Embed Size (px)
Citation preview

Evidence Basis/Outcomes inMinimally Invasive SpinalScoliosis Surgery
Neel Anand, MD, Mch Ortha,*, Eli M. Baron, MDb,Sheila Kahwaty, PA-CcKEYWORDS
� Adult scoliosis � Minimally invasive spine surgery � Evidence basis � Outcomes
KEY POINTS
� Minimally invasive spinal surgery (MISS) scoliosis correction may allow for adult scoliosis correctionwith significantly less tissue destruction and less blood loss than open procedures.
� MISS scoliosis correction without osteotomies has limits using present technologies in terms ofcorrecting sagittal plane deformity and has a ceiling effect of about 40� of coronal Cobb correction.
� MISS scoliosis correction has a different complication profile from traditional open scoliosis correc-tion; this may be largely reflective of the use of the lateral transpsoas approach and reduced bloodloss.
� Long-term level II and III studies are needed to compare outcomes between MISS and open adultscoliosis correction.
INTRODUCTION: NATURE OF THE PROBLEM
The principal goal of adult scoliosis surgery is ob-taining both sagittal and coronal balance of thespine.1 However, traditional scoliosis correctionhas been associated with high-volume blood lossand significant medical complications.2–4 Giventhis situation, minimally invasive spinal surgery(MISS) for the treatment of adult scoliosis is partic-ularly attractive. MISS techniques have been usedfor the treatment of lumbar degenerative scoliosis,iatrogenic scoliosis, and adult idiopathic scoliosis.Theoretically, blood loss can be limited, and med-ical complication rates can possibly be reducedwith less invasive procedures. Nevertheless, clin-ical and radiographic outcomes of MISS scoliosiscorrection need to be comparable with open sur-gery before recommending widespread adoption
a Department of Surgery, Spine Trauma, Spine Center,Boulevard, Suite 800, Los Angeles, CA 90048, USA; b
Sinai Medical Center, 444 South San Vicente Boulc Department of Surgery, Spine Center, Cedars Sinai Me800, Los Angeles, CA 90048, USA* Corresponding author.E-mail address: [email protected]
Neurosurg Clin N Am 25 (2014) 361–375http://dx.doi.org/10.1016/j.nec.2013.12.0141042-3680/14/$ – see front matter � 2014 Elsevier Inc. All
of these techniques for the treatment of adultscoliosis. MISS principles and surgical techniquesused in MISS scoliosis correction are reviewed inthis article, as well as outcomes, complications,and limitations of this rapidly evolving area of spi-nal surgery.
THERAPEUTIC OPTIONS OR SURGICALTECHNIQUE(S)
Indications for adult scoliosis correction includedeformity progression, sagittal or coronal imbal-ance with unremitting back pain, radiculopathy onthe side of the concavity of the curve caused byforaminal stenosis, lumbar hyperlordosis, patientswith a history of flat-back syndrome and backpain, fixed lateral listhesis within the degenerativecurve when motion is present on side-bending
Cedars Sinai Medical Center, 444 South San VicenteDepartment of Neurosurgery, Spine Center, Cedarsevard, Suite 800, Los Angeles, CA 90048, USA;dical Center, 444 South San Vicente Boulevard, Suite
rights reserved. neurosurgery.th
eclinics.com
Anand et al362
films, and when extensive decompressionincluding facetectomy or the violation of the parsis planned.5 A relative indication is progressivelyworsening deformity with pain as the rib cage abutsthe pelvis.In our practice, adult patients who undergo
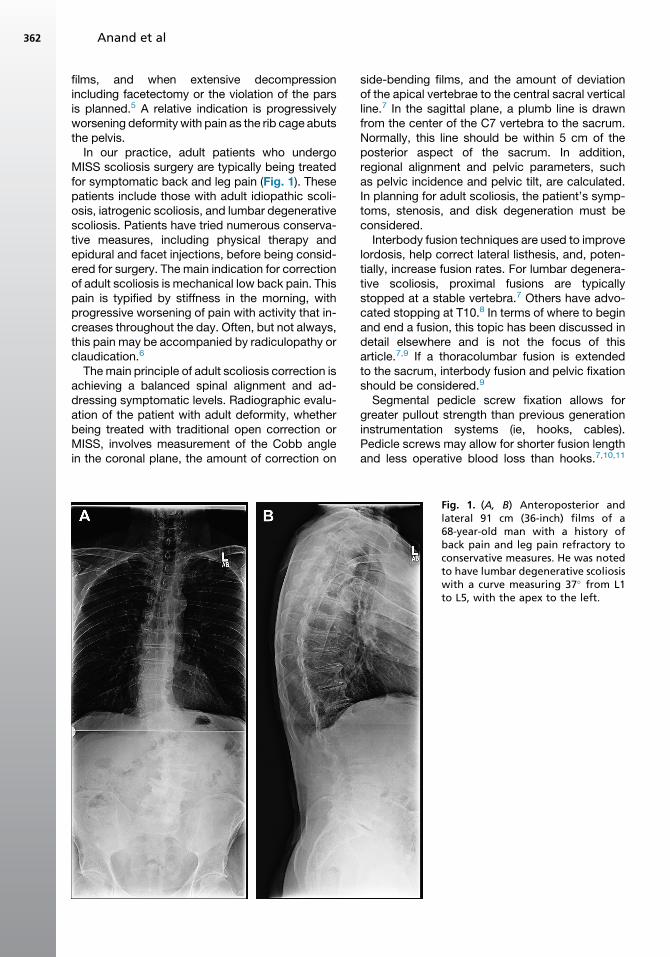
MISS scoliosis surgery are typically being treatedfor symptomatic back and leg pain (Fig. 1). Thesepatients include those with adult idiopathic scoli-osis, iatrogenic scoliosis, and lumbar degenerativescoliosis. Patients have tried numerous conserva-tive measures, including physical therapy andepidural and facet injections, before being consid-ered for surgery. The main indication for correctionof adult scoliosis is mechanical low back pain. Thispain is typified by stiffness in the morning, withprogressive worsening of pain with activity that in-creases throughout the day. Often, but not always,this pain may be accompanied by radiculopathy orclaudication.6
Themain principle of adult scoliosis correction isachieving a balanced spinal alignment and ad-dressing symptomatic levels. Radiographic evalu-ation of the patient with adult deformity, whetherbeing treated with traditional open correction orMISS, involves measurement of the Cobb anglein the coronal plane, the amount of correction on
side-bending films, and the amount of deviationof the apical vertebrae to the central sacral verticalline.7 In the sagittal plane, a plumb line is drawnfrom the center of the C7 vertebra to the sacrum.Normally, this line should be within 5 cm of theposterior aspect of the sacrum. In addition,regional alignment and pelvic parameters, suchas pelvic incidence and pelvic tilt, are calculated.In planning for adult scoliosis, the patient’s symp-toms, stenosis, and disk degeneration must beconsidered.Interbody fusion techniques are used to improve
lordosis, help correct lateral listhesis, and, poten-tially, increase fusion rates. For lumbar degenera-tive scoliosis, proximal fusions are typicallystopped at a stable vertebra.7 Others have advo-cated stopping at T10.8 In terms of where to beginand end a fusion, this topic has been discussed indetail elsewhere and is not the focus of thisarticle.7,9 If a thoracolumbar fusion is extendedto the sacrum, interbody fusion and pelvic fixationshould be considered.9
Segmental pedicle screw fixation allows forgreater pullout strength than previous generationinstrumentation systems (ie, hooks, cables).Pedicle screws may allow for shorter fusion lengthand less operative blood loss than hooks.7,10,11
Fig. 1. (A, B) Anteroposterior andlateral 91 cm (36-inch) films of a68-year-old man with a history ofback pain and leg pain refractory toconservative measures. He was notedto have lumbar degenerative scoliosiswith a curve measuring 37� from L1to L5, with the apex to the left.
MISS Scoliosis Surgery 363
Traditional scoliosis surgery allows for variousopen corrective maneuvers, such as derotation,vertebral coplanar alignment, and in situ rodbending.12–14 In addition, open surgery allows forboth structural interbody techniques and osteoto-mies to assist in further deformity correction, withthe creation of lumbar lordosis as needed.1,7
A systematic review of adult scoliosis surgeryshowed that adult scoliosis surgery is associatedwith long-term improvement in patient radio-graphic and clinical outcomes. At a mean follow-up of 3.6 years, average curve reduction wasnoted to be 40.7% and mean Oswestry DisabilityIndex (ODI) was reduced by 15.7.15 In terms ofscoliosis deformity correction, sagittal balanceimprovement seems to be the strongest predictorof improved clinical outcomes, with correction ofcoronal balance being a lesser factor.16
Open adult scoliosis correction has certain limi-tations. Medical complication rates associatedwith open adult deformity correction may be ashigh as 70%.2 Large volume blood loss is not un-usual in these complex procedures. Seo and col-leagues17 reported outcomes in 152 patientsolder than 20 years undergoing open adult scoli-osis correction. These investigators noted amean blood loss of 2855.8 mL � 1822.9 mL.Transfeldt and colleagues18 noted a mean bloodloss of 1538 mL in patients undergoing full fusionand decompression of their degenerative scolioticcurves. The population undergoing adult scoliosissurgery is often elderly, with significant medicalcomorbidities and high cardiac risk. Given this sit-uation, the decision to proceed operatively withadult surgical deformity correction in the olderpopulation must be made carefully.19 Consideringthese limitations, MISS options may be attractive ifsimilar results can be obtained with less blood lossand less tissue trauma.
MISS Scoliosis Correction
A portion of the morbidity associated with tradi-tional spinal surgery occurs because of muscledamage associated with exposure and retractionand subsequent muscular devascularization anddenervation.20–23 Tubular approaches for diskec-tomy, decompression, and minimally invasive sur-gery posterior fusion were developed to minimizethese complications.24–29 MISS interbody fusiontechniques followed. This was an important devel-opment, because interbody fusion may havehigher fusion rates than posterolateral fusion tech-niques.7,30 In addition, diskectomy and graftplacement may allow the achievement of anteriordeformity release and alignment.31–34 Current op-tions for MISS interbody fusion techniques include
transforaminal lumbar interbody fusion (TLIF), min-iopen and MISS anterior lumbar interbody fusion(ALIF), lateral transpsoas interbody fusion andthe presacral approach for interbody fusion (Axia-LIF) (Table 1). All of these options have subse-quently been used in MISS correction of adultscoliosis.35–41
The combined use of 3 techniques to facilitatecircumferential MISS scoliosis correction was re-ported in 2008.42 These techniques included thetranspsoas approach for diskectomy and inter-body fusion, the presacral approach for L5-S1fusion, and percutaneous pedicle screw and rodplacement. Percutaneous screw and rod place-ment has proved to be a major determinant ofcorrection of apical vertical translation, evenbeyond diskectomy and interbody fusion.6 Subse-quently, other series have reported outcomes us-ing a combination of MISS techniques for adultscoliosis.
Most articles reporting MISS scoliosis correc-tion rely heavily on the lateral transpsoasapproach. This factor allows the surgeon MISS ac-cess to the spine, where diskectomy, deformityrelease, and interbody fusion can be achieved formultiple levels with minimal tissue disruption. Thecurrent technique, as described by Luiz Pimentaand published by Ozgur and colleagues,43 buildson the experience of other historical approachesin which MISS techniques were used to achieveALIF.44–46 The techniques of Thalgott and col-leagues47 and that of McAfee and colleagues48
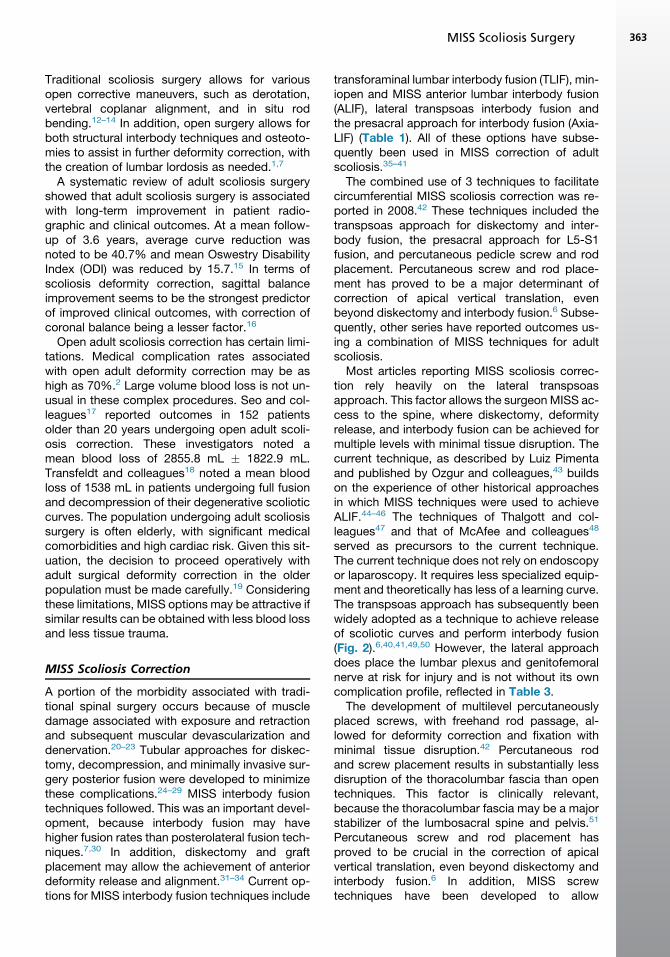
served as precursors to the current technique.The current technique does not rely on endoscopyor laparoscopy. It requires less specialized equip-ment and theoretically has less of a learning curve.The transpsoas approach has subsequently beenwidely adopted as a technique to achieve releaseof scoliotic curves and perform interbody fusion(Fig. 2).6,40,41,49,50 However, the lateral approachdoes place the lumbar plexus and genitofemoralnerve at risk for injury and is not without its owncomplication profile, reflected in Table 3.
The development of multilevel percutaneouslyplaced screws, with freehand rod passage, al-lowed for deformity correction and fixation withminimal tissue disruption.42 Percutaneous rodand screw placement results in substantially lessdisruption of the thoracolumbar fascia than opentechniques. This factor is clinically relevant,because the thoracolumbar fascia may be a majorstabilizer of the lumbosacral spine and pelvis.51
Percutaneous screw and rod placement hasproved to be crucial in the correction of apicalvertical translation, even beyond diskectomy andinterbody fusion.6 In addition, MISS screwtechniques have been developed to allow
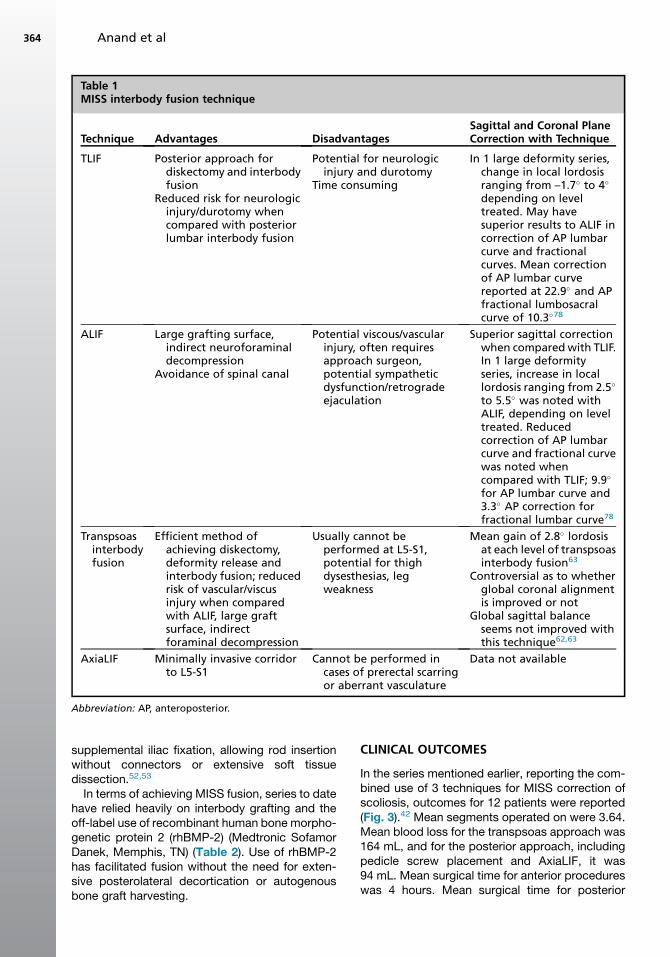
Table 1MISS interbody fusion technique
Technique Advantages DisadvantagesSagittal and Coronal PlaneCorrection with Technique
TLIF Posterior approach fordiskectomy and interbodyfusion
Reduced risk for neurologicinjury/durotomy whencompared with posteriorlumbar interbody fusion
Potential for neurologicinjury and durotomy
Time consuming
In 1 large deformity series,change in local lordosisranging from –1.7� to 4�
depending on leveltreated. May havesuperior results to ALIF incorrection of AP lumbarcurve and fractionalcurves. Mean correctionof AP lumbar curvereported at 22.9� and APfractional lumbosacralcurve of 10.3�78
ALIF Large grafting surface,indirect neuroforaminaldecompression
Avoidance of spinal canal
Potential viscous/vascularinjury, often requiresapproach surgeon,potential sympatheticdysfunction/retrogradeejaculation
Superior sagittal correctionwhen comparedwith TLIF.In 1 large deformityseries, increase in locallordosis ranging from 2.5�
to 5.5� was noted withALIF, depending on leveltreated. Reducedcorrection of AP lumbarcurve and fractional curvewas noted whencompared with TLIF; 9.9�
for AP lumbar curve and3.3� AP correction forfractional lumbar curve78
Transpsoasinterbodyfusion
Efficient method ofachieving diskectomy,deformity release andinterbody fusion; reducedrisk of vascular/viscusinjury when comparedwith ALIF, large graftsurface, indirectforaminal decompression
Usually cannot beperformed at L5-S1,potential for thighdysesthesias, legweakness
Mean gain of 2.8� lordosisat each level of transpsoasinterbody fusion63
Controversial as to whetherglobal coronal alignmentis improved or not
Global sagittal balanceseems not improved withthis technique62,63
AxiaLIF Minimally invasive corridorto L5-S1
Cannot be performed incases of prerectal scarringor aberrant vasculature
Data not available
Abbreviation: AP, anteroposterior.
Anand et al364
supplemental iliac fixation, allowing rod insertionwithout connectors or extensive soft tissuedissection.52,53
In terms of achieving MISS fusion, series to datehave relied heavily on interbody grafting and theoff-label use of recombinant human bone morpho-genetic protein 2 (rhBMP-2) (Medtronic SofamorDanek, Memphis, TN) (Table 2). Use of rhBMP-2has facilitated fusion without the need for exten-sive posterolateral decortication or autogenousbone graft harvesting.
CLINICAL OUTCOMES
In the series mentioned earlier, reporting the com-bined use of 3 techniques for MISS correction ofscoliosis, outcomes for 12 patients were reported(Fig. 3).42 Mean segments operated on were 3.64.Mean blood loss for the transpsoas approach was164 mL, and for the posterior approach, includingpedicle screw placement and AxiaLIF, it was94 mL. Mean surgical time for anterior procedureswas 4 hours. Mean surgical time for posterior
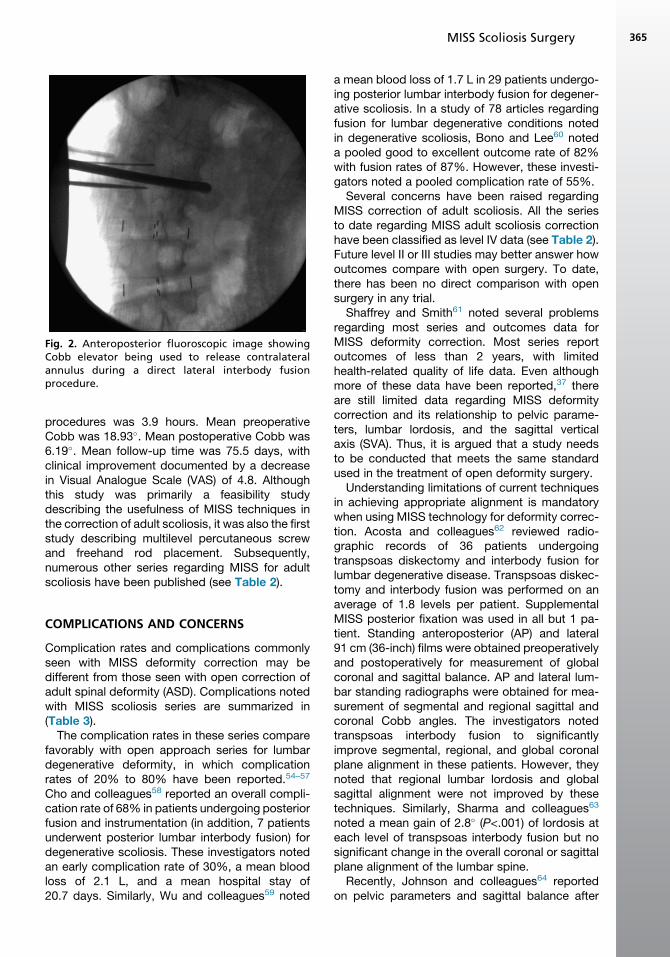
Fig. 2. Anteroposterior fluoroscopic image showingCobb elevator being used to release contralateralannulus during a direct lateral interbody fusionprocedure.
MISS Scoliosis Surgery 365
procedures was 3.9 hours. Mean preoperativeCobb was 18.93�. Mean postoperative Cobb was6.19�. Mean follow-up time was 75.5 days, withclinical improvement documented by a decreasein Visual Analogue Scale (VAS) of 4.8. Althoughthis study was primarily a feasibility studydescribing the usefulness of MISS techniques inthe correction of adult scoliosis, it was also the firststudy describing multilevel percutaneous screwand freehand rod placement. Subsequently,numerous other series regarding MISS for adultscoliosis have been published (see Table 2).
COMPLICATIONS AND CONCERNS
Complication rates and complications commonlyseen with MISS deformity correction may bedifferent from those seen with open correction ofadult spinal deformity (ASD). Complications notedwith MISS scoliosis series are summarized in(Table 3).
The complication rates in these series comparefavorably with open approach series for lumbardegenerative deformity, in which complicationrates of 20% to 80% have been reported.54–57
Cho and colleagues58 reported an overall compli-cation rate of 68% in patients undergoing posteriorfusion and instrumentation (in addition, 7 patientsunderwent posterior lumbar interbody fusion) fordegenerative scoliosis. These investigators notedan early complication rate of 30%, a mean bloodloss of 2.1 L, and a mean hospital stay of20.7 days. Similarly, Wu and colleagues59 noted
a mean blood loss of 1.7 L in 29 patients undergo-ing posterior lumbar interbody fusion for degener-ative scoliosis. In a study of 78 articles regardingfusion for lumbar degenerative conditions notedin degenerative scoliosis, Bono and Lee60 noteda pooled good to excellent outcome rate of 82%with fusion rates of 87%. However, these investi-gators noted a pooled complication rate of 55%.
Several concerns have been raised regardingMISS correction of adult scoliosis. All the seriesto date regarding MISS adult scoliosis correctionhave been classified as level IV data (see Table 2).Future level II or III studies may better answer howoutcomes compare with open surgery. To date,there has been no direct comparison with opensurgery in any trial.
Shaffrey and Smith61 noted several problemsregarding most series and outcomes data forMISS deformity correction. Most series reportoutcomes of less than 2 years, with limitedhealth-related quality of life data. Even althoughmore of these data have been reported,37 thereare still limited data regarding MISS deformitycorrection and its relationship to pelvic parame-ters, lumbar lordosis, and the sagittal verticalaxis (SVA). Thus, it is argued that a study needsto be conducted that meets the same standardused in the treatment of open deformity surgery.
Understanding limitations of current techniquesin achieving appropriate alignment is mandatorywhen using MISS technology for deformity correc-tion. Acosta and colleagues62 reviewed radio-graphic records of 36 patients undergoingtranspsoas diskectomy and interbody fusion forlumbar degenerative disease. Transpsoas diskec-tomy and interbody fusion was performed on anaverage of 1.8 levels per patient. SupplementalMISS posterior fixation was used in all but 1 pa-tient. Standing anteroposterior (AP) and lateral91 cm (36-inch) films were obtained preoperativelyand postoperatively for measurement of globalcoronal and sagittal balance. AP and lateral lum-bar standing radiographs were obtained for mea-surement of segmental and regional sagittal andcoronal Cobb angles. The investigators notedtranspsoas interbody fusion to significantlyimprove segmental, regional, and global coronalplane alignment in these patients. However, theynoted that regional lumbar lordosis and globalsagittal alignment were not improved by thesetechniques. Similarly, Sharma and colleagues63
noted a mean gain of 2.8� (P<.001) of lordosis ateach level of transpsoas interbody fusion but nosignificant change in the overall coronal or sagittalplane alignment of the lumbar spine.
Recently, Johnson and colleagues64 reportedon pelvic parameters and sagittal balance after
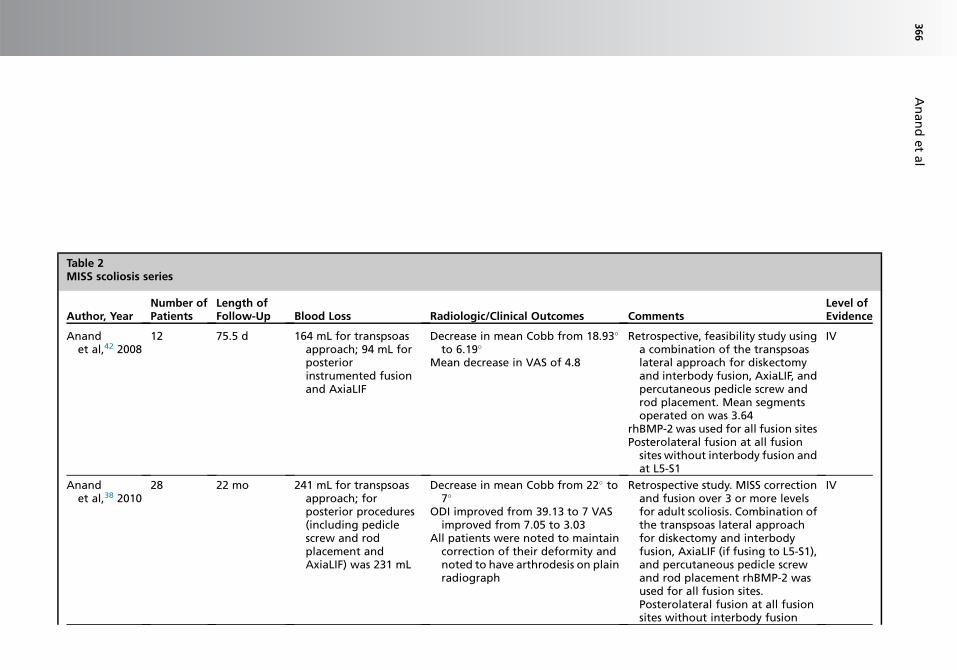
Table 2MISS scoliosis series
Author, YearNumber ofPatients
Length ofFollow-Up Blood Loss Radiologic/Clinical Outcomes Comments
Level ofEvidence
Anandet al,42 2008
12 75.5 d 164 mL for transpsoasapproach; 94 mL forposteriorinstrumented fusionand AxiaLIF
Decrease in mean Cobb from 18.93�
to 6.19�
Mean decrease in VAS of 4.8
Retrospective, feasibility study usinga combination of the transpsoaslateral approach for diskectomyand interbody fusion, AxiaLIF, andpercutaneous pedicle screw androd placement. Mean segmentsoperated on was 3.64
rhBMP-2 was used for all fusion sitesPosterolateral fusion at all fusionsites without interbody fusion andat L5-S1
IV
Anandet al,38 2010
28 22 mo 241 mL for transpsoasapproach; forposterior procedures(including pediclescrew and rodplacement andAxiaLIF) was 231 mL
Decrease in mean Cobb from 22� to7�
ODI improved from 39.13 to 7 VASimproved from 7.05 to 3.03
All patients were noted to maintaincorrection of their deformity andnoted to have arthrodesis on plainradiograph
Retrospective study. MISS correctionand fusion over 3 or more levelsfor adult scoliosis. Combination ofthe transpsoas lateral approachfor diskectomy and interbodyfusion, AxiaLIF (if fusing to L5-S1),and percutaneous pedicle screwand rod placement rhBMP-2 wasused for all fusion sites.Posterolateral fusion at all fusionsites without interbody fusion
IV
Anandetal
366
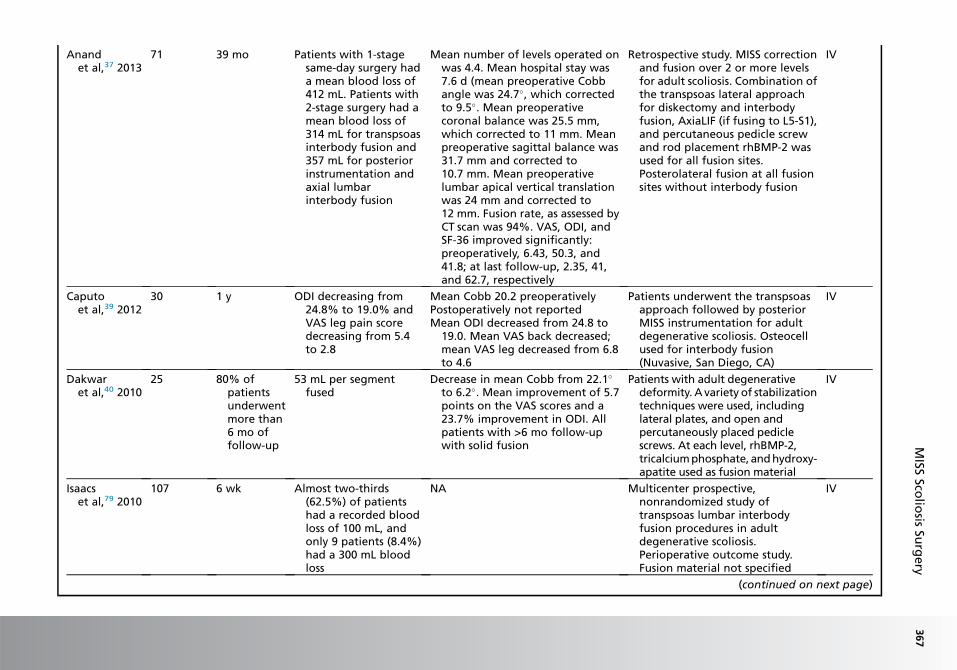
Anandet al,37 2013
71 39 mo Patients with 1-stagesame-day surgery hada mean blood loss of412 mL. Patients with2-stage surgery had amean blood loss of314 mL for transpsoasinterbody fusion and357 mL for posteriorinstrumentation andaxial lumbarinterbody fusion
Mean number of levels operated onwas 4.4. Mean hospital stay was7.6 d (mean preoperative Cobbangle was 24.7�, which correctedto 9.5�. Mean preoperativecoronal balance was 25.5 mm,which corrected to 11 mm. Meanpreoperative sagittal balance was31.7 mm and corrected to10.7 mm. Mean preoperativelumbar apical vertical translationwas 24 mm and corrected to12 mm. Fusion rate, as assessed byCT scan was 94%. VAS, ODI, andSF-36 improved significantly:preoperatively, 6.43, 50.3, and41.8; at last follow-up, 2.35, 41,and 62.7, respectively
Retrospective study. MISS correctionand fusion over 2 or more levelsfor adult scoliosis. Combination ofthe transpsoas lateral approachfor diskectomy and interbodyfusion, AxiaLIF (if fusing to L5-S1),and percutaneous pedicle screwand rod placement rhBMP-2 wasused for all fusion sites.Posterolateral fusion at all fusionsites without interbody fusion
IV
Caputoet al,39 2012
30 1 y ODI decreasing from24.8% to 19.0% andVAS leg pain scoredecreasing from 5.4to 2.8
Mean Cobb 20.2 preoperativelyPostoperatively not reportedMean ODI decreased from 24.8 to
19.0. Mean VAS back decreased;mean VAS leg decreased from 6.8to 4.6
Patients underwent the transpsoasapproach followed by posteriorMISS instrumentation for adultdegenerative scoliosis. Osteocellused for interbody fusion(Nuvasive, San Diego, CA)
IV
Dakwaret al,40 2010
25 80% ofpatientsunderwentmore than6 mo offollow-up
53 mL per segmentfused
Decrease in mean Cobb from 22.1�
to 6.2�. Mean improvement of 5.7points on the VAS scores and a23.7% improvement in ODI. Allpatients with >6 mo follow-upwith solid fusion
Patients with adult degenerativedeformity. Avariety of stabilizationtechniques were used, includinglateral plates, and open andpercutaneously placed pediclescrews. At each level, rhBMP-2,tricalciumphosphate, andhydroxy-apatite used as fusion material
IV
Isaacset al,79 2010
107 6 wk Almost two-thirds(62.5%) of patientshad a recorded bloodloss of 100 mL, andonly 9 patients (8.4%)had a 300 mL bloodloss
NA Multicenter prospective,nonrandomized study oftranspsoas lumbar interbodyfusion procedures in adultdegenerative scoliosis.Perioperative outcome study.Fusion material not specified
IV
(continued on next page)
MISS
Scolio
sisSu
rgery
367
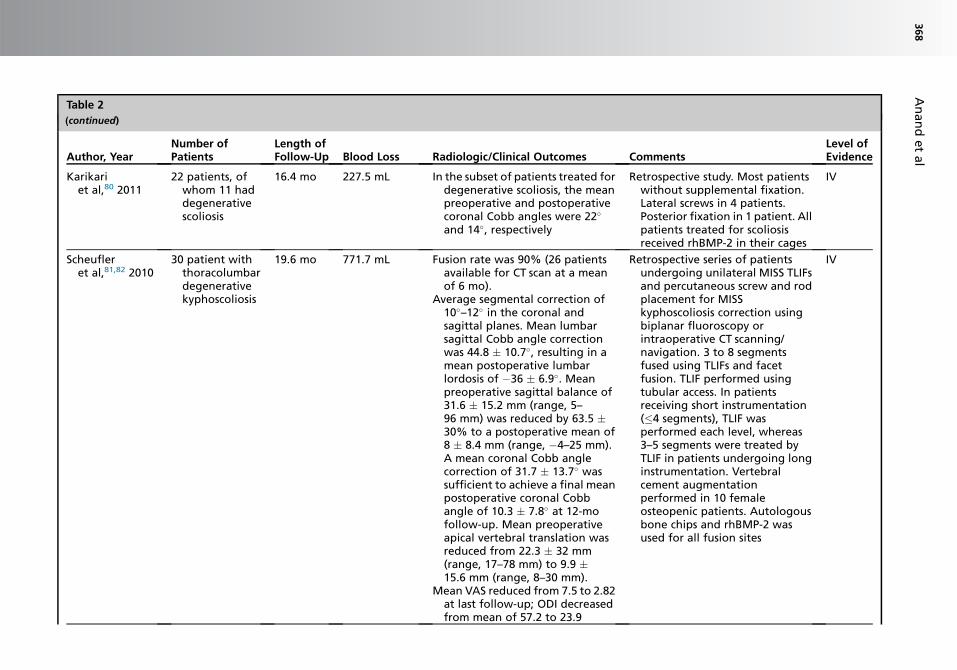
Table 2
(continued)
Author, YearNumber ofPatients
Length ofFollow-Up Blood Loss Radiologic/Clinical Outcomes Comments
Level ofEvidence
Karikariet al,80 2011
22 patients, ofwhom 11 haddegenerativescoliosis
16.4 mo 227.5 mL In the subset of patients treated fordegenerative scoliosis, the meanpreoperative and postoperativecoronal Cobb angles were 22�
and 14�, respectively
Retrospective study. Most patientswithout supplemental fixation.Lateral screws in 4 patients.Posterior fixation in 1 patient. Allpatients treated for scoliosisreceived rhBMP-2 in their cages
IV
Scheufleret al,81,82 2010
30 patient withthoracolumbardegenerativekyphoscoliosis
19.6 mo 771.7 mL Fusion rate was 90% (26 patientsavailable for CT scan at a meanof 6 mo).
Average segmental correction of10�–12� in the coronal andsagittal planes. Mean lumbarsagittal Cobb angle correctionwas 44.8 � 10.7�, resulting in amean postoperative lumbarlordosis of �36 � 6.9�. Meanpreoperative sagittal balance of31.6 � 15.2 mm (range, 5–96 mm) was reduced by 63.5 �30% to a postoperative mean of8 � 8.4 mm (range, �4–25 mm).A mean coronal Cobb anglecorrection of 31.7 � 13.7� wassufficient to achieve a final meanpostoperative coronal Cobbangle of 10.3 � 7.8� at 12-mofollow-up. Mean preoperativeapical vertebral translation wasreduced from 22.3 � 32 mm(range, 17–78 mm) to 9.9 �15.6 mm (range, 8–30 mm).
Mean VAS reduced from 7.5 to 2.82at last follow-up; ODI decreasedfrom mean of 57.2 to 23.9
Retrospective series of patientsundergoing unilateral MISS TLIFsand percutaneous screw and rodplacement for MISSkyphoscoliosis correction usingbiplanar fluoroscopy orintraoperative CT scanning/navigation. 3 to 8 segmentsfused using TLIFs and facetfusion. TLIF performed usingtubular access. In patientsreceiving short instrumentation(�4 segments), TLIF wasperformed each level, whereas3–5 segments were treated byTLIF in patients undergoing longinstrumentation. Vertebralcement augmentationperformed in 10 femaleosteopenic patients. Autologousbone chips and rhBMP-2 wasused for all fusion sites
IV
Anandetal
368
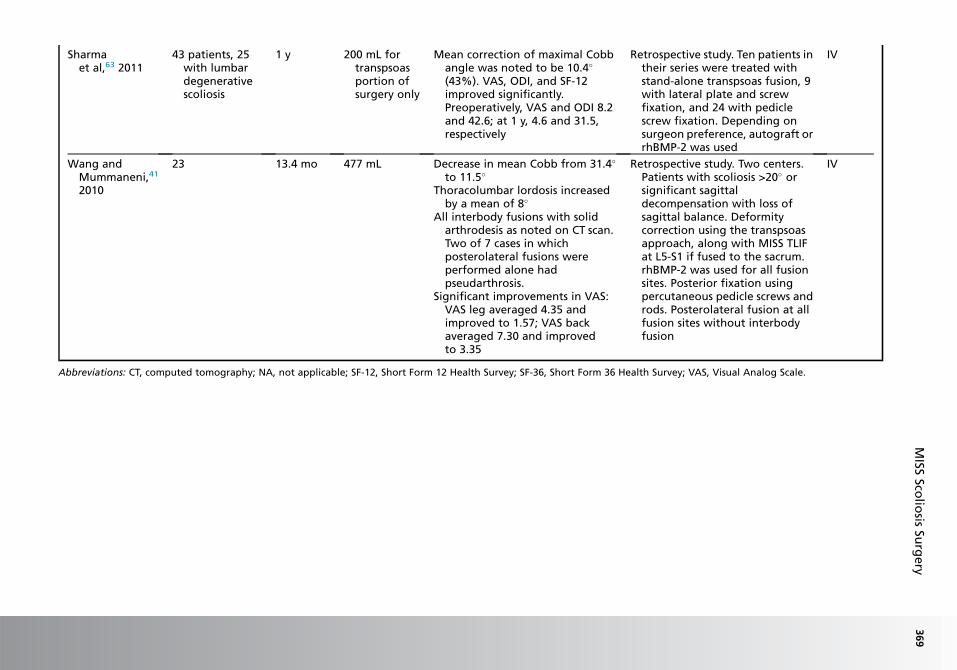
Sharmaet al,63 2011
43 patients, 25with lumbardegenerativescoliosis
1 y 200 mL fortranspsoasportion ofsurgery only
Mean correction of maximal Cobbangle was noted to be 10.4�
(43%). VAS, ODI, and SF-12improved significantly.Preoperatively, VAS and ODI 8.2and 42.6; at 1 y, 4.6 and 31.5,respectively
Retrospective study. Ten patients intheir series were treated withstand-alone transpsoas fusion, 9with lateral plate and screwfixation, and 24 with pediclescrew fixation. Depending onsurgeon preference, autograft orrhBMP-2 was used
IV
Wang andMummaneni,41
2010
23 13.4 mo 477 mL Decrease in mean Cobb from 31.4�
to 11.5�
Thoracolumbar lordosis increasedby a mean of 8�
All interbody fusions with solidarthrodesis as noted on CT scan.Two of 7 cases in whichposterolateral fusions wereperformed alone hadpseudarthrosis.
Significant improvements in VAS:VAS leg averaged 4.35 andimproved to 1.57; VAS backaveraged 7.30 and improvedto 3.35
Retrospective study. Two centers.Patients with scoliosis >20� orsignificant sagittaldecompensation with loss ofsagittal balance. Deformitycorrection using the transpsoasapproach, along with MISS TLIFat L5-S1 if fused to the sacrum.rhBMP-2 was used for all fusionsites. Posterior fixation usingpercutaneous pedicle screws androds. Posterolateral fusion at allfusion sites without interbodyfusion
IV
Abbreviations: CT, computed tomography; NA, not applicable; SF-12, Short Form 12 Health Survey; SF-36, Short Form 36 Health Survey; VAS, Visual Analog Scale.
MISS
Scolio
sisSu
rgery
369
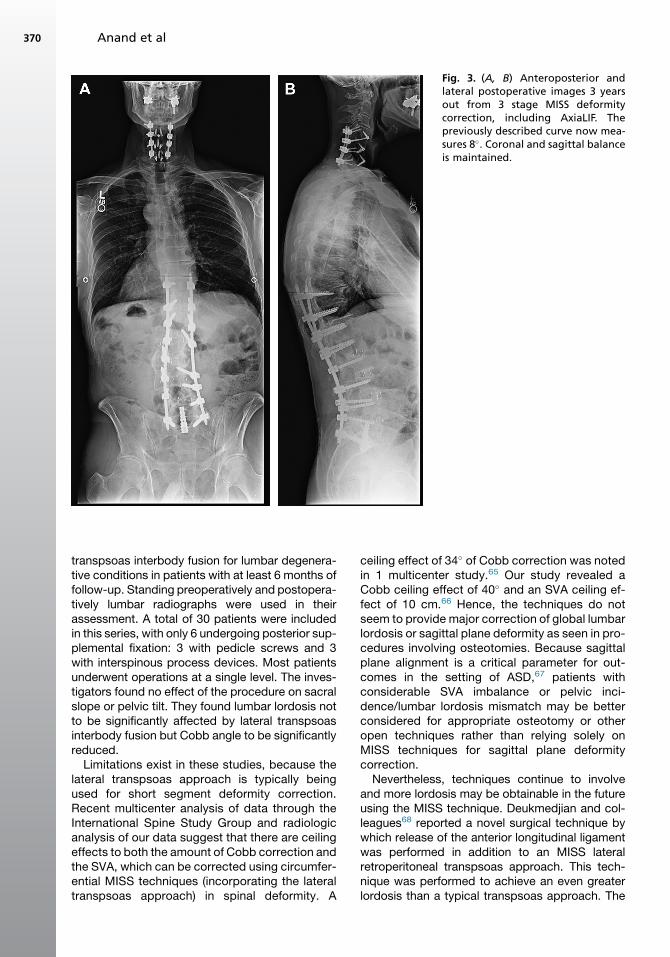
Fig. 3. (A, B) Anteroposterior andlateral postoperative images 3 yearsout from 3 stage MISS deformitycorrection, including AxiaLIF. Thepreviously described curve now mea-sures 8�. Coronal and sagittal balanceis maintained.
Anand et al370
transpsoas interbody fusion for lumbar degenera-tive conditions in patients with at least 6 months offollow-up. Standing preoperatively and postopera-tively lumbar radiographs were used in theirassessment. A total of 30 patients were includedin this series, with only 6 undergoing posterior sup-plemental fixation: 3 with pedicle screws and 3with interspinous process devices. Most patientsunderwent operations at a single level. The inves-tigators found no effect of the procedure on sacralslope or pelvic tilt. They found lumbar lordosis notto be significantly affected by lateral transpsoasinterbody fusion but Cobb angle to be significantlyreduced.Limitations exist in these studies, because the
lateral transpsoas approach is typically beingused for short segment deformity correction.Recent multicenter analysis of data through theInternational Spine Study Group and radiologicanalysis of our data suggest that there are ceilingeffects to both the amount of Cobb correction andthe SVA, which can be corrected using circumfer-ential MISS techniques (incorporating the lateraltranspsoas approach) in spinal deformity. A
ceiling effect of 34� of Cobb correction was notedin 1 multicenter study.65 Our study revealed aCobb ceiling effect of 40� and an SVA ceiling ef-fect of 10 cm.66 Hence, the techniques do notseem to provide major correction of global lumbarlordosis or sagittal plane deformity as seen in pro-cedures involving osteotomies. Because sagittalplane alignment is a critical parameter for out-comes in the setting of ASD,67 patients withconsiderable SVA imbalance or pelvic inci-dence/lumbar lordosis mismatch may be betterconsidered for appropriate osteotomy or otheropen techniques rather than relying solely onMISS techniques for sagittal plane deformitycorrection.Nevertheless, techniques continue to involve
and more lordosis may be obtainable in the futureusing the MISS technique. Deukmedjian and col-leagues68 reported a novel surgical technique bywhich release of the anterior longitudinal ligamentwas performed in addition to an MISS lateralretroperitoneal transpsoas approach. This tech-nique was performed to achieve an even greaterlordosis than a typical transpsoas approach. The
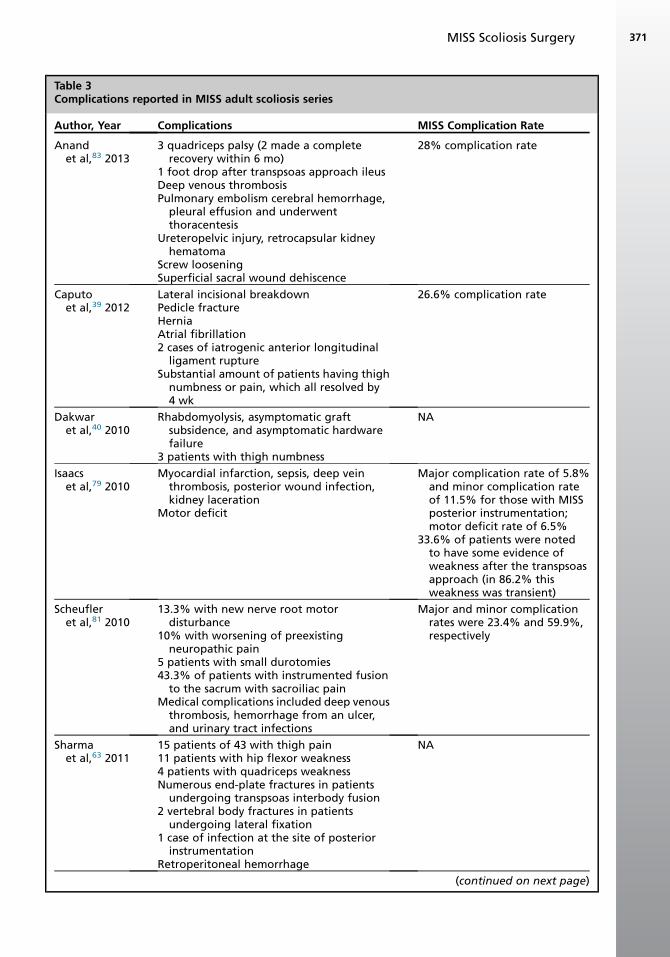
Table 3Complications reported in MISS adult scoliosis series
Author, Year Complications MISS Complication Rate
Anandet al,83 2013
3 quadriceps palsy (2 made a completerecovery within 6 mo)
1 foot drop after transpsoas approach ileusDeep venous thrombosisPulmonary embolism cerebral hemorrhage,
pleural effusion and underwentthoracentesis
Ureteropelvic injury, retrocapsular kidneyhematoma
Screw looseningSuperficial sacral wound dehiscence
28% complication rate
Caputoet al,39 2012
Lateral incisional breakdownPedicle fractureHerniaAtrial fibrillation2 cases of iatrogenic anterior longitudinal
ligament ruptureSubstantial amount of patients having thigh
numbness or pain, which all resolved by4 wk
26.6% complication rate
Dakwaret al,40 2010
Rhabdomyolysis, asymptomatic graftsubsidence, and asymptomatic hardwarefailure
3 patients with thigh numbness
NA
Isaacset al,79 2010
Myocardial infarction, sepsis, deep veinthrombosis, posterior wound infection,kidney laceration
Motor deficit
Major complication rate of 5.8%and minor complication rateof 11.5% for those with MISSposterior instrumentation;motor deficit rate of 6.5%
33.6% of patients were notedto have some evidence ofweakness after the transpsoasapproach (in 86.2% thisweakness was transient)
Scheufleret al,81 2010
13.3% with new nerve root motordisturbance
10% with worsening of preexistingneuropathic pain
5 patients with small durotomies43.3% of patients with instrumented fusion
to the sacrum with sacroiliac painMedical complications included deep venous
thrombosis, hemorrhage from an ulcer,and urinary tract infections
Major and minor complicationrates were 23.4% and 59.9%,respectively
Sharmaet al,63 2011
15 patients of 43 with thigh pain11 patients with hip flexor weakness4 patients with quadriceps weaknessNumerous end-plate fractures in patients
undergoing transpsoas interbody fusion2 vertebral body fractures in patients
undergoing lateral fixation1 case of infection at the site of posterior
instrumentationRetroperitoneal hemorrhage
NA
(continued on next page)
MISS Scoliosis Surgery 371

Table 3
(continued)
Author, Year Complications MISS Complication Rate
Tormentiet al,49 2010
2 cases of motor weakness; 1 transientCecal perforation
NA75% of patients to have thighparesthesias or dysesthesias
Wang &Mummaneni,41
2010
Thigh numbness, pain, and weakness in 30.4%of patients undergoing the transpsoasapproach, on the same side of the approach
Cerebrospinal fluid leakage Hardware pulloutPneumothoraxOne case of significant blood loss
NA
Abbreviation: NA, not applicable.
Anand et al372
investigators reported good results in 7 patients, inwhom they noted an increase in global lumbarlordosis of 24�, segmental lordosis of 17� per levelof anterior longitudinal ligament release, and adecrease in pelvic tilt of 7�. They also noted adecrease in SVA of 4.9 cm. They noted that a mini-mally invasive lateral retroperitoneal transpsoasapproach in addition to release of the anterior lon-gitudinal ligament might be a feasible alternative incorrecting sagittal plane deformity. Wang andMadhavan69 reported using an MISS techniquein association with a miniopen approach for per-formance of pedicle subtraction osteotomy. Theseinvestigators described the technique as an evolu-tion of minimally invasive techniques now beingused for the treatment of fixed sagittal imbalance.Similarly, Wang70 described using a hybrid MISSapproach for deformity correction with goodlordosis restoration using a combination of unilat-eral multilevel facet osteotomies, TLIF, expand-able cages, and percutaneous screw/rodinstrumentation.From our experience, we advise in addition
against using these techniques in their presentform in cases of truly rigid scoliosis, for curvesgreater than 100� in magnitude, and for congenitaland neuromuscular deformities. Osteoporosiswith a T-score of less than –2.0 is also acontraindication.6
Other criticisms of MISS techniques in general,but specifically for deformity correction, include alarger learning curve than for open techniques,the need for specialized equipment, disorientationof the surgeon, and increased radiation expo-sure.26,71–73 With proper training and experience,the disadvantages of learning curve and equip-ment investment are reduced with time. Disorien-tation may be an issue with certain deformities,especially with suboptimal imaging or poor bonedensity. Surgeon radiation exposure remains a
serious concern regarding these procedures.When a technique is performed properly, adheringto radiation safety guidelines, many of these pro-cedures can be performed yearly withoutexceeding occupational dose limits.74 In addition,neuronavigation may be useful in increasing sur-geon accuracy with instrumentation placementand reducing radiation exposure.75–77
SUMMARY
MISS scoliosis surgical correction continues toevolve, and its use has increased in recent years.Theoretic advantages of these techniques overopen procedures include reduced blood loss,potentially reduced complication rates, andreduced tissue trauma. These techniques may beuseful in their present form when up to 40� of coro-nal Cobb correction is desired and with fixedsagittal imbalance less than 10 cm. Questionsremainas to thedurability of the resultsand towhichdeformities are better served with open correctionmethods. Although long-term follow-up has beenreported, more data are necessary to ensure thatthe results are comparable in the long-term withopen deformity correction. Future level II or IIIstudies should be designed to help answer whatis the role of MISS technologies in the setting ofscoliosis when compared with the open technique.
REFERENCES
1. Heary RF. Evaluation and treatment of adult spinal
deformity. Invited submission from the Joint Section
Meeting on Disorders of the Spine and Peripheral
Nerves, March 2004. J Neurosurg Spine 2004;
1(1):9–18.
2. Baron EM, Albert TJ. Medical complications of sur-
gical treatment of adult spinal deformity and how to
avoid them. Spine 2006;31(Suppl 19):S106–18.
MISS Scoliosis Surgery 373
3. Hu SS. Blood loss in adult spinal surgery. Eur Spine
J 2004;13(Suppl 1):S3–5.
4. Moller H, Hedlund R. Instrumented and noninstru-
mented posterolateral fusion in adult spondylolis-
thesis–a prospective randomized study: part 2.
Spine 2000;25(13):1716–21.
5. Herkowitz HN, Sidhu KS. Lumbar spine fusion in
the treatment of degenerative conditions: current
indications and recommendations. J Am Acad Or-
thop Surg 1995;3(3):123–35.
6. Anand N, Baron EM. Minimally invasive ap-
proaches for the correction of adult spinal defor-
mity. Eur Spine J 2013;22(Suppl 2):S232–41.
7. Mok JM, Hu SS. Surgical strategies and choosing
levels for spinal deformity: how high, how low, front
and back. Neurosurg Clin North Am 2007;18(2):
329–37.
8. ShufflebargerH, Suk SI,Mardjetko S. Debate: deter-
mining the upper instrumented vertebra in the man-
agement of adult degenerative scoliosis: stopping
at T10 versus L1. Spine 2006;31(Suppl 19):
S185–94.
9. Bridwell KH. Selection of instrumentation and
fusion levels for scoliosis: where to start and where
to stop. Invited submission from the Joint Section
Meeting on Disorders of the Spine and Peripheral
Nerves, March 2004. J Neurosurg Spine 2004;
1(1):1–8.
10. Kim YJ, Lenke LG, Cho SK, et al. Comparative
analysis of pedicle screw versus hook instrumenta-
tion in posterior spinal fusion of adolescent idio-
pathic scoliosis. Spine (Phila Pa 1976) 2004;
29(18):2040–8.
11. Liljenqvist U, Lepsien U, Hackenberg L, et al.
Comparative analysis of pedicle screw and hook
instrumentation in posterior correction and fusion
of idiopathic thoracic scoliosis. Eur Spine J 2002;
11(4):336–43.
12. Cheng I, Hay D, Iezza A, et al. Biomechanical anal-
ysis of derotation of the thoracic spine using
pedicle screws. Spine (Phila Pa 1976) 2010;
35(10):1039–43.
13. Charles YP, Meyer N, Steib JP. Sagittal alignment
correction of the thoracolumbar junction in idio-
pathic scoliosis by in situ bending technique.
Stud Health Technol Inform 2008;140:72–8.
14. Vallespir GP, Flores JB, Trigueros IS, et al. Vertebral
coplanar alignment: a standardized technique for
three dimensional correction in scoliosis surgery:
technical description and preliminary results in
Lenke type 1 curves. Spine (Phila Pa 1976) 2008;
33(14):1588–97.
15. Yadla S, Maltenfort MG, Ratliff JK, et al. Adult scoli-
osis surgery outcomes: a systematic review. Neu-
rosurg Focus 2010;28(3):E3.
16. Daubs MD, Lenke LG, Bridwell KH, et al. Does
correction of preoperative coronal imbalance
make a difference in outcomes of adult patients
with deformity? Spine (Phila Pa 1976) 2013;38(6):
476–83.
17. Seo HJ, Kim HJ, Ro YJ, et al. Non-neurologic com-
plications following surgery for scoliosis. Korean J
Anesthesiol 2013;64(1):40–6.
18. Transfeldt EE, Topp R, Mehbod AA, et al. Surgical
outcomes of decompression, decompression with
limited fusion, and decompression with full curve
fusion for degenerative scoliosis with radiculop-
athy. Spine (Phila Pa 1976) 2010;35(20):1872–5.
19. Akbarnia BA, Ogilvie JW, Hammerberg KW.
Debate: degenerative scoliosis: to operate or not
to operate. Spine 2006;31(Suppl 19):S195–201.
20. Gejo R, Matsui H, Kawaguchi Y, et al. Serial
changes in trunk muscle performance after poste-
rior lumbar surgery. Spine 1999;24(10):1023–8.
21. Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury
after posterior lumbar spine surgery. Part 2: histo-
logic and histochemical analyses in humans. Spine
1994;19(22):2598–602.
22. Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury
after posterior lumbar spine surgery. Part 1: histo-
logic and histochemical analyses in rats. Spine
1994;19(22):2590–7.
23. Kawaguchi Y, Yabuki S, Styf J, et al. Back muscle
injury after posterior lumbar spine surgery. Topo-
graphic evaluation of intramuscular pressure and
blood flow in the porcine back muscle during sur-
gery. Spine 1996;21(22):2683–8.
24. Cervellini P, De Luca GP, Mazzetto M, et al. Micro-
endoscopic-discectomy (MED) for far lateral disc
herniation in the lumbar spine. Technical note.
Acta Neurochir Suppl 2005;92:99–101.
25. Derby R, Baker RM, Lee CH. Evidence-informed
management of chronic low back pain with mini-
mally invasive nuclear decompression. Spine J
2008;8(1):150–9.
26. Eck JC, Hodges S, Humphreys SC. Minimally inva-
sive lumbar spinal fusion. J Am Acad Orthop Surg
2007;15(6):321–9.
27. Foley KT, Holly LT, Schwender JD. Minimally inva-
sive lumbar fusion. Spine 2003;28(Suppl 15):
S26–35.
28. Foley KT, Lefkowitz MA. Advances in minimally
invasive spine surgery. Clin Neurosurg 2002;49:
499–517.
29. Ivanov A, Faizan A, Sairyo K, et al. Minimally inva-
sive decompression for lumbar spinal canal steno-
sis in younger age patients could lead to higher
stresses in the remaining neural arch–a finite
element investigation. Minim Invasive Neurosurg
2007;50(1):18–22.
30. Lidar Z, Beaumont A, Lifshutz J, et al. Clinical and
radiological relationship between posterior lumbar
interbody fusion and posterolateral lumbar fusion.
Surg Neurol 2005;64(4):303–8 [discussion: 308].
Anand et al374
31. Anand N, Hamilton JF, Perri B, et al. Cantilever TLIF
with structural allograft and RhBMP2 for correction
and maintenance of segmental sagittal lordosis:
long-term clinical, radiographic, and functional
outcome. Spine 2006;31(20):E748–53.
32. Christensen FB, Hansen ES, Eiskjaer SP, et al.
Circumferential lumbar spinal fusion with Brantigan
cage versus posterolateral fusion with titanium
Cotrel-Dubousset instrumentation: a prospective,
randomized clinical study of 146 patients. Spine
2002;27(23):2674–83.
33. DeBerard MS, Colledge AL, Masters KS, et al. Out-
comes of posterolateral versus BAK titanium cage
interbody lumbar fusion in injured workers: a retro-
spective cohort study. J South Orthop Assoc 2002;
11(3):157–66.
34. Yashiro K, Homma T, Hokari Y, et al. The Steffee
variable screw placement system using different
methods of bone grafting. Spine 1991;16(11):
1329–34.
35. Comparison of traditional midline approach versus
muscle splitting paraspinal approach for posterior
non-fusion stabilization of the lumbar spine–an
analysis of functional outcome. 2007 AANS/CNS
Section on Disorders of the Spine and Peripheral
Nerves. Phoenix (AZ); 2007.
36. Anand N, Baron EM, Bray RS. Modified muscle-
sparing paraspinal approach for stabilization and
interlaminar decompression: a minimally invasive
technique for pedicle screw-based posterior non-
fusion stabilization. SAS Journal 2008;2:131–3.
37. Anand N, Baron EM, Khandehroo B, et al. Long
term 2 to 5 year clinical and functional outcomes
of minimally invasive surgery (MIS) for adult scoli-
osis. Spine (Phila Pa 1976) 2013;38(18):1566–75.
38. Anand N, Rosemann R, Khalsa B, et al. Mid-term to
long-term clinical and functional outcomes of mini-
mally invasive correction and fusion for adults with
scoliosis. Neurosurg Focus 2010;28(3):E6.
39. Caputo AM, Michael KW, Chapman TM Jr, et al.
Clinical outcomes of extreme lateral interbody
fusion in the treatment of adult degenerative scoli-
osis. ScientificWorldJournal 2012;2012:680643.
40. Dakwar E, Cardona RF, Smith DA, et al. Early out-
comes and safety of the minimally invasive, lateral
retroperitoneal transpsoas approach for adult
degenerative scoliosis. Neurosurg Focus 2010;
28(3):E8.
41. Wang MY, Mummaneni PV. Minimally invasive sur-
gery for thoracolumbar spinal deformity: initial clin-
ical experience with clinical and radiographic
outcomes. Neurosurg Focus 2010;28(3):E9.
42. Anand N, Baron EM, Thaiyananthan G, et al. Mini-
mally invasive multilevel percutaneous correction
and fusion for adult lumbar degenerative scoliosis:
a technique and feasibility study. J Spinal Disord
Tech 2008;21(7):459–67.
43. Ozgur BM, Aryan HE, Pimenta L, et al. Extreme
lateral interbody fusion (XLIF): a novel surgical
technique for anterior lumbar interbody fusion.
Spine J 2006;6(4):435–43.
44. Chung SK, Lee SH, Lim SR, et al. Comparative
study of laparoscopic L5-S1 fusion versus open
mini-ALIF, with a minimum 2-year follow-up. Eur
Spine J 2003;12(6):613–7.
45. Kaiser MG, Haid RW Jr, Subach BR, et al. Compar-
ison of the mini-open versus laparoscopic
approach for anterior lumbar interbody fusion: a
retrospective review. Neurosurgery 2002;51(1):
97–103 [discussion: 103–5].
46. Zucherman JF, Zdeblick TA, Bailey SA, et al. Instru-
mented laparoscopic spinal fusion. Preliminary re-
sults. Spine (Phila Pa 1976) 1995;20(18):2029–34
[discussion: 2034–5].
47. Thalgott JS, Chin AK, Ameriks JA, et al. Gasless
endoscopic anterior lumbar interbody fusion utiliz-
ing the B.E.R.G. approach. Surg Endosc 2000;
14(6):546–52.
48. McAfee PC, Regan JJ, Geis WP, et al. Minimally
invasive anterior retroperitoneal approach to the
lumbar spine. Emphasis on the lateral BAK. Spine
1998;23(13):1476–84.
49. Tormenti MJ, Maserati MB, Bonfield CM, et al.
Complications and radiographic correction in adult
scoliosis following combined transpsoas extreme
lateral interbody fusion and posterior pedicle screw
instrumentation. Neurosurg Focus 2010;28(3):E7.
50. RodgersWB, Gerber EJ, Patterson J. Intraoperative
and early postoperative complications in extreme
lateral interbody fusion: an analysis of 600 cases.
Spine (Phila Pa 1976) 2011;36(1):26–32.
51. Willard FH, Vleeming A, Schuenke MD, et al. The
thoracolumbar fascia: anatomy, function and clin-
ical considerations. J Anat 2012;221(6):507–36.
52. O’Brien JR, Matteini L, Yu WD, et al. Feasibility of
minimally invasive sacropelvic fixation: percuta-
neous S2 alar iliac fixation. Spine 2010;35(4):460–4.
53. Wang MY. Percutaneous iliac screws for minimally
invasive spinal deformity surgery. Minim Invasive
Surg 2012;2012:173685.
54. Aebi M. The adult scoliosis. Eur Spine J 2005;
14(10):925–48.
55. Carreon LY, Puno RM, Dimar JR 2nd, et al. Periop-
erative complications of posterior lumbar decom-
pression and arthrodesis in older adults. J Bone
Joint Surg Am 2003;85(11):2089–92.
56. Raffo CS, Lauerman WC. Predicting morbidity and
mortality of lumbar spine arthrodesis in patients in
their ninth decade. Spine 2006;31(1):99–103.
57. Zurbriggen C, Markwalder TM, Wyss S. Long-term
results in patients treated with posterior instrumen-
tation and fusion for degenerative scoliosis of the
lumbar spine. Acta Neurochir (Wien) 1999;141(1):
21–6.
MISS Scoliosis Surgery 375
58. Cho KJ, Suk SI, Park SR, et al. Complications in
posterior fusion and instrumentation for degenera-
tive lumbar scoliosis. Spine 2007;32(20):2232–7.
59. Wu CH, Wong CB, Chen LH, et al. Instrumented
posterior lumbar interbody fusion for patients with
degenerative lumbar scoliosis. J Spinal Disord
Tech 2008;21(5):310–5.
60. Bono CM, Lee CK. The influence of subdiagnosis
on radiographic and clinical outcomes after lumbar
fusion for degenerative disc disorders: an analysis
of the literature from two decades. Spine 2005;
30(2):227–34.
61. Shaffrey CI, Smith JS. Editorial: minimally invasive
spinal deformity surgery. J Neurosurg Spine
2013;18(1):1–3.
62. Acosta FL, Liu J, Slimack N, et al. Changes in cor-
onal and sagittal plane alignment following mini-
mally invasive direct lateral interbody fusion for
the treatment of degenerative lumbar disease in
adults: a radiographic study. J Neurosurg Spine
2011;15(1):92–6.
63. Sharma AK, Kepler CK, Girardi FP, et al. Lateral
lumbar interbody fusion: clinical and radiographic
outcomes at 1 year: a preliminary report. J Spinal
Disord Tech 2011;24(4):242–50.
64. Johnson RD, Valore A, Villaminar A, et al. Pelvic pa-
rameters of sagittal balance in extreme lateral inter-
body fusion for degenerative lumbar disc disease.
J Clin Neurosci 2013;20(4):576–81.
65. Wang M, Mummaneni P, Fu KM, et al. Less inva-
sive surgery for treating adult spinal deformities
(ASD): ceiling effects for Cobb angle correction
with three different techniques. 20th International
Meeting on Advanced Spine Techniques. Vancouver
(Canada), July 10–13, 2013.
66. Anand N, Khanderoo B, Kahwaty S, et al. Is there a
limitation to correction of sagittal balance with
circumferential minimally invasive surgical (CMIS)
correction of adult spinal deformity (ASD)? North
American Spine Society 28th Annual Meeting.
New Orleans, October 9–12, 2013.
67. Schwab F, Lafage V, Patel A, et al. Sagittal plane
considerations and the pelvis in the adult patient.
Spine (Phila Pa 1976) 2009;34(17):1828–33.
68. Deukmedjian AR, Dakwar E, Ahmadian A, et al.
Early outcomes of minimally invasive anterior longi-
tudinal ligament release for correction of sagittal
imbalance in patients with adult spinal deformity.
ScientificWorldJournal 2012;2012:789698.
69. Wang MY, Madhavan K. Mini-open pedicle sub-
traction osteotomy: surgical technique. World Neu-
rosurg 2012. [Epub ahead of print].
70. Wang MY. Improvement of sagittal balance and
lumbar lordosis following less invasive adult spinal
deformity surgery with expandable cages and
percutaneous instrumentation. J Neurosurg Spine
2013;18(1):4–12.
71. Mariscalco MW, Yamashita T, Steinmetz MP, et al.
Radiation exposure to the surgeon during open
lumbar microdiscectomy and minimally invasive
microdiscectomy: a prospective, controlled trial.
Spine (Phila Pa 1976) 2011;36(3):255–60.
72. Ropper AE, Chi JH. Maximal radiation exposure
during minimally invasive spine surgery? Neurosur-
gery 2011;68(4):N23–4.
73. Payer M. “Minimally invasive” lumbar spine sur-
gery: a critical review. Acta Neurochir (Wien)
2011;153(7):1455–9.
74. Taher F, Hughes AP, Sama AA, et al. How safe is
lateral lumbar interbody fusion for the surgeon? A
prospective in-vivo radiation exposure study. Spine
(Phila Pa 1976) 2013;38(16):1386–92.
75. Houten JK, Nasser R, Baxi N. Clinical assessment
of percutaneous lumbar pedicle screw placement
using the O-arm multidimensional surgical imaging
system. Neurosurgery 2012;70(4):990–5.
76. Cho JY, Chan CK, Lee SH, et al. The accuracy of
3D image navigation with a cutaneously fixed
dynamic reference frame in minimally invasive
transforaminal lumbar interbody fusion. Comput
Aided Surg 2012;17(6):300–9.
77. Kim CW, Lee YP, Taylor W, et al. Use of navigation-
assisted fluoroscopy to decrease radiation expo-
sure during minimally invasive spine surgery. Spine
J 2008;8(4):584–90.
78. Dorward IG, Lenke LG, Bridwell KH, et al. Transfora-
minal versus anterior lumbar interbody fusion in long
deformity constructs: a matched cohort analysis.
Spine (Phila Pa 1976) 2013. [Epub ahead of print].
79. Isaacs RE, Hyde J, Goodrich JA, et al.
A prospective, nonrandomized, multicenter evalua-
tion of extreme lateral interbody fusion for the treat-
ment of adult degenerative scoliosis: perioperative
outcomes and complications. Spine (Phila Pa
1976) 2010;35(Suppl 26):S322–30.
80. Karikari IO, Nimjee SM, Hardin CA, et al. Extreme
lateral interbody fusion approach for isolated
thoracic and thoracolumbar spine diseases: initial
clinical experience and early outcomes. J Spinal
Disord Tech 2011;24(6):368–75.
81. Scheufler KM, Cyron D, Dohmen H, et al. Less
invasive surgical correction of adult degenera-
tive scoliosis. Part II: complications and clinical
outcome. Neurosurgery 2010;67(6):1609–21
[discussion: 1621].
82. Scheufler KM, Cyron D, Dohmen H, et al. Less
invasive surgical correction of adult degenerative
scoliosis, part I: technique and radiographic re-
sults. Neurosurgery 2010;67(3):696–710.
83. Anand N, Khanderoo B, Kahwaty S, et al. Compli-
cations of minimally invasive spinal surgery
(MISS) for correction of spinal deformity–a 5 year
experience. Chicago (IL): American Academy of
Orthopaedic Surgeons; 2013.





























