUSION Volume 38, July 1998
AUTOMATED MICROBIOLOGICAL CULTURE
TABLE 2. F of E. Coll detection* Time of culture bottle inoculation Sampling volume (mL) (hrs) 0.5 1 .o 2.0
0 17/36 (47) 24/36 (67) 25/36 (69) 6 33/36 (92) 33/36 (92) 33/36 (92)
24 36/36 (100) 36/36 (100) 36/36 (100) 40 36/36 1100) 36/36 (100) 36/36 (100)
Data shown as number positivelnumber inoculated (percentage of detection).
TABLE 4. F, of S. epldermldls detection' Time of culture bottle inoculation Sampling volume (mL) (hrs) 0.5 1 .o 2.0
0 16/36 (44) 22/36 (61) 22/36 (61) 6 ' 22/36 (61) 23/36 (64) 27/36 (75)
24 31/36 (86) 30136 (83) 32/36 (89) 48 36/36 (100) 36/36 (100) 36/36 (100)
Data shown as number positivelnumber inoculated (percentage of detection).
:. epidermidis at the time of first detection. At t = 6 hours, the frequency of detecting S. epidermidis was 75 percent with a 2.0-mL inoculation volume (p>0.05 when compared with sampling at 24 hours) and 64 percent with a 1.0-mL in- oculation volume (p<0.05, when compared with sampling at 24 hours).
DISCUSSION This study evaluated the time to first detection and the fre- quency of detection of two deliberately inoculated organ- isms in PCs. The time to first detection of either E. colior s. epidermidis depended primarily on the time interval be- tween the initial PC inoculation and the culture bottle in- oculation. For both organisms, the greater the period be- tween PC inoculation and culture bottle inoculation, the less time to first detection and typically, the greater the cor- responding bacterial level in the PC. In general, the fre- quency of detection was often greater with increasing sam- pling volume. This result is similar to those observed in early studies by Hall and coworkers.24 However, the im- provement in the frequency of detection with larger sample volumes did not reach statistical significance (p>0.05 for 0.5-mL vs. 2.0-mL sample volumes) in this study when re- sults from the same sampling time were compared. This
conclusion is similar to those expressed by Gong and col- l eague~,~ who observed that the sensitivity of detection us- ing a 0.5-mL sample volume was only slightly less than re- sults using a 4-mL volume.
White cell levels in the PCs did not affect the time to or frequency of detection by automated culture in these ex- periments. 'Iko other studies have investigated the effect of prior white cell-reduction on the subsequent inoculation and growth of bacteria in PCs 25 or buffy coats.26 Unlike the outcomes of these studies, we did not observe any differ- ence in bacterial growth in PCs or detection in culture bottles between filtered and unfiltered PCs. These differ- ences may be caused by the use of organisms with differ- ent susceptibilities for phagocytosis or cell-mediated kill- ing. A number of studies have also reported that white cell filtration of previously contaminated PCs does not affect the rate or extent of bacterial g r ~ w t h . ~ ~ * ~ ~ * ~ Other studies found either small or no reduction of bacterial levels in PCs by fil- tration depending on the organism ~ t u d i e d . ~ ~ * ~ ~
The BacT/Alert 240 was unable to predict the presence of organisms in contaminated PCs in some experiments. This may have been caused by the failure to transfer at least one viable organism in the volume used to inoculate cul- ture bottles, because inconsistent detection tended to oc- cur when: I ) the level of initial PC contamination was low
(11.0 CFU/mL); 2) inoculation vol-
TABLE 3. F of and T, (hours) to S. epldermldls detectlon SamDlina volume ImL)
_ _ _ _ _ ~ ~
Time of culture 0.5 bottle inoculation (hrs) F- T, F- T, F. T.4
1 .o 2.0
. . 9
10 CFUlmL initial PC inoculum 0 10112 46.7 10112 47.9 11/12 51.6 6 12/12 41.4 12/12 44.6 12/12 41.2
24 12/12 22.6 12/12 22.1 12/12 21.0 48 12/12 8.8 12/12 8.3 12/12 7.6
1 .O CFUlmL initial PC inoculum 0 5/12 43.3 6/12 43.9 10112 39.3 6 9/12 36.3 11/12 40.6 12/12 37.0
24 12/12 24.3 12/12 24.0 12/12 23.1 48 12/12 12.1 12/12 11.6 12/12 10.8
0 1/12 57.6 6/12 37.0 0112 ND' 6 1/12 43.3 0112 ND' 3/12 44.3
24 7/12 26.3 6/12 28.6 8/12 27.0 40 12/12 13.0 12/12 12.8 12/12 11.9
0.1 CFUImL initial PC inoculum
ND = not detected.
umes were small (e.g., 0.5 mL); 3) PC storage times prior to sampling were short (e.g., t = 0); and 4) PCs were con- taminated with a slower growing or- ganism (i.e., S. epidermidis). As indi- cated by these results, some time must be allowed for bacteria to pro- liferate in the PC before a sample is obtained for culture bottle inocula- tion.
Results from this preliminary study suggest that Emli and S. epi- dermidis can be detected with a fre- quency of 100 percent and 89 per- cent, respectively, if sampling is per- formed 24 hours after the initial con- tamination of the PC. Under these
Volume 38, July 1998 TRANSFUSION 677

WAGNER AND ROBlNElTE
conditions, the average time to first detection of S. epidermidis was 23.8 hours. However, a total of 37 hours was required for the BacT/Alert 240 to detect the organism in all experiments that eventuallyresulted in positive cultures. Therefore, testing under this scenario would require a mininum of 61 hours (24 + 37 hrs). Alternatively, if sampling of the PC is performed at 48 hours, E. coli andS. epidermidis could be detected at a 100 percent frequency. Under these conditions, the average time to first detection of S. epidermidiswas 10.7 hours. Amaximum time of 17.3 hours would be required to detect the organism in all experi- ments, resulting in a minimum of 65 hours (48 + 17 hrs) for test completion. With either scenario, 3 days would be re- quired for test completion.
Another study suggests that an even longer time might be required for prospective te~t ing.~’ A recent pilot study of an automated culturing system reported that four of 16,290 PCs sampled on Day 1 were culture-positive. The same four were positive when sampled on Day 3, as well as an addi- tional three PCs that were culture-negative when sampled on Day 1. No information was given on the additional amount of time required for detection of the positive PCs sampled on Day 3. Nevertheless, effective microbiologic screening of blood by automated culture, where sampling would be performed sometime between Days 1 and 3, would result in less time available for platelets to be trans- fused. Although PCs are not usually available for transfu- sion until Days 1 or 2, a further delay in platelet distribu- tion might affect availability during times of scarce blood supply, or during 3- or 4-day holiday weekends.
Ultimately, the time for the completion of an auto- mated bacterial culture and the distribution of components would have to be in line with the adequate provision of platelets. The current 5-day storage period for platelets was reduced from 7 days because of concerns about increased sepsis from platelet components stored for extended peri- o d ~ . ~ ~ W h e t h e r the 5-day storage time of platelets could be extended again, in conjunction with bacterial testing, would depend on the reliability of the test and the clinical efficacy of transfusing an older component.
Another issue of concern is the frequency of false-posi- tive units that might be unnecessarily destroyed. While not addressed in this study, this issue has been evaluated in a pilot study by Blajchman and colleague^.^^ Roughly one- half of cultures that tested positive were 1) actual “false” positives, where bacteria that were originally present in the PC were eventually killed by phagocytosis or complement- mediated inactivation; 2) positive due to breeches in asep- tic technique or defective (cracked) culture vials; or 3) (to a lesser extent) positive due to instrument error. Thus, roughly one in 1000 PCs had cultures that tested falsely positive. This is similar to the frequency of the true positives measured in the study.
Finally, it is unclear whether automated blood cultur- ing, if adopted, should take place in hospitals or blood cen- ters. Many hospitals already utilize automated culturing systems in their microbiology departments and have trained personnel. However, platelet utilization, inventory control, and transfusion practice vary greatly among hos- pitals and might make standardization of testing difficult. Standardized testing might best be performed in a blood center or consolidated laboratory. However, the feasibility of using an automated blood culture for bacterial detection in PC(s) may ultimately depend more on whether there would be enough time after testing to routinely supply platelets for all patients than where testing might best be performed.
ACKNOWLEDGMENT
The authors gratefully acknowledge helpful comments by Alfred Katz, MD, regarding the presentation of experimental results and statistical analysis.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Goldman M, Blajchman MA. Blood product-associated bacterial sepsis. Transfus Med Rev 1991;5:73-83. Wagner SJ, Friedman LI, Dodd RY. Transfusion-associated bacterial sepsis. Clin Microbiol Rev 1994;7:290-302. Gong J, Hogman CF, Lundholm M, Gustafsson I. Novel au- tomated microbial screening of platelet concentrates.
Blajchman MA, Ali AM. Bacteria in the blood supply: an overlooked issue in transfusion medicine. In: Nance ST, ed. Blood safety: current challenges. Bethesda: American Asso- ciation of Blood Banks, 1992213-28. Burstain JM, Brecher ME, Workman K, et al. Rapid identifi- cation of bacterially contaminated platelets using reagent strips: glucose and pH analysis as markers of bacterial me- tabolism. Transfusion 1997;37:255-8. Wagner SJ, Robinette D. Evaluation of swirling, pH, and glucose tests for the detection of bacterial contamination in platelet concentrates. Transfusion 1996;36:989-93. Myhre BA, Demianew SH, Yoshimori RN, et al. pH changes caused by bacterial growth in contaminated platelet con- centrates. Ann Clin Lab Sci 1985:509-14. Brecher ME, Boothe G, Kerr A. The use of a chemilumines- cence-linked universal bacterial ribosomal RNA gene probe and blood gas analysis for the rapid detection of bacterial contamination in white cell-reduced and nonreduced platelets. Transfusion 1993;33:450-7. Kim DM, Brecher ME, Bland LA, et al. Prestorage removal of Yersiniu enterocoliticu from red cells with white cell-re- duction filters. Transfusion 1992;32:658-62. Yomtovian R, Lazarus HM, Goodnough LT, et al. A prospec- tive microbiologic surveillance program to detect and pre-
APMIS 1994;102:72-8.
678 TRANSFUSION Volume 38, July 1998
AUTOMATED MICROBIOLOGICAL CULTURE
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
vent the transfusion of bacterially contaminated platelets. Transfusion 1993;33:902-9. Morrow JF, Braine HG, Kickler TS, et al. Septic reactions to platelet transfusions. A persistent problem. JAMA
Reik H, Rubin SJ. Evaluation of the buffy-coat smear for rapid detection of bacteremia. JAMA 1981;245:357-9. Anderson KC, Lew MA, Gorgone BC, et al. Transfusion-re- lated sepsis after prolonged platelet storage. Am J Med
Barrett BB, Anderson JW, Anderson KC. Strategies for the avoidance of bacterial contamination of blood compo- nents. Transfusion 1993;33:228-34. Chiu EKW, Yuen KY, Lie AKW, et al. A prospective study of symptomatic bacteremia following platelet transfusion and of its management. Transfusion 1994;34:950-4. McCarthy LR, Senne JE. Evaluation of acridine orange stain for detection of microorganisms in blood cultures. J Clin Microbiol 1980;11:281-5. Chongokolwatana V, Morgan M, Feagin JC, et al. Compari- son of microscopy and a bacterial DNA probe for detecting bacterially contaminated platelets (abstract). Transfusion
Feng P, Keasler SP, Hill WE. Direct identification of Yersinia enterocolitica in blood by polymerase chain reaction ampli- fication. Transfusion 1992;32:850-4. Krishnan LA, Brecher ME. Transfusion-transmitted bacte- rial infection. Hematol Oncol Clin North Am 1995;9:167-85. Halpin TJ, Kilker S, Epstein J, Tourault M. Bacterial con- tamination of platelet pools-Ohio, 1991. MMWR Morb Mortal Wkly Rep 1992;41:36-7. Bufill JA, Ritch PS. Yersinia enterocolitica serotype 0:3 sepsis after blood transfusion (letter). N Engl J Med 1989;320:810. McAllister SK, Bland LA, Arduino MJ, et al. Patient cytokine response in transfusion-associated sepsis. Infect Immun
Muder RR, Yee YC, Rihs JD, Bunker M. Staphylococcus epidermidis bacteremia from transfusion of contaminated platelets: application of bacterial DNA analysis. Transfu- sion 1992;32:771-4.
199 1 ;266:555-8.
1986;81:405-11.
1993;33 (Suppl) :50s.
1994;62:2126-8.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Hall MM, Ilstrup DM, Washington JA. Effect of volume of blood cultured on detection of bacteremia. J Clin Microbiol
Sanz C, Pereira A, Vila J, et al. Growth of bacteria in platelet concentrates obtained from whole blood stored for 16 hours at 22°C before component preparation. Transfusion
Hogman CF, Gong J, Eriksson L, et al. White cells protect donor blood against bacterial contamination. Transfusion
Sherburne B, McCullough A, Dzik WH, DeGirolami P. Bac- terial proliferation in platelet concentrates is unaffected by pre-storage leukocyte depletion (abstract). Blood 1991;78 (Suppl):350a. Wenz B, Ciavarella D, Freundlich L. Effect of prestorage white cell reduction on bacterial growth in platelet concen- trates. Transfusion 1993;33:520-3. Buchholz DH, AuBuchon JP, Snyder EL, et al. Effects of white cell reduction on the resistance of blood components to bacterial multiplication. Transfusion 1994;34:852-7. Wagner SJ, Moroff G, Katz AJ, Friedman LI. Comparison of bacteria growth in single and pooled platelet concentrates after deliberate inoculation and storage. Transfusion
Blajchman MA, Lyn P, Rosenberg E, et al. Bacterial surveil- lance of platelet concentrates: a comparison of day 1 versus day 3 bacterial cultures (abstract). Blood 1996;88(Suppl 1):286a. Septic reactions after platelet transfusions. Department of Health and Human Services and Food and Drug Adminis- tration. In: Blood products, 16th meeting, vol 1: Tran- scripts. Washington: Baker, Hames and Burkes Reporting,
Blajchman MA, Ali AM, Richardson HL. Bacterial contami- nation of cellular blood components. Vox Sang
1976;3:643-5.
1997;37:251-4.
1991 ;3 1 :620-6.
1995;35:298-302.
1986: 151 -241.
1994;67(S~ppl3):25-33.
AUTHORS
Stephen J. Wagner, PhD, Senior Scientist, Holland Laboratory for the Biomedical Sciences, Rockville, MD. [Reprint requests]
Department, Holland Laboratory for the Biomedical Sciences. Daniel Robinette, BS, Technologist, Product Development
Volume 38, July 1998 TRANSFUSION 679
















![3.Controlul Microbiologic Al Alimentelor[1]](https://img.pdfslide.net/doc/110x75/55cf9cfe550346d033abd0c6/3controlul-microbiologic-al-alimentelor1.jpg)