Embed Size (px)
Citation preview
Evaluation of information systems
Nicolette de KeizerDept Medical Informatics
AMC - University of Amsterdam
Outline
Significance of evaluationProcess of evaluationEvaluation questionsMethods – study design, data collectionTriangulation
• Reduction of medication error by CPOE• Better treatment / diagnostics by decision-support systems• Increase quality of documentation• Reduce costs by telemedical applications
IT in health care: possible benefits

Unintended Consequences of Information Technologies
Aim Determine the effect on mortality of introducing CPOE into Pittsburgh
childrens hospital Methods
Demography, clinical and mortality data collected on all children transported to a hospital where CPOE implemented institution-wide in 6 days. Trends for 13 months prior and 5 months after compared.
Results Mortality rate increased from 2.80% (39 of 1394) to 6.57% (36 of 548) After adjustment for other covariables, CPOE independently
associated with increased odds of mortality (odds ratio 3.28, 95% C.I. 1.94 – 5.55)
Conclusion When implementing CPOE systems, institutions should continue to
evaluate mortality effects, in addition to medication error rates Importance
Received disproportionate media attention due to reactionary message
Follow-on study in Seattle, using same vendor system, also published in Pediatrics, showed no increase in mortality
Unintended Consequences of Information Technologies
• Brigham and Womens' Hospital, Boston introduced a CPOE system, that allows physicians to order the medication online (and not on paper anymore).
• After implementation, the rate of intercepted Adverse Drug Events (ADE) doubled!
• Reason: The system allowed to easily order much too large dosages of potassium chloride without clear indicating that it be given in divided doses.
Bates et al The impact of computerized physician order entry on medication error prevention. JAMIA 1999, 6(4), 313-21.
Negative effects of CPOE: Example 2
Unintended Consequences of Information Technologies
Reference Linder et al., Arch Intern Med. 2007 Jul
9;167(13):1400-5. [Brigham & Women’s Hospital] Aim
Assess effects of Electronic Health Records on quality of care delivered in ambulatory settings
Methods Retrospective, cross-sectional analysis of 17
quality measures from 2003-2004 National Ambulatory Medical Care Survey, correlated with use of EHRs.
Results EHRs used in 18% of 1.8 billion visits For 14 of 17 quality measures, fraction of visits where
recommended best practice occurred was no different in EHR settings than manual records settings.
2 better with EHR: avoiding benzodiazepines in depression, avoiding routine urinalysis
1 worse with EHR: prescribing statins for hypercholesteremia (33% vs. 47%, p=0.01)
Conclusion As implemented, EHRs not associated with better quality
ambulatory care
Unintended Consequences of Information Technologies
Reference Linder et al., Arch Intern Med. 2007 Jul
9;167(13):1400-5.
Importance Received disproportionate media attention due to
reactionary message Lost in the media hype: Less than 40% of EHR
implementations have all elements important for effects on quality (e-prescribing, test ordering, results, clinical notes, decision support).
Best performance regardless of infrastructure was suboptimal (< 50% adherence to best practice).
Unintended Consequences of Information Technologies
• London Ambulance Dispatch System collapsed due to inadequate testing. Thousands of emergency calls were answered not or too late.
http://www.cs.ucl.ac.uk/staff/A.Finkelstein/las.html
• The malfunction of Therac-25, a medical linear accelerator caused the death of three patients in the late 1980th.
http://courses.cs.vt.edu/~cs3604/lib/Therac_25/Therac_1.html
• University hospital stops introduction of Order Entry System due to user boycott. Costs: up to 34 MIO dollars
Ornstein C (2003) Los Angeles Times Jan 22nd, 2003
Other examples
Insufficiently designed, badly integrated or wrongly used IT systems can lead to user frustration and errors.
„Bad health informatics can kill“
Ammenwerth E, Shaw NT. Bad health informatics can kill - is evaluation the answer? Methods of Information in Medicine 2005;44:1-3.
Examples: http://iig.umit.at/efmi/ -> Bad Health Informatics can Kill
Need for Evaluation
IT systems can have large impact
on quality of careIT systems are costly
IT systems can fail or be sub-optimal designed
Evaluation is a way
to provide better IT Systems
Systematic Evaluation of IT is essential
Formative (constructive): evaluation looking forward
Summative: evaluation looking backward
• Evaluation is • the act of measuring or exploring properties
• of a health information system (in planning, in development, in implementation, or in operation),
• the result of which informs a decision to be made concerning that system in a specific context.
Ammenwerth E, Brender J, Nykänen P, Prokosch U, Rigby M, Talmon J. Visions and strategies to improve evaluations of health information systems - reflections and lessons based on the HIS-EVAL workshop in Innsbruck. Int J Med Inform 2004 Jun 30;73(6):479-91.
Evaluation: Definition (1/2)
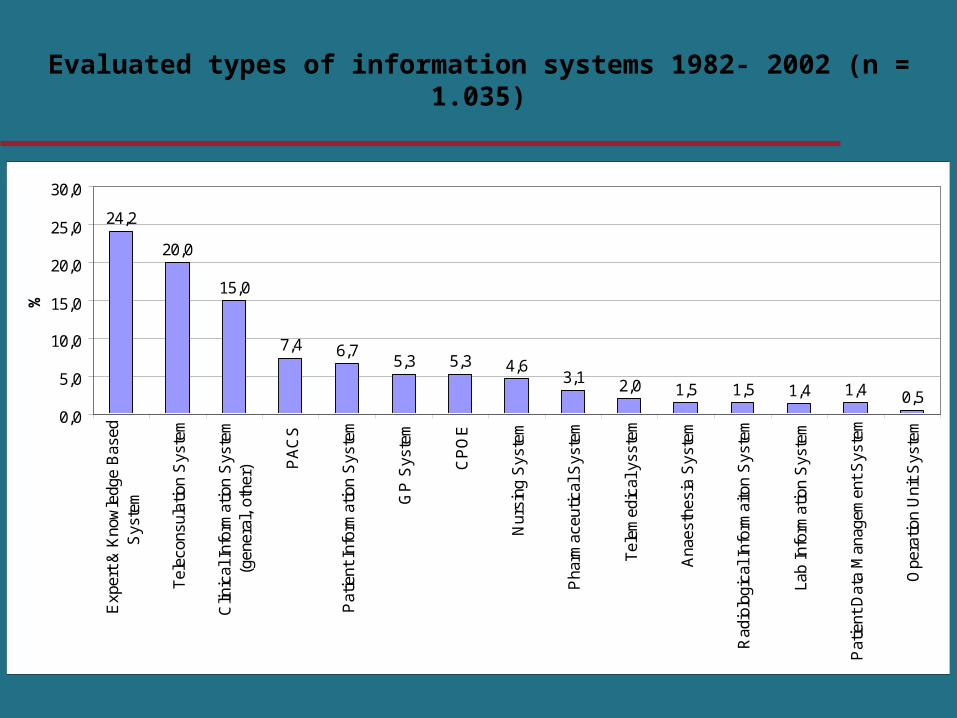
24,2
20,0
15,0
7,4 6,75,3 5,3 4,6
3,1 2,0 1,5 1,5 1,4 1,4 0,50,0
5,0
10,0
15,0
20,0
25,0
30,0
Exp
ert
& K
now
ledg
e B
ased
Sys
tem
Tel
econ
sula
tion
Sys
tem
Clin
ical
Inf
orm
atio
n S
yste
m(g
ener
al,
othe
r) PA
CS
Pat
ient
Inf
orm
atio
n S
yste
m
GP
Sys
tem
CP
OE
Nur
sing
Sys
tem
Pha
rmac
eutic
al S
yste
m
Tel
emed
ical
yss
tem
Ana
esth
esia
Sys
tem
Rad
iolo
gica
l Inf
orm
aito
n S
yste
m
Lab
Info
rmat
ion
Sys
tem
Pat
ient
Dat
a M
anag
emen
t S
yste
m
Ope
ratio
n U
nit
Sys
tem
%
Evaluated types of information systems 1982- 2002 (n = 1.035)

0
20
40
60
80
100
120
140
Num
ber
of
stu
die
s p
ublis
hed e
ach y
ear
Annualy published papers in PubMed on IT evaluation in health care (PubMed analysis)
0.6% of all papers
1.0% of all papers
Ammenwerth, de Keizer (2004)
Evaluation in Informatics is Notoriously Difficult
We live in a pluralistic world. There will be many points of view on need, benefit, quality.
Real people using deployed technology: things can go wrong or right for very complicated reasons
Intersection of 3 domains where progress is very rapid: Work in the domain (health care, bio-science) Information technology Evaluation methods
Sometimes they don’t really want to know...
Outline
Significance of evaluationProcess of evaluationEvaluation questionsMethods – study design, data collectionTriangulationPublication bias
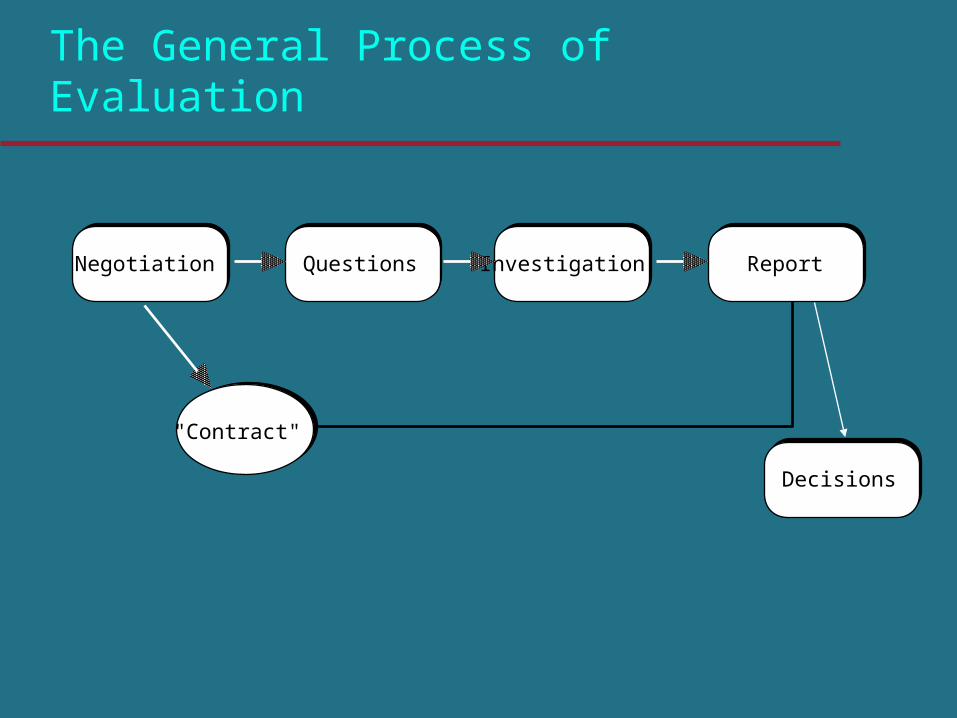
The General Process of Evaluation
"Contract"
Questions ReportInvestigationNegotiation
Decisions
Negotiation and Contract
Identify the primary audience(s) and interact with them
"Contract"
Questions ReportInvestigationNegotiation
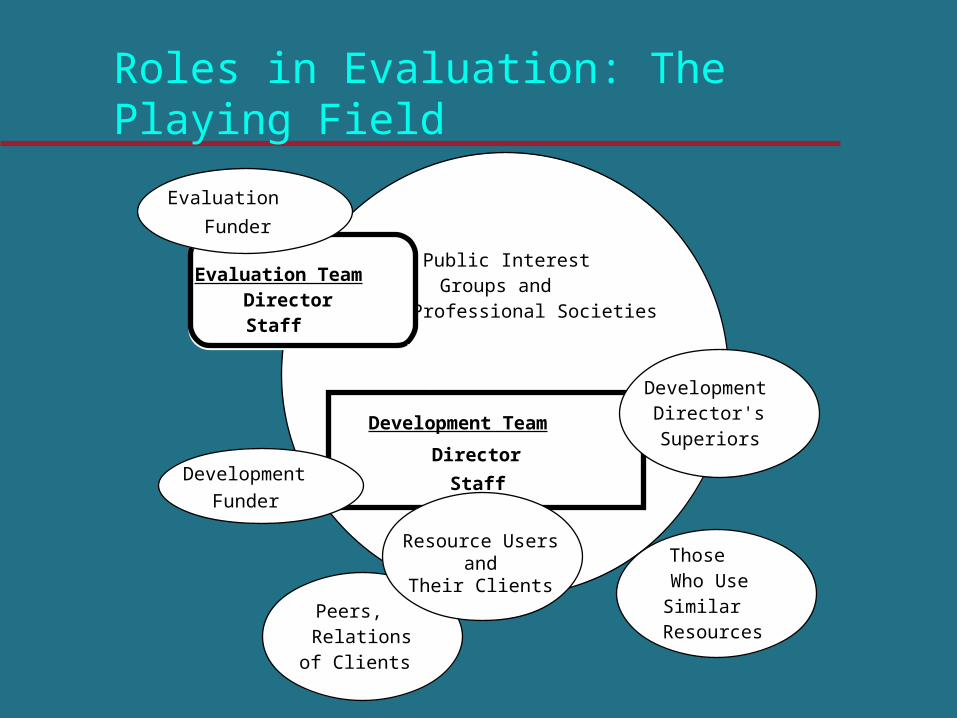
Roles in Evaluation: The Playing Field
Director
StaffFunder
Evaluation
Funder
Peers,Relations
of Clients
ThoseWho UseSimilarResources
Public InterestGroups and
Professional Societies
Evaluation TeamDirectorStaff
Development Team Director'sSuperiors
Development
Development
Resource Users and
Their Clients
Negotiation and Contract
Identify the primary audience(s) and interact with them Set general goals and purposes of the study Identify, in general, the methods to be used Identify permissions, accesses, confidentiality issues
and other key administrative aspects of the study Describe the result reporting process Reflect this in a written agreement
"Contract"
Questions ReportInvestigationNegotiation
Questions
Specific questions derived from the general Maximum 5-10 They do not have to be stated as hypotheses Depending on methods used, the questions can
change over the course of the study
"Contract"
Questions ReportInvestigationNegotiation
Investigation
Choose data collection methods There are two major families of investigational
approaches: objectivist and subjectivist Although some studies use both families,
typically you will choose one or the other
"Contract"
Questions ReportInvestigationNegotiation
Report
Process of communicating findings: reporting is often done in stages
It doesn’t have to be a written document exclusively
Targeted at the audience(s), in language they can understand
Report must conform the evaluation agreement
"Contract"
Questions ReportInvestigationNegotiation
Subjectivistic vs. objectivistic
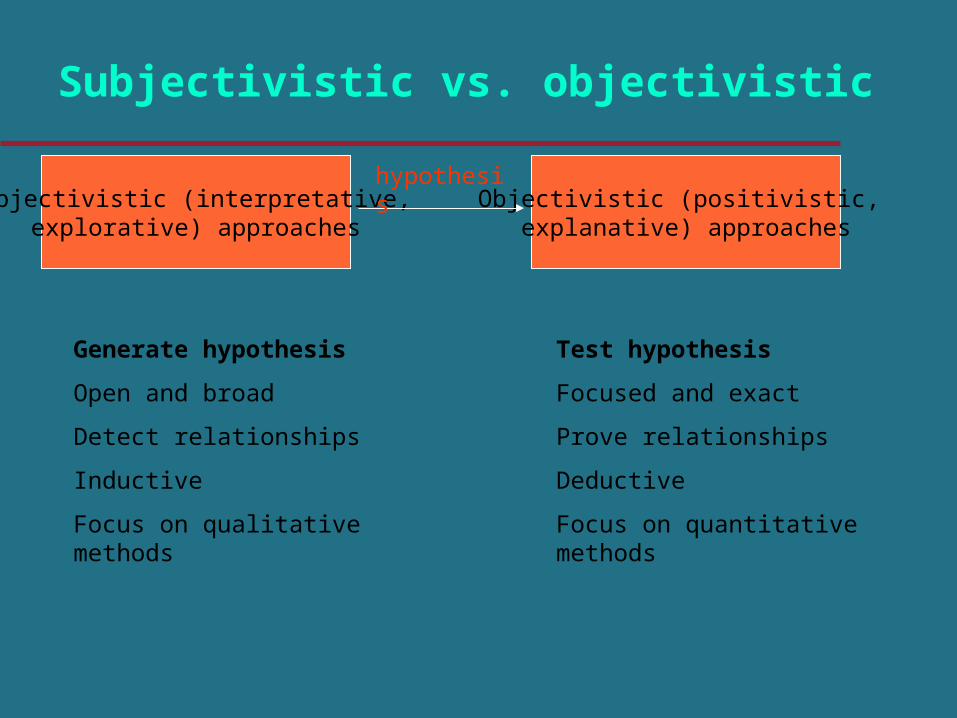
Generate hypothesis
Open and broad
Detect relationships
Inductive
Focus on qualitative methods
Subjectivistic (interpretative, explorative) approaches
Objectivistic (positivistic, explanative) approaches
Test hypothesis
Focused and exact
Prove relationships
Deductive
Focus on quantitative methods
hypothesis
Group work
Judge abstracts 1 and 2: Subjectivist or objectivist study?
Outline
Significance of evaluationProcess of evaluationEvaluation questionsMethods – study design, data collectionTriangulation
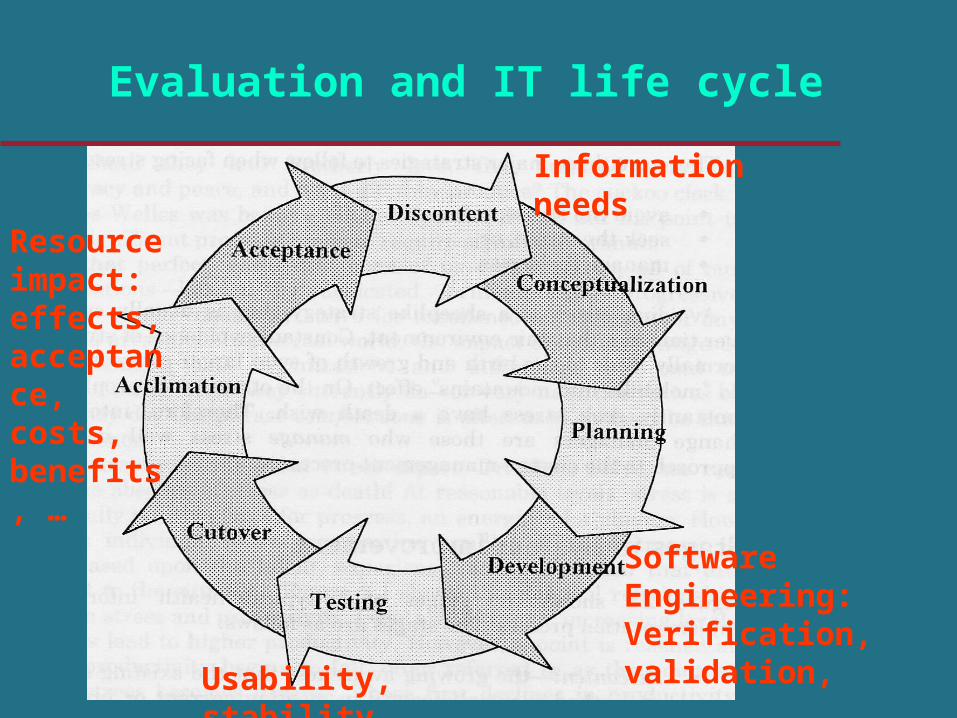
Evaluation and IT life cycle
Resource impact: effects, acceptance, costs, benefits, …
Usability, stability, …
Software Engineering: Verification, validation,
Information needs
Group work
What kind of aspects do you want to evaluate if your hospital implement a nursing documentation system or a DSS application? Physician Nurse Manager Developer
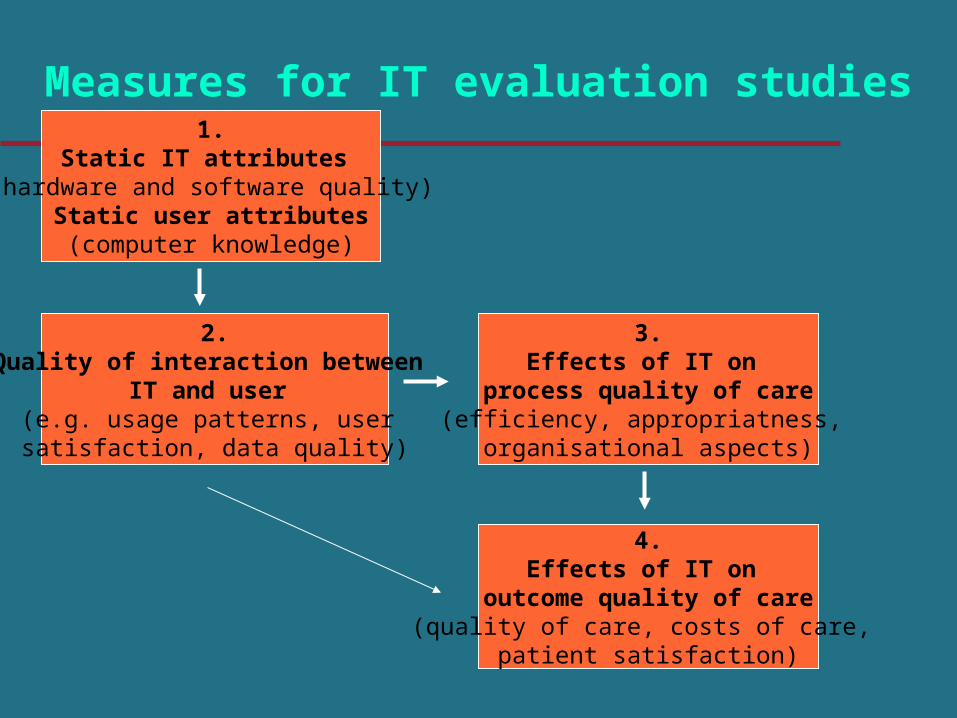
Measures for IT evaluation studies1.
Static IT attributes (hardware and software quality)
Static user attributes(computer knowledge)
2.Quality of interaction between
IT and user (e.g. usage patterns, user satisfaction, data quality)
3.Effects of IT on
process quality of care(efficiency, appropriatness,
organisational aspects)
4.Effects of IT on
outcome quality of care(quality of care, costs of care,
patient satisfaction)
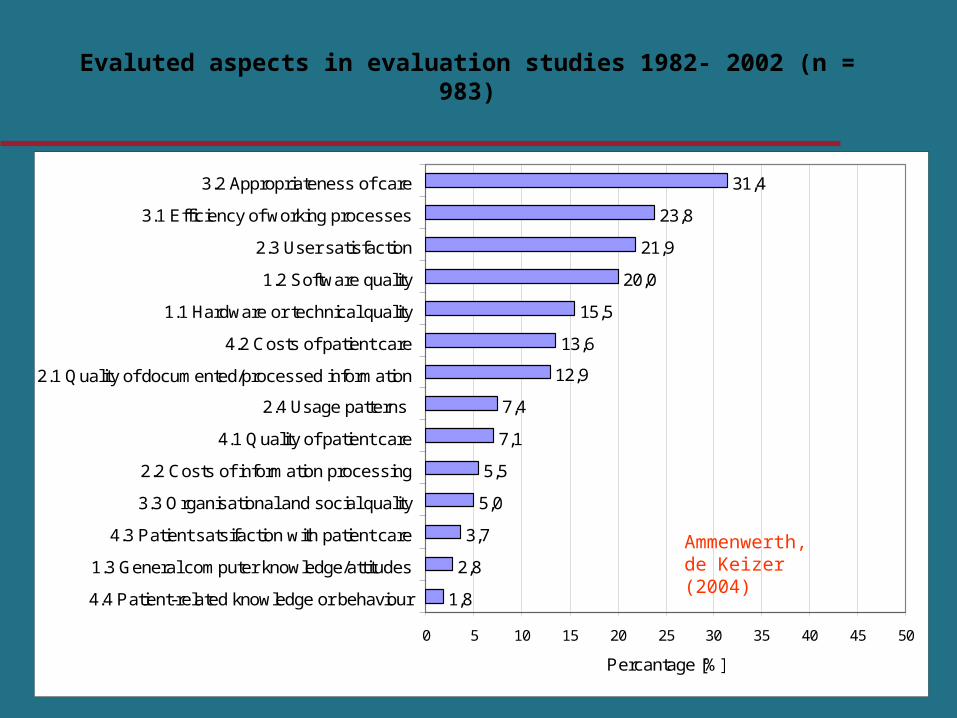
1,8
2,8
3,7
5,0
5,5
7,1
7,4
12,9
13,6
15,5
20,0
21,9
23,8
31,4
0 5 10 15 20 25 30 35 40 45 50
4.4 Patient-related knowledge or behaviour
1.3 General computer knowledge/attitudes
4.3 Patient satsifaction with patient care
3.3 Organisational and social quality
2.2 Costs of information processing
4.1 Quality of patient care
2.4 Usage patterns
2.1 Quality of documented/processed information
4.2 Costs of patient care
1.1 Hardware or technical quality
1.2 Software quality
2.3 User satisfaction
3.1 Efficiency of working processes
3.2 Appropriateness of care
Percantage [%]
Evaluted aspects in evaluation studies 1982- 2002 (n = 983)
Ammenwerth, de Keizer (2004)
Why formulate questions ?
Crystallize thinking of evaluators and key “stakeholders”
There is a need to focus and prioritize It converts broad aims into specific questions that
can potentially be answered
Further benefits of identifying questions
Stakeholders can see where their concerns are being addressed
The choice of methods follows from the question
A list discourages evaluators from focusing only on questions amenable to their preferred methods
• Evaluation is part of the whole IT life cycle
• Any evaluation must have a clear evaluation question (there is no „global“ or „absolute“ evaluation).
• The evaluation questions should be decided by the stakeholders.
Evaluation question: Recommendations
Take the time for elaborating clear and agreed evaluation questions!
Outline
Significance of evaluationProcess of evaluationEvaluation questionsMethods – data collection & study designTriangulation
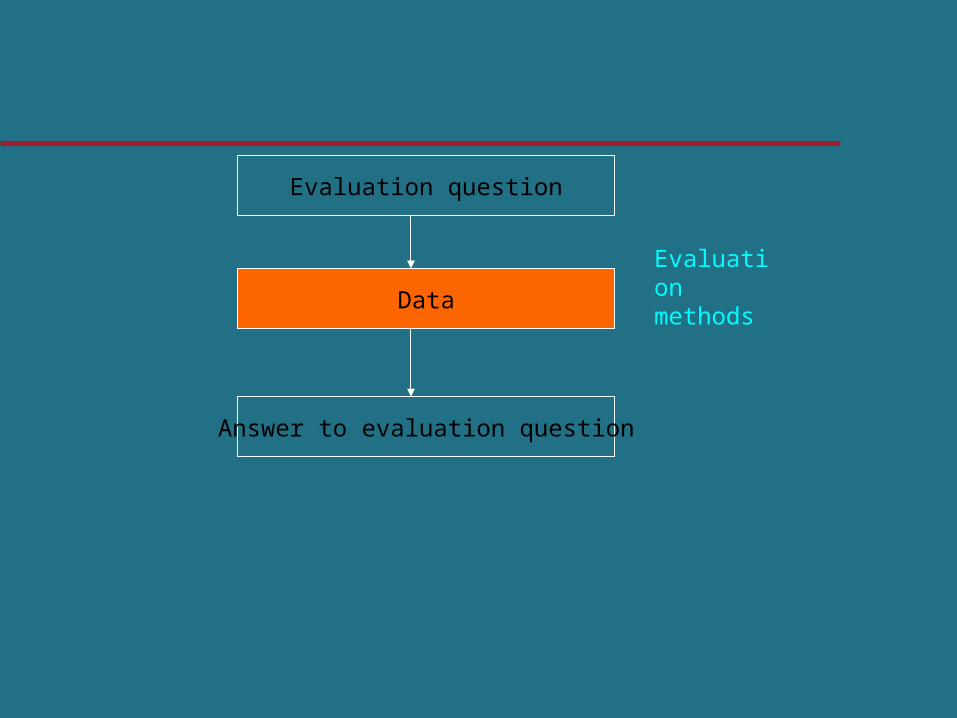
Evaluation question
Answer to evaluation question
Data
Evaluation methods
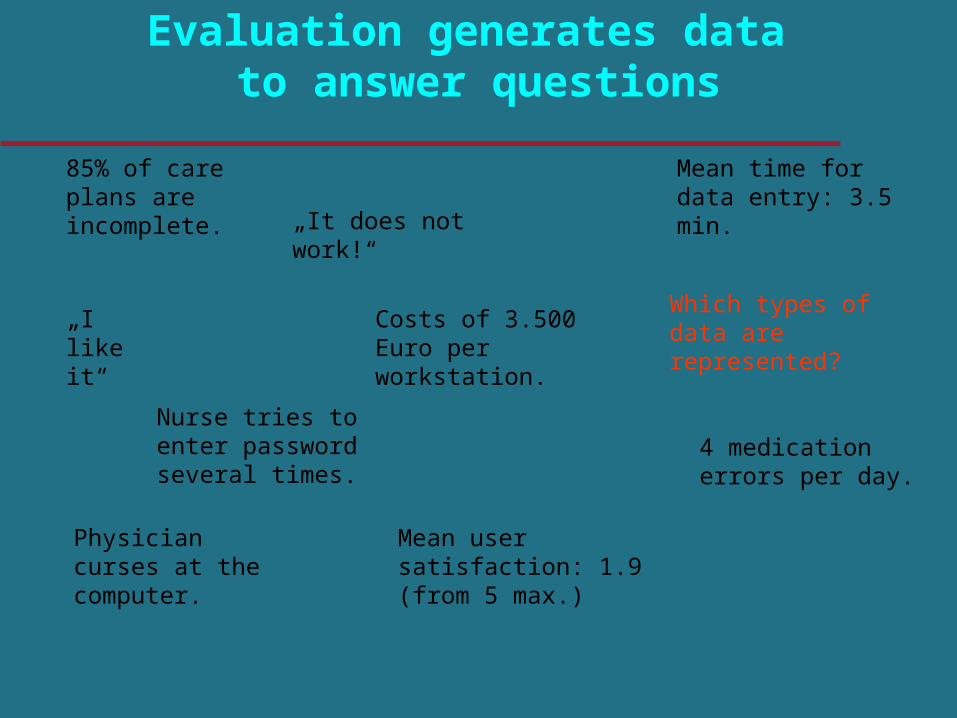
Evaluation generates data to answer questions
„I like it“
„It does not work!“
Physician curses at the computer.
Nurse tries to enter password several times.
Mean time for data entry: 3.5 min.
Mean user satisfaction: 1.9 (from 5 max.)
85% of care plans are incomplete.
4 medication errors per day.
Costs of 3.500 Euro per workstation.
Which types of data are represented?
Data
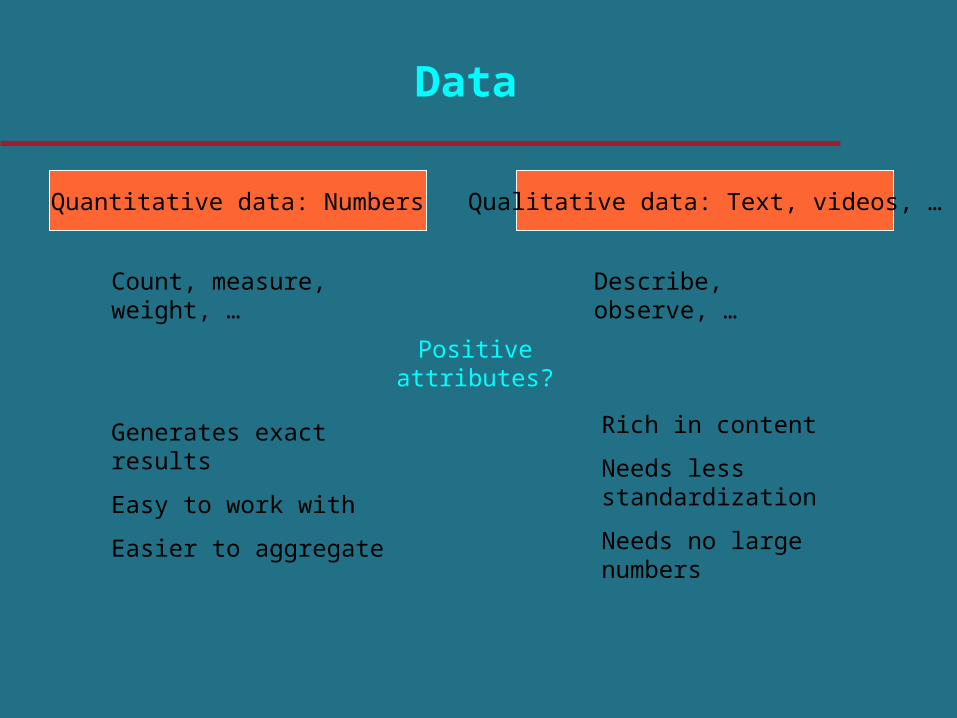
Quantitative data: Numbers Qualitative data: Text, videos, …
Count, measure, weight, … Describe, observe, …
Generates exact results
Easy to work with
Easier to aggregate
Rich in content
Needs less standardization
Needs no large numbers
Positive attributes?

0
10
20
30
40
50
60
70
80
90
100
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
Per
cent
age
[%]
more quantitativemethods usedmore qualitativemethods usedmixed or unclear
Quantitative vs. qualitative methods in evaluation studies 1982- 2002 (n = 983)
Ammenwerth, de Keizer (2004)
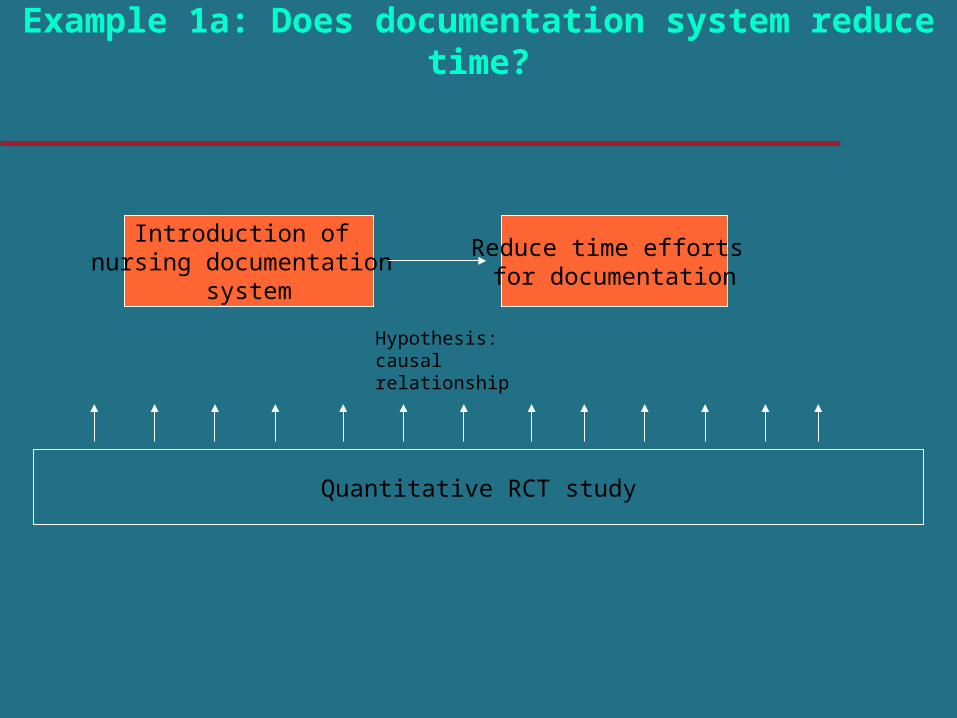
Quantitative RCT study
Introduction of nursing documentation
system
Reduce time efforts for documentation
Hypothesis: causal relationship
Example 1a: Does documentation system reduce time?
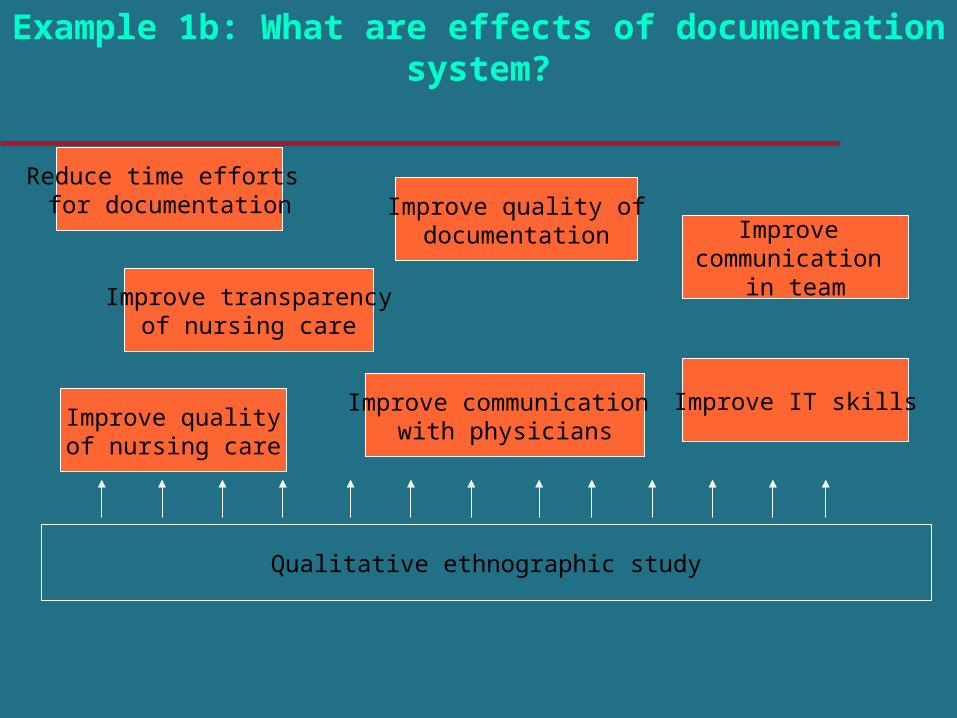
Example 1b: What are effects of documentation system?
Improve transparencyof nursing care
Reduce time efforts for documentation
Improve communication with physicians
Improve communication
in team
Improve qualityof nursing care
Improve IT skills
Improve quality ofdocumentation
Qualitative ethnographic study
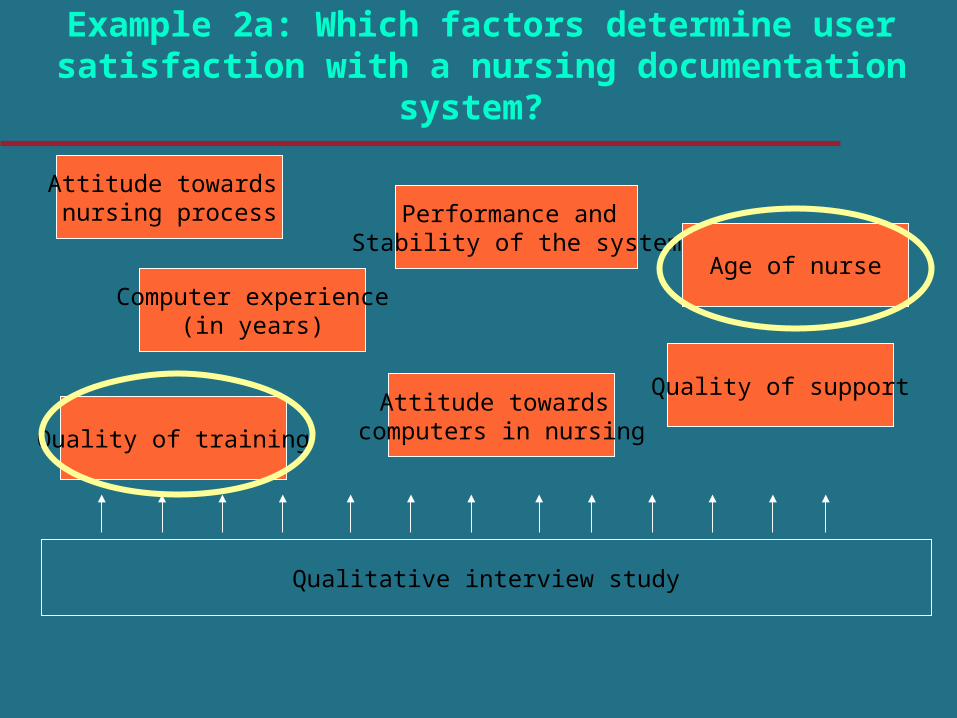
Example 2a: Which factors determine user satisfaction with a nursing documentation system?
Computer experience(in years)
Attitude towards nursing process
Attitude towards computers in nursing
Age of nurse
Quality of training
Quality of support
Performance and Stability of the system
Qualitative interview study
Quality of training
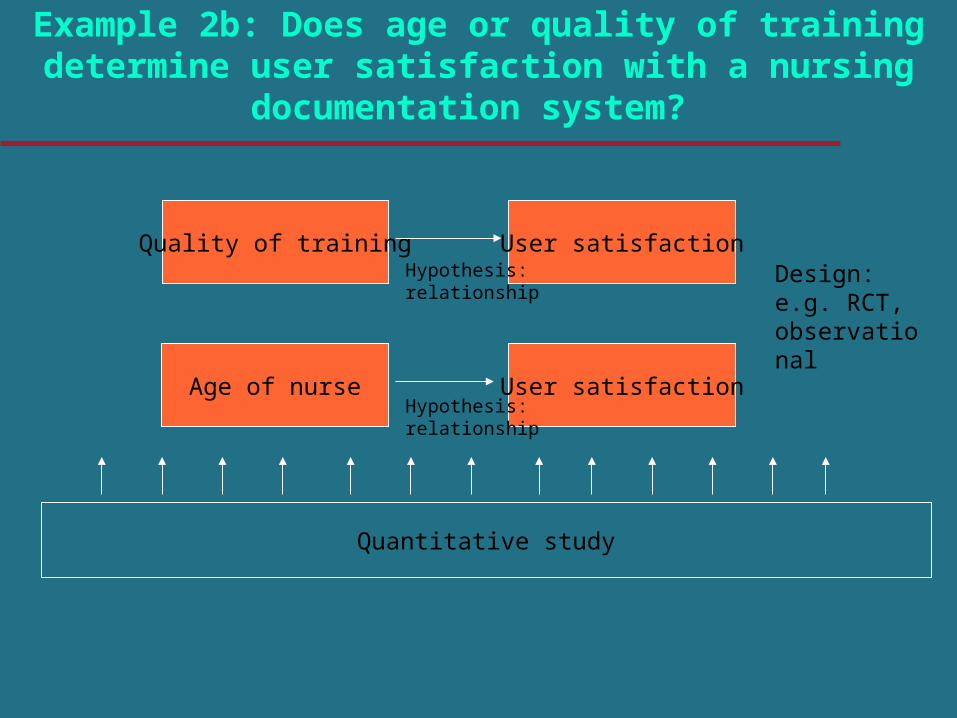
Quantitative study
Example 2b: Does age or quality of training determine user satisfaction with a nursing documentation system?
User satisfaction
User satisfactionAge of nurse
Hypothesis: relationship
Hypothesis: relationship
Design: e.g. RCT, observational
Kinds of evaluation study
Objectivist studiesSubjectivist studies
Evaluation studies
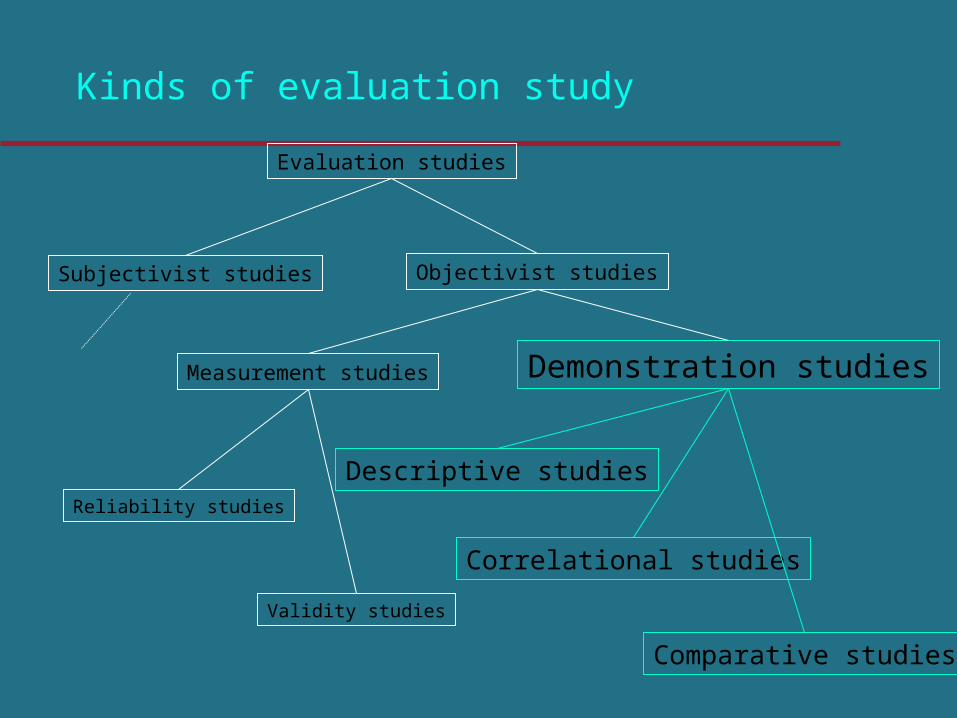
Kinds of evaluation study
Objectivist studiesSubjectivist studies
Measurement studies Demonstration studies
Descriptive studies
Correlational studies
Comparative studies
Reliability studies
Validity studies
Evaluation studies
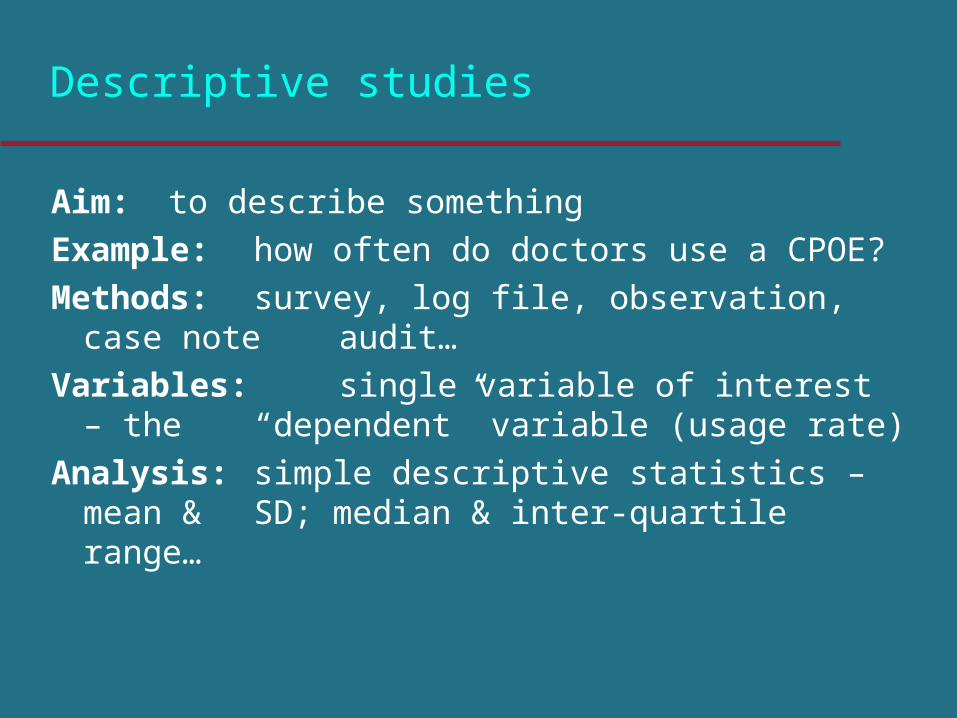
Descriptive studies
Aim: to describe something
Example: how often do doctors use a CPOE?
Methods: survey, log file, observation, case note audit…
Variables: single variable of interest – the “dependent” variable (usage rate)
Analysis: simple descriptive statistics – mean & SD; median & inter-quartile range…
Correlational studies
Aim: to correlate something with something else
Example: is CPOE use associated with less calls from pharmacy to department ?
Methods: survey, log file, observation, case note audit…
Variables: “dependent” variable (calls) + independent variables (usage rate, age…)
Analysis: univariate or multivariate regression
Comparative studies
Aim: to assess cause and effectExample: does CPOE cause less medication
errors? Methods: experiments: before-after, interrupted
time series, randomised trial…Variables: “dependent” variable (errors) +
independent variable (allocation to CPOE, actual usage rate, pt. age…)
Analysis: hypothesis testing or estimation (t tests, chi squared, analysis of variance…)
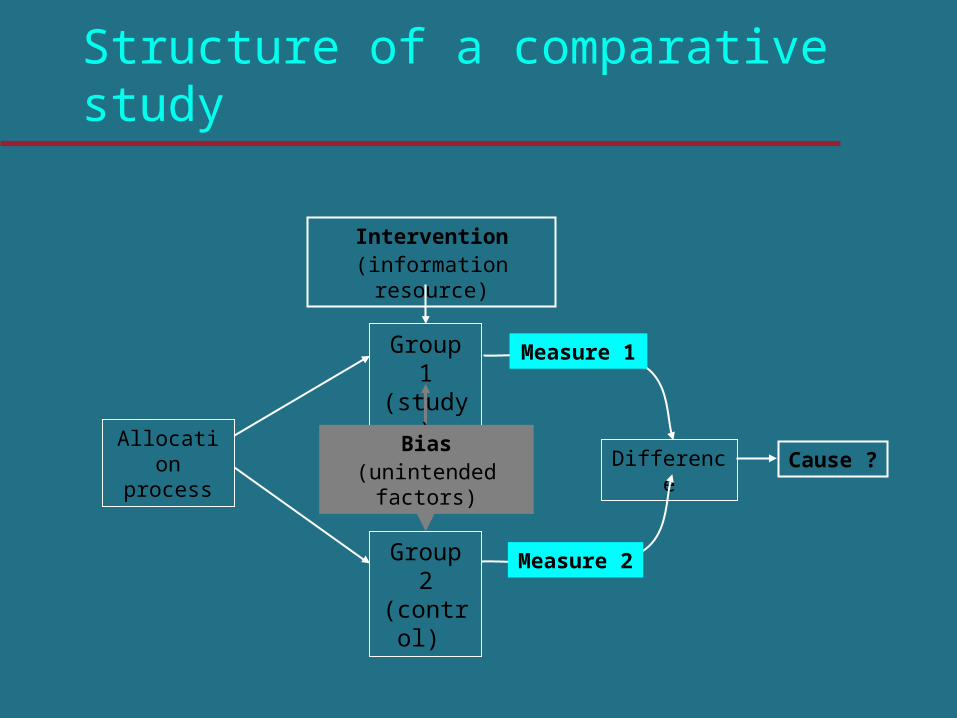
Structure of a comparative study
Group 2 (control)
Group 1 (study)
Intervention(information resource)
Difference Cause ?Bias
(unintended factors)
Allocation process
Measure 1
Measure 2
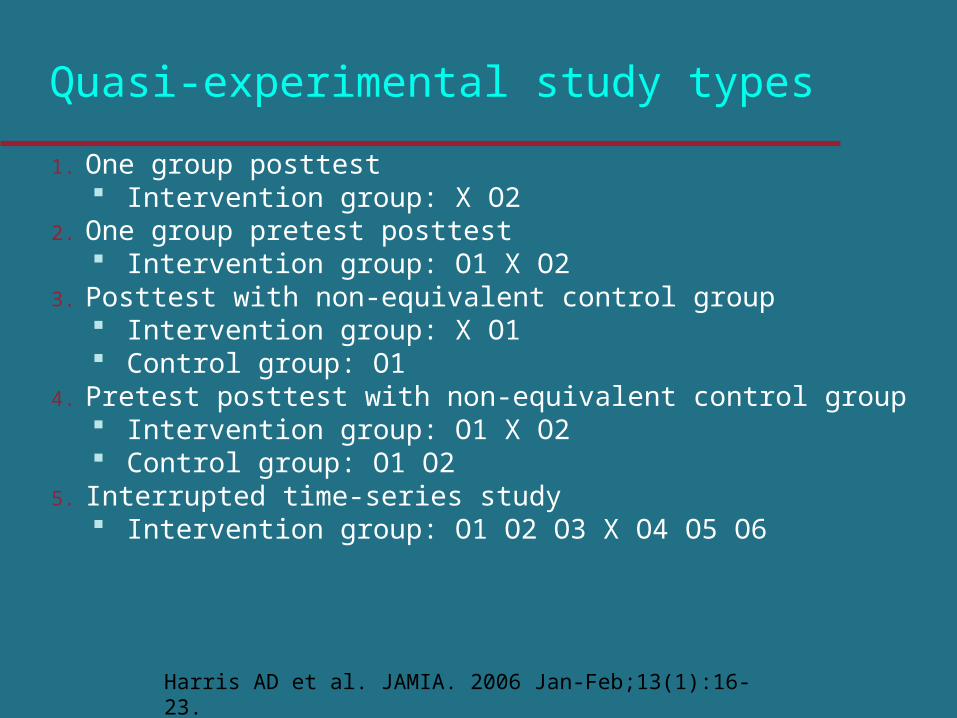
Quasi-experimental study types
1. One group posttest Intervention group: X O2
2. One group pretest posttest Intervention group: O1 X O2
3. Posttest with non-equivalent control group Intervention group: X O1 Control group: O1
4. Pretest posttest with non-equivalent control group Intervention group: O1 X O2 Control group: O1 O2
5. Interrupted time-series study Intervention group: O1 O2 O3 X O4 O5 O6
Harris AD et al. JAMIA. 2006 Jan-Feb;13(1):16-23.
Group work
Study design of abstract 2, 3, 4, 5, 6
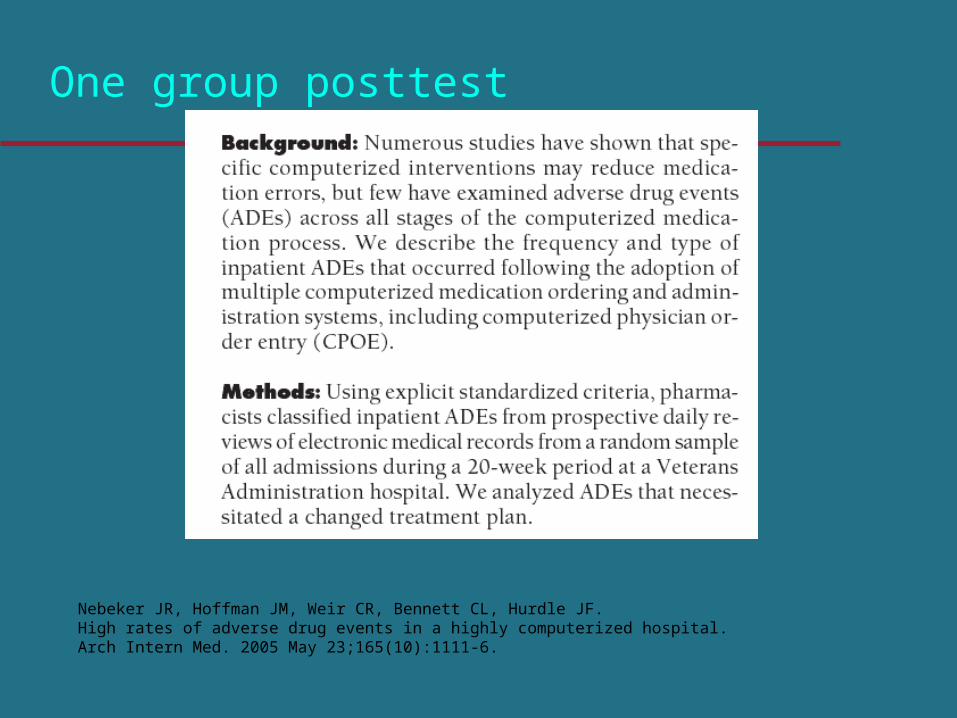
One group posttest
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital.Arch Intern Med. 2005 May 23;165(10):1111-6.
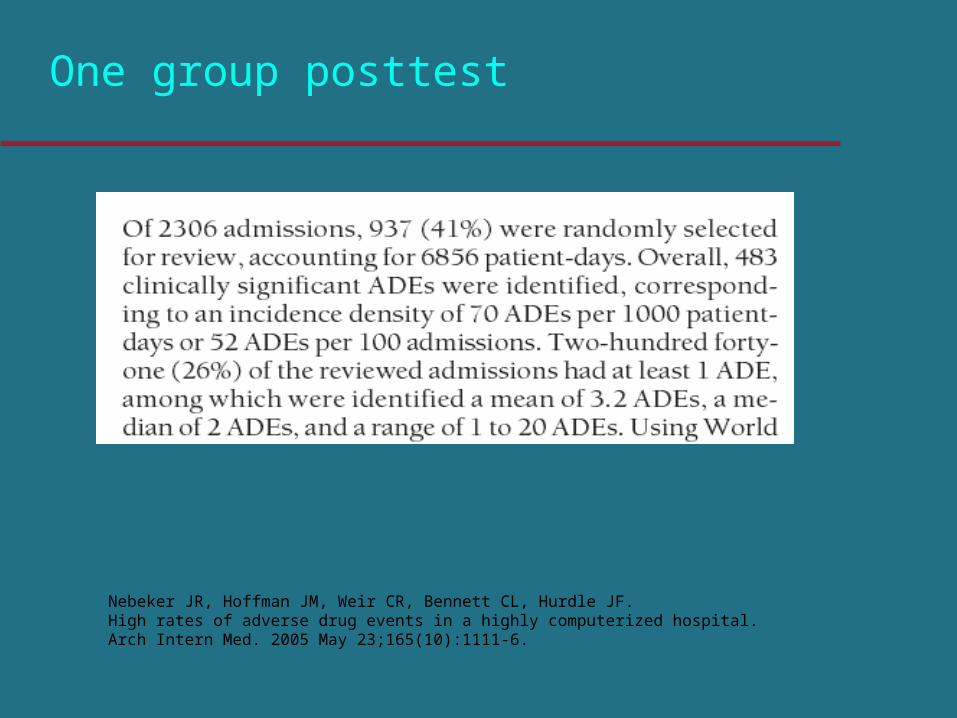
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital.Arch Intern Med. 2005 May 23;165(10):1111-6.
One group posttest
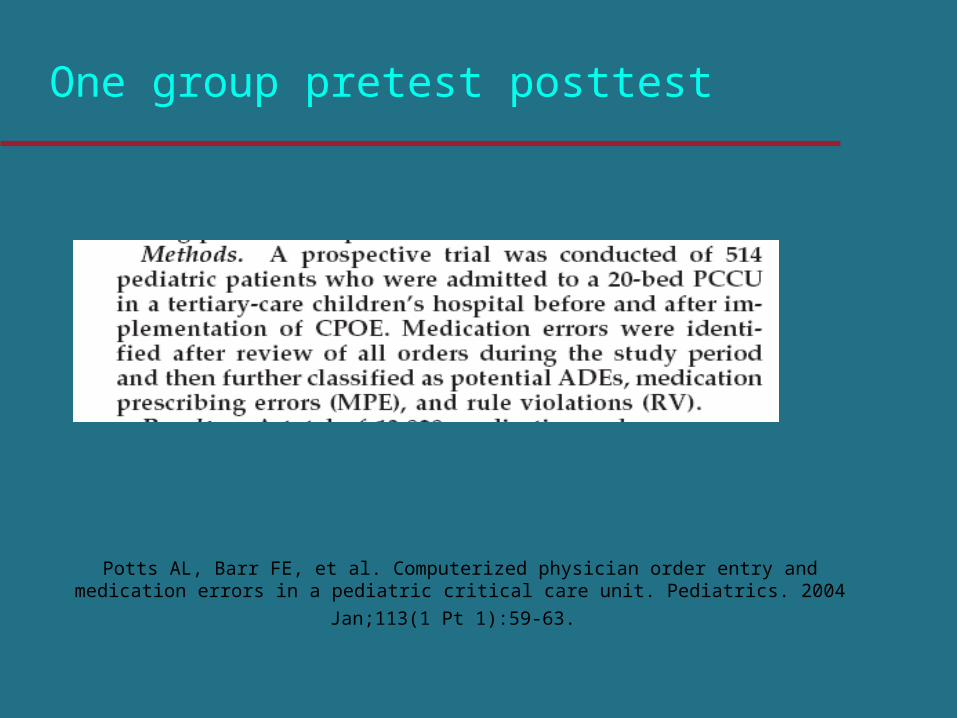
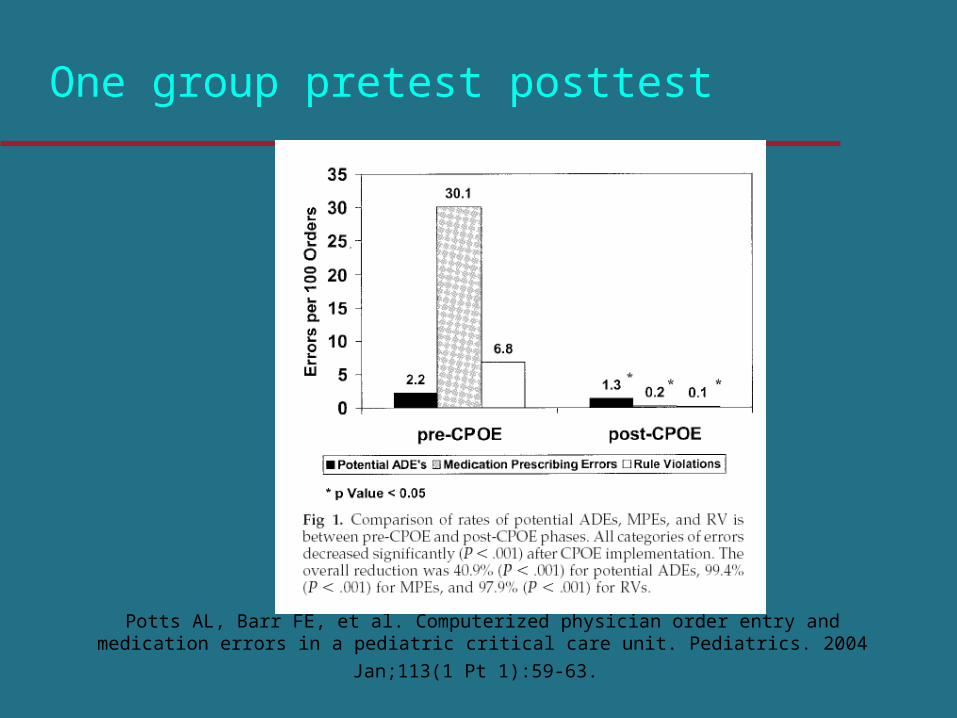
One group pretest posttest
Potts AL, Barr FE, et al. Computerized physician order entry and medication errors in a pediatric
critical care unit. Pediatrics. 2004 Jan;113(1 Pt 1):59-63.
One group pretest posttest
Potts AL, Barr FE, et al. Computerized physician order entry and medication errors in a pediatric
critical care unit. Pediatrics. 2004 Jan;113(1 Pt 1):59-63.
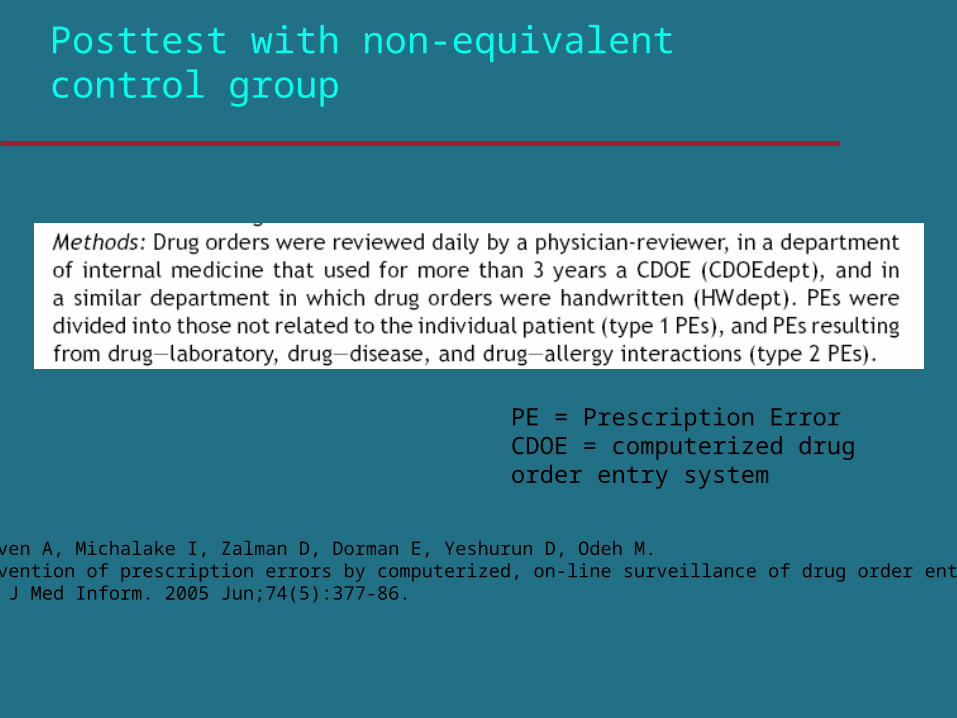
Posttest with non-equivalent control group
PE = Prescription ErrorCDOE = computerized drug order entry system
Oliven A, Michalake I, Zalman D, Dorman E, Yeshurun D, Odeh M. Prevention of prescription errors by computerized, on-line surveillance of drug order entry.Int J Med Inform. 2005 Jun;74(5):377-86.
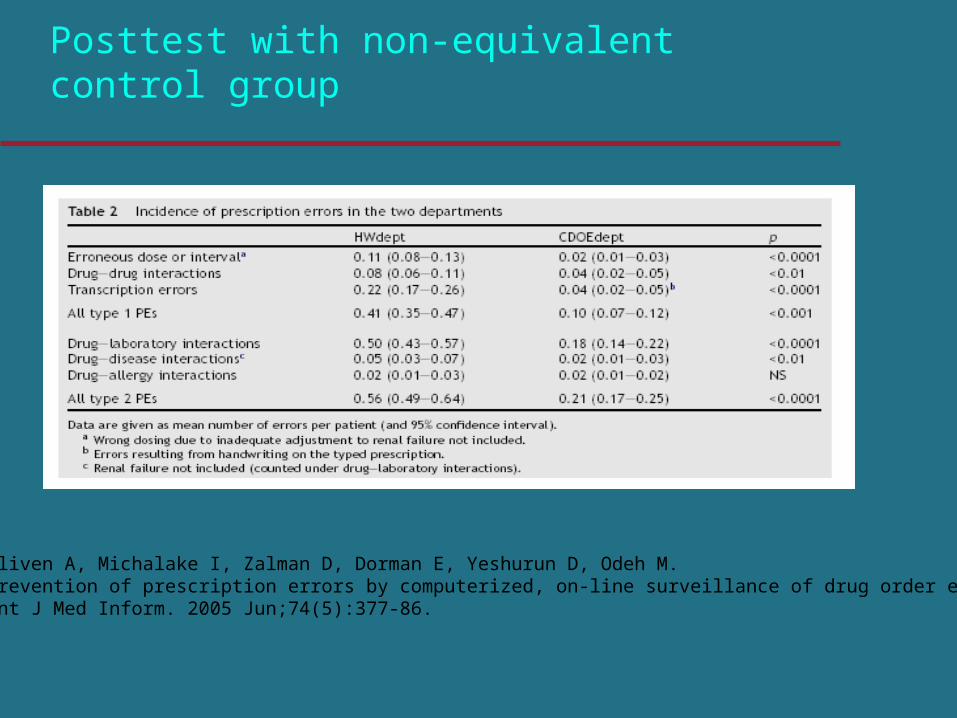
Posttest with non-equivalent control group
Oliven A, Michalake I, Zalman D, Dorman E, Yeshurun D, Odeh M. Prevention of prescription errors by computerized, on-line surveillance of drug order entry.Int J Med Inform. 2005 Jun;74(5):377-86.
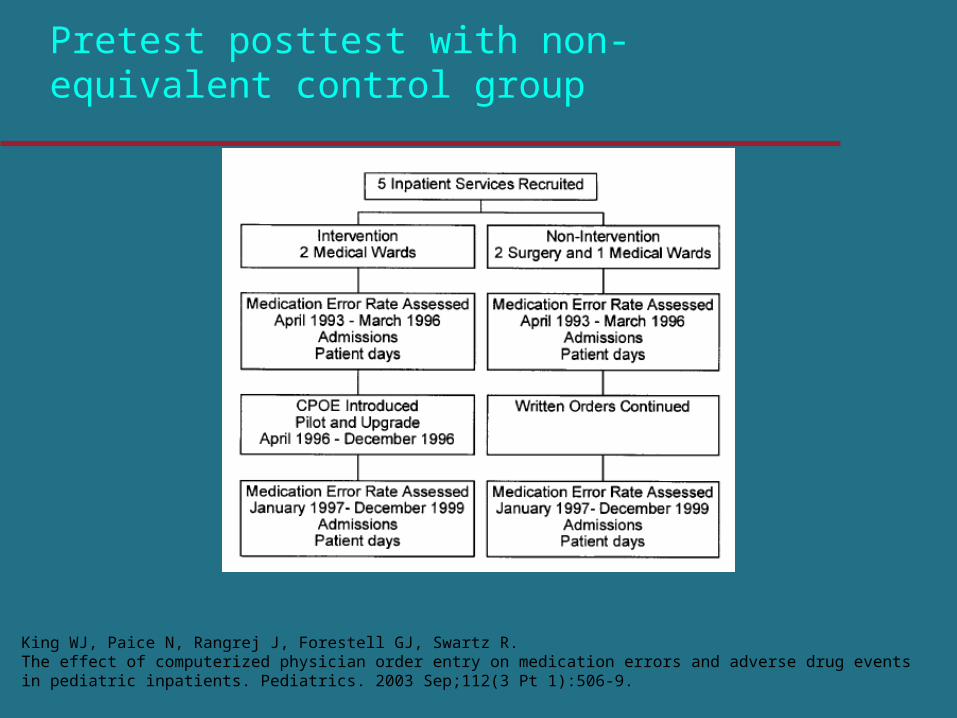
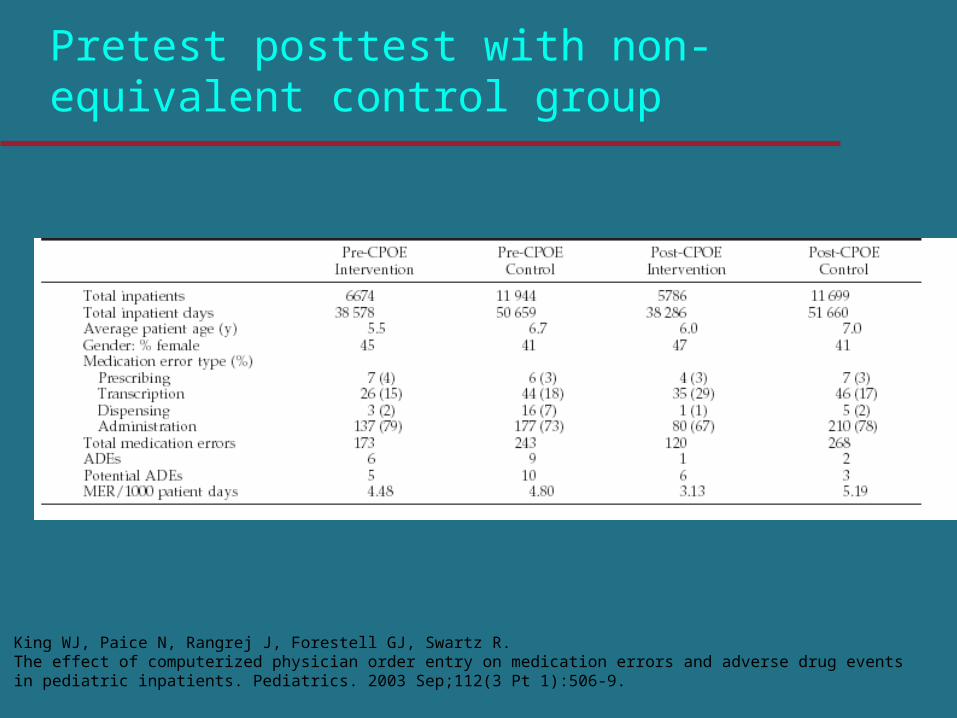
Pretest posttest with non-equivalent control group
King WJ, Paice N, Rangrej J, Forestell GJ, Swartz R. The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients. Pediatrics. 2003 Sep;112(3 Pt 1):506-9.
King WJ, Paice N, Rangrej J, Forestell GJ, Swartz R. The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients. Pediatrics. 2003 Sep;112(3 Pt 1):506-9.
Pretest posttest with non-equivalent control group
Problems with (one group) before-after studies
Other internal changes: insights from health care redesign, staff training, re-deployment…
External changes in health policies, practice guidelines, technologies, professional training, staff shortages, patient case-mix, expectations, eHealth…
Problems with (one group) before-after studies
Result: confounding - were differences due to system, to redesign, to improved data, or something else ?
Need to control for confounding: option 1: carefully chosen external and internal controls
Controlled before-after studies
External control: same data / practice in one or more matched external
groups of practitioners subject to the same confounders not exposed to the intervention
Internal control: similar data / practice in the same target practitioners subject to the same confounders not susceptible to the intervention
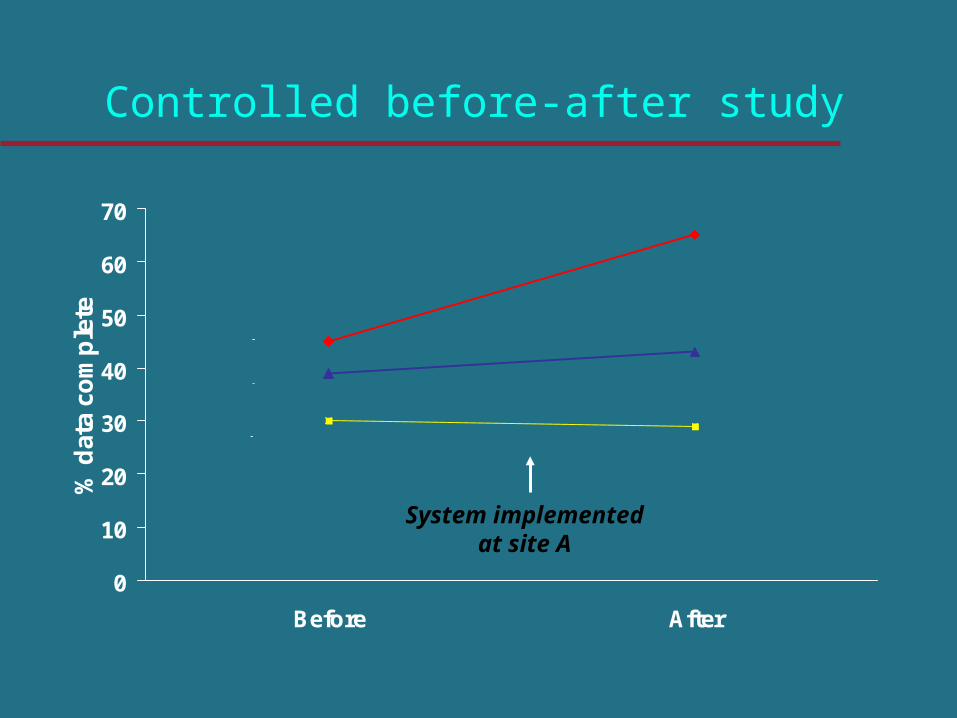
Controlled before-after study
0
10
20
30
40
50
60
70
Before After
% d
ata
com
ple
te
asthma, site A
diabetes, site A
asthma, site B
System implemented at site A
Problems with before-after studies
Result: confounding - were differences due to system, to redesign, to improved data, or something else ?
Need to control for confounding: option 1: carefully chosen external and internal controls option 2: interrupted time series
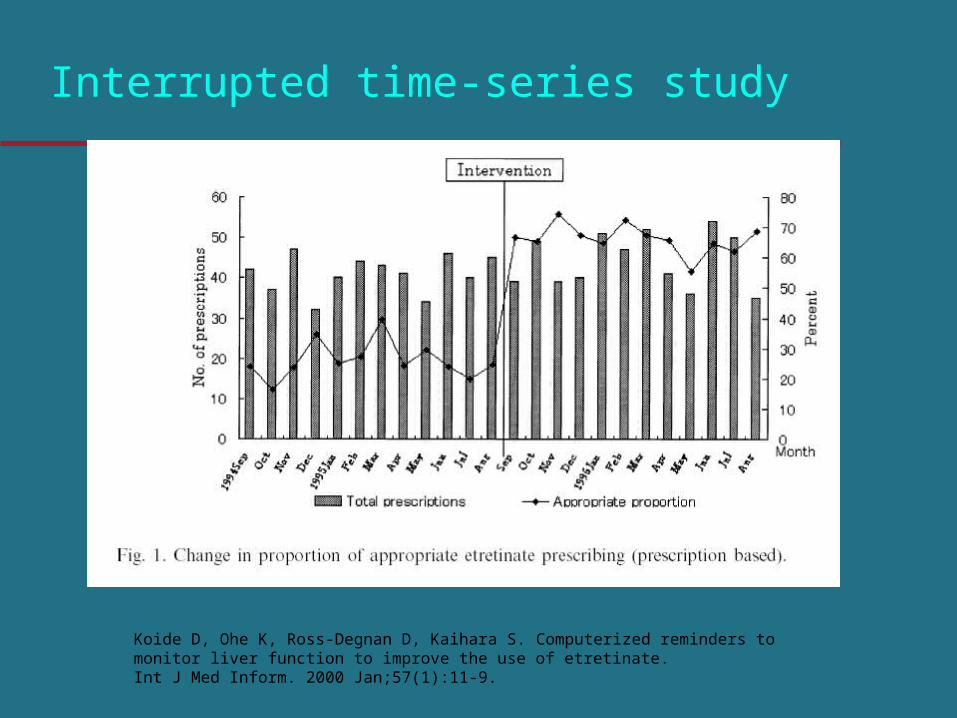
Interrupted time-series study
Koide D, Ohe K, Ross-Degnan D, Kaihara S. Computerized reminders to monitor liver function to improve the use of etretinate.Int J Med Inform. 2000 Jan;57(1):11-9.
Interrupted time series
At least 3 pre- and 3 post-intervention measurements
Aim to demonstrate regression discontinuity
Problems: Cost of making repeated measurements -use routine data Difficulty separating intervention from baseline drift,
seasonal effects...
Problems with before-after studies
Result: confounding - were differences due to system, to redesign, to improved data, or something else ?
Need to control for confounding: option 1: carefully chosen external and internal controls option 2: interrupted time series option 3: randomized controlled trial
Randomization
Berner ES et al. Improving ambulatory prescribing safety with a handheld decision support system: a randomized controlled trial.J Am Med Inform Assoc. 2006 Mar-Apr;13(2):171-9.
CDSS = computerized decision support system
NSAID = nonsteroidal anti-inflammatory drug
„The randomized controlled trial (RCT) is the gold standard of evaluation“
(Rotman 1996)
What do you think?
For which questions is the RCT useful?Are there situations where RCT is not possible?For which questions is the RCT not useful?
Study design
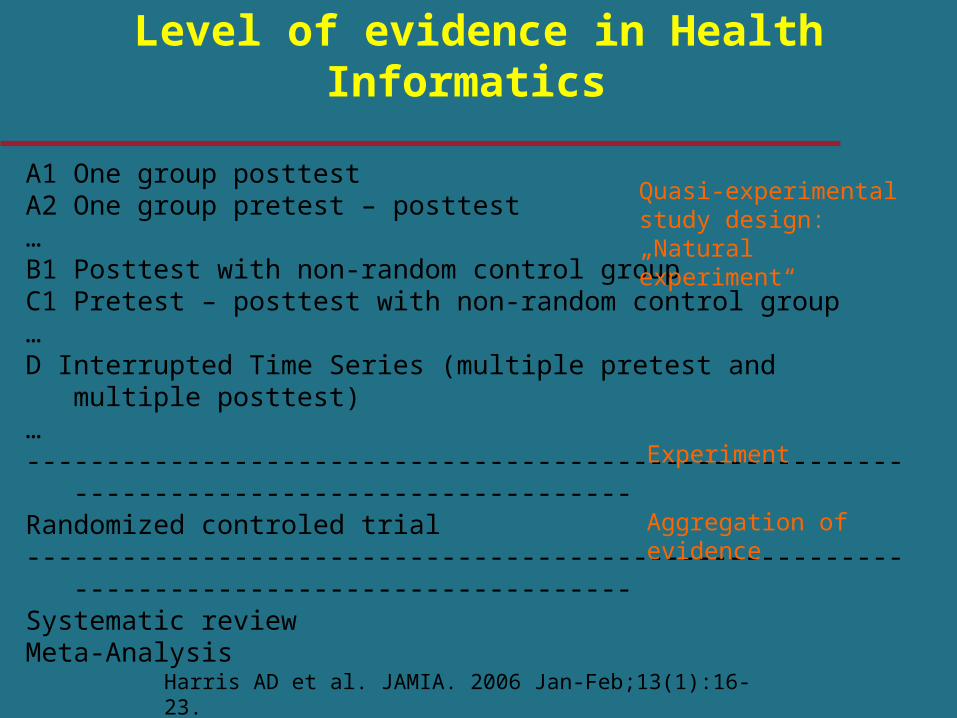
A1 One group posttestA2 One group pretest – posttest…B1 Posttest with non-random control groupC1 Pretest – posttest with non-random control group…D Interrupted Time Series (multiple pretest and multiple posttest)…------------------------------------------------------------------------------------------Randomized controled trial------------------------------------------------------------------------------------------Systematic reviewMeta-Analysis
Level of evidence in Health Informatics
Quasi-experimental study design: „Natural experiment“
Experiment
Aggregation of evidence
Harris AD et al. JAMIA. 2006 Jan-Feb;13(1):16-23.
Problems in RCTs: contamination
Explanation: carry-over from intervention to control groups
Risk factors: if nurses / doctors can apply information (eg. guidelines) to control patients, share information with control staff; cross cover, rotations...
Result: reduce apparent effect (type II error)
Solutions: quantify in a pilot; randomise clusters (clinician, team, hospital…) instead of individual patients
Cluster trials
Problems: Need 30-100% more patients Risk of “unit of analysis” error Analyses more complicated
Problems in RCTs: confounding
Explanation: extra actions in addition to intended intervention
Risk factors: if training, extra support for information resource users
Result: exaggerate apparent effect (type I error)
Solutions: avoid co-intervention; apply it to control group;
Conclusions
Demonstration studies: descriptive, correlational, comparative
RCTs are gold standard for answering effectiveness questions
It may prove difficult or unethical to carry out an RCT; several variant designs may help
Subjectivistic studies: why does(not) it work
Outline
Significance of evaluationProcess of evaluationEvaluation questionsMethods – study design, data collectionTriangulation
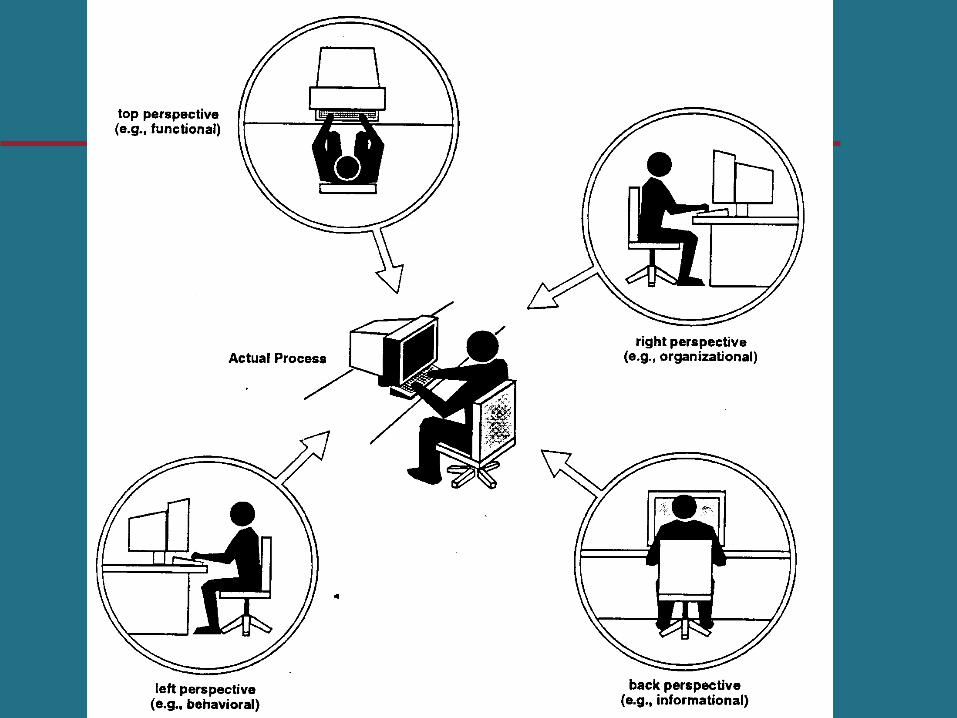
Views
The choice of methods determines which data you will obtain which insight you will be able to get
Broader picture of reality and improved reliability
Triangulation
Evaluation: Multiple employments of Data sources, Observers, Methods, Theories, In investigation of the same phenomenon
Aim: Increasing the completeness of results Validation of results by comparing findings
Triangulation
Data triangulation: Various data sources are used Time: Questionnaires repeated at different times Person: Interviews with various health care professionals
Methods triangulation: Combination of methods for data collection and data analysis (e.g. interviews and observation)
Investigator triangulation: Researchers with different backgrounds take part in study
Evaluation methods: Recommendations
Be aware of the large amount of available methods
Chose adequate methods with regard to your study question.
Consider applying triangulation
• Evaluation is an ethical imperative for health informaticians
DO IT!
• Methods and approaches must be adequatly selected to ensure that the important questions are answered
AND DO IT RIGHT!
Final comments