Embed Size (px)
Citation preview
Journal of Critical Care (2010) 25, 112–119
Factors associated with anemia in patients with canceradmitted to an intensive care unit☆
Marylou Cardenas-Turanzas MD, DrPHa,⁎, Mark A. Cesta MDb, Chris Wakefield BS a,Susannah Kish Wallace MSN, RN c, Rudolph Puana MDa,Kristen J. Price MDa, Joseph L. Nates MD, MBA, FCCMa
aDepartment of Critical Care Medicine, The University of Texas M. D. Anderson Cancer Center, Houston, TX 77030, USAbEmergency Health Centre at Willowbrook, Houston, TX 77070, USAcDepartment Medical Informatics, The University of Texas M. D. Anderson Cancer Center, Houston, TX 77030, USA
U
CAfa
0d
Keywords:Anemia;Cancer;Prevalence;Risk factors;Intensive care unit
AbstractPurpose: The study aimed to evaluate the relative impact of clinical and demographic factorsassociated with the prevalence and incidence of anemia (hemoglobin [Hb] b12 g/dL) in critically illpatients with cancer.Materials and Methods: We performed an electronic chart review for demographic and clinical data ofadult patients with cancer with or without anemia admitted to the intensive care unit (ICU). Prevalenceof anemia was determined at admission, and incidence determined if anemia developed during ICUstay. Anemia was classified as mild, moderate, or severe. The additive impact of clinical anddemographic factors was evaluated by using a hierarchical linear regression model.Results: A total of 4705 patients were included in the study. The prevalence and incidence of anemiawere 68.0% and 46.6%, respectively. In prevalent cases, we found that the clinical covariates modifiedsequential organ failure assessment score, admission to the medical ICU, prior chemotherapy, diagnosisof hematologic cancer, and length of hospital stay before ICU admission explained 18.7% of thevariance in the model, whereas the demographic covariates (age, sex, and race) explained only anadditional 0.6%. The pattern was similar for incidence cases.Conclusions: Clinical factors are more influential than demographic factors in the observed rates ofprevalence and incidence of anemia in the ICU; thus, protocols are needed to identify subgroups ofpatients with cancer who could benefit from novel management strategies.© 2010 Elsevier Inc. All rights reserved.
☆ This study was performed at the Department of Critical Care, Theniversity of Texas M. D. Anderson Cancer Center, Houston.⁎ Corresponding author. Division of Anesthesiology, Pain, and Critical
are, Department of Critical Care Medicine, The University of Texas M. D.nderson Cancer Center, Houston, TX 77030, USA. Tel.: +1 713 563 4303;x: +1 713 745 1869.E-mail address: [email protected] (M. Cardenas-Turanzas).
883-9441/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jcrc.2009.02.004
1. Introduction
The prevalence of anemia in patients with cancer has beenwell documented, with rates ranging from 30% to 39% [1-3].In patients with cancer, anemia has been shown to decreaseresponse to chemotherapy and quality of life [4] as well as to

113Factors associated with anemia in patients with cancer
increase the financial burden of the disease [5]. Certainsubgroups of patients are at higher risk of developing anemiaduring the course of the disease, as described by Seshadriet al [3] in a survey of patients with cancer monitored for6 months. Researchers observed that 73% of the patientsreceiving chemotherapy and radiation presented with anemiacompared with only 58% of those receiving chemotherapyalone. The recently completed European Cancer AnaemiaSurvey (ECAS), a large multinational prospective survey,also provided information about the incidence, prevalence,and clinical characteristics (ie, disease status, tumor type, andtreatment status) of anemia in a broad spectrum of patients[2]. Overall, anemia was associated with poor performancestatus; the threshold to start anemia treatment was ahemoglobin (Hb) level of 9.7 g/dL.
The prevalence and incidence of anemia in patients withcancer in need of critical care are not known. Patients withanemia who are admitted to the intensive care unit (ICU)commonly report being more fatigued, have higher mortalityrates, and develop more comorbidities than those admittedwithout anemia [4]. Thus, knowing prevalence and incidencerates will help in identifying groups who may benefit morefrom treatment options.
There are many obstacles in describing the prevalence andincidence of anemia in patients with cancer admitted to theICU. First, a large sample size must be accrued to evaluatethe different types of patients with cancer. Second, the needto adjust for the risk of mortality in a population already veryill is another important factor to take into consideration. Forinstance, most ICU severity-of-illness or risk-of-mortalityscoring systems, such as the Acute Physiology and ChronicHealth Evaluation II, which has been used in cancer research,include the measurement of Hb levels to calculate the score[6]. However, to evaluate cancer-related anemia, the ICUseverity-of-illness scoring system selected for adjustmentshould not include Hb levels in the overall score.
In this study, we evaluated the relative impact of clinicaland demographic factors associated with the prevalence andincidence of anemia in a large sample of patients with canceradmitted into the ICU of a US comprehensive cancer center.
2. Patients and methods
After receiving approval from the institutional reviewboard for this study, we performed a retrospective chartreview of adult patients (those who were 18 years or older)admitted into the ICU at The University of Texas M. D.Anderson Cancer Center, Houston, between September 1,2001, and August 31, 2005. For patients with multiple ICUadmissions during the study period, only the first admissionwas included. Patients younger than 18 years, those whostayed in the ICU 24 hours or less, and those with incompletedemographic information such as race were excluded fromthe study.
2.1. Study outcomes
The Hb levels of patients were measured at ICUadmission, and patients with Hb levels less than 12 g/dLwere diagnosed with anemia. Hemoglobin levels 12 g/dL orhigher were considered normal (anemia not present). Weclassified the severity of anemia as mild (10 g/dL ≤ Hbb 12 g/dL), moderate (8 g/dL ≤ Hb b 10 g/dL), or severe(Hb b 8 g/dL) in accordance with the Common Terminol-ogy Criteria for Adverse Events v3.0 from the NationalCancer Institute [7]. We evaluated the incidence of anemiaduring the ICU stay by using the same cutoff points as thoseused to evaluate the prevalence of anemia at ICU admission.
2.2. Data collection
We analyzed the demographic information collected at thetime of ICU admission (ie, age, sex, race, and marital status).Race was categorized as white, Hispanic, African American,and other. Marital status was classified as married, single,divorced/separated, and widowed.
We also analyzed the clinical information collected at thetime of ICU admission (ie, type of cancer recently treated inthis cancer center, type of admitting ICU [surgical vsmedical], previous cancer treatments, and length of stay[LOS] before the ICU admission). The types of cancer wereclassified as follows: neurologic cancer, thoracic carcinomacancer, gastrointestinal cancer, leukemia or lymphoma, headand neck cancer, genitourinary, gynecological cancer,sarcoma, breast cancer, and other. Patients were classifiedas “surgical” if they were referred to the ICU directly fromthe operating room after a surgical intervention; otherwise,they were classified as “medical.”We found 12 (0.3%) caseswith unknown type of admitting ICU and excluded themfrom the univariate and multivariate analysis. Cancertreatments received during the 8-week period before thedate of ICU admission were categorized as any chemother-apy (alone or in combination with radiotherapy) and none.We recorded the number of days since the date of hospitaladmission to the date of admission to the ICU.
2.3. Sequential organ failure assessmentscoring system
Because the patients admitted to the ICU were diagnosedwith different comorbidities andwere referred to the ICUwithdiverse medical diagnoses, we measured the risk of mortalityby computing a sequential organ failure assessment (SOFA)score at the time of ICU admission. The use of electronicclinical records at our ICU to calculate the SOFA score wasthe main reason for selecting this ICU severity-of-illnessscoring system. The SOFA score utilizes markers of organand system failure to quantify the level of organ dysfunction/failure and risk ofmortality. The SOFA score is composed of ascore from each of 6 organ systems: respiratory (PaO2/FIO2

114 M. Cardenas-Turanzas et al.
ratio), coagulation (platelets/100 000 mm3), hepatic (bilir-ubin level), renal (creatinine or urinary output), cardiovas-cular (hypotension), and neurologic (Glasgow Coma Score[GCS]) [8,9]. Each organ/system is graded from 0 to 4; thus,the total SOFA score ranges from 0 (no dysfunction) to 24(severe dysfunction), with higher scores representing agreater degree of organ dysfunction/failure and, conse-quently, a higher risk of mortality. In our study, we computeda modified SOFA (mSOFA) score, which did not include theGCS (which we lacked) and details on the vasopressor dosesused (which varied widely), to measure the severity of illness.The mSOFA score, then, ranged from 0 to 20, with the higherscores corresponding to higher risks of mortality.
2.4. Statistical analysis
Statistical analysis was performed using SPSS forWindows (version 15.0; SPSS, Inc, Chicago, Ill). Here wereport frequencies and measures of central tendency. Weanalyzed the association between continuous variables andstudy outcomes by using Student t tests and that betweencategorical and ordinal variables by using χ2 tests. Weevaluated the effect of covariates such as age and sex on theassociations between independent variables and outcomevariables. P b .05 was considered statistically significant.
To determine the impact of each variable on studyoutcomes, we constructed multivariate models. With the aimto include all factors potentially associated with the studyoutcomes, we selected independent variables that had a P ≤.20 in the univariate analysis. In constructing the multivariatemodels, the following were analyzed as dichotomousvariables: type of cancer (hematologic vs nonhematologic),race (white vs nonwhite), and cancer treatment received(chemotherapy vs nonchemotherapy). Patients in the che-motherapy group included those who had received che-motherapy alone or in combination with radiotherapy. Agewas included a priori in the models because it is recognizedas an important clinical factor influencing anemia.
Fig. 1 Adult patients with cancer admitted into the ICU duringthe study period.
To study anemia severity, we constructed 2 linearregression models, one for anemia present at ICU admission(prevalence) and one for anemia developed during the ICUstay (incidence).
To examine the relative impact of the clinical ordemographic factors on the severity of prevalent and incidentanemia, we used hierarchical models to separate the effect ofthese variables on the severity of the anemia. Thus, wereported the variance explained by each block of factors(clinical or demographic) separately. In these models, anemiawas categorized as not present, mild, moderate, and severe.
A total of 6285 patients were admitted into the ICU duringthe study period; of these patients, 4705 were eligible forinclusion in this study. A flow chart of patient disposition ispresented in Fig. 1.
3. Results
Clinical and demographic data for the 4705 patientsenrolled in this study are shown in Table 1. As shown, 57%(2699/4705) of the patients were men. The mean age was56.7 years (median age, 58 years), but the men tended to besignificantly older than the women (57.4 vs 55.8 years,respectively) (P b .001). In regard to race, 79% (3700/4705)of the patients were white, but when accounting for sexwithin race, more women than men were nonwhite. Wefound that among Hispanics, 46% were women, 52% of theAfrican Americans were women, and 46% were womenamong other minority groups compared with only 41%women of who were whites (P b .001). Most of the patients(74%; 3452/4705) were admitted into the surgical ICU(SICU), but when adjusting for sex, more men than womenreceived critical care after surgical procedures (75% vs 72%,respectively) (P b .01).
Overall, the mean mSOFA score was 2.47, but we foundpatients admitted to the medical ICU (MICU) had asignificantly higher mean score than those admitted intothe SICU (4.6 vs 1.7, respectively) (P b .001). Thisdifference disappeared when we adjusted for age and sex(data not shown).
In this sample, 25% (1190/4705) of the patients werediagnosed with neurologic cancers followed by thoraciccarcinomas (14%; 634/4705) and gastrointestinal cancers(13%; 630/4705). These 3 types of cancers accounted forslightly more than half (52%) of the cancers diagnosed in thisstudy population. The average LOS before ICU admissionwas 2.2 days, and the medical patients had significantlylonger stays than surgical patients: 4.7 vs 1.3 days,respectively (P b .001) (data not shown).
3.1. Prevalence of anemia at admission
The prevalence of anemia at ICU admission was 68%(3203/4705). Of the total patients enrolled in the study, 38%
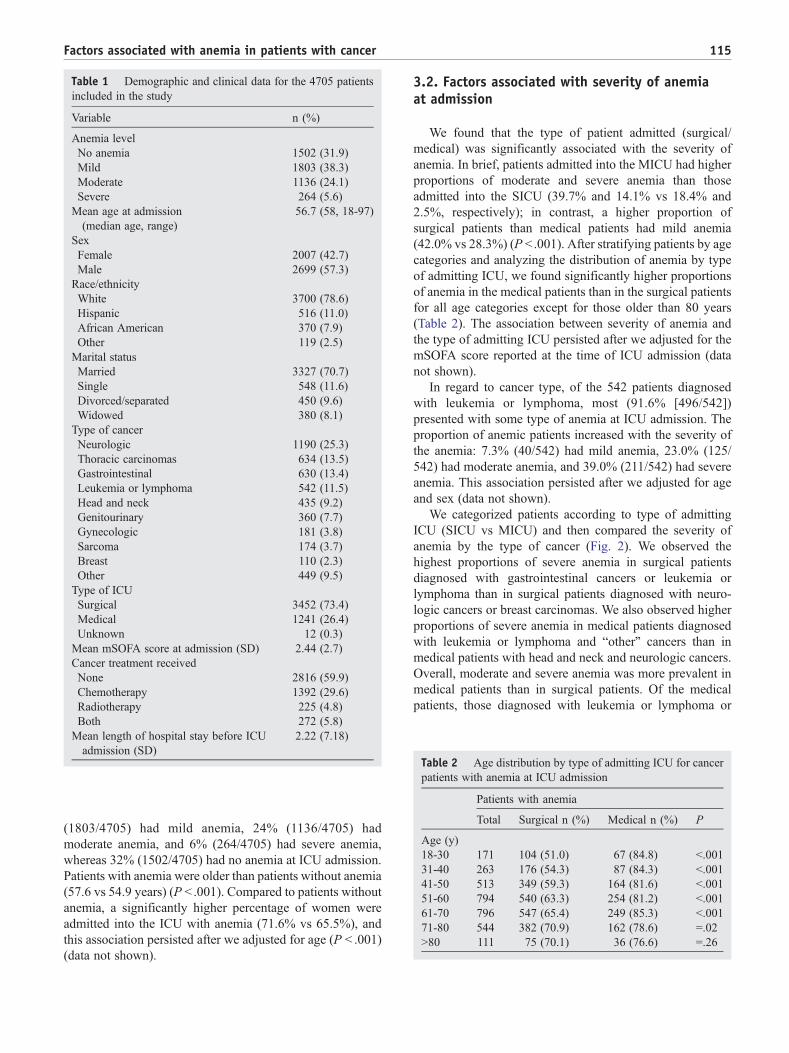
Table 1 Demographic and clinical data for the 4705 patientsincluded in the study
Variable n (%)
Anemia levelNo anemia 1502 (31.9)Mild 1803 (38.3)Moderate 1136 (24.1)Severe 264 (5.6)
Mean age at admission(median age, range)
56.7 (58, 18-97)
SexFemale 2007 (42.7)Male 2699 (57.3)Race/ethnicityWhite 3700 (78.6)Hispanic 516 (11.0)African American 370 (7.9)Other 119 (2.5)Marital statusMarried 3327 (70.7)Single 548 (11.6)Divorced/separated 450 (9.6)Widowed 380 (8.1)
Type of cancerNeurologic 1190 (25.3)Thoracic carcinomas 634 (13.5)Gastrointestinal 630 (13.4)Leukemia or lymphoma 542 (11.5)Head and neck 435 (9.2)Genitourinary 360 (7.7)Gynecologic 181 (3.8)Sarcoma 174 (3.7)Breast 110 (2.3)Other 449 (9.5)
Type of ICUSurgical 3452 (73.4)Medical 1241 (26.4)Unknown 12 (0.3)Mean mSOFA score at admission (SD) 2.44 (2.7)Cancer treatment receivedNone 2816 (59.9)Chemotherapy 1392 (29.6)Radiotherapy 225 (4.8)Both 272 (5.8)
Mean length of hospital stay before ICUadmission (SD)
2.22 (7.18)
Table 2 Age distribution by type of admitting ICU for cancerpatients with anemia at ICU admission
Patients with anemia
Total Surgical n (%) Medical n (%) P
Age (y)18-30 171 104 (51.0) 67 (84.8) b.00131-40 263 176 (54.3) 87 (84.3) b.00141-50 513 349 (59.3) 164 (81.6) b.00151-60 794 540 (63.3) 254 (81.2) b.00161-70 796 547 (65.4) 249 (85.3) b.00171-80 544 382 (70.9) 162 (78.6) =.02N80 111 75 (70.1) 36 (76.6) =.26
115Factors associated with anemia in patients with cancer
(1803/4705) had mild anemia, 24% (1136/4705) hadmoderate anemia, and 6% (264/4705) had severe anemia,whereas 32% (1502/4705) had no anemia at ICU admission.Patients with anemia were older than patients without anemia(57.6 vs 54.9 years) (P b .001). Compared to patients withoutanemia, a significantly higher percentage of women wereadmitted into the ICU with anemia (71.6% vs 65.5%), andthis association persisted after we adjusted for age (P b .001)(data not shown).
3.2. Factors associated with severity of anemiaat admission
We found that the type of patient admitted (surgical/medical) was significantly associated with the severity ofanemia. In brief, patients admitted into the MICU had higherproportions of moderate and severe anemia than thoseadmitted into the SICU (39.7% and 14.1% vs 18.4% and2.5%, respectively); in contrast, a higher proportion ofsurgical patients than medical patients had mild anemia(42.0% vs 28.3%) (P b .001). After stratifying patients by agecategories and analyzing the distribution of anemia by typeof admitting ICU, we found significantly higher proportionsof anemia in the medical patients than in the surgical patientsfor all age categories except for those older than 80 years(Table 2). The association between severity of anemia andthe type of admitting ICU persisted after we adjusted for themSOFA score reported at the time of ICU admission (datanot shown).
In regard to cancer type, of the 542 patients diagnosedwith leukemia or lymphoma, most (91.6% [496/542])presented with some type of anemia at ICU admission. Theproportion of anemic patients increased with the severity ofthe anemia: 7.3% (40/542) had mild anemia, 23.0% (125/542) had moderate anemia, and 39.0% (211/542) had severeanemia. This association persisted after we adjusted for ageand sex (data not shown).
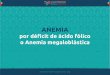
We categorized patients according to type of admittingICU (SICU vs MICU) and then compared the severity ofanemia by the type of cancer (Fig. 2). We observed thehighest proportions of severe anemia in surgical patientsdiagnosed with gastrointestinal cancers or leukemia orlymphoma than in surgical patients diagnosed with neuro-logic cancers or breast carcinomas. We also observed higherproportions of severe anemia in medical patients diagnosedwith leukemia or lymphoma and “other” cancers than inmedical patients with head and neck and neurologic cancers.Overall, moderate and severe anemia was more prevalent inmedical patients than in surgical patients. Of the medicalpatients, those diagnosed with leukemia or lymphoma or
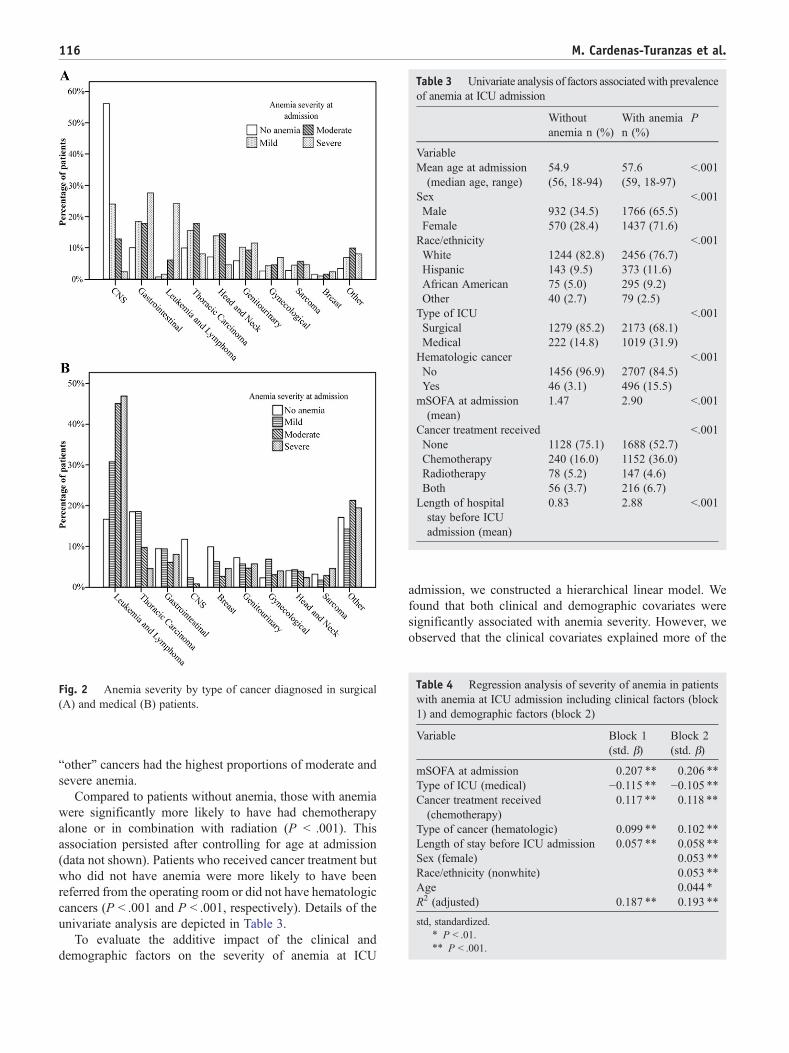
Table 4 Regression analysis of severity of anemia in patientswith anemia at ICU admission including clinical factors (block1) and demographic factors (block 2)
Variable Block 1(std. β)
Block 2(std. β)
mSOFA at admission 0.207 ⁎⁎ 0.206 ⁎⁎
Type of ICU (medical) −0.115 ⁎⁎ −0.105 ⁎⁎Cancer treatment received(chemotherapy)
0.117 ⁎⁎ 0.118 ⁎⁎
Type of cancer (hematologic) 0.099 ⁎⁎ 0.102 ⁎⁎
Length of stay before ICU admission 0.057 ⁎⁎ 0.058 ⁎⁎
Sex (female) 0.053 ⁎⁎
Race/ethnicity (nonwhite) 0.053 ⁎⁎
Age 0.044 ⁎
R2 (adjusted) 0.187 ⁎⁎ 0.193 ⁎⁎
std, standardized.⁎ P b .01.⁎⁎ P b .001.
Fig. 2 Anemia severity by type of cancer diagnosed in surgical(A) and medical (B) patients.
Table 3 Univariate analysis of factors associatedwith prevalenceof anemia at ICU admission
Withoutanemia n (%)
With anemian (%)
P
VariableMean age at admission(median age, range)
54.9(56, 18-94)
57.6(59, 18-97)
b.001
Sex b.001Male 932 (34.5) 1766 (65.5)Female 570 (28.4) 1437 (71.6)Race/ethnicity b.001White 1244 (82.8) 2456 (76.7)Hispanic 143 (9.5) 373 (11.6)African American 75 (5.0) 295 (9.2)Other 40 (2.7) 79 (2.5)Type of ICU b.001Surgical 1279 (85.2) 2173 (68.1)Medical 222 (14.8) 1019 (31.9)
Hematologic cancer b.001No 1456 (96.9) 2707 (84.5)Yes 46 (3.1) 496 (15.5)mSOFA at admission(mean)
1.47 2.90 b.001
Cancer treatment received b.001None 1128 (75.1) 1688 (52.7)Chemotherapy 240 (16.0) 1152 (36.0)Radiotherapy 78 (5.2) 147 (4.6)Both 56 (3.7) 216 (6.7)Length of hospitalstay before ICUadmission (mean)
0.83 2.88 b.001
116 M. Cardenas-Turanzas et al.
“other” cancers had the highest proportions of moderate andsevere anemia.
Compared to patients without anemia, those with anemiawere significantly more likely to have had chemotherapyalone or in combination with radiation (P b .001). Thisassociation persisted after controlling for age at admission(data not shown). Patients who received cancer treatment butwho did not have anemia were more likely to have beenreferred from the operating room or did not have hematologiccancers (P b .001 and P b .001, respectively). Details of theunivariate analysis are depicted in Table 3.
To evaluate the additive impact of the clinical anddemographic factors on the severity of anemia at ICU
admission, we constructed a hierarchical linear model. Wefound that both clinical and demographic covariates weresignificantly associated with anemia severity. However, weobserved that the clinical covariates explained more of the
117Factors associated with anemia in patients with cancer
variance in the model than the demographic covariates(18.7% and 0.6%, respectively) (Table 4).
3.3. Incidence of anemia
Of the 1502 patients without anemia at ICU admission,46.6% (701/1502) developed anemia during the ICU stay.Of these patients, 65.6% (460/701) were eventuallydiagnosed with mild anemia, 29.0% (203/701) withmoderate anemia, and 5.4% (38/701) with severe anemia.In contrast to patients with anemia at ICU admission,patients in whom anemia developed in the ICU were morelikely to be divorced/separated or widowed than to bemarried or single (P b .001). This association persistedafter we adjusted for age (data not shown). Patients whodeveloped anemia in the ICU had significantly longerLOS before admission than those without anemia, 2.6 vs0.5 days, respectively (P b .001), and this differencepersisted after adjusting for the type of ICU admission(surgical or medical) and treatment received (chemother-apy or no chemotherapy).
We found that all the factors significantly predictingincident anemia during ICU stay were similar to thoseassociated with prevalent anemia at ICU admission.
The linear regression model showed that the clinicalcovariates explained 23.6% of the variance in the model,whereas the demographic covariates explained an additional1.7%. Collectively, the 2 blocks of variables explained25.3% of the total variance in this model (Table 5). We foundsignificant interactions between age and admission to theMICU as well as between age and female sex. The trend ofthe interactions suggested that anemia is more likely to beincident in patients of young age admitted to the MICU andmore likely to occur in women of old age (P b .001 and P b.001, respectively) (data not shown).
Table 5 Regression analysis of severity of anemia in patientswho developed anemia during ICU stay including clinicalfactors (block 1) and demographic factors (block 2)
Variable Block 1(std. β)
Block 2(std. β)
mSOFA at admission 0.329 ⁎⁎ 0.324 ⁎⁎
Type of ICU (medical) −0.007 −0.005Cancer treatment received(chemotherapy)
0.094 ⁎⁎ 0.147 ⁎⁎
Type of cancer (hematologic) 0.146 ⁎⁎ 0.105 ⁎⁎
LOS before ICU admission 0.047 ⁎ 0.050 ⁎⁎
Sex (female) 0.072 ⁎⁎
Race/ethnicity (nonwhite) 0.073 ⁎⁎
Age 0.081 ⁎⁎
Marital status (nonmarried) −0.023R2 (adjusted) 0.236 ⁎⁎ 0.253 ⁎⁎
std, standardized.⁎ P b .01.⁎⁎ P b .001.
4. Discussion
This study successfully identified clinicopathologic anddemographic characteristics of patients with cancer that areassociated with anemia in the ICU setting. Specifically, wefound that determinants such as severity-of-illness score,admission to the MICU, prior chemotherapy, diagnosis of ahematologic cancer, and LOS before ICU admission wereindependent clinical prognostic indicators of prevalence ofanemia. The independent demographic determinants werefemale sex, nonwhite ethnicity, and age.
We found a high prevalence and incidence of anemia inpatients with cancer who were admitted into our ICU. Theprevalence of anemia was 68%, and the incidence was46.6%. We also found that up to 23.6% of the varianceexplained in the severity of anemia was attributed to clinicalfactors and up to 1.7% to demographic factors.
Anemia is a common complication in critically illpatients, as well as in patients with cancer. It has beenassociated with an impaired quality of life and a poorprognosis. Quality-of-life issues include lack of self-motiva-tion, sadness, frustration, and fatigue, the latter sometimesbeing so debilitating that patients express feelings that life isnot worth living given the reduced quality associated withanemia [10]. Other studies have observed increased risk ofmortality and complications such as pulmonary edema [1].
Thus, an early assessment of the risk factors for anemiamay help physicians optimize the care of critically ill patientswith cancer.
Several researchers have previously found a highprevalence and incidence of anemia in patients with cancer.For instance, the ECAS [2] reported that the prevalence ofanemia (Hb b 12.0 g/dL) in patients with cancer was 39.3%.We observed a higher rate of prevalence of anemia (68%)than that reported in the ECAS, but we believe this differenceis related to our focus on critically ill patients with cancer (ie,those in need of critical care). It is also noteworthy thatpatients with cancer in need of critical care and who are alsoanemic may require different clinical management of theanemia to improve their outcomes.
The difference between these rates of prevalence may alsobe due to the clinical characteristics of critically ill patientssuch as poor performance status, acute physiologic change,and poor nutrition due to the severity of illness, which mayresult in cancer-related anemia [11,12], especially in thosepatients who had longer LOS before the ICU admission andmay have received more aggressive treatment.
We found that prior chemotherapy was a clinicalprognostic factor of anemia. This was expected becausechemotherapy is a well-known bone marrow depressant andacute cytotoxic agent [13,14]. Medical ICU admission, aclinical factor associated with the prevalence of anemia, wasnot independently associated with the incidence of anemia,but the interactions we found point toward 2 subgroups ofpatients vulnerable to developing anemia after admission:elderly women and young patients with hematologic cancers.

118 M. Cardenas-Turanzas et al.
The development of cancer-related anemia is partly due tothe physiologic response of the immune system to the actionof several cytokines on different iron-homeostasis anderythrocyte- production pathways, which may result inbone marrow suppression [15]. The direct and indirecthemopoietic effects of uncontrolled leukocytosis andcytokine formation are potential causes of anemia in patientswith hematologic malignancies [16]. This would explain ourfinding that incident anemia is more likely to occur in youngpatients admitted to the MICU. Compared to older patients,young patients may receive more aggressive therapies;nevertheless, more research is needed to better understandthe determinants of incident anemia in elderly women withcancer who need critical care.
The last major clinical prognostic indicator of anemia wasseverity of illness, which was measured using an mSOFAscore. We used the SOFA scoring system rather than theAcute Physiology and Chronic Health Evaluation II oranother ICU severity-of-illness scoring system because itdoes not include Hb measurements in its calculation, whichmade it possible for us to independently evaluate the severityof illness as a prognostic indicator of cancer-related anemia.Although an mSOFA score was used owing to the absence ofGCS data and vasopressor doses at ICU admission, this wasnot a limitation of our study because previous studies haveshown that even without a GCS, the SOFA score provides areliable and accurate measure of organ dysfunction/failure[17,18]. Although we lacked GCS information in ourcalculation of the SOFA score, this was not a limitation ofour study. Other researchers have used a similar modificationof the SOFA score. In their prospective, observational cohortstudy, Shime et al [17] concluded that GCS can confound thedegree of neurologic dysfunction in a pediatric sampleadmitted to the ICU because heavy sedation and neuromus-cular blockade are commonly used in these patients. Becausethe reliability of the GCS in pediatric ICU patients can bevariable, the validity of the SOFA score could be negativelyaffected by the inclusion of this score.
Many humeral and direct hematopoietic effects of theseverity of illness in critically ill patients are associated withanemia. Two factors of anemia related to severity of illnessare reduced red blood cell production due to the directinhibitory effects of cytokines on red blood cell genesiswithin the bone marrow and impaired erythropoiesis due toblunted endogenous erythropoietin production [19,20].Other factors involve complicated vascular permeabilitypathways that lead to increased microvascular permeabilityand poor organ perfusion. This increase in microvascularpermeability and decrease in organ perfusion lead todecreased erythropoietin production from the kidneys, directbone marrow suppression, and localized bowel ischemia,which causes nutritional deficiencies such as an iron, folate,or vitamin B12 deficiency [21,22]. A limitation of our studyis the lack of information about anemia treatments, forexample, blood transfusions or erythropoietic therapies,administered before ICU admission. Assuming that some
patients did receive anemia treatments before admission, weobserved a remarkably high prevalence and incidence ofanemia in our study population. We recognize that anemiamay be due to the underlying cause for the ICU referral suchas relapse or exacerbation of the cancer, infection, or renalfailure. In incident cases, blood loss could continue after ICUadmission and only be worsened by an abnormal coagulationor depressed bone marrow function caused by prioradministration of chemotherapy.
Because our study focused on the clinical and demo-graphic factors associated with prevalence and incidence ofanemia in the ICU and not on the impact of anemia on thehealth outcomes of critically ill patients, future researchshould seek to identify the patient populations who maybenefit the most from currently available anemia treatments.Indeed, we need to learn if these anemia therapies have animpact on health outcomes such as survival or LOS inpatients with cancer admitted to the ICU. Our study is a stepin that direction because it provides information that can beused to identify groups of patients at higher risk of anemia.Optimal cancer management should include effective anemiatreatments for these groups.
Acknowledgments
We want to thank Lionel Santibañez and Kate JulietNewberry for their contributions, which enhanced the clarityof the manuscript.
References
[1] Caro JJ, Salas M, Ward A, et al. Anemia as an independent prognosticfactor for survival in patients with cancer: a systemic, quantitativereview. Cancer 2001;91:2214-21.
[2] Ludwig H, Van Belle S, Barrett-Lee P, et al. The European CancerAnaemia Survey (ECAS): a large, multinational, prospective surveydefining the prevalence, incidence, and treatment of anaemia in cancerpatients. Eur J Cancer 2004;40:2293-306.
[3] Seshadri T, Prince HM, Bell DR, et al. The Australian Cancer AnaemiaSurvey: a snapshot of anaemia in adult patients with cancer. Med JAust 2005;182:453-7.
[4] Varlotto J, Stevenson MA. Anemia, tumor hypoxemia, and the cancerpatient. Int J Radiat Oncol Biol Phys 2005;63:25-36.
[5] Lyman GH, Berndt ER, Kallich JD, et al. The economic burden ofanemia in cancer patients receiving chemotherapy. Value Health 2005;8:149-56.
[6] Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity ofdisease classification system. Crit Care Med 1985;13:818-29.
[7] Cancer Therapy Evaluation Program. Common terminology criteriafor adverse events v3.0. NIH, NCI Bethesda, MD; 2006. http://ctep.cancer.gov. Accessed 6/2/09.
[8] Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related OrganFailure Assessment) score to describe organ dysfunction/failure. Onbehalf of the Working Group on Sepsis-Related Problems of theEuropean Society of Intensive Care Medicine. Intensive Care Med1996;22:707-10.
[9] Vincent JL, de Mendonca A, Cantraine F, et al. Use of the SOFA scoreto assess the incidence of organ dysfunction/failure in intensive care

119Factors associated with anemia in patients with cancer
units: results of a multicenter, prospective study. Working group on“sepsis-related problems” of the European Society of Intensive CareMedicine. Crit Care Med 1998;11:1793-800.
[10] Harper P, Littlewood T. Anaemia of cancer: impact on patient fatigueand long-term outcome. Oncology 2005;69:S2-7.
[11] Ludwig H, Strasser K. Symptomatology of anemia. Semin Oncol2001;28(2 Suppl 8):7-14.
[12] Glaspy J. Anemia and fatigue in cancer patients. Cancer 2001;92(6Suppl):1719-24.
[13] Grossi A, Balestri F, Santini S. Darbepoetin alpha in the treatment ofcancer chemotherapy-induced anemia. Ther Clin Risk Manag 2007;3:269-75.
[14] Jessen BA, Lee L, Koudriakova T, et al. Peripheral white blood celltoxicity induced by broad spectrum cyclin-dependent kinase inhibitors.J Appl Toxicol 2007;27:133-42.
[15] Grotto HZ. Anaemia of cancer: an overview of mechanisms involvedin its pathogenesis. Med Oncol 2008;25(1):12-21.
[16] Catalano L, Improta S, de Laurentiis M, et al. Prognosis of chronicmyelomonocytic leukemia. Haematologica 1996;81:324-9.
[17] Shime N, Kageyama K, Ashida H, et al. Application of a modifiedsequential organ failure assessment score in children after cardiacsurgery. J Cardiothorac Vasc Anesth 2001;15(4):463-8.
[18] Ferreira FL, Bota DP, Bross A, et al. Serial evaluation of the SOFAscore to predict outcome in critically ill patients. JAMA 2001;286:1754-8.
[19] Napolitano LM. Scope of the problem: epidemiology of anemia anduse of blood transfusions in critical care. Crit Care 2004;8:S1-8.
[20] Corwin HL. Anemia and blood transfusion in the critically ill patient:role of erythropoietin. Crit Care 2004;8:S42-4.
[21] Puana R, McAllister RK, Hunter FA, et al. Morphine attenuatesmicrovascular hyperpermeability via a protein kinase A–dependentpathway. Anesth Analg 2008;106(2):480-5.
[22] Sanford K. Reintroduction to nutrition and cancer treatment. SeminOncol Nurs 2005;21:164-72.



![[PPT]PEMERIKSAAN LABORATORIUM PADA ANEMIA … · Web viewPEMERIKSAAN LABORATORIUM PADA ANEMIA HEMOLITIK ELLYZA NASRUL Anemia hemolitik - Klasifikasi anemia berdasarkan morfologi anemia](https://img.pdfslide.net/doc/110x75/5c85338309d3f279718c7183/pptpemeriksaan-laboratorium-pada-anemia-web-viewpemeriksaan-laboratorium-pada.jpg)