Embed Size (px)
Citation preview
Exercise Management
Pacemakers and Implantable Cardioverter Defibrillators
Chapter 10
Exercise Management
Overview of the Pathophysiology
• Loss of the normal sequence of atrial and ventricular filling and contraction can result in:
– deterioration of hemodynamics, and – significant symptoms of cardiovascular compromise at rest and during exercise.
• Pacing equipment can normalize these aberrations and improve symptoms while enhancing exercise performance
Exercise Management
•Individuals who cannot increase their heart rate in response to increased metabolic demand usually have sinus node dysfunction and may require cardiac pacing.
•Other individuals who have life-threatening ventricular arrhythmias are sometimes
candidates for an implantable cardioverter defibrillator (ICD).
Exercise Management
Pacing Terminology
Chronotropic incompetenceThe inability to augment the heart rate to an appropriate level with increases in metabolic demand. It is confirmed by peak exercise HR <85% of age-predicted max, or failure to reach > 80% of HRR during any stage of an exercise test.
Exercise Management
Symptomatic bradycardia
Symptoms directly attributable to a slow HR (< 50 bpm) include activity intolerance, transient dizziness, lightheadedness, and complete or near loss of consciousness (syncope), SOB and weak pulse.
Exercise Management
Pacemaker syndrome
• Constellation of clinical signs and symptoms – A consequence of the inadequate timing of atrial and ventricular contraction. – Most typically results from single chamber (i.e., ventricular) pacing with loss of atrioventricular synchrony and retrograde atrial activation.
• Symptoms result from a reduced cardiac output, negative atrial contribution to stroke volume, or both.
• Symptoms include lethargy, fatigue, lightheadedness, hypotension, shortness of breath, syncope, neck pulsations, and. impaired exercise capacity.
Exercise Management
Sudden cardiac death syndrome
A clinical scenario during which the person experiences loss of consciousness usually due to a ventricular tachyarrhythmia, usually ventricular tachycardia and /or ventricular fibrillation.
Unless there is prompt restoration to normal rhythm, death ensues. Severe bradycardia and asystole can also account for sudden death in a minority of cases.
Requires use of AED or ICD for return to NSR.
Exercise Management
Rate-adaptive pacemakers
Pacemakers equipped with sensors that allow adaptation of the pacemaker's rate commensurate with increases in demand (i.e.,exercise). These units utilize various types of sensors, including those that respond to physiological, mechanical, or electrical signals. This facilitates pacing in a more physiologic manner.
Exercise Management
Tiered therapy
ICDs that utilize antitachycardia pacing, shock therapies, and bradycardia safety pacing in a step-wise approach to the treatment of life-threatening ventricular arrhythmias.
Exercise Management
Pacemakers
Indications for Pacemaker Implantation
• Sick sinus syndrome with symptomatic bradycardia
• acquired AV block
• persistent advanced AV block after myocardial infarction.
Exercise Management
Pacemakers are categorized by a standardized code: (for typical placement and function, see p. 80)
• the first letter represents the chamber paced• the second is the chamber sensed• the third connotes the response to a sensed event. • the fourth position is utilized to indicate that the pacemaker has rate-response capabilities.
Exercise Management
Pacemakers are categorized by a standardized code:
For example, if [ V V I R ]is the abbreviation used, then • the ventricle (V) is the chamber being paced and sensed. •when the pacemaker senses a normal ventricular contraction, the pacemaker is inhibited (I). •The R indicates that the pulse generator is rate responsive during exercise.
Exercise Management
Dual Chamber Pacemaker (DDDR)
• paces and senses both the atrium and ventricle
• triggers or inhibits dependent upon normal conduction signal that is above the programmed rate cutoff on the pacemaker
• is considered the “optimal” pacemaker type for those individuals who have normal SA node function
Exercise Management
Implantable Cardioverter Defibrillators (ICD)
• are utilized to electrically terminate life threatening ventricular tachyarrhythmias
• when a tachyarrhythmia is detected, preprogrammed therapies are sent back to terminate the arrhythmia.
• ICDs can pace-terminate an arrhythmia and/or deliver electric cardioversion / defibrillation shocks.
Exercise Management
Effects on the Exercise Response
Pacing devices
• Patients with pacing devices benefit from an improved heart rate response to exercise.• Inadequate heart rate responses to exercise can be improved with pacemaker technologies.
Exercise Management
Effects on the Exercise Response
ICDsPatients are at risk of receiving inappropriate shocks during exercise if • the heart rate exceeds the programmed threshold rate for therapy• the person develops an exercise-induced supraventriculartachycardia.
Thus, patients with ICDs should be closely monitored during exercise to ensure that their heart rate does not approach the activation rate for the device.
Exercise Management
Effects of Exercise Training
• Recent technologic advances have dramatically advanced pacemaker function to the point where pacemakers can nearly mimic normal cardiac function, both at rest and during exercise.•These advances allow cardiac supply to meet the increase in cardiac demand.•Exercise heart rate thresholds on the ICD must be set above (10%) the upper end of the exercise heart rate•Heart rate must be closely monitored during the entire exercise session
Exercise Management
Recommendations for Exercise Testing
• Exercise testing may be used to determine the effectiveness of rate-responsive pacemakers
•LLGXT and small incremental protocols are appropriate.
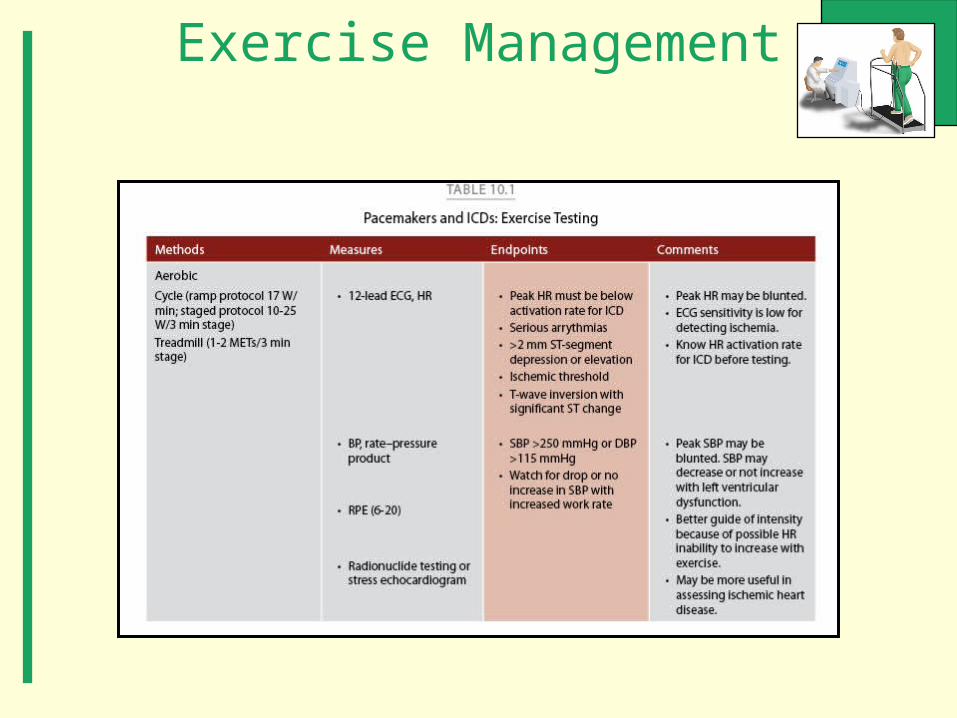
•See Table 10.1, (slide follows) note exercise endpoints, especially for peak HR with ICD’s and blood pressure response to exercise.
Exercise Management
Recommendations for Exercise Testing
• Exercise HR must stay below the ICD HR threshold
•Radionuclide testing or stress echo may improve the test sensitivity (also you will need to be aware of underlying CV pathologies)
•See Table 10.1, (slide follows) note exercise endpoints, especially for peak HR with ICD’s and blood pressure response to exercise.
Exercise Management
Exercise Management
Recommendations for Exercise Programming
• Before an exercise program begins, the upper training heart rate should be established and documented.• Activities should be selected so that the intensity can be carefully regulated during exercise. • Because some upper body movement may dislodge implanted leads, upper body exercises are not advised initially for people with pacemakers (resistance training should not begin until 4-6 wks post-implantation).• The upper exercise training intensity must be set below the person's ischemic threshold and must not approach a heart rate causing activation of the ICD
Exercise ManagementRecommendations for Exercise Programming
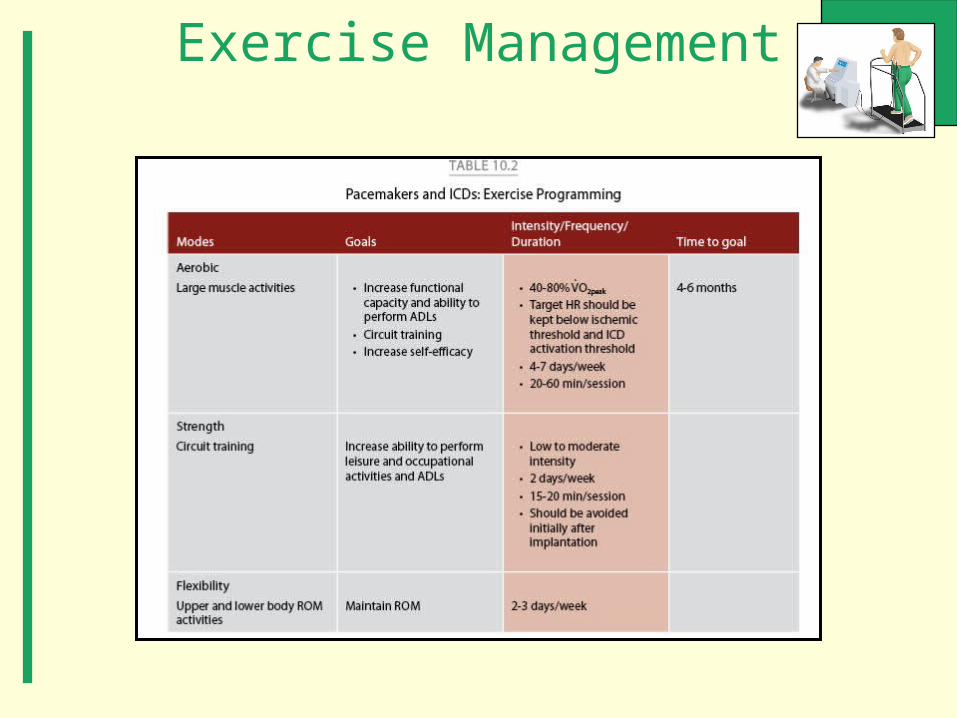
Specific ICD information should include:• ICD detection threshold in bpm•Whether if device is for V fib or V tach•How quickly should HR increase•What is the sustained VT setting (how long will the episode last before a therapy is delivered?)•What is the specific type of ICD therapy (Pacing, shock, etc..)?•See Exercise Programming, Table 10.2, p.82, (next slide)
Exercise Management
Exercise Management
End of Presentation





























