Embed Size (px)
Citation preview

784 Letters to Editor
Iran J Pediatr; Vol 24 (No 6), Dec 2014Published by: Tehran University of Medical Sciences (http://ijp.tums.ac.ir)
Extramedullary Hematopoiesis in Adrenal
Gland. An Uncommon Cause of Adrenal
Incidentaloma in Sickle Cell Disease
Negar Azarpira1,2, MD; Mina Heidari Esfahani2, MD;Shahram Paydar3, MD
1 Transplant Research Center, 2Department of Pathology,3Department of Surgery, Shiraz University of Medical Sciences,Shiraz, IranReceived: Feb 14, 2014; Accepted: Nov 11, 2014;First Online Available: Dec 12, 2014
Dear EditorExtramedullary hematopiesis (EMH) is a responseto insufficient blood cell production by producingof blood elements outside of the marrow cavity. Itoccurs most often due to hemolytic anemias suchas thalasemia, hereditary spherocytosis and sicklecell anemia. It also could be seen in prolonged irondeficiency anemia, myelofibrosis, polycythemia,leukemia and lymphoma[1,2,3].EMH occurs most commonly in thereticuloendothelial system such as spleen andliver, but it may also be seen in organs, such asbowel, breast, brain, pleura and adrenals[2,4].In our review of literature we found reports ofadrenal gland EMH in patients with beta-thalasemia, agnogenic myeloid metaplasia andhereditary spherocytosis. EMH in sickle cellanemia has been reported in paranasal sinuses,mediastinum and retroperitoneum.Here we report a case of adrenal gland EMH asadrenal incidentaloma in a patient with sickle cellanemia; in literature review no similar result isfound[1-8].The patient was a 15 year-old female withhomozygous sickle cell disease. She was diagnosedas a case of sickle cell at the age of two years whenshe presented with bone pain. After that she wasunder routine clinical follow-up. She had history ofmultiple painful bone crises and one episode ofacute splenic sequestration in childhood. Duringhospital course she complained of vagueabdominal and left flank pain. In physicalexamination, findings were normal vital signs, paleconjunctivae and skin with mild softhepatomegaly. No abdominal tenderness wasnoticed. No supra renal mass was detected on
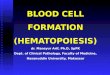
physical examination. Routine work/up forevaluation of abdominal pain was done.Laboratory investigation showed hemoglobin11 g/dL, WBC count 1.0×109/ L, platelet count390×109/ L, MCV 70.1 fl, MCH 21.6 pg.Biochemical investigations were: serum bilirubin1.8 mg/dL; conjugated bilirubin 0.8 mg/ dL, bloodurea 27 mg/ dL, serum creatinine 0.7 mg/dL,serum calcium 8.2 mg/ dL, serum phosphorous 6.6mg/dL, fasting blood sugar 100 mg/dL; alanineaminotransferase 41 IU/ dL, aspartateaminotransferase 50 IU/dL. Tests for hepatitis Cvirus (anti HCV antibody) and HIV antibodies(Anti HIV-1,2) serum HBsAg and HBc antibodywere negative. Fasting serum cortisol level was 13mcg/dL. Urinalysis was normal. Abdominalsonography showed mild hepatomegaly and awell-defined left suprarenal solid mass in size of7.7×5.3 cm. Abdominal CT scan confirmed a 7cmwell defined suprarenal mass (Fig 1).Surgical plan was considered and left adrenal-ectomy done. On gross examination, a brown massmeasuring 7×5×3 cm was detected, surroundedwith a rim of normal adrenal gland parenchyma.The definite diagnosis was confirmed withhistopathology that revealed active hematopoiesisin adrenal gland (extramedullary hemopoiesis)(Fig. 2). Her postoperative course was uneventfuland she was discharged from hospital in goodcondition.Adrenal incidentaloma has a prevalence of 5%in the general population. EMH is a rare cause ofincidentaloma and is seen in patients withhematologic disorders such as beta-thalasemia,
Fig. 1: Right supra renal mass.* Corresponding Author; Address: Transplant Research Center,Zand Street, Nemazi Hospital, Postal Code Number: 7193711351,Shiraz University of Medical Sciences, Shiraz, IranE-mail: [email protected]

785Letters to Editor
Iran J Pediatr; Vol 24 (No 6), Dec 2014Published by: Tehran University of Medical Sciences (http://ijp.tums.ac.ir)
Fig. 2: Remnant of adrenal cortical tissue with foci ofhematopoietic cells including erythro-myeoloid,megakaryocytic cells with hemosiderin deposit (H&E ×400)(Yellow Arrow)agnogenic myeloid metaplasia and hereditaryspherocytosis.EMH is a physiologic or pathologiccompensatory mechanism that occurs because ofimbalance between bone marrow erythropoiesisand circulatory blood demands. In histopathology,this intends to mimic a normal bone marrow withall marrow elements[1,2,3].EMH occurs most commonly in thereticuloendothelial system, but it may also bedeveloped in organs such as lungs, gastrointestinaltract, breast, brain and kidney and rarely inadrenal[4,5].The exact mechanism of EMH in the adrenalgland is unknown, but several hypotheses aresuggested. The adrenal gland has hematopoieticcapacity during the fetal period and EMH maydevelop from primitive rests in diseasedcondition. Other scientists believe thatembolization of hematopoietic stem cells andhoming in adrenal gland may occur. Chronichypoxia is another presumptive cause of EMH[3,6,7].EMH is seen in hemoglobinopathies such asthalassemia, hereditary spherocytosis and inhematologic diseases including myelofibrosis andmyeloproliferative disorders. In the literature,most cases were associated with intermediatethalassemia. The frequency of extramedullaryhematopiesis in thalassemia major was very low,especially, when ineffective erythropoiesis wassuppressed by regular transfusion. In infrequenttransfusion, chronic hypoxia and subsequentlyEMH develops[4,5,8,9]. EMH is rare in patients withsickle cell disease. Although few cases ofintrathoracic, pelvic and paranasal have been
documented in literature[8,9], our case was the firstone reported as adrenal incidentaloma.EMH is usually asymptomatic and discoveredincidentally. Symptomatic cases occur due to masseffect with compression to adjacent organ[8,9]. Thesurgical indication for excision of the adrenalincidentalomas is the tumor size. Adrenal tumorlarger than 6 cm in diameter must be excised. Inthese cases, the risk of adrenal cancer is 35% to98%[8,9].Treatment options for patients with EMH aredescribed for thalassemia patients and depend onthe location and symptoms. Different approachesincluded surgery, local radiation, bloodtransfusion and hydroxyurea. Hydroxyureastimulates the synthesis of hemoglobin F andtherefore participates in inactivation andshrinking of EMH. This effect was documented inthalassemia diseases. For paraspinal/epidurallesions, directed low-dose radiotherapy isrecommended[9]. In conclusion, extramedullaryhematopiesis should be considered in thedifferential diagnosis of patients with sickle celldisease that present with a solitary mass. The CT-guided biopsy can exclude a true neoplasm andalter the management and prognosis.Key words: Extramedullary Hematopoiesis; Sickle Cell;Adrenal GlandReferences1. Sproat IA, Dobranowski J, Chen V, et al. Presacralextramedullary hematopoiesis in thalassemiaintermedia. Can Assoc Radiol J 1991;42(4):278-82.2. Chuang CK, Chu SH, Fang JT, et al. Adrenalextramedullary hematopoietic tumor in a patientwith beta-thalassemia. J Formos Med Assoc 1998;97(6):431-3.3. Porcaro AB, Novella G, Antoniolli SZ, et al. Adrenalextramedullary hematopoiesis: report on a pediatriccase and update of the literature. Int Urol Nephrol2001;33(4):601-3.4. King BF, Kopecky KK, Baker MK, et al.Extramedullary hematopoiesis in the adrenalglands: CT characteristics. J Comput Assist Tomogr1987; 11(2):342-3.5. Keikhaei B, Shirazi AS, Pour MM. Adrenalextramedullary hematopoiesis associated with β-thalassemia major. Hematol Rep 2012;4(2):e7.6. Bastounis EA, Karayiannakis AJ, Anapliotou ML, etal. Incidentalomas of the adrenal gland: diagnosticand therapeutic implications. Am Surg 1997;63(4):356-60.

786 Letters to Editor
Iran J Pediatr; Vol 24 (No 6), Dec 2014Published by: Tehran University of Medical Sciences (http://ijp.tums.ac.ir)
7. Asnani M, Char G, Reid M, et al. Intrathoracic andpelvic extramedullary hematopoiesis in sickle celldisease: a case report. West Indian Med J 2007;56(6):540-3.8. Verani R, Olson J, Moake JL. Intrathoracicextramedullary hematopoiesis: report of a case in apatient with sickle-cell disease-beta-thalassemia.Am J Clin Pathol 1980;73(1):133-7.9. Arkadopoulos N, Kyriazi M, Yiallourou AI, et al. Arare coexistence of adrenal cavernous hemangiomawith extramedullar hemopoietic tissue: a casereport and brief review of the literature. World JSurg Oncol 2009;7:13.
Chicken Meat Anaphylaxis in a Child with
No Allergies to Eggs or Feathers
Ceren Can*1, MD; Mehtap Yazicioglu1, MD;Gokce Ciplak2, MD
1Department of Pediatric Allergy, 2Gokce Ciplak, Department ofPediatrics, Trakya University Faculty of Medicine, Edirne,TurkeyReceived: Mar 11, 2012; Accepted: Sep 16, 2014;First Online Available: Dec 12, 2014Poultry meat is very popular in today’s healthydiet. Despite the fact that chicken meat is widelyconsumed, allergy to chicken meat is rarelyreported[1]. However, we present here a case of achild with chicken meat anaphylaxis, yet who hasexperienced no allergies to eggs or to feathers.A fifteen-year-old male patient with a personalhistory of chicken meat allergy was referred to ourclinic. Aged seven, he experienced angioedema ofthe lips, redness of the face and trunk, itching eyes,and hoarseness five minutes after he ate chickenmeat. His symptoms gradually resolved withoutadmission to hospital. Subsequently, he did notconsume any chicken meat until last year (2013),when he reported nasal itching and irritabilitywhile passing by restaurants serving chickendoner kebab. Last year, he also reported similarcomplaints after consuming chicken wings. He wasadmitted to a public hospital where symptomatictreatment was given. He was advised not to eatchicken meat and continued to display similarsymptoms whenever he failed to comply with thediet and did consume it. He never ate turkey, duck,or goose, and was tolerant to eggs. He had nophysical contact with birds. His personal and
family history was unremarkable, and he had noknown drug allergies, including antibiotics. Hisphysical examination was normal.Laboratory results on admission: CBC withwhite blood cell differential was within normalrange; serum total IgE was 351 IU/ml. Skin pricktests (SPTs) with commercial allergenic extracts ofchicken (Alyostal Stallergenes, France), egg white,and egg yolk (ALK Abello, Denmark) werepositive. SPT was negative for a feather mixture(Alyostal Stallergenes, France). Skin prick–pricktests (PPTs) were performed with raw and cookedchicken and turkey meat: they were all positive(Fig 1). Both SPTs with the same commercialallergenic extracts and PPTs with raw and cookedchicken meat were performed on four healthy,non-atopic adult volunteers, all resulting negative.The specific IgE serum level for chicken meat inour patient was 10.20 kU/L (Class III)(chemiluminescence immunoassay). An oralchallenge test with chicken meat was notperformed due to the risk of precipitating a severereaction. The clinical history of our patient and theresults of in vivo and in vitro tests werecompatible with chicken meat allergy. We advisedhim not to consume any avian meats andprescribed an epinephrine autoinjector to use incase of anaphylactic emergency.Allergic reactions to chicken meat are veryrare[1]. The prevalence of chicken meat allergy infood allergic patients is 0.6%–5%[2]. Patients withchicken meat allergy can be separated into two
Fig. 1: Skin prick tests with commercial allergenicextracts of chicken, egg white, egg yolk, feather mixture,skin prick-prick tests with raw and cooked chicken andturkey meat* Corresponding Author; Address: Department of Pediatric Allergy,Trakya University , Edirne, Turkey
E-mail: [email protected]