Embed Size (px)
Citation preview

IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 8 Ver. VI (Aug. 2015), PP 105-122 www.iosrjournals.org
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 105 | Page
Evaluation of Gallbladder Content Spillage in Laparoscopic
Cholecystectomy
Dr. Keval Sansiya1, Dr. Hardik Dodia
2, Dr. Dimple Patel
3, Dr. Neel Patel
4
1(General Surgery department, B.J. Medical College/ Gujarat University,India) 21(General Surgery department, B.J. Medical College/ Gujarat University,India) 1(General Surgery department, B.J. Medical College/ Gujarat University,India) 1(General Surgery department, B.J. Medical College/ Gujarat University,India)
Abstract:With increasing number of laparoscopic cholecystectomy performed worldwide, there has been
increasing cases of complications related to it. One of which is gallbladder content spillage and its
complications. Here I present study of 25 such cases randomly selected during my period of surgical residency
from july 2012 to november 2014, I have tried to evaluate factors affecting it, its age/sex incidence, incidence
according to gall bladder status, post operative complications in form of Surgical site infection, Peritonitis,
Increased hospital stay, etc
Keywords:Bile spillage in laparoscopic cholecystectomy, Gall bladder perforation during laparoscopic cholecystectomy, post operative complication in bile spillage, Factors causing bile spillage in laparoscopic
cholecystectomy
I. Introduction Gallstones are present in about 10% to 15% of the adult population & 3-6 % of adult Indian
population19. Between 1% and 4% become symptomatic in a year requiring cholecystectomy, making
cholecystectomy one of the most common operations performed by general surgeons. Before 20 years open
cholecystectomy was operation of choice for cholecystitis. It is since last 20 years that laparoscopic
cholecystectomy is established as gold standard surgery for the cholelithiasis. laparoscopic cholecystectomy has
clear cut advantages over open cholecystectomy so much so as to establish laparoscopic approach as the
treatment of choice. However, with the increase in the number of laparoscopic operations performed, there has
also been a noticeable increase in the number of complications specific to these procedures. Gallstones can be spilled during an open cholecystectomy, but these stones are eliminated usually through direct removal, copious
irrigation and mopping with laparotomy sponges. In laparoscopic procedures, these techniques are more difficult
or unavailable and so stones can disappear from view and can become "lost". Studies show that the incidence of
spilled gallstones during laparoscopic cholecystectomy accounts for 6 to 40% of procedures performed, while
incidence of stone loss is unknown5. Complications from stones that are left within the peritoneal cavity can
cause unusual but significant morbidity. So I want to evaluate the cases in which gallbladder perforation and
spillage occurred in laparoscopic cholecystectomy to evaluate the postoperative outcome and the risk factors for
spillage as well.
Index
1) Table of contents 2) Aims and objectives of study
3) Materials and methods / Data Collection
4) Review of literature
5) Observation and Discussion
6) Summary
7) Conclusion
8) References
Acknowledgements 2) Aims of Study
1. To study and evaluate the predisposing risk factors for gallbladder spillage during laparoscopic
cholecystectomy.
2. To study and evaluate all possible postoperative outcomes that occur during laparoscopic cholecystectomy
with gallbladder perforation and spillage.
3. To study and evaluate the predisposing risk factors for developing complications in a patient with
gallbladder spillage during laparoscopic cholecystectomy.
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 106 | Page
II. Material And Method Hospital Setting
The study was conducted at the surgical unit of civil hospital, Ahmedabad, a publicly funded tertiary care institution, which serves as the major referral centre for other public and private hospitals within Gujarat
state and surrounding states particularly Rajasthan and Madhya Pradesh. Hospital has also 24 hours emergency
care service with ICU care.
Data collection
A total of 25 patients, with a diagnosis of chronic calculus cholecystitisthat underwent laparoscopic
cholecystectomy with intra operative Gallbladder spillage from July 2012 to December 2014, were collected.
Patients were interviewed according to the proforma. Data was obtained from surgical records to complete
proforma and summarize events. Data collected included clinical features, past history, laboratory
investigations, imaging, intraoperative or postoperative complications and duration of hospital stay.
Inclusion criteria
Patients with cholelithiasis proven by ultrasonography with atleast one attack of upper abdominal pain and
considered fit for cholecystectomy were included in the study.
Exclusion criteria
The patients having history or investigation suggestive of common bile duct stone were excluded from the
study.
Patient with acute cholecytitis were excluded.
Review of Literature HISTORY:(3)
1420: The first account of gallstones was given by a Florentine pathologist Antonio Benevieni, in an
autopsy of a woman who died with abdominal pain.
1687: Stal Pert Von Der Wiel, while operating a patient with purulent peritonitis accidentally found
gallstones.
1733: Jean-Louis Petit, the founder of gall bladder surgery suggested removal of gallstone and drainage of
the gall bladder, thus creating fistula in patients with empyema, which he successfully performed in 1743.
1859: J.L.W Thudichum proposed a two-stage elective cholecystostomy. In the first stage, the inflamed gall
bladder was sewed to the anterior abdominal wall through a small incision, which served as a route for the
removal of gall stone at a later date.
1867: Dr John StoughBobbs from Indianopolis, Indiana while operating on a patient with suspected ovarian
cyst found an inflamed and adhered sac containing “several solid ordinary rifle bullet” like structures. He opened the sac, which incidentally happened to be the gall bladder packed with multiple gallstones. He
removed the gallstones and left the gall bladder in the abdomen after closing the defect in the gall bladder
(cholecystostomy).
1878: Marion Simms performed first cholecystostomy on a 45-year-old woman with obstructive jaundice.
Though the patient died on the eighth postoperative day due to massive internal haemorrhage, it paved the
way for Theodor Kocher to perform the first successful cholecystostomy in June 1878.
1882: Carl Johann August Langenbuch who observed that these measures were only temporary and rallied
to find a definite solution for the disease. He developed the technique of cholecystectomy through cadeveric
dissection and he successfully removed the gall bladder of a 43-year-old man who was suffering from the
disease for 16 years. Langenbuch found two gallstones and a chronically inflamed and thickened gall
bladder. The patient was discharged uneventfully from the hospital after six weeks.
By the turn of the century it was established that cholecystectomy could guarantee permanent relief from
pain whereas cholecystostomy gave a permanent fistula and not a pain-free state.
1987: Mouret from France performed the first human laparoscopic cholecystectomy. On that day as he was
completing a gynaecologic laparoscopy on a woman also suffering from symptomatic gallstones, he shifted
his laparoscope to the subhepatic area. Upon finding a comparatively free and supple gall bladder he
decided to remove it laparoscopically instead of opening up. He performed the procedure successfully and
the patient recovered without complications.
1992: Within two years, in the USA, the procedure was being adopted and because of the massive demand
from the patients, standard traditional stages of scientific evaluation were bypassed. Finally, in September
1992 a NIH consensus conference held in Bethesda concluded that laparoscopic cholecystectomy was the
treatment of choice for cholelithiasis.
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 107 | Page
Actually Prof Dr Med Erich Mühe of Böblingen, Germany, performed the first laparoscopic
cholecystectomy on September 12, 1985. The German Surgical Society rejected Mühe in 1986 after he
reported that he had performed the first laparoscopic cholecystectomy, yet in 1992 he received their highest
award, the German Surgical Society Anniversary Award.
Perissat, Berci, Cuschieri, Dubois, and Mouret were recognized by SAGES for performing early laparoscopic cholecystectomies, but Mühe was not. However, in 1999 he was recognized by SAGES for
having performed the first laparoscopic cholecystectomy–SAGES invited Mühe to present the Storz
Lecture.
In Mühe’s presentation, titled “The First Laparoscopic Cholecystectomy,” which he gave in March1999 in
San Antonio, Texas, he described the first procedure.
Finally, Mühe had received the worldwide acclaim that he deserved for his pioneering work.
Complications of laparoscopic cholecystectomy(6)
Haemorrhage
Bile duct injury
Bile leak
Gallstone spillage
Pancreatitis
Wound infection
Incisional hernia
Pneumoperitoneum related: CO2 embolism, vasovagal reflex, hypercarbic acidosis, cardiac arrhythmias
Trocar related: abdominal wall bleeding, hematoma, visceral injury, vascular injury
Wound infection and/or abscess
Deep vein thrombosis
Conversion to open procedure
Laparoscopic cholecystectomy has its own new complications other than of open cholecystectomy.
These are mainly trocar related complications and spillage from gallbladder perforation. Spillage of bile and
stone leads to some short term and long term complications but in a very low rate.
Studies on Gallbladder Spillage
A number of animal studies have been undertaken to determine the potential consequences of spilled
gallstones in the abdominal cavity. Welch et al.20 investigated the effects of unretrieved gallstones in a rabbit
model. These researchers placed unwashed human gallstones (cholesterol, pigmented and mixed) retrieved from
Laparoscopic cholecystectomy in the peritoneal cavity of rabbits within 6 hours of collection. Wound infection
did not develop in any of the animals, and at autopsy no intra-abdominal sepsis or marked adhesions were
discovered.
Furthermore, a 25% decrease in the size of pigmented stones was noticed after 2 months, raising the possibility of spontaneous absorption by the peritoneum. Welch et al.20 concluded that free intraperitoneal
gallstones are harmless and thus do not warrant exploratory laparotomy.
However, a larger animal study by Johnston et al.21 using rats found that leakage of bile in combination
with gallstones was associated with a significant risk of postoperative adhesion formation and possible
intraabdominal abscesses in contradiction to the aforementioned study. These authors, however, did not endorse
the policy of routine laparotomy, except when a large number of stones were unretrievable during Laparoscopic
cholecystectomy.
Leland and Dawson22 conducted an experimental study using Sprague Dawley rats as a model to
determine the incidence of intra-abdominal adhesions 88 days after sterile artificial cholesterol stones were
placed in the peritoneal cavity. They noted formations ranging from thin and flimsy membranes to thick and
well-developed stalks in 27% of their animals. However, they did not observe any major complication or absorption of these stones. These authors suggested that intraperitoneal stones could lead to an even higher
incidence of adhesion formation in association with contaminated bile. They observed, furthermore, that other
minerals present in the naturally occurring human gallstones could result in a much stronger inflammatory
response in humans. Leland and Dawson therefore concluded that unretrieved gallstones are not benign and
should be aggressively removed to decrease long-term complications.
Cline et al.23, using Sprague-Dawley rats, reported the effects of various numbers of gallstones lost in the
peritoneal cavity. The authors placed no gallstones, one gallstone, and five gallstones in the peritoneal cavity of
these rats. They killed these animals after 2, 4, and 8 weeks and looked for adhesions, fistulae, perforations, or
obstructions. Except for a trend toward more stones becoming fixed within the abdomen over time, no other
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 108 | Page
complications were noted in any of these groups. These authors concluded that spilled gallstones do not increase
morbidity after Laparoscopic cholecystectomy.
One of the definitive studies from the Mayo clinic24 addressed the long-term consequences of
intraoperative spillage of bile and gallstones during Laparoscopic cholecystectomy. This study analyzed
prospectively data from 1,059 consecutive Laparoscopic cholecystectomies performed over a 3-year period. The iatrogenic gallbladder perforation was 29%. The factors associated with higher incidence of gallbladder
perforation included male gender, increasing age, body weight, and the presence of omental adhesions.
The Mayo study demonstrated that spillage of gallbladder content is associated with statistically
significant incidences of intra-abdominal abscesses compared with intact Laparoscopic cholecystectomy.
However, the overall risk of serious complications is very low. The authors emphasized the need for removal of
as many calculi as possible laparoscopically. However, they advised conversion to an open procedure in patients
for whom it is not possible to retrieve the majority of the gallstones laparoscopically, especially when
bacteriobilia is suspected or confirmed by Gram stain of the bile. They noticed that percutaneous drainage of
intra-abdominal abscesses in most of their patients was ineffective if the inciting gallstones were not removed.
In retrospective study from Switzerland25, which analyzed 10,174 Laparoscopic cholecystectomies
performed at 82 surgical institutions over a 3-year period, the incidence of iatrogenic gallbladder perforation
was only 6%, and serious postoperative complications occurred very rarely (0.08%). This study concluded that elderly patients who have acute cholecystitis with infected bile and spilled stones may experience an increased
risk of intra-abdominal abscess formation. Therefore, perforation of the gallbladder should be prevented
whenever possible. They also emphasized the need to retrieve spilled gallstones and irrigate the abdominal
cavity to dilute the infected bile and spilled stones. They reiterated the message of previous studies that the
laparoscopic procedure should not be converted to an open one just for the retrieval of stones because the
incidence and the mortality rate of serious complications are extremely low.
Risk of Gallbladder Perforation
Certain situations lead to higher risk of gallbladder perforation during laparoscopic cholecystectomy.
Patients with acutely inflamed gallbladders have friable tissue which is susceptible to tear. Dense adhesions
around the gallbladder make dissection potentially more difficult, and a tense, distended gallbladder that has not been decompressed is at risk of perforation8. This usually occurs when the gallbladder is manipulated by
laparoscopic instruments or when it is dissected from the liver bed or during gallbladder extraction. Spilled
stones are also caused by the slipping of the cystic duct clip or the tearing of the gallbladder while it is retrieved
from the port site9.
There is also a well recognised learning curve for performing laparoscopic cholecystectomies, and the
risk of perforation is high early in a surgeon's laparoscopic career8.
Risk of Complications from Spillage
Although lost gallstones were initially considered innocuous, it is now recognised that they can be a
small but significant source of postoperative morbidity (0.1 to 6%)11. The presentation of complications will
vary from patient to patient. Recognised symptoms include abdominal pain, fever, abdominal masses, bowel
obstruction and the presence of a sinus infection or fistula9, 10. In most instances, the diagnosis is made retrospectively, or after visualisation of the stones on imaging and revisiting the patient's surgical history.
Most complications occur within the first few months, but presentations up to ten years after the
procedure have also been documented13. Zehetner et al.10 looked into all documented complications from lost
gallstones and these ranged from the most common like intra-abdominal and subcutaneous abscesses and
fistulas, to the less common, such as liver abscess, staphylococcus bacteraemia, broncholithiasis and
expectoration, empyema, granulomas, bowel obstruction and incarceration within a hernial sac.
Studies also show risk factors for complications after spilled stones, such as the presence of infected
bile, spillage of pigmented gallstones, multiple stones (>15), stone size (>1.5 cm) and old age10.
Complications from Gallbladder Spillage (27)
1. Intraabdominal abscesses Subphrenic abscess
Subhepatic abscess
Retroperitoneal abscess
Pouch of douglas abscess
Cutaneous Complications
Port site wound infection
Port site sinus tract formation
Cutaneous fistula
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 109 | Page
Anterior abdominal wall abscess
Gastrointestinal
Acute pancreatitis
Small bowel obstruction Sigmoid colon erosion
Partial necrosis and perforation of small bowel
Respiratory
Pleural effusion
Empyema
Pleurolithiasis
Hemoptysis
Cholelithoptysis
Miscellaneous
Incarceration within hernia sac Cholelithiasis of ovary
Peritoneal granuloma
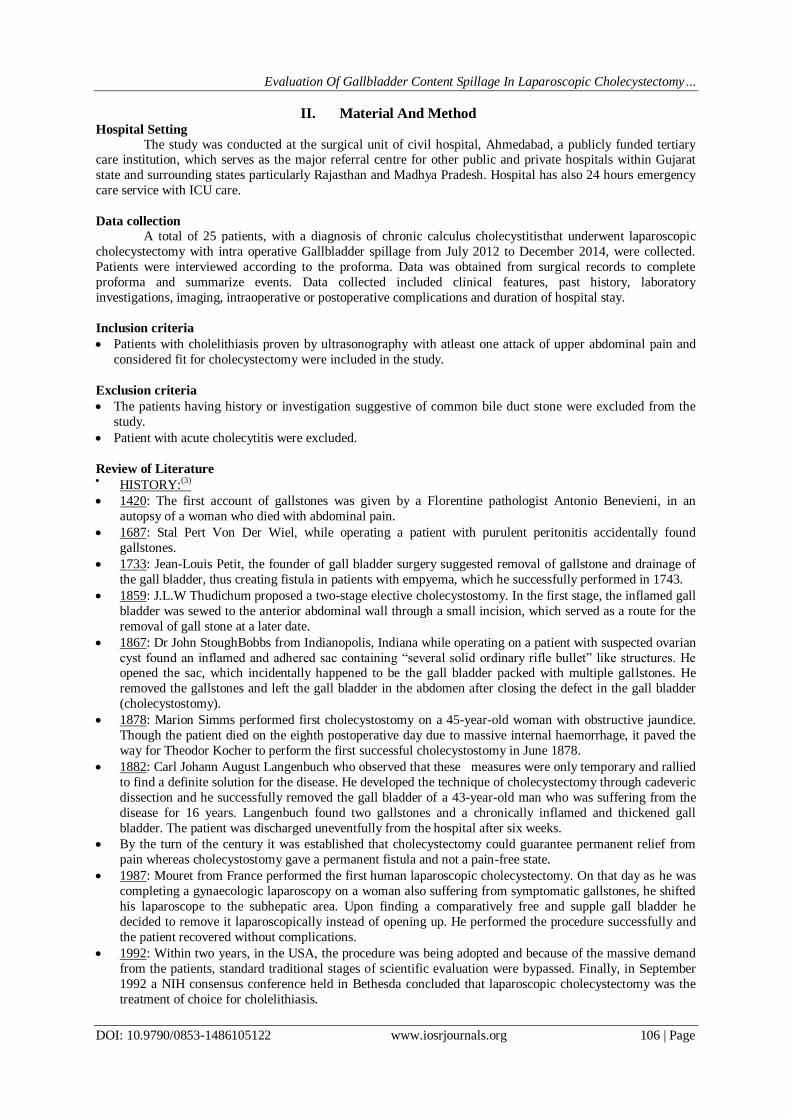
Fig.1 Single Gall bladder perforation during callots triangle dissection.
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 110 | Page
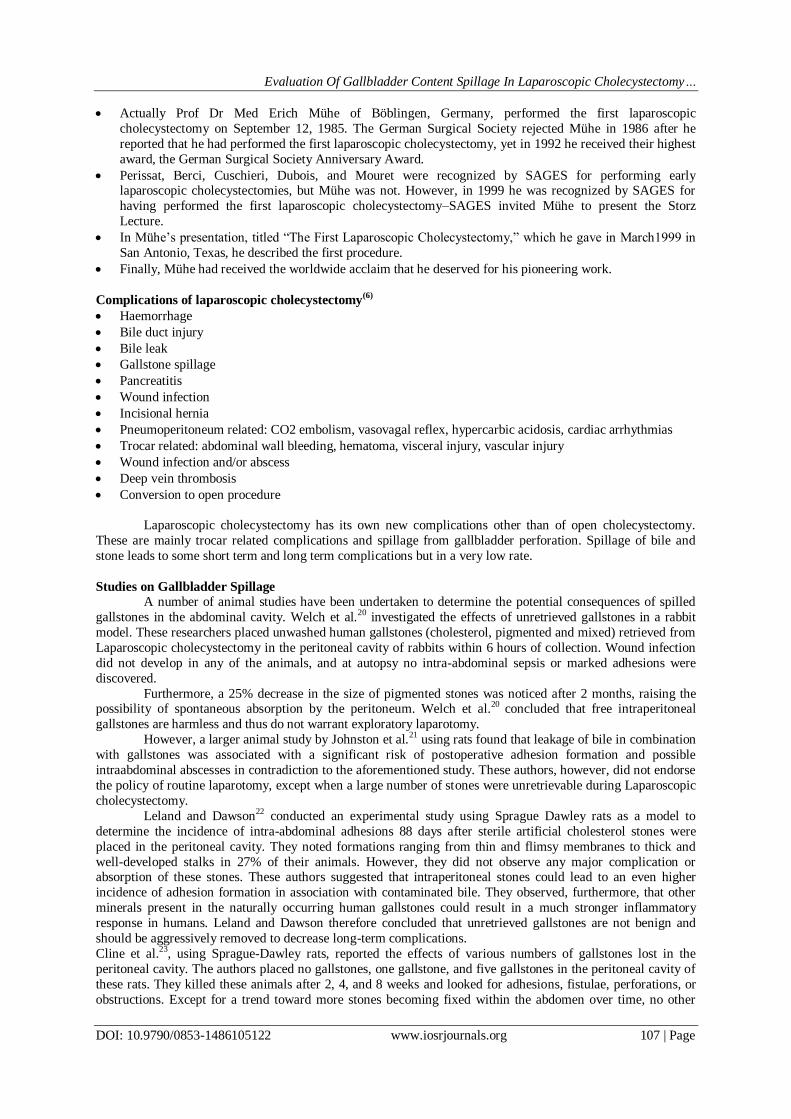
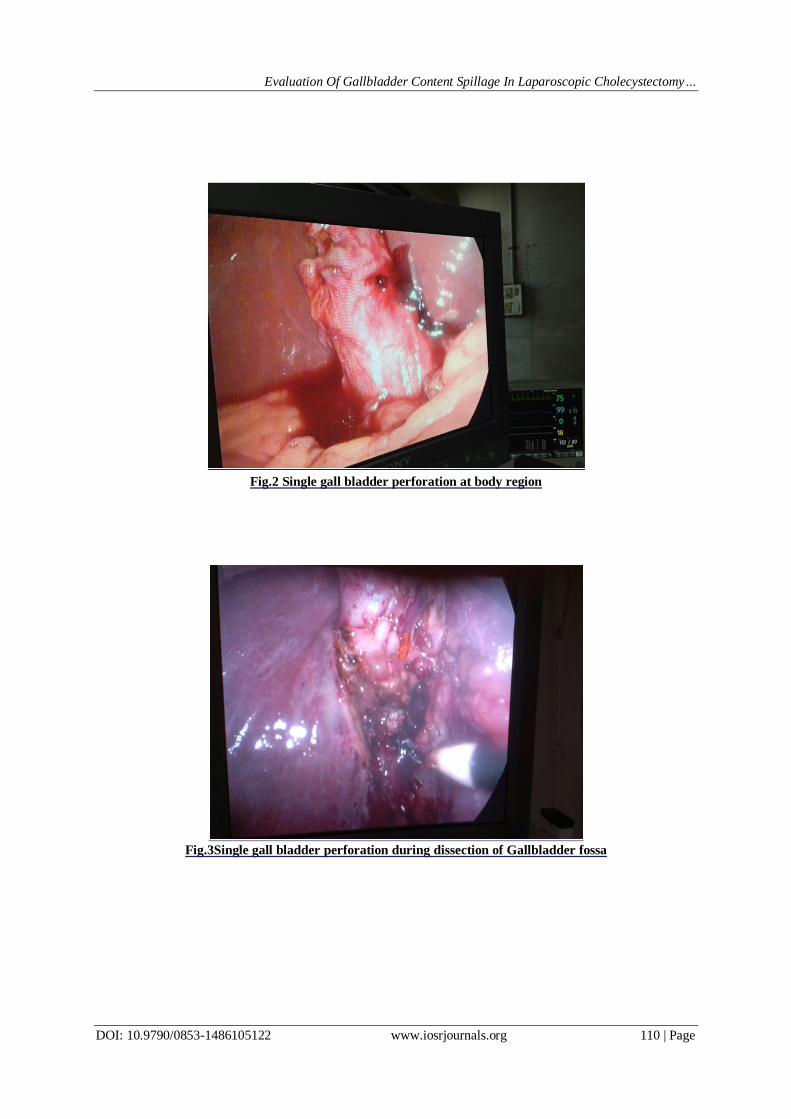
Fig.2 Single gall bladder perforation at body region
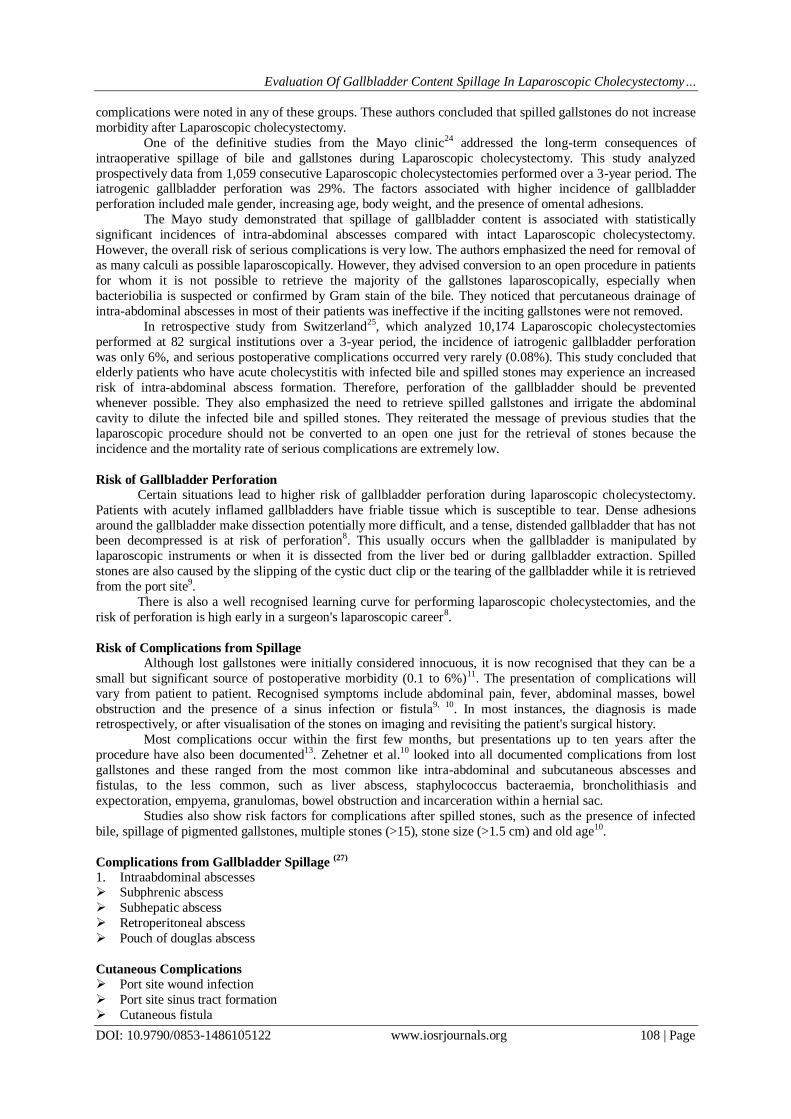
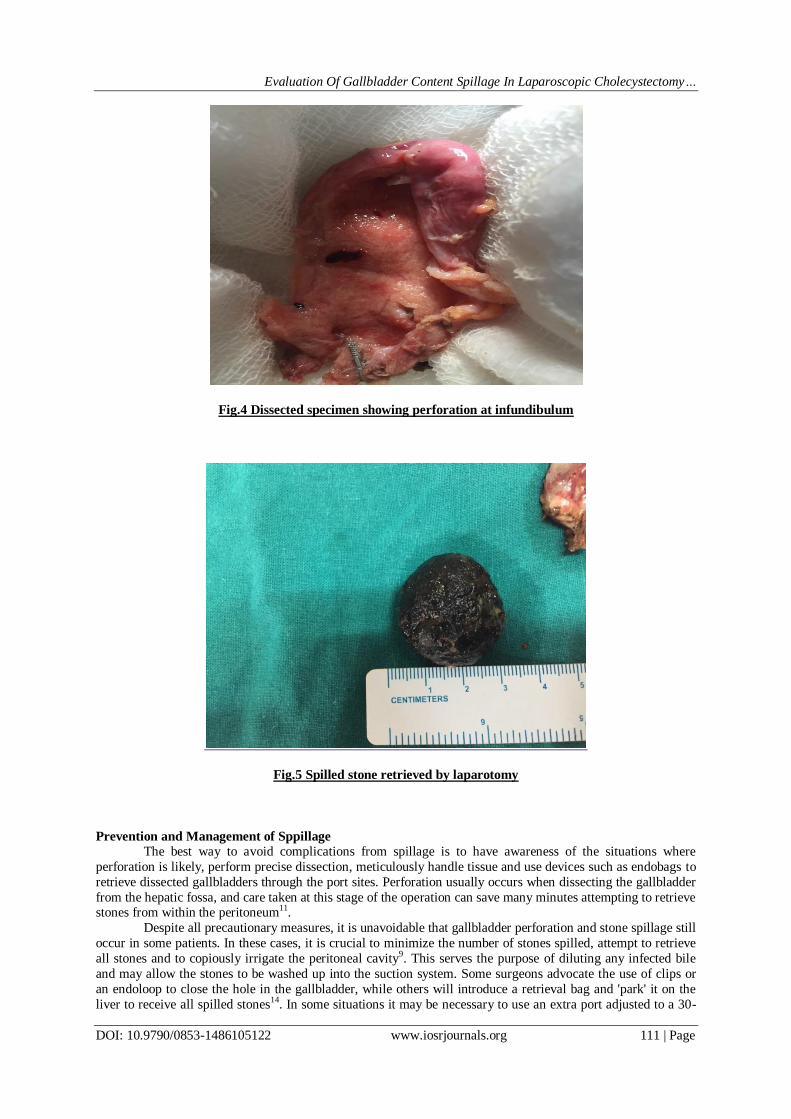
Fig.3Single gall bladder perforation during dissection of Gallbladder fossa
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 111 | Page
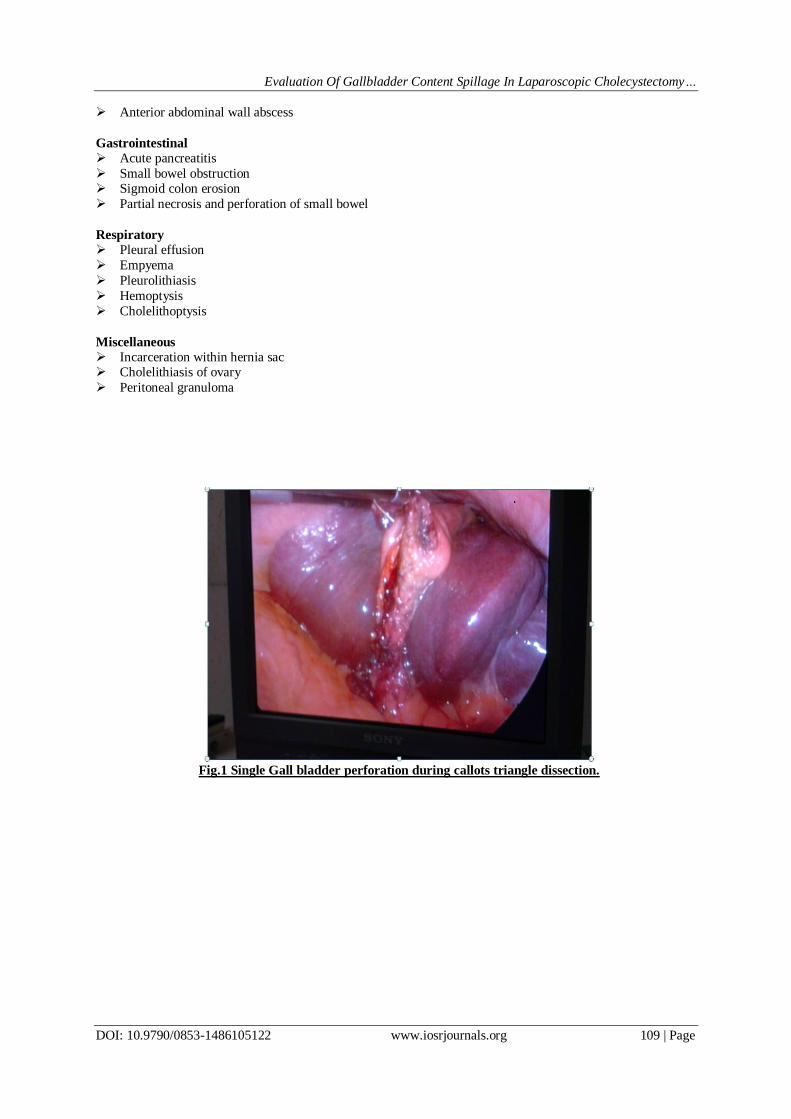
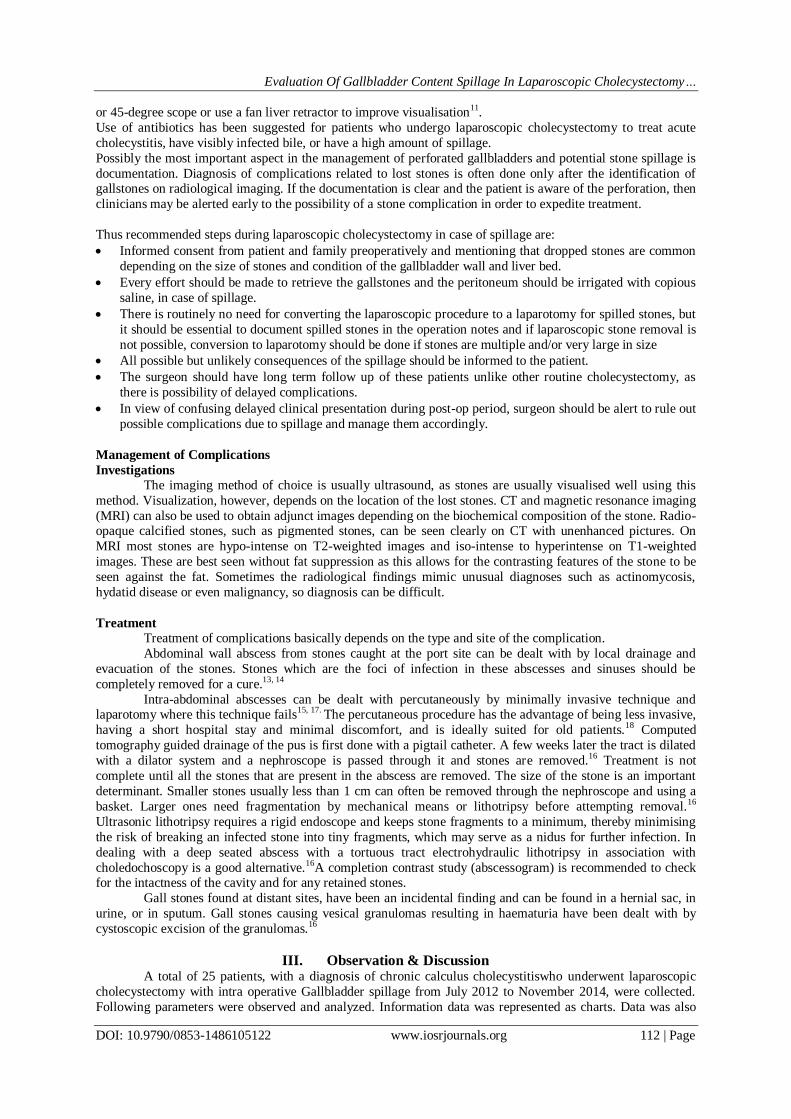
Fig.4 Dissected specimen showing perforation at infundibulum
Fig.5 Spilled stone retrieved by laparotomy
Prevention and Management of Sppillage
The best way to avoid complications from spillage is to have awareness of the situations where
perforation is likely, perform precise dissection, meticulously handle tissue and use devices such as endobags to
retrieve dissected gallbladders through the port sites. Perforation usually occurs when dissecting the gallbladder
from the hepatic fossa, and care taken at this stage of the operation can save many minutes attempting to retrieve stones from within the peritoneum11.
Despite all precautionary measures, it is unavoidable that gallbladder perforation and stone spillage still
occur in some patients. In these cases, it is crucial to minimize the number of stones spilled, attempt to retrieve
all stones and to copiously irrigate the peritoneal cavity9. This serves the purpose of diluting any infected bile
and may allow the stones to be washed up into the suction system. Some surgeons advocate the use of clips or
an endoloop to close the hole in the gallbladder, while others will introduce a retrieval bag and 'park' it on the
liver to receive all spilled stones14. In some situations it may be necessary to use an extra port adjusted to a 30-
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 112 | Page
or 45-degree scope or use a fan liver retractor to improve visualisation11.
Use of antibiotics has been suggested for patients who undergo laparoscopic cholecystectomy to treat acute
cholecystitis, have visibly infected bile, or have a high amount of spillage.
Possibly the most important aspect in the management of perforated gallbladders and potential stone spillage is
documentation. Diagnosis of complications related to lost stones is often done only after the identification of gallstones on radiological imaging. If the documentation is clear and the patient is aware of the perforation, then
clinicians may be alerted early to the possibility of a stone complication in order to expedite treatment.
Thus recommended steps during laparoscopic cholecystectomy in case of spillage are:
Informed consent from patient and family preoperatively and mentioning that dropped stones are common
depending on the size of stones and condition of the gallbladder wall and liver bed.
Every effort should be made to retrieve the gallstones and the peritoneum should be irrigated with copious
saline, in case of spillage.
There is routinely no need for converting the laparoscopic procedure to a laparotomy for spilled stones, but
it should be essential to document spilled stones in the operation notes and if laparoscopic stone removal is
not possible, conversion to laparotomy should be done if stones are multiple and/or very large in size
All possible but unlikely consequences of the spillage should be informed to the patient.
The surgeon should have long term follow up of these patients unlike other routine cholecystectomy, as
there is possibility of delayed complications.
In view of confusing delayed clinical presentation during post-op period, surgeon should be alert to rule out
possible complications due to spillage and manage them accordingly.
Management of Complications
Investigations
The imaging method of choice is usually ultrasound, as stones are usually visualised well using this
method. Visualization, however, depends on the location of the lost stones. CT and magnetic resonance imaging
(MRI) can also be used to obtain adjunct images depending on the biochemical composition of the stone. Radio-opaque calcified stones, such as pigmented stones, can be seen clearly on CT with unenhanced pictures. On
MRI most stones are hypo-intense on T2-weighted images and iso-intense to hyperintense on T1-weighted
images. These are best seen without fat suppression as this allows for the contrasting features of the stone to be
seen against the fat. Sometimes the radiological findings mimic unusual diagnoses such as actinomycosis,
hydatid disease or even malignancy, so diagnosis can be difficult.
Treatment
Treatment of complications basically depends on the type and site of the complication.
Abdominal wall abscess from stones caught at the port site can be dealt with by local drainage and
evacuation of the stones. Stones which are the foci of infection in these abscesses and sinuses should be
completely removed for a cure.13, 14
Intra-abdominal abscesses can be dealt with percutaneously by minimally invasive technique and laparotomy where this technique fails
15, 17. The percutaneous procedure has the advantage of being less invasive,
having a short hospital stay and minimal discomfort, and is ideally suited for old patients.18 Computed
tomography guided drainage of the pus is first done with a pigtail catheter. A few weeks later the tract is dilated
with a dilator system and a nephroscope is passed through it and stones are removed.16 Treatment is not
complete until all the stones that are present in the abscess are removed. The size of the stone is an important
determinant. Smaller stones usually less than 1 cm can often be removed through the nephroscope and using a
basket. Larger ones need fragmentation by mechanical means or lithotripsy before attempting removal.16
Ultrasonic lithotripsy requires a rigid endoscope and keeps stone fragments to a minimum, thereby minimising
the risk of breaking an infected stone into tiny fragments, which may serve as a nidus for further infection. In
dealing with a deep seated abscess with a tortuous tract electrohydraulic lithotripsy in association with
choledochoscopy is a good alternative.16A completion contrast study (abscessogram) is recommended to check for the intactness of the cavity and for any retained stones.
Gall stones found at distant sites, have been an incidental finding and can be found in a hernial sac, in
urine, or in sputum. Gall stones causing vesical granulomas resulting in haematuria have been dealt with by
cystoscopic excision of the granulomas.16
III. Observation & Discussion A total of 25 patients, with a diagnosis of chronic calculus cholecystitiswho underwent laparoscopic
cholecystectomy with intra operative Gallbladder spillage from July 2012 to November 2014, were collected.
Following parameters were observed and analyzed. Information data was represented as charts. Data was also
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 113 | Page
compared with similar studies in the past.
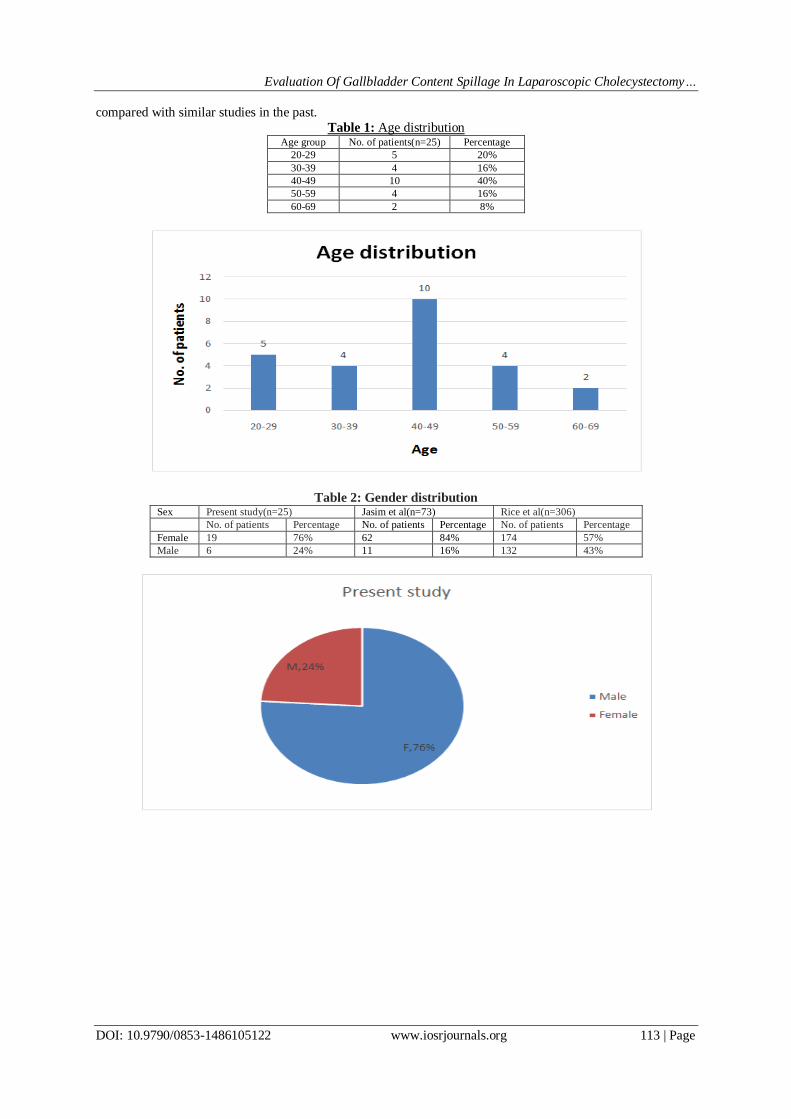
Table 1: Age distribution Age group No. of patients(n=25) Percentage
20-29 5 20%
30-39 4 16%
40-49 10 40%
50-59 4 16%
60-69 2 8%
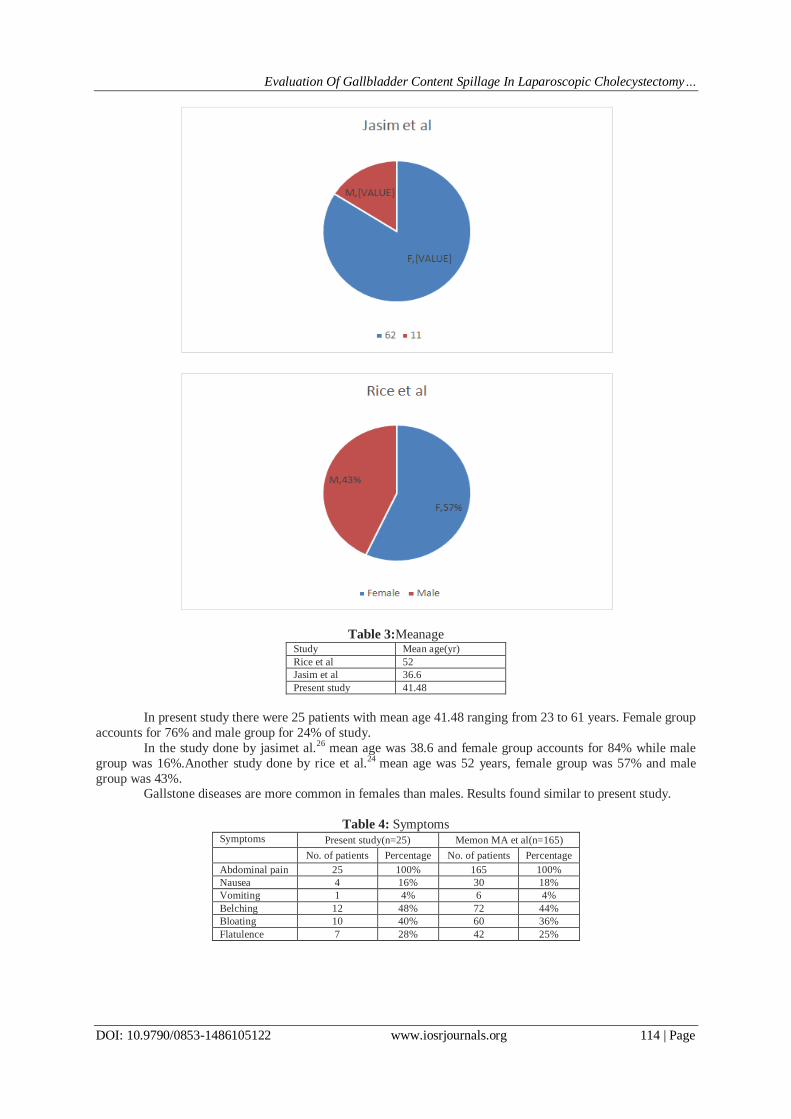
Table 2: Gender distribution Sex Present study(n=25) Jasim et al(n=73) Rice et al(n=306)
No. of patients Percentage No. of patients Percentage No. of patients Percentage
Female 19 76% 62 84% 174 57%
Male 6 24% 11 16% 132 43%
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 114 | Page
Table 3:Meanage Study Mean age(yr)
Rice et al 52
Jasim et al 36.6
Present study 41.48
In present study there were 25 patients with mean age 41.48 ranging from 23 to 61 years. Female group
accounts for 76% and male group for 24% of study.
In the study done by jasimet al.26 mean age was 38.6 and female group accounts for 84% while male
group was 16%.Another study done by rice et al.24 mean age was 52 years, female group was 57% and male
group was 43%. Gallstone diseases are more common in females than males. Results found similar to present study.
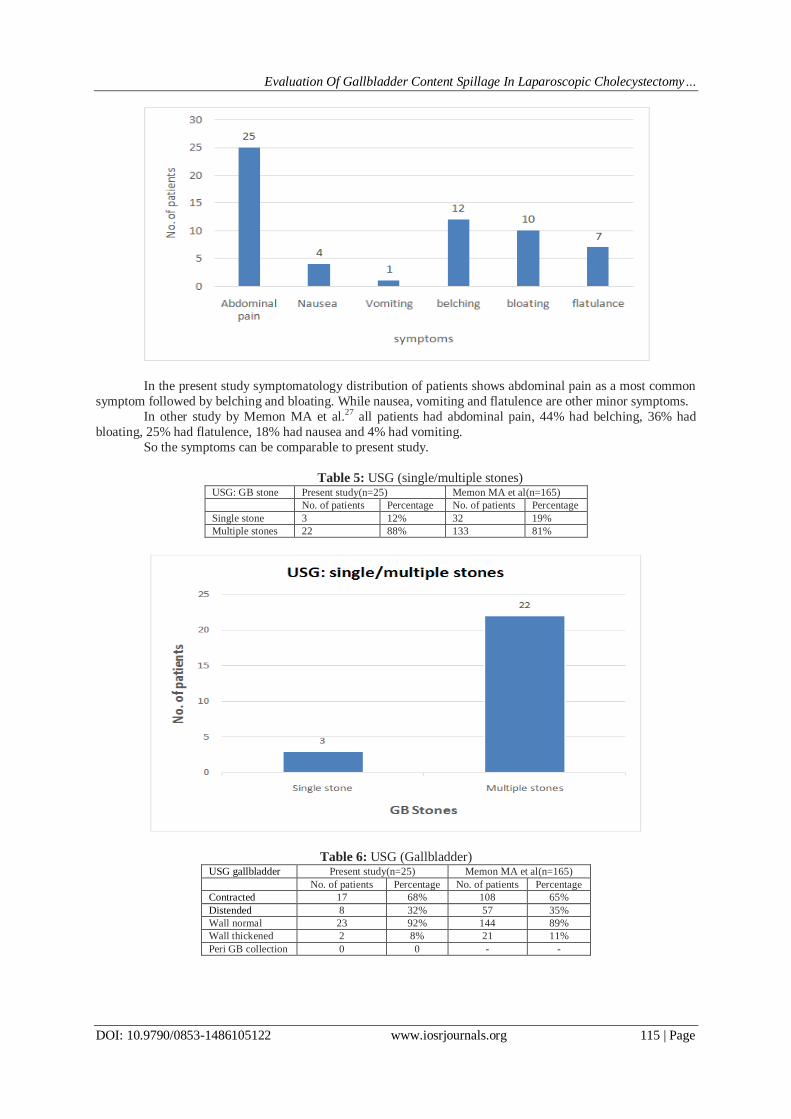
Table 4: Symptoms Symptoms Present study(n=25) Memon MA et al(n=165)
No. of patients Percentage No. of patients Percentage
Abdominal pain 25 100% 165 100%
Nausea 4 16% 30 18%
Vomiting 1 4% 6 4%
Belching 12 48% 72 44%
Bloating 10 40% 60 36%
Flatulence 7 28% 42 25%
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 115 | Page
In the present study symptomatology distribution of patients shows abdominal pain as a most common
symptom followed by belching and bloating. While nausea, vomiting and flatulence are other minor symptoms.
In other study by Memon MA et al.27 all patients had abdominal pain, 44% had belching, 36% had
bloating, 25% had flatulence, 18% had nausea and 4% had vomiting.
So the symptoms can be comparable to present study.
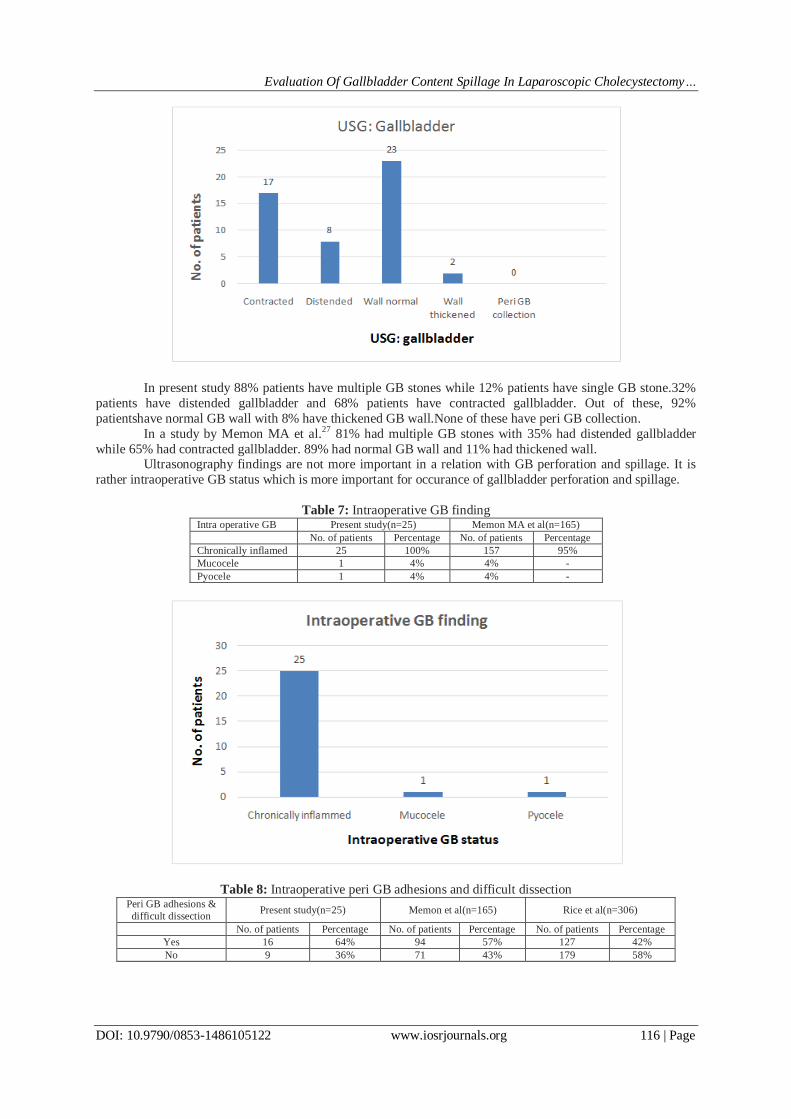
Table 5: USG (single/multiple stones) USG: GB stone Present study(n=25) Memon MA et al(n=165)
No. of patients Percentage No. of patients Percentage
Single stone 3 12% 32 19%
Multiple stones 22 88% 133 81%
Table 6: USG (Gallbladder) USG gallbladder Present study(n=25) Memon MA et al(n=165)
No. of patients Percentage No. of patients Percentage
Contracted 17 68% 108 65%
Distended 8 32% 57 35%
Wall normal 23 92% 144 89%
Wall thickened 2 8% 21 11%
Peri GB collection 0 0 - -
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 116 | Page
In present study 88% patients have multiple GB stones while 12% patients have single GB stone.32%
patients have distended gallbladder and 68% patients have contracted gallbladder. Out of these, 92%
patientshave normal GB wall with 8% have thickened GB wall.None of these have peri GB collection.
In a study by Memon MA et al.27 81% had multiple GB stones with 35% had distended gallbladder
while 65% had contracted gallbladder. 89% had normal GB wall and 11% had thickened wall. Ultrasonography findings are not more important in a relation with GB perforation and spillage. It is
rather intraoperative GB status which is more important for occurance of gallbladder perforation and spillage.
Table 7: Intraoperative GB finding Intra operative GB Present study(n=25) Memon MA et al(n=165)
No. of patients Percentage No. of patients Percentage
Chronically inflamed 25 100% 157 95%
Mucocele 1 4% 4% -
Pyocele 1 4% 4% -
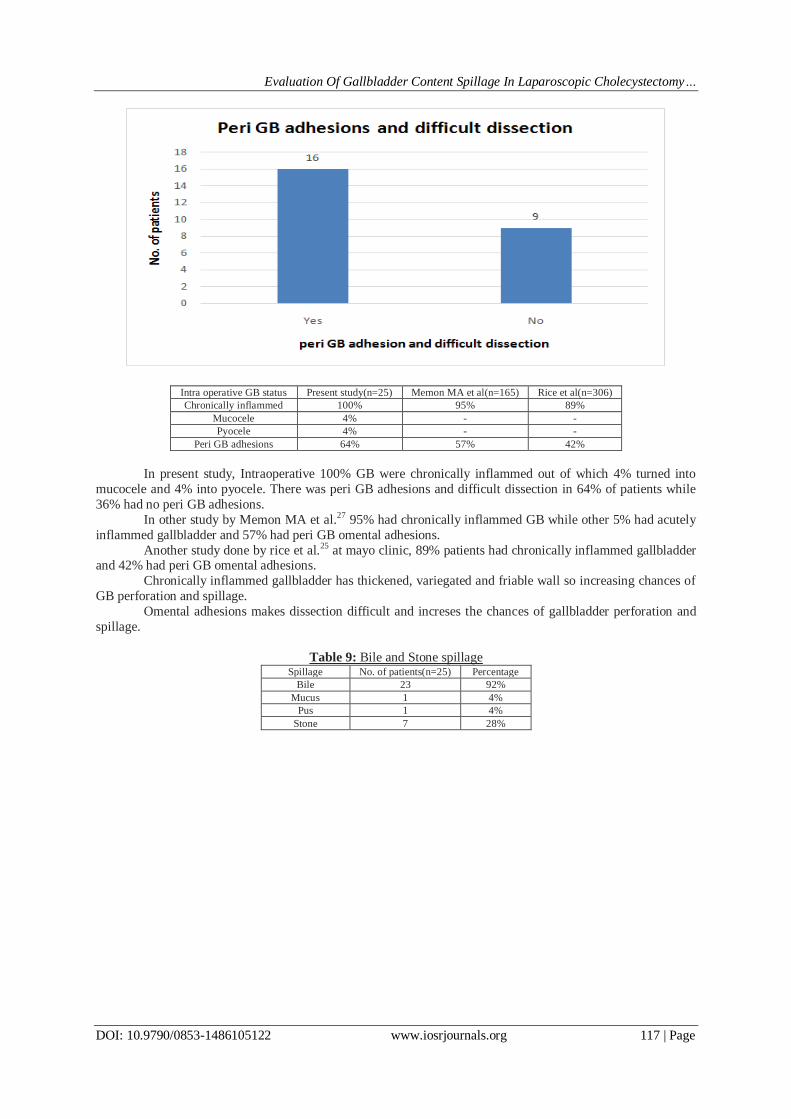
Table 8: Intraoperative peri GB adhesions and difficult dissection Peri GB adhesions &
difficult dissection Present study(n=25) Memon et al(n=165) Rice et al(n=306)
No. of patients Percentage No. of patients Percentage No. of patients Percentage
Yes 16 64% 94 57% 127 42%
No 9 36% 71 43% 179 58%
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 117 | Page
Intra operative GB status Present study(n=25) Memon MA et al(n=165) Rice et al(n=306)
Chronically inflammed 100% 95% 89%
Mucocele 4% - -
Pyocele 4% - -
Peri GB adhesions 64% 57% 42%
In present study, Intraoperative 100% GB were chronically inflammed out of which 4% turned into
mucocele and 4% into pyocele. There was peri GB adhesions and difficult dissection in 64% of patients while
36% had no peri GB adhesions.
In other study by Memon MA et al.27 95% had chronically inflammed GB while other 5% had acutely
inflammed gallbladder and 57% had peri GB omental adhesions.
Another study done by rice et al.25 at mayo clinic, 89% patients had chronically inflammed gallbladder and 42% had peri GB omental adhesions.
Chronically inflammed gallbladder has thickened, variegated and friable wall so increasing chances of
GB perforation and spillage.
Omental adhesions makes dissection difficult and increses the chances of gallbladder perforation and
spillage.
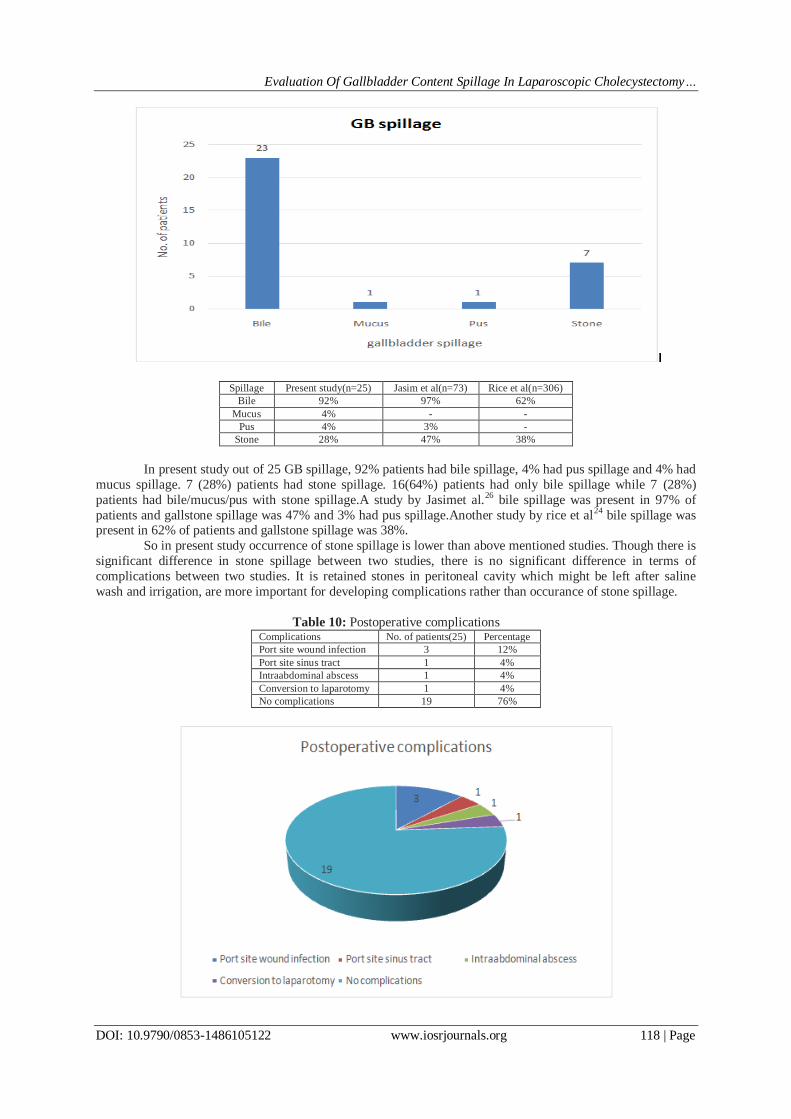
Table 9: Bile and Stone spillage Spillage No. of patients(n=25) Percentage
Bile 23 92%
Mucus 1 4%
Pus 1 4%
Stone 7 28%
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 118 | Page
Spillage Present study(n=25) Jasim et al(n=73) Rice et al(n=306)
Bile 92% 97% 62%
Mucus 4% - -
Pus 4% 3% -
Stone 28% 47% 38%
In present study out of 25 GB spillage, 92% patients had bile spillage, 4% had pus spillage and 4% had
mucus spillage. 7 (28%) patients had stone spillage. 16(64%) patients had only bile spillage while 7 (28%)
patients had bile/mucus/pus with stone spillage.A study by Jasimet al.26 bile spillage was present in 97% of
patients and gallstone spillage was 47% and 3% had pus spillage.Another study by rice et al24 bile spillage was present in 62% of patients and gallstone spillage was 38%.
So in present study occurrence of stone spillage is lower than above mentioned studies. Though there is
significant difference in stone spillage between two studies, there is no significant difference in terms of
complications between two studies. It is retained stones in peritoneal cavity which might be left after saline
wash and irrigation, are more important for developing complications rather than occurance of stone spillage.
Table 10: Postoperative complications Complications No. of patients(25) Percentage
Port site wound infection 3 12%
Port site sinus tract 1 4%
Intraabdominal abscess 1 4%
Conversion to laparotomy 1 4%
No complications 19 76%
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 119 | Page
Table 11: Comparison of complications
Table 12: Relation between gallbladder spillage and complications Complications developed No complications Total
Bile only 1 17 18
Bile/mucus/pus+stone 5 2 7
Total 6 9 25
In present study no complications occurred in 76% cases. 6 patients (24%) developed complications of
which 3 patients had port site wound infection, 1 had intraabdominal abscess, 1 had sinus tract formation and 1
was converted to open cholecystectomy 20% complicated cases had both stone and bile/pus spillage while 4% had only bile spillage.
In other study by Jasimet al26 complication rate was 23.53%. In that study, out of 34 patients 3
patients(8.8%) developed intaabdominal abscess,3 patients(8.8%) developed port site wound infection, 1
patient(2.94%) developed port site sinus tract formation and other 1 patient(2.94%) developed persistant
abdominal pain due to retained gallstone in peritoneal cavity.
So wound infection and intraabdominal abscess are common complications occurred after gallbladder
spillage.
The p value of table 11 is 0.000535 (p<0.05) which is significant. So chances of postoperative
complications are more in case of bile and stone spillage rather than only bile spillage.
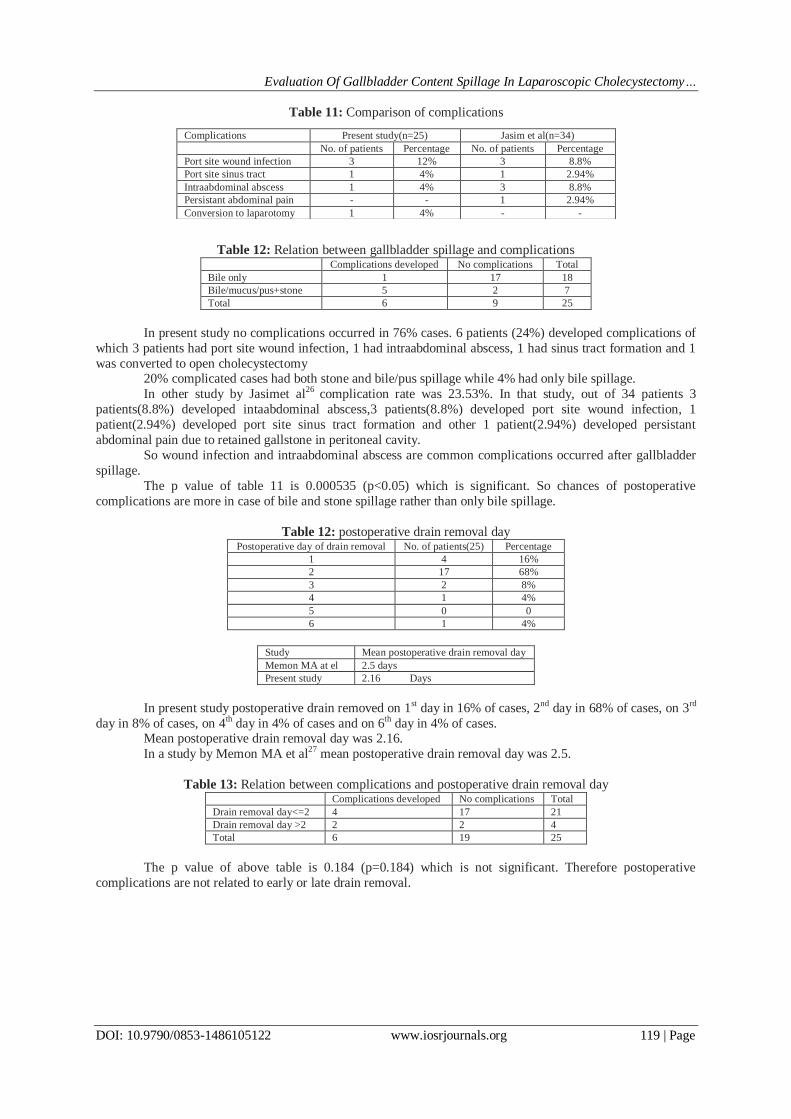
Table 12: postoperative drain removal day Postoperative day of drain removal No. of patients(25) Percentage
1 4 16%
2 17 68%
3 2 8%
4 1 4%
5 0 0
6 1 4%
Study Mean postoperative drain removal day
Memon MA at el 2.5 days
Present study 2.16 Days
In present study postoperative drain removed on 1st day in 16% of cases, 2nd day in 68% of cases, on 3rd
day in 8% of cases, on 4th day in 4% of cases and on 6th day in 4% of cases. Mean postoperative drain removal day was 2.16.
In a study by Memon MA et al27 mean postoperative drain removal day was 2.5.
Table 13: Relation between complications and postoperative drain removal day Complications developed No complications Total
Drain removal day<=2 4 17 21
Drain removal day >2 2 2 4
Total 6 19 25
The p value of above table is 0.184 (p=0.184) which is not significant. Therefore postoperative
complications are not related to early or late drain removal.
Complications Present study(n=25) Jasim et al(n=34)
No. of patients Percentage No. of patients Percentage
Port site wound infection 3 12% 3 8.8%
Port site sinus tract 1 4% 1 2.94%
Intraabdominal abscess 1 4% 3 8.8%
Persistant abdominal pain - - 1 2.94%
Conversion to laparotomy 1 4% - -
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 120 | Page
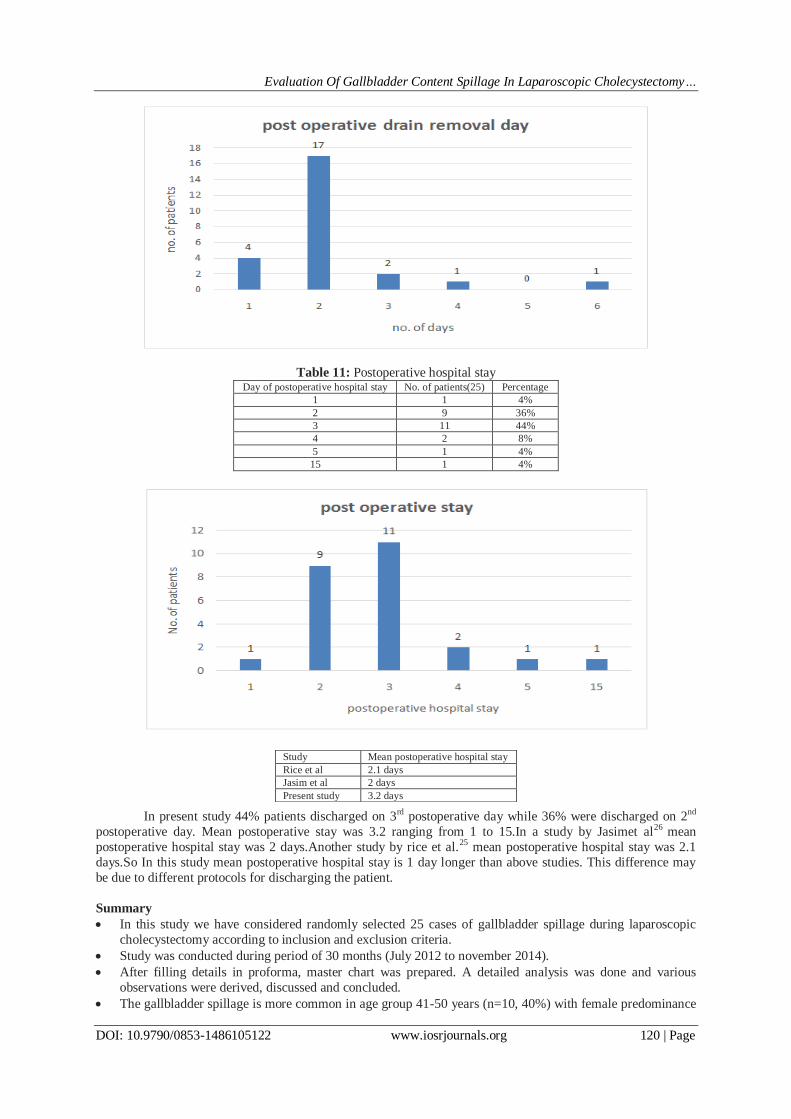
Table 11: Postoperative hospital stay Day of postoperative hospital stay No. of patients(25) Percentage
1 1 4%
2 9 36%
3 11 44%
4 2 8%
5 1 4%
15 1 4%
In present study 44% patients discharged on 3rd postoperative day while 36% were discharged on 2nd
postoperative day. Mean postoperative stay was 3.2 ranging from 1 to 15.In a study by Jasimet al26 mean
postoperative hospital stay was 2 days.Another study by rice et al.25 mean postoperative hospital stay was 2.1
days.So In this study mean postoperative hospital stay is 1 day longer than above studies. This difference may
be due to different protocols for discharging the patient.
Summary
In this study we have considered randomly selected 25 cases of gallbladder spillage during laparoscopic
cholecystectomy according to inclusion and exclusion criteria.
Study was conducted during period of 30 months (July 2012 to november 2014).
After filling details in proforma, master chart was prepared. A detailed analysis was done and various
observations were derived, discussed and concluded.
The gallbladder spillage is more common in age group 41-50 years (n=10, 40%) with female predominance
Study Mean postoperative hospital stay
Rice et al 2.1 days
Jasim et al 2 days
Present study 3.2 days
Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 121 | Page
(F:M:19:6)as gallstone disease itself is more common in females with 41-50 age group.
All patients (n=25, 100%) presented with abdominal pain with 12(48%) patients had belching, 10(40%)
patients had bloating, 7(28%) patients had flatulence, 4(16%) patients had nausea and 1(4%) patient had
vomiting. Abdominal pain, belching and bloating are common clinical features associated with gallstone
disease.
In ultrasonography, 17(68%) patients had contracted gallbladder and 8(32%) patients had distended
gallbladder. 23(92%) patients had normal gallbladder wall and 2(8%) patients had thickened gallbladder
wall. None of them had peri GB collection. 22(88%) patients had multiple GB stones while 3(12%) patients
had single GB stone.
Intraoperative, all patients (100%) had chronically inflammed gallbladder with 1(4%) patient had mucocele
and 1(4%) had pyocele. Out of them, 16(64%) patients had peri GB omental adhesions with difficult
dissection.
Bile spillage was present in 23(92%) patients. 1(4%) patient had pus spillage and 1(4%) patient had mucus
spillage. 7(28%) patients had stone spillage as well. So 16(64%) patients had only bile spillage and 7(28%)
patients had both bile/pus/mucus and stone spillage.
Postoperative complication rate was 24% (n=6). 3(12%) patients developed port site wound infection, 1(4%) patient had intraabdominal abscess formation, 1(4%) patient had port site sinus tract formation and
1(4%) case was converted to laparotomy. Out of these 6 patients, 5(20%) patients had bile/pus with stone
spillage while 1(4%) patient had only bile spillage.
Postoperative, in 17(68%) patients drain was removed on 2nd postoperative day, in 4(16%) patients drain
was removed on 1st day while in 4(16%) patients drain was removed after 2 days.
In 11(44%) patients postoperative hospital stay was 3 days, in 9(36%) patients it was 2 days and 1(4%)
patient discharged on 1st postoperative day. In 4(16%) patients postoperative hospital stay was more than 3
days.
IV. Conclusion Laparoscopic cholecystectomy is the gold standard for gallstone disease.
Gallbladder perforation occurs as a result of intraoperative retraction, dissection and extraction of
gallbladder especially when gallbladder is acutely inflammed and fragile and there is peri GB omental
adhesions.
Gallbladder content spillage is an uncommon occurrence in most of the cases but when it occurs, main goal
of all surgeons should be to manage these complications with minimal harm to the patients and to minimize
unwanted consequences of these complications.
Surgeon should take utmost care and attempt to remove all visible stones and should irrigate abdominal
cavity to dilute infected bile.
If spillage occurs it should be recorded and such patients should be kept under close follow up to aid in
early diagnosis of late complications.
There is no indication for routine conversion to open surgery just for sake of removal of spilled gallstones.
Though complications arises from spillage of gallbladder during laparoscopic cholecystectomy are rare,
they can present months to years later after surgery with septic complications.
Complications are more common after spillage of both bile and stones rather than bile only.
Most of the complications of spillage can be managed by minimal invasive techniques like percutaneous
drainage of abscess. However laparotomy may be needed to address large abscess formation with mass
within it.
Gallbladder spillage during laparoscopic cholecystectomy can be a source of morbidity. So every attempt
should be made to prevent it rather than managing it afterwards.
Acknowledgement I express my sincere gratitude, indebtedness and respect to Dr. G.H.Rathod Professor and Head of
department, Department of Surgery, B.J Medical college and Civil Hospital, Ahmedabad who by his
constant encouragement and concern, inspired and guided me from the very first step of preparation of this
dissertation. His depth of knowledge and insight into the subject of surgery has helped me to study this
topic. His kindness, compassion, perfection, and loving approach to the patients as well as his students has
left a deep impact on my life which will remain throughout my career.
I am also thankful to Dr. H.R. Chauhan, Associate professor Sola Civil Ahmedabad, Dr. R.A Makwana,
Assistant Professor, Dr R.P Gadani, Assistant Profesor and Dr. R.K. Patel, Assistant Professor Department
of Surgery, B.J.Medical College and for their support and invaluable guidance.
I am also thankful to Dr. M.M. Prabhakar, Medical Superintendent, Civil Hospital, for allowing me to carry
out my study in Civil Hospital, Ahmedabad, and for allowing me to use all the invaluable resources.

Evaluation Of Gallbladder Content Spillage In Laparoscopic Cholecystectomy…
DOI: 10.9790/0853-1486105122 www.iosrjournals.org 122 | Page
I am grateful to my parents who have always inspired me in every sphere of my life.
Last but not the least, I am thankful to all my patients and my colleagues and juniors for their cooperation
which helped to complete my study.
References [1]. Bailey and Love short practice of surgery 25th Edition chapter 63
[2]. Laparoscopic cholecystectomy an evidence based guide by ferdinandoagresta, 1st edition, page no. 23,24.
[3]. Evolution of cholecystectomy: A tribute to Carl August Langenbuch. Indian Journal of Surgery 2004;66:97-100.
[4]. Gray’s anatomy, 39th edition, page no. 243-245.
[5]. Laparoscopic surgery of the abdomen By Bruce V. MacFadyen, 1st edition, chapter 15, page no.127
[6]. Maingot’s abdominal operations 11th edition
[7]. Mastery of surgery, 5th edition, chapter 97
[8]. Frola C, Cannici F, Cantoni S, et al.: Peritoneal abscess formation as a late complication of gallstones spilled during laparoscopic
cholecystectomy. British Journal of surgery 1999, 72:201-203.
[9]. Hand AH, Self ML, Dunn E: Abdominal wall abscess formation two years after laparoscopic cholecystectomy. Journal of surgical
endoscopy 2006, 10:105-107.
[10]. Zehetner J, Shamiyeh A, Wayand W: Lost gallstones in laparoscopic cholecystectomy: all possible complications. American
Journal of Surgery 2007, 193:73-78.
[11]. Chowbey PK, Bagchi N, sharma A, et al.: Abdominal Wall Sinus: An unusual presentation of spilled gallstone. Journal of
Laparoscopic and endoscopic Surgery Tech A 2006, 16:613-615.
[12]. Patterson EJ, Nagy AG: Don't cry over spilled stones? Complications of gallstones spilled during laparoscopic cholecystectomy:
case report and literature review. Canadian Journal of Surgery 1997, 40:300-304.
[13]. Cacdac RG, Lakra YP. Abdominal wall sinus tract secondary to gall stones. A complication of laparoscopic cholecystectomy.
Journal of Laparoscopic and endoscopic Surgery 1993; 3: 509–11.
[14]. Yao CC, Wong HH, Yang CC, et al. Abdominal wall abscess secondary to spilled gallstones: late complication of laparoscopic
cholecystectomy and preventive measures. Journal of laparoscopic and endoscopic surgery 2001;11:47–51.
[15]. Albrecht RM, Eghtestad B, Gibel L, et al. Percutaneous removal of spilled gallstones in a subhepatic abscess. American journal of
Surgery2002;68:193–5
[16]. Brueggemeyer MT, Saba AK, Thibodeaux LC. Abscess formation following spilled gallstones during laparascopic
cholecystectomy. Journal of the Society of the Laparoscopic and endoscopic surgery1997;1:145–52.
[17]. Zamir G, Lyass S, Pertsemlidis D, et al. The fate of dropped gallstones during cholecystectomy. Journal of Surgical
endoscopy1999;13:68–70.
[18]. Campbell WB, McGarity WC. An unusual complication of laparoscopic cholecystectomy. American journal of surgery
1992;58:641–42.
[19]. Singh V, Trikha B, Nain CK, Singh K, Bose SM. Epidemiology of gallstone disease in india: A community-based study. Journal of
Gastroenterology 2001; 16: 560-563.
[20]. Welch N, Hinder RA, Fitzgibbons RJ Jr, Rouse JW (1991) Gallstones in the peritoneal cavity: a clinical and experimental study.
Journal of Laparoscopic and Endoscopic surgery 1: 246–247
[21]. Johnston S, O’Malley K, McEntee G, Grace P, Smyth E, Bouchier Hayes D (1994) The need to retrieve the dropped stone during
laparoscopic cholecystectomy. American Journal of Surgery 167: 608–610
[22]. Leland DG, Dawson DL (1993) Adhesions and experimental intraperitoneal gallstones. International journal of Contemporary
Surgery 42: 273–27
[23]. Cline RW, Poulos E, Clifford EJ (1994) An assessment of potential complications caused by intraperitoneal gallstones. American
journal of Surgery 60: 303-305
[24]. Rice DC, Jamison RL, et al (1997) Long-term consequences of intraoperative spillage of bile and gallstones during laparoscopic
cholecystectomy. Journal of Gastrointestinal Surgery 1: 85–91
[25]. Schafer M, Suter C, Klaiber CH, Wehrli H, Frei E, Krahenbuhl L(1998) Spilled gallstones after laparoscopic cholecystectomy: a
relevant problem? A retrospective analysis of 10,174 laparoscopic cholecystectomies. Journal of Surgical Endoscopy 12: 305–309
[26]. Jasim D Saud, MazinA Abdulla &Mushtaq Ch. Abu-Alhail spilled gallstones during laparoscopic cholecystectomy: a prospective
study. (2011) basrah journal of surgery 2: 123-127
[27]. M. A. Memon, R. K. Deeik, T. R. Maffi, R. J. Fitzgibbons The outcome of unretrieved gallstones in the peritoneal cavity
during laparoscopic cholecystectomy: A prospective analysis Journal of Surgical Endoscopy (1999) 13: 848–857





























