Embed Size (px)
Citation preview
454
TABLE II—RESPONSE TO FOLIC-ACID ADMINISTRATION IN 2 MALE COMPLETE DENTURE WEARERS WITH ANGULAR CHEILOSIS
Fig. 2-The same patient 1 month after the start of folic-acidadministration; angular cheilosis not present.
cheilosis than in controls, and that there were signifi-cantly more patients with low (<3 ng. per ml.) serum-folate levels than controls. Thus, in the particularsamples selected, angular cheilosis was associated witha low serum-folate level.The further finding that angular cheilosis healed in
two patients whilst on folic-acid therapy and whilsttheir serum-folate levels rose from low to high andnormal, respectively, suggests that the association is acausal one.
Such a conclusion based on only two cases mustobviously be only tentative, and a more extensivecontrolled clinical trial is required. However, thefindings suggest that a deficiency is probably capableof acting as a causative factor in the development ofangular cheilosis.
I thank Prof. S. F. Fish, department of prosthetic dentistry,and Dr. Adam L. Turnbull, medical unit, London Hospital, forvaluable help.
REFERENCES
1. Rose, J. A. PH.D. thesis, University of London, 1971 (to be presented).2. Burket, L. W. Oral Medicine. London, 1965.3. Mäkilä, E. Acta odont. scand. 1969, 27, 655.4. Spray, G. H. J. clin. Path. 1964, 17, 660.5. Siegel, S. Nonparametric Statistics. New York, 1956.
FACTORS INFLUENCING RETURN TO
WORK AFTER MYOCARDIAL INFARCTION
ROBERT NAGLE
RAJAN GANGOLACardiac Department, Selly Oak Hospital, Birmingham 29
IAN PICTON-ROBINSON
British Leyland, Longbridge, Birmingham
Summary 115 patients who had been working atthe time of a myocardial infarct were
examined four months later, when it was found thatonly half of them had returned to work. Organicheart-disease and non-cardiac factors including anxietywere equally common causes of invalidism. Therewas a good correlation between signs of cardiac
damage found at follow-up and those observed duringthe initial few days of the illness.
Introduction
THis study is concerned with the quality of sur-vival after myocardial infarction and, in particular,the factors which determine whether or not a patientwill be able to earn his living. The proportion achiev-ing this in previous surveys has varied from less than50% 1, 2 to more than 80%.3-7
Patients and Methods
The patients were derived from 217 unselected patientsadmitted to the coronary-care unit of this district generalhospital who were shown, by means of the history, electro-cardiogram, and serum-transaminases, to have suffereddefinite myocardial infarction. 40 patients died in hospitaland another 11 before follow-up; 13 failed to attend theclinic and 38 were retired, or housewives at home, at thetime of their acute illness. There were, therefore, 115surviving male employed patients who are the subjectsof this study.Every patient is examined daily on the coronary care
unit by the cardiologist or his registrar for signs of cardiacdamage, which are recorded in coded numerical form.We have classified these signs as minor (breathlessness on
455
exertion, atrial gallop sounds, radiological pulmonaryvenous congestion, persistent tachycardia, or basal crepita-tions) and major, representing more definite and severecardiac damage and including breathlessness at rest, loudatrial or third heart-sounds, abnormal sustained cardiacpulsation either at the apex beat or elsewhere over theprecordium B,9 and radiological cardiac enlargement or pul-monary oedema.The patients were seen at a follow-up clinic between
three and five months after their admission to hospital, andthe same signs of cardiac damage were sought. In addition,attention was paid to the patient’s emotional and mentalstate, and an ordinary physician’s history of these matterswas recorded. No formal psychological testing was carriedout, and the terms " anxiety " and " depression " referto obvious states of mind which were readily apparent andreadily admitted by the patient.
Results
Only 57 (49-5%) out of 115 patients had returnedto work, and this proportion was not significantlydifferent whether they were seen three, four, or fivemonths after the original attack. Older patients,aged 56-65, were less likely to return to work (45%)than younger ones aged 36-45 (56.5%), but thisdifference is not statistically significant.Angina was a symptom in 41 patients and it occurred
on mild exertion in 16. However, the proportion ofpatients with angina who were at work (48-5%) wasno different from that among those free of it (51 %).
Patients who had had more than one infarct weremuch less likely to return to work. Table I shows a
highly significant association between the degree ofcardiac damage, according to our criteria, and returnto work. 6 men with severe, major damage wereable to work, but 30 were still at home despite theabsence of any sign of damage.The signs of cardiac damage at follow-up were
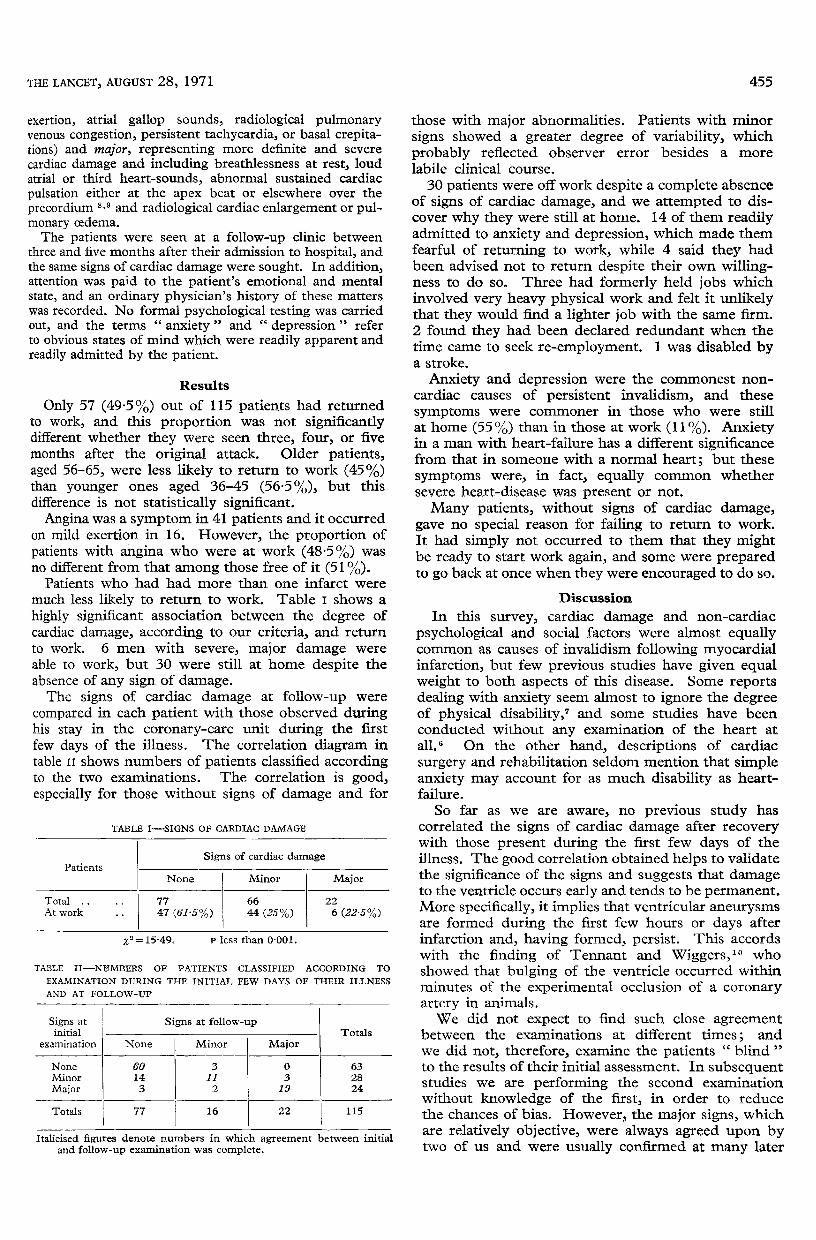
compared in each patient with those observed duringhis stay in the coronary-care unit during the firstfew days of the illness. The correlation diagram intable 11 shows numbers of patients classified accordingto the two examinations. The correlation is good,especially for those without signs of damage and for
those with major abnormalities. Patients with minorsigns showed a greater degree of variability, whichprobably reflected observer error besides a more
labile clinical course.30 patients were off work despite a complete absence
of signs of cardiac damage, and we attempted to dis-cover why they were still at home. 14 of them readilyadmitted to anxiety and depression, which made themfearful of returning to work, while 4 said they hadbeen advised not to return despite their own willing-ness to do so. Three had formerly held jobs whichinvolved very heavy physical work and felt it unlikelythat they would find a lighter job with the same firm.2 found they had been declared redundant when thetime came to seek re-employment. 1 was disabled bya stroke.
Anxiety and depression were the commonest non-cardiac causes of persistent invalidism, and thesesymptoms were commoner in those who were stillat home (55 %) than in those at work (11 %). Anxietyin a man with heart-failure has a different significancefrom that in someone with a normal heart; but thesesymptoms were, in fact, equally common whethersevere heart-disease was present or not.
Many patients, without signs of cardiac damage,gave no special reason for failing to return to work.It had simply not occurred to them that they mightbe ready to start work again, and some were preparedto go back at once when they were encouraged to do so.
Discussion
In this survey, cardiac damage and non-cardiacpsychological and social factors were almost equallycommon as causes of invalidism following myocardialinfarction, but few previous studies have given equalweight to both aspects of this disease. Some reportsdealing with anxiety seem almost to ignore the degreeof physical disability,’ and some studies have beenconducted without any examination of the heart at
all. 6 On the other hand, descriptions of cardiac
surgery and rehabilitation seldom mention that simpleanxiety may account for as much disability as heart-failure.
So far as we are aware, no previous study hascorrelated the signs of cardiac damage after recoverywith those present during the first few days of theillness. The good correlation obtained helps to validatethe significance of the signs and suggests that damageto the ventricle occurs early and tends to be permanent.More specifically, it implies that ventricular aneurysmsare formed during the first few hours or days afterinfarction and, having formed, persist. This accordswith the finding of Tennant and Wiggers, 10 whoshowed that bulging of the ventricle occurred withinminutes of the experimental occlusion of a coronaryartery in animals.We did not expect to find such close agreement
between the examinations at different times; andwe did not, therefore, examine the patients " blind "to the results of their initial assessment. In subsequentstudies we are performing the second examinationwithout knowledge of the first, in order to reducethe chances of bias. However, the major signs, whichare relatively objective, were always agreed upon bytwo of us and were usually confirmed at many later

456
examinations when these patients were studied furtherby cardiac catheterisation. Other prospective studies,such as that of Gorlin et al., tend to confirm ourfindings.We have not considered here the differentiation
between ventricular hypertrophy and ventricular
aneurysm,8,9,11 and which is to be the subject of afuture study. Both indicate a substantial degree ofabnormality and both are classified as major signs.Because of some ambiguity in the current definitionof "cardiac aneurysm", we prefer to diagnose" severe cardiac damage" in cases with abnormal,sustained, precordial cardiac impulses and evidence ofenlargement of the heart. 8,9, 11-13 The possibility ofmisdiagnosing severe cardiac damage in a patient whohas left ventricular hypertrophy due to pre-existinghypertension seems, in fact, to be more theoreticalthan real.Few of our patients had severe angina and, although
our results differ from those of Friedberg, 14 they aresupported by the findings of Solem et al.15 S Therewas no general correlation between angina and failureto work.Our methods of assessing the psychological state
of our patients were less precise than those for thephysical disease, and we hope in the future to applyestablished methods of psychological testing whichmay indicate an even higher prevalence of anxietythan was apparent to us. However, many of ourpatients suffered from simple lack of instruction andreassurance, rather than any formal psychiatric disease,and we regard our principal conclusions as valid.Here our second main finding assumes practical
importance. If cardiac damage, which may cause ill-health later, is present and recognisable during theinitial few days of the illness, then rehabilitation,which should begin during these early days, can bedirected along the right lines from the start with ahigh degree of accuracy. Certain practical measuresto improve the management of patients in this hos-pital immediately suggested themselves as a result ofthis study. 16 Essentially the problem seems to be oneof education of hospital staff, general practitioners,employers, relatives, and the patients themselves.
Requests for reprints should be addressed to R. N.
REFERENCES
1. Pell, S., D’Alonzo, C. A. New Engl. J. Med. 1964, 270, 915.2. Ball, C. O. T., Billings, T., Furman, R. H., Brothers, G. B., Thomas,
J., Meneely, G. R. Circulation, 1955, 11, 749.3. Biorck, G. J. chron. Dis. 1964, 17, 653.4. Master, A. M., Jaffe, H. L., Teich, E. M., Brinberg, L. J. Am. med.
Ass. 1954, 156, 1552.5. Kellerman, J. J., Modan, B., Levy, M., Feldman, S., Kariv, I.
Geriatrics, 1968, 23, 151.6. Wincott, E. A., Caird, F. I. Br. med. J. 1966, ii, 1302.7. Groden, B. M. Scott, med. J. 1967, 12, 297.8. Mourdjinis, A., Olsen, E., Raphael, M. J., Mounsey, J. P. D.
Br. Heart J. 1968, 30, 479.9. Davie, J. C., Langley, J. O., Dodson, W. H., Eddleman, E. E.
Am. Heart J. 1962, 63, 776.10. Tennant, R., Wiggers, C. J. Am. J. Physiol. 1935, 112, 351.11. Gorlin, R., Klein, M. D., Sullivan, J. M. Circulation, 1967, 42, 512.12. Beilin, L., Mounsey, J. P. D. Br. Heart J. 1962, 24, 409.13. Nagle, R. E., Tamara, F. A. ibid. 1967, 29, 735.14. Friedberg, C. K. Diseases of the Heart; p. 878. Philadelphia,
1966.15. Solem, J. H., Helle, I., Jorgensen, W. Acta med. scand. 1963,
174, 315.16. Nagle, R. E., Picton-Robinson, I. Proc. R. Soc. Med. (in the press).
NUTRITIONAL OSTEOMALACIA INIMMIGRANTS IN AN URBAN COMMUNITY
C. H. J. SWANW. T. COOKE
Nutritional and Intestinal Unit, General Hospital,Birmingham 4
Summary Between 1964 and 1970, twenty-fivepatients from Indian or Pakistani fami-
lies presented with osteomalacia at a Birminghamhospital. Not every case could be explained by lowdietary levels of vitamin D, and this, together withevidence of resistance to calciferol in six cases, suggeststhat some Asian immigrants may have a defect atsome point in the conversion of vitamin D2 to its
physiologically active metabolite.
Introduction
OSTEOMALACIA in immigrants to the United King-dom seems to be limited to Indian and Pakistanifamilies. In Glasgow this has been attributed to in-adequate amounts of vitamin D in their diet due inthe main to religious restrictions on various foodsrather than poverty.l We have been impressed at therelative frequency of the disorder in the Midlands, andwe present here our observations on a series of Indianand Pakistani patients referred to this unit between1964 and 1970.
Methods
Full Hæmatological AssessmentHæmoglobin, peripheral blood-film, serum-folate, serum-
vitamin-B12’ and serum-iron and total iron-bindingcapacity were done routinely as part of the screeningprocedures to exclude malabsorption. Haemoglobin wasmeasured by a standard cyanmethæmoglobin technique,while packed-cell volume was obtained from a Hawkesleymicrohsematocrit. Serum-folate (Lactobacillus casei) acti-vity was measured by the aseptic addition method,2 whileserum-vitamin-B12 was measured by the technique of
Meynell et awl. with cyanide addition. 4 Serum-iron andtotal iron-binding capacity were measured by the method ofYoung and Hicks.5Biochemical AssessmentSerum electrolytes, albumin, globulin, calcium, and alka-
line phosphatase were determined by ’AutoAnalyzer’techniques. Urinary calcium excretion and serum-inorganic-phosphorus were not measured routinely. Fæcal fats weredetermined by the van de Kamer method. 6
HistologyIliac-crest bone biopsy was done under local anaesthesia
using a Nicholson-Williams needle, and assessed by thepoint-scoring technique of Garner and Ball.’ 7
Dietary AssessmentThis was done by dietary recall, but was difficult in
some patients, even with the aid of an interpreter.
Results
Sex and Age at Onset of Symptoms (fig. 1) )There were eight men and seventeen women
varying in age from 11 to 36 years, twelve being Paki-stani and thirteen Indian. The men were seen in late
puberty with a mean age of 17-6 years. The women fellinto two groups, a pubertal group of five patients with amean age at diagnosis of 13 -8 years, and an adult post-

















