Embed Size (px)
Citation preview

Acta Tropica 76 (2000) 169–173
Factors affecting adverse event reporting during massivermectin treatment for onchocerciasis
C.P. Chijioke *Department of Pharmacology and Therapeutics, Uni6ersity of Nigeria Teaching Hospital, P.M.B. 01129, Enugu,
Enugu State, Nigeria
Received 28 January 1998; received in revised form 9 February 2000; accepted 17 March 2000
Abstract
This study examines the effect of age, sex, dosing round, time of day, and distance from the nurse monitor onadverse event reporting during mass ivermectin administration at Achi, south-east Nigeria. There was a significantincrease in adverse event reporting with age but no significant difference between the sexes. Both compliance and theincidence of reported adverse events were less during the second dosing round than during the first. Only three (2%)out of 144 subjects interviewed gave adverse events as a reason for non-compliance. Significantly fewer adverse eventswere reported as starting at night (22:00–06:00 h) than by day. The effect of distance on adverse event reporting wasnot statistically significant for distances up to 1 km. © 2000 Elsevier Science B.V. All rights reserved.
Keywords: Ivermectin; Adverse events; Onchocerciasis; Pharmaco-epidemiology
www.elsevier.com/locate/actatropica
1. Introduction
Ivermectin distribution has become the main-stay of onchocerciasis control. There has been anexponential rise in ivermectin consumption withover 33 million treatments approved by the Mecti-zan™ Donation Program in 1997 (Mectizan Pro-gram Notes, 1999). Adverse reactions toivermectin may be severe and even life-threatening(De Sole et al., 1989; Chijioke and Okonkwo,1992; Barkwell and Shields 1997; Gardon et al.,1997). Barkwell and Shields (1997), albeit con-tested by Alexander et al. (1998), report an in-
creased death rate following ivermectin treatment.The possibility, of severe toxicity, makes it impor-tant to assess the safety of mass ivermectinchemotherapy. Undetected or unreported toxicitymay result in unwarranted optimism as regardsthe safety of ivermectin, and could account forpoor compliance during subsequent closingrounds. We have investigated this possibility bystudying factors which may influence whether anadverse event is reported or not.
2. Patients and methods
The study was undertaken at Achi in Enugustate, south-eastern Nigeria. A total of 14 189
* Tel.: +234-42-459171; fax: +234-42-253397.E-mail address: [email protected] (C.P. Chijioke).
0001-706X/00/$ - see front matter © 2000 Elsevier Science B.V. All rights reserved.
PII: S 0001 -706X(00 )00074 -7
C.P. Chijioke / Acta Tropica 76 (2000) 169–173170
people from 4090 households were registered in apreliminary census and invited to attend for skinsnip. The first dosing round was undertaken inOctober and November 1990 and the secondround in June and July 1991. Dosing and adverseevent monitoring were all undertaken as previ-ously described (Chijioke and Okonkwo, 1992).Adverse events were graded as mild (did notprevent work), moderate (prevented work) orsevere (confined to bed). Free treatment and ad-vice were provided for adverse reactions.
The effect of distance on adverse event report-ing was studied in detail at Ehuhe village, in Achi,with 1094 inhabitants. It was assumed that thedistance travelled was proportional to that of astraight line connecting the patient’s house to themonitor. The distance was estimated by dividingEhuhe village into ten concentric distance zones,each 100 m wide. The nurse monitors were lo-cated at the centre. The total area of 1 km radiusencompassed 1078 (99%) of the village inhabi-tants. The number of inhabitants in each zonewas compared with the number dosed and thenumber of adverse event reporters in the zone.
A survey was undertaken after the second dos-ing round to investigate the drop in complianceduring the second round, as compared to the first.One hundred and forty-four non-compliant sub-jects were chosen during the follow-up conductedby means of random cluster sampling of house-holds. A structured questionnaire was adminis-tered by the author to ascertain reasons for nottaking ivermectin. These reasons included (A) notwanting to take the drug because (i) the subjectbelieves there is no need for the drug (his/her skinis normal or has improved), (ii) the drug causesadverse reactions, (iii) the subject believes thedrug is not effective and (B) wanting to take thedrug but not receiving it because of (i) a timingproblem (not aware of time of dosing, too busy,too late, away from village), (ii) dosing exclusioncriteria (age under 5, serious illness, pregnancy, orlactation), or (iii) other reasons such as dislike ofskin snip.
Data were computerized and analyzed usingEPI INFO version 5.01b (World Health Organi-zation, Geneva) and SPSS (release 6.0, 1993). Sex,age-group and distance-zone differences in ad-
verse event reporting were assessed by logisticregression analysis. The significance of logisticregression model coefficients was assessed withthe Wald test.
Ethics committees at the World Health Organi-zation and the University of Nigeria TeachingHospital approved the study. The local commu-nity gave informed consent.
3. Results
A total of 3067 individuals underwent skin snipbefore the first dosing round. The prevalence ofskin microfilarial infection was 49% (95% CI 47–51%) and the community microfilarial load was2.6 mf/mg skin. A total of 7556 subjects weredosed during the first round and 992 (13%) re-ported adverse events. The corresponding figuresfor the second round were microfilarial prevalence22% (95% CI 20–24%), community microfilarialload 0.4 mf/mg skin, 4401 dosed and 356 (8%)adverse event reports.
In the survey of 144 subjects to investigatereduced coverage during the second dosing round,reasons for not taking ivermectin were, in decreas-ing order of frequency: timing problem in 72(50%), 58 (40.5%) met exclusion cirteria, beliefthat there is no need for the drug in six (4%),dislike of skin snip in three (2%), and belief thatthe drug is ineffective in two (1.5%). Only threesubjects (2%) gave adverse reactions as a reasonfor non-compliance.
The analyses below refer to adverse events re-ported during the first dosing round. First roundadverse events were mostly mild (964 events, 97%)with just 26 moderate (3%) and two severe events(Chijioke and Okonkwo, 1992).
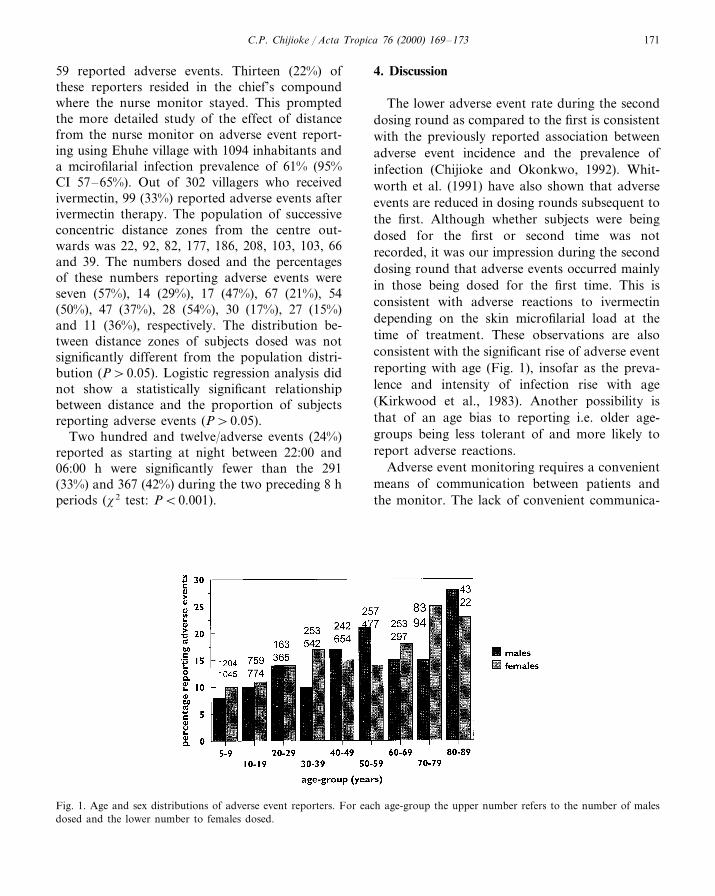
Fig. 1 shows the age and sex distributions ofadverse event reporters. Logistic regression analy-sis shows no significant difference between malesand females in adverse event reporting (P\0.05).There is a significant rise in adverse event report-ing with age (PB0.0001).
At Gbaragu village, in Achi, with 303 inhabi-tants and a microfilarial infection prevalence of76% (95% CI 69–83%), (Okonkwo et al., 1991) itwas observed that out of 232 inhabitants dosed,
C.P. Chijioke / Acta Tropica 76 (2000) 169–173 171
59 reported adverse events. Thirteen (22%) ofthese reporters resided in the chief’s compoundwhere the nurse monitor stayed. This promptedthe more detailed study of the effect of distancefrom the nurse monitor on adverse event report-ing using Ehuhe village with 1094 inhabitants anda mcirofilarial infection prevalence of 61% (95%CI 57–65%). Out of 302 villagers who receivedivermectin, 99 (33%) reported adverse events afterivermectin therapy. The population of successiveconcentric distance zones from the centre out-wards was 22, 92, 82, 177, 186, 208, 103, 103, 66and 39. The numbers dosed and the percentagesof these numbers reporting adverse events wereseven (57%), 14 (29%), 17 (47%), 67 (21%), 54(50%), 47 (37%), 28 (54%), 30 (17%), 27 (15%)and 11 (36%), respectively. The distribution be-tween distance zones of subjects dosed was notsignificantly different from the population distri-bution (P\0.05). Logistic regression analysis didnot show a statistically significant relationshipbetween distance and the proportion of subjectsreporting adverse events (P\0.05).
Two hundred and twelve/adverse events (24%)reported as starting at night between 22:00 and06:00 h were significantly fewer than the 291(33%) and 367 (42%) during the two preceding 8 hperiods (x2 test: PB0.001).
4. Discussion
The lower adverse event rate during the seconddosing round as compared to the first is consistentwith the previously reported association betweenadverse event incidence and the prevalence ofinfection (Chijioke and Okonkwo, 1992). Whit-worth et al. (1991) have also shown that adverseevents are reduced in dosing rounds subsequent tothe first. Although whether subjects were beingdosed for the first or second time was notrecorded, it was our impression during the seconddosing round that adverse events occurred mainlyin those being dosed for the first time. This isconsistent with adverse reactions to ivermectindepending on the skin microfilarial load at thetime of treatment. These observations are alsoconsistent with the significant rise of adverse eventreporting with age (Fig. 1), insofar as the preva-lence and intensity of infection rise with age(Kirkwood et al., 1983). Another possibility isthat of an age bias to reporting i.e. older age-groups being less tolerant of and more likely toreport adverse reactions.
Adverse event monitoring requires a convenientmeans of communication between patients andthe monitor. The lack of convenient communica-
Fig. 1. Age and sex distributions of adverse event reporters. For each age-group the upper number refers to the number of malesdosed and the lower number to females dosed.

C.P. Chijioke / Acta Tropica 76 (2000) 169–173172
tions facilities in developing countries meansthat trained personnel must be available on siteto deal with adverse events after mass iver-mectin admin-istration. If patients or their rela-tions have to walk to report adverse events thena distance bias may arise. In the smaller com-munity of Gbaragu there appeared to be a dis-tance bias but this was not confirmed in thedetailed analysis of Ehuhe village. Distance biasis thus not of concern for adverse event moni-toring zones of up to 1 km radius. This is con-sistent with the mean 2.6 km distance thatsubject are prepared to trek to get ivermectin(Gardon et al., 1996).
Relativley few adverse events were reported asstarting at night (22:00–06:00 h). Even fewerwere actually reported at night: the nurses wereonly woken by adverse event reporters on 15occassions (1.5%), out of 992 adverse events re-ported. Evidently some patients experiencing ad-verse events at night postponed reporting themor did not report them at all. Under-reportingat night suggests that trekking to a central mon-itor is an inadequate arrangement for monitor-ing at night. Nocturnal deterrents to reportinginclude assailants, snakes and scorpions.
Studying factors which influence adverse eventreporting may help to explain the variability ofpublished adverse event rates following iver-mectin administration. Rothova et al. (1989) re-ported a 71% incidence of adverse events,Zea-Flores et al. (1992) reported 67%, Gardonet al. (1997) 26.3%, Pacque et al. (1990) about25%, Chijioke and Okonkwo (1992) 13.1%, andDe Sole et al. (1989) 9.0%. These trials werefairly uniform as regards mobilization and infor-mation of the community, and severity of ad-verse events experienced. The rates above refermainly to adverse events which correspond toour definition of ‘mild’ events. However, the tri-als differed in their method of monitoring. Thestudy by Rothova et al. (1989) was hospital-based while the next three trials quoted aboveinvolved house-to-house visits by monitors seek-ing adverse events. These four studies found anexpectedly higher adverse rate than the last twostudies in which patients had to report to a cen-tral monitor.
This study has shown that factors such astime of day, age and dosing round may affectadverse event reporting. The method of moni-toring also affects the reported adverse eventrate. For a centralized monitoring system, dis-tances of up to 1 km from the nurse monitordo not significantly bias adverse event reporting.These observations should help to standardizeadverse event monitoring, such that reported ad-verse event rates are more comparable.
Acknowledgements
This investigation received financial supportfrom the UNDP/WORLD BANK/WHO SpecialProgramme for Research and Training in Tropi-cal Diseases (TDR). Ivermectin was supplied bythe Mectizan™ Donation Program (Merck andCo.). The contributions by field workers, nurs-ing staff and data entry clerks are acknowl-edged. I thank Professor P.O. Okonkwo for theopportunity to take part in the onchocerciasisresearch programme at Enugu, Nigeria andstudy ivermectin-related adverse events.
References
Alexander, N.D.E., Bockaric, M.J., Kastens, W.A., Kazura,J.W., Alpers, M.P., 1998. Absence of ivermectin-associatedexcess deaths. Trans. R. Soc. Trop. Med. Hyg. 92, 342.
Barkwell, R., Shields, S., 1997. Deaths associated with iver-mectin treatment of scabies. Lancet 349, 1144–1145.
Chijioke, C.P., Okonkwo, P.O., 1992. Adverse events followingmass ivermectin therapy for onchocerciasis. Trans. R. Soc.Med. Hyg. 86, 284–286.
De Sole, G., Remme, J., Awadzi, K., et al., 1989. Adversereactions after large scale treatment of onchocerciasis withivermectin: combined results from eight community trials.Bull. WHO 67, 707–719.
Gardon, J., Mace, J.M., Cadot, E., Ogil, C., Godin, C.,Boussinesq, M., 1996. Ivermectin-based control ofonchocerciasis in nothern Cameroon: individual factorsinfluencing participation in community treatment. Trans. R.Soc. Trop. Med. Hyg. 90, 218–222.
Gardon, J., Gardon-Wendel, N., Ngangue, D., Kamgno, J.,Chippaux, J.P., Boussinesq, M., 1997. Serious reactions aftermass treatment of onchocerciasis with ivermectin in an areaendemic for Loa loa infection. Lancet 350, 18–22.
Kirkwood, B., Smith, P., Marshall, T., Prost, A., 1983. Varia-tions in the prevalence and intensity of microfilarial infec-tions by age, sex, place and time in the area of the
C.P. Chijioke / Acta Tropica 76 (2000) 169–173 173
Onchocerciasis Control Programme. Trans. R. Soc. Trop.Med. Hyg. 77, 857–861.
Mectizan Program Notes, 1999. Issue 22. Mectizan Dona-tion Program, Decatur, Georgia, USA.
Okonkwo, P., Akpa, A., Ihekwaba, A., Nwagbo, D., Umeh,R., Adibua, S., Ezike, V., Ogbuokiri, J., 1991. Studies ononchocerciasis in forest-savannah mosaic areas of Nige-ria. I. Investigations in Gbaragu, Oji River. Ann. Trop.Med. Parasitol. 85, 617–623.
Pacque, M., Munoz, B., Greene, B.M., White, A.T.,Dukuly, Z., Taylor, H.R., 1990. Safety of and compli-ance with community-based ivermectin therapy. Lancet335, 1377–1380.
Rothova, A., Van der Lelij, A., Stilma, J.S., Wilson, W.R.,Barbe, R., 1989. Side effects of ivermectin in treatmentof onchocerciasis. Lancet i, 1439–1441.
Whitworth, J.A., Morgan, D., Maude, G.H., Downham,M.D., Taylor, D.W., 1991. A community trial of iver-mectin for onchocerciasis in Sierra Leone: adverse reac-tions after the first five treatment rounds. Trans. R. Soc.Trop. Med. Hyg. 85, 501–505.
Zea-Flores, R., Richards, F.O., Gonzalez-Peralta, C., et al.,1992. Adverse reactions after community treatment ofonchocerciasis with ivermectin in Guatemala. Trans. R.Soc. Trop. Med. Hyg. 86, 663–666.
.




























