Embed Size (px)
Citation preview

Familial Idiopathic CardiomegalyBy WAYNE H. SCHRADER, M.D., GEORGE A. PANKEY, M.D.,
RICHARD B. DAVIS, M.D., AND ATHANASIos THEOLOGIDES, M.D.
AMONG CAUSES of cardiac enlargementOf obscure origin that confront the clini-
cian and pathologist alike are subendocardialfibroelastosis, inflammatory myocardiopathies,glycogen-storage disease, amyloidosis, muscu-lar subaortic stenosis,' asymmetrical hyper-trophy of the heart,2 idiopathic myocardi-opathy,3 and familial cardiomegaly. Familialcardiomegaly, originally named in 1949 byEvans,4 has been the subject of many commu-nications, primarily in the European litera-ture, but it is little better understood nowthan after the original report. Various theo-ries to explain the cardiomegaly include car-diac involvement with toxoplasma5 andtrypanosomiasis, a myocardiopathy similarto that seen in Friedreich ataxia but withoutneurologic involvement,4 glycogen-storage dis-ease, and an inheritable disorder of the myo-cardium transmitted as a Mendelian domi-nant,6 with sex linkage. Similar to theenigma of causation, the question of the spe-cificity of the clinical picture and of the au-topsy findings has been controversial with afamilial occurrence being the only unequivo-cal common denominator. Unfortunately, rel-atively little emphasis has been devoted to thecharacter and specificity of the morphologicfindings, with the majority of reports havingappeared in clinical literature.
It is the purpose of this paper to presentthe clinical and necropsy studies of two sisterswho died in young adulthood of progressivecardiac disease. Family history and the sig-nificance of specific anatomic findings are dis-cussed with a few remarks regarding etiology.
Case ReportsCase 1
This 21-year-old white girl was well until age17 years, when she noticed nervousness, tremorof the hands, and a "throbbing" in her neck. At age
From the Departments of Pathology and InternalMedicine, University of Minnesota Hospitals, Minne-apolis, Minnesota.
181/2 years she was told her heart was enlarged,and she received digitalis for 2 months. At age20 she noticed decreased effort tolerance. In Janu-ary 1949, at age 21 years, she was hospitalized fordyspnea and hemoptysis. Two sputum cultureswere positive for tubercle bacilli, but the diagnosisof tuberculosis was not further substantiated. InMarch 1949 she noticed ankle swelling.There was no history of scarlet fever, acute
rheumatic fever, chorea, or tonsillitis. Vertigoand cyanosis had not been present in her child-hood years, and she had tolerated an appendectomyat age 15 without difficulty.Abnormal findings were limited to the heart,
which was enlarged both to the left and to theright. Ectopic ventricular beats were heard butthere were no murmurs.
Electrocardiograms showed left axis deviationand an accelerated atrioventricular conduction pat-tern suggestive of Wolff-Parkinson-White syn-drome. A diagnosis of idiopathic cardiac hyper-trophy was made at cardiac fluoroscopy. Acomplete blood count, erythrocytic sedimentationvelocity, and basal metabolism rate were all nor-mal.The patient gained weight (from 114 to 134
pounds) despite digitalization. On one visit tothe clinic jaundice with hepatomegaly was noted.On July 1, 1949, she had an episode of syncope.On August 19, 1949, she was admitted to the
University of Minnesota Hospitals with severecongestive heart failure. She also gave a historyof occasional hemoptysis and had noted swellingof the right arm. Physical findings included apulse of 110, blood pressure of 90/70, and temper-ature of 98.6 F. At this time a gallop rhythmwas noted at the apex but again no murmurs wereaudible. Physical findings in the right upper ex-tremity were suggestive of thrombophlebitis of theaxillary vein.On August 20, 1949, the patient had a grand
mal seizure following an intravenous injection ofaminophylline. The patient's congestive heartfailure failed to respond, she became semicomatose,and died on September 8, 1949.At necropsy there was moderate pitting edema
of the lower extremities and slight cyanosis of thelips and nailbeds. Approximately 1 liter of clearstraw-colored fluid was present in each pleural.space and in the peritoneal space, and 50 ml. werein the pericardial sac. No pleural or pericardialadhesions were present.
Circulation, Volume XXIV, September 1961 599
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

SCHRADER ET AL.
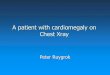
Figure 1Case 1. Section from left ventricle showing atypical area of loose fibrosis surrounded by intactmyocardium. Hematoxylin and eosin stain.
The heart weighed 400 Gm. and was globularin shape. The epicardial surface was pale grayand firm, grayish nodules were present that ex-tended into the myocardium and were surroundedby muscle of softer-than-normal consistency. Thethickness of both ventricular walls varied marked-ly. The very dilated right ventricle measured 2to 3 mm. anteriorly near the apex and was 5 mm.in other areas. The left ventricular wall variedfrom 5 to 15 mm. and revealed diffuse patchyfibrosis. The interventricular septum likewiseshowed rather marked, fine, patchy fibrotic change.In the thinned areas the fibrosis was much more
evident. Underlying the fibrotic area of the leftventricle was a mural thrombus. Remaining en-
docardium, valves, and coronary arteries were un-remarkable.The lungs were heavy, weighing 470 and 425
Gm. each. Several wedge-shaped fresh pulmonaryinfarcts were noted in each lung, but no largepulmonary emboli were found. The lungs exudedbloody fluid when cut. In the right lower lobewere several small, white, nodular areas surround-ing a 1-cm. subpleural firm nodule. This nodulecontained a thick white fluid in its central por-tion. No lymphadenopathy was noted.The liver weighed 1,600 Gm. and grossly re-
vealed the pattern of severe passive congestion.The kidneys and spleen were unremarkable ex-cept for several depressed fibrotic areas over theirsurfaces.
In the right superior parietal area of the brain,a 1.5-cm. circumscribed, firm area was noted withpetechiae scattered through it. Other portions ofthe brain and remaining organs were unremark-able.On microscopic examination multiple sections
of myocardium stained with hematoxylin andeosin showed severe muscular degeneration with
early fibrous replacement in many areas (fig. 1).Hypertrophy, with pallor, granularity and vacuoli-zation of the muscle fibers, was noted. The nucleiwere often swollen or pyknotic and of bizarreshape (fig. 2). A few scattered small mononu-clear cells were present in areas of degeneration.A periodic acid-Schiff stain for glycogen in themyocardial vacuoles revealed only very minimalpositive material. A Giemsa stain of some sec-tions revealed no toxoplasma.The cerebral and pulmonary lesions proved to
be typical granulomatous reactions with centralnecrosis, and epithelioid and Langhans' giant cells.An acid-fast stain of the lung revealed no organ-isms, however. Pulmonary infarets were present,and sections of liver and spleen showed passivecongestion. The remainder of the microscopicexamination was normal.Case 2
This patient, a 17-year-old sister of case 1, gavea history of easy fatigability of many years' dur-ation. At age 12 years cardiomegaly was noted ona routine chest x-ray. At age 14 she began tohave mild exertional dyspnea, which progressedslowly over the next 3 years. Congestive heartfailure was diagnosed and treated with digitalis,low-salt diet, and diuretics. She also noted ver-tigo but had no syncopal episodes. There was nohistory of cyanosis or rheumatic fever.On physical examination abnormal findings in-
cluded pulsating neck veins, cardiomegaly with-out murmurs, protodiastolic gallop rhythm, andhepatomegaly. The clinical impression was famil-ial myocardiopathy.
Electrocardiograms revealed a typical Wolff-Parkinson-White syndrome. Complete blood count,erythrocytic sedimentation rate, and urinalysiswere normal. The patient responded to treat-ment with digitalis and diuretics, and quinidinewas given to prevent arrhythmias.
Three weeks later, on November 6, 1959, thepatient was hospitalized because of increasing con-gestive heart failure and episodes suggestive ofparoxysmal supraventricular tachycardia.
Physical findings were essentially unchangedwith the exception that posterior basilar rales andpedal edema were noted. Again a protodiastolicgallop rhythm was heard, but no murmurs wereaudible. During her hospitalization the patientbecame jaundiced. She also had symptoms of aschizophrenic reaction. Treatment for her con-gestive heart failure was without success and shedied on December 2, 1959.At necropsy 3,000 ml. of clear straw-colored
fluid were removed from the pleural spaces, 2,000ml. from the peritoneum, and 100 ml. from thepericardial sac.
Circulation, Volume XXIV, September 1961
600
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

FAMILIAL IDIOPATHIC CARDIOMEGALY
Figure 2Case 1. Section from periphery of fibrotic area
seen in figure 1. Note the degenerating, pale, finelyvacuolated muscle cell near the upper margin.Giant bizarre nuclei are also present in the musclecells. Hematoxillin and eosin stain.
The heart was globular and massively enlargedto 920 Gm. No pericardial adhesions were pres-
ent. The ventricular walls were thickened. Theleft ventricular wall varied in thickness from 20to 25 mm., and the right ventricular wall measured10 mm. at its thickest cross section (fig. 3). Densewhite fibrous bands extended through the left andright ventricles. The interventricular septum re-
vealed severe fibrous replacement. No evidence ofacute necrosis or gross areas of removal of necroticmuscle were found. The remaining myocardiumwas pale and somewhat soft. No fibrosis of atrialmuscle was evident grossly. The endocardium ofboth ventricles was mildly thickened, but even
after formalin fixation it did not appear like sub-endocardial fibroelastosis. Fresh-appearing muralthrombi were seen in both ventricles. Examinationof valves and of coronary circulation revealed no
congenital or acquired abnormalities.Weights and appearances of lungs, liver, and
spleen were characteristic of severe acute andchronic passive congestion. A small fresh infaretof the left kidney was also present. The remain-ing organs were grossly normal.
Microscopic examination of left ventricular tis-sue revealed massive replacement of structure bydense bands of fibrous connective tissue (fig. 4).Remaining muscle fibers were often pale andgranular or contained clear vacuoles of irregularshape and size. Their nuclei were often of unusualsize and shape, and occasional giant nuclei were
noted. A mild nmononuelear infiltrate was seen inonly a few sections. In the right ventricle andatria only the loose early fibrotic change andsevere vacuolization were present. The sectionsof interventricular septum revealed dense hyalinescar. Special stains were negative for amyloid
Circulation, Volume XXIV, September 1961
Figure 3Case 2. Opened left ventricle showing marked
thickening of ventricular wall and small muralthrombus designated by an arrow. Also qote theslightly thickened endocardium which appears
very fibrous here due to lighting artifact.
with methyl violet, negative for fat with Sudanstains, negative for glycogen with Best's carmine,and negative for toxoplasma and other organismswith Giemsa stain.Mural thrombi were verified on microscopic ex-
amination of both ventricles. The endocardiumwas not remarkably altered in any area.
Sections of lungs, liver, spleen, and pancreasshowed evidence of passive congestion, both acuteand chronic. A small fresh infarct was presentin the right kidney.The large cells of the nuclei tuberes laterales
of the brain were significantly altered. Theneurons were severely swollen, and their distend-ed cytoplasm was filled with faintly eosinophilicgranules. Nissl-stained sections showed only faintstaining of these granules. Fat stains, periodicacid-Schiff stain, and Bielschowsky stain revealedno abnormal structures. Phosphotungstic acid-hematoxylin stain showed no surrounding glialreaction. This entire appearance is without ade-quate explanation.*
The family history of these two sisters was ex-tensively studied. Their mother died at age 34,in 1946. She had been hospitalized elsewhere in1944 for "miiyocardial heart disease and asthma."
*These sections were examined by Dr. L. J.Rubinstein of the London Hospital Medical Collegeand by the Armed Forces Institute of Pathology.It is their opinion that no similar abnormality haspreviously been reported in the literature.
601
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

SCHRADER ET AL.
Figure 4Case 2. Section from left ventricle showing densefibrosis surrounding retained islands of myocar-
dium. This is representative of left ventricularmyocardium. Hematoxylin and eosin stain.
In 1946 she was rehospitalized and a diagnosis of"myocarditis" was made. She was dischargedwith a poor prognosis and died at home. Noautopsy was obtained. One brother of the sistersdied at age 16, when he was hit in the anteriorchest by a baseball. He had been well prior tothat time.
The patient's father, age 54, two sisters, age 28and 30, one brother, age 15, and all five nieces andnephews, age 21/2 to 9 years, were examined. In no
case was there any history suggestive of heartdisease. Physical examination, electrocardiogram,and x-ray studies of the heart failed to show any
abnormalities except that the father was slightlyhypertensive. One brother, age 20, was not avail-able for these studies, but he was known to behealthy and there was no history of heart disease.
CommentThe final, and most complete, classification
of disease entities characterized by cardio-megaly must fall to the pathologist. The usualcauses of an enlarged heart are well knownand need not be dwelt upon here. Reports ofidiopathic cardiomegaly have recently becomemore numerous. This syndrome appears unre-
lated to any known cardiovascular anomalyor to the aging process. It is characterized bya cardiac demise in a young adult with a
large heart and is considered basically a myo-
cardial disease. Autopsy reveals massive en-
largement and dilatation of the heart, pre-
dominantly left-sided, and with or withoutfibrosis. Hypertrophy of myocardial fiberswith patchy vacuolization and fibrosis is seen
microscopically. No evidence of significantendocardial or epicardial abnormality isnoted.
Dr. William Evans described an interestingvariant of this complex in 1949.4 The presenceof a definite familial tendency was suggestedwith his presentation of three families withcardiomegaly and symptomatic heart disease.Since that time several other families havebeen presented as examples of this idiopathicfamilial cardiopathy. A recent excellent re-view by Beasley5 of some 38 cases in 14 fami-lies would seem to verify the existence of suchan entity. The two cases described in this re-port along with their family background areoffered as further evidence of such a familialdisease.
Clinical CommentIt is apparent that many of the reported
cases of familial cardiomegaly had unrecog-nized heart disease for some years as was doc-umented in our second case. The age of onsetof symptoms is highly variable, but is usuallybetween the ages of 5 and 20 years. Dyspneaon exertion, palpitation, giddiness, and synco-pal episodes are common symptoms beforeovert congestive heart failure is manifest.On physical examination most of these pa-
tients appear to be of normal habitus and arewell nourished. Abnormal findings includegeneralized cardiomegaly without a murmur.In those cases that do show murmurs, theymost often are of low intensity and question-able significance. No murmurs were heard ineither of the two present cases. A protodias-tolic gallop or triple rhythm is often heard.As the disease progresses, the signs of left-and right-sided congestive heart failure be-eome increasingly evident. There are no signsor symptoms that are pathognomonic of famil -ial cardiomegaly, however, and the diseasemay be manifest clinically only by suddenunexplained death.
Useful laboratory studies are limited to thex-ray and electrocardiogram. The formershows generalized cardiomegaly with left-sided preponderance but without pulmonarycongestion initially. Electrocardiographic find-ings are quite varied, but most commonly an
Circulation, Volume XXIV, September 1961
602
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

FAMILIAL IDIOPATHIC CARDIOMEGALY
abnormal conduction pattern is found. Thismay be manifest as intraventricular block(usually left bundle), partial atrioventricu-lar block or as the Wolff-Parkinson-Whitesyndrome. The latter should especially alertthe clinician to the possibility of familial car-diomegaly although it occurs in other condi-tions such as Ebstein's anomaly."The age at death varies but most reported
cases have died before 30 years of age.10 Deathusually results from intractable heart failureor the development of an arrhythmia such asparoxysmal supraventricular tachycardia.
Pathologic CommentIn comparing the cases presented here with
those in the literature one notes the followingpoints.
Hearts of previously autopsied cases havebeen markedly enlarged, weighing up to 1,134Gm., with an average of 658 Gm.8 The 920-Gm. heart of our case 2 certainly would fit inthe classification of cardiomegaly, and thesmaller 400-Gm. heart, though only moder-ately enlarged by weight, appeared markedlyenlarged owing to dilatation of the chambers.This rather marked difference in weight isunexplained but suggests that a long-termprocess is involved with heart size possiblydependent on the ability of the patient towithstand the progressive cardiac deteriora-tion. This view is somewhat borne out by ex-amination of the literature, in that cases withthe longest history of symptoms also had thelargest hearts. This is also true in the presentcases with cardiomegaly noted in our secondcase 5 years prior to demise. Increased weightis not a true indication of heart size, however,and the importance of marked dilatation ofthe heart has been stressed by many ob-servers.
Fibrosis varied from dense hyaline scar,predominantly left-sided, to loose, more re-cently developed fibrosis in other areas. Thesmaller heart was also the least fibrotic andshowed much looser fibrosis in the presentcases. By Evans' criteria, fibrosis must bepresent in cases designated as familial cardio-megaly.4 However, cases discussed in 194211Circulation, Volume XXIV, September 1961
showed no fibrosis, yet were considered as thefirst recorded examples of this familial entity.Garrett suggested that the disease should becategorized by the presence or absence of fi-brosis. He noted that both fibrotic and non-fibrotic cases have not been observed in thesame family.12 Such a superficial distinctionhas little merit in the face of the similarity ofthese cases in all other respects. This variableappears to be a manifestation of only one fac-tor, possibly a time factor.Vacuoles were prominent within muscle
fibers in both cases presented. These werenoted in islands of retained muscle fibers sur-rounded by fibrosis and also in the atria andright ventricle where fibrosis was not somarked. Vacuolization has been describedboth with and without associated fibrosis,6' 13
and is thought to represent degenerative, pos-sibly ischemic, change in muscle fibers. Thecontents of these vacuoles do not stain withperiodic acid-Schiff, Best 's carmine, or fatstains.Although endocardial disease is not a sig-
nificant component of this complex, muralthrombosis was present in both of our cases.A high incidence of mural thrombosis andsecondary embolization is not noted in pre-vious cases. Flynn and Mann14 postulated,however, that the dilated ventricle in a fail-ing heart results in decreased emptying anda subsequent decreased oxygen content ofblood to nourish endocardial and subendocar-dial tissues. The damage may result in muralthrombosis and possible Thebesian veinthrombosis.
Etiologic considerations may be dividedinto four main groups: infectious, allergic,mechanical and chemical, and congenital. Thepossibility of a myocarditis as the underlyingcause of progressive myocardial disease wasentertained frequently in discussions of ear-lier isolated cases of cardiomegaly.15' 16 Withthe familial aspects of the syndrome apparent,an infectious etiology has become less attrac-tive, though Sommers17 presented three casesin a family in all of which enlarged heartsshowed active inflammation. Two families de-scribed by Paulley et al.5 showed a high mci-
603
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

SCHRADER ET AL
dence of positive serologic tests for toxoplas-mosis as well as high familial incidence ofcardiomegaly and cardiac symptomatology.The organism was never isolated, however, byexamination of autopsy specimens or by in-oculation studies. Doubt has also been ex-pressed12, 13 that these serologic tests signifytoxoplasma infection and over the postulatedexistence of a special strain involving onlymyocardium that Paulley has suggested. Mul-tiple microscopic sections from both hearts inthe present cases also failed to reveal anytoxoplasma pseudoeysts. The presence of ac-tive tuberculosis in our case 1; in one ofEvans' original cases,4 and in a recent casedescribed by Beasley8 is of some interest. Thatthese were all recent acute infections is ap-parent from the descriptions, and most likelyare related to the cardiac abnormality only byhastening the patient's inevitable demise. In-fection in other recorded cases could hardlybe suspected as an etiology without fever, pre-disposing illness, or microscopic evidence ofan inflammatory reaction.
Allergic diseases such as rheumatic feverand the collagen diseases have been consid-ered. The lack of valvular, vascular, or epi-cardial changes speaks strongly against sucha relationship. The general lack of findings inother organs, the absence of fever, joint symp-toms, skin lesions, and a predisposing hyper-sensitivity reaction in association with thecardiopathy are also of importance. Of thecollagen diseases, systemic scleroderma hasmore in common with familial cardiomegalythan any other. Diffuse fibrosis of heartmuscle with a lack of inflammatory reactionis noted in both. Both may be associated withclinical heart failure, conduction abnormali-ties, and radiographic cardiac enlargement.Here the similarity ends, however. Sclero-derma heart disease is most common as a partof systemic scleroderma and occurs mainly inthe fourth and fifth decades. No specific fa-milial tendency has been noted. Hearts do notundergo the massive enlargement seen in fa-milial cardiomegaly. Fibrosis is more oftenfine and interstitial in type and does not showthe predominant left-sided increase noted in
familial cardiomegaly. Microscopic differ-ences are also apparent with a quite cellularand often very vascular fibrous tissue infiltra-tion with secondary muscular degenerationand replacement in scleroderma. Remainingisolated muscle fibers often appear quite nor-mal, despite being surrounded by fibrous tis-sue.18 The fibrosis in the present two casesdiffers markedly from this, and suggests adegenerative myocardial abnormality with asecondary replacement fibrosis.
Mechanical and chemical changes in theheart can also cause cardiomegaly. Absenceof hypertension, coronary disease, congenitaldefects, valvular disease, or electrolyte ab-normality rules out a likely relationship inthis category.
Recent interest in incomplete subaortic ste-nosis has been expressed by several authors.A report by Brent et al.' described two fami-lies with such a clinical entity. All were char-acterized by cardiomegaly, heart failure, andthe presence of heart murmurs. Walther etal.10 suggested that the progressive familialcardiomegaly with left ventricular hyper-trophy may lead to a partial outflowobstruction. Such obstruction could then bea stimulus for further severe hypertrophy.Descriptions of the hearts in most cases ofidiopathic cardiomegaly, however, includemarked dilatation as well as hypertrophy ofthe cardiac chambers. This plus the absenceof murmurs in a large proportion of patientswith familial cardiomegaly would make un-likely a mechanism like subaortic stenosis.Of interest, also, is the work of McAllen,19
who cited two cases of longstanding potassiumdeficiency that resulted in severe diffuse myo-cardial fibrosis. The hearts were not enlargedsignificantly, however, and degenerative le-sions with necrosis and inflammatory cellscould be seen even in the longstanding de-ficiencies.
Last and most important, is the possibilityof a congenital defect of the myocardium. Thetwo most important abnormalities related tocardiomegaly are Friedreich's ataxia and VonGierke 's disease. The latter has been men-tioned and discarded by most previous au-
Circulation, Volume XXIV, September 1961
604
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

FAMILIAL IDIOPATHIC CARDIOMEGALY
thors because of the following characteristicsof Von Gierke 's disease that are not found inidiopathic cardiomegaly: Involvement ofheart with death prior to 1 year of age; defectin glycogenolysis, i.e., ketosis, hypoglycemia,and abnormal glucose tolerance tests; andmassive glycogen deposits in multiple organs
on autopsy. Evans found a moderate amountof glycogen in the heart of one of his originalcases but thought it was insignificant andcould be seen in any degenerative conditionsuch as heart failure.4 No significant increasein glycogen was found in the present case 2.(Only case 2 was studied with alcohol fixationand Best's carmine stain.)
Friedreich ataxia is often associated withcardiac abnormalities and was suggested byEvans as a related familial congenital abnor-mality. Electrocardiographic findings in 38cases of Friedreich ataxia were reported byEvans in an earlier publication, with signifi-cant abnormality in 10 of these.20 DorothyRussel described myocardiopathy in fourcases of Friedreich ataxia at autopsy. Hyper-
trophy with left predominance, diffuse fibro-sis, and scattered degenerative areas with in-flammation were present.21 Familial tendencyof Friedreich ataxia is apparent, but no fam-ily has been found showing isolated cardio-megaly in one member and Friedreich's dis-ease in another.
Campbell and Turner-Warwick6 have pos-
tulated a genetic basis for idiopathic cardio-megaly and suggested that it is inherited as
a Mendelian dominant. Inheritance onlythrough the maternal half of a family hasbeen demonstrated in several two-generationstudies,7 suggesting sex-linked transmission.Although no autopsy study of the mother was
made in the family presented here, involve-ment of the mother 's heart by an abnormalityof myocardial nature is suggested. Such a
family relationship would not offer any proofof a sex-linked transmission, but would fit thegeneral scheme of such a concept.Of interest is the possible relationship of in-
fantile hypertrophy of the heart to adult myo-cardial disease. The infantile variety alsoshows a marked familial tendency but no fam-
Circulation, Volume XXIV, September 1961
ily has been described showing an adult-infant disease pattern. That the infantilehypertrophic disease is basically myocardialis suggested by the work of Black-Schafferand Turner.22 They postulated an abnormalcell division of myocardium, which may resultin the loss of efficiency of the myocardium dueto shortened fibers. Secondary dilatation andhypertrophy would result, with formation ofendocardial fibrosis in some cases. Althougha basic shortcoming of adult cardiomegaly asa congenital abnormality is the long latentperiod, one could still postulate a basic myo-cardial defect originating in development.Such a concept would necessitate the reachingof "critical size" as described by Linzbach23after which marked myocardial change takesplace. Whether this change involves an anoxicphenomenon due to progressive hypertrophyand decreased vessel-fiber ratio or is due to abasic myocardial fiber abnormality, possiblyenzymatic, with dilatation and degenerationis not known. With present increased interestin histochemical technics, enzymatic studies insubsequent cases may be of real value in clar-ifying a very cloudy disease complex. In orderto accomplish such studies, however, this dis-ease entity must be recognized at the autopsytable or earlier in order that valid metabolicstudies be completed.
SummaryTwo young adult sisters are described with
clinical and pathologic findings of myocardialdisease. These cases along with a suggestivefamily history are presented as examples offamilial idiopathic cardiomegaly. Pathologicfindings are compared and contrasted withthose in the literature, and etiologic conceptsare discussed. It is concluded that a congeni-tal myocardial abnormality is the most likelyetiology and suggestions for further studiesare presented.
AcknowledgmentWe wish to express appreciation to Dr. Jerome
Krovetz, of the Pediatric Department, who examinedthe children in the family under study. We arealso grateful to Miss Josephine Walaszek for hertechnical aid in the preparation of this paper.
605
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

SCHRADER ET AL.
References1. BRENT, L. B., ABURANO, A., FISHER, D. L.,
MORAN, T. J., MYERS, J. D., AND TAYLOR,W. J.: Familial muscular subaortic stenosis.Circulation 21: 167, 1960.
2. TEARE, D.: Asymmetrical hypertrophy of theheart in young adults. Brit. Heart J. 20: 1,1958.
3. LEVY, R. L., AND VON GLAUN, W. C.: Cardiachypertrophy of unknown cause. Am. HeartJ. 28: 714, 1944.
4. EVANS, W.: Familial cardiomegaly. Brit. HeartJ. 11: 68, 1949.
5. PAULLEY, J. W., JONES, R., GREEN, W. P. D.,AND KANE, E. P.: Myocardial toxoplasmosis.Brit. Heart J. 18: 55, 1956.
6. CAMPBELL, M., AND TURNER-WARWICK, M.: Twomore families with cardiomegaly. Brit. HeartJ. 18: 393, 1956.
7. McKuSICK, V. A.: Genetic factors in cardio-vascular diseases. II. Disorders of primarilygenetic etiology. Mod. Concepts Cardiovase.Dis. 28: 547, 1959.
8. BEASLEY, 0. C., JR.: Familial myocardial dis-ease. Am. J. Med. 29: 476, 1960.
9. SCHIEBLER, G., ADAMS, P. JR., AND ANDERSON,R. C.: Familial cardiomegaly in associationwith the Wolff-Parkinson-White syndrome. Am.Heart J. 58: 113, 1959.
10. WALTHER, R. J., MADOFF, I. M., AND ZINNER, K.:Cardiomegaly of unknown cause occurring ina family. New England J. Med. 263: 1104,1960.
11. Case Records of Massachusetts General Hospitalno. 28042. New England J. Med. 226: 158,1942.
12. GARRETT, G., HAY, W. J., AND RICKARDS, A. G.:
Familial cardiomegaly. J. Clin. Path. 12: 355,1959.
13. GAUNT, R. T., AND LECUTIER, M. A.: Familialcardiomegaly. Brit. Heart J. 18: 251, 1956.
14. FLYNN, J. E., AND MANN, F. D.: The presenceand pathogenesis of endocardial and subendo-cardial degeneration, mural thrombi, and throm-boses of the Thebesian veins in cardiac failurefrom causes other than myocardial infarction.Am. Heart J. 31: 757, 1946.
15. LINZBAoH, A. J.: Cber die sogenannte idio-pathische herzhypertrophie. Virchows Arch.path. Anat. 314: 595, 1947.
16. Case Records of Massachusetts General Hospitalno. 28102. New England J. Med. 226: 395,1942.
17. SOMMERS, B.: Problems in clinical diagnosisand classification of ventricular hypertrophyin adults. III. Familial cardiopathy. MinnesotaMed. 39: 153, 1956.
18. HURLEY, J., COE, J., AND WEBER, L.: Sclerodermaheart disease. Am. Heart J. 42: 758, 1951.
19. McALLEN, P. M.: Myocardial changes occurringin potassium deficiency. Brit. Heart J. 17:5, 1955.
20. EVANS, W., AND WRIGHT, G.: The electrocardio-gram in Friedreich disease. Brit. Heart J.4: 91, 1942.
21. RUSSE., D. S.: Myocarditis in Friedreich 'sataxia. J. Path. & Bact. 58: 739, 1946.
22. BLACK-SCHAFFER, B., AND TURNER, M. E.:Hyperplastic infantile cardiomegaly. Am. J.Path. 34: 745, 1958.
23. LINEBACH, A. J.: Die Muskelfaserkonstante unddas Wachstumsgesetz der menschlichen herz-kammern. Virchows Arch. path. Anat. 318:575, 1950.
Though old Fort Crawford on the upper Mississippi has vanished, the results of theexperiments Beaumont conducted within its walls have come down to us with undiminishedluster through more than a hundred years and are an enduring portion of America's giftsto science. "Truth, like beauty," Beaumont wrote, "when unadorned is adorned the most,and in prosecuting these experiments and inquiries I believe I have been guided by itslight." Such is the ideal and such is the faith of the frontiersman in science, and in so faras he is loyal to his convictions he will leave behind him, as Beaumont did in his records,lasting contributions from his fleeting years.-WALTER B. CANNON, M.D., The Way ofAn Investigator. New York, W. W. Norton & Company, Inc., 1945, p. 29.
Circulation, Volume XXIV, September 1961
606
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

ATHANASIOS THEOLOGIDESWAYNE H. SCHRADER, GEORGE A. PANKEY, RICHARD B. DAVIS and
Familial Idiopathic Cardiomegaly
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1961 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.24.3.5991961;24:599-606Circulation.
http://circ.ahajournals.org/content/24/3/599located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from










![arXiv:1705.09850v3 [cs.CV] 27 Sep 2017 · the cardiomegaly localization is that the heart and its sur-rounding region is most responsible for cardiomegaly detec-tion, in contrast](https://img.pdfslide.net/doc/110x75/5e34802d595379010310239f/arxiv170509850v3-cscv-27-sep-2017-the-cardiomegaly-localization-is-that-the.jpg)