Embed Size (px)
Citation preview

Eye Movement Abnormalities Correlate with Genotype in Autosomal Dominant
Cerebellar Ataxia Type I Sophie Rwaud-Pechoux, PhD,* Alexandra Durr, MD,* Bertrand Gaymard, MD, PhD,t GCraldine Cancel,*
Christoph J. Ploner, MD,$ Yves Agid, MD, PhD,* Alexis Brice, MD,* and Charles Pierrot-Deseilligny, MDS
We compared horizontal eye movements (visually guided saccades, antisaccades, and smooth pursuit) in control subjects (n = 14) and patients with three forms of autosomal dominant cerebellar ataxias type I: spinocerebellar ataxias 1 and 2 (SCA1, n = 11; S W , n = 10) and SW/Machado-Joseph disease (MJD) (n = 16). In SCA1, saccade amplitude was significantly increased, resulting in hypermetria. The smooth pursuit gain was decreased. In S W , saccade velocity was markedly decreased. The percentage of errors in antisaccades was greatly increased and was significantly correlated with age at disease onset. In addition, a correlation between smooth pursuit gain and the number of trinucleotide repeats was found. In S W , gaze-evoked nystagmus was often present as was saccade hypometria and smooth pursuit gain was markedly decreased. Three major criteria, saccade amplitude, saccade velocity, and presence of gaze-evoked nystagmus, permitted the correct assignment of 90% of the SCAl, 90% of the S W , and 93% of the patients with S W to their genetically confirmed patient group and, therefore, may help orient diagnoses of SCA1, S W , and SCA3 at early clinical stages of the diseases.
Rivaud-Pechoux S , Diirr A, Gaymard B, Cancel G, Ploner CJ, Agid Y, Brice A, Pierrot-Deseilligny C. Eye movement abnormalities correlate with genotype in autosomal dominant cerebellar
ataxia type I. Ann Neurol 1998;43:297-302
Ocular motor abnormalities are frequent in patients with autosomal dominant cerebellar ataxias (ADCAs). Slow saccades, saccade dysmetria, horizontal or verti- cal nystagmus, impairment of vestibular function, and smooth pursuit have been reported.'-12 Eye movement disorders have been compared in patients with Fried- reich's ataxia, olivopontocerebellar atrophy, and cere- bellar atrophy.*-" However, analysis of ADCAs, par- ticularly type I, is difficult, because they are genetically and clinically heterogeneous. Five gene loci associated with ADCA type I have been mapped, and three of the mutated genes have been identified. All three genes show expansion of unstable trinucleotide cytidine- adenosine-guanosine (CAG) repeats encoding polyglu- tamine tracts: spinocerebellar ataxia (SCA) 1 on chro- mosome 6p,I3 SCA2 on chromosome l2q,'*-I6 and SCAS, or Machado-Joseph disease (MJD), on chromo- some 14q. l7 Because several eye movement disorders have been reported in SCAl and a decrease in saccade velocity has been noted in SCA2,1'7'2 we systematically compared eye movements in patients with genetically confirmed SCAl, SCA2, and SCA3. Smooth pursuit
and visually guided saccades were studied, and an antisaccade paradigm was used to evaluate the cogni- tive component of ocular motor control, especially that of the frontal cortex. The study has shown that each of the subgroups of ADCA type I exhibits a characteristic pattern of ocular abnormalities.
Patients and Methods Patients Three groups of patients with ADCA type I and a control group of normal subjects were studied. The clinical charac- teristics of the three patient groups are presented in Table 1.
Patient complaints and findings on physical examination were assessed at the time of eye movement recordings. Func- tional handicap was evaluated as mild: walking without help; moderate: walking with assistance; and severe: wheelchair bound or bedridden. Genotypes at the three SCA loci were d e t e r ~ n i n e d , ' ~ , ' ~ , ' ~ and the number of CAG repeats was compared with that of normal and expanded alleles that had been sequenced for each gene."-"
A control group of 14 subjects (mean age, 43 -C 12 years) without neurological disorders was studied with the same paradigms. All subjects gave their informed consent.
From 'INSERM U289 and Ftdkration de Neurologie, tService d'Explorarion Fonctionnelle du Sysreme Nerveux, f a i n i k fur Neu- rologie, Charirt, Berlin, and %Service de Neurologie I. Received JuI 10, 1997, and in revised form Oct 8. Accepted for publication Oct 17, 1997.
Address correspondence to Dr Rivaud-Pechoux, INSERM U289, Hapita1 de la Salpkrrikre, 47 Boulevard de l'Hapita1, 75651 Paris Cedex 13, France.
Copyright 0 1998 by the American Neurological Association 297

Table 1. Clinical Characteristics o f the Three Patient Groups with Autosomal Dominant Cerebellar Ataxia at the Time of Eye Movement Recordings
SCAl SCA2 SCA3
Number of patients (families) Menlwomen Mean age at onset (years, range) Mean age at examination Functional handicap (n)
Mild Moderate Severe
Mean CAG repeat length (range)
Frequency of clinical signs (%) Cerebellar gait ataxia Cerebellar dysarthria Increased reflexes in the lower limbs Decreased reflexes in the lower limbs Extensor plantar response Swallowing difficulties Sphincter disturbances Decreased vibration sense at ankles Memory disturbances or dementiad
11 (4) 417 28 -t 7 (19-45) 3 4 2 10
4 3 4
53 2 5 (44-
100 82 82
0 40 73 18 36 0
-63)
10 (3) 416 30 ? 11 (14-46) 4 0 ? 14
3 3 4
41 t 3 (38-48)
90 100 20 50 30 50 40 56 10
16 (6) 917 40 -C 12 (17-67) 4 7 2 13
3 6 7
72 2 3 (67-77)
94 94 63 44 47 56 25 63 6
"Dementia was assessed with the MATTIS scale, and memory performance with the California Verbal Learning test.
Methods The subject's head was immobilized, and eye movements were recorded by horizontal direct-current electro-oculog- raphy in complete darkness with four electrodes (two hori- zontal temporal and two vertical on one eye for controlling blinks). The electrical signal was amplified and filtered (bandwidth, 0-100 Hz), and the spatial resolution was 0.5". Visual cues were presented at a distance of 95 cm with red LEDs embedded in a curved ramp. LEDs were 0.15 degree and 5 cd/m2 in luminance. Each session was preceded by 10 minutes of dark adaptation. The velocity threshold criterion for definition of saccades was 30"lsec. Data were sampled with a frequency of 200 Hz. System calibration was per- formed before each paradigm.
In the gap task, a central fixation point was switched off 200 msec (gap) before the onset of a luminous lateral target located 25" to the right or to the left of the central fixation point. After 1 second, the lateral target was switched off and the central fixation point was simultaneously switched on. The subject was instructed to fixate the central point, to look at the lateral target as soon as it appeared, and then to go back to the central fixation point. The target was presented pseudorandomly to the right or to the left, with unpredict- able timing (between 2 and 4 seconds). Left and right sac- cade latencies were calculated for each subject by averaging 20 measurements in each direction. Accuracy of centrifugal and centripetal saccades was expressed as gain (amplitude of the first saccade over the eccentricity of the target). The mean saccade velocity was determined only for saccades with amplitudes of 25" -C 2".
In the antisaccade tusk, presentation of targets was the same as in the gap task, except that the subject was instructed to look in the opposite direction from the lateral target without looking at it. The percentage of errors (misdirected saccades,
regardless of whether they reached the target or were only directed to it) was determined in each direction right or left.
Smooth pursuit was evaluated with a small horizontal target moving sinusoidally with a total amplitude of 40", peak ve- locity of 23"/sec, and a frequency of 0.18 Hz. The mean rightward and leftward gains (peak eye velocity over peak target velocity) were calculated from 10 consecutive cycles.
Gaze-evoked nystagmus was observed in some patients; that is, an inability to fix the eyes in an eccentric gaze elicited a centripetal drift, followed by a centrifugal corrective saccade. A gaze position of 25" of eccentricity for 1 second was cho- sen to clearly distinguish a pathological gaze-evoked nys- tagmus from a physiological end-gaze nystagmus. The per- centage of patients showing gaze-evoked nystagmus was calculated for each patient group.
Statistical Analysis No significant lateralization was found for mean saccade pa- rameters either in the patient groups or in controls. Statisti- cal analysis was therefore carried out using mean values of a subject's total of values. Saccade latency, saccade velocity, centrifugal and centripetal gain, and smooth pursuit gain were compared between patient group and control group by analysis of variance. Multiple comparisons between each patient group and control group were made using the Newman-Keuls test. The percentage of errors in the antisac- cade task was compared with the control group using the Kruskal-Wallis test. The percentages of subjects with gaze- evoked nystagmus in each group were compared with the x2 test. Correlations among saccade parameters, CAG repeat number, disease duration, and age at onset were evaluated using the Spearman rank-sum correlation. Results were con- sidered to be statistically significant at a p 5 0.05 level.
298 Annals of Neurology Vol 43 No 3 March 1998

Table 2. Horizontal Eye Movement Parameters
Visually Guided Saccades
Accuracy (Gain) (Mean 2 SD) Antisaccades Smooth Pursuit Gaze-Evoked
Latency (ms) Velocity (o/s) (% Errors): (Gain) Nystagmus (Yo (Mean 2 SD) (Mean 5 SD) Centrifugal Centripetal Mean (Range) (Mean f SD) of Patients)
Controls (n = 14) 167 i 40 289 i 44 0.95 t 0.02 0.99 _t 0.03 4 (0-17) 0.99 2 0.04 -
S C A 3 (n = 16) 1 7 2 i 29 274 i 60 0.87 i 0.18b 0.98 t 0.19 31 (O-lOO)d 0.68 2 0.17' 63d
Comparisons are between each patient group and the control group: =p < 0.01; 'p < 0.05; 'p < 0.0001; 'p < 0.001.
SCAl (n = 11) 187 i 35 226 i 49" 1.06 i 0.13" 1.09 i 0.13" I 5 ( 0 ~ 4 1 . 5 ) ~ 0.78 2 0.25" 9 SCA2 (n = 10) 210 i 51 142 i 64' 0.92 2 0.07 1.03 t 0.09 42 (0-79)' 0.82 Ifr 0.27 0
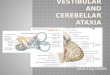
Results The results are summarized in Table 2. In spite of some overlap, each subgroup of patients with ADCA type I exhibited a distinct pattern of abnormalities. In no case was there a significant difference in the latency of visually guided saccades. All patients made errors in the antisaccade paradigm, but to highly different de- grees. In patients with SCA1, ocular motor deficits were mild but present in all paradigms. Visually guided saccades, both centrifugal and centripetal, were hyper- metric ( p < 0.015 and p < 0.02, respectively) (Fig lC), whereas smooth pursuit gain was decreased ( p < 0.003). It is unlikely, that age differences to the control group (34 vs 43 years) account for these findings, be- cause saccade accuracy is not significantly affected by age. This hypermetria was characteristic for patients with SCAl. In patients with SCA2, only the velocity of visually guided saccades was reduced ( p < 0.0001) (see Fig 1D) and the percentage of errors on the anti- saccade task was increased ( p < 0.0001); but the def- icits were severe. A similar decrease in saccade velocity was not observed in the other two groups, even if a slight but significant decrease was also present in pa- tients with SCAl ( p < 0.005). In patients with SCM, in addition to errors on the antisaccade task ( p < 0.0002), a significant hypometria in the centrifugal vi- sually guided saccades ( p < 0.04) (see Fig 1E) and decreased smooth pursuit gain were found ( p < 0.0002). These patients also differed from the remain- der by the presence of gaze-evoked nystagmus, which was noted in 63% of cases. Such a nystagmus was ob- served in only 1 other patient with SCA1.
The specificity of the deficits associated with each of these diseases shows that recordings of horizontal sac- cades can be highly discriminative between ADCA sub- groups. In the recording of 1 patient with SCA1, hy- permetria is evident and corresponds either to true
22
b Fig 1. Recordings of horizontal saccades in the gap task: (A) stimulation, (B) control subject, (C) SGHI patient, (0) SCA2 patient, (E) SCA3 patient. C = central fixation; L = lefi; R = right and t = target. The dotted line indicates the ex- tinction of the central fixation point (gap = 200 msec).
L
L I 25" 1 sec -
Rivaud-Pechoux et al: Eye Movements in ADCA 299

hypermetria, with a hypermetric saccade followed by one or several corrective saccades of diminishing am- plitude separated by short pauses, or to a pulse step mismatch, as illustrated in Figure lC, where the hy- permetric saccade is followed by a drift to the intended target position. Such a deficit may be observed at an early stage of the disease. In patients with SCA2, the decreased velocity can be observed after only 2 years of evolution of the disease and may even be clinically ob- vious at bedside examination (see Fig ID). In patients with SCA3, hypometria and gaze-evoked nystagmus are often evident at the course of disease (see Fig 1E).
To determine characteristic abnormalities that might serve as diagnostic criteria for each patient group, we calculated for each group the percentage of patients with values outside ?3.3 standard deviations (SD) of the control group (corresponding to a 99.9% probabil- ity to be outside the values of the control group (Table 3). In the SCAl group, 54% of the patients had hy- permetric centrifugal saccades. In the SCA2 group, slow saccades were present in 70% of the patients. In the SCA3 group, centrifugal saccades were frequently hypometric (56% of patients) and occasionally hyper- metric (1 8% of patients). Furthermore, gaze-evoked nystagmus was observed in 63% of these patients. La- tency, centripetal gain, and smooth pursuit were less discriminative between groups, as was percentage of er- rors in the antisaccade task.
To validate the diagnostic sensitivity of the just- mentioned criteria, we calculated the frequency of pa- tients fulfilling at least two of three of the criteria char- acteristic for each ADCA I subgroup. In the SCAl group, 90% of patients fulfilled at least two of three and 45% of patients fulfilled three of three of the fol- lowing criteria: normal velocity, hypermetric centrifu- gal saccades (normal mean + 3.3 SD), and absence of gaze-evoked nystagmus. In the SCA2 group, 30% of patients fulfilled at least two of three and 60% of pa- tients fulfilled three of three of the following criteria: decreased saccade velocity (control mean - 3.3 SD), normal saccade amplitude, and absence of gaze-evoked nystagmus. In the SCA3 group, 93% of patients ful- filled at least two of three and 25% of patients fulfilled
three of three of the following criteria: normal sac- cade velocity, hypometric centrifugal saccades (control mean - 3.3 SD), and presence of gaze-evoked nystagmus.
We further determined whether age at onset and/or the number of CAG repeats in the mutated gene were correlated with the observed eye movement abnormal- ities. Age at onset was negatively correlated with the percentage of errors in the antisaccade task in patients with SCAl (Y = -0.664, p < 0.03) and with smooth pursuit gain in patients with SCA2 ( v = -0.624, p < 0.05). Smooth pursuit gain was positively correlated with the number of CAG repeats in patients with SCA2 ( r = 0.812, p < 0.0004). There were no signif- icant correlations in the SCA3 group. The disease du- ration was not correlated with saccade parameters for each group.
Discussion The analysis of eye movements in our group of pa- tients with ADCA type I has revealed characteristic patterns of abnormalities for each genotype: (1) in pa- tients with SCA1: moderate decrease of saccade veloc- ity and overshooting of centrifugal and centripetal sac- cades, increase in percentage of errors in antisaccades, and decrease of smooth pursuit gain; (2) in patients with SCA2: marked decrease of saccade velocity and increased percentage of errors in antisaccades; and (3) in patients with SCA3: saccade hypometria, frequent presence of gaze-evoked nystagmus, increased percent- age of errors in antisaccades, and decrease of smooth pursuit gain.
O n physical examination, patients of all groups pre- sented with cerebellar gait ataxia and the mean level of motor disability in each group was similar, indicating clinical homogeneity between groups. However, the different patterns of ocular motor abnormalities ob- served in our patient groups may reflect differences in the topography of the degenerative process that may be missed on physical examination. Although the observed abnormalities of gaze-evoked nystagmus and saccade hypermetria are frequent clinical signs in a great variety of cerebellar disorders, their presence or absence in combination with a family history of an autosomal
Table 3. Percentage o f Patients with Values Outside Control Mean 2 3.3 SD of Contvols
Visually Guided Saccades
Accuracy Smooth Pursuit
Latency Velocity Centrifugal Gain Centripetal Gain Gain
>3.3 SD <3.3 SD >3.3 SD <3.3 SD >3.3 SD (3.3 SD <3.3 SD
SCAl 0 9 54 0 45 9 54 S C M 0 70 0 20 30 10 70 SCA3 0 0 18 56 19 19 81
300 Annals of Neurology Vol 43 No 3 March 1998

dominant cerebellar ataxia points to distinct ADCA I subgroups.
In patients with SCA1, saccade hypermetria was a prominent finding and appeared at an early stage of the disease, as previously ~bserved ,~ and was associated with a decrease in saccade velocity, as in 3 previously reported cases. l2 These authors have also reported other ocular motor deficits, such as upward gaze paral- ysis, gaze-evoked nystagmus, and decreased vestibu- loocular reflex gain. In our study, gaze-evoked nystag- mus was observed in only one patient with SCA1. Neurophysiologic studies in nonhuman primates sug- gest that, in cerebellar disorders, saccade hypermetria may result either from true saccade hypermetria due to dysfunction of the fastigial nuclei23224 or to a pulse-step mismatch due to dysfunction of the f l o c c ~ l u s . ~ ~ In- deed, hypermetric saccades have been observed in hu- mans with bilateral lesions of the fastigial ocular motor region. Moreover, the increased errors in antisaccades in patients with SCAl with early onset suggest that frontal functions are affe~ted,~’ which may be spared in patients with SCAl of late onset.
In the patients with SCA2, the major finding, a marked decrease in saccade velocity, is consistent with previous studies.’ 1,28x29 This deficit could result from damage to the paramedian pontine reticular formation (PPRF), which controls horizontal saccade velocity.30 In a postmortem study, degeneration of the PPRF was found in an Indian patient with hereditary cerebellar ataxia and slow s a ~ c a d e s , ~ ~ compatible with SCA2. This putative pontine degeneration in SCA2 seems to depend on disease duration, because saccade velocity was normal in the patient with the shortest disease du- ration (1 year) but clearly present in patients with longer disease durations. A high percentage of errors in the antisaccade task in patients with early onset of the disease also suggests frontal dysfunction in these pa- tients. A postmortem study in two patients with SCA2, with age at onset younger than 25 years, showed prom- inent atrophy in the frontal and temporal lobes.32 By contrast, smooth pursuit deficits were more severe in patients with late-onset disease, probably as a result of cerebellar rather than frontotemporal degeneration.
In SCA3, gaze-evoked nystagmus, which has not been previously reported to our knowledge, suggests that the saccade integrator (ie, the nucleus prepositus hypoglossi/flocculus network)30 is affected at an early stage of the disease. The association of saccade hy- pometria with decreased smooth pursuit gain suggests atrophy of the posterior cerebellar vermis, which is in- volved in the control of saccade accuracy and smooth pursuit gain in As in patients with SCAl and SCA2, the percentage of errors in the anti- saccade task suggests a loss of frontal inhibitory func- tions in patients with SCA3 as well.
In conclusion, this study has shown the existence of
26
characteristic ocular motor abnormalities in three ge- netically distinct forms of ADCA type I that may per- mit a differential diagnosis based on eye movement ex- amination at an early stage of the disease: saccade hypermetria in SCAl, decreased saccade velocity in SCA2, and saccade hypometria and gaze-evoked nys- tagmus in SCA3. Decreased saccade velocity and gaze- evoked nystagmus can usually be detected at bedside examination. Although the presence of only one of these eye movement abnormalities may not be suffi- cient to orient diagnosis in an individual patient, the association with other ocular motor and clinical criteria can be highly discriminative. Our study showed that three parameters (saccade accuracy, saccade velocity, and gaze-evoked nystagmus) could predict the geno- type of patients with ADCA I with probabilities of 90%, 90%, and 93% in SCAl, SCA2, and SCA3, re- spectively. Further studies will have to elucidate whether other ADCA I subgroups equally exhibit dis- tinct patterns of ocular motor abnormalities that may help to clinically orient the diagnosis to the probable genotype. Moreover, future anatomical studies may provide better insight into the correlation between oc- ular motor abnormalities and the topography of the degenerative process in patients with ADCA type I.
This research was supported by the Association Fransaise Contre les Myopathies (AFM), the VERUM Foundation, the Association pour le Dtveloppement de la Recherche sur les Maladies Gtnk- tiques Neurologiques et Psychiatriques, Biomed ( N T E E BMH4- CT960244 and Biomed Concerted Action (CEE BMH 1-CT94- 1243). G.C. was supported by the AFM, and C.P. was supported by the Deutsche Forschungsgemeinschaft (grant PI 24811-1).
We thank H. Chneiweiss, G. Ftnelon, V. Hahn-Barma, I. Lagroua, and M. Ruberg for their contribution for this study.
References 1. Wadia NHS, Swami RK. A new form of heredo-familial spino-
cerebellar degeneration with slow eye movements (nine fami- lies). Brain 1971;94:359-374
2. Zee DS, Yee RD, Cogan DG, et al. Ocular motor abnormali- ties in hereditary cerebellar ataxia. Brain 1976;99:207-234
3. Murphy MJ, Goldblatt D. Slow eye movements, with absent saccades in a patient with hereditary ataxia. Arch Neurol 1977; 34:191-195
4. Furman JM, Baloh RW, Yee RD. Eye movement abnormalities in a family with cerebellar vermian atrophy. Acta Otolaryngol
5. Hutton JT, Albrecht JW, Kuskowski M, et al. Abnormal ocular motor function predicts clinical diagnosis of familial ataxia. Neurology 1987;37:698-701
6. Mizutani T, Satoh J, Morimatsu Y. Neuropathological back- ground of oculomotor disturbances in olivopontocerebellar at- rophy with special reference to slow saccade. Clin Neuropathol 1988;7:53-61
7. Al-Din ASN, Al-Kurdi A, A-Salem MK, et al. Autosomal re- cessive ataxia, slow eye movements, dementia, and extrapyrami- dal disturbances. J Neurol Sci 1990;96:191-205
8. Shimizu N, Takiyama Y, Mizuno Y, et al. Characteristics of
(Stockh) 1986;101:371-377
Rivaud-Pechoux et al: Eye Movements in ADCA 301

oculomotor disorders of a family with Joseph‘s disease. J Neurol
9. Al-Din ASN, Al-Kurdi A, Dasouki M, et al. Autosomal reces- sive ataxia, slow eye movements and psychomotor retardation. J Neurol Sci 1994;124:61-66
10. Moschner C, Perlman S, Baloh RW. Comparison of oculomo- tor findings in the progressive acaxia syndromes. Brain 1994; 1 17:15-25
11. Biirk K, Abele M. Fetter M, et al. Autosomal dominant cere- bellar ataxia type I: Clinical features and magnetic resonance imaging findings in families with SCA1, SCA2 and SCA3 mu- tation. Brain 1997;119:1497-1505
12. Klostermann W, Zlihlke C, Heide W, et al. Slow saccades and other eye movement disorders in spinocerebellar atrophy type 1. J Neurol 1997;244:105-111
13. Orr HT, Chung M-Y, Banfi S, et al. Expansion of an unstable trinucleotide CAG repeat in spinocerebellar ataxia type I . Nat Genet 1993;4:221-226
14. Pulst SM, Nechiporuk A, Nechiporuk T, et al. Moderate ex- pansion of a normally biallelic trinucleotide repeat in spinocer- ebellar ataxia type 2. Nat Genet 1996;14:269-276
15. Imbert G, Saudou F, Yvert G, et al. Cloning of the gene for spinocerebellar ataxia 2 reveals a locus with a high sensitivity to expanded CAG/glutamine repeats. Nat Genet 1996; 14:285- 29 1
16. Sanpei K, Takano H, Igarashi S, et al. Identification of the spinocerebellar ataxia type 2 gene using a direct identification of repeat expansion and cloning technique, DIRECT. Nat Genet 1996;14:277-284
17. Kawaguchi Y, Okamoto T, Taniwaki M, et al. CAG expansions in a novel gene for Machado-Joseph disease at chromosome 14q32.1. Nat Genet 1984;8:221-228
18. Cancel G, Abbas N, Stevanin G, et al. Marked phenotypic het- erogeneity associated with expansion of a CAG repeat sequence at the spinocerebellar ataxia 3IMachado-Joseph disease locus. Am J Hum Genet 1995;57:809-816
13. Dubourg 0, Durr A, Cancel G, et al. Analysis of the SCAl CAG repeat in a large number of families with dominant ataxia: clinical and molecular correlations. Ann Neurol 1395;37: 176- 180
20. Durr A, Stevanin G, Cancel G, et al. Spinocerebellar ataxia 3 and Machado-Joseph disease: clinical, molecular, and neuro- pathologicai features. Ann Neurol 1996;33:490-499
21. Cancel G, Durr A, Didierjean 0, et al. Molecular and clinical correlations in spinocerebellar ataxia 2: a study of 32 families. Hum Mol Genet 1997;6:709-715
1990;237:393-398 22. Sweeney JA, Berman RA. Spatial working memory and oculo-
motor control in the elderly. SOC Neurosci Abstr 1995;21(2): 502.2
23. Robinson FR, Straube A, Fuchs AF. Role of the caudal fastigial nucleus in saccade generation: 11. Effects of muscimol inactiva- tion. J Neurophysiol 1993;70:1741-1758
24. Kurzan R, Straube A, Buttner U. The effect of muscimol mi- croinjections into fastigial nucleus on the optokinetic response and the vestibulo-ocular reflex in the alert monkey. Exp Brain Res 1993;94:252-260
25. Zee DS, Yamazaki A, Butler PH, et al. Effect of ablation of flocculus and paraflocculus on eye movements in primate. J Neurophysiol 1981;46:878-899
26. Buttner U, Staube A, Spuler A. Saccadic dysmetria and “intact” smooth pursuit eye movements after bilateral deep cerebellar nuclei lesions. J Neurol Neurosurg Psychiatry 1994;57:832- 834
27. Pierrot-Deseilligny C, Rivaud S, Gaymard B, et al. Cortical control of saccades. Ann Neurol 1995;37:557--567
28. Orozco Diaz G, Nodarse Fleites A, CordovCs Sagaz R, Au- burger G. Autosomal dominant cerebellar ataxia: clinical anal- ysis of 263 patients from homogeneous population in Holguin, Cuba. Neurology 1990;40:1369-1375
29. Lopes-Cendes I, Andermann E, Attig E, et al. Confirmation of the SCA-2 locus as an alternative locus for dominantly inher- ited spinocerebellar ataxias and refinement of the candidate re- gion. Am J Hum Genet 1334;54:774-781
30. Leigh RJ, Zee DS. The neurology of eye movements. Philadelphia: FA Davis, 1991
31. Biittner-Ennever JA, Wadia NH, Sakai H, Schwendeman G. Neuroanatomy of oculomotor structures in olivopontocerebellar atrophy (OPCA) patient with slow saccades. J Ncurol 1985;
32. Durr A, Smadja D, Cancel G, et al. Aucosomal dominanr cer- ebellar ataxia type I in Martinique (French West Indies): clini- cal and neuropathological analysis of 53 patients from three un- related SCA2 families. Brain 1995;118:1573-1581
33. Pierroc-Deseilligny C, Amarenco P, Roullet E, Marteau R. Ver- ma1 infarct with pursuit eye movement disorders. J Neurol Neurosurg Psychiatry 1990;53:519-520
34. Vahedi K, Rivaud S, Amarenco P, Pierrot-Deseilligny C. Hor- izontal eye movement disorders after posterior vermis infarc- tions. J Neurol Neurosurg Psychiatry 1935;58:91-94
232(Supp1):285
302 Annals of Neurology Vol 43 No 3 March 1998









![Ataxia telangiectasia: a reviewataxia, oculocutaneous telangiectasia and frequent pul-monary infection [1]. Definition A-T is an autosomal recessive cerebellar ataxia [2]. It has also](https://img.pdfslide.net/doc/110x75/60c0274fdc425b48211dfd10/ataxia-telangiectasia-a-review-ataxia-oculocutaneous-telangiectasia-and-frequent.jpg)









![Spinocerebellar ataxia: an update · ataxia with pigmentary macular degeneration and con-sists of only SCA 7 [20]. ADCA type 3 refers to ‘pure’ cerebellar ataxia, which includes](https://img.pdfslide.net/doc/110x75/5f60a23d2190f22226185a55/spinocerebellar-ataxia-an-update-ataxia-with-pigmentary-macular-degeneration-and.jpg)