Embed Size (px)
Citation preview

Evaluation of Therapeutic Methods in High Altitude Pulmonary Edema
EMILIO MARTICORENA, MD, FACC* HERBERT N. HULTGREN, MD, FACC
Stanford and Palo Alto, California Lima and La Oroya, Peru
The effect of treatment with bed rest alone was evaluated in 16 patients with high altitude pulmonary edema of mild to moderate severity at an altitude of 3,750 meters in the Central Peruvian Andes. The results Were compared with those in 20 patients who received conventional therapy including the continuous administration of oxygen and bed rest. A system of grading the severity of high altitude pulmonary edema based on clinical symptoms and signs, radiologic findings and heart rate and respiratory rate was developed. The severity of pulmonary edema as evaluated with the grading system was similar in the •two groups of patients. Treatment With bed rest alone resulted in complete recovery in all • patients over a mean period of 60 hours. NO treatment failure occurred. Similar results were obtained with oxygen therapy combined with bed rest, except that the relief of symptoms was more rapid, the decrease in heart rate and respiratory rate was greater and the recovery period was slightly shorter. High altitude pulmonary edema of mild to moderate severity can be treated successfully with bed rest alone without the administration of oxygen and without moving the patient to a lower altitude. Oxygen therapy is more effective and when available should be used in all cases of high altitude pulmonary edema.
From the Departments of Medicine, Palo Alto Veterans Administration Hospital, Palo Alto and Stanford University School of Medicine, Stanford, California; and the Institute of Andean Biology, San Marcos University, Lima and the Chulec General Hospital, La Oroya, Peru.* This study was sup- ported in part by Veterans Administration Re- search Funds. Manuscript received November 10, 1977; revised manuscript received August 4, 1978, accepted September 1, 1978.
Address for reprints: Herbert N. Hultgren, M.D. Veterans Administration Hospital, 3801 Miranda Avenue, Palo Alto, California 94304.
High altitude pulmonary edema occurs in persons who ascend rapidly to altitudes higher than 2,500 meters. 1,2 Recent studies 3 indicated that the incidence rate of pulmonary edema after an ascent to 3,750 meters is approximately 0.6 percent in persons over 20 years of age and 2.5 percent in those under age 20. Severe episodes occurred more frequently in young subjects (73 percent) than in adults (22 percent). Fatalities occur when the condition is not diagnosed correctly, when prompt de- scent cannot be accomplished or when oxygen is not available. 4,~ The conventional t reatment of high altitude pulmonary edema is removal of the patient to a lower altitude, bed rest and the administration of 100 percent oxygen. 6 Many other methods of t reatment have been used, including the administration of furosemide, morphine, digitalis and corticosteroids. 7,s,9 These methods have not been evaluated properly because most of the studies lack control data and used treatment by bed rest in addition to the administration of a therapeutic agent. No data are available on the effect of bed rest alone in the t reatment of high al- t i tude pulmonary edema. In some circumstances, such as mountain- eering, prompt descent may be impossible, difficult or dangerous, and oxygen may not be available. Thus bed rest may be the only method of therapy available until the patient can be evacuated to a lower altitude or oxygen can be supplied. Therefore this study was performed at an altitude of 3,750 meters to compare two methods of treating high altitude pulmonary edema: bed restalone and bed rest combined with the ad- ministration of oxygen.
February 1979 The American Journal of CARDIOLOGY Volume 43 307
HIGH ALTITUDE PULMONARY EDEMA--MARTICORENA ET AL.
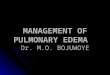
TABLE I
Severity Classification of High Altitude Pulmonary Edema
Grade Clinical Symptoms
Respir- Heart atory Rate Rate
(beats/ (breaths/ rain) rain)
Chest X-ray Film
1. Mild
2. Moderate
3. Serious
4. Severe
Minor symptoms with dyspnea on moderate exertion. May be able to perform light activity.
Symptoms of dyspnea, weakness, fatigue on slight effort. Cannot perform light activity. Headache with cough, dyspnea at rest.
Severe dyspnea, headache, weakness, nausea at rest. Loose recurrent productive cough. Wheezy, difficult respirations with obvious cyanosis.
Clouded consciousness, stupor or coma. Unable to stand or walk. Severe cyanosis. Bubbling rales present with copious sputum, usually bloody. Severe respiratory distress.
<110 <20
110-120 20-30
121-140 31-40
>140 >40
Minor opacities involving less than 1/4 of one lung field.
Opacities involving at least 1/2 of one lung field.
Opacities involving at least 1/2 of each lung field or Unilateral exudate involving all of One lung field.
Bilateral opacities involving more than 1/2 of each lung field.
M e t h o d s and M a t e r i a l s
The study was performed in the Chulec General Hospital in La Oroya, Peru. La Oroya is the center of the mining and smelting operations of the Centromin-Peru corporation in the central Peruvian Andes. The city is located on the Mantaro River at an altitude of 3,750 meters. Of the city's approxi- mately 40,000 inhabitants, about 17 percent are employed by the corporation. La Oroya is easily reached from the sea coast by road or rail in 3 to 5 hours, and families in La Oroya fre- quently travel to lower altitudes for vacations or business purposes. For many years pulmonary edema has been ob- served among newcomers to the high altitude and also in residents who return there after an extended visit at sea level. 4 Excellent medical facilities are available at the Chulec General Hospital, and the staff is experienced in diagnosing and treating high altitude pulmonary edema.
GRADE 1
G R A O E 2 - -
GRADE 3 / /
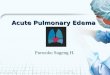
- n FIGURE 1. Diagram of method of assessing the radiologic severity of high altitude pulmonary edema. Grade 1 = 1/4 of lung field occupied by densities.
m
Clinical diagnosis and grading of severity: In this study the diagnosis of high altitude pulmonary edema was based on the following criteria: (1) The onset of typical symptoms, in- cluding Cough and dyspnea at rest, within 3 days after arrival at high altitude either for the f i r s t t ime or after a sea level sojourn of more than 10 days. Patients who had symptoms before arrival at high altitude were excluded. (2)The absence of signs of infection such as nasal discharge, sore throat or significant fever ( temperature greater than 39 ° C). (3) The presence of pulmonary rales and cyanosis. (4) Infiltrate in the chest X-ray film compatible with pulmonary edema.
To determine whether the t rea tment groups had a similar degree of severity of high altitude pulmonary edema, a grading system was used (Table i), based on the following data: (1) the clinical severity of symptoms and signs, (2) heart rate and respiratory rate, and (3) the amount of infiltrate in the chest X-ray film.
The clinical grade was determined by the presence and severity of symptoms such as dyspnea, cough and cyanosis and the degree to which normal activity was impaired by dyspnea, fatigue and clouded mentation.
Heart rate and respiratory rate were used as an additional objective grade of severity because these rates increase in patients with this condition and can be determined easily under field conditions. The heart rate was determined from the resting electrocardiogram, . and the respiratory rate was counted at the bedside for 1 minute. The heart rate grade and the respiratory rate grade were added and divided by 2 to obtain a single grade. For example, if the heart rate was 116 beats/min (grade 2) and the respiratory rate 48 breaths/min (grade 4), the score was (2 + 4)/2 = 3.
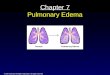
The amount Of infiltrate in the chest X-ray f i lmwas esti- mated by the degree to which the lung fields were involved by patchy or confluent densities (Fig. 1). Chest-films were graded independently by an observer who did not know the patient's name or the clinical details of the illness. Representative ex' amples of four degrees of severity of radiol0gic signs of high altitude pulmonary edema are shown in Figure 2. In each patient the scores were added to obtain a total score of symptom severity. Observations of the clinical findings were repeated at 12 hour intervals. Chest films were obtained at 24 hour intervals.
Patients: Informed consent was obtained from consecutive patients admitted to the hospital with a proved diagnosis of high alt i tude pulmonary edema. For ethical reasons, only patients with pulmonary edema of mild or moderate severity
308 February 1979 The American Journal of CARDIOLOGY Volume 43
HIGH ALTITUDE PULMONARY EDEMA~MARTICORENA ET AL.
. . . . . . . . . . . . . . .
• " • " . . . . . : . . . . . . ' . . . . . . . : : . : , i . . i i : : : : : : : . . . . . . . . . . . . . . . . . . . . . . . . : :.: :,...,.. ,.~.. :~ • . . . . . . : . . ~ ~ . . : . :~ .~ : :~ . . : . ;~
• . : . : . . . . . . . . . : : . : ~ .~ .~ : . ~ :~ .~
. . . • . . .~. : . . : . . .~: : : . . . : : : : : : . : : : . : : . : : : : : :
. . . . . . . . . . : . ~ . : . : . : . : ~ . : . , . : : . ~ : : ~ .~ . . . .
. . . . . . . . . . . :.: . . . . . . . . . . . . :: . . . . .
• " " . : . : " " " : . . . : : ) : . . : ) " " ' : . . . :" ." . . : : i! : : i~ ' i : i~: ,~-: .
~iiii!~?i~ii!}ii!:i!:ii~i~!~ii:i~}~iiiii~:ii:!~iii~:~!!~!ii:}ii~!i~ii::~i~ii:~iii~iiii~:i~i~i~iiii!!~:ii~!:~:~:~:~i~i~::~i~ii!ii!:::~?~::i:i!~:i~i~i~i~:!i!ii~:~:~:i~i~::~:::,~ii~i~iiii~::i!ii~i:~!~!i~!i~i~i!~i~:~i ~ : :~ !~ i~ i~ i i ~ i i : : i i : ~ :~ :~ i~ i~ i i ~ :~ : i i i : : i : i ~ i : : : ! ~ : : i ~ :~ : : i : : : i ~ i ~ :~ :~ i~ :~ :~ i~ :~ :~ i~ : : i ! : : i ~ i : ~ i i i : : i ~ :~ i~ : i i ~ :~ : : i ! : ~ : : ~ :~ i i i i ~ :~ : i : i ` : ~ i ~ :~ :~ :~ :~ :~ i i ~ i ~ : : : ~ :~ i ! : ~ i i i : ~ i : : i i : ~ i ~ ` i : : i : : ~ i ! : : i ~ :~ i : : i ~ :~ i : : : : : : i ~ ` i ~ : : i : i :
~~,~-~-':~%-~:%~;~:~fii:~i!~:~-ii~'ii ~i~i~;ii~i~i!:~i~i:~ii~i~i~!:!~i~i~:ii~i~i:~:iiiiii~i:iii~ii~::~i~i:;~iii~ii~i~i~:~i~ii~ii~ii~]i!i~
• ~ ~:~ ~ : ~ ~ : ~ - ~ : ~ ? ~ ~ : ~ : ~ ~ : ~ : ~ - ~ : ~ , ~ - ~ : ~ : ~ ~ : ~ : ~ : ~ - ~ ~:~ ~ ~ ~ ~ : ~ ~ : ~ : ~ ~ ~ ~ :v~:.::-~:¢:~ ~ : ~ : ~ ~ ~ ~ : ~ ~ ~ ~ - - : ~ : -
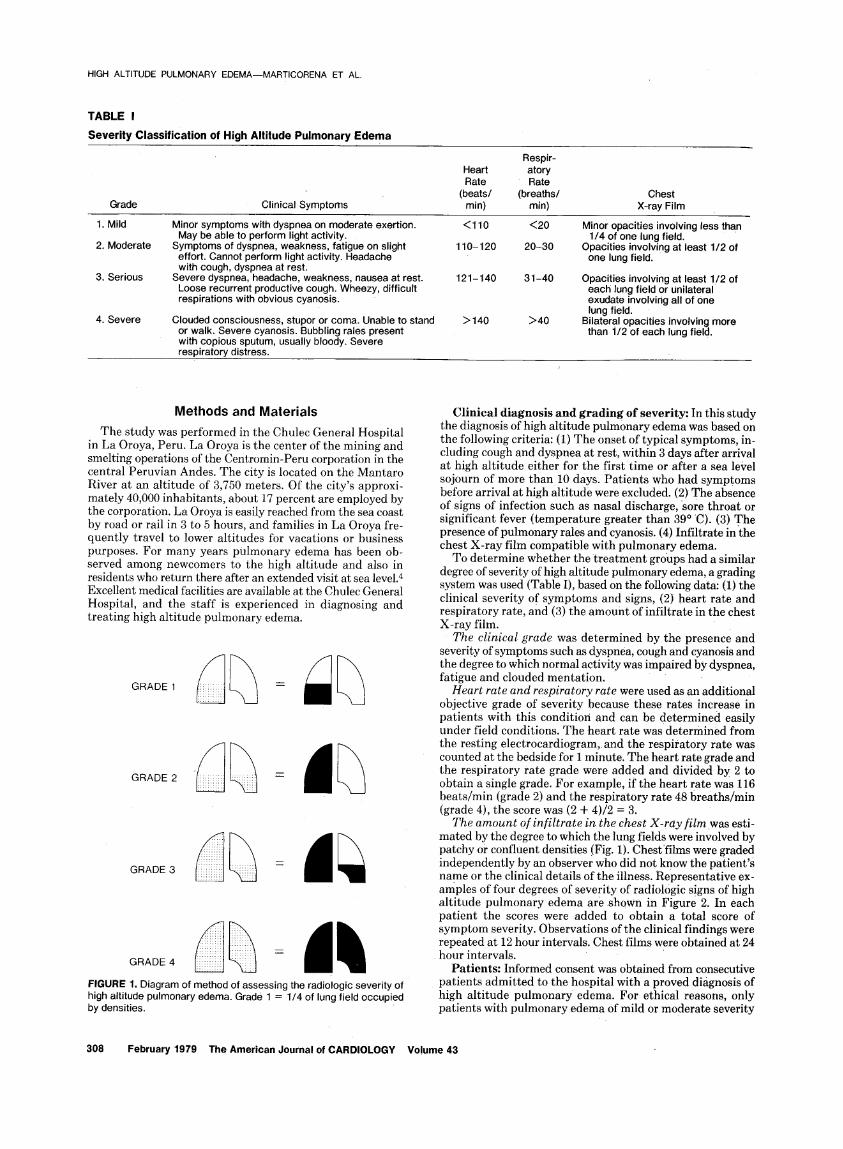
FIGURE 2. Chest films showing four • grades of radiologic severity. A, grade 1. The exudate involves the lower half of the right lung field. The patient was a 30 year old man with moderate symptoms (grade 2). Heart rate was118 beats/min and respiratoryrate 24 breaths/rain. Total severity of symptoms was grade 5. B, grade 2. The exudate involves most of. the right lung field, The heart rate was 120 beats/rain and the respiratory rate 35 breaths/rain. Clinical severity was grade 3 and arterial oxygen saturation 56 percent. Total severity of symptoms was grade 7.5. C, grade 3. The exudate involves 3/4 of the lung fields. The patient was a 17 year old boy with clinically severe symptoms (grade 3). The heart rate was 135 beats/rain and the respiratory rate 35 breaths/min. Total severity of symptoms was grade 9. D, grade 4. There is exudate in all lung fields. Clinical severity wa~, grade 3, heart rate 114 beats/min and respiratory rate 44 breaths/min. Total severity of symptoms was grade 10.
(total scoreof less than 12) were included in the study. Any patient in the bed rest group whose symptoms increased in severity was given oxygen. Fourteen patients declined to enter the study; the severity of pulmonary edema in these patients was similar to that in the study patients. The study period was June 1964 to July 1968. One patient with severe pulmonary edema.was excluded from the study. She was a 52 year old woman who was treated at home by her family without the aid of a physician. On admission to the hospital she was comatose, and she died despite intensive therapy including the admin- istration of oxygen. The autopsy revealed severe pulmonary edema and chronic emphysema but no cardiac disease.
A total of 36 patients was studied. Their mean age was 9.8
years (range 3 to 19, median age 10 years). Twenty-one pa- tients were male and 15 female. All episodes of high altitude pulmonary edema occurred in the vicinity of La Oroya (3,750 meters). The clinical data on both t reatment groups are summarized in Tables II and III.
T r e a t m e n t groups: The methods of t rea tment were as- signed in sequence. Sixteen consecutive patients were treated with bed rest alone. The next 20 consecutive patients were treated with bed rest and oxygen. The two methodsof treat- ment were as follows:
(!) Bed rest and oxygen: Bed rest with lavatory privileges combined with the administration of 100 percent high flow oxygen (6 to 12 liters/min) using a plastic face mask or nasal prongs. In children under age 8 years, oxygen was adminis-
February •1979 The American Journal of CARDIOLOGY Volume 43 309
HIGH ALTITUDE PULMONARY EDEMA--MARTICORENA ET AL.
tered in a small plastic tent covering the upper portion of the bed at a flow rate of 12 liters/min. The oxygen concentration in the tent was approximately 40 percent. Aspirin was given for headache and penicillin was given if coexisting infection was suspected.
(2) Bed rest alone: The above regimen was used but no oxygen was administered,
The effectiveness of therapy was determined with the following evaluations: (i) the relief of symptoms, (2) the change in heart rate and respiratory rate 24 hours after hos' pital entry, and (3) the length of hospitalization.
Patients were discharged from the hospital when these symptoms had disappeared, no rales were detected with auscultation and the pulmonary infiltrate in the chest roentgenogram was completely cleared.
S ta t i s t i ca l methods: For continuous data (means) the independent t test was used to compare the treatments. The Fisher exact test Was used to assess the effect of sex differences between the two groups. When two measurements were available in an individual patient, the paired t test was used to compare the means between time points within each treatment.
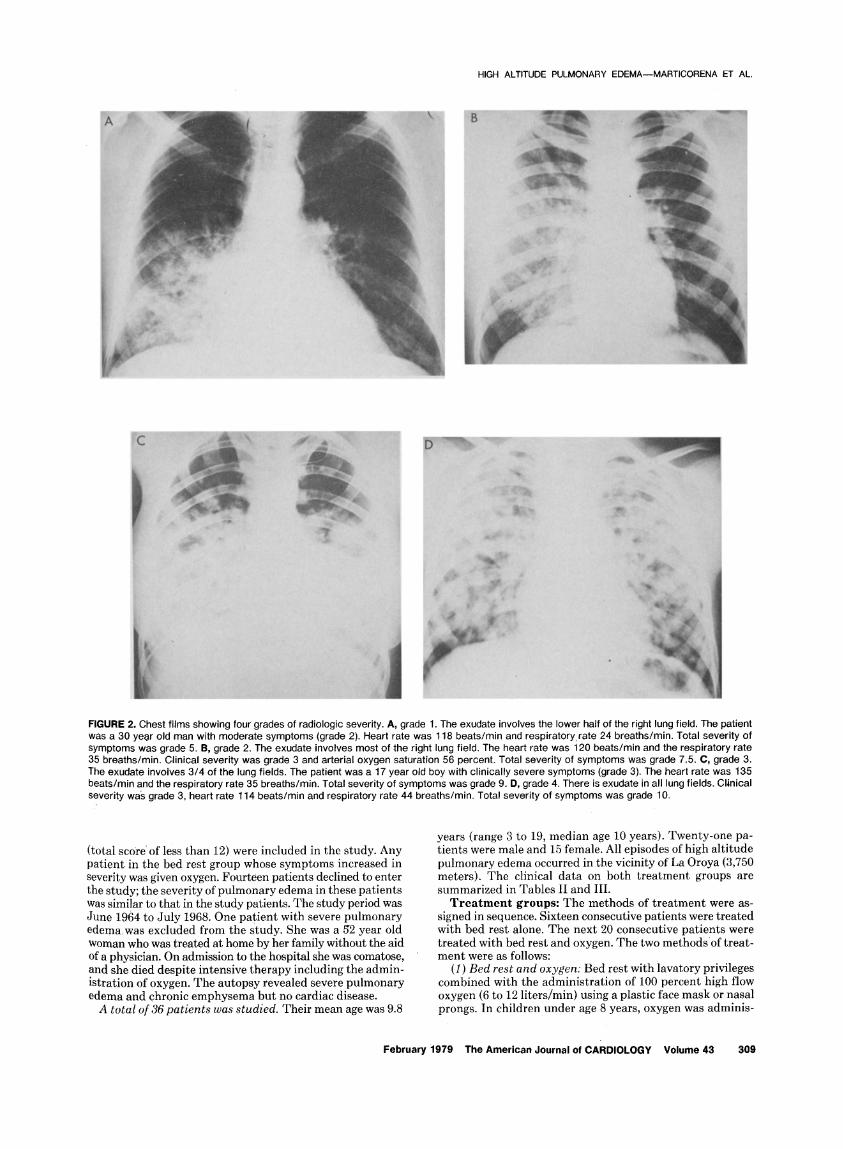
TABLE II
Clinical Data on 16 Patients Treated With Bed Rest Alone
Heart Rate Case Age Hours in (beats/min) no. (yr) Sex Hospital Entry 24 hr*
Chest Respiratory Rate X-ray
(breaths/min) Clinical Film HR-RR Total Entry 24 hr* Grade Grade Grade Grade
1 11 F 48 98 82 2 4 M 44 112 88 3 4 F 26 116 120 4 17 M 173 134 142 5 16 F 70 120 128 6 10 M 53 128 100 7 6 F 64 155 96 8 10 M 48 150 110 9 10 F 50 150 136
10 8 F 48 136 136 11 10 M 50 106 88 12 7 F 45 150 130 13 5 M 69 166 120 14 11 F 42 142 125 15 12 M 44 155 95 16 6 F 92 105 95 Mean 4- 9 ± . . . 60 4- 133 ± 112 ±
SD 3.8 . . . 33.6 21.1 9.9 Median 10 . . . 49.5 135 115
20 20 2 1 1.5 4.5 24 22 2 1 2 5 36 34 2 3 2.5 7.5 43 38 4 , 4 3.5 11.5 36 38 2 3 2.5 7.5 60 24 2 3 3.5 8.5 32 32 2 1 3.5 6.5 32 22 2 2 3.5 7.5 48 24 3 3 4 10 52 30 3 3 3.5 9.5 26 24 1 1 1.5 3.5 56 32 2 2 4 8 52 36 2 2 4 8 32 30 1 1 3.5 5.5 38 22 2 3 3.5 5.5 28 22 2 1 1.5 4.5 38 4- 28 4- 2.1 4- 2.1 -t- 3 ± 7.1 4-
12.1 6.3 0.7 1.0 0.9 2.2 36 27 2 2 3.5 7.5
* Rate 24 hours after entry into the hospital. HR-RR - heart rate-respiratory rate; SD = standard deviation.
TABLE iii
Clinical Data on 20 Patients Treated With Oxygen and Bed Rest
Heart Rate Case Age Hours in (beats/min) no. (yr) Sex Hospital Entry 24 hr*
Chest Respiratory Rate X-ray
(breaths/min t Clinical Film HR-RR Total Entry 24 hr* Grade Grade Grade Grade
1 17 M 50 100 60 2 7 M 74 180 108 3 3 F 48 168 130 4 10 M 60 140 130 5 8 M 32 140 95 6 16 M 49 104 71 7 9 M 12 117 82 8 8 F 24 150 104 9 9 M 24 150 106
10 9 M 42 156 106 11 10 F 8 132 100 12 10 F 78 150 80 13 19 M 106 125 94 14 4 M 27 132 100 15 19 M 67 140 105 16 4 M 48 180 104 17 17 M 58 92 94 18 7 M 34 95 75 19 13 F 113 148 120 20 13 F 65 140 88 Mean 4- 10.6 4- . . . 51 ± 137 4- 98 ±
SD 4.9 . . . 28.0 25.7 18.2 Median 9.5 . . . 48.5 140 100
28 26 1 1 1.5 3.5 80 28 2 3 4 9 32 30 1 1 3.5 5.5 36 26 1 1 3 5 30 18 1 1 2.5 4.5 20 20 2 3 1.5 6,5 34 15 2 2 2.5 6.5 32 26 1 1 3.5 5.5 26 24 1 1 3 5 24 20 1 1 3 5 24 20 1 1 2.5 4.5 56 21 3 3 4 10 32 18 3 1 3 7 48 32 2 1 3.5 6.5 20 18 2 1 2.5 5.5 58 32 2 3 4 9 24 20 2 2 1.5 5.5 30 22 2 1 1.5 4.5 48 20 3 4 4 11 26 20 ,2 1 2.5 8.5 35 4- 23 + 1.8 4- 1.7 -I- 2.9 -I- 6.4 4-
15.3 4.9 0.7 1.0 0.9 2.1 31 20.5 2 1 3 5.5
* Rate 24 hours after entry into the hospital. HR-RR = heart rate -- respiratory rate; SD -- standard deviation.
310 February 1979 The American Journal of CARDIOLOGY Volume 43

HIGH ALTITUDE PULMONARY EDEMA--MARTICORENA ET AL.
TABLE IV
Characteristics, of the Study Groups on Entry into the Study
Bed Bed Rest & Rest Oxygen t P Values
Age Mean 9.2 10.6 0.97 NS SD 3.9 4.9
HR on entry Mean 132.7 137.0 0.59 NS SD 21,1 25.7
RR on entry Mean 38.4 35.4 - 0 , 6 7 NS SD 12.1 15.3
HR-RR Grade Mean 3.0 2.9 - 0 . 4 9 NS SD 0.9 0.9
Clinical grade Mean 2.1 1.8 - 1.57 NS SD 0.7 0.7
Chest X-ray film Mean 2.1 1.7 - 1.07 NS SD 1.0 1.0
Total severity Mean 7.1 6.4 - 0 , 9 2 NS SD 2.2 2.1
Sex Male 7 14 Female 9 6
P* = 0.54, NS
* P (probability) as determined with Fisher's exact test. HR = heart rate; NS = not significant; RR = respiratory rate; SD =
standard deviation.
Results
Comparison of the s tudy groups: At entry the two groups were similar in regard to heart rate, respiratory rate, severity of clinical symptoms and degree of ra- diologic pulmonary edema. The group treated with bed rest alone was younger, had fewer males (44 percent versus 70 percent) a n d h a d a slightly higher clinical, radiologic and total severity grade than the group treated with bed rest and oxygen. The differences were small and, except for sex, not statistically significant (Table IV).
Resul t s of treatment: Symptoms including head- ache, nausea, vomiting, dyspnea and restlessness dis- appeared more rapidly in the patients who received oxyge n . In these patients symptoms were usually re- lieved in 4 to 6 hours after entry into the study, whereas in the other group of patients symptoms were not re- lieved until 12 to 24 hours after entry. The patients who received oxygen had a slightly shorter hospital stay than the patients who did not (Table V). No patient studied had a relapse. The decrease in heart rate was greater in the patients who received oxygen (mean decrease 39 percent) than in those who did not (mean decrease 21 percent, P = <0.01). The decrease in respiratory rate was also greater in the patients who received oxygen (mean decrease 13 percent) than in those who did no t (mean decrease 10 percent), but the differerce was not significant.
DiscuSsion
Poss ible l imitat ions of study: A grading system to classify the severity of high altitude pulmonary edema has not previously been used. The system used in this study has several limitations. Most of the patients were
TABLE V
Effect of Two Methods of Treatment in High Altitude Pulmonary Edema
Bed Bed Rest Between Treatment Rest & Oxygen P value
Heart rate On entry 132.7 137,0 NS 24 hours 111.9 97.6 0.03 Mean decrease 20.8* 39.4" <0.01
Respiratory rate On entry 38.4 35.4 NS 24 hours 28.1 22.8 <0.01 Mean decrease 10.3 12.6 NS
Hours in hospital 60.4 51.0 NS
* Within treatment paired t test, P <0.01. Heart rate and respiratory rate decreased with both treatments. The
decrease in heart rate was significantly greater in the group treated with bed rest and oxygen. The decrease in respiratory rate was about the same in each group; the difference was not significant.
NS = not significant.
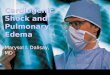
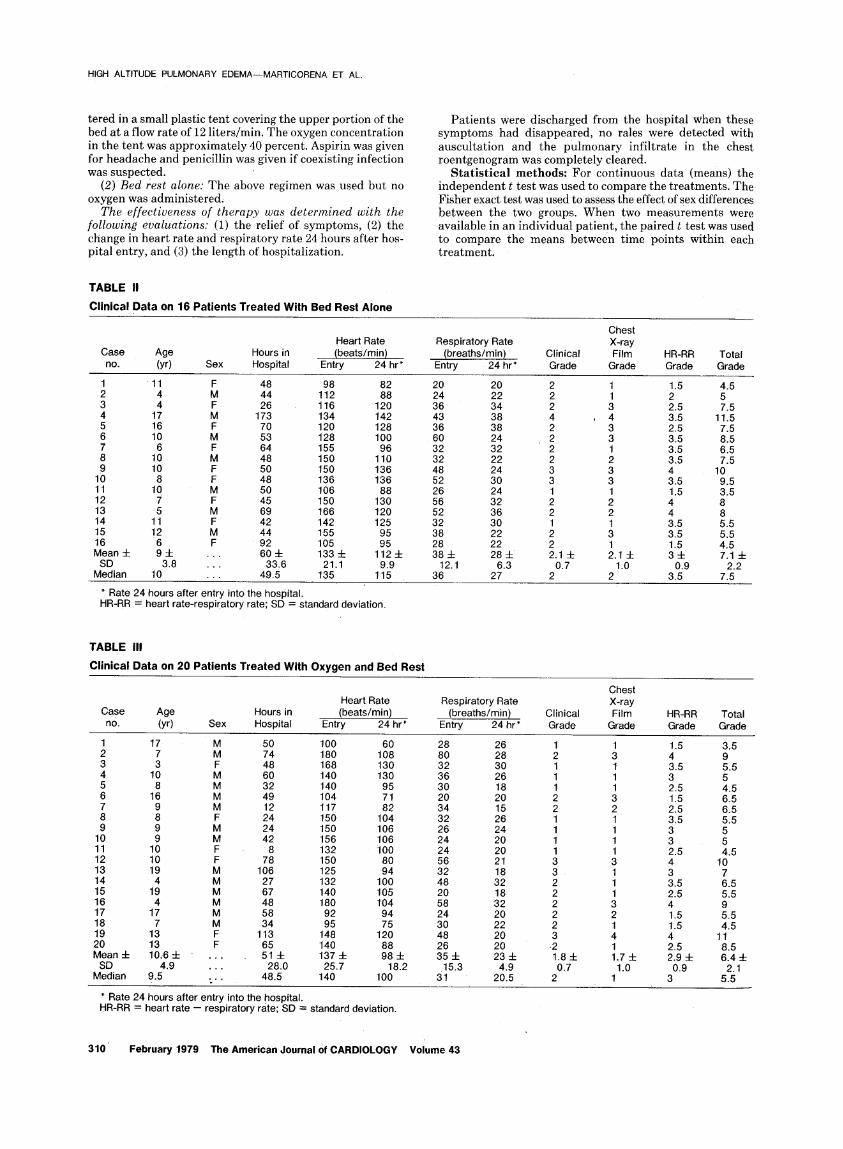
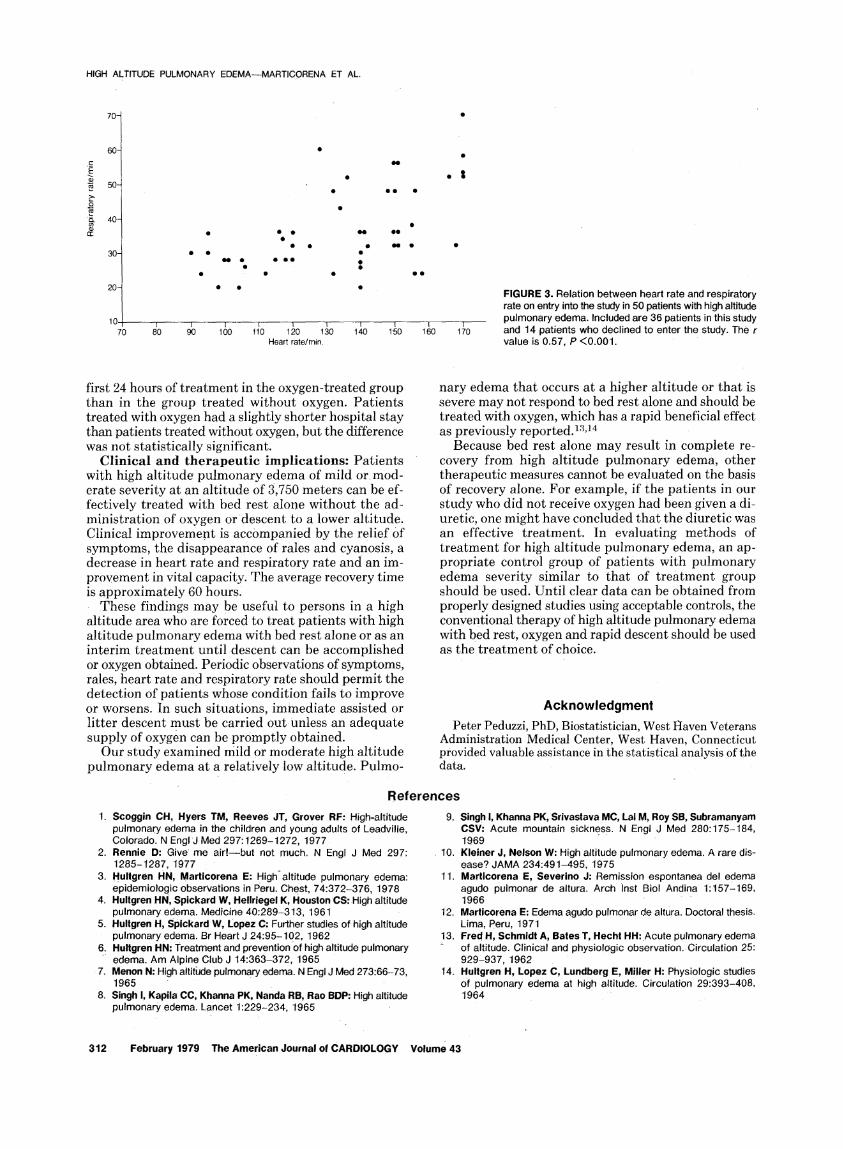
children; clinical signs and symptoms are more difficult to evaluate and heart rates and respiratory rates are higher and more labile in children than in adults. Most of the patients had only mild or moderately severe pulmonary edema, and most were high altitude resi- dents with pulmonary edema that developed after a return from a sojourn at sea level. Although the group treated with bed rest alone included fewer boys, there is no evidence that boys in this age group respond to treatment differently than girls. Heart rate and respi- ratory rate both increase with high altitude pulmonary edema; the relation of these two variables at entry into the study is shown in Figure 3. The r value is +0.47 for the 36 patients studied. The mechanism of the increase in heart rate and respiratory rate is unknown, but hypoxia and altered pulmonary compliance are proba- bly important factors. Arterial oxygen saturation would be an additional useful measure of the severity of pul- monary edema; in severe cases oxygen saturation may fall as low as 57 percent (partial pressure of oxygen 28 mm). 1° Unfortunately, laboratory facilities for the routine determination of blood gases were not available at the hospital during the study period. Despite these limitations, the grading system was useful in classifying the severity of pulmonary edema and in determining that the patients in the two treatment groups had high altitude pulmonary edema of comparable severity.
The grading system of estimating severity should be useful under field conditions when a physician or first aider must decide whether to treat the patient with bed rest or move him to a lower altitude. The System is also useful in evaluating therapeutic measures because it provides an estimate of the severity of high altitude pulmonary edema.
Bed rest versus rest p l u s oxygen: This study demonstrated that bed rest therapy without oxygen resulted in recovery in 16 patients with high altitude pulmonary edema of moderate severity: These data confirm two earlier published reports of similar re- sults, 11,12 The administration of oxygen resulted in a more rapid improvement in symptoms. Hear t ra te and respiratory rate decreased to a greater degree during the
February 1979 The American Journal of CARDIOLOGY Volume 43 311
HIGH ALTITUDE PULMONARY EDEMA--MARTICORENA ET AL.
70-
60-
E 50-
O
• ~. 40- co
n'-
30-
20-
~1} 0 0
• N
1 0 . . . . . . . . . .
~ 0 10 ~0 ' ' 100 110 120 130 1~,0 1"50 Heart rate/min.
f 160
• t
I 170
FIGURE 3. Relation between heart rate and respiratory rate on entry into the study in 50 patients with high altitude pulmonary edema, included are 36 patients in this study and 14 patients who declined to enter the study. The r value is 0.57, P <0.001.
first 24 hours of treatment in the oxygen-treated group than in the group treated without oxygen. Patients treated with oxygen had a slightly shorter hospital stay than patients treated without oxygen, but the difference was not statistically significant.
Cl inical and t h e r a p e u t i c impl ica t ions : Patients with high altitude' pulmonary edema of mild or.mod- erate severity at an altitude of 3,750 meters can be ef- fectively treated with bed rest alone without the ad- ministration of oxygen or descent to a lower altitude. Clinical improvement is accompanied by the relief Of symptoms, the disappearance of rales and cyanosis, a decrease in heart rate and respiratory rate and an im- provement in vital capacity. The average recovery time is approximately 60 hoursl
These findings may be useful to persons in a high altitude area who are forced to treat patients with high altitude pulmonary edema with bed rest alone or as an interim treatment unt i ldescent can be accomplished or oxygen obtained. Periodic observations of symptoms, rales, heart rate and respiratory rate should permit the detection of patients whose condition fails to improve or worsens. In such situations, immediate assisted or litter descent must be carried outunless an adequate supply of oxygen can beprompt ly obtained.
Our study examined mild or moderate high altitude pulmonary edema at a relatively low altitude. Pulmo-
nary edema that occurs at a higher altitude or that is severe may not respond to bed rest alone and should be treated with oxygen, which has a rapid beneficial effect as previously reported. 1~,t4
Because bed rest alone may result in complete re- covery from high altitude pulmonary edema, other therapeutic measures cannot be evaluated on the basis of recovery alone. For example, if the patients in our study who did not receive oxygen had been given a di- uretic, one might have concluded that the diuretic was an effective treatment. In evaluating methods of t reatment for high altitude pulmonary edema, an ap- propriate control group of patients with pulmonary edema severity similar to that of t reatment group should be used. Until clear data can be Obtained from properly designed studies using acceptable controls, the conventional therapy of high altitude pulmonary edema with bed rest, oxygen and rapid descent should be used as the t reatment of choice.
Acknowledgment
Peter Peduzzi, PhD, Biostatistician, West Haven Veterans Administration Medical Center, West Haven, Connecticut provided valuable assistance in the statistical analysis of the data.
References
1. Scoggin CH, Hyers TM, Reeves JT, Grover RF: High-altitude pulmonary edema in the •children and young adults of Leadville, Colorado. N EngiJ Med 297:1269-1272, 1977
2. Rennie D: Give me air!--but not much. N Engl J Med 297: 1285-1287, 1977
3. Hultgren HN, Marticorena E: High-altitude pulmonary edema: epidemiologic observations in Peru. Chest, 74:372-376, 1978
4. Hultgren HN, Spickard W, Hellriegel K, Houston CS: High altitude pulmonary edema. Medicine 40:289-313, 1961
5. Hu!tgren H, Spickard w, Lopez C: Further studies of high altitude pulmonary edema. Br Heart J 24:95-102, 1962
6. Hultgren HN: Treatment and prevention of high altitude pulmonary ' edema. Am Alpine Club J 14:363-372, 1965
• 7. Menon N: High altitiJde pulmonary edema. N Engl J Med 273:66-73, 1965
8. Singh I, Kapila CC, Khanna PK, Nanda RB, Rao BDP: High altitude pulmonary edema. Lancet 1:229-234, 1965
9. Singh I, Khanna PK, Srivastava MC, Lal M, Roy SB, Subramanyam CSV: Acute mountain sickness. N Engl J Med 280:175-184, 1969
10. Kleiner J, Nelson W: High altitude pulmonary edema. A rare dis- ease? JAMA 234:491-495, 1975
11. Marticorena E, Severino J: Remission espontanea del edema agudo pulmonar de altura. Arch inst Biol Andina 1:t57-169, 1966 • .
12. Marticorena E: Edema agudo pulmonar de altura. Doctoral thesis. Lima, Peru, 1971
13. Fred H, Schmidt A, Bates T, Hecht HH:Acute pulmonary edema ° of altitude. Clinical and physiologic observation. Circulation 25:
929"937, 1962 14. Hultgren H, Lopez C, Lundberg E, Miller H: Physiologic studies
of pulmonary edema at high altitude. Circulation 29:393-408, 1964
312 February 1979 The American Journal of CARDIOLOGY Volume 43